莫西沙星简介ppt课件
- 格式:ppt
- 大小:933.00 KB
- 文档页数:18


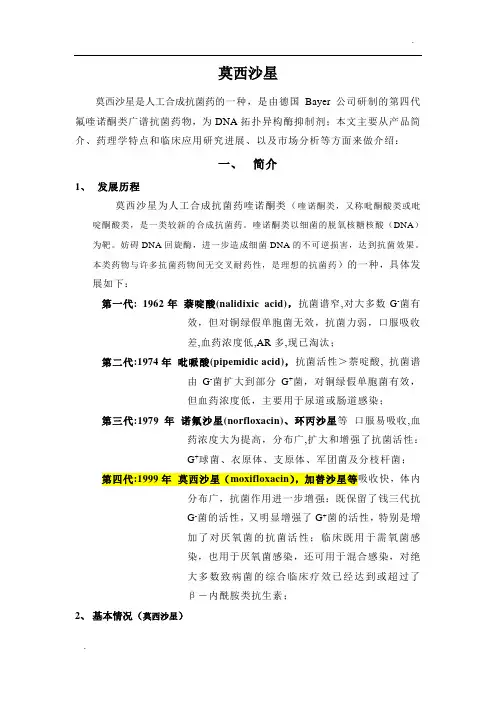
莫西沙星莫西沙星是人工合成抗菌药的一种,是由德国Bayer公司研制的第四代氟喹诺酮类广谱抗菌药物,为DNA拓扑异构酶抑制剂;本文主要从产品简介、药理学特点和临床应用研究进展、以及市场分析等方面来做介绍:一、简介1、发展历程莫西沙星为人工合成抗菌药喹诺酮类(喹诺酮类,又称吡酮酸类或吡啶酮酸类,是一类较新的合成抗菌药。
喹诺酮类以细菌的脱氧核糖核酸(DNA)为靶。
妨碍DNA回旋酶,进一步造成细菌DNA的不可逆损害,达到抗菌效果。
本类药物与许多抗菌药物间无交叉耐药性,是理想的抗菌药)的一种,具体发展如下:第一代: 1962年萘啶酸(nalidixic acid),抗菌谱窄,对大多数G-菌有效,但对铜绿假单胞菌无效,抗菌力弱,口服吸收差,血药浓度低,AR多,现已淘汰;第二代:1974年吡哌酸(pipemidic acid),抗菌活性>萘啶酸, 抗菌谱由G-菌扩大到部分G+菌,对铜绿假单胞菌有效,但血药浓度低,主要用于尿道或肠道感染;第三代:1979年诺氟沙星(norfloxacin)、环丙沙星等口服易吸收,血药浓度大为提高,分布广,扩大和增强了抗菌活性:G+球菌、衣原体、支原体、军团菌及分枝杆菌;第四代:1999年莫西沙星(moxifloxacin),加替沙星等吸收快,体内分布广,抗菌作用进一步增强:既保留了钱三代抗G-菌的活性,又明显增强了G+菌的活性,特别是增加了对厌氧菌的抗菌活性;临床既用于需氧菌感染,也用于厌氧菌感染,还可用于混合感染,对绝大多数致病菌的综合临床疗效已经达到或超过了β-内酰胺类抗生素;2、基本情况(莫西沙星)通用名:Moxifloxacin商品名:Actira(Bayer)CAS登录号:151096-09-2CAS登录号(盐酸盐):186826-86-8化学名:1-环丙基-6-氟-1,4-二氢-8-甲氧基-7-[(4a S,7a S)-八氢-6H-吡咯并[3,4-b]吡啶-6-基]-4-氧代-3-喹啉羧酸1-Cyclopropyl-6-fluoro-1,4-dihydro-8-methoxy-7-[(4a S,7a S)-octahydro-6H-pyrrolo[3,4-b]pyridin-6-yl]-4-oxo-3-quinolinecarboxylic acid结构式:分子式(相对分子量):C21H24FN3O4(401.43)理化性质(盐酸盐):白色至淡黄色结晶性粉末,熔点324-325℃上市情况:1999年在德国首次上市,同年12月在美国上市;2002年在我国上市;适应症:细菌感染用法与用量:拜复乐片,一日1次,每次400mg。

【药品名】莫西沙星【英文名】Mosifloxacin【别名】莫昔沙星【剂型】片剂:200mg。
【药理作用】莫西沙星的抗菌作用是抑制细菌细胞的合成。
细菌摄入药物后,DNA螺旋酶受到抑制,导致mRNA和蛋白质的合成不能控制,使细胞不再分裂,从而起到杀菌作用。
莫西沙星对绝大多数革兰阴性菌和很多革兰阳性菌及厌氧菌、支原体、衣原体、军团菌、脊髓灰质炎病毒等都具有较强的抗菌活性。
在体外抗菌试验中,本品对肺炎链球菌的抗菌活性比环丙沙星强4~16倍;对金黄色葡萄球菌(包括MRSA)的活性比环丙沙星强16倍,比司氟沙星强2倍;对厌氧菌的抗菌活性比环丙沙星强16倍;对支原体和衣原体的抗菌活性比环丙沙星强66~125倍。
莫西沙星的生物学特征是对革兰阳性球菌特别是葡萄球菌及肺炎球菌有很高的抗菌活性。
国外临床资料显示,肺炎链球菌对本品很敏感,是第4代氟喹诺酮类抗菌药物中活性最强者之一。
该药用于呼吸系统感染时,对与呼吸系统感染有关的细菌和绿色链球菌的抑制作用比头孢呋辛和红霉素要强,且不受β-内酰胺酶的影响。
但对甲氧西林耐药的葡萄球菌作用较弱。
莫西沙星在结构上进行修饰,在抗菌活性、抗菌范围、药动学性质上都明显发生改变,表现在下述方面:1.抗菌谱更广,既保留了前3代药物抗革兰阴性菌的高活性,又明显增强了抗革兰阳性菌的活性,并对厌氧菌、军团菌、支原体、衣原体等均显示出较强的作用。
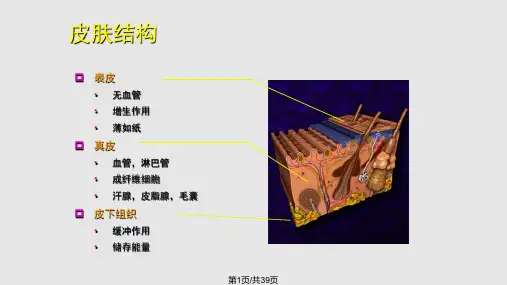
2.体内分布好,对组织的穿透力较强,可向炎性渗出液、痰液、胆汁、前列腺液、皮肤、软组织、耳、鼻、喉、女性生殖器等组织转运,以肺、肾的药物浓度最高,且可持续6h。
3.莫西沙星的细菌耐药性非常低,毒副反应发生率也较低,没有某些抗生素出现过的严重过敏反应。
【药动学】口服在肠道吸收完全,吸收率为75%~86%,并能很快达到血浆药物峰浓度,血浆药物浓度达峰时间为1.5h。
单剂量200mg顿服后,血浆药物浓度达峰时间为2~4h,血浆药物峰浓度为1.16μg/ml,与空腹服用相比较,与食物同服或餐后给药使血浆浓度达峰时间延长1.5h,但血浆半衰期和药-时曲线下面积几无改变。
1 AVELOX ®2 (moxifloxacin hydrochloride) Tablets3 AVELOX ® I.V.4 (moxifloxacin hydrochloride in sodium chloride injection)508918409, R X12/08WARNING:Fluoroquinolones, including AVELOX ®, are associated with an increased risk oftendinitis and tendon rupture in all ages. This risk is further increased in older patientsusually over 60 years of age, in patients taking corticosteroid drugs, and in patients withkidney, heart or lung transplants (see WARNINGS). 6To reduce the development of drug-resistant bacteria and maintain the effectiveness of 7 AVELOX and other antibacterial drugs, AVELOX should be used only to treat or prevent8 infections that are proven or strongly suspected to be caused by bacteria.9 DESCRIPTION10 AVELOX (moxifloxacin hydrochloride) is a synthetic broad spectrum antibacterial agent and is11 available as AVELOX Tablets for oral administration and as AVELOX I.V. for intravenous 12 administration. Moxifloxacin, a fluoroquinolone, is available as the monohydrochloride salt of 13 1-cyclopropyl-7-[(S,S)-2,8-diazabicyclo[4.3.0]non-8-yl]-6-fluoro-8-methoxy-1,4-dihydro-4-oxo-314 quinoline carboxylic acid. It is a slightly yellow to yellow crystalline substance with a molecular 15 weight of 437.9. Its empirical formula is C 21H 24FN 3O 4 *HCl and its chemical structure is as16follows:AVELOX Tablets are available as film-coated tablets containing moxifloxacin hydrochloride 17 18 19 (equivalent to 400 mg moxifloxacin). The inactive ingredients are microcrystalline cellulose, 20 lactose monohydrate, croscarmellose sodium, magnesium stearate, hypromellose, titanium 21 dioxide, polyethylene glycol and ferric oxide.22 AVELOX I.V. is available in ready-to-use 250 mL latex-free flexibags as a sterile, preservative free, 23 0.8% sodium chloride aqueous solution of moxifloxacin hydrochloride (containing 400 mg 24 moxifloxacin) with pH ranging from 4.1 to 4.6. The appearance of the intravenous solution is 25 yellow. The color does not affect, nor is it indicative of, product stability. The inactive26 ingredients are sodium chloride, USP, Water for Injection, USP, and may include hydrochloric 27 acid and/or sodium hydroxide for pH adjustment. AVELOX I.V. contains approximately 34.2 28 mEq (787 mg) of sodium in 250 mL. 29 30CLINICAL PHARMACOLOGY31 Absorption32 Moxifloxacin, given as an oral tablet, is well absorbed from the gastrointestinal tract. The33 absolute bioavailability of moxifloxacin is approximately 90 percent. Co-administration with a34 high fat meal (i.e., 500 calories from fat) does not affect the absorption of moxifloxacin.35 Consumption of 1 cup of yogurt with moxifloxacin does not significantly affect the extent or rate36 of systemic absorption (AUC).37 The mean (± SD) C max and AUC values following single and multiple doses of 400 mg38 moxifloxacin given orally are summarized below.C max (mg/L)AUC(mg•h/L)Half-life(hr)Single Dose OralHealthy (n = 372) 3.1 ± 1 36.1 ± 9.1 11.5 - 15.6* Multiple Dose OralHealthy young male/female (n = 15) Healthy elderly male (n = 8) Healthy elderly female (n = 8) Healthy young male (n = 8) Healthy young female (n = 9) 4.5 ± 0.53.8 ± 0.34.6 ± 0.63.6 ± 0.54.2 ± 0.548 ± 2.751.8 ± 6.754.6 ± 6.748.2 ± 949.3 ± 9.512.7 ± 1.939 * Range of means from different studies40 The mean (± SD) C max and AUC values following single and multiple doses of 400 mg41 moxifloxacin given by 1 hour I.V. infusion are summarized below.C max (mg/L)AUC(mg•h/L)Half-life(hr)Single Dose I.V.Healthy young male/female (n = 56)Patients (n = 118)3.9 ± 0.9 39.3 ± 8.6 8.2 - 15.4*Male (n = 64) 4.4 ± 3.7Female (n = 54) 4.5 ± 2< 65 years (n = 58) 4.6 ± 4.2≥ 65 years (n = 60) 4.3 ± 1.3Multiple Dose I.V.Healthy young male (n = 8) 4.2 ± 0.8 38 ± 4.7 14.8 ± 2.2Healthy elderly (n =12; 8 male, 4 female)Patients** (n = 107)6.1 ± 1.3 48.2 ± 0.9 10.1 ± 1.6Male (n = 58) 4.2 ± 2.6Female (n = 49) 4.6 ± 1.5< 65 years (n = 52) 4.1 ± 1.4≥ 65 years (n = 55) 4.7 ± 2.742 * Range of means from different studies43 ** Expected C max (concentration obtained around the time of the end of the infusion)44 Plasma concentrations increase proportionately with dose up to the highest dose tested (1200 mg45 single oral dose). The mean (± SD) elimination half-life from plasma is 12 ± 1.3 hours; steady-state46 is achieved after at least three days with a 400 mg once daily regimen.49 47 Mean Steady-State Plasma Concentrations of Moxifloxacin Obtained With 48Once Daily Dosing of 400 mg Either Orally (n=10) or by I.V. Infusion (n=12)50 Distribution51 Moxifloxacin is approximately 30-50% bound to serum proteins, independent of drug 52 concentration. The volume of distribution of moxifloxacin ranges from 1.7 to 2.7 L/kg. 53 Moxifloxacin is widely distributed throughout the body, with tissue concentrations often 54 exceeding plasma concentrations. Moxifloxacin has been detected in the saliva, nasal and 55 bronchial secretions, mucosa of the sinuses, skin blister fluid, subcutaneous tissue, skeletal muscle, 56 and abdominal tissues and fluids following oral or intravenous administration of 400 mg. 57 Moxifloxacin concentrations measured post-dose in various tissues and fluids following a 400 mg 58 oral or I.V. dose are summarized in the following table. The rates of elimination of moxifloxacin 59from tissues generally parallel the elimination from plasma.60 Moxifloxacin Concentrations (mean ± SD) in Tissues61 and the Corresponding Plasma Concentrations After a Single 400 mg Oral or62 Intravenous Dose §Tissue or Fluid NPlasmaConcentration(µg/mL)Tissue or FluidConcentration(µg/mL or µg/g)TissuePlasmaRatio:RespiratoryAlveolar Macrophages 5 3.3 ± 0.7 61.8± 27.3 21.2 ± 10Bronchial Mucosa 8 3.3 ± 0.7 5.5± 1.3 1.7 ± 0.3Epithelial Lining Fluid 5 3.3 ± 0.7 24.4± 14.7 8.7 ± 6.1SinusMaxillary Sinus Mucosa 4 3.7 ± 1.1† 7.6± 1.7 2 ± 0.3Anterior Ethmoid Mucosa 3 3.7 ± 1.1† 8.8± 4.3 2.2 ± 0.6Nasal Polyps 4 3.7 ± 1.1† 9.8± 4.5 2.6 ± 0.6Skin, MusculoskeletalBlister Fluid 5 3 ± 0.5‡ 2.6 ± 0.9 0.9 ± 0.2Subcutaneous Tissue 6 2.3 ± 0.4# 0.9 ± 0.3* 0.4 ± 0.6Skeletal Muscle 6 2.3 ± 0.4# 0.9 ± 0.2* 0.4 ± 0.1Intra-AbdominalAbdominal tissue 8 2.9 ± 0.5 7.6 ± 2 2.7 ± 0.8Abdominal exudate 10 2.3±0.5 3.5±1.2 1.6 ± 0.7Abscess fluid 6 2.7 ± 0.7 2.3 ±1.5 0.8±0.463 §all moxifloxacin concentrations were measured 3 hours after a single 400 mg dose, except the64 abdominal tissue and exudate concentrations which were measured at 2 hours post-dose and65 the sinus concentrations which were measured 3 hours post-dose after 5 days of dosing.66 † N = 567 ‡N = 768 #N = 1269 * Reflects only non-protein bound concentrations of drug.70 Metabolism71 Approximately 52% of an oral or intravenous dose of moxifloxacin is metabolized via72 glucuronide and sulfate conjugation. The cytochrome P450 system is not involved in73 moxifloxacin metabolism, and is not affected by moxifloxacin. The sulfate conjugate (M1)74 accounts for approximately 38% of the dose, and is eliminated primarily in the feces.75 Approximately 14% of an oral or intravenous dose is converted to a glucuronide conjugate76 (M2), which is excreted exclusively in the urine. Peak plasma concentrations of M2 are77 approximately 40% those of the parent drug, while plasma concentrations of M1 are generally78 less than 10% those of moxifloxacin.79 In vitro studies with cytochrome (CYP) P450 enzymes indicate that moxifloxacin does not inhibit80 CYP3A4, CYP2D6, CYP2C9, CYP2C19, or CYP1A2, suggesting that moxifloxacin is unlikely to81 alter the pharmacokinetics of drugs metabolized by these enzymes.82 Excretion83 Approximately 45% of an oral or intravenous dose of moxifloxacin is excreted as unchanged84 drug (~20% in urine and ~25% in feces). A total of 96% ± 4% of an oral dose is excreted as85 either unchanged drug or known metabolites. The mean (± SD) apparent total body clearance86 and renal clearance are 12 ± 2 L/hr and 2.6 ± 0.5 L/hr, respectively.87 Special Populations88 Geriatric89 Following oral administration of 400 mg moxifloxacin for 10 days in 16 elderly (8 male; 8 female)90 and 17 young (8 male; 9 female) healthy volunteers, there were no age-related changes in91 moxifloxacin pharmacokinetics. In 16 healthy male volunteers (8 young; 8 elderly) given a92 single 200 mg dose of oral moxifloxacin, the extent of systemic exposure (AUC and C max) was93 not statistically different between young and elderly males and elimination half-life was94 unchanged. No dosage adjustment is necessary based on age. In large phase III studies, the95 concentrations around the time of the end of the infusion in elderly patients following96 intravenous infusion of 400 mg were similar to those observed in young patients.97 Pediatric98 The pharmacokinetics of moxifloxacin in pediatric subjects have not been studied.99 Gender100 Following oral administration of 400 mg moxifloxacin daily for 10 days to 23 healthy males101 (19-75 years) and 24 healthy females (19-70 years), the mean AUC and C max were 8% and 16%102 higher, respectively, in females compared to males. There are no significant differences in103 moxifloxacin pharmacokinetics between male and female subjects when differences in body104 weight are taken into consideration.105 A 400 mg single dose study was conducted in 18 young males and females. The comparison of106 moxifloxacin pharmacokinetics in this study (9 young females and 9 young males) showed no107 differences in AUC or C max due to gender. Dosage adjustments based on gender are not necessary. 108 Race109 Steady-state moxifloxacin pharmacokinetics in male Japanese subjects were similar to those110 determined in Caucasians, with a mean C max of 4.1 µg/mL, an AUC24 of 47 µg•h/mL, and an111 elimination half-life of 14 hours, following 400 mg p.o. daily.112 Renal Insufficiency113 The pharmacokinetic parameters of moxifloxacin are not significantly altered in mild, moderate,114 severe, or end-stage renal disease. No dosage adjustment is necessary in patients with renal115 impairment, including those patients requiring hemodialysis (HD) or continuous ambulatory116 peritoneal dialysis (CAPD).117 In a single oral dose study of 24 patients with varying degrees of renal function from normal to118 severely impaired, the mean peak concentrations (C max) of moxifloxacin were reduced by 21% 119 and 28% in the patients with moderate (CL CR ≥ 30 and ≤ 60 mL/min) and severe (CL CR < 30 120 mL/min) renal impairment, respectively. The mean systemic exposure (AUC) in these patients121 was increased by 13%. In the moderate and severe renally impaired patients, the mean AUC for122 the sulfate conjugate (M1) increased by 1.7-fold (ranging up to 2.8-fold) and mean AUC and123 C max for the glucuronide conjugate (M2) increased by 2.8-fold (ranging up to 4.8-fold) and124 1.4-fold (ranging up to 2.5-fold), respectively.125 The pharmacokinetics of single dose and multiple dose moxifloxacin were studied in patients with 126 CL CR < 20 mL/min on either hemodialysis or continuous ambulatory peritoneal dialysis (8 HD, 8 127 CAPD). Following a single 400 mg oral dose, the AUC of moxifloxacin in these HD and CAPD 128 patients did not vary significantly from the AUC generally found in healthy volunteers. C max values of 129 moxifloxacin were reduced by about 45% and 33% in HD and CAPD patients, respectively, compared 130 to healthy, historical controls. The exposure (AUC) to the sulfate conjugate (M1) increased by 1.4- to 131 1.5-fold in these patients. The mean AUC of the glucuronide conjugate (M2) increased by a factor of 132 7.5, whereas the mean C max values of the glucuronide conjugate (M2) increased by a factor of 2.5 to 3, 133 compared to healthy subjects. The sulfate and the glucuronide conjugates of moxifloxacin are not 134 microbiologically active, and the clinical implication of increased exposure to these metabolites in 135 patients with renal disease including those undergoing HD and CAPD has not been studied.136 Oral administration of 400 mg QD moxifloxacin for 7 days to patients on HD or CAPD produced 137 mean systemic exposure (AUC ss) to moxifloxacin similar to that generally seen in healthy 138 volunteers. Steady-state C max values were about 22% lower in HD patients but were comparable 139 between CAPD patients and healthy volunteers. Both HD and CAPD removed only small 140 amounts of moxifloxacin from the body (approximately 9% by HD, and 3% by CAPD). HD and 141 CAPD also removed about 4% and 2% of the glucuronide metabolite (M2), respectively.142 Hepatic Insufficiency143 No dosage adjustment is recommended for mild, moderate, or severe hepatic insufficiency144 (Child-Pugh Classes A, B, or C). However, due to metabolic disturbances associated with hepatic 145 insufficiency, which may lead to QT prolongation, moxifloxacin should be used with caution in 146 these patients. (See WARNINGS and DOSAGE AND ADMINISTRATION).147 In 400 mg single oral dose studies in 6 patients with mild (Child-Pugh Class A) and 10 patients 148 with moderate (Child-Pugh Class B) hepatic insufficiency, moxifloxacin mean systemic 149 exposure (AUC) was 78% and 102%, respectively, of 18 healthy controls and mean peak 150 concentration (C max) was 79% and 84% of controls.151 The mean AUC of the sulfate conjugate of moxifloxacin (M1) increased by 3.9-fold (ranging 152 up to 5.9-fold) and 5.7-fold (ranging up to 8-fold) in the mild and moderate groups,153 respectively. The mean C max of M1 increased by approximately 3-fold in both groups (ranging 154 up to 4.7- and 3.9-fold). The mean AUC of the glucuronide conjugate of moxifloxacin (M2) 155 increased by 1.5-fold (ranging up to 2.5-fold) in both groups. The mean C max of M2 increased 156 by 1.6- and 1.3-fold (ranging up to 2.7- and 2.1-fold), respectively. The clinical significance of 157 increased exposure to the sulfate and glucuronide conjugates has not been studied. In a subset 158 of patients participating in a clinical trial, the plasma concentrations of moxifloxacin and159 metabolites determined approximately at the moxifloxacin Tmax following the first160 intravenous or oral moxifloxacin dose in the Child-Pugh Class C patients (n=10) were similar 161 to those in the Child-Pugh Class A/B patients (n=5), and also similar to those observed in162 healthy volunteer studies.163 Photosensitivity Potential164 A study of the skin response to ultraviolet (UVA and UVB) and visible radiation conducted in 32 165 healthy volunteers (8 per group) demonstrated that moxifloxacin does not show phototoxicity in 166 comparison to placebo. The minimum erythematous dose (MED) was measured before and after 167 treatment with moxifloxacin (200 mg or 400 mg once daily), lomefloxacin (400 mg once daily), or 168 placebo. In this study, the MED measured for both doses of moxifloxacin were not significantly 169 different from placebo, while lomefloxacin significantly lowered the MED. (See170 PRECAUTIONS, Information for Patients.)171 It is difficult to ascribe relative photosensitivity/phototoxicity among various fluoroquinolones 172 during actual patient use because other factors play a role in determining a subject’s 173 susceptibility to this adverse event such as: a patient’s skin pigmentation, frequency and 174 duration of sun and artificial ultraviolet light (UV) exposure, wearing of sunscreen and protective 175 clothing, the use of other concomitant drugs and the dosage and duration of fluoroquinolone 176 therapy (See ADVERSE REACTIONS and ADVERSE REACTIONS/Post-Marketing 177 Adverse Event Reports).178 Drug-drug Interactions179 The potential for pharmacokinetic drug interactions between moxifloxacin and itraconazole, 180 theophylline, warfarin, digoxin, atenolol, probenecid, morphine, oral contraceptives, ranitidine, 181 glyburide, calcium, iron, and antacids has been evaluated. There was no clinically significant 182 effect of moxifloxacin on itraconazole, theophylline, warfarin, digoxin, atenolol, oral 183 contraceptives, or glyburide kinetics. Itraconazole, theophylline, warfarin, digoxin, probenecid, 184 morphine, ranitidine, and calcium did not significantly affect the pharmacokinetics of 185 moxifloxacin. These results and the data from in vitro studies suggest that moxifloxacin is 186 unlikely to significantly alter the metabolic clearance of drugs metabolized by CYP3A4, 187 CYP2D6, CYP2C9, CYP2C19, or CYP1A2 enzymes.188 As with all other quinolones, iron and antacids significantly reduced bioavailability of 189 moxifloxacin.190 Itraconazole: In a study involving 11 healthy volunteers, there was no significant effect of 191 itraconazole (200 mg once daily for 9 days), a potent inhibitor of cytochrome P4503A4, on the 192 pharmacokinetics of moxifloxacin (a single 400 mg dose given on the 7th day of itraconazole 193 dosing). In addition, moxifloxacin was shown not to affect the pharmacokinetics of itraconazole. 194 Theophylline: No significant effect of moxifloxacin (200 mg every twelve hours for 3 days) on the 195 pharmacokinetics of theophylline (400 mg every twelve hours for 3 days) was detected in a study 196 involving 12 healthy volunteers. In addition, theophylline was not shown to affect the 197 pharmacokinetics of moxifloxacin. The effect of co-administration of a 400 mg dose of moxifloxacin 198 with theophylline has not been studied, but it is not expected to be clinically significant based on in 199 vitro metabolic data showing that moxifloxacin does not inhibit the CYP1A2 isoenzyme.200 Warfarin: No significant effect of moxifloxacin (400 mg once daily for eight days) on the 201 pharmacokinetics of R- and S-warfarin (25 mg single dose of warfarin sodium on the fifth day) 202 was detected in a study involving 24 healthy volunteers. No significant change in prothrombin 203 time was observed. (See PRECAUTIONS, Drug Interactions.)204 Digoxin: No significant effect of moxifloxacin (400 mg once daily for two days) on digoxin (0.6 205 mg as a single dose) AUC was detected in a study involving 12 healthy volunteers. The mean 206 digoxin C max increased by about 50% during the distribution phase of digoxin. This transient 207 increase in digoxin C max is not viewed to be clinically significant. Moxifloxacin 208 pharmacokinetics were similar in the presence or absence of digoxin. No dosage adjustment for 209 moxifloxacin or digoxin is required when these drugs are administered concomitantly.210 Atenolol: In a crossover study involving 24 healthy volunteers (12 male; 12 female), the mean 211 atenolol AUC following a single oral dose of 50 mg atenolol with placebo was similar to that 212 observed when atenolol was given concomitantly with a single 400 mg oral dose of moxifloxacin. 213 The mean C max of single dose atenolol decreased by about 10% following co-administration with214 a single dose of moxifloxacin.215 Morphine: No significant effect of morphine sulfate (a single 10 mg intramuscular dose) on the 216 mean AUC and C max of moxifloxacin (400 mg single dose) was observed in a study of 20 healthy 217 male and female volunteers.218 Oral Contraceptives: A placebo-controlled study in 29 healthy female subjects showed that 219 moxifloxacin 400 mg daily for 7 days did not interfere with the hormonal suppression of oral 220 contraception with 0.15 mg levonorgestrel/0.03 mg ethinylestradiol (as measured by serum 221 progesterone, FSH, estradiol, and LH), or with the pharmacokinetics of the administered 222 contraceptive agents.223 Probenecid: Probenecid (500 mg twice daily for two days) did not alter the renal clearance and total 224 amount of moxifloxacin (400 mg single dose) excreted renally in a study of 12 healthy volunteers. 225 Ranitidine: No significant effect of ranitidine (150 mg twice daily for three days as 226 pretreatment) on the pharmacokinetics of moxifloxacin (400 mg single dose) was detected in a 227 study involving 10 healthy volunteers.228 Antidiabetic agents: In diabetics, glyburide (2.5 mg once daily for two weeks pretreatment and 229 for five days concurrently) mean AUC and C max were 12% and 21% lower, respectively, when 230 taken with moxifloxacin (400 mg once daily for five days) in comparison to placebo. Nonetheless, 231 blood glucose levels were decreased slightly in patients taking glyburide and moxifloxacin in 232 comparison to those taking glyburide alone, suggesting no interference by moxifloxacin on the 233 activity of glyburide. These interaction results are not viewed as clinically significant.234 Calcium: Twelve healthy volunteers were administered concomitant moxifloxacin (single 400 235 mg dose) and calcium (single dose of 500 mg Ca++ dietary supplement) followed by an additional 236 two doses of calcium 12 and 24 hours after moxifloxacin administration. Calcium had no 237 significant effect on the mean AUC of moxifloxacin. The mean C max was slightly reduced and the 238 time to maximum plasma concentration was prolonged when moxifloxacin was given with 239 calcium compared to when moxifloxacin was given alone (2.5 hours versus 0.9 hours). These 240 differences are not considered to be clinically significant.241 Antacids: When moxifloxacin (single 400 mg tablet dose) was administered two hours before, 242 concomitantly, or 4 hours after an aluminum/magnesium-containing antacid (900 mg aluminum 243 hydroxide and 600 mg magnesium hydroxide as a single oral dose) to 12 healthy volunteers there 244 was a 26%, 60% and 23% reduction in the mean AUC of moxifloxacin, respectively. Moxifloxacin 245 should be taken at least 4 hours before or 8 hours after antacids containing magnesium or 246 aluminum, as well as sucralfate, metal cations such as iron, and multivitamin preparations with 247 zinc, or VIDEX® (didanosine) chewable/ buffered tablets or the pediatric powder for oral solution. 248 (See PRECAUTIONS, Drug Interactions and DOSAGE AND ADMINISTRATION.)249 Iron: When moxifloxacin tablets were administered concomitantly with iron (ferrous sulfate 100 mg 250 once daily for two days), the mean AUC and C max of moxifloxacin was reduced by 39% and 59%, 251 respectively. Moxifloxacin should only be taken more than 4 hours before or 8 hours after iron products. 252 (See PRECAUTIONS, Drug Interactions and DOSAGE AND ADMINISTRATION.)253 Electrocardiogram: Prolongation of the QT interval in the ECG has been observed in some 254 patients receiving moxifloxacin. Following oral dosing with 400 mg of moxifloxacin the mean (± 255 SD) change in QTc from the pre-dose value at the time of maximum drug concentration was 6 256 msec (± 26) (n = 787). Following a course of daily intravenous dosing (400 mg; 1 hour infusion 257 each day) the mean change in QTc from the Day 1 pre-dose value was 9 msec (± 24) on Day 1 (n =258 69) and 3 msec (± 29) on Day 3 (n = 290). (See WARNINGS.)259 There is limited information available on the potential for a pharmacodynamic interaction in 260 humans between moxifloxacin and other drugs that prolong the QTc interval of the 261 electrocardiogram. Sotalol, a Class III antiarrhythmic, has been shown to further increase the 262 QTc interval when combined with high doses of intravenous (I.V.) moxifloxacin in dogs. 263 Therefore, moxifloxacin should be avoided with Class IA and Class III antiarrhythmics. (See 264 ANIMAL PHARMACOLOGY, WARNINGS, and PRECAUTIONS.)265 MICROBIOLOGY266 Moxifloxacin has in vitro activity against a wide range of Gram-positive and Gram-negative 267 microorganisms. The bactericidal action of moxifloxacin results from inhibition of the 268 topoisomerase II (DNA gyrase) and topoisomerase IV required for bacterial DNA replication, 269 transcription, repair, and recombination. It appears that the C8-methoxy moiety contributes to 270 enhanced activity and lower selection of resistant mutants of Gram-positive bacteria compared to 271 the C8-H moiety. The presence of the bulky bicycloamine substituent at the C-7 position prevents 272 active efflux, associated with the NorA or pmrA genes seen in certain Gram-positive bacteria. 273 The mechanism of action for quinolones, including moxifloxacin, is different from that of 274 macrolides, beta-lactams, aminoglycosides, or tetracyclines; therefore, microorganisms resistant 275 to these classes of drugs may be susceptible to moxifloxacin and other quinolones. There is no 276 known cross-resistance between moxifloxacin and other classes of antimicrobials.277 In vitro resistance to moxifloxacin develops slowly via multiple-step mutations. Resistance to 278 moxifloxacin occurs in vitro at a general frequency of between 1.8 x 10–9 to < 1 x 10–11 for 279 Gram-positive bacteria.280 Cross-resistance has been observed between moxifloxacin and other fluoroquinolones against 281 Gram-negative bacteria. Gram-positive bacteria resistant to other fluoroquinolones may, 282 however, still be susceptible to moxifloxacin.283 Moxifloxacin has been shown to be active against most strains of the following microorganisms, 284 both in vitro and in clinical infections as described in the INDICATIONS AND USAGE section. 285 Aerobic Gram-positive microorganisms286 Enterococcus faecalis (many strains are only moderately susceptible)287 Staphylococcus aureus (methicillin-susceptible strains only)288 Streptococcus anginosus289 Streptococcus constellatus290 Streptococcus pneumoniae (including multi-drug resistant strains [MDRSP]*)291 Streptococcus pyogenes292 * MDRSP, Multi-drug resistant Streptococcus pneumoniae includes isolates previously known 293 as PRSP (Penicillin-resistant S. pneumoniae), and are strains resistant to two or more of the 294 following antibiotics: penicillin (MIC ≥ 2 μg/mL), 2nd generation cephalosporins (e.g., 295 cefuroxime), macrolides, tetracyclines, and trimethoprim/sulfamethoxazole.296 Aerobic Gram-negative microorganisms297 Enterobacter cloacae298 Escherichia coli299 Haemophilus influenzae300 Haemophilus parainfluenzae301 Klebsiella pneumoniae302 Moraxella catarrhalis303 Proteus mirabilis304 Anaerobic microorganisms305 Bacteroides fragilis306 Bacteroides thetaiotaomicron307 Clostridium perfringens308 Peptostreptococcus species309 Other microorganisms310 Chlamydia pneumoniae311 Mycoplasma pneumoniae312 The following in vitro data are available, but their clinical significance is unknown.313 Moxifloxacin exhibits in vitro minimum inhibitory concentrations (MICs) of 2 µg/mL or less314 against most (≥ 90%) strains of the following microorganisms; however, the safety and315 effectiveness of moxifloxacin in treating clinical infections due to these microorganisms have not316 been established in adequate and well-controlled clinical trials.317 Aerobic Gram-positive microorganisms318 Staphylococcus epidermidis (methicillin-susceptible strains only)319 Streptococcus agalactiae320 Streptococcus viridans group321 Aerobic Gram-negative microorganisms322 Citrobacter freundii323 Klebsiella oxytoca324 Legionella pneumophila325 Anaerobic microorganisms326 Fusobacterium species327 Prevotella species328 Susceptibility Tests329 Dilution Techniques: Quantitative methods are used to determine antimicrobial minimum330 inhibitory concentrations (MICs). These MICs provide estimates of the susceptibility of bacteria331 to antimicrobial compounds. The MICs should be determined using a standardized procedure.332 Standardized procedures are based on a dilution method1 (broth or agar) or equivalent with333 standardized inoculum concentrations and standardized concentrations of moxifloxacin powder.334 The MIC values should be interpreted according to the following criteria:335 For testing Enterobacteriaceae and methicillin-susceptible Staphylococcus aureus:336 MIC (µg/mL) Interpretation(S)337 ≤ 2 Susceptible 338 4 Intermediate (I)339 ≥ 8 Resistant (R)。