ACCFACGAHA专家共识更新
- 格式:doc
- 大小:25.00 KB
- 文档页数:3

ACCF/ACG/AHA专家共识更新作者:河北省人民医院郭艺芳整理来源:中国医学论坛报为减少抗血小板药物对胃肠道的不良影响,美国心脏病学会基金会(ACCF)、美国胃肠病学会(ACG)及美国心脏学会(AHA)于2008年联合发表专家共识,建议接受抗血小板或(和)非类固醇类抗炎药(NSAID)治疗的患者积极应用质子泵抑制剂(PPI)。
然而2009年初所公布的一项大型病例对照研究却显示,联合应用氯吡格雷与PPI可能会增加心血管不良事件的发生。
此研究一度引起广泛关注,但随后陆续发表的一系列研究所得的结论却存在分歧,令临床医师无所适从。
2010年11月8日,ACCF/ACG/AHA对相关文献进行总结与分析后,更新了2008年版的专家共识。
虽然关于PPI是否会影响氯吡格雷的抗血小板作用尚无最终定论,但更新的指南仍根据现有证据为临床医师的临床实践提供了建议,这无疑是一个进步。
新版《共识》要点对于降低抗血小板治疗和应用NSAID的胃肠道风险,更新的《ACCF/ACG/AHA降低抗血小板治疗和应用NSAID的胃肠道风险专家共识》(简称《共识》)主要有以下11点要点。
1. 氯吡格雷是预防动脉粥样硬化性心血管病患者血栓事件的有效药物。
2. 与单独使用阿司匹林相比,联合应用氯吡格雷与阿司匹林可进一步降低冠心病患者以及支架置入术后患者的血栓形成事件风险。
3. 氯吡格雷与阿司匹林单独或联合应用可增加胃肠道出血风险。
4. 胃肠道出血的高危人群包括:曾有胃肠道出血史,高龄,同时接受抗凝剂、类固醇类抗炎药或NSAID(包括阿司匹林)治疗,以及幽门螺杆菌感染者。
存在上述多种危险因素者的胃肠道出血危险可进一步增高。
5. 与单用抗血小板药物相比,加用PPI或组胺2(H2)受体拮抗剂可降低上消化道出血危险,而PPI的疗效优于H2受体拮抗剂。
6. 对于需要接受抗血小板治疗的患者,建议对曾有胃肠道出血史者预防性应用PPI,对于存在多种其他出血高危因素者,也可考虑应用PPI预防胃肠道出血。
是胃食管反流病不是“冠心病”发表时间:2008-11-20发表者:申海涛(访问人次:913)一般资料:石X X,男,53岁,某旅游巴士有限公司员工。
因“胸背痛、胸闷、憋气8年,加重7个月”于2008-01-09入我院。
患者在8年前无明显诱因出现胸背痛。
发作时胸痛主要表现为胸骨后明显,为闷痛。
向后背部放散,伴有胸闷、出汗、休息及活动后均可以发作。
每次发作持续数十分钟至数小时。
含服硝酸甘油效果不理想。
无反酸、无反胃,无明显烧心症状。
因胸背痛发作多次就诊于北大医院急诊科,心电图无明显动态改变,心肌酶谱及胸片均无异常,服用异舒吉(异舒吉作用与硝酸甘油相似,但较持久,能维持4小时以上),症状可以稍缓解,但是仍旧反复发作。
于2007年5月因再次发作就诊于解放军第305医院,诊断“冠心病”。
并行冠脉造影结果显示前降支30-40%狭窄,回旋支30-40%狭窄,右冠95%狭窄。
遂行右冠脉植入支架1枚。
术后坚持服用阿斯匹林、波立维、消心痛。
但是症状较前无明显改善,仍反复发作胸痛、胸憋。
患者平素有腹胀、偶有嗳气、咽部不适感。
为进一步诊治。
遂在305医院行食管压力测定结果LESP正常,食管体部静息压正常,LES功能完整。
食管24小时测酸结果为轻度酸反流,DeMeester评分40.35。
胃镜结果为慢性浅表性胃炎。
心脏超声显示左室舒张功能减低。
动态心电图显示1.窦性心率,2.偶发房早。
胸部CT检查:未见明显异常。
遂给予雷贝拉唑、硫糖铝、加斯清等药后胸骨后疼痛、胸憋症状有缓解。
为进一步诊治。
到我院就诊。
以“胃食管反流病”收入我院。
患者既往高血压病史7年,最高达180/110mmHg,近年规律服用“比索洛尔、洛活喜”。
发现空腹血糖异常8个月,最高达8.2mmol/L,未明确诊断糖尿病。
入院后按胃食管反流病给予药物诊断性试验治疗一周(埃索美拉唑20mg 2/日口服、铝碳酸镁片1g 3/日,多潘立酮片 10mg 3/日口服)。
胸背痛有明显缓解,原来一直存在的咽部不适症状改善最明显。

应用NSAID胃肠道风险及降低抗血小板治疗的专家共识2011-1越来越多的证据证实抗血小板药物在预防动脉粥样硬化血栓事件中的获益,抗血小板药物的应用不断增加。
然而应用抗血小板药物确实存在风险,尤其是胃肠道并发症,例如消化性溃疡及与之相关的消化道出血。
这些风险在抗血小板药物联合应用,及与其他的药物如非甾体类抗炎药(NSAID)、糖皮质激素及抗凝药合用时会进一步增加。
基于临床上抗血小板治疗的广泛性,医生有必要了解抗血小板治疗在预防心脑血管事件发生中的获益以及相关的风险。
只有了解了这些,临床医生才能合理充分的评估每个患者的风险与获益,给予最佳的治疗方案。
2008年发布的美国心脏病学院基金会/美国胃肠病学会/美国心脏协会(ACCF/ACG/AHA)降低抗血小板治疗及应用NSAID胃肠道风险的专家共识对于抗血小板药物应用给出了与以往不同的建议。
(CircuLation,2008,118:1894—190%)1阿司匹林和其他NSAID的胃肠道并发症建议:当服用任何NSAID时,包括COX-2选择性药物和非处方剂量的传统NSAID以及心脏病治疗剂量的阿司匹林,都会增加溃疡并发症的风险,对于具有溃疡风险的患者应同时处方胃肠道保护药物。
上消化道事件包括有症状的以及并发的溃疡,在NSAID服用者中每20例有1例发生,每7例老年人有1例发生,占上消化道事件相关的住院和死亡的30%消化不良定义为上腹痛或上腹部不适,可发生于服用NSAID包括阿司匹林的患者。
消化不良不能准确的提示溃疡的存在,因为它的发生太常见了。
NSAID还会加重一些胃食管反流病患者的症状。
每年NSAID相关的上消化道事件的发生率为2.O%,4.5%,出血、穿孔、梗阻的风险为0.2,1.9%。
每年因NSAID导致的住院为10,20/1000,死亡率增加4倍。
仅在美国,关节炎患者中每年因服用NSAID导致10700次住院和16500例死亡。
联合应用阿司匹林和其他NSAID的人群是另一组高危人群。

2021版:ACC 优化心衰治疗的决策路径专家共识更新版(最全版)1 引言心衰的患病率正迅速升高(5)。
除此之外,心衰是一种消耗大量医疗资源的疾病,造成相当大的发病率和死亡率,并严重影响患者的生活质量。
重要的突破包括广泛的药物治疗、设备和管理策略,重新定义了改变疾病自然史的机会。
本次ECDP重点更新,目的是用新兴研究的数据补充2017年的ECDP,并继续为HFrEF患者的管理提供简洁实用的指导。
保留了2017 ECDP中10个关键问题的格式,并更新了其相关的治疗方案和表格以适应这一不断发展的新证据。
HFrEF中的十个关键问题1.如何开始、添加或转换为新的循证指南导向的HFrEF治疗;2.如何实现心衰患者的最佳治疗,包括使用改变指南推荐方案的多种药物及强化临床评估(例如,影像学数据、生物标志物和充盈压);3.何时将患者转诊至心衰专家;4.如何应对管理协调方面的挑战;5.如何提高用药依从性;6.特定的患者队列(非裔美国人、老年人和体弱者)的需求;7.如何管理患者的费用和改善心衰药物的可及性;8.如何管理日益复杂的心衰;9.如何管理常见共病;10.如何整合姑息治疗和过渡至临终关怀。
2 方法最初的2017年ACC ECDP采用结构化格式起草,该格式是2016年和2017年ACC/AHA/心衰SA对2013年ACCF/AHA 心衰指南重点更新发布之后创建的(2,4,6)。
ECDP的演进涉及提出问题,以发现证据差距,并召集一个多学科的参与方小组,他们对文献进行综述以汇总涉及当代心衰治疗的相关证据。
当时,ECDP主席和副主席分别对参考文献进行了审查,并制定了议定的纲要。
在2016年7月19日于ACC心脏之家举行的现场圆桌会议之前,已向小组的每个成员提供了参考文献的印刷本。
心衰圆桌会议的参与者包括心脏病专家、内科医师、急诊医师、住院医师、护士、患者权益团体代表、药剂师、培训研究员、质量改进专家、流行病学家和生物统计学家。
#述评#氯吡格雷与质子泵抑制剂朱国英*关键词氯吡格雷;质子泵抑制剂;胃肠道出血今年初陆续发表于5加拿大医学会杂志6和5美国医学会杂志6的两项大规模回顾性研究显示,氯吡格雷与质子泵抑制剂(PPI)联用增加心血管事件发生风险。
/一石激起千层浪0,引起了心血管医生和消化科医生的极大关注,围绕抗血小板治疗引发了更多的思考,也还有待问题的澄清。
1抗血小板治疗与消化道出血越来越多的证据证实抗血小板治疗在预防动脉粥样硬化血栓事件中获益,使抗血小板药物的应用不断增加。
2007年和2008年欧洲心脏病学会(ESC)和美国心脏病学会/美国心脏协会(ACC/AHA)发布的/非ST段抬高急性冠状动脉(冠脉)综合征(NSTE-ACS)0和/ST段抬高急性冠脉综合征(STE-ACS)0以及/冠脉介入治疗(PC I)0指南中都强调了抗血小板治疗的重要性,推荐:/所有患者0、/尽早应用0、/双联药物(阿司匹林+氯吡格雷)0、/氯吡格雷负荷量+维持量0和/长期应用0等抗血小板治疗建议。
全球有近10万名ACS患者参与了氯吡格雷的各种大型随机化、双盲对照研究,充分验证了氯吡格雷的疗效和安全性。
在阿司匹林基础上加用氯吡格雷的双联抗血小板治疗得到了包括ESC,ACC/AHA和美国胸科医师学会(ACCP)在内的众多国际权威指南推荐。
然而,随着抗血小板治疗的人群基数加大、从一级预防到二级预防以及用药时间之长(通常为数十年),在减少心血管事件的同时却增加了胃肠道并发症包括消化性溃疡及与之相关的消化道大出血发生率(0119j~ 116j),这些风险在抗血小板药物的联合用药以及与其他药物如非甾体类抗炎药(NSA I D)、糖皮质激素及抗凝药物合用时会进一步增加。
因此,抗血小板治疗出血风险不容忽视,医生必须合理评估每个患者的风险与获益,给予最佳的治疗方案。
为此,2008年10月由美国心脏病学会基金会/美国胃肠病学会/美国心脏协会(ACCF/ ACG/AHA)共同发布的/降低抗血小板治疗及应用NSA I D的胃肠道风险的临床专家共识0,对于抗血小板药物应用建议如下:由于NSA I D与抗血小板制剂(如阿司匹林)可以增加患者溃疡性胃肠道合并症的危险,故对于胃肠道出血高危患者应给予必要的胃肠道保护性治疗。
解读美国心脏病学院和美国心脏协会最新心力衰竭治疗指南美国心脏病学院基金会(ACCF)和美国心脏协会(AHA)新近联合发表了心力衰竭(简称心衰)患者治疗临床实用指南[1]。
为了帮助临床医师选择具体患者的最佳治疗策略,新指南对心衰的定义和分类进行了修订,重点强调以患者为中心的结果,例如生活质量、参与决策、护理协调、过渡和姑息治疗。
一、新版指南的主要内容1.心衰的分类与定义分为2类4期。
第1类:左室射血分数(LVEF)减低(≤40%)的心衰(HFrEF),也称为收缩期心衰。
第2类:LVEF保留(≥50%)的心衰(HFpEF),也称为舒张期心衰,又分为LVEF临界(41-49%)和LVEF 改善(>40%)两种。
A期:心衰高危但无结构性心脏病或心衰症状。
B 期:有结构性心脏病但无心衰体征或症状。
C期:有结构性心脏病且(曾)有心衰症状。
D期:顽固性心衰且需要特殊干预。
ACC和AHA的这种分期强调疾病的发生与进展,用于描述具体的患者和人群。
纽约心脏协会(NYHA)的分级则强调运动能力和疾病的症状状态。
2.心衰(包括HFpEF)患者的初次和多次评估病史和物理检查应认真询问病史并进行全面的物理检查,寻找导致心衰发生或加速进展的心性和非心性疾患或行为。
在特发性扩张型心肌病(DCM)患者,询问3代家族史,帮助诊断家族性DCM。
在患者每次就诊时评估其容量状态和生命体征,包括多次评估体重、颈静脉压和有否外周水肿或端坐呼吸。
风险评分多变量风险评分可评估门诊或住院患者发生死亡的风险。
应用风险评分预测慢性患者结果的模型包括西雅图心衰模型、心衰存活评分、CHARM风险评分和CORONA风险评分。
I-PRESERVE评分尤其适合于慢性HFpEF。
在急性失代偿性患者,应用ADHERE分类回归树状模型、AHA随指南而行评分、EFFECT风险评分、ESCAPE风险模型和出院评分、以及优化心衰风险预测列线图。
诊断性检查初次化验检查包括全血细胞计数、尿液分析、血清电解质(包括钙与镁)、血尿素氮、血清肌酐、血糖、空腹血脂、肝功能和甲状腺刺激素。
质子泵抑制剂的合理使用目前质子泵抑制剂包括奥美拉唑、兰索拉唑、泮托拉唑、雷贝拉唑、埃索美拉唑等药物。
这些药物可使正常人及溃疡患者的基础胃酸分泌及由组胺、胃泌素等刺激引起的胃酸分泌明显受到抑制;还可对胃黏膜有保护作用,尤其对阿司匹林、乙醇、应激所致的胃黏膜损伤有保护作用;也可增强抗菌药如阿莫西林、克拉霉素、甲硝唑、四环素、呋喃唑酮等对幽门螺杆菌的根除率(可能与通过抑制细菌ATP酶活性而抑制细菌生长有关),故常用于十二指肠溃疡、胃溃疡、反流性食管炎和卓-艾综合征(胃泌素瘤)等病,是治疗消化性溃疡病的良药。
质子泵抑制剂对十二指肠溃疡、胃溃疡的剂量为每日20 mg,每日1~2次。
对十二指肠溃疡2~4周为一疗程;胃溃疡愈合一般为4~6周,病情严重时,4~8周为一疗程,即可有效缓解溃疡症状,亦可促进溃疡愈合,但多和抗菌药联合应用,使用抗菌药根除幽门螺杆菌也是治疗该病或防止复发的关键措施。
尽管溃疡病属慢性病,但一般经过4~8周的持续治疗后,大多数溃疡可愈合,病情痊愈,因此该药的疗程应尽可能控制在8周之内。
为了防止消化道溃疡病的复发,此后医生还会要求患者继续服用小剂量抗溃疡药,以巩固疗效。
对此,应小剂量服用H2受体阻断剂,该类药物不良反应小;还可选用增强胃黏膜屏障作用的药物,如米索前列醇、恩前列素、硫糖铝、麦滋林S、替普瑞酮、蒙脱石等,这些药物有促进黏液和碳酸氢盐分泌;促进胃黏膜受损上皮细胞的重建和增殖,增强细胞屏障;或在溃疡面形成保护屏障;或促进黏膜合成前列腺素,增加血流量,刺激黏膜细胞再生,增强胃黏膜屏障能力;或杀灭幽门螺杆菌等。
应用这类药物可有效降低溃疡病的再复发,但不宜选用抑酸作用强及不良反应较多的质子泵抑制剂长期治疗和预防消化道溃疡。
质子泵抑制剂作用强而持久,每日口服奥美拉唑200 mg,连续7天,基础胃酸p H值可从1.4升至5.3;一次服用40 mg,3天后,胃酸分泌部分受到限制。
所以,在质子泵抑制剂应用期间不宜长期或大剂量与抗酸药及胃酸抑制剂联用,如抗酸药碳酸氢钠片、鼠李铋镁片、三硅酸镁、铝碳酸镁等;胃酸抑制药如H2受体阻断剂西咪替丁、法莫替丁、雷尼替丁等;胆碱受体阻断剂如阿托品、哌仑西平等,以免胃酸被过度抑制,引起其他疾病。
2011年ACCF/AHA不稳定型心绞痛/非ST段抬高心肌梗死治疗指南(2007年指南的焦点更新)J Am Coll Cardiol, doi:10.1016/j.jacc.2011.02.009 (Published online 28 March 2011)/cgi/content/full/j.jacc.2011.02.009v13. 早期院内治疗3.2 可能或者确定诊断为UA/NSTEMI病人的抗血小板/抗凝治疗的推荐3.2.1 抗血小板治疗的推荐(表2)3.2.3抗血小板和抗凝之外的治疗推荐表3 抗血小板和抗凝之外的治疗推荐3.3.起初保守治疗还是起初侵入性治疗策略(参见表4)表4 最初侵入性治疗策略与保守性治疗策略的推荐5.住院后期护理,出院和出院后护理5.2. 长期的药物治疗和二级预防5.2.1. 抗血小板治疗的推荐(表5)表 5 抗血小板治疗推荐5.2.6. 华法令抗凝治疗的推荐6.5 慢性肾脏疾病(CKD)推荐在使用造影剂之前的至少12小时内进行水化,以达到扩容的目的,并同时抑制肾素系统。
造影剂使用完毕后水化要持续12-20小时(Nephrol Dial Transplant 1999;14:1064-1066.)。
水化的基本原则是单独使用等张或者半浓度的生理盐水(0.45%),这是传统的金标准。
最近,正在试验使用碳酸氢钠作为水化溶液。
一些研究认为在预防造影剂诱发的肾病(CIN)上碳酸氢钠优于生理盐水。
最新的研究显示造影剂体积与肌酐清除率的比值>3.7是血清肌酐浓度异常升高的显著性的、独立的预测因子。
References1 ACCF/AHA Task Force on Practice Guidelines Methodologies and Policies from the ACCF/AHA Task Force on Practice Guidelines /Methodology_Manual_for_ACC_AHA_Writing_Committees.pdf Accessed December 20, 2010.2 Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction) J Am Coll Cardiol 2007;50:e1-e157.[Free Full Text]3 Antiplatelet Trialists' Collaboration Collaborative overview of randomised trials of antiplatelet therapy– I. Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. BMJ 1994;308:81-106.[Abstract/Free Full Text]4 Cairns JA, Gent M, Singer J, et al. Aspirin, sulfinpyrazone, or both in unstable angina. Results of a Canadian multicenter trial. N Engl J Med 1985;313:1369-1375.[Web of Science][Medline]5 Cohen M, Adams PC, Parry G, et al. Combination antithrombotic therapy in unstable rest angina and non-Q-wave infarction in nonprior aspirin users. Primary end points analysis from the ATACS trial Antithrombotic Therapy in Acute Coronary Syndromes Research Group. Circulation 1994;89:81-88.[Abstract/Free Full Text]6 Lewis Jr HD, Davis JW, Archibald DG, et al. Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina. Results of a Veterans Administration Cooperative Study. N Engl J Med 1983;309:396-403.[Web of Science][Medline]7 The RISC Group Risk of myocardial infarction and death during treatment with low dose aspirin and intravenous heparin in men with unstable coronary artery disease Lancet 1990;336:827-830.[CrossRef][Web of Science][Medline]8 Theroux P, Ouimet H, McCans J, et al. Aspirin, heparin, or both to treat acute unstable angina N Engl J Med1988;319:1105-1111.[Web of Science][Medline]9 Baigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials Lancet2009;373:1849-1860.[CrossRef][Web of Science][Medline]10 Ridker PM, Cushman M, Stampfer MJ, et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men N Engl J Med 1997;336:973-979.[CrossRef][Web of Science][Medline]11 CAPRIE Steering Committee A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE) Lancet 1996;348:1329-1339.[CrossRef][Web of Science][Medline]12 Gollapudi RR, Teirstein PS, Stevenson DD, et al. Aspirin sensitivity: implications for patients with coronary artery disease JAMA 2004;292:3017-3023.[Abstract/Free Full Text]13 Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation N Engl J Med 2001;345:494-502.[CrossRef][Web of Science][Medline]14 Abraham NS, Hlatky MA, Antman EM, et al. ACCF/ACG/AHA 2010 expert consensus document on the concomitant use of proton pump inhibitors and thienopyridines: a focused update of the ACCF/ACG/AHA 2008 Expert Consensus Document on Reducing the Gastrointestinal Risks of Antiplatelet Therapy and NSAID Use J Am Coll Cardiol 2010;56:2051-2066.[Free Full Text]15 Steinhubl SR, Berger PB, Mann III JT, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial JAMA 2002;288:2411-2420.[Abstract/Free Full Text]16 Stone GW, Bertrand ME, Moses JW, et al. Routine upstream initiation vs deferred selective use of glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: the ACUITY Timing trial JAMA 2007;297:591-602.[Abstract/Free Full Text]17 Mehta SR, Yusuf S, Peters RJ, et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study Lancet 2001;358:527-533.[CrossRef][Web of Science][Medline]18 Boersma E, Harrington RA, Moliterno DJ, et al. Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes:a meta-analysis of all major randomised clinical trials Lancet 2002;359:189-198.[CrossRef][Web of Science][Medline]19 PRISM-PLUS Study Investigators Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non-Q-wave myocardial infarction. Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. N Engl J Med 1998;338:1488-1497.[CrossRef][Web of Science][Medline]20 PURSUIT Trial Investigators Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. The PURSUIT Trial Investigators. Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy. N Engl J Med 1998;339:436-443.[CrossRef][Web of Science][Medline]21 CAPTURE Study Investigators Randomised placebo-controlled trial of abciximab before and during coronary intervention in refractory unstable angina: the CAPTURE Study Lancet 1997;349:1429-1435.[CrossRef][Web of Science][Medline]22 Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes N Engl J Med 2007;357:2001-2015.[CrossRef][Medline]23 Ottervanger JP, Armstrong P, Barnathan ES, et al. Long-term results after the glycoprotein IIb/IIIa inhibitor abciximab in unstable angina: one-year survival in the GUSTO IV-ACS (Global Use of Strategies To Open Occluded Coronary Arteries IV–Acute Coronary Syndrome) Trial Circulation 2003;107:437-442.[Abstract/Free Full Text]24 Simoons ML. Effect of glycoprotein IIb/IIIa receptor blocker abciximab on outcome in patients with acute coronary syndromes without early coronary revascularisation: the GUSTO IV-ACS randomised trial Lancet2001;357:1915-1924.[CrossRef][Web of Science][Medline]25 Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban N Engl J Med2001;344:1879-1887.[CrossRef][Web of Science][Medline]26 FRagmin and Fast Revascularisation during InStability in Coronary artery disease Investigators Invasive compared with non-invasive treatment in unstable coronary-artery disease: FRISC II prospective randomised multicentre study Lancet 1999;354:708-715.[CrossRef][Web of Science][Medline]27 Kastrati A, Mehilli J, Neumann FJ, et al. Abciximab in patients with acute coronary syndromes undergoing percutaneous coronary intervention after clopidogrel pretreatment: the ISAR-REACT 2 randomized trial JAMA2006;295:1531-1538.[Abstract/Free Full Text]28 Mehta SR, Tanguay JF, Eikelboom JW, et al. Double-dose versus standard-dose clopidogrel and high-dose versus low-dose aspirin in individuals undergoing percutaneous coronary intervention for acute coronary syndromes (CURRENT-OASIS 7): a randomised factorial trial Lancet 2010;376:1233-1243.[CrossRef][Web of Science][Medline]29 Patti G, Colonna G, Pasceri V, et al. Randomized trial of high loading dose of clopidogrel for reduction of periprocedural myocardial infarction in patients undergoing coronary intervention: results from the ARMYDA-2 (Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty) study Circulation 2005;111:2099-2106.[Abstract/Free Full Text]30 Cuisset T, Frere C, Quilici J, et al. Benefit of a 600-mg loading dose of clopidogrel on platelet reactivity and clinical outcomes in patients with non-ST-segment elevation acute coronary syndrome undergoing coronary stenting J Am Coll Cardiol 2006;48:1339-1345.[Abstract/Free Full Text]31 von Beckerath N, Taubert D, Pogatsa-Murray G, et al. Absorption, metabolization, and antiplatelet effects of 300-, 600-, and 900-mg loading doses of clopidogrel: results of the ISAR-CHOICE (Intracoronary Stenting and Antithrombotic Regimen: Choose Between 3 High Oral Doses for Immediate Clopidogrel Effect) Trial Circulation2005;112:2946-2950.[Abstract/Free Full Text]32 Kushner FG, Hand M, Smith Jr SC, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines J Am Coll Cardiol2009;54:2205-2241.[Free Full Text]33 Stone GW, Ware JH, Bertrand ME, et al. Antithrombotic strategies in patients with acute coronary syndromes undergoing early invasive management: one-year results from the ACUITY trial JAMA 2007;298:2497-2506.[Abstract/Free Full Text]34 Stone GW, White HD, Ohman EM, et al. Bivalirudin in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a subgroup analysis from the Acute Catheterization and Urgent Intervention Triage strategy (ACUITY) trial Lancet 2007;369:907-919.[CrossRef][Web of Science][Medline]35 Prasugrel [package insert]. Indianapolis, IN: Eli Lilly & Co; 2009. /us/effient.pdf. Accessed 1/31/2011.36 Subherwal S, Bach RG, Chen AY, et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score Circulation 2009;119:1873-1882.[Abstract/Free Full Text]37 Giugliano RP, White JA, Bode C, et al. Early versus delayed, provisional eptifibatide in acute coronary syndromes N Engl J Med 2009;360:2176-2190.[CrossRef][Medline]38 Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes N Engl J Med 2009;360:2165-2175.[CrossRef][Medline]39 Yusuf S, Wittes J, Friedman L. Overview of results of randomized clinical trials in heart disease. I. Treatments following myocardial infarction. JAMA 1988;260:2088-2093.[Abstract/Free Full Text]40 Cohen M, Demers C, Gurfinkel EP, et al. A comparison of low-molecular-weight heparin with unfractionated heparin for unstable coronary artery disease. Efficacy and Safety of Subcutaneous Enoxaparin in Non-Q-Wave Coronary Events Study Group. N Engl J Med 1997;337:447-452.[CrossRef][Web of Science][Medline]41 Antman EM, McCabe CH, Gurfinkel EP, et al. Enoxaparin prevents death and cardiac ischemic events in unstable angina/non-Q-wave myocardial infarction. Results of the thrombolysis in myocardial infarction (TIMI) 11B trial. Circulation 1999;100:1593-1601.[Abstract/Free Full Text]42 Antman EM, Cohen M, Radley D, et al. Assessment of the treatment effect of enoxaparin for unstable angina/non-Q-wave myocardial infarction. TIMI 11B-ESSENCE meta-analysis. Circulation 1999;100:1602-1608.[Abstract/Free Full Text]43 Mehta SR, Granger CB, Eikelboom JW, et al. Efficacy and safety of fondaparinux versus enoxaparin in patients with acute coronary syndromes undergoing percutaneous coronary intervention: results from the OASIS-5 trial J Am Coll Cardiol 2007;50:1742-1751.[Abstract/Free Full Text]44 The Antithrombotic Trialists' Collaboration Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients BMJ2002;324:71-86.[Abstract/Free Full Text]45 Goldman S, Copeland J, Moritz T, et al. Improvement in early saphenous vein graft patency after coronary artery bypass surgery with antiplatelet therapy: results of a Veterans Administration Cooperative Study Circulation1988;77:1324-1332.[Abstract/Free Full Text]46 Bybee KA, Powell BD, Valeti U, et al. Preoperative aspirin therapy is associated with improved postoperative outcomes in patients undergoing coronary artery bypass grafting Circulation 2005;112:I286-I292.[Web of Science][Medline]47 Dacey LJ, Munoz JJ, Johnson ER, et al. Effect of preoperative aspirin use on mortality in coronary artery bypass grafting patients Ann Thorac Surg 2000;70:1986-1990.[Abstract/Free Full Text]48 Mangano DT. Aspirin and mortality from coronary bypass surgery N Engl J Med 2002;347:1309-1317.[CrossRef][Web of Science][Medline]49 Lincoff AM, LeNarz LA, Despotis GJ, et al. Abciximab and bleeding during coronary surgery: results from the EPILOG and EPISTENT trials. Improve Long-term Outcome with abciximab GP IIb/IIIa blockade Evaluation of Platelet IIb/IIIa Inhibition in STENTing. Ann Thorac Surg 2000;70:516-526.[Abstract/Free Full Text]50 Bizzarri F, Scolletta S, Tucci E, et al. Perioperative use of tirofiban hydrochloride (Aggrastat) does not increase surgical bleeding after emergency or urgent coronary artery bypass grafting J Thorac Cardiovasc Surg2001;122:1181-1185.[Abstract/Free Full Text]51 Dyke CM, Bhatia D, Lorenz TJ, et al. Immediate coronary artery bypass surgery after platelet inhibition with eptifibatide: results from PURSUIT. Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrelin Therapy. Ann Thorac Surg 2000;70:866-871.[Abstract/Free Full Text]52 Clark SC, Vitale N, Zacharias J, et al. Effect of low molecular weight heparin (fragmin) on bleeding after cardiac surgery Ann Thorac Surg 2000;69:762-764.[Abstract/Free Full Text]53 Kincaid EH, Monroe ML, Saliba DL, et al. Effects of preoperative enoxaparin versus unfractionated heparin on bleeding indices in patients undergoing coronary artery bypass grafting Ann Thorac Surg 2003;76:124-128.[Abstract/Free Full Text]54 Jones HU, Muhlestein JB, Jones KW, et al. Preoperative use of enoxaparin compared with unfractionated heparin increases the incidence of re-exploration for postoperative bleeding after open-heart surgery in patients who present with an acute coronary syndrome: clinical investigation and reports Circulation 2002;106(Suppl 1):I19-I22.[CrossRef][Web of Science][Medline]55 Mehta SR, Yusuf S, Granger CB, et al. Design and rationale of the MICHELANGELO Organization to Assess Strategies in Acute Ischemic Syndromes (OASIS)-5 trial program evaluating fondaparinux, a synthetic factor Xa inhibitor, in patients with non-ST-segment elevation acute coronary syndromes Am Heart J 2005;150:1107.[Web of Science][Medline]56 Yusuf S, Mehta SR, Chrolavicius S, et al. Comparison of fondaparinux and enoxaparin in acute coronary syndromes N Engl J Med 2006;354:1464-1476.[CrossRef][Web of Science][Medline]57 Stone GW, Bertrand M, Colombo A, et al. Acute Catheterization and Urgent Intervention Triage strategY (ACUITY) trial: study design and rationale Am Heart J 2004;148:764-775.[CrossRef][Web of Science][Medline]58 Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes N Engl J Med2006;355:2203-2216.[CrossRef][Medline]59 Plavix (clopidogrel bisulfate) [package insert]. New York NY, and Bridgewater, NJ: Bristol-Myers Squibb Sanofi-aventis; 2009.60 Kim JH, Newby LK, Clare RM, et al. Clopidogrel use and bleeding after coronary artery bypass graft surgery Am Heart J 2008;156:886-892.[CrossRef][Web of Science][Medline]61 Knudtson ML, Flintoft VF, Roth DL, et al. Effect of short-term prostacyclin administration on restenosis after percutaneous transluminal coronary angioplasty J Am Coll Cardiol 1990;15:691-697.[Abstract]62 Montalescot G, Sideris G, Meuleman C, et al. A randomized comparison of high clopidogrel loading doses in patients with non-ST-segment elevation acute coronary syndromes: the ALBION (Assessment of the Best Loading Dose of Clopidogrel to Blunt Platelet Activation, Inflammation and Ongoing Necrosis) trial J Am Coll Cardiol2006;48:931-938.[Abstract/Free Full Text]63 Mahaffey KW, Ferguson JJ. Exploring the role of enoxaparin in the management of high-risk patients with non-ST-elevation acute coronary syndromes: the SYNERGY trial Am Heart J 2005;149:S81-S90.[CrossRef][Web of Science][Medline]64 Roe MT, Granger CB, Puma JA, et al. Comparison of benefits and complications of hirudin versus heparin for patients with acute coronary syndromes undergoing early percutaneous coronary intervention Am J Cardiol2001;88:1403-1406.[CrossRef][Web of Science][Medline]65 Ferguson JJ, Califf RM, Antman EM, et al. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial JAMA 2004;292:45-54.[Abstract/Free Full Text]66 Deleted in proof.67 White H. Thrombin-specific anticoagulation with bivalirudin versus heparin in patients receiving fibrinolytic therapy for acute myocardial infarction: the HERO-2 randomised trial Lancet 2001;358:1855-1863.[CrossRef][Web ofScience][Medline]68 Lincoff AM, Kleiman NS, Kereiakes DJ, et al. Long-term efficacy of bivalirudin and provisional glycoprotein IIb/IIIa blockade vs heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary revascularization: REPLACE-2 randomized trial JAMA 2004;292:696-703.[Abstract/Free Full Text]69 De Winter RJ, Windhausen F, Cornel JH, et al. Early invasive versus selectively invasive management for acute coronary syndromes N Engl J Med 2005;353:1095-1104.[CrossRef][Web of Science][Medline]70 Luchi RJ, Scott SM, Deupree RH. Comparison of medical and surgical treatment for unstable angina pectoris. Results of a Veterans Administration Cooperative Study. N Engl J Med 1987;316:977-984.[Web of Science][Medline]71 Peterson ED, Shaw LJ, Califf RM. Risk stratification after myocardial infarction Ann Intern Med1997;126:561-582.[Abstract/Free Full Text]72 Takaro T, Hultgren HN, Lipton MJ, et al. The VA cooperative randomized study of surgery for coronary arterial occlusive disease II. Subgroup with significant left main lesions. Circulation 1976;54:III107-III117.[Medline]73 Bonello L, Camoin-Jau L, Armero S, et al. Tailored clopidogrel loading dose according to platelet reactivity monitoring to prevent acute and subacute stent thrombosis Am J Cardiol 2009;103:5-10.[CrossRef][Web of Science][Medline]74 Breet NJ, van Werkum JW, Bouman HJ, et al. Comparison of platelet function tests in predicting clinical outcome in patients undergoing coronary stent implantation JAMA 2010;303:754-762.[Abstract/Free Full Text]75 Marcucci R, Gori AM, Paniccia R, et al. Cardiovascular death and nonfatal myocardial infarction in acute coronary syndrome patients receiving coronary stenting are predicted by residual platelet reactivity to ADP detected by a point-of-care assay: a 12-month follow-up Circulation 2009;119:237-242.[Abstract/Free Full Text]76 Matetzky S, Shenkman B, Guetta V, et al. Clopidogrel resistance is associated with increased risk of recurrent atherothrombotic events in patients with acute myocardial infarction Circulation2004;109:3171-3175.[Abstract/Free Full Text]77 Sofi F, Marcucci R, Gori AM, et al. Clopidogrel non-responsiveness and risk of cardiovascular morbidity. An updated meta-analysis. Thromb Haemost 2010;103:841-848.[Web of Science][Medline]78 American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents, American Heart Association, Society for Cardiovascular Angiography and Interventions, et al ACCF/AHA clopidogrel clinical alert: approaches to the FDA "boxed warning": a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the American Heart Association J Am Coll Cardiol 2010;56:321-341.[Free Full Text]79 Collet JP, Hulot JS, Pena A, et al. Cytochrome P450 2C19 polymorphism in young patients treated with clopidogrel after myocardial infarction: a cohort study Lancet 2009;373:309-317.[CrossRef][Web of Science][Medline]80 Giusti B, Gori AM, Marcucci R, et al. Relation of cytochrome P450 2C19 loss-of-function polymorphism to occurrence of drug-eluting coronary stent thrombosis Am J Cardiol 2009;103:806-811.[CrossRef][Web of Science][Medline]81 Mega JL, Close SL, Wiviott SD, et al. Cytochrome p-450 polymorphisms and response to clopidogrel N Engl J Med 2009;360:354-362.[CrossRef][Web of Science][Medline]82 Shuldiner AR, O'Connell JR, Bliden KP, et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy JAMA 2009;302:849-857.[Abstract/Free Full Text]83 Simon T, Verstuyft C, Mary-Krause M, et al. Genetic determinants of response to clopidogrel and cardiovascular events N Engl J Med 2009;360:363-375.[CrossRef][Web of Science][Medline]84 Trenk D, Hochholzer W, Fromm MF, et al. Cytochrome P450 2C19 681G>A polymorphism and high on-clopidogrel platelet reactivity associated with adverse 1-year clinical outcome of elective percutaneous coronary intervention withdrug-eluting or bare-metal stents J Am Coll Cardiol 2008;51:1925-1934.[Abstract/Free Full Text]85 Fibrinolytic Therapy Trialists' (FTT) Collaborative Group Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients Lancet 1994;343:311-322.[CrossRef][Web of Science][Medline]86 US Food and Drug Administration Early communication about an ongoing safety review of clopidogrel bisulfate (marketed as Plavix) /cder/drug/early_comm/clopidogrel_bisulfate.htm 1994Accessed April 6, 2009.87 Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes N Engl J Med 2009;361:1045-1057.[CrossRef][Medline]88 James S, Akerblom A, Cannon CP, et al. Comparison of ticagrelor, the first reversible oral P2Y(12) receptor antagonist, with clopidogrel in patients with acute coronary syndromes: rationale, design, and baseline characteristics of the PLATelet inhibition and patient Outcomes (PLATO) trial Am Heart J 2009;157:599-605.[CrossRef][Web of Science][Medline]89 Lau WC, Gurbel PA. The drug-drug interaction between proton pump inhibitors and clopidogrel CMAJ2009;180:699-700.[Free Full Text]90 Ho PM, Maddox TM, Wang L, et al. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome JAMA 2009;301:937-944.[Abstract/Free Full Text]91 Sofi F, Giusti B, Marcucci R, et al. Cytochrome P450 2C19*2 polymorphism and cardiovascular recurrences in patients taking clopidogrel: a meta-analysis Pharmacogenomics J March 30, 2010 doi:10.1038/tpj.2010.21 .92 Sibbing D, Stegherr J, Latz W, et al. Cytochrome P450 2C19 loss-of-function polymorphism and stent thrombosis following percutaneous coronary intervention Eur Heart J 2009;30:916-922.[Abstract/Free Full Text]93 Roden DM, Stein CM. Clopidogrel and the concept of high-risk pharmacokinetics Circulation2009;119:2127-2130.[Free Full Text]94 Mega JL, Close SL, Wiviott SD, et al. Cytochrome P450 genetic polymorphisms and the response to prasugrel: relationship to pharmacokinetic, pharmacodynamic, and clinical outcomes Circulation 2009;119:2553-2560.[Abstract/Free Full Text]95 Varenhorst C, James S, Erlinge D, et al. Genetic variation of CYP2C19 affects both pharmacokinetic and pharmacodynamic responses to clopidogrel but not prasugrel in aspirin-treated patients with coronary artery disease Eur Heart J 2009;30:1744-1752.[Abstract/Free Full Text]96 Mehta SR, Bassand JP, Chrolavicius S, et al. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes N Engl J Med 2010;363:930-942.[CrossRef][Web of Science][Medline]97 Bhatt DL, Scheiman J, Abraham NS, et al. ACCF/ACG/AHA 2008 expert consensus document on reducing the gastrointestinal risks of antiplatelet therapy and NSAID use: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents J Am Coll Cardiol 2008;52:1502-1517.[Free Full Text]98 Grines CL, Bonow RO, Casey Jr DE, et al. Prevention of premature discontinuation of dual antiplatelet therapy in patients with coronary artery stents: a science advisory from the American Heart Association, American College of Cardiology, Society for Cardiovascular Angiography and Interventions, American College of Surgeons, and American Dental Association, with representation from the American College of Physicians J Am Coll Cardiol 2007;49:734-739.[Abstract/Free Full Text]99 Juurlink DN, Gomes T, Ko DT, et al. A population-based study of the drug interaction between proton pump inhibitors and clopidogrel CMAJ 2009;180:713-718.[Abstract/Free Full Text]100 Deleted in proof.101 O'Donoghue ML, Braunwald E, Antman EM, et al. Pharmacodynamic effect and clinical efficacy of clopidogrel and prasugrel with or without a proton-pump inhibitor: an analysis of two randomised trials Lancet 2009;374:989-997.[CrossRef][Web of Science][Medline]102 Deleted in proof.103 Ramirez JF, Selzer F, Chakaprani R. Proton pump inhibitor and clopidogrel combination is not associated with adverse clinical outcomes after PCI: the NHLBI dynamic registry J Am Coll Cardiol 2009;53:A27-A28Abstract.104 Gilard M, Arnaud B, Cornily JC, et al. Influence of omeprazole on the antiplatelet action of clopidogrel associated with aspirin: the randomized, double-blind OCLA (Omeprazole CLopidogrel Aspirin) study J Am Coll Cardiol2008;51:256-260.[Abstract/Free Full Text]105 Sibbing D, Morath T, Stegherr J, et al. Impact of proton pump inhibitors on the antiplatelet effects of clopidogrel Thromb Haemost 2009;101:714-719.[Web of Science][Medline]106 Small DS, Farid NA, Payne CD, et al. Effects of the proton pump inhibitor lansoprazole on the pharmacokinetics and pharmacodynamics of prasugrel and clopidogrel J Clin Pharmacol 2008;48:475-484.[Abstract/Free Full Text]107 Wiviott SD, Trenk D, Frelinger AL, et al. Prasugrel compared with high loading- and maintenance-dose clopidogrel in patients with planned percutaneous coronary intervention: the Prasugrel in Comparison to Clopidogrel for Inhibition of Platelet Activation and Aggregation-Thrombolysis in Myocardial Infarction 44 trial Circulation2007;116:2923-2932.[Abstract/Free Full Text]108 Bhatt DL, Cryer BL, Contant CF, et al. Clopidogrel with or without omeprazole in coronary artery disease N Engl J Med 2010;363:1909-1917.[CrossRef][Medline]109 Boersma E, Simoons ML. Reperfusion strategies in acute myocardial infarction Eur Heart J1997;18:1703-1711.[Free Full Text]110 Hamm CW, Heeschen C, Goldmann B, et al. Benefit of abciximab in patients with refractory unstable angina in relation to serum troponin T levels. c7E3 Fab Antiplatelet Therapy in Unstable Refractory Angina (CAPTURE) Study Investigators. N Engl J Med 1999;340:1623-1629.[CrossRef][Web of Science][Medline]111 Heeschen C, Hamm CW, Goldmann B, et al. Troponin concentrations for stratification of patients with acute coronary syndromes in relation to therapeutic efficacy of tirofiban. PRISM Study Investigators. Platelet Receptor Inhibition in Ischemic Syndrome Management. Lancet 1999;354:1757-1762.[CrossRef][Web of Science][Medline]。
ACCF/ACG/AHA专家共识更新
降低抗血小板治疗和应用NSAID的胃肠道风险
河北省人民医院郭艺芳整理
为减少抗血小板药物对胃肠道的不良影响,美国心脏病学会基金会(ACCF)、美国胃肠病学会(ACG)及美国心脏学会(AHA)于2008年联合发表专家共识,建议接受抗血小板或(和)非类固醇类抗炎药(NSAID)治疗的患者积极应用质子泵抑制剂(PPI)。
然而2009年初所公布的一项大型病例对照研究却显示,联合应用氯吡格雷与PPI可能会增加心血管不良事件的发生。
此研究一度引起广泛关注,但随后陆续发表的一系列研究所得的结论却存在分歧,令临床<SPAN class =t_tag onclickclick=tagshow(event) href="tag.php?name=%D2%BD%CA%A6">医师无所适从。
2010年11月8日,ACCF/ACG/AHA对相关文献进行总结与分析后,更新了2008年版的专家共识。
虽然关于PPI是否会影响氯吡格雷的抗血小板作用尚无最终定论,但更新的指南仍根据现有证据为临床医师的临床实践提供了建议,这无疑是一个进步。
在本期《消化·肝病周刊》我们刊登了新版共识的要点(D1版),并邀请国内知名消化病专家及心血管病专家对该共识进行了解读(D 2版),希望对读者的临床工作有所帮助。
新版《共识》要点
对于降低抗血小板治疗和应用NSAID的胃肠道风险,更新的《ACCF/ACG/AH A降低抗血小板治疗和应用NSAID的胃肠道风险专家共识》(简称《共识》)主要有以下11点要点。
1. 氯吡格雷是预防动脉粥样硬化性心血管病患者血栓事件的有效药物。
2. 与单独使用阿司匹林相比,联合应用氯吡格雷与阿司匹林可进一步降低冠心病患者以及支架置入术后患者的血栓形成事件风险。
3. 氯吡格雷与阿司匹林单独或联合应用可增加胃肠道出血风险。
4. 胃肠道出血的高危人群包括:曾有胃肠道出血史,高龄,同时接受抗凝剂、类固醇类抗炎药或NSAID(包括阿司匹林)治疗,以及幽门螺杆菌感染者。
存在上述多种危险因素者的胃肠道出血危险可进一步增高。
5. 与单用抗血小板药物相比,加用PPI或组胺2(H2)受体拮抗剂可降低上消化道出血危险,而PPI的疗效优于H2受体拮抗剂。
6. 对于需要接受抗血小板治疗的患者,建议对曾有胃肠道出血史者预防性应用PPI,对于存在多种其他出血高危因素者,也可考虑应用PPI预防胃肠道出血。
7. 对于上消化道出血风险较低者,不建议常规预防性应用PPI或H2受体拮抗剂。
8. 对于每例患者,均需要谨慎地权衡利弊,评估其心血管获益与胃肠道出血并发症之间的平衡,然后决定是否需要在应用抗血小板的同时预防性应用PP I。
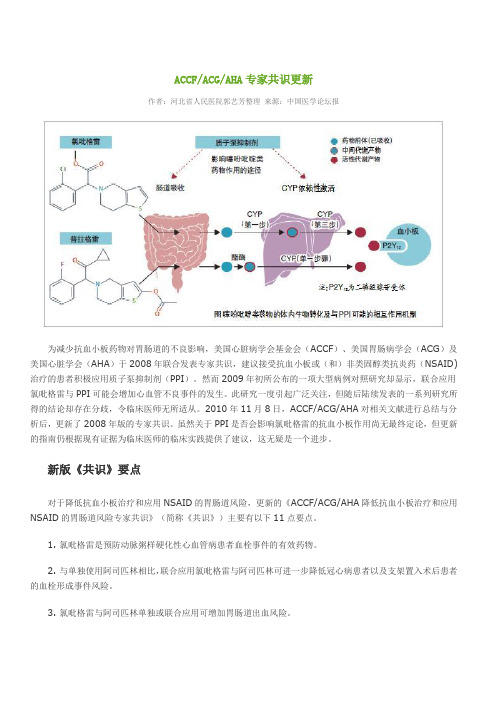
9. 药理学研究显示,同时应用氯吡格雷与PPI可降低前者的抗血小板疗效,其中以奥美拉唑对氯吡格雷的影响最为显著。
但尚不明确这种影响是否具有重要的临床意义。
10. 关于同时应用氯吡格雷与PPI是否可增加心血管不良事件的发生率,现有研究未能得出一致性的结论,仍需要进行更多的研究来进一步论证。
11. 根据药物基因学检测或血小板功能测定来评估氯吡格雷与PPI之间的相互影响的临床价值尚有待论证。
关于氯吡格雷与PPI联合应用的解释
PPI影响氯吡格雷疗效目前证据不充分
《共识》指出,现有部分观察性临床研究显示,联合应用PPI可对氯吡格雷疗效产生轻中度影响。
但观察性临床研究结果可能受到多种因素影响,证据力度有限,其结论尚须大规模随机对照试验证实。
迄今唯一一项旨在探讨联合应用PPI与氯吡格雷对临床终点事件影响的随机对照试验COGENT研究(氯吡格雷与胃肠道事件优化研究)结果显示,奥美拉唑并未显著降低氯吡格雷疗效。
但该研究随访期较短,据此不能得出最终结论。
体外研究显示,PPI可抑制细胞色素氧化酶P450(CYP)同工酶2C19的活性,而后者正是氯吡格雷代谢为活性形式所必须的关键物质,因而两类药物之间的相互影响具有药代动力学基础。
虽然不同PPI类药物的药代动力学特性相似,但药理学研究证实只有奥美拉唑可显著抑制氯吡格雷的抗血小板作用,并未发现其他PPI有此作用。
因此,在获取更为确凿的循证医学证据前,不应轻易否定PPI与噻吩吡啶类药物联合应用的治疗策略。
正在进行中的SPICE(他汀和PPI影响氯吡格雷抗血小板作用的评估)试验将为此提供更有价值的信息。
须对患者实施个体化预防消化道出血策略
《共识》强调,与任何药物一样,噻吩吡啶类均存在有益与有害的两方面作用。
对于部分高危心血管病患者,氯吡格雷可显著减少不良心脏事件,但同时也会增加胃肠道出血风险。
不同基线特征的患者接受氯吡格雷治疗时的获益风险比明显不同。
因此,在临床工作中,须对每例患者进行认真评估,并为之制定个体化治疗方案。
对于具有上消化道出血病史或其他出血高危因素的患者,接受氯吡格雷治疗的胃肠道出血风险显著增高,此时预防消化道并发症与降低心血管风险同样重要。
在此情况下,预防性应用PPI可有效降低消化道出血风险。
即使在氯吡格雷治疗时加用PPI可能会影响前者的抗血小板作用,但其总获益仍会超过潜在风险,因而仍被视为一种有效的治疗策略。
对于患有其他胃肠道疾病(如消化不良等)的患者,氯吡格雷治疗可能会加重消化道不适症状,而加用PPI有助于患者更好地耐受抗血小板治疗。
H2受体拮抗剂与PPI
虽然H2受体拮抗剂也可有效降低抗血小板制剂胃肠道危险,但其疗效逊于PPI。
在临床实践中,H2受体拮抗剂可作为PPI的替代治疗,用于胃肠道出血风险较低的患者。
由于西咪替丁可竞争性抑制CYP2C19活性,故对于正在接受氯吡格雷治疗者,应选择其他的H2受体拮抗剂。
抗血小板治疗的挑战
《共识》认为,关于氯吡格雷增加胃肠道出血风险机制尚有待进一步阐明。
如何在保证心血管获益的前提下降低噻吩吡啶类药物的胃肠道出血风险很值得深入研究。
通过较大规模的随机对照试验了解PPI或大剂量H2受体拮抗剂对抗血小板药物心血管保护作用的影响,将为制定临床决策提供重要依据。
不同患者对于抗血小板药物的反应性存在很大差异,如何通过实验室技术判定患者对氯吡格雷等药物的敏感性应成为优先研究的课题。
在今后的临床研究中,还应对通过实验室技术指导抗血小板药物临床应用的价值进行探讨。
此外,我们还需要更多了解不同剂量药物与临床转归之间的关系,以努力避免同时服用大剂量的PPI与氯吡格雷。