精神分裂症 英文病历报告
- 格式:docx
- 大小:14.70 KB
- 文档页数:2
病例报告英文范文医护英语Title: Case Report: Management of a Complex Surgical Case with Multi-system Involvement.Introduction:Surgical cases with multi-system involvement present unique challenges to the treating healthcare team. This case report outlines the management of a complex surgical case with involvement of multiple organ systems, highlighting the importance of interdisciplinary collaboration and comprehensive preoperative planning.Case Presentation:The patient, a 56-year-old male with a history of hypertension and type 2 diabetes, presented to the emergency department with complaints of severe abdominal pain and distension. Initial evaluation revealed a large abdominal mass with ascites. Computed tomography (CT) scanconfirmed the presence of a large, complex abdominal mass with extension into the retroperitoneum, compressing the adjacent organs and vessels.Diagnostic Workup:The patient underwent a series of diagnostic tests including blood work, imaging studies, and consultations with various specialists. The laboratory tests revealed anemia and elevated liver enzymes. The imaging studies, including CT scan and magnetic resonance imaging (MRI), demonstrated a large mass with heterogeneous enhancement, compressing the adjacent organs and vessels. The mass was suspected to be a malignant neoplasm, possibly originating from the pancreas or adrenal glands.Preoperative Planning:Given the complexity of the case and the involvement of multiple organ systems, a preoperative planning meeting was held with the surgeons, anesthesiologists, intensivists, radiologists, pathologists, and oncology team. The plan wasto perform a laparotomy with excision of the mass, followed by reconstruction of the affected organs and vessels. The anesthesiologists recommended a general anesthetic with invasive monitoring, while the intensivists recommended postoperative admission to the intensive care unit (ICU)for close monitoring.Surgical Procedure:The laparotomy was performed through a midline incision. Intraoperatively, the mass was found to be adherent to multiple organs and vessels, including the liver, spleen, kidney, and inferior vena cava. Careful dissection was performed to separate the mass from the adjacent structures, while preserving the vascular integrity. The mass was successfully excised, and the affected organs were reconstructed using sutures and patches. The patient tolerated the procedure well, and hemostasis was achieved.Postoperative Course:The patient was admitted to the ICU for closemonitoring. Postoperatively, he developed transient respiratory failure and required mechanical ventilation. He also developed wound dehiscence due to the extensive surgical dissection. The ICU team managed the patient's respiratory status and provided wound care. The patient gradually improved and was extubated on the third postoperative day. He was transferred to the general surgical floor on the fifth postoperative day and discharged home on the tenth postoperative day.Pathological Analysis:The pathological examination of the excised mass revealed a poorly differentiated adenocarcinoma, likely originating from the pancreas. The surgical margins were negative for tumor involvement. The patient was referred to the oncology team for further management, including adjuvant chemotherapy and follow-up surveillance.Conclusion:This case report demonstrates the successful managementof a complex surgical case with multi-system involvement. The interdisciplinary collaboration and comprehensive preoperative planning were essential for achieving a successful outcome. The case highlights the importance of a multidisciplinary approach in the management of complex surgical cases, ensuring optimal patient care.。
英语病例报告范文Case Report: A Rare Case of Acute Myeloid Leukemia with Unusual Presentation。
Introduction:Acute Myeloid Leukemia (AML) is a malignant disorder characterized by the proliferation of abnormal myeloid cells in the bone marrow. It typically presents with symptoms such as fatigue, fever, and easy bruising. However, in some rare cases, AML can manifest with atypical symptoms, leading to diagnostic challenges. This report presents a unique case of AML with an unusual presentation.Case Presentation:A 45-year-old male presented to the emergency department with complaints of severe headaches, dizziness, and blurred vision. He had a history of chronic migraines and was initially treated for a severe migraine attack. However, his symptoms did not improve with standard migraine medications. On further evaluation, the patient was found to have profound anemia, with a hemoglobin level of 6 g/dL.Investigations:A complete blood count revealed severe pancytopenia, with a white blood cell count of 1.2 × 10^9/L, hemoglobin of 6 g/dL, and platelet count of 50 × 10^9/L. Peripheral blood smear examination showed blasts comprising 70% of the total nucleated cells, suggesting the possibility of acute leukemia. Bone marrow aspiration and biopsy were performed to confirm the diagnosis.Diagnosis:The bone marrow examination revealed hypercellularity with infiltration of blasts comprising more than 80% of the nucleated cells. Flow cytometry analysis showed expression of myeloid markers (CD13, CD33) and absence of lymphoid markers,confirming the diagnosis of acute myeloid leukemia. Cytogenetic analysis revealed the presence of a complex karyotype, which is associated with a poor prognosis.Treatment and Outcome:The patient was promptly started on induction chemotherapy with a combination of cytarabine and daunorubicin. He experienced severe myelosuppression and required supportive care, including red blood cell and platelet transfusions. Despite the initial response to chemotherapy, the patient developed refractory disease and relapsed within six months of completing consolidation therapy. Salvage chemotherapy and allogeneic stem cell transplantation were considered, but the patient declined further treatment due to poor prognosis and opted for palliative care.Discussion:This case highlights the importance of considering acute leukemia in the differential diagnosis of atypical presentations, even in the absence of classic symptoms. The unusual symptoms of severe headaches, dizziness, and blurred vision initially misled the clinicians to suspect migraine as the primary cause. However, the presence of profound anemia and pancytopenia raised suspicion of an underlying hematological disorder. Timely evaluation and appropriate diagnostic tests, including bone marrow examination, were crucial in establishing the correct diagnosis.Conclusion:This case report emphasizes the need for a high index of suspicion for acute leukemia, especially in patients presenting with unusual symptoms. Prompt diagnosis and initiation of appropriate treatment are essential for improving patient outcomes. Further research is warranted to better understand the underlying mechanisms of atypical presentations in AML and to develop targeted therapies for patients with poor prognostic factors.。

关于三个病人病历的报告英语作文英文回答:Patient #1。
Presenting complaint: abdominal pain, nausea, and vomiting.History of present illness: The patient is a 54-year-old male who presents to the emergency department with a 2-day history of severe abdominal pain, nausea, and vomiting. The pain is located in the periumbilical area and is described as sharp and intermittent. He has also experienced several episodes of non-bilious vomiting. The patient has not had any bowel movements or flatus in the past 2 days.Past medical history: The patient has a history of hypertension and hyperlipidemia. He is currently taking lisinopril and atorvastatin.Physical examination: The patient is afebrile and in moderate distress. His abdomen is soft and non-tender to palpation. There is no rebound tenderness or guarding. Bowel sounds are hypoactive.Laboratory tests: The patient's white blood cell count is elevated at 12,000/μL. His liver function tests are normal.Imaging: A CT scan of the abdomen shows a small bowel obstruction in the distal ileum.Diagnosis: Small bowel obstruction.Treatment: The patient is admitted to the hospital and treated with intravenous fluids and antibiotics. He is also placed on a bowel rest regimen.Patient #2。
病例报告英语范文深度解析与中文对照**[English Version]****Case Report: Unusual Manifestations of Acute Appendicitis in a Pediatric Patient****Abstract** This case report presents an unusual case of acute appendicitis in a 12-year-old male patient. The patient presented with atypical symptoms, making the initial diagnosis challenging. The aim of this report is to highlight the importance of clinical suspicion and thorough investigation in diagnosing uncommon presentations of common conditions.**Introduction** Acute appendicitis is a common surgical emergency, typically presenting with right lower quadrant abdominal pain, fever, and leukocytosis. However, atypical presentations are not uncommon, especially in pediatric patients. This case report describes an instance where the classic symptoms were absent, leading to delayed diagnosis.**Case Presentation** A 12-year-old male patient presented to the emergency department with a history ofvague abdominal discomfort for the past three days. Thepain was intermittent and located in the epigastric region, radiating to the back. The patient had no history of fever, vomiting, or changes in bowel habits. Physical examination revealed mild tenderness in the epigastric region, with no rebound tenderness or guarding. Laboratory tests were remarkable for a mildly elevated white blood cell count.Initial differential diagnosis included gastroenteritis, urinary tract infection, and pancreatitis. However, due to persistent abdominal discomfort and the presence of mild leukocytosis, the possibility of appendicitis was entertained. Abdominal ultrasound revealed a distended appendix with peri-appendiceal fluid, confirming the diagnosis of acute appendicitis.**Discussion** This case highlights the challenges in diagnosing acute appendicitis in pediatric patients, especially when the classic symptoms are absent. Clinicians must maintain a high index of suspicion, consideringatypical presentations, especially in children. Detailed history, thorough physical examination, and appropriatediagnostic testing are crucial in making an accurate diagnosis.**Conclusion** Acute appendicitis can present with atypical symptoms in pediatric patients, making diagnosis challenging. Clinicians should be aware of these presentations and utilize diagnostic tools such as ultrasound to aid in the prompt and accurate diagnosis of appendicitis. Prompt surgical intervention is essential to prevent complications and ensure patient recovery.**[Chinese Version]****病例报告:儿童急性阑尾炎的非典型表现****摘要** 本病例报告介绍了一名12岁男性患者的急性阑尾炎非典型表现。
Ref: Mr. FlynnJune 5, 2010Our local doctor in SH led patient to Shanghai Mental Health Center at 2 PM this afternoon then visited psychiatrian there. Following is updated information for the patient. The insured came to Shanghai in Dec of 2009 to study Chinese. In January 2010 the Chinese course finished then he started to live in an apartment alone. He admitted since April of 2010 visual/audio hallucination started. On May 9 he visited psychiatrian in UFH of Shanghai then Olanzapine was administered in out-patient department, until he was admitted there on May 29 for operation of Tibia/fibula fracture. Upon discharge of UFH SH, anti-schizophrenia agent Abilify 5 mg Bid and Clonazapam 2mg QN were ever prescript. Upon enquiry by the psychiatrian in SH Mental Health Center this afternoon, the insured showed state of alert, easy contact. He still complained instructive audio-hallucination and persecutive feeling (delusion). He felt somtimes his thought was fully perspected by others. However, no tendency of violent assaulting or obvious depression were noted. He had no recognization of his condition being sicked.Diagnosis: schizophreniaTreatment/advice: 1. Olanzapine 5 mg Bid.2. He should follow up in out-patient department 1week later to regulate(add?) dose of Olanzapine.3. His current condition permits travel now, butunder medical escort.4. He should be monitored by relation or caregiverfor regular use of medication after back to UK. Inthis case, there is no need to be admitted intohospital for therapy. If there is none to look afterhim for medication taking, admission of hospital isadvised after he is back to UK.After the visit of psychiatrian finished this afternoon, the insured was sent to Changning District Central Hospital for cardiologist visit.There was no discomfort complaint of chest depress or shortness of breath. His vital signs as BP, T, RR, HR and oxygen saturation were in normal range. Heart and lungs (-).ECG of this afternoon: normal.Labs done this afternoonBlood routine: WBC 10800(normal < 10000), with LYM 41%.CK, CK-MB, Tryponin etc were in normal range.Coagulation function tests were basically in normal range.Blood platelet cell: 380000(100000-300000)D-dimmer result was normal.The cardiologist thought his heart condition was stable now, no impression of cardiac ischemia. Then he was prescript Cefuroxime tabs and L-Glutamine, Sodium Gualenate Granules. The cardiologist thought his heart condition would not disturb his travel.The current medications he is taking now:1. Oxycodone/Paracetamol tabs (painkiller)2. Cefuroxime tabs3. L-Glutamine, Sodium Gualenate Granules4. Aripiprozole tabsHope above information will be helpful to you.。
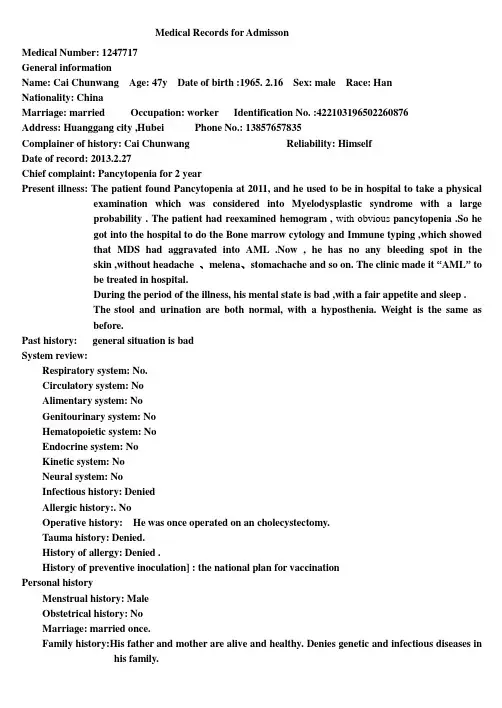
Medical Records for AdmissonMedical Number: 1247717General informationName: Cai Chunwang Age: 47y Date of birth :1965. 2.16 Sex: male Race: HanNationality: ChinaMarriage: married Occupation: worker Identification No. :422103************Address: Huanggang city ,Hubei Phone No.: 138********Complainer of history:Cai Chunwang Reliability: HimselfDate of record: 2013.2.27Chief complaint: Pancytopenia for 2 yearPresent illness: The patient found Pancytopenia at 2011, and he used to be in hospital to take a physical examination which was considered into Myelodysplastic syndrome with a largeprobability . The patient had reexamined hemogram , with obvious pancytopenia .So hegot into the hospital to do the Bone marrow cytology and Immune typing ,which showedthat MDS had aggravated into AML .Now , he has no any bleeding spot in theskin ,without headache 、melena、stomachache and so on. The clinic made it “AML” tobe treated in hospital.During the period of the illness, his mental state is bad ,with a fair appetite and sleep .The stool and urination are both normal, with a hyposthenia. Weight is the same asbefore.Past history: general situation is badSystem review:Respiratory system: No.Circulatory system: NoAlimentary system: NoGenitourinary system: NoHematopoietic system:NoEndocrine system:NoKinetic system:NoNeural system:NoInfectious history: DeniedAllergic history:. NoOperative history: He was once operated on an cholecystectomy.Tauma history: Denied.History of allergy: Denied .History of preventive inoculation] : the national plan for vaccinationPersonal historyMenstrual history:MaleObstetrical history:NoMarriage: married once.Family history:His father and mother are alive and healthy. Denies genetic and infectious diseases in his family.Physical examinationT 37℃, P95 /min, R 20 /min, BP 124/78 mmHg. He is well developed and moderately nourished. Active position. The skin was not stained yellow. Cyanosis. No pigmentation. No skin eruption. Spider angioma was not seen. No pitting edema. Superficial lymph nodes were not found enlarged in his neck.HeadCranium: size : normal large small deformity. No coxycephaly squared skull deforming skull. No tenderness mass sunk .Ear: Auricle is normal .No excretions of external auditory canal. No Tenderness of mastoid.Nose: Shape is normal .No nosalala flap obsruction excretions nasal sinus tenderness .Eye: Eyes eyelid、eye ball、Sclera、Pupils and reaction to light are normal.Mouth: Mouth lips is normal .Opening of parotid gland duct: normal .Tongue : normal.Gums: normal .lead line tooth:regular.Tonsils: pharynx: voice: normal.Neck: No resistence.Hepatojugular reflux:(-).thyroid: normal.ChestChest wall: normalThorax : normal.Breast:normal symmetricalLungs : Inspection : movement of respiration : normal .Intercostal space :normal .Palpation : vocal fremitus : normal .pluernal friction rubs: No.Subcutaneous crepitus: No.percussion:resonance.Dusculation: breath regular.Breath sound: normal.Rale: No.Vocal conduction:norma .Plueral friction rubs: No.Heart:Inspection:bulging in precordial region : No.apex impulse:normal. position: normal .Palpation: apex impulse : normal .Thrills :No.Percardial friction rub s:NO.Percussion:relative cardiac outline: normal.Ausculation: heart rate 95bpm/min ,rhythm:regular.Heart sound:S1 normal.S2 normal.S3 No. S4 no. Extra heartsound No. Opening snap others murmurs: N.Pericardial friction rubs no. Peripheral vessals:normal.Abdomen:Inspection: shape normal .Abdominal respiration: existence .Umbilicus: normal protruding excretions others: NO.Palpation: soft.Tenderness: NO.Mass NO.li ver:can’t be touched.gallbladder: can’t be touched.tenderness No.spleen: can’t be touched.Kideny:can’t betouched.tenderness mobility tenderness of ureters: No.Percussion: borders of liver dull:existence .pper borders of liver on right midclavicular line intercostal space shifting dullnessNo. tenderness in renal region No.Ausculation : borhorygmus normal .Gurgling No.vessalbruits No.Extremities: Spine : normal.Spinous process :no.Mobility : normal. Extremeties: normal.Neural system:not found any abnormality.Genitourinary system: not examined.Rectum:not examinedHistory summary1.General information: Cai Chunwang ,male ,47y.2.Chief complaint: Pancytopenia for 2 year.3. past history: general situation is bad, Infectious history: Denied. Allergic history:. No.Operative history:He was once operated on an cholecystectomy. Tauma history: Denied. History of allergy:Denied . Historyof preventive inoculation] : the national plan for vaccination4. Physical examination: T 37℃, P95 /min, R 20 /min, BP 124/78 mmHg. his mental state is bad.Superficial lymph nodes were not found enlarged in his neck. heart rate 95 bpm/min ,rhythm:regular.Heart sound:S1 normal. S2 normal. S3 No. S4 no. shape normal . Abdominal respiration: existence .Umbilicus: normal protruding excretions others: NO. Palpation: soft. Tenderness: NO. Mass NO.liver:can’t be touched. gallbladder: can’t be touched. tenderness No. spleen: can’t be touched.Kideny:can’t be touched. tenderness mobility tenderness of ureters: No. Percussion: borders of liver dull: existence . pper borders of liver on right midclavicular line intercostal space shifting dullness No.tenderness in renal region No. Ausculation : borhorygmus normal . Gurgling No. vessal bruits No.movement of respiration : normal . Intercostal space :normal . Palpation : vocal fremitus : normal .pluernal friction rubs: No. Subcutaneous crepitus: No. percussion: resonance. Dusculation: breath regular. Breath sound: normal. Rale: No. Vocal conduction: norma .5.Specialist case:serious anemia. The skin was not stained yellow. Cyanosis. No pigmentation. No skin eruption. Spider angioma was not seen. No pitting edema. Superficial lymph nodes were not found enlarged in his neck.No tenderness of sternum. Ausculation of the heart and lung has not obvious abnormality. Abdomen is soft . Tenderness: NO. Mass NO. liver:can’t be touched. gallbladder: can’t be touched. tenderness No. spleen: can’t be touched. Extremeties are normal .6 . investigation information: one medical record of 2013 year.Impression: AMLSignature: Huang QiulanDate: 2013.2.27。
病历包括:体温检查表,长期医嘱单,临时医嘱单,病史记录,病人入院评估表,护理记录单,精神科宣教,健康指导表,入院须知,精神疾病患者住院知情同意书,体检检查记录表。
病史记录第一次-第三次住院病史摘要患者73年无明显原因精神异常,当时主要猜疑有人在陷害他,吵闹不安,工作不能胜任。
当时由单位及家属陪同到医院就诊,诊断精神分裂症,给予氯丙嗪奋反静等治疗后,缓解后出院,先后于74-76年期间在总院三次住院,均诊断精神分裂症,给予氯丙嗪奋反静治疗,好转出院,85年病情加重,表现为耳闻人语,夜眠差,自言自语,行为紊乱,猜疑,冲动打人,故于85.9-86.4第五次住本院,诊断精神分裂症,给予氯丙嗪氯氮平治疗后出院。
94.9.18-01.10.8,02.6.21-03.1.6住院,诊断精神分裂症,显著缓解后出院。
第四次住院病史(本次09.2.5――)03年1月6日,出院后开始能坚持服药,病情稳定,生活能自理,08年9月病情出现反复,表现:耳闻人语,说党中央有人害他,自称“华国锋”,乱说乱跑,自己写信到公安,告知罪行等。
近一月来病情加重表现,易激惹,企图凶杀,有人害他,要自己自杀,把刀乱舞,影响社区安全,夜眠差等,劝说无效,来医院要求住院治疗。
本次发病以来,舞消极自杀行为,由冲动、外出行为,进食尚可,夜眠差,个人生活尚能自理,大小便正常。
过去史:07年发慢支,痔疮病史,目前无治疗,情绪稳定,未发现器质性疾病,无感染,抽搐,脑外伤,骨折史,无传染病史,有过敏史(青霉素),无输血史,预防接种不祥。
个人史:1、生长发育:排行老五,足月顺产,体健,发育正常2、学习工作情况:适龄上学,学习成绩尚可,65年初中毕业,毕业后在上海电机厂读校,68年毕业留单位工作,能胜任,自73年患病后就未上班,00年12月30日正式退休手续。
3、恋爱婚姻史:无恋爱,婚姻史。
4、病前性格及不良嗜好,个性内向,倔犟,不合群,有吸烟嗜好。
家族史:1、家族成员姓名、性别、年龄、工作状态、疾病2、二系三代精神发作史否认二系三代有精神病疾病史体格检查神清心肺(一)BP120/180MMG辅助检查正在进行中一般情况1、意识,清2、定向:对时间,地点,人物,定向力强(现在是甚么地方?)“精神病医院”(现在几月几日?)“2.6”(我是干什么的?)“医生”3、仪表:欠整4、接触:欠合作5、注意力:欠集中感知1、错觉:未引出(这是甚么?)“钢笔”(对)(这是甚么?)“听诊器”(对)2、幻觉:存在言语性幻听(没有人的时候有人和你讲话吗?)“有的”(什么人?)“确有”(男的女的?)“不清楚”(讲的甚么?)“要害我,你也是来的”3、感知综合障碍:未发现躯体和时间问题思维1、思维联想障碍(你知道为什么住院?)“病发了”(为什么会这样?)“不知道”(这样住院几次)“四次”2、思维逻辑障碍:未发现(谁送过来的)“家人”(知道为什么?)“不知道”(在家干什么?)“作作家务,也没啥”3、思维内容障碍:存在被害妄想,夸大妄想(有人害你)“是的,党中央派人”(家里有人害你吗?)“有的,饭里放毒”(你怎么发现的)“我吃上去感觉不适”(华国锋怎么回事?)“就是我,你不认识”(你多大了)“你看看”(华国锋是干什么的?)“你说呢,自己面子很好,有邓小平、江泽民多人害我,你也是派来的”4、思维属性障碍:未引出(自己不讲你的事,别人会知道吗?)“不会的”(别人的想法你知道吗?)“不会的”(有人跟踪你吗?)“没有”情感:1、根据病人的姿态、动作、言语、面部表情等外在表现,表情平淡,情感反应不协调。


关于三个病人病历的报告英语作文{z}Title: Report on the Medical Records of Three PatientsIntroduction:This report aims to provide a comprehensive overview of the medical records of three patients.The patients" backgrounds, diagnoses, and treatments will be discussed in detail.Patient 1:ame: Sarah JohnsonAge: 35 yearsGender: FemaleMedical History:Sarah has a history of diabetes mellitus type 2.She has been suffering from the condition for the past 5 years.She has been on insulin therapy and a balanced diet.Complaints:Sarah visited the hospital due to persistent vomiting and abdominal pain.She also complained of dizziness and weakness.Diagnosis:Upon examination and laboratory tests, Sarah was diagnosed with diabetic ketoacidosis (DKA).The high blood sugar levels and the presence of ketones in her urine confirmed the diagnosis.Treatment:Sarah received intravenous fluids to correct the dehydration.Insulin therapy was adjusted to lower her blood sugar levels.Close monitoring of her blood sugar levels and urine ketone levels was done.Patient 2:ame: Mark ThompsonAge: 45 yearsGender: MaleMedical History:Mark has a history of hypertension and myocardial infarction.He has been on medication for the past 2 years to manage his blood pressure and prevent further heart complications.Complaints:Mark visited the hospital with complaints of severe chest pain and shortness of breath.He also experienced sweating and nausea.Diagnosis:Upon evaluation, Mark was diagnosed with unstable angina.An electrocardiogram (ECG) revealed ST-segment depression, indicating myocardial ischemia.Treatment:Mark was stabilized with intravenous medications to relieve chest pain and improve blood flow to the heart.He was also given medications to lower his blood pressure and reduce the risk of further heart attacks.Patient 3:ame: Emily WilsonAge: 28 yearsGender: FemaleMedical History:Emily has a history of irritable bowel syndrome (IBS).She experiences periodic abdominal pain and diarrhea.Complaints:Emily sought medical attention due to severe abdominal cramps and frequent bowel movements.She also complained of bloating and flatulence.Diagnosis:Upon examination and laboratory tests, Emily was diagnosed with acute appendicitis.An ultrasound revealed an enlarged appendix.Treatment:Emily underwent emergency appendectomy to remove the inflamed appendix.She was given antibiotics to prevent感染and manage any postoperative complications.Conclusion:This report highlights the medical records of three patients with different health conditions.Sarah was diagnosed with diabetic ketoacidosis, Mark experienced unstable angina, and Emily underwentappendectomy due to acute appendicitis.Timely diagnoses and appropriate treatments were provided to improve their health conditions.。
⏹Case History⏹DefinitionA case history is a medical record of a patient’s illness. It records the whole medical case and functions as the basis for medical practitioners to make an accurate diagnosis and proposes effective treatment or preventive measures.Case histories fall into two kinds:in-patient case histories and out-patient case histories.⏹Language FeaturesHistory and Physical usually involves past tense ( for history of present illness, past medical history, family history and review of systems concerning past information), and present tense ( review of system, physical examination, laboratory data, and plans ). Structurally, noun phrases are frequently used in physical examination, and ellipsis of subject is very common in review of system.⏹In-patient Case HistoriesAn in-patient case history is also termed as History and Physical. It is an account of a patient’s present complaints with descriptions of his past medical history,and the description of the present conditions as well as physical examinations and impression about the conditions.FormatIt usually consists of chief complaint, history of present illness, past medical history, review of systems, physical examination, impression, family history, social history, medications, allergies, laboratory on admission, and plan. However, what parts are included depends on the needs.住院病人病历完整模式病历(Case History)(Name) 职业(Occupation)性别(Sex) 住址(Address)年龄(Age or DOB) 供史者(Supplier of history)婚姻(Marital status) 入院日期(Date of admission)籍贯(Place of birth) 记录日期(Date of record)民族(Race)主述(C.C.)现病史(HPI or P.I.)过去史(PMH or P.H.)社会活动史/个人史(SHx or Per.H.)家族史(FHx or F.H.)曾用药物(Meds)过敏史(All)To be continued系统回顾(ROS)体格检查(PE or P.E.)体温(T) 呼吸(R)血压(BP) 脉搏(P)一般状况(General status)皮肤黏膜(Skin & mucosa)头眼耳鼻喉(HEENT)颈部(Neck)胸部与心肺(Chest, Heart and Lungs)腹部(Abdomen)肛门直肠(Anus & rectum)外生殖器(External genitalia)四肢脊柱(Extremities & spine)神经反射(Nerve reflex)To be continued化验室资料(Lab data)(Blood test, Chem-7, EKG, EEG, X-ray examinations or X-ray slides, CT and NMR…)印象与诊断(Impression and diagnosis, or Imp)住院治疗情况记录(Hospital course)出院医嘱(Discharge instructions or recommendations)出院后用药(Discharge medications)医师签名(Signature)⏹Patterns and contents of an out-patient case historyContents: general data (GD), chief complaint (CC), present illness (PI), physical examination (PE), tentative diagnosis (TD) or impression (Imp), treatment (Rp), etc.An out-patient case history should be written in brief and to the very point. More abbreviations and noun phrases are used.⏹Sample of an out-patient case historyMale, 39 year oldCC: Fever, headache and cough for two days.PE: G.C. looks fair. Pharynx congested and tonsils enlarged. Chest and abdomen negative. Imp: U.R.I.Rp: Penicillin 400,000u. (i.m.) q.d. x 3 days.Aspirin 1 tab. t.i.d. x 2 days.Vit C 100 mg t.i.d. x 3 daysSignature ______⏹Chief Complaint (C.C.)⏹ 1. Sentence patterns in chief complaint•症状+for+时间•症状+of+时间+duration•症状+时间+in duration•时间+of+症状•症状+since+时间⏹Chief Complaint (C.C.)⏹ 2. Commonly-used complaints:•weakness, malaise, chills, fever, pain, headache, nausea and vomiting, diarrhea, neuro-psychiatric disorders, shortness of breath, bleeding or discharge,insomnia, stomachache, dyspepsia, no appetite, dysuria, cough, difficulty incoughing up sputum, sore throat, dizziness, palpitation, restlessness, etc.•弱点,不适感,发冷、发烧、疼痛、头痛、恶心、呕吐、腹泻、neuro-psychiatric紊乱、气短、出血或排放、失眠、胃痛,消化不良,没有胃口,排尿困难、咳嗽、咳痰、困难、喉咙痛、头晕、心悸、不安等。
病例报告英语作文Patient Case Report。
Introduction:The patient is a 45-year-old male who presented to the emergency room with complaints of chest pain and shortness of breath. The patient has a history of hypertension and hyperlipidemia. He also has a family history of heart disease.Medical History:The patient has been previously diagnosed with hypertension and hyperlipidemia for the past 5 years. He has been taking medications for both conditions as prescribed by his primary care physician. The patient has also been advised to follow a healthy diet and exercise regularly.Physical Examination:On physical examination, the patient was found to havea blood pressure of 160/100 mmHg, a heart rate of 100 beats per minute, and an oxygen saturation of 95% on room air.The patient appeared to be in distress and was sweating profusely. The chest examination revealed bilateralcrackles on auscultation.Diagnostic Tests:The patient was immediately taken for an electrocardiogram (ECG), which revealed ST-segmentelevation in leads V1-V4. The patient was then taken for a cardiac catheterization, which revealed a 90% stenosis inthe left anterior descending artery. The patient was diagnosed with acute myocardial infarction.Treatment:The patient was immediately started on aspirin, heparin, and nitroglycerin. The patient was also taken forpercutaneous coronary intervention (PCI), during which a stent was placed in the left anterior descending artery.The patient was then transferred to the cardiac care unitfor further management.Follow-up:The patient was monitored closely in the cardiac care unit for 48 hours. The patient's condition improved gradually, and he was discharged on the fourth day afterthe acute myocardial infarction. The patient was advised to follow up with his primary care physician regularly and to adhere to a healthy lifestyle.Conclusion:In conclusion, this case highlights the importance of timely diagnosis and management of acute myocardial infarction. The patient's history of hypertension and hyperlipidemia, as well as his family history of heart disease, put him at a higher risk for cardiovascular events. The prompt administration of aspirin, heparin, andnitroglycerin, as well as the timely PCI, helped in the successful management of this patient's acute myocardial infarction. The patient was advised to follow a healthy lifestyle and to adhere to his medications to prevent future cardiovascular events.。
第1篇Good morning/afternoon. It is my great honor to stand before you today to deliver a report on a patient with an unknown condition, commonly referred to as "None." This case presents a unique challenge in medical diagnosis and treatment, as we often find ourselves at the crossroads of uncertainty and hope.Introduction:The patient, a 45-year-old male, presented to our hospital with a chief complaint of persistent abdominal pain and a gradual loss of appetite over the past three months. The patient has a medical history of hypertension and type 2 diabetes mellitus, both well-controlled with medication. He has no history of gastrointestinal diseases, travel to endemic areas, or exposure to infectious diseases.Physical Examination:On initial examination, the patient appeared pale and weak. His blood pressure was 120/80 mmHg, heart rate was 85 bpm, and respiratory rate was 16 bpm. Abdominal examination revealed tenderness in the upper quadrant, with no palpable masses or organomegaly. Laboratory tests showed a normal complete blood count, liver function tests, and renal function tests. However, the patient's serum albumin level was slightly decreased (3.2 g/dL), and his C-reactive protein level was elevated (5.6 mg/L).Diagnostic Process:Given the patient's symptoms and initial laboratory results, we conducted a series of investigations to rule out common causes of abdominal pain. This included abdominal ultrasound, CT scan, endoscopy, and biopsies of the liver and spleen. However, these tests yielded no definitive findings. The patient's condition remained enigmatic, leaving us in a state of uncertainty.Management:In the absence of a clear diagnosis, we adopted a conservative approach to manage the patient's symptoms. We started him on a proton pumpinhibitor to reduce stomach acid production and alleviate abdominal pain. Additionally, we adjusted his diabetes medication to maintain blood glucose levels within the target range. The patient's condition improved slightly, with a decrease in abdominal pain and an increase in appetite.Future Directions:As we continue to investigate the patient's condition, we areconsidering the following strategies:1. Repeating investigations: We plan to repeat abdominal imaging and biopsies to rule out any new findings or changes in the patient's condition.2. Referral to a specialist: Given the complexity of the case, we will consult with a gastroenterologist and a hematologist to gain insights from their expertise.3. Long-term follow-up: We will closely monitor the patient's symptoms and laboratory results to detect any potential progression or recurrence of the condition.Conclusion:The case of "None" presents a challenging scenario in medical practice, where we are faced with a patient whose condition remains enigmatic. Despite the uncertainty, we remain committed to providing the best possible care and support to our patients. Our ongoing investigation and management of this case serve as a reminder of the importance of perseverance and collaboration in the face of unknown challenges.Thank you for your attention.第2篇Good [morning/afternoon/evening]. It is my pleasure to present to you a case report on a patient with a diagnosis of None. While the term "None" might seem vague or indicative of an incomplete medical record, it isimportant to approach such cases with a thorough and analytical mindset. Today, I will discuss the patient's history, clinical presentation, diagnostic considerations, and treatment plan.---Introduction:The patient in question is a [age]-year-old [gender] presenting with [briefly describe the presenting complaint or symptoms]. The term "None" in the medical record suggests that there was no specific diagnosis made at the time of initial presentation or during the course of thepatient's care. This can occur for various reasons, including miscommunication, incomplete information, or the complexity of the case itself.---Patient History:The patient's history is significant for [list any relevant medical history, such as chronic conditions, medications, allergies, etc.]. The patient reports that [describe any specific symptoms or changes in health]. The patient also mentions [any notable past medical or surgical history].---Clinical Presentation:Upon physical examination, the patient exhibited [describe the physical findings, such as vital signs, dermatological changes, organomegaly, etc.]. The patient's symptoms [describe how they evolved or remained stable over time].---Diagnostic Considerations:Given the patient's presentation, the following diagnostic tests were considered and/or performed:1. Laboratory Tests: [List any laboratory tests conducted, such as blood work, urine analysis, etc.]2. Imaging Studies: [Discuss any imaging studies performed, such as X-rays, CT scans, MRI, etc.]3. Specialty Consultations: [Mention any consultations with other specialists]The results of these tests were [summarize the findings, including any abnormalities or incongruences].---Differential Diagnoses:The differential diagnoses included [list the possible conditions that could explain the patient's symptoms and findings]. These were considered based on the patient's history, physical examination, and initial diagnostic results.---Treatment Plan:Given the lack of a definitive diagnosis, the treatment plan was [describe the initial approach, such as supportive care, symptom management, or further investigations]. The patient was [mention any changes in treatment over time, if applicable].---Outcome:At the time of this report, the patient's condition remains [describe the current status, including any improvements, stabilizations, or worsening]. Further investigations and management are [mention any ongoing or planned steps].---Conclusion:In conclusion, the case of the patient with a diagnosis of None presents a challenge to the healthcare provider. It is crucial to maintain a comprehensive approach, including thorough history-taking, meticulous physical examination, and judicious use of diagnostic tests. While the lack of a specific diagnosis can be frustrating, it also serves as a reminder to consider all possibilities and to remain vigilant for any new or evolving symptoms.Thank you for your attention.---Please note that this is a general template and should be adapted to fit the specific details of the patient's case.。
英语病例报告作文Title: A Case Report: Management of Infectious Mononucleosis in a Young Adult。
Abstract:Infectious mononucleosis (IM), caused by the Epstein-Barr virus (EBV), is a common viral illness characterized by fever, pharyngitis, lymphadenopathy, and fatigue. This case report discusses the presentation, diagnosis, and management of IM in a 22-year-old female.Case Presentation:A 22-year-old female presented to the outpatient clinic with complaints of fever, sore throat, and fatigue for the past week. She reported a recent history of close contact with a friend who had been diagnosed with IM. On examination, she had cervical lymphadenopathy and pharyngeal erythema with exudates. The monospot test waspositive, confirming the diagnosis of IM.Management:The patient was counseled on the nature of IM and advised to rest, maintain hydration, and avoid contact sports due to the risk of splenic rupture. Symptomatic management with acetaminophen for fever and analgesia was recommended. Corticosteroids were not initiated due to the absence of severe complications such as airway obstruction or hemolytic anemia. The patient was educated on the importance of good hand hygiene to prevent transmission of the virus to others.Follow-up:The patient was followed up in the clinic after two weeks. By this time, her fever had resolved, and she reported improvement in sore throat and fatigue. Repeat monospot test was negative, indicating resolution of acute EBV infection. She was advised to gradually resume normal activities but to avoid strenuous exercise for another fewweeks to prevent relapse.Discussion:IM typically presents with a triad of fever, pharyngitis, and lymphadenopathy, often accompanied by fatigue. Diagnosis is confirmed by a positive monospot test or Epstein-Barr virus-specific serology. Management is largely supportive, focusing on symptom relief and prevention of complications. While corticosteroids may be considered in severe cases, they are not routinely recommended due to potential adverse effects and lack of conclusive evidence of benefit. Patients should be educated about the self-limiting nature of the disease and the importance of rest and hydration. Close follow-up is essential to monitor for complications and ensureresolution of symptoms.Conclusion:Infectious mononucleosis is a common viral illness that predominantly affects young adults. Prompt recognition andappropriate management are essential to alleviate symptoms and prevent complications. Clinicians should be familiar with the typical presentation of IM and be prepared to provide supportive care while ensuring patient education and follow-up.。
精神病患者病历范文英文回答:As a mental health professional, I have encountered numerous cases of patients with psychiatric disorders. One particular case that comes to mind is that of a 35-year-old male diagnosed with schizophrenia. This patient, whom Iwill refer to as John, presented with symptoms such as hallucinations, delusions, disorganized speech, and social withdrawal.John's medical history revealed that he had been experiencing these symptoms for the past five years. His family reported that he had become increasingly isolated and paranoid, often claiming that he was being followed or that his thoughts were being controlled by external forces. These delusions severely affected his ability to functionin daily life and maintain relationships.During our initial assessment, John appeared agitatedand distrustful. He exhibited disorganized speech, jumping from one topic to another without any logical connection. He also displayed inappropriate emotional responses, laughing or crying without any apparent reason. These symptoms indicated a severe disruption in his thought processes and emotional regulation.After a thorough evaluation, John was diagnosed with paranoid schizophrenia. Treatment was initiated with a combination of antipsychotic medication and psychotherapy. The medication helped to alleviate his hallucinations and delusions, while psychotherapy focused on improving his coping skills and social functioning.Over time, John's symptoms gradually improved. He became more engaged in therapy sessions and started to develop a support network through group therapy. With continued treatment and support, he was able to regain some level of normalcy in his life. However, it is important to note that schizophrenia is a chronic condition, and ongoing treatment is necessary to manage symptoms and prevent relapse.中文回答:作为一名心理健康专业人士,我遇到过许多患有精神疾病的患者。
June 5, 2010
Our local doctor in SH led patient to Shanghai Mental Health Center at 2 PM this afternoon then visited psychiatrian there. Following is updated information for the patient. The insured came to Shanghai in Dec of 2009 to study Chinese. In January 2010 the Chinese course finished then he started to live in an apartment alone. He admitted since April of 2010 visual/audio hallucination started. On May 9 he visited psychiatrian in UFH of Shanghai then Olanzapine was administered in out-patient department, until he was admitted there on May 29 for operation of Tibia/fibula fracture. Upon discharge of UFH SH, anti-schizophrenia agent Abilify 5 mg Bid and Clonazapam 2mg QN were ever prescript. Upon enquiry by the psychiatrian in SH Mental Health Center this afternoon, the insured showed state of alert, easy contact. He still complained instructive audio-hallucination and persecutive feeling (delusion). He felt somtimes his thought was fully perspected by others. However, no tendency of violent assaulting or obvious depression were noted. He had no recognization of his condition being sicked.
Diagnosis: schizophrenia
Treatment/advice: 1. Olanzapine 5 mg Bid.
2. He should follow up in out-patient department 1
week later to regulate(add?) dose of Olanzapine.
3. His current condition permits travel now, but
under medical escort.
4. He should be monitored by relation or caregiver
for regular use of medication after back to UK. In
this case, there is no need to be admitted into
hospital for therapy. If there is none to look after
him for medication taking, admission of hospital is
advised after he is back to UK.
After the visit of psychiatrian finished this afternoon, the insured was sent to Changning District Central Hospital for cardiologist visit.
There was no discomfort complaint of chest depress or shortness of breath. His vital signs as BP, T, RR, HR and oxygen saturation were in normal range. Heart and lungs (-).
ECG of this afternoon: normal.
Labs done this afternoon
Blood routine: WBC 10800(normal < 10000), with LYM 41%.
CK, CK-MB, Tryponin etc were in normal range.
Coagulation function tests were basically in normal range.
Blood platelet cell: 380000(100000-300000)
D-dimmer result was normal.
The cardiologist thought his heart condition was stable now, no impression of cardiac ischemia. Then he was prescript Cefuroxime tabs and L-Glutamine, Sodium Gualenate Granules. The cardiologist thought his heart condition would not disturb his travel.
The current medications he is taking now:
1. Oxycodone/Paracetamol tabs (painkiller)
2. Cefuroxime tabs
3. L-Glutamine, Sodium Gualenate Granules
4. Aripiprozole tabs
Hope above information will be helpful to you.。