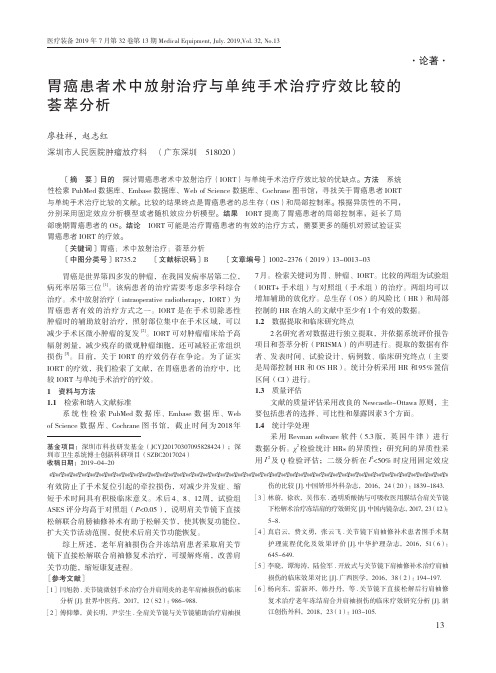
EORTC-ROG欧洲癌症治疗研究组放疗协作组对胃食管接合部肿 瘤及胃癌放疗专家共识分别勾画各淋巴结引流
- 格式:pdf
- 大小:1.98 MB
- 文档页数:12

局部进展期胃癌新辅助化疗和转化治疗的现状与进展完整版胃癌是全世界常见恶性肿瘤之一,其发病率在东西方差异较大,东亚地区的发病率远高于欧美地区。
我国是胃癌发病例数最多的国家,约占全世界胃癌患者的42%。
多数患者确诊时已进入进展期,因早期胃癌常缺乏典型的临床表现,且胃镜检查普及程度不同。
中国胃肠肿瘤外科联盟收集全国85家医学中心88 340例胃癌手术患者资料,其中局部进展期胃癌比例高达70.8%。
目前,手术治疗为局部进展期胃癌的首选治疗方案,但若病情处于局部晚期阶段,则手术切除难度较大且复发率较高。
为提高胃癌的根治性切除率、改善预后,国际上广泛开展针对局部进展期胃癌治疗模式的探索。
对于初期可切除的局部进展期胃癌患者,新辅助化疗能缩小肿瘤体积,实现肿瘤降期及根除微转移,可提高手术R0率;而对于不可切除的局部进展期胃癌患者,转化治疗则为患者提供了新方向。
一、新辅助化疗(一)新辅助化疗适用人群近年来,世界各国学者针对局部进展期胃癌积极开展前瞻性临床研究,探讨新辅助治疗的疗效,并据此制订针对不同地区和患者情况的胃癌治疗指南。
根据最新版本的不同指南,新辅助化疗在适应人群范围存在差异。
NCCN的胃癌临床实践指南推荐:全身状况良好、潜在可切除病灶且临床分期为cT2~4N0~3期的患者首选新辅助化疗或新辅助放化疗,将术前辅助化疗联合术后辅助治疗模式作为临床分期≥cT2N0期胃癌的首选治疗方式。
欧洲肿瘤内科学会推荐的适用范围较NCCN更广,推荐为临床分期≥cT1N0期可切除胃癌患者。
日本胃癌协会治疗指南对局部进展期胃癌的新辅助治疗适应证相对较保守,推荐的新辅助化疗适应证为:(1)预计可R0切除但复发风险较高的患者,如cTNM ⅢA~ⅢC期[cT4,cN+,无腹膜和(或)肝转移]患者。
(2)预计可R0或R1切除但预后较差的患者,如淋巴结广泛转移、体积较大的Borrmann Ⅲ型、Borrmann Ⅳ型患者。
中国临床肿瘤学会胃癌临床指南对新辅助化疗的适应证进行明确规定,推荐临床分期Ⅲ期(cT3~4aN1~3M0)胃癌和临床分期Ⅱ期(cT1~2N1~3M0及cT3~4N0M0)的胃食管结合部胃癌患者行包括SOX、XELOX、FOLFOX(5-氟尿嘧啶+亚叶酸钙+奥沙利铂)DOS及FLOT 方案的新辅助治疗。

局部晚期胃癌术后同步放化疗研究进展
王鑫;金晶
【期刊名称】《实用肿瘤杂志》
【年(卷),期】2011(26)3
【摘要】胃癌是全球最常见的恶性肿瘤之一,尽管其发病率在近几十年问呈下降趋势,但在世界每年新发肿瘤中胃癌仍占10%,并占所有死亡病例的12%。
尤其在日本、中国、西欧和拉丁美洲等地区,胃癌已成为主要的癌症死因。
因胃癌患者临床症状不典型,就诊时多为局部晚期,根治性手术(R0切除)是其唯一的治愈手段,
【总页数】4页(P225-228)
【关键词】胃肿瘤;药物疗法;放射疗法;淋巴转移;复发
【作者】王鑫;金晶
【作者单位】中国医学科学院肿瘤医院放疗科
【正文语种】中文
【中图分类】R735.2
【相关文献】
1.局部晚期宫颈癌术前新辅助同步放化疗与术后辅助同步放化疗临床疗效研究 [J], 葛俊丽;孙季冬;李佳;吕小慧;荆茹;魏莉;陈必良
2.晚期直肠癌术前局部同步放化疗与术后同步放化疗的临床研究 [J], 唐锟
3.单纯化疗与同步放化疗在局部进展期胃癌术后中的应用效果对比 [J], 胡彬;黄勇;
孟曼;姚荣杰;程莹星
4.单纯化疗与同步放化疗在局部进展期胃癌术后中的应用效果对比 [J], 胡彬;黄勇;孟曼;姚荣杰;程莹星
5.局部晚期胃癌术后同步放化疗临床研究 [J], 涂向阳
因版权原因,仅展示原文概要,查看原文内容请购买。

食管胃结合部腺癌的定义和分型:从历史到现状摘要当前,学界对食管胃结合部腺癌的关注度日渐升高。
食管胃结合部跨越胸腔和腹腔两大解剖区域,具有不同于食管和胃的组织学特征,相关学科对其定义和分型等基本问题普遍存在分歧。
日本《胃癌处理规约》总结各方观点,对食管胃结合部给出了全面的定义。
近年来,食管胃结合部在概念上逐渐扩展为复杂的功能解剖区域,范围涵盖了远端食管至近端胃。
食管胃结合部的静脉和淋巴管网具有双向流动的特点,是该部位肿瘤侵袭和转移规律的重要解剖学基础。
Nishi分型和Siewert分型的出现,推动了食管胃结合部癌临床研究的发展。
Siewert分型获得广泛认可,被相继引入国际主要临床指南。
目前一般建议,Siewert Ⅰ型和Ⅱ型肿瘤分期和治疗参照食管癌处理,Siewert Ⅲ型肿瘤参照胃癌处理。
但日本食管癌和胃癌治疗指南中,对食管胃结合部癌仍使用Nishi分型。
近期,国内多学科专家共同制定了食管胃结合部腺癌外科治疗的中国专家共识,对当前相关领域的主要争议进行了总结,并结合国内情况提出了建议。
只有回归基本的解剖学、生理学视角,加强多学科的沟通合作,借助新兴的生物信息学、数字技术、材料科学技术,才有望走出传统食管胃结合部腺癌分型和分期面临的困境。
近年来,食管胃结合部腺癌(adenocarcinoma of esophagogastric junction,AEG)的发病率明显上升,引起学界的日益重视[1, 2]。
但食管胃结合部(esophagogastric junction,EGJ)横跨胸腔和腹腔两大解剖区域,又具有不同于食管和胃的组织学特征,即便是定义、分型等基本问题,不同学科的认识并不一致,东西方学者的观点也多有分歧,从而导致治疗策略、手术方式、预后判断等关键问题难以统一观点[3]。
除腺癌外,EGJ还会发生鳞状细胞癌,其临床特点和处理原则又与AEG不同。
我们拟从历史的维度,对EGJ及AEG定义和分型的变迁,以及存在的争议和分歧加以梳理,以期为相关研究提供借鉴。

eortc评价标准
EORTC(欧洲癌症研究组织)评价标准是指由欧洲癌症研究组织
制定的一套用于评估肿瘤治疗效果和患者生存质量的标准体系。
这
些评价标准涵盖了多个方面,包括肿瘤的临床表现、组织病理学特征、影像学表现、治疗反应、生存率等。
从临床表现的角度来看,EORTC评价标准会考虑肿瘤的大小、
位置、浸润范围等因素,以及患者的临床症状和体征。
这些信息有
助于评估肿瘤的严重程度和对患者生活质量的影响。
在组织病理学特征方面,EORTC评价标准会关注肿瘤的组织学
类型、分化程度、浸润深度、淋巴结转移等因素。
这些信息有助于
评估肿瘤的生物学行为和预后。
在影像学表现方面,EORTC评价标准会考虑各种影像学检查结果,如CT、MRI、PET-CT等,以评估肿瘤的大小、范围、转移情况等。
在治疗反应方面,EORTC评价标准会根据患者接受治疗后肿瘤
的缩小程度、病灶的变化以及患者的耐受性等因素来评估治疗效果。
最后,在生存率方面,EORTC评价标准会根据患者的存活时间、生存率等指标来评估治疗效果和预后情况。
总的来说,EORTC评价标准是一个综合的评估体系,涵盖了肿
瘤的临床、病理、影像学表现,治疗反应以及生存率等多个方面,
可以帮助医生全面评估肿瘤患者的病情和治疗效果,指导临床决策
和个体化治疗方案的制定。

RTRadiotherapy,Radiation Therapy放疗,放射治疗IMRTIntensity Modulated Radiation Therapy调强放射治疗MLCMultiLeaf Collimator多叶准直器,多叶光栅QA & QCQuality Assurance & Quality Control质量保证和质量控制AAPMAmerican Association of Physicists in Medicine美国医学物理学家协会SADSource to Axis Distance源轴距SADSource to Axis Distance源轴距放射源到机架旋转或机器等中心的距离。
SSDSource to Surface Distance源皮距放射源到模体表面照射野中心的距离。
3DCRT、X刀、IMRT等技术都采用SAD技术,国内常规放疗正在普及SAD等中心照射技术,希望大家能尽早放弃SSD技术,只在某些特定情况下采用SSD技术。
PDDPercentage Depth Dose百分深度剂量定义为射野中心轴上某一深度处的吸收剂量率与参考点深度处剂量率的百分比。
对于高能X (γ)射线,参考深度一般取在射野中心轴上最大剂量点深度处。
TMRTissue Maximum Ratio组织最大剂量比定义为模体中射野中心轴上任意一点的剂量率与空间同一点模体中射野中心轴上最大剂量点深度处同一射野的剂量率之比。
LALinear Accelerator直线加速器DVHDose V olume Histogram剂量体积直方图三维治疗计划系统中用DVH表示某感兴趣区域如靶区或OAR的体积内有多少体积受到多高剂量的照射。
DVH是评估计划设计方案的最有力的工具,根据DVH图可以直接评估高剂量区与靶区的适合度。
但是,考虑到串型器官的耐受剂量特性,DVH应该与相应计划的等剂量分布图结合来综合评估。
胃癌术后辅助放射治疗的原理和实践共识
谢松喜
【期刊名称】《循证医学》
【年(卷),期】2005(005)004
【摘要】放射治疗目前已作为高危的完全切除的胃癌和胃食管结合部癌标准辅助治疗方案的重要组成部分。
本文将总结相关文献资料和放射治疗的原理,并讨论临床实践中如何应用放射治疗。
【总页数】7页(P225-231)
【作者】谢松喜
【作者单位】广东省人民医院肿瘤中心放疗科,广州,510080
【正文语种】中文
【中图分类】R735.2
【相关文献】
1.计算机辅助教学在《机械原理》课程教学中的实践 [J], 陈红亮
2.计算机辅助教学在《机械原理》课程教学中的实践 [J], 陈红亮;
3.Matlab辅助激光原理与技术教学的实践 [J], 王东;谢黎旭;郝树宏;莫绪涛
4.微信公众平台对《医学影像成像原理》的辅助教学实践 [J], 韩豆
5.语料库辅助英语教学:原理、模式与实践 [J], 张春青
因版权原因,仅展示原文概要,查看原文内容请购买。
三维适形放疗联合TACE治疗肝癌并发门静脉癌栓疗效的Meta分析张立洁;彭泉;芦东徽;侯宇宸;付贵峰【期刊名称】《实用肝脏病杂志》【年(卷),期】2015(018)003【摘要】Objective To analyze the short and long-term effects of three-dimensional conformal radiation therapy (3D-CRT) combined with TACE versus TACE alone for treatment of patients with hepatocellular carcino-ma with portal vein tumor thrombus (PVTT). Methods Retrieval was performed according to the principles of systemic assessment,then we conducted a meta-analysis to compare 3-DCRT combined with TACE versus TACE alone for treatment of patients with hepatocellular carcinoma with PVTT. Results A total of 8 randomized con-trolled trials were included,and 463 cases receiving 3-DCRT combined with TACE and 386 receiving TACE alone were recruited. Compared with in TACE alone,the 3D-CRT combined with TACE treatment had advantages in tumour therapeutic response [OR2.871,95%CI(1.426,5.783),P<0.05],control rate [OR 2.871,95%CI(1.426,5.783),P<0.05],1-year survival [OR 2.993,95%CI(1.713,5.230),P<0.05] and 2-year survival [OR 3.054,95%CI (1.170,7.973),P<0.05]. Conclusion 3D-CRT combined with TACE is better than TACE alone in treatment of patients with hepatocellular carcinoma with PVTT,which warrants further study.%目的应用荟萃(Meta)分析法探讨三维适形放疗(3-DCRT)联合TACE与单纯TACE治疗肝癌伴门脉癌栓的近期及远期疗效.方法按系统评价原则,对2000年~2014 年公开发表的有关3-DCRT 联合TACE与单纯TACE治疗肝癌伴门脉癌栓的临床随机对照研究进行系统评价.结果共有8篇文献纳入研究,累计3D-CRT联合TACE 治疗463例,单纯TACE治疗386例,纳入研究存在异质性,采用随机效应模型分析.Meta分析显示:3D-CRT联合TACE组与单纯TACE组在有效率[OR2.871,95%CI(1.426,5.783)]、控制率[OR 2.871,95%CI (1.426,5.783)]、1 a生存率[OR 2.993,95%CI(1.713,5.230)]、2 a生存率[OR3.054,95%CI(1.170,7.973)]均存在统计学差异(P<0.05).结论 3-DCRT 联合TACE 治疗肝癌伴门脉癌栓的近期及远期疗效优于单纯TACE 治疗,值得进一步验证.【总页数】4页(P254-257)【作者】张立洁;彭泉;芦东徽;侯宇宸;付贵峰【作者单位】230031 合肥市解放军第105 医院肿瘤中心;230031 合肥市解放军第105 医院普通外科;230031 合肥市解放军第105 医院肿瘤中心;山东大学rn医学生;230031 合肥市解放军第105 医院肿瘤中心【正文语种】中文【相关文献】1.三维适形放疗联合TACE与单纯TACE治疗肝癌疗效的meta分析 [J], 张耀伟;张勇;凌志海;李启生;陈龙华2.TACE联合三维适形放疗治疗肝癌合并门静脉癌栓的疗效观察 [J], 刘永国3.三维适形放疗联合TACE治疗肝癌伴门静脉癌栓的有效性与安全性的Meta分析[J], 王亚运;胡欢;王世垚;王龙;张勇;彭为;郑鹏飞;程志斌4.TACE术联合放疗治疗原发性肝癌并发门静脉癌栓疗效及免疫指标影响 [J], 邓成清; 时海峰; 唐爱群5.TACE术联合放疗治疗原发性肝癌并发门静脉癌栓疗效及免疫指标影响 [J], 邓成清; 时海峰; 唐爱群因版权原因,仅展示原文概要,查看原文内容请购买。
食管胃结合部腺癌外科治疗中国专家共识(2024年版)中国医师协会内镜医师分会腹腔镜外科专业组;国际食管疾病学会中国分会;中国食管胃结合部腺癌研究协作组;中国抗癌协会胃癌专业委员会;中华医学会肿瘤学分会胃肠肿瘤学组;胡建昆;陈龙奇;季加孚;李印【期刊名称】《消化肿瘤杂志(电子版)》【年(卷),期】2024(16)2【摘要】《食管胃结合部腺癌外科治疗中国专家共识(2018版)》自颁布以来,很大程度上促进了我国食管胃结合部腺癌(AEG)的规范化、同质化诊疗,提升了我国AEG的外科治疗水平。
经过5年的临床实践,该共识普适性和可行性已得到广泛证实。
鉴于AEG发病率持续上升的趋势及其解剖部位、临床病理特征和分子生物学特征的特殊性,AEG成为近5年来外科临床研究的热点之一,并不断有新的临床研究证据发表。
但是,对于AEG的定义、分型、分期、手术路径、切除范围、淋巴结清扫规范和消化道重建等外科问题,仍旧存在争议。
鉴于此,有必要对2018版的共识进行更新。
《食管胃结合部腺癌外科治疗中国专家共识(2024版)》在前一版的基础上,整合并分析5年来新的最佳临床证据,参考最新国际指南与共识,结合我国外科专家组意见,针对AEG外科治疗关键环节,包括AEG的定义和分型、手术径路、手术方式、淋巴结清扫范围、消化道重建方式及外科围手术期治疗等存在争议的问题,提出相关推荐建议,以期更好地规范AEG的外科治疗方式。
在本共识中未解决的相关问题,尚需积极开展高质量的临床研究,以逐步探索和解决。
【总页数】20页(P133-152)【作者】中国医师协会内镜医师分会腹腔镜外科专业组;国际食管疾病学会中国分会;中国食管胃结合部腺癌研究协作组;中国抗癌协会胃癌专业委员会;中华医学会肿瘤学分会胃肠肿瘤学组;胡建昆;陈龙奇;季加孚;李印【作者单位】不详【正文语种】中文【中图分类】R73【相关文献】1.基于快速康复外科理念的护理干预在管状胃重建治疗食管胃结合部腺癌患者中的应用效果2.食管-胃结合部腺癌手术治疗的共识与争议3.《子宫颈胃型腺癌临床诊治中国专家共识(2021年版)》解读4.中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)5.《中国肿瘤临床》文章推荐:来那度胺治疗淋巴瘤中国专家共识(2024年版)因版权原因,仅展示原文概要,查看原文内容请购买。
理念与实践结合-重视食管胃结合部腺癌的新辅助治疗王军;张彦军【期刊名称】《世界华人消化杂志》【年(卷),期】2016(0)21【摘要】近年来食管胃结合部腺癌(adenocarcinoma of esophagogastric junction,AEG)的发病率急剧上升,其作为一类独立于食管癌、胃癌疾病的观点被越来越多的学者接受.手术切除是AEG获得根治性治疗的基石,只有完整切除原发肿瘤及D2淋巴结清扫才能达到有效的治疗目的.关于各型AEG根治术的手术径路、食管胃切除范围、淋巴结清扫范围等问题尚存在一些争议.此外由于多数患者确诊时已处于局部进展期,单纯手术治疗局部复发率高,生存状况较差,因此AEG的新辅助治疗受到较多关注.目前相关临床研究显示新辅助化疗使AEG患者5年生存获益,新辅助放化疗亦可作为标准的治疗手段应用于临床实践,而有关新辅助治疗的最佳方式以及新辅助放化疗和新辅助化疗的疗效比较仍需要更多前瞻性临床研究数据.【总页数】9页(P3223-3231)【关键词】食管胃结合部腺癌;手术治疗;新辅助治疗【作者】王军;张彦军【作者单位】河北医科大学第四医院放疗科【正文语种】中文【中图分类】R735.1【相关文献】1.新辅助同步放化疗和单纯化疗在Ⅲ期食管胃结合部腺癌治疗中的应用对比观察[J], 曹铭富;彭涛;王国强;苏卓彬;张育;高强;毕仁杰;李曙光2.新辅助同步放化疗联合手术对比直接手术治疗SiewertⅡ、Ⅲ型食管胃结合部腺癌随机对照试验的远期预后分析 [J], 田园;赵群;王强;王军;乔学英;张钧;林叶成;李勇;范立侨;杨沛刚3.新辅助治疗在食管胃结合部腺癌的研究进展 [J], 毕仁杰;黄迪;彭涛;武文龙;李曙光4.新辅助治疗对食管胃结合部腺癌的效果观察 [J], 张发展;任维维;何明彦5.PD-1抑制剂联合SOX化疗方案在进展期胃食管结合部腺癌新辅助治疗中的疗效及安全性初探 [J], 尹玉平;张鹏;蔡明;陈俊华;李伟;李钢;王征;王国斌;陶凯雄因版权原因,仅展示原文概要,查看原文内容请购买。
GuidelinesEORTC-ROG expert opinion:Radiotherapy volume and treatment guidelines for neoadjuvant radiation of adenocarcinomas of the gastroesophageal junction and the stomachOscar Matzinger a,b,*,Erich Gerber c ,Zvi Bernstein d ,Philippe Maingon e ,Karin Haustermans f ,Jean François Bosset g ,Akos Gulyban a ,Philip Poortmans h ,Laurence Collette a ,Abraham Kuten daEORTC Headquarters,Brussels,BelgiumbCHU Vaudois,Department of Radiation Oncology,Lausanne,Switzerland cRadiation Oncologist,Vienna,Austria dRambam Health Care Campus,Oncology Department,Haifa,Israel eCentre Georges-Francois Leclerc,Department of Radiation Oncology,Dijon,France fU.Z.Gasthuisberg,Department of Radiation Oncology,Leuven,Belgium gCHR de Besancon,Department of Radiation Oncology,Besancon,France hDr.Bernard Verbeeten Institute,Department of Radiation Oncology,Tilburg,The Netherlandsa r t i c l e i n f o Article history:Received 12January 2009Accepted 5March 2009Available online 15April 2009Keywords:Guideline GastricGastroesophageal Radiotherapy Target volume Neoadjuvanta b s t r a c tPurpose:The Gastro-Intestinal Working Party of the EORTC Radiation Oncology Group (GIWP-ROG)developed guidelines for target volume definition in neoadjuvant radiation of adenocarcinomas of the gastroesophageal junction (GEJ)and the stomach.Methods and materials:Guidelines about the definition of the clinical target volume (CTV)are based on a systematic literature review of the location and frequency of local recurrences and lymph node involve-ment in adenocarcinomas of the GEJ and the stomach.Therefore,MEDLINE was searched up to August 2008.Guidelines concerning prescription,planning and treatment delivery are based on a consensus between the members of the GIWP-ROG.Results:In order to support a curative resection of GEJ and gastric cancer,an individualized preoperative treatment volume based on tumour location has to include the primary tumour and the draining regional lymph nodes area.Therefore we recommend to use the 2nd English Edition of the Japanese Classification of Gastric Carcinoma of the Japanese Gastric Cancer Association which developed the concept of assigning tumours of the GEJ and the stomach to anatomically defined sub-sites corresponding respectively to a distinct lymphatic spread pattern.Conclusion:The GIWP-ROG defined guidelines for preoperative irradiation of adenocarcinomas of the GEJ and the stomach to reduce variability in the framework of future clinical trials.Ó2009Elsevier Ireland Ltd.All rights reserved.Radiotherapy and Oncology 92(2009)164–175Gastric and oesophageal cancers are highly lethal malignancies.Even if the incidence of distal Gastric Cancer (GC)has been decreasing over the past decades,the incidence of newly diagnosed proximal cancers (localized at cardia and gastroesophageal junc-tion (GEJ)),has dramatically increased [1].The mainstay of curative treatment of GC is a radical surgical resection [2].More than half of all patients with advanced stage disease undergoing radical tumour resection relapse and die with-in five years [3]despite considerable progress in this surgical pro-cedure in Japanese and Western countries [4].Several clinicalfollow-up and autopsy series have shown high rates of loco-regio-nal recurrences and systemic metastases [5,6].This highlights the need of further efforts to standardize and optimize new multi-modal strategies combining different neoadjuvant and/or adjuvant protocols [2,7].There are two main pathological presentations of oesophageal cancer:squamous cell cancer (SCC)and adenocarcinoma (AC).ACs of the oesophagus were treated until recently similarly to squamous cell carcinomas of the oesophagus whereas ACs of the cardia were often mixed with GC [8].An increasing amount of evi-dence supports the view that ACs of the junction have clearly to be considered separately to other tumours of the stomach and of the oesophagus as these tumours differ in terms of pathogenesis,epidemiology,prognosis as well as in the surgical approach [9–16].0167-8140/$-see front matter Ó2009Elsevier Ireland Ltd.All rights reserved.doi:10.1016/j.radonc.2009.03.018*Corresponding author.Address:Department of Radiation Oncology,Centre Hospitalier Universitaire Vaudois (CHUV),Rue du Bugnon 46,1011Lausanne,Switzerland.E-mail address:Oscar.Matzinger@ (O.Matzinger).Radiotherapy and Oncology 92(2009)164–175Contents lists available at ScienceDirectRadiotherapy and Oncologyj o u r n a l h o m e p a g e :w w w.t h e g r e e n j o u r n a l.c omAn important goal of preoperative chemoradiation is to reduce the primary tumour volume to facilitate surgery and increase R0 resections(resulting in a decreased local recurrence rate).Other theoretical benefits include a potentially earlier effect on micro metastatic disease and a change in the ability of tumour cells that may be spread at the time of surgical resection to implant at other locations.Moreover,patients may be diagnosed with rapidly growing metastatic carcinoma before surgery,thus avoid-ing unnecessary procedures and toxicity[17].In addition,preop-erative therapy may be better tolerated than postoperative therapy[18],and a pathologic evaluation of the response to pre-operative treatment may offer important prognostic information [19].The Gastrointestinal Working Party of the Radiation Oncology Group(GIWP-ROG)of the European Organization for Research and Treatment of Cancer(EORTC)has committed itself to develop guidelines for target volume definition in neoadjuvant radiation of AC of the GEJ and the stomach.The current assessment of target and organ at risk volume definitions,of imaging modalities and of the planning and verification procedures can be regarded as a guide to a clinical quality assurance concept.Methods and materialsWe performed a systematic review(MEDLINE(http:// )search up to August2008)of all reported data concerning prescription,planning,treatment delivery as well as the location and frequency of local recurrences and lymph node involvement in AC of the GEJ and the stomach.The members of the GIWP-ROG of the EORTC reached a consensus based on this extensive literature review resulting in the following guidelines. ResultsGuidelines for neoadjuvant radiotherapy of adenocarcinomas of the gastroesophageal junction and the stomachDose prescription and fractionationThe regime consists of a total dose of45Gy in25daily fractions of1.8Gy onfive days a week.Dose prescription and recording has to comply with the recom-mendations of the ICRU50/62.Treatment delayA maximum overall treatment time of37days shall be aimedfor.Treatment imaging,patient positioning and immobilizationPlanning CT is mandatory and has to be performed before the initiation of any induction chemotherapy.The intravenous administration of contrast medium is recommended.The oral administration of positive or negative contrast media for the planning CT is not recommended,but supported for an addi-tional diagnostic CT.The slice-thickness must not be larger than3mm.In case of induction chemotherapy and more than10%weight loss,a second planning CT is necessary.Patients should be treated supine.Legs with knee support,arms lifted above the head.Patient immobilization with thermoplastic device or vacuum cushion is recommended.Treatment delivery techniqueA linear accelerator with3D-CRT or IMRT capability with energyof4–18MV should be used.The volume should be treated by only one treatment plan(with-out superposition of different plans).Treatment with opposed pairfields alone is not acceptable.Target volume definitionOnly one volume should be considered throughout radiotherapy and no cone-down or boost volume should be foreseen.The tumour site and extent should be defined by endoscopy, endoscopic ultra sound(EUS)and computed tomography(CT) prior to induction chemotherapy and assigned to one of the fol-lowing six locations:s tumours of the gastroesophageal junction type;I;II;III (Fig.1)or;s tumours of the proximal third of the stomach(with their tumour centre outside the gastroesophageal junction);tumours of the middle or distal third(Fig.2).Gross tumour volumes(GTV)have to be delineated for the pri-mary tumour(GTV tumour)as well as for the involved lymph nodes(GTV nodal).GTV tumour has to include the primary tumour and the perigastric tumour extension.The global clinical target volume(CTV global)will be obtained by the addition of the following structures(including the lymphatic spread ways in between these volumes):–CTV tumour;which will be obtained by adding a margin of1.5cm to GTVtumourFig.1.Adenocarcinoma of the gastroesophageal junction.Based on the anatomic location of the tumour centre three subtypes can be defined[10]:Type I tumours have their tumour centres more than1cm above the anatomical gastroesophageal junction;Type II tumours are the true carcinomas of the cardia and have their tumour centres located within1cm oral and2cm aboral of the anatomical gastroesophageal junction;Type III tumours have their tumour centre more than 2cm but not more than5cm below the anatomical gastroesophageal junction.O.Matzinger et al./Radiotherapy and Oncology92(2009)164–175165–CTV nodal ;which will be obtained by adding a margin of 0.5cm to GTV nodal–For GC only;a CTV gastric which will be defined asi.GC of the proximal third of the stomach:CTV gastric =con-tour of the stomach with exclusion of pylorus and antrum (a minimal margin of 5cm from the GTV has however to be respected).ii.GC of the middle third of the stomach:CTV gastric =contourof the stomach (from cardia to pylorus).iii.GC of the distal third of the stomach:CTV gastric =contourof the stomach with exclusion of cardia and fundus (a minimal margin of 5cm from the GTV has however to be respected).In case of infiltration of the pylorus or the duodenum,CTV has to be expanded along the duodenum with a margin of 3cm from the tumour.–The elective lymph node stations (CTV elective )corresponding to the specific tumour location as defined in Table 1and illus-trated in Figures 3–10.The CTV elective volume should be defined by a 5mm margin around the corresponding vessels. An Internal Target Volume (ITV)should be included in the treat-ment planning process as recommended by ICRU 62report [20]in order to take into account the target motion.A Planning Target Volume (PTV)should be defined according to the ICRU 50and 62report:For GEJ tumours–Individualized identification of the target volume motion has to be performed if possible.–If no facilities allowing the evaluation of the target volume motion are present,the minimal recommended 3-D margins to be added from the CTV to get the ITV are:1cm radial margin;1.5cm distal margin and 1cm proximal margin [21–24].–PTV will then be defined as the ITV-volume plus a 3-D margin of 5mm (except if the centre has defined its own measures of posi-tioning inaccuracy).For gastric tumours–Individualized identification of the target volume motion has to be performed if possible.–If no facilities allowing the evaluation of the target volume motion are present,the minimal recommended 3-D margins to be added from the CTV to get the ITV are:1.5cm to all directions [21].–PTV will then be defined as the ITV-volume plus a 3-D margin of 5mm (except if the centre has defined its own measures of positioning inaccuracy).All margins should be added in 3D.Organ at risk (OAR)volume definition and dose limitationThe complete volumes of the lungs,the liver,the kidneys and the heart have to be delineated.Spinal cord must be outlined along the whole volume interested by the beams plus 2cm above or below this volume.Whenever possible,without missing the PTV,attempts should be made to limit the dose to all organs-at-risk.The maximal spinal cord dose must not exceed a total dose of 45Gy.In case of combined modality treatment with oxaliplatin this dose should not exceed 40Gy [25–29].The combined lung volume receiving more than 20Gy has to be less than 20%(V20<20%).Furthermore the combined lung vol-ume receiving less than 5Gy should be higher than 2300cc.(<10%chance of postoperative pulmonary complication [30,31]). The whole heart must not have more than 30%exposed to a total dose of 40Gy and not more than 50%exposed to a total dose of 25Gy.At least 70%of one physiologically functioning kidney should receive a total dose of less than 20Gy (V20<70%).For the con-tralateral kidney the volume exposed to more than 20Gy has to be less than 30%(V20<30%)[32,33].s The glomerular filtration rate of each kidney has to be taken into account in case of suspicion of a decreased renal func-tion.Overall,not more than 50%of the combined functional renal volume should receive more than 20Gy.s Caution is requested if the treatment is combined with oxa-liplatin,as there are no reports of the effect of combined treatment of oxaliplatin and radiation on renal function and only scarce reports of renal failures following oxaliplatin delivery [34,35].The liver must not have more than 30%of its volume exposed to more than 30Gy (V30<30%)[36].Treatment planning3D treatment planning with inhomogeneity corrections should be performed.The use of DVH for planning is mandatory.The dose volume histograms (DVH)of all delineated volumes (target and OAR)have to be calculated using a calculation grid of 3mm maximum on an appropriate calculation mode using a high point density.Use of shielding blocks/MLC is mandatory.The coverage and homogeneity of the PTV should conform to ICRU 50/62criteria.The dose homogeneity within the volume has to be kept within À5%and +7%of the prescribed dose. The PTV should be encompassed by the 95%isodose-volume. Underdosage is only allowed if requested by the proximity of serial OAR.In this situation a maximum of 5%of the PTV volume should receive less than 95%of the prescribed dose.The ICRU ‘‘hot spot”(i.e.the dose outside of the PTV with a vol-ume of at least 1.8cc)should not exceed the prescription dose by more than7%.Fig.2.Three portions are defined by subdividing both lesser and greater curvatures into three equal lengths.Tumours of the upper (or proximal),middle,lower (or distal)third have their main tumour masses in the respective parts of the stomach.166EORTC guidelines for neoadjuvant radiation of gastroesophageal and stomach cancerTreatment verificationDaily patient set-up shall be performed using laser align-ment to reference marks on the skin of the patient.As a minimum requirement,an off-line set-up correction protocol must be in place that requires imaging at least once a week.It is highly advised to adhere to the adapted ‘‘shrinking action level”(SAL)or extended ‘‘no action level”(eNAL)off-line proto-cols as described in the literature [37,38].Daily on-line set-up verification and correction is also allowed but not mandatory.A non-daily on-line correction protocol is not allowed.The protocol can be based on bony anatomy.However,soft-tis-sue or marker based set-up corrections are to be preferred.If the total portal imaging dose is expected to exceed 2%(0.9Gy)of the prescribed dose,this should be taken into account during planning.DiscussionParameters of interest for radiotherapy planning include tradi-tionally the gross tumour volume (GTV),the clinical target volume (CTV)and the planning target volume (PTV).However,the Interna-tional Commission on Radiation Units and Measurements (ICRU)Report 50(1993)and ICRU Supplement to Report 62(1999)Fig.3.The classification of the lymph node stations of the stomach and the perigastric region according to the JGCA [58].O.Matzinger et al./Radiotherapy and Oncology 92(2009)164–175167168EORTC guidelines for neoadjuvant radiation of gastroesophageal and stomach cancerFig.4.Corresponding elective lymph node stations for tumours of the gastroesophageal junction.Type I:1right paracardial LN;2,left paracardial LN;7,LN along the left gastric artery;9,LN around the celiac artery;19,infradiaphragmatic LN;20,LN in the oesophageal hiatus of the diaphragm;110,paraoesophageal LN in the lower thorax;LN.111,supradiaphragmatic LN;112,posterior mediastinalFig.5.Corresponding elective lymph node stations for tumours of the gastroesophageal junction Type II:1,right paracardial LN;2,left paracardial LN;3,LN along the lesser curvature;4sa,LN along the short gastric vessels;7,LN along the left gastric artery;9,LN around the celiac artery;11p,LN along the proximal splenic artery;19, infradiaphragmatic LN;20,LN in the oesophageal hiatus of the diaphragm;110,paraoesophageal LN in the lower thorax;111,supradiaphragmatic LN.describe the current recommendation for incorporation of tumour motion into radiotherapy planning.Therefore the planning target volume (PTV)is defined as the internal target volume (ITV)plus the set-up margin.The ITV takes into account physiologic organ motion,in particular motion caused by respiration,to ensure adequate CTV coverage throughout the respiratory cycle.Variations in the CTV position and shape are ac-counted for by using the internal margin (IM)[20,39].Tumour imagingEndoscopic ultrasound (EUS),CT and PET are all generally able to visualize the GTV.However the apparent longitudinal extent and location may vary between the different modalities.CT of chest and abdomen and EUS has been regarded as the best modal-ity for staging GEJ and gastric tumours.More recently,the role of 18-fluorodeoxy-D -glucose positron emission tomography (FDG-PET)in staging and RT planning has been investigated.CT has a central role in the treatment volume definition as it is used for the RT dose calculation.EUS is a valuable addition in view of its accuracy in T and N staging [40,41]but it cannot be directly used for RT planning.Therefore,CT scan of the abdomen/thorax and EUS is mandatory for an exact preoperative tumour and node metastases staging [2,42].The role of PET in the delineation of the primary tumour re-mains uncertain [43].Key problems are the lack of studies using pathology as the reference and the lack of a standardized method-ology to determine the extent of the primary tumour [44].Both CT and PET have a poor sensitivity for detection of nodal involvement and should therefore not be used to exclude nodal volumes.On the other hand,PET-positive nodes outside the usual elective nodalvolume should be included in the target volume in view of the high specificity of PET for nodal disease,[45].In conclusion and at the present time,treatment volume selec-tion and delineation should be based on a combination of all avail-able imaging,with CT and EUS as mandatory and PET as recommended modalities [46].Target volume delineationThe lack of randomized,controlled studies to determine de-tails of radiation fields,resulted in the past in neoadjuvant radi-ation directed to the whole stomach and large lymph node areas [47].Pilot studies with radiation individualized for the tumour location and a limited lymph node volume were not pursued [48].The UICC TNM 6th ed.[49]classifies GEJ tumours as gastric can-cers,but in the past they were classified inconsistently as either oesophageal or gastric cancers.Most clinical trials recruited pa-tients with a mixture of histological types and anatomical loca-tions.ACs of the junction (defined as tumours infiltrating the GEJ and having their tumour centres within 5cm oral and aboral of the anatomical GEJ)have however clearly to be considered sepa-rately to the other tumours of the stomach or the oesophagus as their pathogenesis,pattern of spread as well as the surgical ap-proach differ considerably [9,10,12–16].The understanding that both location and histological type may influence the best treat-ment modality has led to increasing worldwide use of the ‘‘Siewert classification’’of AC of the GEJ [10](Fig.1).An individualized and standardized clinical treatment volume based on tumour location has to be defined in order to support a curative resection of gastroesophageal and GC.The reliabilityofFig.6.Corresponding elective lymph node stations for tumours of the gastroesophageal junction.Type III:1,right paracardial LN;2,left paracardial LN;3,LN along the lesser curvature 4sa LN along the short gastric vessels;7;LN along the left gastric artery;9,LN around the celiac artery;10,LN at the splenic hilum;11p,LN along the proximal splenic artery;11d,LN along the distal splenic artery;19,infradiaphragmatic LN;20,LN in the oesophageal hiatus of the diaphragm;110,paraoesophageal LN in the lower thorax;111,supradiaphragmatic LN.O.Matzinger et al./Radiotherapy and Oncology 92(2009)164–175169pretherapeutic imaging to obtain information about lymphatic disease is however still limited in carcinomas of the oesophageal junction and of the stomach [41,50,51,46].Therefore a preoper-ative clinical treatment volume has to be composed of the gross tumour volume and its potential extensions in the oesophageal and gastric wall,of the involved regional lymph nodes as well as of the draining lymph nodes areas [52–55].The proposed elective lymph node areas of the GEJ I,II and III are derived from the 6th edition of the TNM Classification of the UICC [49].Tumours of the gastroesophageal junction (Fig.1):s Type I,II,III.The Japanese literature extensively investigated the pattern of lymph node spread [56,57].They developed the concept of assign-ing tumours of the stomach to three anatomically defined tumour sites corresponding respectively to their different lymphatic spread patterns:Tumours of the stomach (Fig.2):s Proximal,middle and distal third.This grouping system is based on the results of studies of lym-phatic flow at various tumour sites,together with the observed survival associated with metastasis at each nodal station [58].The result of this extensive data is integrated in the 2nd English Edition of the Japanese Classification of Gastric Carcinoma of the Japanese Gastric Cancer Association (JGCA)[58].This distribution of lymph node involvement according to the location of the primary tumour has been validated by many other pathological studies [59,52,56,60,12–15,61,62].Gastric clinical target volumeThe usual CTV in gastric cancer has always included the entire stomach from cardia to pylorus [53,54,63].This volume definition was based on the consideration that gastric tumour position is dif-ficult to be assessed with certainty and to be sure not to have a geographical miss.In order to avoid unnecessary toxicity,and in the framework of modern 3-D planning,the definition of this large volume should however be reconsidered in order to avoid toxicity.Surgical series show that less than 5%of the patients have tumour cells more than 3cm from the macroscopic edge of the primary le-sion [64].We propose therefore to define:CTV stomach for proximal GC:stomach without pylorus or antrum.A minimal margin of 5cm from the GTV has however to be respected in order to have a comfortable security margin.CTV stomach for medial GC:entire stomach,including cardia and pylorus.CTV stomach for distal GC:stomach without cardia and fundus.A minimal margin of 5cm from the GTV has however to be respected.In case of infiltration of the pylorus or the duodenum,CTV has to be expanded along the duodenum with a margin of 3cm from the tumour.Target volume motionTumours of the GEJ exhibit a significant respiration-induced motion.Only a few studies on GEJ tumour motion have been published [24,21,23,65,22].Yaremko et al.studied 31distal oesophageal cancer patients using 4D-CT during free breathing with feedback guidance.CTV–ITV margins of 0.8cmradiallyFig.7.Corresponding elective lymph node stations for GC tumours of the proximal third with their tumour centre outside of the gastroesophageal junction:1,right paracardial LN;2,left paracardial LN;3,LN along the lesser curvature;4sa,LN along the short gastric vessels;4sb,LN along the left gastroepiploic vessels;7,LN along the left gastric artery;9,LN around the celiac artery;10,LN at the splenic hilum;11p,LN along the proximal splenic artery;11d,LN along the distal splenic artery;19,infradiaphragmatic LN.170EORTC guidelines for neoadjuvant radiation of gastroesophageal and stomach cancerFig.8.Corresponding elective lymph node stations for GC tumours of the middle third:1,right paracardial LN;2,left paracardial;LN;3,LN along the lesser curvature;4sa,LN along the short gastric vessels;4sb,LN along the left gastroepiploic vessels;4d,LN along the right gastroepiploic vessels;5,suprapyloric LN;6,Infrapyloric LN;7,LN along the left gastric artery;8a,LN along the common hepatic artery (anterosuperior group);8b,LN along the common hepatic artery (posterior group);9,LN around the celiac artery;10,LN at the splenic hilum;11p,LN along the proximal splenic artery;11d,LN along the distal splenic artery;18,LN along the inferior margin of the pancreas;19infradiaphragmaticLN.Fig.9.Corresponding elective lymph node stations for GC tumours of the distal third:3,LN along the lesser curvature;4d,LN along the right gastroepiploic vessels;5,suprapyloric LN;6,infrapyloric LN;7,LN along the left gastric artery;8a,LN along the common hepatic artery (anterosuperior group);8b,LN along the common hepatic artery (posterior group)9,LN around the celiac artery;11p,LN along the proximal splenic artery;12a,LN in the hepatoduodenal ligament (along the hepatic artery);12b,LN in the hepatoduodenal ligament (along the bile duct);12p,LN in the hepatoduodenal ligament (behind the portal vein);13,LN on the posterior surface of the pancreatic head;17,LN on the anterior surface of the pancreatic head;18,LN along the inferior margin of the pancreas.O.Matzinger et al./Radiotherapy and Oncology 92(2009)164–175171and 1.8cm axially were recommended when 4D-CT is not available for planning.Zhao et al.studied 25patients with oesophageal cancer near the GEJ.They used respiratory-corre-lated 4D-CT images.Their measured tumour mobility sug-gested the use of asymmetric margins: 1.0cm left,0.8cm right, 1.1cm anterior,0.6cm posterior, 1.0cm superior and 1.6cm inferior.Dieleman et al.[21]analysed the mobility for 29non-oesophageal malignancy patients during normal respiration using normal breathing 4D-CT images.They con-cluded that 9-mm lateral and 8-mm AP margins were needed for the section of oesophagus 2-cm above the GEJ.However,they did not evaluate the superior–inferior motion.Considering the above-mentioned data that are still sparse and that are still need to be confirmed by new studies,we propose to define in the meanwhile 1cm radial;1.5cm distal and 1cm prox-imal margins from CTV to ITV if no individualized identification of the target motion is available.GC target volume definition continues to be the subject of re-search because of considerable intrafractional stomach motion and remarkable interfractional variability of gastric distension in response to variations in stomach filling and respiratory motion as confirmed by two recent studies [66,67].Some centres advocate the use of respiratory gating devices to reduce intrafractional position variability.Daily cone-beam CT (im-age guided radiotherapy (IGRT))could also be useful to assess interfractional variability.However no standard procedure can be recommended based on evidence until now.We recommend therefore a minimal 3-D mar-gin of 1.5cm in all directions to be added from the CTV to the ITV [21]if the centres do not perform routinely respiratory gating or IGRT.ConclusionPreoperative radiochemotherapy is a promising development in the field of gastric and gastroesophageal tumours.The Gas-tro-Intestinal Working Party of the Radiation Oncology Group of the EORTC defined hereby a set of guidelines for preoperative irradiation of AC of the GEJ and the stomach.This consensus-based guideline should reduce inter-observer variability in tar-get volume delineation as well as standardize the planning and the radiotherapy delivery in the framework of future clini-cal trials.Therein,particular attention will be given to the pat-terns of recurrence to ensure the appropriateness of our guidelines.Table 1Elective lymph node stations corresponding to the different localization of GEJ and GT.Tumour localization Elective lymph node stations numbers and name GEJ type I 1Right paracardial LN 2Left paracardial LN(Figs.3,4and 10)7LN along the left gastric artery 9LN around the celiac artery 19Infradiaphragmatic LN20LN in the oesophageal hiatus of the diaphragm 110Paraoesophageal LN in the lower thorax 111Supradiaphragmatic LN 112Posterior mediastinal LN GEJ type II 1Right paracardial LN 2Left paracardial LN(Figs.3,5and 10)3LN along the lesser curvature 4sa LN along the short gastric vessels 7LN along the left gastric artery 9LN around the celiac artery11p LN along the proximal splenic artery 19Infradiaphragmatic LN20LN in the oesophageal hiatus of the diaphragm 110Paraoesophageal LN in the lower thorax 111Supradiaphragmatic LN GEJ type III 1Right paracardial LN 2Left paracardial LN(Figs.3,6and 10)3LN along the lesser curvature 4sa LN along the short gastric vessels 7LN along the left gastric artery 9LN around the celiac artery 10LN at the splenic hilum11p LN along the proximal splenic artery 11d LN along the distal splenic artery 19Infradiaphragmatic LN20LN in the oesophageal hiatus of the diaphragm 110Paraoesophageal LN in the lower thorax 111Supradiaphragmatic LN GC:proximal third 1Right paracardial LN 2Left paracardial LN(Figs.3,7and 10)3LN along the lesser curvature 4sa LN along the short gastric vessels4sb LN along the left gastroepiploic vessels 7LN along the left gastric artery 9LN around the celiac artery 10LN at the splenic hilum11p LN along the proximal splenic artery 11d LN along the distal splenic artery 19Infradiaphragmatic LN GC:middle third 1Right paracardial LN 2Left paracardial LN(Figs.3,8and 10)3LN along the lesser curvature 4sa LN along the short gastric vessels4sb LN along the left gastroepiploic vessels 4d LN along the right gastroepiploic vessels 5Suprapyloric LN 5Infrapyloric LN7LN along the left gastric artery8a LN along the common hepatic artery (Anterosuperior group)8b LN along the common hepatic artery (Posterior group)9LN around the celiac artery 10LN at the splenic hilum11p LN along the proximal splenic artery 11d LN along the distal splenic artery18LN along the inferior margin of the pancreas 19infradiaphragmatic LNGC:distal third 3LN along the lesser curvature4d LN along the right gastroepiploic vessels (Figs.3,9and 10)5Suprapyloric LN 6Infrapyloric LN7LN along the left gastric artery8a LN along the common hepatic artery (Anterosuperior group)8b LN along the common hepatic artery (Posterior group)9LN around the celiac artery11pLN along the proximal splenic arteryTable 1(continued)Tumour localizationElective lymph node stations numbers and name 12a LN in the hepatoduodenal ligament (along the hepatic artery)12b LN in the hepatoduodenal ligament (along the bile duct)12p LN in the hepatoduodenal ligament (behind the portal vein)13LN on the posterior surface of the pancreatic head17LN on the anterior surface of the pancreatic head18LN along the inferior margin of the pancreasRemark:The CTV elective volume should be defined by a 5mm margin around the corresponding vessels.The upper border of the CTV in GEJ tumours Type I and II is limited by a margin of 3cm from the cranial extension of the primary tumour [68].The upper border of the CTV in GEJ tumours type III is limited either by a margin of 3cm from the cranial extension of the primary tumour or by the superior end of the oesophageal hiatus as defined by planning CT [68].The most cranial of these two borders will define the upper border of the CTV and be delineated.172EORTC guidelines for neoadjuvant radiation of gastroesophageal and stomach cancer。