二尖瓣反流示意图
- 格式:pdf
- 大小:94.91 KB
- 文档页数:1
二尖瓣三尖瓣轻度反流是什么意思?该怎么办?看了你的问题,我觉得你应该是偶有心慌,胸闷,去医院就诊,大夫给你做了一系列的检查,其他的都没有问题,唯有这个彩超显示:二尖瓣、三尖瓣轻度返流。
并且很可能大夫给你来了句:“没有大问题,继续观察”,之后因就诊时间问题,你一脸懵的回来了。
心想着“我有明明有心慌、胸闷,心脏彩超显示有问题,大夫又说没问题?到底是怎么个情况?”今天我就以你的角度从以下几个方面解答你内心的疑问,“二尖瓣、三尖瓣轻度返流是什么意思?怎么造成的?要不要紧?该怎么办?”“心慌可能是什么原因造成的?是应做哪些检查?需要排除什么疾病?”一、二尖瓣、三尖瓣轻度返流是什么意思?怎么造成的?要不要紧?该怎么办?大家看一下面这个图片,记住二尖瓣三尖瓣的位置大家可以看到瓣膜是起到一个防止血液往回流的作用,让血液按照指定的方向往前一步一步的走,但随着瓣膜用的时间久了,老化必然会出现弹性下降,动作缓慢,功能下降,人体就像一台机器,机器老了,出现小问题很正常,只要大的方面正常,可以使可以使用就行了。
就像我们农村老家的木门用的时间久了,关不紧,漏风是必然的,但是它的作用在于晚上的时候把牛羊赶回家,关上大门,然后再把牛羊赶到羊圈里去;早晨的时候打开羊圈门,把牛羊赶出来,再关上羊圈门,打开大门,让牛羊去外面吃草,按路线行走,什么时候门关不关对牛羊都能跑出去,那就该修一修了。
同样的道理,二尖瓣一样无论开着或者是关闭对其中的血液顺流的作用,已经很小了,其中的血液大部分已经不听话了,这时候我们就需要通过手术或者其他的方法修复瓣膜,恢复它的功能。
轻度的瓣膜老化、返流是一种人随着生命发展的必然。
这里插一句,我们汉字博大精深,为甚返流而不是反流?是因为血液流过去,一部分返回来了,而不是流反了。
日常需要注意的是,1、定期复查观测瓣膜功能,别出了大问题才知道。
2、剧烈运动的运动耐力会下降,容易在激动后容易出现因供血供氧不足引起来的心慌,胸闷,但一般能很快自行缓解(其实,你反过来想想,正常人累了,也心慌,不用紧张)。

二尖瓣反流面积分度标准二尖瓣反流面积分度标准是一种用于判断二尖瓣反流严重程度的量化指标,它通常通过超声心动图来测量。
在评估二尖瓣反流时,医生会测量反流面积分度,并根据其大小来判断病情的严重程度。
下面我们来具体了解一下二尖瓣反流面积分度标准及其临床意义。
一、二尖瓣反流面积分度的测量方法二尖瓣反流面积分度通常通过超声心动图来测量,医生会利用超声波探头在患者胸部进行扫描,以获取心脏内部的图像。
通过观察超声心动图,医生可以清晰地看到反流血流的情况,并进行测量。
具体测量的方法包括以下几个步骤:1.测量二尖瓣口径:医生首先会测量二尖瓣口径的大小,这个数据是计算反流面积分度的基础。
2.测量反流速度:医生会用多普勒超声心动图测量反流血流的最大速度,这个速度值可以用来计算反流面积分度。
3.计算反流面积:通过测量二尖瓣口径和反流速度,可以利用连续多普勒方法计算反流面积分度。
通过以上步骤的测量,医生可以得到患者的二尖瓣反流面积分度的具体数值,这个数值可以用来评估病情的严重程度。
二、二尖瓣反流面积分度的临床意义二尖瓣反流面积分度是评估二尖瓣反流严重程度的重要指标,它对临床诊断和治疗具有重要意义。
具体来说,它有以下几个方面的临床意义:1.指导治疗方案:通过测量反流面积分度,可以帮助医生确定病情的严重程度,并制定合理的治疗方案。
一般来说,反流面积分度越大,表示反流程度越严重,需要更积极的治疗。
2.监测病情变化:二尖瓣反流面积分度可以帮助医生监测病情的变化,及时发现病情的进展,为临床治疗提供依据。
3.评估手术指征:对于一些二尖瓣反流严重的患者,可能需要进行二尖瓣置换手术或修补手术。
反流面积分度可以作为评估手术指征的重要依据,帮助医生确定是否需要进行手术治疗。
三、二尖瓣反流面积分度标准的临床应用二尖瓣反流面积分度标准的临床应用主要包括以下几个方面:1.评估病情严重程度:二尖瓣反流面积分度可以帮助医生评估病情的严重程度,根据其大小来确定治疗方案。


二尖瓣反流面积分度标准英文回答:Mitral valve regurgitation, also known as mitral valve insufficiency or mitral valve incompetence, is a condition where the mitral valve in the heart does not close properly, causing blood to flow backward into the left atrium during ventricular contraction. The severity of mitral valve regurgitation can be assessed by measuring the regurgitant orifice area (ROA) using echocardiography.The grading of mitral valve regurgitation based on ROAis as follows:Mild regurgitation: ROA less than 0.2 cm²。
Moderate regurgitation: ROA between 0.2 and 0.4 cm²。
Severe regurgitation: ROA greater than 0.4 cm²。
The ROA is a quantitative measurement that provides an objective assessment of the severity of mitral valve regurgitation. It is a useful tool for clinicians to determine the appropriate management and treatment options for patients with this condition.中文回答:二尖瓣反流,也称为二尖瓣不全或二尖瓣功能不全,是一种心脏疾病,指的是心脏中的二尖瓣无法完全关闭,导致血液在心室收缩时逆流进入左心房。
2024急性和慢性二尖瓣反流的临床表现差异二尖瓣反流是最常见的心脏瓣膜病之一。
据文献报道,在65岁以上老年人群中,中度及以上二尖瓣反流的患病率超过7%,但在我国仍处于患病知晓率及治疗率低的阶段。
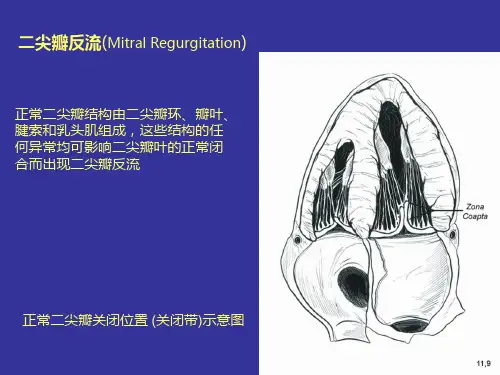
二尖瓣反流定义二尖瓣结构主要包括瓣叶、瓣环、腱索、乳头肌四部分。
正常二尖瓣的功能有赖于此四部分及左心的结构和功能完整性,任何一个部分发生结构异常或功能失调,均可导致二尖瓣关闭不全。
例如常见的二尖瓣瓣叶风湿性损害,多见于女性。
二尖瓣瓣环退行性变,或由左室扩大、左心衰竭造成二尖瓣瓣环扩大也可导致瓣叶关闭不全。
此外,先天性、自发性的,或继发于感染性心内膜炎、风湿热的腱索断裂也是MR的常见病因。
其他病因还包括乳头肌缺血或坏死,或先天性心脏病、肉芽肿、淀粉样变、结节病、肥厚型心肌病等造成的二尖瓣结构或功能异常。
二尖瓣反流(MR)又称二尖瓣关闭不全。
MR是人群中最常见的心脏瓣膜病。
预计到2030年,美国的中重度MR患者将增长到400万。
在我国,MR具有发病率较高、知晓率低和治疗率低的特点,MR检出率随着年龄增长而增加,≥65岁人群MR检出率可达25.2%,但仅有不到1/5的患者入院前知悉病情。
二尖瓣反流的病因根据起病急缓分类:急性&慢性根据起病的急缓及病因,可以分为两类:一类是急性MR,主要发生原因为腱索断裂、乳头肌功能不全或断裂、感染性心内膜炎,此类情况往往伴随急性血流动力学障碍或心衰等,需要紧急医疗干预;另一类是慢性MR,主要发生原因为瓣膜黏液样变性、风湿性心脏损害或二尖瓣退行性变,病情进展相对较慢,患者出现症状的时间较晚。
在我国,慢性MR最常见的病因已由过去的风湿热转变为腱索断裂,而在发达国家为二尖瓣黏液样变性。
根据发生机制分类:原发性/器质性&继发性/功能性根据发生机制不同,可将MR分为两类,一类称为原发性二尖瓣反流或器质性二尖瓣反流,常由瓣叶或腱索病变造成;另一类称为继发性二尖瓣反流或功能性二尖瓣反流,常由左心扩张和或二尖瓣瓣环扩张而导致。
·298·A:凹陷;B:平直;C:袋装;D、E、F是通过内窥镜功能看到的与A、B、C相对应的凹陷、平直、袋装结构。
I,APW=左心房后肇:LIPV=左下肺静脉;LSPV=左卜肺静脉;MA=二尖瓣环;MI=二尖瓣峡酃;MV=二尖瓣;Appendage=左心耳(引自JCardiovascElectrophysiol,2006,17:1274一1278)图1多排CT显尔的二尖瓣峡部形态管冠状静脉窦常有左心房心肌包绕,心大静脉无左心房心肌包绕,消融径线应向左侧偏向冠状静脉窦的方向,而不是右侧心大静脉的方向。
心大静脉并不与二尖瓣环平行,在二尖瓣环的下部心大静脉与二尖瓣环分离,其到二尖瓣环的平均距离是8.5(3—15)nlnl。
这种异常在冠状静脉窦或心大静脉中进行二尖瓣峡部消融时,可造成消融径线不完整,导致传导缝隙的存在,引发消融术后房性心律失常的发生。
另外在10%的标本中发现二尖瓣峡部延伸到二尖瓣瓣叶约lmm,这可能是二尖瓣峡部消融径线不完整而造成消融后发生房性心律失常的原因之一。
在二尖瓣峡部消融径线上,有左回旋支动脉和右冠状动脉分布。
左回旋支动脉分支到二尖瓣峡部心内膜面距离<5mm,在二尖瓣峡部的消融过程中,由于左回旋支动脉和右冠状动脉分支血流的冲刷作用使得局部消融温度降低,消融能量损失而影响消融效果,而且消融过程中容易造成左l旦I旋支动脉分支的损伤(图2)。
Marshall静脉是冠状静脉窦在心房侧的一个分支,于心外膜面呈斜形走行至左下肺静脉。
冠状静脉窦入口的解剖位置和或MamhMl静脉经冠状静脉窦传导至心房的径路的一部分正好位于左心房峡部区域(图2)。
研究发现Marshall静脉自律性增加可诱发房颤,对Marshall静脉进行消融后可治愈一部分局灶起源房颤¨J。
二尖瓣峡部在房颤发生与发展中的作用Vias等"1对19例患者左心房激动特征分析发现由于左心房心内膜纤维方向的变异,肺静脉fs】隔侧与左心房后壁双侧肺静脉延伸至二尖瓣环心房肌纤维融合形成一解剖障碍区。
Mitral regurgitation/insufficiency
Basics:
Mitral regurgitation/insufficiency (MR/MI) results from a dilated mitral annulus, diseased leaflets, or abnormal leaflet coaptation (including a leaflet cleft). Severe MR can lead to left atrial enlargement, atrial fibrillation and heart failure since the heart must pump more to maintain adequate systemic flow. Left ventricular hypertrophy and impaired myocardial perfusion can result. Surgical correction is aimed at repairing the physical valve or replacing it with a tissue valve or mechanical valve. Mitral valve repair in pediatric patients is favored over mechanical replacement since it allows for growth and may preclude the need for lifelong anticoagulation, especially in active young patients. Repair of the valve may include placing an annuloplasty ring that helps control the annulus size and provide for improved leaflet coaptation. Mechanical replacement is more common as one progresses through the adult years.
Bypass notes:
• Maximum anticipated flow for equipment selection: 3.0 L/min/m2.
• Cardioplegia is required. Consideration must be given to higher cardioplegia delivery pressures/flows if significant ventricular hypertrophy exists. This will help ensure proper myocardial distribution of cardioplegia.• Bicaval cannulation is required.
• Left ventricular vent is common.
• Target temperature is 28–32 °C.
• Minimum dilutional hematocrit is 25–30%. An increased hematocrit before coming off bypass must be considered for sick myocardium.
• Valve irrigation solution is ideally scavenged with cell saver or wall suction.
• Valve testing solution may be scavenged with pump suckers or the cell saver suction.
• Excessive valve testing solution returned to the pump will require sodium bicarbonate for buffering. The patient’s sodium may rise if bicarbonate administration is regular.
• Consideration should be given to informing the surgeon of the sodium load when the patient’s sodium level rises above 150 mmol/L.
• Aggressive conventional ultrafiltration may be helpful in maintaining the hematocrit.
• DUF or ZBUF may be helpful in adjusting the sodium level when relatively large volumes of test solution are returned to the pump.• Severe and/or long-standing MR may negatively impact the pulmonary vasculature. Inhaled nitric oxide is com-monly made available when there is concern for pulmonary hypertension after bypass.
• It is not uncommon to see reoperative mitral valve repairs (See section “Reoperations” in Chapter 5)
.
Figure 6.32 Mitral regurgitation. Adapted from Mullins and Mayer [1]. Reproduced with permission of John Wiley & Sons.。