冠状动脉的解剖与冠脉造影
- 格式:ppt
- 大小:8.70 MB
- 文档页数:60

龙源期刊网
冠状动脉CTA与冠脉造影比较
作者:王金会 秦小娜 王晓艳
来源:《中西医结合心血管病电子杂志》2015年第14期
【摘要】目的 分析冠状动脉CT血管造影(CTA)与冠脉造影(CAG)的差异,探讨冠状动脉CTA对冠心病的临床诊断价值。方法 分别对冠状动脉钙化和积分、斑块和狭窄、心肌桥-壁血管显示、支架术前、术后、心脏不良事件等进行评估对比并分析记录。结果 冠状动脉CTA无法看到分支血管及小血管病变,清晰和准确程度不如冠脉造影。结论 冠状动脉CTA易漏诊,受影响产生伪像的几率大,因此冠脉造影值得临床推广与运用。
【关键词】冠状动脉CTA;冠脉造影;对比
【中图分类号】R541.4 【文献标识码】B 【文章编号】ISSN.2095-6681.2015.014.00.03
【Abstract】Objective To analyze the coronary CTA and coronary angiography differences
investigate the clinical diagnostic value of CTA artery for coronary artery disease.Methods In contrast
to respectively coronary artery calcification and integral, plaque and stenosis and display myocardial
bridge and vessel wall and stent with preoperative, postoperative and adverse cardiac events such as
for comparative evaluation and analysis of the recorded. Results Coronary artery CTA can not see the
2015年5月B第3卷第14期 May.2015Vo1.3No.14 中西医结合心血管病杂志 Cardiovascular Disease Journal of integrated traditional Chinese and Western Medicine 9 冠状动脉CTA与冠脉造影比较 王金会,秦小娜,王晓艳 (山东省威海市立医院心内科,山东威海264200) 【摘要】目的 分析冠状动脉CT- ̄-管造影(CTA)与冠脉造影(CAG)的差异,探讨冠状动脉CTA 对冠心病的临床诊断价值。方法分别对冠状动脉钙化和积分、斑块和狭窄、心肌桥一壁血管显示、支架术 前、术后、心脏不良事件等进行评估对比并分析记录。结果 冠状动脉CTA无法看到分支血管及小血管病 变,清晰和准确程度不如冠脉造影。结论冠状动脉CTA易漏诊,受影响产生伪像的几率大,因此冠脉造影 值得临床推广与运用。 【关键词】冠状动脉CTA;冠脉造影;对比 【中图分类号】R541.4 【文献标识码】B 【文章编号】ISSN.2095-6681.2015.014.009.03 Comparison between CTA and coronary angiography in coronary artery WANG Jin-hui,QIN Xiao-na,WANG Xiao-yan (Department of Cardiology,Shandong Province Weihai Municipal Hospital,Shandong Weihai 264200,China) 【Abstract]0bjective To analyze the coronary CTA and coronary angiography differences investigate the clinical diagnostic value of CTA artery for coronary artery disease.Methods In contrast to respectively coronary artery calcification and integral,plaque and stenosis and display myocardial bridge and vessel wall and stent with preoperative,postoperative and adverse cardiac events such as for comparative evaluation and analysis of the recorded. Results Coronary artery CTA Can not see the branch of the blood vessel and small vessel disease,clear and accurate degree is inferior to the coronary angiography.Conclusion Coronary artery CTA is likely to be misdiagnosed, artifactsofhighprobability,SO coronaryangiographyworthmoreforawide range ofclinicalappficafion. [Key words]Coronary CTA;Coronary angiography;Contrast 对比冠状动脉CTA ̄IJCAG之间的差异,分析冠 状动脉CTA对于冠心病诊断的敏感性和特异性。具体 如下。 1 冠状动脉钙化和积分的评估 CAG对钙化的敏感性不及冠状动脉cTA敏 感,CT钙化斑块的敏感性为89% ̄95%,特异性为 94%~96%,纤维斑块82% ̄92%,特异性87%,易 损斑块的主要特征:低密度、偏心或溃疡形成,斑 块部位血管正性重构。冠状动脉CTA检查可以确定 斑块性质。血栓的CT值约20 Hu,脂质斑块CT值约 50 Hu,纤维斑块CT值约70~120 Hu。钙化斑块CT值 为130 Hu以上。脂质斑块为不稳定斑块,临床需高度 重视及监测,有临床资料提示对于不稳定斑块应当尽 快实施介入治疗,以防止破裂形成血栓。依据CTA值 对非钙化进一步分类存在不足,世界范围内的大多数 多排螺旋(MD)CT有关于冠脉成像的研究都提示钙 化是影响结果判断的主要因素[1]。Rubinshtein等通过研 究发现,lO0 ̄J患者中有29例存在钙化,导致无法对冠 脉成像情况进行评价;同时,Cademartiri等学者通过 16.MDCT对冠心病患者进行CTA与CAG的研究,100例 患者的冠状动脉平均钙化积分为(294±604)分, 高钙化积分组平均值为(575±758)分,而其中低钙 化积分组的平均值为(12±15)分,差异有统计学意 义(P<0.05),进一步研究发现,低钙化积分组患者 应用CTA得到的冠脉狭窄段识别的敏感性为89.7%、 特异性为97.6%、阳性预测结果为83.5%、阴性预测 值则为98.6%;高钙化积分组患者的结果则为93.3%、 92.8%、75.4%以及98_3%。结果表明,尽管患者的钙 化积分非常高,MDCT分析结果也不会对整体诊断精 度造成过大的影响[2】。 2斑块和狭窄的评估 目前评价冠状动脉内斑块最准确的方法是血管内 超声pJ,但须经皮冠脉介入手术完成,其有创且价格 昂贵限制了推广。随着CT在时间、空间分辨率的不 断提高,冠状动脉CTA作为一种有效的无创检查日益

冠状动脉CTA与冠脉造影比较
目的 分析冠状动脉CT血管造影(CTA)与冠脉造影(CAG)的差异,探讨冠状动脉CTA对冠心病的临床诊断价值。方法 分别对冠状动脉钙化和积分、斑块和狭窄、心肌桥-壁血管显示、支架术前、术后、心脏不良事件等进行评估对比并分析记录。结果 冠状动脉CTA无法看到分支血管及小血管病变,清晰和准确程度不如冠脉造影。结论 冠状动脉CTA易漏诊,受影响产生伪像的几率大,因此冠脉造影值得临床推广与运用。
标签:冠状动脉CTA;冠脉造影;对比
【Abstract】Objective To analyze the coronary CTA and coronary angiography
differences investigate the clinical diagnostic value of CTA artery for coronary artery
disease.Methods In contrast to respectively coronary artery calcification and integral,
plaque and stenosis and display myocardial bridge and vessel wall and stent with
preoperative, postoperative and adverse cardiac events such as for comparative
evaluation and analysis of the recorded. Results Coronary artery CTA can not see the
branch of the blood vessel and small vessel disease, clear and accurate degree is
inferior to the coronary angiography. Conclusion Coronary artery CTA is likely to be
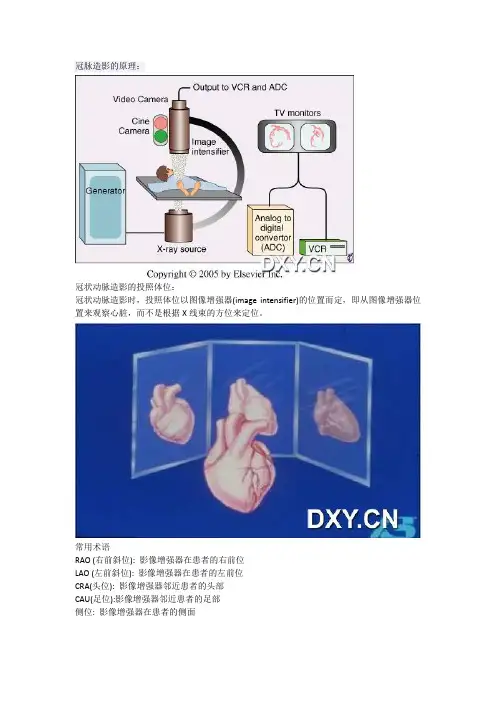
冠脉造影的原理:
冠状动脉造影的投照体位:
冠状动脉造影时,投照体位以图像增强器(image intensifier)的位置而定,即从图像增强器位
置来观察心脏,而不是根据X线束的方位来定位。
常用术语
RAO (右前斜位): 影像增强器在患者的右前位
LAO (左前斜位): 影像增强器在患者的左前位
CRA(头位): 影像增强器邻近患者的头部
CAU(足位):影像增强器邻近患者的足部
侧位: 影像增强器在患者的侧面
体位示意图:
冠状动脉投照体位及X线解剖:
左前斜位60°时,投照从心尖穿过,为心脏的正面观
右前斜30°时,投照垂直通过心脏的长轴,为心脏的侧面观
由于冠状动脉造影是一个二维平面图像,同一病变在两个互相垂直的投射体位才能充分地显
示清楚。冠状动脉造影的目标就是利用两个相互垂直、图像清楚的投照体位对病变行准确评
价。基于此病变的处理才能有的放矢,并可及时观察手术并发症。
左冠状动脉造影体位一览图
右冠状动脉造影体位一览图
正常冠状动脉的x线解剖示意图
不同体位下的冠状动脉造影示意图
冠状动脉造影详述
右冠脉造影比较简单,那就先说一下右冠造影。
右冠状动脉常用投照体位:
常用体位
LAO:观察RCA开口、起始部至后降支
RAO:观察RCA中段
AP+CRA :观察RCA远端分支及其开口情况
右冠状动脉常用投照体位
左前斜(LAO) 45°
右冠状动脉呈“C”型,观察RCA开口、起始部至后降支;
The left anterior oblique view (LAO straight) shows the proximal and midportions of the right
coronary artery (RCA) as well as the acute marginal branches (AM) and termination of the RCA in
the posterior left ventricular branches (PLV).