PRES+RCVS可逆性脑后部综合征和可逆性脑血管收缩综合征
- 格式:pdf
- 大小:283.75 KB
- 文档页数:4
可逆性脑血管收缩综合征临床表现、影像学特征及鉴别诊断可逆性脑血管收缩综合征是一类较为罕见的脑血管疾病,其特点是大脑中动脉狭窄和扩张可逆性变化,临床表现为严重的头痛、癫痫发作或局灶性神经功能障碍。
常见临床症状霹雳性头痛。
RCVS的主要临床表现为突发剧烈的霹雳性头痛,通常在数秒内达到高峰,持续数天至数周。
头痛发作呈弥漫性,可能位于枕部或顶部,患者常伴有恶心和对光敏感。
虽然大多数患者在数分钟至数小时内疼痛有中等程度的缓解,但接下来仍可能出现突发的严重头痛发作,持续数日。
诱因。
许多RCVS患者的发病与特定诱因有关,如体力活动、急性应激或情绪化状态、Valsalva动作(如用力、咳嗽和打喷嚏)、沐浴和游泳等。
这些诱因可能加重患者的症状,导致病情恶化。
血压。
患者初始血压可能会升高,这可能是由于剧烈头痛、疾病本身或相关因素引起的,对患者的血压进行监测和控制是治疗过程中的重要环节。
神经系统受累。
尽管头痛仍是许多RCVS唯一症状,部分患者可能因基础缺血性脑卒中、脑内出血或可逆性脑水肿而出现局灶性神经功能障碍。
患者可能表现为偏瘫、震颤、反射亢进、共济失调和失语等症状。
视觉障碍也较常见,包括暗点、视物模糊、偏盲和皮质盲等。
影像学特征初始神经影像学检查:在出现广泛脑血管收缩的RCVS患者中,约30%-70%的初始神经影像学检查可能未见异常。
然而,大约75%的住院患者最终会出现脑实质病变。
最常见的病变包括缺血性脑卒中和皮质表面(凸面)非动脉瘤性蛛网膜下腔出血,其次是可逆性血管源性脑水肿和脑实质出血。
图1. RCVS的各类初始神经影像学特点注:(A) 头颅CT血管造影:显示双侧前脑动脉呈经典“香肠串”形态的矢状最大密度投影图像。
(B) 头颅CT:轴向图像显示右额叶上覆盖的蛛网膜下出血(箭头)。
(C) 脑MRI:同一患者的轴向FLAIR图像显示右额蛛网膜下出血(箭头)以及双半球脑沟内的多个点状高信号(箭头),提示扩张的皮质表面动脉存在。

PRES可逆性后部脑病的影像诊断与鉴别诊断概述PRES影像表现鉴别诊断小结概述•PRES:一种可逆性神经系统损伤和特异性影像学表现为主的临床影像学综合症。
•所有人群都可发病,女性多见,儿童也可发病。
•急性-亚急性,雷击样头痛。
•儿童的临床表现多与成人相仿,影像表现多不典型。
临床特征•癫痫多为首发症状。
•视觉异常:视野受损、模糊、幻觉,皮质盲、矢认症、安东综合征。
•精神异常:躁动、不安、淡漠。
•少见表现:小脑综合征、偏瘫。
•CSF:多为正常,可有蛋白的升高。
•EEG:慢波、癫痫改变。
•LDH:升高,提示有内皮细胞损伤。
•高血压急症。
•子痫及子痫前期。
•严重的肾脏疾病。
•自身免疫性疾病。
•使用免疫抑制药物/细胞毒性药物。
发病机制•血压快速增高及高灌注。
•内皮细胞受损。
•血管痉挛继发缺血。
发病机制治疗•高血压:纠正高血压到可控范围,但是要避免降压过快导致缺血。
•子痫前期:目标是在分娩时的血压管理,硫酸镁防止癫痫发作。
•药物导致:逐渐缩小或完全停药。
•低镁血症可能示PRES的病因,因此推荐补充镁作为辅助治疗。
•可复发:在血压未控制好、或者需要继续用药的病人。
影像特点部位:•典型:顶枕叶。
•不典型:额叶、颞叶、小脑、脑干、基底节、深部白质、胼胝体、脊髓。
分布: •双侧对称。
•白质较灰质明显。
影像表现:•典型:血管源性水肿。
•不典型 :出血(5-30%)、强化、弥散受限(11-26%)。
典型影像表现-CT•平扫:双侧顶枕叶斑片状低密度影。
•血管造影:不规则局部或血管多发狭窄(串珠征)、局部血管扩张,最常见于主干和二级分支。
典型影像表现-CT34岁 女 急性淋巴性白血病化疗 甲氨喋呤鞘内注射 出现右侧偏瘫 收缩压200mmHg 串珠征(箭头)血管局部扩张(箭号)24 男坏死性肺炎典型影像表现-MRI•等-稍长T1、长T2信号。
•FLAIR呈高信号。
•DWI呈等高信号、ADC呈高信号。
•MRS:Cho、Cr升高;NAA、NAA/Cr减低;乳酸增加提示缺血。


可逆性脑血管收缩综合征转载自:神经病学医学网一本神经的神经作者:秦伟教授可逆性脑血管收缩综合征(RCVS)在临床上并不罕见,但存在认识不足。
临床中也遇到了这种病例,从怀疑是这个病到找到诊断证据,颇费了一番周折,又想起之前会诊的1例产后多次剧烈头痛的患者,当时脑CT及MRI都是正常的,查到当时的MRA,确信也是RCVS。
看来这个综合征并不少见,查阅了一些资料,做成幻灯,分享给大家!该课件主要基于相关的英文文献,精力有限,错误难免,内容较为粗糙,也未能解释清楚大家普遍有困惑的地方,见谅!——秦伟以上五个病例均来自文献,这些疾病的共同表现就是可逆的颅内动脉多发节段性狭窄。
由此,引出我们将要谈及的内容,RCVSLancet Neurology 2012年一篇综述的摘要,总结了该综合征的情况RCVS于2007年以后才广泛应用,之前有各种称呼,从表现上,都是RCVS该综合征主要以霹雳头痛起病,多有触发因素,有诱因,多次发作,不同时期有不同的并发症,为动态的病程脑组织影像所见就是PRES该例病例更像PRES而非RCVS,未有血管证实,作者认为还是RCVS高分辨核磁的血管壁成像对该病和PACNS的鉴别有重要作用早期的征象可合并存在其他颅内病变常见的影像技术均能用到,复查很重要可能的发病机制,血脑屏障破坏是近期提出的目前的诊断标准一般参考2007年提出的结合该综合征的临床表现,要鉴别霹雳头痛、SAH等该综合征与颈部动脉夹层和偏头痛关系较为密切血管影像学上主要与PACNA鉴别该综合征与PRES的关系,很密切,但是具体的鉴别点没找到1篇妊娠和产后神经急症的综述对产后RCVS和PRES的不同进行了对比,可以参考治疗包括一般处理、对症、药物治疗等预后较好一篇病例报道总结的诊断流程,可资参考,实际工作中,考虑的要比这复杂其实该综合征也很简单,总结起来,就一张表:临床上一是想不到,二是想到了有时不好证实开头提到的病例都是RCVS。
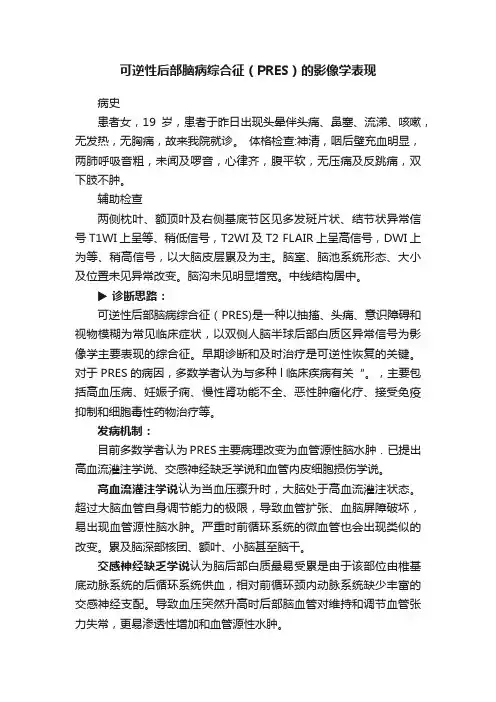
可逆性后部脑病综合征(PRES)的影像学表现病史患者女,19岁,患者于昨日出现头晕伴头痛、鼻塞、流涕、咳嗽,无发热,无胸痛,故来我院就诊。
体格检查:神清,咽后壁充血明显,两肺呼吸音粗,未闻及啰音,心律齐,腹平软,无压痛及反跳痛,双下肢不肿。
辅助检查两侧枕叶、额顶叶及右侧基底节区见多发斑片状、结节状异常信号T1WI上呈等、稍低信号,T2WI及T2 FLAIR上呈高信号,DWI上为等、稍高信号,以大脑皮层累及为主。
脑室、脑池系统形态、大小及位置未见异常改变。
脑沟未见明显增宽。
中线结构居中。
▶诊断思路:可逆性后部脑病综合征(PRES)是一种以抽搐、头痛、意识障碍和视物模糊为常见临床症状,以双侧人脑半球后部白质区异常信号为影像学主要表现的综合征。
早期诊断和及时治疗是可逆性恢复的关键。
对于PRES的病因,多数学者认为与多种l临床疾病有关“。
,主要包括高血压病、妊娠子痫、慢性肾功能不全、恶性肿瘤化疗、接受免疫抑制和细胞毒性药物治疗等。
发病机制:目前多数学者认为PRES主要病理改变为血管源性脑水肿.已提出高血流灌注学说、交感神经缺乏学说和血管内皮细胞损伤学说。
高血流灌注学说认为当血压骤升时,大脑处于高血流灌注状态。
超过大脑血管自身调节能力的极限,导致血管扩张、血脑屏障破坏,易出现血管源性脑水肿。
严重时前循环系统的微血管也会出现类似的改变。
累及脑深部核团、额叶、小脑甚至脑干。
交感神经缺乏学说认为脑后部白质最易受累是由于该部位由椎基底动脉系统的后循环系统供血,相对前循环颈内动脉系统缺少丰富的交感神经支配。
导致血压突然升高时后部脑血管对维持和调节血管张力失常,更易渗透性增加和血管源性水肿。
血管内皮细胞损伤学说认为结缔组织病变等产牛的循环系统内细胞毒素及抗血管内皮细胞抗体引起血管内皮细胞破坏,导致血管源性水肿。
免疫抑制和细胞毒性药物引起PRES的机制可能与药物的直接毒性作用有关。
影像学表现:PRES最突出的影像学表现为双侧大脑半球后部广泛性白质异常。
移植相关护理:可逆性后部脑病综合征可逆性后部脑病综合征简介:可逆性后部脑病综合征(posterior reversible encephalopathy syndrome,PRES)是造血干细胞移植(hematopoietic stem cell transplantation, HSCT)后少见的神经系统并发症之一。
1996年Hinchey最先提出可逆性后部白质脑病综合征(RPLS)这一临床影像综合征。
随着对疾病的进一步认识,发现其还可累及顶枕叶白质以外的其他区域和大脑皮质.于是Casey等[2]提出了后部可逆性脑病综合征(PRES)这一概念。
概念:可逆性脑病综合征(PRES)是一种与多种致病因素相关的临床影像学综合征,以头痛、癫痫发作、精神症状、视觉障碍、意识障碍为主要临床表现,影像学以顶枕叶可逆性脑白质病变为主。
该病如果能够得到及时的诊断与治疗,大部分患者的临床症状及影像学改变可以消失。
病因:可逆性后部脑病综合征病因复杂,与多种基础疾病有关 ,常见原因有高血压脑病、肾脏疾病、肾功能不全、子痫前期或子痫,恶性肿瘤化疗,免疫抑制剂及细胞毒性药物应用的毒性副反应,少数患者产后情绪波动也可引起本病。
常见的可引起PRES的免疫抑制剂及细胞毒性药物包括:甲氨喋呤、环孢素、他克莫司、阿糖胞苷、L—ASP、环磷酰胺、糖皮质激素、顺铂等。
而甲氨蝶呤及环孢素是导致PRES的重要诱因。
发病机制:PRES 发病机制目前尚不十分明确,广泛认为有“高灌注学说”、“脑血管痉挛学说”以及“血管内皮损伤学说”。
高灌注学说:血压升高,超过脑血流的正常自动调节能力,脑血流灌注过度,血管扩张,液体透过血脑屏障外渗至脑实质内产生血管源性水肿。
脑血管痉挛学说:各种原因使脑血管调解机制过度反应,脑血管痉挛,脑组织缺血使血管通透性增加,细胞内液渗透到细胞外间隙导致脑水肿。
血管内皮损伤学说:各种高危因素造成血管内皮细胞损伤,血脑屏障破坏,血管通透性增加,血管内一些水分子和大分子进入脑织间隙造成血管源性水肿。
可逆性后部脑病综合征PRES(可逆性后部脑病综合征)是一种新提出的临床影像综合症,其病因各异,临床诊断困难,如处理不及时,会迅速导致昏迷甚至死亡。
PRES最初由Hinchey等于1996年描述报道,临床主要表现为头痛、视觉障碍、意识改变、癫痫发作等症状,而局灶性神经功能缺损少见。
影像学表现为双侧大脑半球后部广泛性白质异常,如顶枕颞叶,也可累及脑干、小脑、丘脑及其他部位。
其临床及影像学表现具有一定的规律,但其病因各异,是一组异质性疾病。
常见的病因有高血压、先兆子痫/子痫、肾功能衰竭及免疫抑制剂如环孢霉素A、FK-506的应用等。
近年来PRES的病理生理机制已进行了广泛的研究,但目前仍存在争议。
目前存在两种截然相反的理论,早期的理论认为是由于脑血管自我调节机制过度反应导致可逆性的血管痉挛,进而导致脑可逆性的缺血损伤,这种理论的主要依据是在个别患者尤其是子痫患者血管造影时可见到血管痉挛,但多数患者并未见大血管痉挛。
目前大多数学者支持PRES的高灌注学说:体循环血压突然升高超过大脑血管的自动调节能力极限,导致区域性血管扩张,即脑的高灌注,增高的脑灌注压导致血脑屏障破坏,导致局灶性液体、大分子及血细胞外渗引起血管源性水肿和淤点样出血,从病理生理学角度可看作毛细血管渗漏综合症。
脑水肿的部位可能与大脑后部交感神经相对缺乏,大脑后动脉在解剖上的易损性,使其在血压急剧升高时对高灌注和血管痉挛特别敏感有关。
本病影像学最突出的特点是病变的分布特征病变主要分布于后循环供血区,最常见的部位为双侧枕叶对称的皮质下白质。
在PRES影像学所表现的病灶并非损毁性的,而是一种血管源性的脑水肿,并未形成梗死灶,这与绝大多数患者的症状能完全恢复是一致的。
根据PRES 的临床症状和影像学表现,主要应与静脉窦血栓、基底动脉尖综合症、MELAS、出血性脑梗死、脑炎、脑胶质瘤等疾病相鉴别。
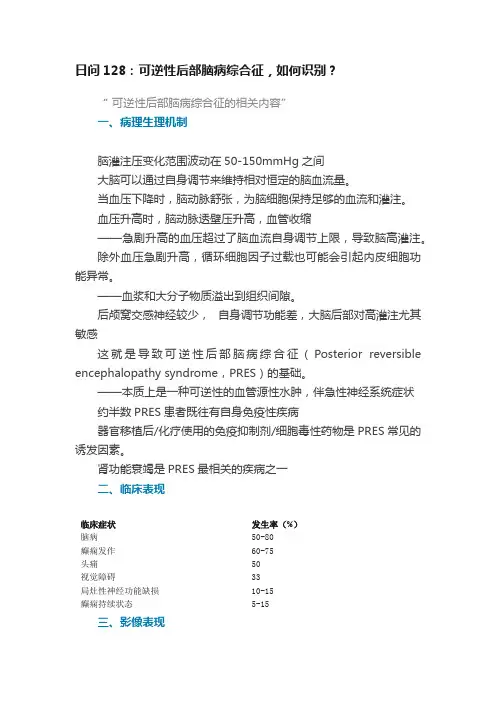
日问128:可逆性后部脑病综合征,如何识别?“可逆性后部脑病综合征的相关内容”一、病理生理机制脑灌注压变化范围波动在50-150mmHg之间大脑可以通过自身调节来维持相对恒定的脑血流量。
当血压下降时,脑动脉舒张,为脑细胞保持足够的血流和灌注。
血压升高时,脑动脉透壁压升高,血管收缩——急剧升高的血压超过了脑血流自身调节上限,导致脑高灌注。
除外血压急剧升高,循环细胞因子过载也可能会引起内皮细胞功能异常。
——血浆和大分子物质溢出到组织间隙。
后颅窝交感神经较少,自身调节功能差,大脑后部对高灌注尤其敏感这就是导致可逆性后部脑病综合征(Posterior reversible encephalopathy syndrome,PRES)的基础。
——本质上是一种可逆性的血管源性水肿,伴急性神经系统症状约半数PRES患者既往有自身免疫性疾病器官移植后/化疗使用的免疫抑制剂/细胞毒性药物是PRES常见的诱发因素。
肾功能衰竭是PRES最相关的疾病之一二、临床表现临床症状发生率(%)脑病50-80癫痫发作60-75头痛50视觉障碍33局灶性神经功能缺损10-15癫痫持续状态5-15三、影像表现(一)典型表现:颅脑MRI典型表现为双侧顶枕叶为主的血管源性水肿,呈T1低信号,T2/FLAIR高信号,DWI等或低信号,ADC高信号。
累及皮质下白质,较少累及皮质。
水肿几乎累及双侧,不完全对称。
(典型的黑水像PRES影像学表现)额叶和颞叶受累者约占75%累及基底节和脑干者有1/3累及小脑者约占半数(均为黑水像;A-C:顶枕型PRES;D-F:全脑分水岭型PRES;G-I:额上回型PRES)(均为黑水像;中央变异型PRES)(二) PRES不常见MRI表现不常见影像学表现发生率(%)弥散受限15-30强化病灶20颅内出血10-25血管造影示血管收缩15-30约15-30%患者在MRI上可见弥散受限。
弥散受限部位通常是位于大片血管源性水肿部位的较小病灶。
可逆性脑血管收缩综合征的临床及影像表现本文原载于《中华放射学杂志》2016年第12期可逆性脑血管收缩综合征(reversible cerebral vasoconstriction syndrome, RCVS)是一组罕见的临床及影像综合征,最早由Call等[1]报道,此后又有类似报道[2,3]。
由于对该综合征认识不足,国内外目前相关文献较少。
现回顾性分析我院3例RCVS患者的临床及影像资料,并结合文献分析,旨在提高对本病的认识及诊断。
一、资料与方法1.临床资料:回顾性分析我院2015年6至10月诊治的3例RCVS患者的临床及影像资料,所有患者的诊断均经临床证实[4]。
3例RCVS患者均为女性,剖宫产术后;年龄分别为35、28和23岁;病程分别为3、1和9 d,均为急性起病。
3例均表现为突发剧烈头痛、肢体抽搐,其中视物模糊2例次、肢体乏力1例次、血压升高1例次。
发病前应用升压药1例、止痛片1例。
既往有明确的偏头痛病史1例。
3例均有不同程度内分泌代谢紊乱,且红细胞沉降率及C反应蛋白(c-reactive protein,CRP)均升高。
脑脊液检查:脑脊液压力230 mmH2O(1 mmH2O=0.0098 kPa),常规及生化正常(1例)。
出院时3例患者临床症状均好转,随访至今无复发。
2.MR扫描:3例患者均行MR平扫和MRA检查,MR增强检查2例,磁敏感加权成像(SWI)2例。
应用德国Siemens Trio Tim 3.0 T超导型MR 仪和32通道头线圈。
扫描参数:轴面SE序列T1WI,TR 2 000.00 ms,TE 9.80 ms,层厚5.0 mm;SE序列T2WI,TR 4 500.00 ms,TE 84.00 ms,层厚5.0 mm;液体衰减反转恢复(FLAIR)序列,TR 8 000.00 ms,TE 94.00 ms,层厚5.0 mm,TI 2 500.00 ms,FOV 220.0 mm×220.0 mm;SWI采用T2*序列,TR27.00ms,TE20.00ms,FOV 230.0 mm×230.0 mm,层厚2.5 mm,层间隔0.2mm,反转角15°。
欧盟采取措施降低伪麻黄碱可逆性后部脑病综合征和可逆性脑
血管收缩综合征风险
佚名
【期刊名称】《中国处方药》
【年(卷),期】2024(22)3
【摘要】近期,欧洲药品管理局的安全委员会(PRAC)建议对含有伪麻黄碱的药物采取新措施,以最大限度地降低可逆性后部脑病综合征(PRES)和可逆性脑血管收缩综合征(RCVS)的风险。
【总页数】1页(PI0001)
【正文语种】中文
【中图分类】R74
【相关文献】
1.产后可逆性脑血管收缩综合征合并可逆性后部白质脑病1例报告
2.常规MRI联合MR脑血管成像在围产期脑后部可逆性脑病综合征中的应用研究
3.加拿大警示含卡铂产品的可逆性后部脑病综合征风险
4.英国警示尼拉帕利的严重高血压及可逆性后部脑病综合征风险
5.全脑血管造影导致可逆性后部脑病综合征1例诊治体会
因版权原因,仅展示原文概要,查看原文内容请购买。
Clinical Reasoning:A 33-year-old woman with severe postpartum occipital headachesNancy Maalouf,MD Sami I.Harik,MDSECTION 1A 33-year-old woman with history of occasional “migraines”complained of severe occipital head-ache,following an uncomplicated full-term vagi-nal delivery under epidural anesthesia.This headache was qualitatively and quantitatively dif-ferent from her usual headaches.The diagnosis of low intracranial pressure headache related to inad-vertent dural puncture was considered and 2epi-dural autologous blood patches were performed with no relief.One week postpartum she pre-sented to an outside hospital with complaints of poor concentration,difficulty in finding words,getting dressed,and feeding herself,and left arm numbness.Examination showed a blood pressure of 179/119mm Hg,poor attention span,apraxia,and decreased sensation in the left hand.General physical examination was unrevealing.Head MRI (day 0)showed fluid-attenuated in-version recovery (FLAIR)hyperintensities (figure 1,A and B)and diffusion restriction with positive apparent diffusion coefficient (ADC)map (figure 1,C and D)in the right parietal lobe and in the splenium of the corpus callosum.The diagnosis of posterior reversible encephalopathy syndromeUpper panel MRI,performed on admission,showed FLAIR hyperintensities and diffusion restriction in the right parietal lobe and in the splenium of the corpus callosum (arrows).Lower panel,done on hospital day 3when the patient deteriorated,showed worsening lesions involving the cortex and subcortical white matter of the parietal,posterior frontal,and occipital lobes,bilaterally (arrows).From theUniversity of Arkansas for Medical Sciences,Little Rock,AR.Disclosure:The authors report no disclosures.Correspondence &reprint requests to Dr.Maalouf:maaloufnancy@RESIDENT &FELLOW SECTIONSection EditorMitchell S.V.Elkind,MD,MS(PRES)was entertained and the patient was treated for that condition with the antihyperten-sive agents nifedipine and lisinopril.The patient’s condition deteriorated.On the third hospital day,she became cortically blind and mute,and had motor perseverations and left-sided weakness. Repeat head MRI showed marked worsening with lesions involving the cortex and subcortical white matter of the parietal,posterior frontal,and occipital lobes,bilaterally(figure1,bottom panel).Question for consideration:1.What is the differential diagnosis?SECTION2The differential diagnosis of multifocal infarcts in the distribution of many vascular territories is wide.It in-cludes emboli from heart and aorta,disseminated intra-vascular coagulopathy,thrombotic thrombocytopenic purpura,moyamoya disease,vasculitis secondary to connective tissue and autoimmune systemic diseases,or viral/bacterial/fungal infections.Another possible rare entity is primary CNS angiitis.The presentation of this patient with postpartum headache,elevated blood pres-sure,and focal neurologic deficits suggested the diagno-sis of PRES to the treating neurologist.The sudden occurrence of severe headache in a young woman postpartum should also raise concern for sentinel headaches and subarachnoid hemorrhage because of their considerable morbidity and mortal-ity and because they are eminently treatable if diag-nosed early.These headaches are usually explosive, reach maximum intensity within minutes,and can last for hours to days.Subarachnoid hemorrhage is usually associated with symptoms and signs of men-ingeal irritation,altered consciousness,and focal neurologic signs.The presence of these signs in a peripartum woman should also raise the possibility of cerebral venous sinus thrombosis.Although these headaches commonly have a subacute onset,they might have a more acute presentation during puerpe-rium.Pituitary apoplexy occurs as well in association with late pregnancy,presenting with acute headache, nausea,decreased visual acuity,ophthalmoplegia, and visual field defects.Question for consideration:1.What studies/tests should be performed?SECTION3In the outside hospital,head magnetic resonance (MR)venography was unrevealing.EEG showed mild diffuse slowing.Lumbar puncture yielded clear CSF that was acellular with normal glucose and pro-tein content.Bacterial and fungal cultures,crypto-coccal antigen,herpes simplex virus PCR,VDRL, and cytology were all negative.Because of clinical deterioration,the patient was transferred to our university hospital where a head CT angiography(CTA)revealed segmental narrowing of many intracranial vessels but primarily involving the vertebral,basilar,posterior,and middle cerebral arteries (figure2,A and B).Transcranial sonography measured increased flow velocities in right middle(170cm/s), right posterior(230cm/s),left middle(130cm/s),and left posterior(140cm/s)cerebral arteries.Vasculitis workup including erythrocyte sedimentation rate,C-reactive protein,rheumatoid factor,antinuclear antibody,anti-neutrophil cytoplasmic antibody,double-stranded DNA,anti-SSA/Ro,anti-SSB/La antibodies,cryoglob-ulin,and angiotensin-converting enzyme was negative.Based on the above,reversible cerebral vasocon-striction syndrome(RCVS)was suspected.The pa-tient was treated with oral nimodipine,60mg every 4hours;aspirin,81mg daily;and methylpred-nisolone,125mg IV every6hours for6days before the results of the vasculitis workup became available. The patient gradually improved:she became more alert but remained apathetic with partial expressive aphasia,apraxia,and perseveration.She perceived light and shades but her visual acuity remained below 20/200.She also had residual mild left hemiparesis with diffuse hyperreflexia and bilateral ankle clonus. Nimodipine was gradually tapered after10days and she was transferred to a rehabilitation facility.Follow-up at2months after discharge showed her to be alert,with near-normal visual acuity(20/25) and intact color vision.She had residual right inferior quadrantanopia,apraxia,mild left hand weakness, and diffuse hyperreflexia.Head MRI showed evi-dence of encephalomalacia in the frontoparietal lobes,left occipital lobe,and splenium of the corpus callosum.Head MR angiography revealed completeresolution of the previously noted vasoconstriction (figure 2,C and D).DISCUSSIONThe most important information re-garding the diagnosis and treatment of this patient was obtained before transfer to our hospital.The findings of positive diffusion-weighted imaging and ADC map in the right parietal lobe and splenium of the corpus callosum was indicative of ischemic stroke which is rarely seen in PRES.1The clinical and MRI worsening after antihypertensive treatment makes the diagnosis of ischemic strokes more convincing.What is the cause of cerebral ischemia?She had no clinical evidence of heart disease.CTA ruled out moyamoya and premature atherosclerosis,and clearly revealed segmental narrowing of large and medium-sized arteries at the base of the brain,highly suggestive of RCVS.RCVS refers to a group of disorders sharing an-giographic and clinical features including reversible segmental and multifocal vasoconstriction of cerebral arteries,and sudden severe headaches with or with-out focal neurologic deficits or seizures.These disor-ders were previously reported as Call-Fleming syndrome,benign angiopathy of the nervous system,and postpartum angiopathy.2The pathophysiology of RCVS remains unknown,though transient distur-bance in the control of cerebral vascular tone was hypothesized.3There is gender preponderance of RCVS in women.Half of the patients give history of mi-graine.2The condition is idiopathic or related to a number of factors,including late pregnancy/post-partum and use of vasoactive substances such as triptans,selective serotonin reuptake inhibitors,pseudoephedrine,cannabinoids,cocaine,amphet-amines,methylenedioxymethamphetamine (ecstasy),bromocriptine,and nasal decongestants.4Postpar-tum angiopathy is an extremely rare complication that usually occurs in a normal pregnancy,as was the case in our patient.Two-thirds of those patients pres-ent in the first postpartum week.5In 50%–70%of cases,it is associated with the use of vasoconstrictors,mostly ergots,to treat postpartum hemorrhage or to inhibit lactation.Intracranial hypotension,whether spontaneous 6or secondary to dural puncture,7was also reported as a possible etiology of RCVS.The diagnosis of RCVS is usually made on ce-rebral arterial imaging which shows diffuse and multifocal segmental narrowing of large and medium-sized arteries.The anterior and posterior brain circulations are involved.Occasional dilated segments,like strings and beads or sausage strings,were described.The diagnosis is confirmed only by documenting reversal of the vasoconstriction within few months.2Vasoactive medications should be stopped.Clini-cal and angiographic resolution occurs spontane-ously;however,calcium channel blockers like nimodipine are used with variable success.Long-term measures include secondary stroke prevention and treatment of complications.6–8A short course of steroids may be justified to cover for cerebral vasculi-tis while awaiting results of workup,although a re-cent retrospective case-series study found worse outcome in patients who received steroids.However,this matter is confounded by the possibility that ste-roids were administered to sicker patients.9The clinical outcome is usually good,with most patients recovering completely within days to weeks.The major complications of RCVS are localized cor-tical subarachnoid hemorrhages (20%–25%of cases)and ischemic strokes (5%–10%).5Hemorrhagic complications and seizures occur earlier (within the first 10days)compared to ischemic events (around 12days from headache onset).2Association with PRES 7and recurrence 10were reported.Patients with severe new-onset headache and focal neurologic deficits must be assessed urgently and sev-eral diagnoses must be considered.Initial diagnosticHead CTA at day 6reveals segmental narrowing of the left middle cerebral artery and the A1segment of the right anterior cerebral artery (A,arrows);segmental narrowing of the posterior cerebral and left distal vertebral arteries with broad narrowing of the basilar ar-tery (B,arrows).Head MRA 2months after discharge shows complete reversal of arterial pathology (C and D).The magnification is similar in all parts of the figure;the white vertical band denotes 5cm.studies should include an unenhanced head CT and lumbar puncture.If both studies are normal,head MRI,MR angiography of the head and neck,and MR venography are necessary.When this workup reveals segmental vasoconstriction,normal or near normal CSF studies,and a lack of any other underly-ing pathology,RCVS should be considered.In the case we presented,PRES was initially suspected,so blood pressure was aggressively controlled,which worsened brain ischemia.Thus,antihypertensive agents should be used with caution in RCVS,just like any other condition causing ischemic strokes.AUTHOR CONTRIBUTIONSDr.Maalouf:drafting/revising the manuscript,study concept or design, analysis or interpretation of data.Dr.Harik:drafting/revising the manu-script,study concept or design,analysis or interpretation of data.REFERENCES1.Finocchi V,Bozzao A,Bonamini M,et al.Magnetic reso-nance imaging in Posterior Reversible Encephalopathy Syndrome:report of three cases and review of literature.Arch Gynecol Obstet2005;271:79–85.2.Ducros A,Boukobza M,Porcher R,Sarov M,Valade D,Bousser MG.The clinical and radiological spectrum ofreversible cerebral vasoconstriction syndrome:a prospec-tive series of67patients.Brain2007;130:3091–3101. 3.Schwedt TJ,Matharu MS,Dodick DW.Thunderclapncet Neurol2006;5:621–631.4.Calabrese LH,Dodick DW,Schwedt TJ,Singhal AB.Narrative review:reversible cerebral vasoconstriction syn-dromes.Ann Intern Med2007;146:34–44.5.Ducros A,Bousser MG.Reversible cerebral vasoconstric-tion syndrome.Pract Neurol2009;9:256–267.6.Schievink WI,Maya MM,Chow W,Louy C.Reversiblecerebral vasoconstriction in spontaneous intracranial hy-potension.Headache2007;47:284–287.7.Chaves C,Freidberg SR,Lee G,Zerris V,Ries S,ChavaliR.Cerebral vasospasm following intracranial hypotension caused by cerebrospinal fluid leak from an incidental lum-bar durotomy:case report.J Neurosurg2005;102:152–155.8.Calado S,Viana-Baptista M.Benign cerebral angiopathy;postpartum cerebral angiopathy:characteristics and treat-ment.Curr Treat Options Cardiovasc Med2006;8:201–212.9.Singhal AB,Hajj-Ali RA,Topcuoglu MA,et al.Reversiblecerebral vasoconstriction syndromes:analysis of139cases.Arch Neurol2011;68:1005–1012.10.Ursell MR,Marras CL,Farb R,Rowed DW,Black SE,Perry JR.Recurrent intracranial hemorrhage due to post-partum cerebral angiopathy:implications for manage-ment.Stroke1998;29:1995–1998.。