利塞膦酸钠的波谱学数据和结构确证
- 格式:doc
- 大小:26.50 KB
- 文档页数:3
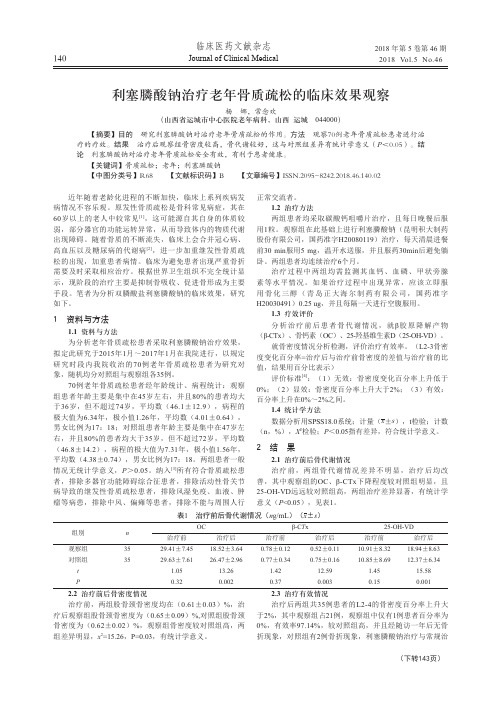
临床医药文献杂志Journal of Clinical Medical 2018 年第 5 卷第 46 期2018 Vol.5 No.46140利塞膦酸钠治疗老年骨质疏松的临床效果观察杨 娜,常念欢(山西省运城市中心医院老年病科,山西运城 044000)【摘要】目的 研究利塞膦酸钠对治疗老年骨质疏松的作用。
方法 观察70例老年骨质疏松患者进行治疗的疗效。
结果 治疗后观察组骨密度较高,骨代谢较好,这与对照组差异有统计学意义(P<0.05)。
结论 利塞膦酸钠对治疗老年骨质疏松安全有效,有利于患者健康。
【关键词】骨质疏松;老年;利塞膦酸钠【中图分类号】R68 【文献标识码】B 【文章编号】ISSN.2095-8242.2018.46.140.02近年随着老龄化进程的不断加快,临床上系列疾病发病情况不容乐观。
原发性骨质疏松是骨科常见病症,其在60岁以上的老人中较常见[1],这可能源自其自身的体质较弱,部分器官的功能运转异常,从而导致体内的物质代谢出现障碍。
随着骨质的不断流失,临床上会合并冠心病、高血压以及糖尿病的代谢病[2],进一步加重继发性骨质疏松的出现,加重患者病情。
临床为避免患者出现严重骨折需要及时采取相应治疗。
根据世界卫生组织不完全统计显示,现阶段的治疗主要是抑制骨吸收、促进骨形成为主要手段。
笔者为分析双膦酸盐利塞膦酸钠的临床效果,研究如下。
1 资料与方法1.1 资料与方法为分析老年骨质疏松患者采取利塞膦酸钠治疗效果,拟定此研究于2015年1月~2017年1月在我院进行,以规定研究时段内我院收治的70例老年骨质疏松患者为研究对象,随机均分对照组与观察组各35例。
70例老年骨质疏松患者经年龄统计、病程统计:观察组患者年龄主要是集中在45岁左右,并且80%的患者均大于36岁,但不超过74岁,平均数(46.1±12.9),病程的极大值为6.34年,极小值1.26年,平均数(4.01±0.64),男女比例为17:18;对照组患者年龄主要是集中在47岁左右,并且80%的患者均大于35岁,但不超过72岁,平均数(46.8±14.2),病程的极大值为7.31年,极小值1.56年,平均数(4.38±0.74),男女比例为17:18。

利塞膦酸钠的合成研究张秀立;张宇佳;王璐璐;方夏琴;陈少华;相莉;刘盟盟;郑稳生【摘要】目的合成新型抗骨质疏松药利塞膦酸钠.方法以烟酸为原料,经酯化、缩合、Willgerodt反应和水解等步骤得到关键中间体3-吡啶乙酸盐酸盐,3-吡啶乙酸盐酸盐与亚磷酸反应后得到利塞膦酸钠.结果在合成过程中,通过探讨Willgerodt 反应的时间和反应条件以及产率,优化合成路线,提高总反应收率.结论此合成路线使利塞膦酸钠的合成方法能较好地适用于工业化生产.【期刊名称】《药学实践杂志》【年(卷),期】2013(031)006【总页数】3页(P448-450)【关键词】利塞膦酸钠;抗骨质疏松药;化学合成【作者】张秀立;张宇佳;王璐璐;方夏琴;陈少华;相莉;刘盟盟;郑稳生【作者单位】中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050;中国医学科学院药物研究所,药物传输技术及新型制剂北京市重点实验室,北京100050【正文语种】中文【中图分类】R914.5随着社会老龄化程度的加剧,骨质疏松症患者数量在逐年增多。
目前,骨质疏松症已跃居世界常见多发病第7位,我国目前有8 400万人患有不同程度的骨质疏松症,尤其是绝经期后的妇女发病率更高。
利塞膦酸钠(risedronate sodium),化学名为2-(3-吡啶基)-1-羟基乙烷-1,1-双膦酸酸单钠盐,是一种吡啶二膦酸盐类骨吸收抑制剂,主要通过降低血清中的钙浓度来保护骨的吸收从而抑制骨的转化,最终增强骨的骨质坚固能力。

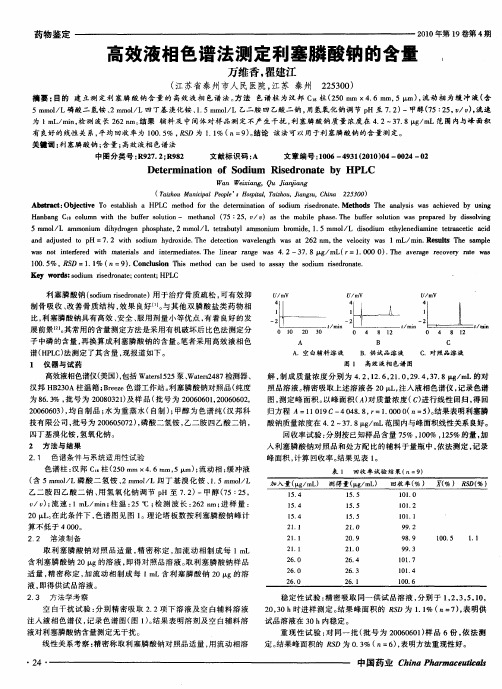
高效液相色谱法测定利塞膦酸钠的含量万维香;瞿建江【摘要】目的建立测定利塞膦酸钠含量的高效液相色谱法.方法色谱柱为汉邦C18柱(250mm×4.6 mm,5μm),流动相为缓冲液(含5 mmol/L磷酸二氢铵、2 mmol/L四丁基溴化铵、1.5 mmol/L乙二胺四乙酸二钠,用氢氧化钠调节pH至7.2)-甲醇(75:25,v/v),流速为1 mL/min,检测波长262 nm.结果辅料及中间体对样品测定不产生干扰,利塞膦酸钠质量浓度在4.2~37.8 μg/mL范围内与峰面积有良好的线性关系,平均回收率为100.5%.RSD为1.1%(n=9).结论该法可以用于利塞膦酸钠的含量测定.【期刊名称】《中国药业》【年(卷),期】2010(019)004【总页数】2页(P24-25)【关键词】利塞膦酸钠;含量;高效液相色谱法【作者】万维香;瞿建江【作者单位】江苏省泰州市人民医院,江苏,泰州,225300;江苏省泰州市人民医院,江苏,泰州,225300【正文语种】中文【中图分类】R927.2:R982利塞膦酸钠(sodium risedronate)用于治疗骨质疏松,可有效抑制骨吸收、改善骨质结构,效果良好[1]。
与其他双膦酸盐类药物相比,利塞膦酸钠具有高效、安全、服用剂量小等优点,有着良好的发展前景[2]。
其常用的含量测定方法是采用有机破坏后比色法测定分子中磷的含量,再换算成利塞膦酸钠的含量。
笔者采用高效液相色谱(HPLC)法测定了其含量,现报道如下。
高效液相色谱仪(美国),包括Waters1525泵、Waters2487检测器、汉邦HB230A柱温箱;Breeze色谱工作站。
利塞膦酸钠对照品(纯度为86.3%,批号为 20080321)及样品(批号为 20060601,20060602,20060603),均自制品;水为重蒸水(自制);甲醇为色谱纯(汉邦科技有限公司,批号为200605072),磷酸二氢铵,乙二胺四乙酸二钠,四丁基溴化铵,氢氧化钠。

反相离子对高效液相色谱法用于利塞膦酸钠有关物质的分离与测定张卫民;杨杰;吴拥军【摘要】建立利塞膦酸钠与有关物质的反相离子对高效液相色谱分离与分析方法.方法:固定相为Hypersil BDSC18柱(250 mm ×4.6 mm,5μm);流动相为甲醇—水(含5 mmol/L磷酸二氢铵,2 mmol/L四丁基溴化铵,1.5mmol/L乙二胺四乙酸二钠)(25∶75,体积分数),流速为0.8 mL/min,检测波长为262 nm.结果:在该色谱条件下,利塞膦酸钠及其有关物质能达到良好分离,二者色谱峰的分离度大于2.5;应用主成分自身对照法计算,杂质峰含量约为0.14%.结论:该方法适用于利塞膦酸钠及其有关物质的常规测定,为利塞膦酸钠的质量控制提供有效依据.【期刊名称】《河南化工》【年(卷),期】2012(029)012【总页数】2页(P55-56)【关键词】反相离子对高效液相色谱法;利塞膦酸钠;有关物质【作者】张卫民;杨杰;吴拥军【作者单位】郑州大学化学系,河南郑州450001【正文语种】中文【中图分类】O657.720 引言利塞膦酸钠是由美国宝洁公司研制开发的第三代双膦酸盐类药物,为西药二类新药。
到目前为止,只开发出少数测定生物基质中利塞膦酸钠的分析方法,包括经酰化和硅烷化形成挥发性衍生物后的气相色谱—质谱法[1]和非常灵敏但极为复杂的酶联免疫吸附测定法[2]。
据文献报道,高效液相色谱法是测定利塞膦酸钠的首选方法[3-5]。
本文介绍一种用于双膦酸盐类药物利塞膦酸钠与有关物质分离的反相离子对高效液相色谱法,该方法操作简便、准确可靠。
1 实验部分1.1 仪器与试药戴安高效液相色谱仪,美国戴安公司;100 μm Hamilton微量进样器,美国;移液枪,Dragon,芬兰;AL 104型电子天平,梅特勒—托利多仪器有限公司。
塞膦酸钠原料药(批号:071100010)由河南天方药业公司提供,利塞膦酸钠化学对照品(批号:100613-200401)购自中国药品生物制品检定所。
利塞膦酸钠的波谱学数据和结构确证目的确证利塞膦酸钠的结构。
方法采用红外(IR)、紫外(UV)、氢谱(1HNMR)、碳谱(13CNMR,DEPT)等进行结构解析。
结果根据氢-氢相关谱(1H-1H COSY)、碳氢相关谱(HMQC)、碳氢远程相关谱(HMBC)对所有的1HNMR和13CNMR谱信号进行了归属;讨论了红外特征吸收峰所对应的官能团的振动形式。
结论确证了利塞膦酸钠的结构。
标签:利塞膦酸钠;核磁共振;归属;红外;紫外利塞膦酸钠是双膦酸盐类药物,化学名为[1-羟基-2-(3-吡啶基)乙叉基]双膦酸单钠盐,其结构式见图1。
在临床研究中显现出其对变形性骨炎及骨质疏松症具有优异的疗效[1-4]。
文献对利塞膦酸钠的制备与药理方面的报道较多,波谱学方面报道较少。
本研究报道了该化合物的红外、紫外、氢氢相关谱、碳谱、碳氢相关谱、碳氢远程相关谱并予以解析,对所有的1HNMR和13CNMR谱信号进行了归属;同时讨论了红外特征吸收峰所对应的官能团的振动形式,并对样品进行热差和热重分析。
现报道如下:1 资料与方法1.1 仪器和测定条件1HNMR、13CNMR、HMQC 和HMBC均在超导核磁共振波谱仪(德国Bruker DPX-400M)核磁共振仪上完成。
以D2O为溶剂,二维谱采用反相检测探头,1HNMR的观测频率为400.144 MHz;13CNMR的观测频率为100.625 MHz;PE-2400型元素分析仪;PERKIN-ELMER LAMBDA17紫外可见分光光度计;美国BIO-RAD FTS-40型傅立叶变换红外分光光度仪,KBr压片;日本岛津DT-40型热分析仪。
1.2 样品制备以3-吡啶乙酸盐酸盐为起始原料,与亚磷酸和PCl3缩合、水解得利塞膦酸钠。
以异丙醇、水精制[4]。
对样品进行HPLC分析,结果表明纯度为99.5%,符合结构鉴定所需纯度。
样品的元素分析测定值(m%)为:C 23.98,H 4.29,N 3.98,P 17.6,与理论值基本符合。
____________________________________________________________________________________________________________________________________ HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to useACTONEL safely and effectively. See full prescribing information forACTONEL. ACTONEL ® (risedronate sodium) tabletsInitial U.S. Approval: 1998----------------------------RECENT MAJOR CHANGES--------------------------Warnings and Precautions (5.3) 7/2009 ----------------------------INDICATIONS AND USAGE---------------------------ACTONEL is a bisphosphonate indicated for: •Treatment and prevention of postmenopausal osteoporosis (1.1), •Treatment to increase bone mass in men with osteoporosis (1.2), •Treatment and prevention of glucocorticoid-induced osteoporosis (1.3), •Treatment of Paget’s disease (1.4). ----------------------DOSAGE AND ADMINISTRATION-----------------------Must be taken with plain water (6 to 8 oz) at least 30 minutes before the firstfood or drink of the day; do not lie down for 30 minutes (2) Treatment of Osteoporosis in Postmenopausal Women: 5 mg daily, 35 mg once a week, 75 mg taken on two consecutive days each month, or 150 mg once a month (2.1) Prevention of Osteoporosis in Postmenopausal Women: 5 mg daily, or 35 mg once a week (2.2)Men with Osteoporosis: 35 mg once a week (2.3)Treatment and Prevention of Glucocorticoid-Induced Osteoporosis: 5 mg daily(2.4)Paget’s Disease: 30 mg daily for 2 months (2.5)---------------------DOSAGE FORMS AND STRENGTHS----------------------Tablets: 5, 30, 35, 75, and 150 mg (3) -------------------------------CONTRAINDICATIONS------------------------------• Inability to stand or sit upright for at least 30 minutes (4, 5.1) • Hypocalcemia (4, 5.2)• Known hypersensitivity to any component of this product (4, 6.2) -----------------------WARNINGS AND PRECAUTIONS------------------------• Upper gastrointestinal irritation may occur. Dosing instructions should be followed. Discontinue use if new or worsening symptoms occur (5.1). • Hypocalcemia may worsen and must be corrected prior to use (5.2). • Osteonecrosis of the jaw has been reported rarely (5.3). • Severe bone, joint, or muscle pain may occur. Consider discontinuing use if severe symptoms develop (5.4, 6.2). • Before initiating treatment in patients with glucocorticoid-induced osteoporosis, sex steroid hormonal status of both men and women should be ascertained and appropriate replacement considered (5.6). • Bisphosphonates may interfere with bone-imaging agents (5.7). ------------------------------ADVERSE REACTIONS-------------------------------Most common adverse reactions reported in >10% of patients treated with ACTONEL and with a higher frequency than placebo are: back pain, arthralgia, abdominal pain, and dyspepsia (6.1). Hypersensitivity reactions (angioedema, generalized rash, bullous skin reactions), and eye inflammation (iritis, uveitis) have been reported rarely (6.2). To report SUSPECTED ADVERSE REACTIONS, contact Procter & Gamble Pharmaceuticals, Inc. at 1-800-836-0658 or FDA at 1-800-FDA1088 or /medwatch.------------------------------DRUG INTERACTIONS-------------------------------Calcium, antacids, or oral medications containing divalent cations interfere with the absorption of ACTONEL (7.1). -----------------------USE IN SPECIFIC POPULATIONS------------------------ACTONEL is not recommended for use in patients with severe renal impairment (creatinine clearance <30 mL/min) (5.5, 8.6, 12.3). ACTONEL is not indicated for use in pediatric patients (8.4).See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling. Revised: 07/2009 FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE 1.1 Postmenopausal Osteoporosis 1.2 Osteoporosis in Men 1.3 Glucocorticoid-Induced Osteoporosis 1.4 Paget’s Disease 2DOSAGE AND ADMINISTRATION 2.1 Treatment of Postmenopausal Osteoporosis [see Indications and Usage (1.1)]2.2 Prevention of Postmenopausal Osteoporosis [see Indications and Usage (1.1)] 2.3Treatment to Increase Bone Mass in Men with Osteoporosis [see Indications and Usage (1.2)] 2.4 Treatment and Prevention of Glucocorticoid-Induced Osteoporosis [see Indications and Usage (1.3)] 2.5 Treatment of Paget’s Disease [see Indications and Usage (1.4)] 3 DOSAGE FORMS AND STRENGTHS 4 CONTRAINDICATIONS 5 WARNINGS AND PRECAUTIONS 5.1 Upper Gastrointestinal Adverse Reactions 5.2 Mineral Metabolism 5.3 Jaw Osteonecrosis 5.4 Musculoskeletal Pain 5.5 Renal Impairment 5.6 Glucocorticoid-Induced Osteoporosis 5.7 Laboratory Test Interactions 6ADVERSE REACTIONS 6.1 Clinical Studies Experience 6.2 Postmarketing Experience 7 DRUG INTERACTIONS 7.1 Calcium Supplements/Antacids 7.2 Hormone Replacement Therapy 7.3 Aspirin/Nonsteroidal Anti-Inflammatory Drugs 7.4 H 2 Blockers and Proton Pump Inhibitors (PPIs) 8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy 8.3 Nursing Mothers 8.4 Pediatric Use 8.5 Geriatric Use 8.6 Renal Impairment 8.7 Hepatic Impairment 10 OVERDOSAGE 11 DESCRIPTION 12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action 12.2 Pharmacodynamics 12.3 Pharmacokinetics 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility 13.2 Animal Toxicology and/or Pharmacology 14 CLINICAL STUDIES 14.1 Treatment of Osteoporosis in Postmenopausal Women 14.2 Prevention of Osteoporosis in Postmenopausal Women 14.3 Men with Osteoporosis 14.4 Glucocorticoid-Induced Osteoporosis 14.5 Treatment of Paget’s Disease 16 HOW SUPPLIED/STORAGE AND HANDLING 17 PATIENT COUNSELING INFORMATION 17.1 FDA-Approved Patient Labeling *Sections or subsections omitted from the full prescribing information are not listed.FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGEOsteoporosis1.1 PostmenopausalACTONEL is indicated for the treatment and prevention of osteoporosis in postmenopausal women. In postmenopausal women with osteoporosis, ACTONEL reduces the incidence of vertebral fractures and a composite endpoint of nonvertebral osteoporosis-related fractures [see Clinical Studies (14.1, 14.2)].1.2 Osteoporosis in MenACTONEL is indicated for treatment to increase bone mass in men with osteoporosis.Osteoporosis1.3 Glucocorticoid-InducedACTONEL is indicated for the treatment and prevention of glucocorticoid-induced osteoporosis in men and women who are either initiating or continuing systemic glucocorticoid treatment (daily dosage of ≥ 7.5 mg prednisone or equivalent) for chronic diseases. Patients treated with glucocorticoids should receive adequate amounts of calcium and vitamin D.Disease1.4 Paget’sACTONEL is indicated for treatment of Paget’s disease of bone in men and women.2 DOSAGE AND ADMINISTRATIONACTONEL should be taken at least 30 minutes before the first food or drink of the day other than water.To facilitate delivery to the stomach, ACTONEL should be swallowed while the patient is in an upright position and with a full glass of plain water (6 to 8 oz). Patients should not lie down for 30 minutes after taking the medication [see Warnings and Precautions (5.1)].Patients should receive supplemental calcium and vitamin D if dietary intake is inadequate [see Warnings and Precautions (5.2)]. Calcium supplements and calcium-, aluminum-, and magnesium-containing medications may interfere with the absorption of ACTONEL and should be taken at a different time of the day. ACTONEL is not recommended for use in patients with severe renal impairment (creatinine clearance <30 mL/min). No dosage adjustment is necessary in patients with a creatinine clearance ≥30 mL/min or in the elderly.2.1 Treatment of Postmenopausal Osteoporosis [see Indications and Usage (1.1)]The recommended regimen is:•one 5 mg tablet orally, taken dailyor•one 35 mg tablet orally, taken once a weekor•one 75 mg tablet orally, taken on two consecutive days for a total of two tablets each monthor•one 150 mg tablet orally, taken once a month2.2 Prevention of Postmenopausal Osteoporosis [see Indications and Usage (1.1)]The recommended regimen is:•one 5 mg tablet orally, taken dailyor•one 35 mg tablet orally, taken once a weekor•alternatively, one 75 mg tablet orally, taken on two consecutive days for a total of two tablets each month may be consideredor•alternatively, one 150 mg tablet orally, taken once a month may be considered2.3 Treatment to Increase Bone Mass in Men with Osteoporosis [see Indications andUsage (1.2)]The recommended regimen is:•one 35 mg tablet orally, taken once a week2.4 Treatment and Prevention of Glucocorticoid-Induced Osteoporosis [see Indicationsand Usage (1.3)]The recommended regimen is:•one 5 mg tablet orally, taken daily2.5 Treatment of Paget’s Disease [see Indications and Usage (1.4)]The recommended treatment regimen is 30 mg orally once daily for 2 months. Retreatment may be considered (following post-treatment observation of at least 2 months) if relapse occurs, or if treatment fails to normalize serum alkaline phosphatase. For retreatment, the dose and duration of therapy are the same as for initial treatment. No data are available on more than 1 course of retreatment.3 DOSAGE FORMS AND STRENGTHS• 5 mg film-coated, oval, yellow tablet with RSN on 1 face and 5 mg on the other.•30 mg film-coated, oval, white tablet with RSN on 1 face and 30 mg on the other.•35 mg film-coated, oval, orange tablet with RSN on 1 face and 35 mg on the other.•75 mg film-coated, oval, pink tablet with RSN on 1 face and 75 mg on the other.•150 mg film-coated, oval, blue tablet with RSN on 1 face and 150 mg on the other.4 CONTRAINDICATIONS•Inability to stand or sit upright for at least 30 minutes [see Dosage andAdministration (2), Warnings and Precautions (5.1)]•Hypocalcemia [see Warnings and Precautions (5.2)]•Known hypersensitivity to any component of this product [see Adverse Reactions(6.2)]5 WARNINGS AND PRECAUTIONS5.1 Upper Gastrointestinal Adverse ReactionsBisphosphonates, including ACTONEL, may cause upper gastrointestinal disorders such as dysphagia, esophagitis, and esophageal or gastric ulcers. ACTONEL should be taken according to the dosing instructions to minimize the risk of these events. Patients should discontinue use if new or worsening symptoms occur. [see Contraindications (4), Adverse Reactions (6.1), Information for Patients (17.1)].Metabolism5.2 MineralHypocalcemia and other disturbances of bone and mineral metabolism should be effectively treated before starting ACTONEL therapy. Adequate intake of calcium and vitamin D is important in all patients, especially in patients with Paget’s disease in whom bone turnover is significantly elevated [see Contraindications (4), Adverse Reactions (6.1), Information for Patients (17.1)].Osteonecrosis5.3 JawOsteonecrosis of the jaw (ONJ), which can occur spontaneously, is generally associated with tooth extraction and/or local infection with delayed healing, and has been reported in patients taking bisphosphonates, including ACTONEL. Known risk factors for osteonecrosis of the jaw include invasive dental procedures (e.g., tooth extraction, dental implants, boney surgery), diagnosis of cancer, concomitant therapies (e.g., chemotherapy, corticosteroids), poor oral hygiene, and co-morbid disorders (e.g., periodontal and/or other pre-existing dental disease, anemia, coagulopathy, infection, ill-fitting dentures).For patients requiring invasive dental procedures, discontinuation of bisphosphonate treatment may reduce the risk for ONJ. Clinical judgment of the treating physician and/or oral surgeon should guide the management plan of each patient based on individual benefit/risk assessment.Patients who develop osteonecrosis of the jaw while on bisphosphonate therapy should receive care by an oral surgeon. In these patients, extensive dental surgery to treat ONJ may exacerbate the condition. Discontinuation of bisphosphonate therapy should be considered based on individual benefit/risk assessment. [see Adverse Reactions (6.2)]5.4 MusculoskeletalPainIn postmarketing experience, there have been reports of severe and occasionally incapacitating bone, joint, and/or muscle pain in patients taking bisphosphonates [see Adverse Reactions (6.2)]. The time to onset of symptoms varied from one day to several months after starting the drug. Most patients had relief of symptoms after stopping medication. A subset had recurrence of symptoms when rechallenged with the same drug or another bisphosphonate. Consider discontinuing use if severe symptoms develop.5.5 Renal ImpairmentACTONEL is not recommended for use in patients with severe renal impairment (creatinine clearance <30 mL/min).Osteoporosis5.6 Glucocorticoid-InducedBefore initiating ACTONEL treatment for the treatment and prevention of glucocorticoid-induced osteoporosis, the sex steroid hormonal status of both men and women should be ascertained and appropriate replacement considered.5.7 Laboratory Test InteractionsBisphosphonates are known to interfere with the use of bone-imaging agents. Specific studies with ACTONEL have not been performed.REACTIONS6 ADVERSE6.1 Clinical Studies ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.Treatment of Postmenopausal OsteoporosisDaily DosingThe safety of ACTONEL 5 mg once daily in the treatment of postmenopausal osteoporosis was assessed in four randomized, double-blind, placebo-controlled multinational trials of 3232 women aged 38 to 85 years with postmenopausal osteoporosis. The duration of the trials was up to three years, with 1619 patients exposed to placebo and 1613 patients exposed to ACTONEL 5 mg. Patients with pre-existing gastrointestinal disease and concomitant use of nonsteroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in these clinical trials. All women received 1000 mg of elemental calcium plus vitamin D supplementation up to 500 IU per day if their 25-hydroxyvitamin D3 level was below normal at baseline.The incidence of all-cause mortality was 2.0% in the placebo group and 1.7% in the ACTONEL 5 mg daily group. The incidence of serious adverse events was 24.6% in the placebo group and 27.2% in the ACTONEL 5 mg group. The percentage of patients who withdrew from the study due to adverse events was 15.6% in the placebo group and 14.8% in the ACTONEL5 mg group. Table 1 lists adverse events from the Phase 3 postmenopausal osteoporosis trials reported in ≥5% of patients. Adverse events are shown without attribution of causality.Table 1Adverse Events Occurring at a Frequency ≥5% in Either Treatment Group Combined Phase 3 Postmenopausal Osteoporosis Treatment TrialsBody System PlaceboN = 16195 mg ACTONELN = 1613% %Body as a WholeInfection 29.931.1 Back Pain 26.1 28.0Accidental Injury 16.8 16.9Pain 14.014.1 Abdominal Pain 9.9 12.2Flu Syndrome 11.6 10.5Headache 10.89.9 Asthenia 4.55.4 Neck Pain 4.7 5.4Chest Pain 5.1 5.0Allergic ReactionCardiovascular System5.9 3.8Hypertension Digestive System 9.810.5Constipation 12.612.9 Diarrhea 10.010.8 Dyspepsia 10.610.8Nausea Metabolic & Nutritional Disorders 11.210.5Peripheral EdemaMusculoskeletal System8.8 7.7Arthralgia 22.123.7 Arthritis 10.19.6 Traumatic Bone Fracture 12.3 9.3Joint Disorder 5.3 7.0Myalgia 6.26.7 Bone PainNervous System4.85.3Dizziness 5.77.1 Depression 6.16.8Insomnia Respiratory System 4.65.0Bronchitis 10.410.0 Sinusitis 9.18.7 Rhinitis 5.16.2 Pharyngitis 5.06.0 Increased CoughSkin and Appendages6.3 5.9Rash Special Senses 7.17.9Cataract Urogenital System 5.76.5Urinary Tract Infection 10.4 11.1Gastrointestinal Adverse Events: The incidence of adverse events in the placebo and ACTONEL 5 mg daily groups were: abdominal pain (9.9% vs. 12.2%), diarrhea (10.0% vs. 10.8%), dyspepsia (10.6% vs. 10.8%), and gastritis (2.3% vs. 2.7%). Duodenitis and glossitis have been reported uncommonly in the ACTONEL 5 mg daily group (0.1% to 1%). In patients with active upper gastrointestinal disease at baseline, the incidence of upper gastrointestinal adverse events was similar between the placebo and ACTONEL 5 mg daily groups.Musculoskeletal Adverse Events: The incidence of adverse events in the placebo and ACTONEL 5 mg daily groups were: back pain (26.1% vs. 28.0%), arthralgia (22.1% vs. 23.7%), myalgia (6.2% vs. 6.7%), and bone pain (4.8% vs. 5.3%).Laboratory Test Findings: Throughout the Phase 3 studies, transient decreases from baseline in serum calcium (<1%) and serum phosphate (<3%) and compensatory increases in serum PTH levels (<30%) were observed within 6 months in patients in osteoporosis clinical trials treated with ACTONEL 5 mg once daily. There were no significant differences in serum calcium, phosphate, or PTH levels between placebo and ACTONEL 5 mg once daily at 3 years. Serum calcium levels below 8 mg/dL were observed in 18 patients, 9 (0.5%) in each treatment arm (placebo and ACTONEL 5 mg once daily). Serum phosphorus levels below 2 mg/dL were observed in 14 patients, 3 (0.2%) treated with placebo and 11 (0.6%) treated with ACTONEL5 mg once daily. There have been rare reports (<0.1%) of abnormal liver function tests.Endoscopic Findings: In the ACTONEL clinical trials, endoscopic evaluation was encouraged in any patient with moderate-to-severe gastrointestinal complaints, while maintaining the blind. Endoscopies were performed on equal numbers of patients between the placebo and treated groups [75 (14.5%) placebo; 75 (11.9%) ACTONEL]. Clinically important findings (perforations, ulcers, or bleeding) among this symptomatic population were similar between groups (51% placebo; 39% ACTONEL).Once-a-Week DosingThe safety of ACTONEL 35 mg once-a-week in the treatment of postmenopausal osteoporosis was assessed in a 1-year, double-blind, multicenter study comparing ACTONEL5 mg daily and ACTONEL 35 mg once-a-week in postmenopausal women aged 50 to 95 years. The duration of the trials was one year, with 480 patients exposed to ACTONEL 5 mg daily and 485 exposed to ACTONEL 35 mg once-a-week. Patients with pre-existing gastrointestinal disease and concomitant use of non-steroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in these clinical trials. All women received 1000 mg of elemental calcium plus vitamin D supplementation up to 500 IU per day if their25-hydroxyvitamin D3 level was below normal at baseline.The incidence of all-cause mortality was 0.4% in the ACTONEL 5 mg daily group and 1.0% in the ACTONEL 35 mg once-a-week group. The incidence of serious adverse events was 7.1% in the ACTONEL 5 mg daily group and 8.2% in the ACTONEL 35 mg once-a-week group. The percentage of patients who withdrew from the study due to adverse events was 11.9% in the ACTONEL 5 mg daily group and 11.5% in the ACTONEL 35 mg once-a-week group. The overall safety and tolerability profiles of the two dosing regimens were similar.Gastrointestinal Adverse Events: The incidence of gastrointestinal adverse events was similar between the ACTONEL 5 mg daily group and the ACTONEL 35 mg once-a-week group: dyspepsia (6.9% vs. 7.6%), diarrhea (6.3% vs. 4.9%), and abdominal pain (7.3% vs. 7.6%).Musculoskeletal Adverse Events: Arthralgia was reported in 11.5% of patients in the ACTONEL 5 mg daily group and 14.2% of patients in the ACTONEL 35 mg once-a-week group. Myalgia was reported by 4.6% of patients in the ACTONEL 5 mg daily group and 6.2% of patients in the ACTONEL 35 mg once-a-week group.Laboratory Test Findings: The mean percent changes from baseline at 12 months were similar between the ACTONEL 5 mg daily and ACTONEL 35 mg once-a-week groups, respectively, for serum calcium (0.4% vs. 0.7%), phosphate (-3.8% vs. -2.6%) and PTH (6.4% vs. 4.2%).Monthly DosingTwo Consecutive Days per MonthThe safety of ACTONEL 75 mg administered on two consecutive days per month for the treatment of postmenopausal osteoporosis was assessed in a double-blind, multicenter study in postmenopausal women aged 50 to 86 years. The duration of the trial was two years; 613 patients were exposed to ACTONEL 5 mg daily and 616 were exposed to ACTONEL 75 mg two consecutive days per month. Patients with pre-existing gastrointestinal disease and concomitant use of non-steroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in this clinical trial. All women received 1000 mg of elemental calcium plus 400 to 800 IU of vitamin D supplementation per day.The incidence of all-cause mortality was 1.0% for the ACTONEL 5 mg daily group and 0.5% for the ACTONEL 75 mg two consecutive days per month group. The incidence of serious adverse events was 10.8% in the ACTONEL 5 mg daily group and 14.4% in the ACTONEL75 mg two consecutive days per month group. The percentage of patients who withdrew from treatment due to adverse events was 14.2% in the ACTONEL 5 mg daily group and 13.0% in the ACTONEL 75 mg two consecutive days per month group. The overall safety and tolerability profiles of the two dosing regimens were similar.Acute Phase Reactions: Symptoms consistent with acute phase reaction have been reported with bisphosphonate use. The overall incidence of acute phase reaction was 3.6% of patients on ACTONEL 5 mg daily and 7.6% of patients on ACTONEL 75 mg two consecutive days per month. These incidence rates are based on reporting of any of 33 acute phase reaction-like symptoms within 5 days of the first dose. Fever or influenza-like illness with onset within the same period were reported by 0.0% of patients on ACTONEL 5 mg daily and 0.6% of patients on ACTONEL 75 mg two consecutive days per month.Gastrointestinal Adverse Events: The ACTONEL 75 mg two consecutive days per month group resulted in a higher incidence of discontinuation due to vomiting (1.0% vs. 0.2%) and diarrhea (1.0% vs. 0.3%) compared to the ACTONEL 5 mg daily group. Most of these events occurred within a few days of dosing.Ocular Adverse Events: None of the patients treated with ACTONEL 75 mg two consecutive days per month reported ocular inflammation such as uveitis, scleritis, or iritis;1 patient treated with ACTONEL 5 mg daily reported uveitis.Laboratory Test Findings: When ACTONEL 5 mg daily and ACTONEL 75 mg two consecutive days per month were compared in postmenopausal women with osteoporosis, the mean percent changes from baseline at 24 months were 0.2% and 0.8% for serum calcium, -1.9% and -1.3% for phosphate, and -10.4% and -17.2% for PTH, respectively. Compared to the ACTONEL 5 mg daily group, ACTONEL 75 mg two consecutive days per month resulted in a slightly higher incidence of hypocalcemia at the end of the first month of treatment (4.5% vs. 3.0%). Thereafter, the incidence of hypocalcemia with these regimens was similar at approximately 2%.Once-a-MonthThe safety of ACTONEL 150 mg administered once a month for the treatment of postmenopausal osteoporosis was assessed in a double-blind, multicenter study in postmenopausal women aged 50 to 88 years. The duration of the trial was one year, with642 patients exposed to ACTONEL 5 mg daily and 650 exposed to ACTONEL 150 mg once-amonth. Patients with pre-existing gastrointestinal disease and concomitant use of non-steroidal anti-inflammatory drugs, proton pump inhibitors, and H2 antagonists were included in this clinical trial. All women received 1000 mg of elemental calcium plus up to 1000 IU of vitamin D supplementation per day.The incidence of all-cause mortality was 0.5% for the ACTONEL 5 mg daily group and 0.0% for the ACTONEL 150 mg once-a-month group. The incidence of serious adverse events was 4.2% in the ACTONEL 5 mg daily group and 6.2% in the ACTONEL 150 mg once-a-month group. The percentage of patients who withdrew from treatment due to adverse events was 9.5% in the ACTONEL 5 mg daily group and 8.6% in the ACTONEL 150 mg once-a-month group. The overall safety and tolerability profiles of the two dosing regimens were similar.Acute Phase Reactions: Symptoms consistent with acute phase reaction have been reported with bisphosphonate use. The overall incidence of acute phase reaction was 1.1% in the ACTONEL 5 mg daily group and 5.2% in the ACTONEL 150 mg once-a-month group. These incidence rates are based on reporting of any of 33 acute phase reaction-like symptoms within3 days of the first dose and for a duration of 7 days or less. Fever or influenza-like illness with onset within the same period were reported by 0.2% of patients on ACTONEL 5 mg daily and 1.4% of patients on ACTONEL 150 mg once-a-month.Gastrointestinal Adverse Events: A greater percentage of patients experienced diarrhea with ACTONEL 150 mg once-a-month compared to 5 mg daily (8.2% vs. 4.7%, respectively). The ACTONEL 150 mg once-a-month group resulted in a higher incidence of discontinuation due to abdominal pain upper (2.5% vs. 1.4%) and diarrhea (0.8% vs. 0.0%) compared to the ACTONEL 5 mg daily regimen. All of these events occurred within a few days of the first dose. The incidence of vomiting that led to discontinuation was the same in both groups (0.3% vs.0.3%).Ocular Adverse Events: None of the patients treated with ACTONEL 150 mg once-amonth reported ocular inflammation such as uveitis, scleritis, or iritis; 2 patients treated with ACTONEL 5 mg daily reported iritis.Laboratory Test Findings: When ACTONEL 5 mg daily and ACTONEL 150 mg once-a-month were compared in postmenopausal women with osteoporosis, the mean percent changes from baseline at 12 months were 0.1% and 0.3% for serum calcium, -2.3% and -2.3% for phosphate, and 8.3% and 4.8% for PTH, respectively. Compared to the ACTONEL 5 mg daily regimen, ACTONEL 150 mg once-a-month resulted in a slightly higher incidence of hypocalcemia at the end of the first month of treatment (0.2% vs. 2.2%). Thereafter, the incidence of hypocalcemia with these regimens was similar at approximately 2%.Prevention of Postmenopausal OsteoporosisDaily DosingThe safety of ACTONEL 5 mg daily in the prevention of postmenopausal osteoporosis was assessed in two randomized, double-blind, placebo-controlled trials. In one study of postmenopausal women aged 37 to 82 years without osteoporosis, the use of estrogen replacement therapy in both placebo- and ACTONEL-treated patients was included. The duration of the trial was one year, with 259 exposed to placebo and 261 patients exposed to ACTONEL 5 mg. The second study included postmenopausal women aged 44 to 63 years without osteoporosis. The duration of the trial was one year, with 125 exposed to placebo and 129 patients exposed to ACTONEL 5 mg. All women received 1000 mg of elemental calcium per day.In the trial with estrogen replacement therapy, the incidence of all-cause mortality was 1.5% for the placebo group and 0.4% for the ACTONEL 5 mg group. The incidence of serious adverse events was 8.9% in the placebo group and 5.4% in the ACTONEL 5 mg group. The percentage of patients who withdrew from treatment due to adverse events was 18.9% in the placebo group and 10.3% in the ACTONEL 5 mg group. Constipation was reported by 1.9% of the placebo group and 6.5% of ACTONEL 5 mg group.In the second trial, the incidence of all-cause mortality was 0.0% for both groups. The incidence of serious adverse events was 17.6% in the placebo group and 9.3% in the ACTONEL5 mg group. The percentage of patients who withdrew from treatment due to adverse events was6.4% in the placebo group and 5.4% in the ACTONEL 5 mg group. Nausea was reported by 6.4% of patients in the placebo group and 13.2% of patients in the ACTONEL 5 mg group. Once-a-Week DosingThere were no deaths in a 1-year, double-blind, placebo-controlled study of ACTONEL 35 mg once a week for prevention of bone loss in 278 postmenopausal women without osteoporosis. More treated subjects on ACTONEL reported arthralgia (placebo 7.8%; ACTONEL 13.9%), myalgia (placebo 2.1%; ACTONEL 5.1%), and nausea (placebo 4.3%; ACTONEL 7.3%) than subjects on placebo.。
气相色谱法测定利塞膦酸钠中的残留溶剂金华;王崇益;陈小红【摘要】目的:建立利塞膦酸钠原料中甲醇、乙醇和乙醚残留溶剂含量的测定方法.方法:采用气相色谱法测定.色谱柱为SE-30石英毛细管柱(30m×0.530mm,1.00μm),柱温为40℃,检测器采用氢火焰离子化检测器(FID),温度为300℃,以氮气为载气,流速为40ml/min.结果:在本文色谱条件下,甲醇、乙醇和乙醚均能得到良好分离,检测浓度在所考察的范围内与峰面积成良好的线性关系,r =0.998 8~0.999 0;平均回收率为96.8%~97.7%,RSD为1.2%~3.9%;甲醇、乙醇和乙醚检测限分别为1.294、1.630、3.164μg/ml.结论:本实验建立的色谱方法简便、准确,适合利塞膦酸钠原料中有机溶剂残留量的检测.【期刊名称】《医学理论与实践》【年(卷),期】2011(024)019【总页数】3页(P2301-2302,2312)【关键词】利塞膦酸钠;残留溶剂;气相色谱法【作者】金华;王崇益;陈小红【作者单位】江苏省淮安药品检验所,江苏省淮安市,223300;江苏正大清江制药有限公司;江苏省淮安药品检验所,江苏省淮安市,223300【正文语种】中文【中图分类】R927.2利塞膦酸钠主要用于治疗绝经后妇女骨质疏松症,也可用于预防高危人群的骨质疏松症。
通过对其生产工艺的分析发现,在利塞膦酸钠合成过程中,使用了多种有机溶剂,产品中可能含有微量的甲醇、乙醇和乙醚等有机溶剂。
笔者参考《中国药典》2005年版(二部)等相关标准,采用了毛细管气相色谱法,以直接进样的方式测定利塞膦酸钠中甲醇、乙醇和乙醚的残留量,方法简便,重现性好。
1 仪器与试药Agilen t 6890N气相色谱仪,F ID检测器;利塞膦酸钠样品(批号 20101113、20101115、20101115)由江苏正大清江制药有限公司提供,红外图谱与利塞膦酸钠标准品图谱一致;甲醇、乙醇、乙醚、正丙醇均为色谱纯。
分光光度法测定治疗骨质疏松症的药物伊尔哈姆和法耶克国家药物管制和研究组织(NODCAR).2003年7月24日.6.阿布哈齐姆ST,埃及,开罗,金字塔,邮政信箱29号专栏.2003年8月30日。
分光光度法用于治疗骨质疏松症的新药物:利塞膦酸钠(I),阿仑膦酸钠(II)和依替膦酸二钠(III)的开发,此方法简单,准确,灵敏。
第一种方法是基于测量的吸光度的差异(△A)的上升,利塞膦酸钠在0.01mol/L的盐酸溶液和0.1mol/L的氢氧化钠中反应,在波长262 nm处测得,,平均恢复系数为99.75±1.22、摩尔吸光系数(ε)为1.891×103。
浓度范围在15-150μg/ml内服从Beer定律。
第二种方法是阿仑膦酸钠浓度为0.05mol/L,在甲醇介质中与茚三酮试剂(II)的伯氨基碳酸氢钠中和反应。
有色产物测量波长为568 nm,线性范围是3.75-45μg/ml、平均回收率为99.77±0.73和ε= 9.425×103。
第三种方法是基于在氧化过程中提到的三个药物与硝酸铈(Ⅳ)在0.5 mol/L的硫酸中在室温和后续计量过量的未反应的铈(Ⅳ)在波长320 nm处的干燥。
三种药物平均回收率为99.79±1.16、99.73 ±1.38、99.86±1.13摩尔吸光系数ε14.427 ×103、13.813×103和14.000×103。
药物I,II,III在浓度范围为2-24μg/m内服从比尔定律。
分别所提出的三种方法成功地应用散装粉末药物和药物制剂的测定。
结果发现,获得了的结果在所报道的方法在统计学上吻合。
此外,该方法进行了验证根据药典规定,通过运用标准品添加技术也进行了评估。
关键词利塞膦酸钠阿仑膦酸钠依替膦酸钠吸光度差异(△A)茚三酮试剂铈(IV)硫酸利塞膦酸钠(I)为三氢钠(1- 羟基-2-(3-吡啶基)亚乙基)二膦酸,阿仑膦酸钠(II),和三氢钠(4 - 氨基-1 - 羟)二膦酸酯(III)的三水合物,依替膦酸二钠为磷酸二氢二钠(1- 羟基亚乙基)二膦酸盐,它们的结构如图.1所示。
利塞膦酸钠对去势骨质疏松白兔的实验研究李蔚;张妍【摘要】Objective To obeserve and analyze of risedronate for osteoporosis inovariectomized rabbits therapeutic effect. Methods 21 rabbits were divided into 3 groups:contro group,OP and treated with risedronate at a low dose(2 mg·kg-1·d-1)and OP and treated with risedronate at a high dose (5mg·kg-1·d-1). OP was induced by ovariectomized. The studies were carried out to determine the effect of risedronate on serum ALP,serum calcium,BMD and bone trabeculae. Results Compared with the control group,risedronate significantly increased due to osteoporosis in ovariectomized rabbit serum ALP,serum calcium (P<0.01),femoral bone mineral density and trabecular bone measured the width of the control group there were significant differences (P<0.01),serum phosphorus value was no significant difference (P>0.05). Conclusion The result of risedronate for osteoporosis in overiectomized rabbits have signffcant therapeutic effect.%目的观察和分析利塞膦酸钠对去势骨质疏松白兔的治疗作用.方法观察利塞膦酸钠(2.3rag·kg<'-1>·d<'-1>)对实验性骨质疏松白兔血清碱性磷酸酶活性,血钙,血磷值,股骨骨密度及骨小梁宽度的影响.结果与对照组相比,利塞膦酸钠可明显增加去势所致骨质疏松白兔血清ALP、血钙值(P<0.01),股骨骨密度及骨小梁宽度的测定与对照组相比有显著差异(P<0.01),血磷值无明显差异(P>0.05).结论利寨膦酸钠对去势所致骨质疏松白兔有明显的治疗作用.【期刊名称】《颈腰痛杂志》【年(卷),期】2011(032)003【总页数】3页(P187-189)【关键词】利寒膦酸钠;骨质疏松;去势【作者】李蔚;张妍【作者单位】解放军第105医院,安徽,合肥,230031;解放军第105医院,安徽,合肥,230031【正文语种】中文【中图分类】R589骨质疏松症是一种以骨量低下、骨微结构破坏,导致骨脆性增加、易发生骨折为特征的全身性骨病。
利塞膦酸钠的波谱学数据和结构确证
目的确证利塞膦酸钠的结构。
方法采用红外(IR)、紫外(UV)、氢谱(1HNMR)、碳谱(13CNMR,DEPT)等进行结构解析。
结果根据氢-氢相关谱(1H-1H COSY)、碳氢相关谱(HMQC)、碳氢远程相关谱(HMBC)对所有的1HNMR和13CNMR谱信号进行了归属;讨论了红外特征吸收峰所对应的官能团的振动形式。
结论确证了利塞膦酸钠的结构。
标签:利塞膦酸钠;核磁共振;归属;红外;紫外
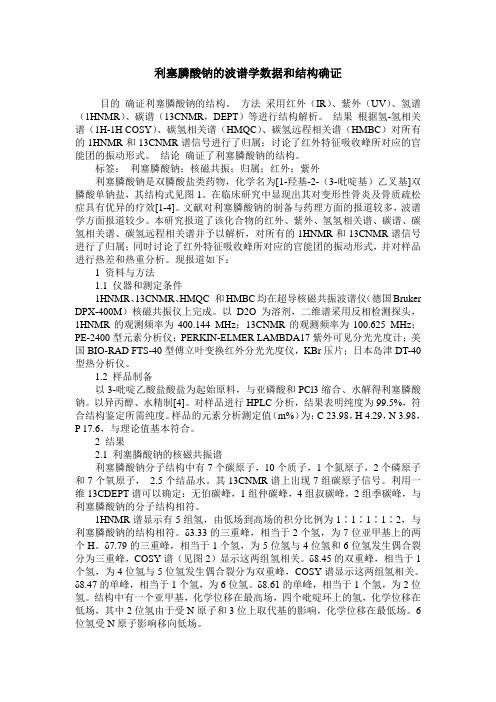
利塞膦酸钠是双膦酸盐类药物,化学名为[1-羟基-2-(3-吡啶基)乙叉基]双膦酸单钠盐,其结构式见图1。
在临床研究中显现出其对变形性骨炎及骨质疏松症具有优异的疗效[1-4]。
文献对利塞膦酸钠的制备与药理方面的报道较多,波谱学方面报道较少。
本研究报道了该化合物的红外、紫外、氢氢相关谱、碳谱、碳氢相关谱、碳氢远程相关谱并予以解析,对所有的1HNMR和13CNMR谱信号进行了归属;同时讨论了红外特征吸收峰所对应的官能团的振动形式,并对样品进行热差和热重分析。
现报道如下:
1 资料与方法
1.1 仪器和测定条件
1HNMR、13CNMR、HMQC 和HMBC均在超导核磁共振波谱仪(德国Bruker DPX-400M)核磁共振仪上完成。
以D2O为溶剂,二维谱采用反相检测探头,1HNMR的观测频率为400.144 MHz;13CNMR的观测频率为100.625 MHz;PE-2400型元素分析仪;PERKIN-ELMER LAMBDA17紫外可见分光光度计;美国BIO-RAD FTS-40型傅立叶变换红外分光光度仪,KBr压片;日本岛津DT-40型热分析仪。
1.2 样品制备
以3-吡啶乙酸盐酸盐为起始原料,与亚磷酸和PCl3缩合、水解得利塞膦酸钠。
以异丙醇、水精制[4]。
对样品进行HPLC分析,结果表明纯度为99.5%,符合结构鉴定所需纯度。
样品的元素分析测定值(m%)为:C 23.98,H 4.29,N 3.98,P 17.6,与理论值基本符合。
2 结果
2.1 利塞膦酸钠的核磁共振谱
利塞膦酸钠分子结构中有7个碳原子,10个质子,1个氮原子,2个磷原子和7个氧原子, 2.5个结晶水。
其13CNMR谱上出现7组碳原子信号。
利用一维13CDEPT谱可以确定:无伯碳峰,1组仲碳峰,4组叔碳峰,2组季碳峰,与利塞膦酸钠的分子结构相符。
1HNMR谱显示有5组氢,由低场到高场的积分比例为1∶1∶1∶1∶2,与利塞膦酸钠的结构相符。
δ3.33的三重峰,相当于2个氢,为7位亚甲基上的两个H。
δ7.79的三重峰,相当于1个氢,为5位氢与4位氢和6位氢发生偶合裂分为三重峰,COSY谱(见图2)显示这两组氢相关。
δ8.45的双重峰,相当于1个氢,为4位氢与5位氢发生偶合裂分为双重峰,COSY谱显示这两组氢相关。
δ8.47的单峰,相当于1个氢,为6位氢。
δ8.61的单峰,相当于1个氢,为2位氢。
结构中有一个亚甲基,化学位移在最高场,四个吡啶环上的氢,化学位移在低场,其中2位氢由于受N原子和3位上取代基的影响,化学位移在最低场。
6位氢受N原子影响移向低场。
由于用氘代水作溶剂,一些活泼氢如磷酸羟基氢和结晶水中的氢与氘发生快速交换而在氢谱中不出现吸收峰。
HMBC谱(见图3)显示无伯碳峰存在。
利塞膦酸钠结构中共有1个仲碳,4个叔碳,2个季碳,碳谱、HMQC(见图4)和HMBC 也显示出这几个不同类型的碳的特征。
δ36.03的碳为仲碳,化学位移在最高场,为7位碳,HMQC显示该碳与7位氢相关。
HMBC显示该碳与δ8.45、δ8.61氢远程相关。
δ73.52的碳为季碳,为8位碳,HMBC也显示该碳无相关氢。
HMBC显示该碳与δ3.33氢远程相关。
δ125.95为吡啶环上的叔碳,HMQC显示该碳与5位氢相关,HMBC显示该碳与δ8.45、δ8.47两组氢远程相关,归属为5位碳。
δ138.68为吡啶环上的叔碳,为6位碳,HMQC显示该碳与δ8.47氢相关。
δ138.50为吡啶环上的叔碳,为4 位碳,HMQC显示该碳与δ8.45氢相关。
δ142.33为吡啶环上的叔碳,为2位碳,HMQC显示该碳与δ8.61氢相关。
δ149.08为吡啶环上的季碳,为3位碳,HMQC显示该碳无相关氢。
HMBC显示该碳与δ8.61,δ8.45,δ7.79远程相关。
结构中有两个季碳,8位碳为饱和季碳,化学位移在次高场;3位碳为吡啶环上不饱和季碳,化学位移在最低场。
吡啶环上另外四个叔碳,其中2位碳由于受N原子和3位上取代基的影响,化学位移在次低场[5-8]。
2.2 利塞膦酸钠的红外吸收光谱
3 368 cm-1为羟基的O-H伸缩振动吸收峰,该峰比较强且宽证明分子中有多个羟基和结晶水。
1 662 cm-1,1 569 cm-1为吡啶环上的C=C、C=N伸缩振动吸收,说明结构中有吡啶环。
1 479 cm-1,1 387 cm-1为亚甲基的变形振动吸收,说明结构中含有亚甲基。
936 cm-1为P-O 的伸缩振动峰,强度中等,537 cm-1,476 cm-1为磷酸基团的骨架振动,说明分子中含有磷酸基团。
890 cm-1,802 cm-1,688 cm-1,630 cm-1为C=C的振动吸收峰(见图5)。
各官能团吸收峰符合该化合物结构特征[5-8]。
2.3 利塞膦酸钠的紫外吸收光谱
样品在水、0.1 mol/L NaOH溶液中的最大吸收波长一致,均为262 nm。
2.4 热分析性质
热差和热重分析结果显示,在200℃以下有3个强吸热峰,63.5℃峰为失去1个结晶水时的吸热峰;150.6℃的峰为又失去1个结晶水时的吸热峰;198.0℃峰为失去剩余结晶水时的吸热峰,说明样品中结晶水比较稳定不易失去。
本品在50~200℃区域发生明显的失重,其质量损失大约为13.0%,与利塞膦酸钠样品失去2.5分子结晶水(质量损失为:12.8%)相一致。
3 讨论
本研究对利塞膦酸钠进行了比较全面的波谱表征,1HNMR和13CNMR谱实验结果与其结构式一致,红外吸收光谱中显示出各基团的特征吸收峰,各图谱归属合理,根据以上分析结果确证了利塞膦酸钠的化学结构,对该类产品的进一步研究有一定的指导意义。
[参考文献]
[1] Rosen CJ,Kessenich CR. Comparative clinical pgamacology and therapeutic use of bishosphonates in metabolic bone diseases[J]. Drugs,1996,51(4):537-551.
[2] Wood J,Bonjean K,Ruetz S,et al. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid[J]. J Pharmacol Exp Ther,2002,302:1055-1061.
[3] 郭郡浩,姚茹冰,赵智明,等. 利塞膦酸钠胶囊治疗绝经后骨质疏松症
疗效再评价[J]. 徐州医学院学报,2010,30(3):171-174.
[4] 张启祥,孔建平. 利塞膦酸钠对糖皮质激素诱导的骨质疏松的疗效观察[J]. 中国现代应用药学,2011,28(6):585-588.
[5] 石庆东,张铜宝,张端杰,等. 利塞膦酸钠合成工艺改进[J]. 广州化工,2011,39(3):87-88.
[6] 宁永成. 有机化合物结构鉴定与有机波谱学[M]. 北京:科学出版社,2000:187-199,212-217.
[7] 刘春河,刘河,陈兰福,等. 辛伐他汀的波谱学数据和结构确证[J]. 分析化学,2005,33(7):985-988.
[8] 黄璐,孙华君,杨波,等. 丁酸氯维地平的波谱学数据与结构确证[J]. 波谱学杂志,2011,28(1):168-175.。