Diagnosis of Middle Cerebral Artery Stenosis by Transcranial Color-Coded Real-Time
- 格式:pdf
- 大小:718.39 KB
- 文档页数:4
椎动脉支架术后闭塞超声表现1例颈动脉、椎动脉(起始段)狭窄或闭塞性病变是导致前、后循环缺血性脑血管病的重要原因,支架置入术成为治疗颈动脉、椎动脉起始段动脉粥样硬化性狭窄或闭塞病变的重要手段之一。
随着对再狭窄影响因素研究的深入,残余狭窄对再狭窄发生率的影响也逐渐引起了学者们的关注,但相关文献报道较少,故需要针对颈动脉支架置入术(carotid artery stenting,CAS)及椎动脉支架置入术后残余狭窄对再狭窄影响的问题进行论述,以期引起相关学科医师重视对支架置入术的质量控制[1]。
当存在双侧椎动脉起始段严重病变时,术后支架置入侧椎动脉可立刻对未置入侧的血流发挥代偿作用。
但这种代偿作用同时也是发生支架内再狭窄的危险因素之一。
标签:部脑部血管超声;脑电;肌电;神经电生理1临床资料患者男,76岁。
左侧椎动脉支架术后7月。
术前超声表现:左侧椎动脉开口原始管径 5.1mm,残余管径 1.3mm,狭窄段血流速度显著增快,约270.0/92.1cm/s,频窗充填,伴涡流,血流声频粗糙,可闻及乐性杂音,椎间隙段有低流速低搏动性改变,血流速度约14.0/8.1cm/s。
超声提示:左侧椎动脉开口狭窄(70~99%)[2]。
10d后实行双侧椎动脉造影术,证实左侧椎动脉开口重度狭窄,并实施左侧椎动脉支架植入术。
于术后1d超声表现:左侧椎动脉开口可探及强回声的网状结构(支架),支架长约13.0mm,支架内径4.0mm,支架内血流速度89.6/24.3cm/s,椎间隙段血流频谱恢复正常。
超声提示:左侧椎动脉支架术后,支架内血流通畅。
术后1个月超声表现:支架内径明显变细,约1.5mm,支架内血流速度显著增快,约403.6/134.5cm/s,频窗充填,伴涡流,血流声频粗糙,可闻及乐性杂音,超声提示:左侧椎动脉支架内径明显变细,血流速度显著增快-考虑正常椎动脉支架术后再狭窄[3]。
重度狭窄组和闭塞组支架侧椎间隙段、颅内段的PSV、EDV均较正常组升高(P<0.05)[4]。
1内頸動脈:internal carotid artery1-①眼動脈:ophthalmic artery1-②後前交通動脈:posterior communicating artery1-③前脈絡動脈:anterior choroidal artery2-①脳梁周囲動脈:pericallosal artery2-②脳梁周縁動脈:callosomarginal artery2-③前頭眼窩動脈:frontoorbital artery2-④前頭極動脈:frontopolar artery2-⑤前内側前頭動脈:anterior internal frontal artery 2-⑥中内側前頭動脈:middle internal frontal artery2-⑦後内側前頭動脈:posterior internal frontal artery 2-⑧傍中心動脈:paracentral artery2-⑨上内側頭頂動脈:superior internal parietal artery1椎骨動脈:vertebral artery2脳底動脈:basilar artery3後下小脳動脈:posterior inferior cerebellar artery4前下小脳動脈:ontorior inferior cerebellar artery5上小脳動脈:superior cerebellar artery6後大脳動脈:posterior cerebellar artery7鳥距動脈:calcarine artery8頭頂後頭動脈:parietooccipital artery9後側頭動脈:posterior temporal artery1椎骨動脈:vertebral artery2脳底動脈:basilar artery3後下小脳動脈:posterior inferior cerebellar artery4前下小脳動脈:ontorior inferior cerebellar artery5上小脳動脈:superior cerebellar artery6後大脳動脈:posterior cerebellar artery7鳥距動脈:calcarine artery8頭頂後頭動脈:parietooccipital artery10視床穿通動脈:thalamoperforating artery11内側後脈絡動脈:medial posterior choroidal artery 12外側後脈絡動脈:lateral posterior choroidal artery 13後脳梁周囲動脈:posterior pericallsal artery14後交通動脈:posterior communicating artery15後大脳鎌動脈:posterior falx artery1外頸動脈:external carotid artery2上行咽頭動脈:ascending pharyngeal artery3上甲状腺動脈:superior thyroid artery4舌動脈:lingual artery5顔面動脈:facial artery6後頭動脈:occipital artery7顎動脈:internal maxillary artery8浅側頭動脈:superficial temporal artery9中硬膜動脈:middle meningeal artery10下歯槽動脈:inferior alveolar artery11副硬膜動脈:accessory meningeal artery1颈内动脉:internal carotid artery1-①眼动脉:ophthalmic artery2大脑前动脉:anterior cerebral artery3大脑中动脉:middle cerebral artery1颈内动脉:internal carotid artery1-①眼动脉:ophthalmic artery1-②后交通动脉:posterior communicating artery1-③脉络膜前动脉:anterior choroidal artery2-①胼周动脉:pericallosal artery2-②胼缘动脉:callosomarginal artery2-③额眶动脉:frontoorbital artery2-④额极动脉:frontopolar artery2-⑤额内前动脉(额叶前内侧动脉):anterior internal frontal artery 2-⑥额内中动脉(额叶中内侧动脉):middle internal frontal artery 2-⑦额内后动脉(额叶后内侧动脉):posterior internal frontal artery 2-⑧旁中央动脉:paracentral artery2-⑨顶内上动脉(楔前动脉):superior internal parietal artery1椎动脉:vertebral artery2基底动脉:basilar artery3小脑后下动脉:posterior inferior cerebellar artery4小脑前下动脉:ontorior inferior cerebellar artery5小脑上动脉:superior cerebellar artery6大脑后动脉:posterior cerebellar artery7距状沟动脉:calcarine artery8顶枕动脉:parietooccipital artery9颞后动脉:posterior temporal artery1椎动脉:vertebral artery2基底动脉:basilar artery3小脑后下动脉:posterior inferior cerebellar artery4小脑前下动脉:ontorior inferior cerebellar artery5小脑上动脉:superior cerebellar artery6大脑后动脉:posterior cerebellar artery7距状沟动脉:calcarine artery8顶枕动脉:parietooccipital artery10丘脑穿动脉:thalamoperforating artery11脉络膜后内侧动脉:medial posterior choroidal artery 12脉络膜后外侧动脉:lateral posterior choroidal artery 13后胼周动脉:posterior pericallsal artery14后交通动脉:posterior communicating artery15大脑镰后动脉:posterior falx artery1颈外动脉:external carotid artery2咽升动脉:ascending pharyngeal artery3甲状腺上动脉:superior thyroid artery4舌动脉:lingual artery5面动脉:facial artery6枕动脉:occipital artery7上颌动脉:internal maxillary artery8颞浅动脉:superficial temporal artery9脑膜中动脉:middle meningeal artery10下牙槽动脉:inferior alveolar artery11脑膜副动脉:accessory meningeal arter。

2019,35(6):510-513.[8] LI R J,ZHANG F Q.Three-dimensional DSA guidance reduces complications and enhances the safety during interventional treatment for patients with hepatocellular carcinoma[J].Journal of B.U.ON.: Official Journal of the Balkan Union of Oncology,2021,26(4):1373-1378.[9]刘新志,赵恒,罗谊,等.DSA 诊断及介入治疗缺血性脑卒中患者颈部血管狭窄的疗效及生存质量[J].昆明医科大学学报,2018,39(10):121-125.[10]李静伟,支兴龙,叶明,等.血管内介入栓塞治疗婴幼儿软脑膜动静脉瘘的效果分析[J].中国脑血管病杂志,2021,18(7):465-471.[11]彭方强,檀书斌,刘旻谛,等.西门子双大平板DSA 机在神经介入治疗中的应用[J].介入放射学杂志,2019,28(12):1215-1218.[12]周桂桃,龚昭惠,谈惠群,等.脑血管侧支循环评估在脑血管介入术后再狭窄及缺血性脑血管事件中的应用[J].海南医学,2018,29(18):2534-2537.[13]方锋.脑血管侧支循环建立程度与介入治疗脑动脉硬化狭窄患者预后的关系分析[J].实用医院临床杂志,2018,15(2):113-117.[14] JIAO S,GONG L,WU ZH B,et al.Assessment of the value of3D-DSA combined with neurointerventional thrombolysis in thetreatment of senile cerebrovascular occlusion.[J].Experimental and Therapeutic Medicine,2020,19(2):891-896.[15]林成,张强,朱安林,等.头颈部3D-CTA 与DSA 影像融合技术在神经介入手术中的初步应用[J].立体定向和功能性神经外科杂志,2018,31(2):97-102.[16]王相阁.数字减影血管造影在缺血性脑血管病患者介入治疗中的作用[J].中国实用神经疾病杂志,2018,21(21):2394-2398.[17]张宪,李彭,赵晖,等.数字减影血管造影对脑梗死患者颈部血管的诊断价值研究[J].中国医学装备,2020,17(2):75-77.[18] ZHANG F F,RAN Y C,ZHU M,et al.The use of pointwiseencoding time reduction with radial acquisition MRA to assess middle cerebral artery stenosis pre-and post-stent angioplasty: comparison with 3D time-of-flight MRA and DSA[J].Frontiers in Cardiovascular Medicine,2021,8:739332.[19]付华文,李光建.数字减影血管造影联合神经介入溶栓术治疗缺血性脑血管疾病临床效果观察[J].实用医院临床杂志,2019,16(6):178-182.[20]谢成仁.旋转数字减影血管造影三维重建在脑血管疾病诊断及鉴别中的应用价值[J].神经疾病与精神卫生,2019,19(10):960-963.(收稿日期:2023-02-08) (本文编辑:马娇)①厦门市第五医院 福建 厦门 361101钆特酸葡胺磁共振动态增强扫描鉴别肝脏局灶性病变性质的价值张锦松①【摘要】 目的:探讨钆特酸葡胺(Gd-DOTA)磁共振动态增强扫描(DCE-MRI)鉴别肝脏局灶性病变性质的价值。
经颅多普勒超声诊断大脑中动脉狭窄体会王芳;袁军;乌依罕【摘要】目的:探讨经颅多普勒(TCD)的血流动力学不同参数对大脑中动脉(MCA)狭窄的敏感性、特异性.方法:门诊收纳临床疑诊为MCA狭窄患者共96例,使用TCD检测双侧(MCA)、大脑前动脉(ACA)以及大脑后动脉(PCA)的收缩期峰值流速(PSA)、舒张末期流速(EDV),并进一步测量了MCA狭窄处,狭窄近、远端的收缩期峰值流速(PSVst,PSVpro,MFVst)以及狭窄段平均流速.通过分析数字减影血管造影(DSA)所显示的ACA、PCA脑膜支代偿情况,确定TCD对不同程度MCA狭窄的敏感性和特异性.结果:(1) 16例MCA中度狭窄患者均未见脑膜支代偿;30例重度狭窄患者中26例存在脑膜支代偿,其中ACA脑膜支代偿的患者为16例,PCA脑膜支代偿的患者为10例(P=-0.263);(2) MCA重度狭窄患者MCA的PSV值均高于中度狭窄者MCA的PSV(P<0.05).重度狭窄者患侧ACA、PCA的PSV、EDV均显著高于健侧ACA、PCA的PSV以及EDV(P<0.01);MCA中度狭窄患者双侧ACA、PCA的PSA、EDV差异均无统计学意义(P>0.05);(3)具有ACA、PCA脑膜支代偿患者的PSV、EDV均较无代偿患者的明显增快(P<0.01),PI值减小(P<0.05).结论:(1)TCD对于MCA狭窄具有肯定的诊断意义;(2)TCD检查所得ACA、PCA血流动力学改变对于MCA中、重度狭窄导致软脑膜支代偿性血流速度增高具有诊断价值.【期刊名称】《内蒙古中医药》【年(卷),期】2013(032)001【总页数】2页(P72-73)【关键词】经颅多普勒超声检查;TCD;大脑中动脉狭窄【作者】王芳;袁军;乌依罕【作者单位】内蒙古自治区人民医院 010017;内蒙古自治区人民医院 010017;内蒙古自治区人民医院 010017【正文语种】中文【中图分类】R445.1.2颅内动脉粥样硬化性狭窄占缺血性脑血管病的8%~10箛,大脑中动脉(MCA)是颅内动脉狭窄最易受累的血管,是引发缺血性脑血管病的重要原因之一。

子宫动脉㊁胎儿脐动脉和大脑中动脉血流频谱对妊娠高血压的价值郝晓英ꎬ高㊀冰ꎬ任㊀郁ꎬ万小梅四川省自贡市妇幼保健院超声科㊀四川㊀自贡㊀643000㊀㊀ʌ摘㊀要ɔ㊀目的㊀探讨子宫动脉㊁胎儿脐动脉(UA)及大脑中动脉(MCA)血流频谱对妊娠高血压综合征(PIH)的价值ꎮ方法㊀选取我院产检的孕妇219例ꎬ均行子宫动脉㊁胎儿脐动脉和大脑中动脉血流频谱检测ꎬ根据临床诊断将孕妇分为研究组(PIH孕妇)41例和对照组(正常妊娠孕妇)178例ꎮ比较子宫动脉㊁胎儿UA㊁MCA血流频谱的搏动指数(PI)㊁阻力指数(RI)㊁收缩期与舒张期流速比(S/D)对PIH的诊断价值ꎮ结果㊀研究组子宫动脉的PI㊁RI㊁S/D明显高于对照组ꎬ研究组的PI㊁RI㊁S/D㊁有V型缺口波阳性率明显高于对照组ꎬ差异有统计学意义ꎻROC曲线分析显示ꎬPI㊁RI㊁S/D㊁有V型缺口波阳性率诊断PIH的AUC分别为0.935㊁0.905㊁0.899㊁0.920ꎬ敏感度和特异度分别为:PI阳性率为92.7%㊁94.4%ꎬRI阳性率87.8%㊁93.3%ꎬS/D阳率为85.4%㊁94.4%ꎬ有V型缺口波阳性率为90.2%㊁93.8%ꎮ研究组UA的PI㊁RI㊁S/D明显高于对照组ꎬ研究组MCA㊁MCA/UA的PI㊁RI㊁S/D明显低于对照组ꎬ差异有统计学意义(P<0.05)ꎮ结论㊀采用超声检测子宫动脉㊁UA㊁MCA的血流频谱ꎬ可早期预测PIHꎬ为临床诊断和治疗提供参考ꎮʌ关键词ɔ㊀子宫动脉ꎻ脐动脉ꎻ大脑中动脉ꎻ血流频谱ꎻ妊娠高血压综合征中图分类号:R445.1ꎻR714.25㊀㊀㊀文献标识码:A㊀㊀㊀文章编号:1006 ̄9011(2020)08 ̄1470 ̄04Thevalueofuterinearteryꎬfetalumbilicalarteryandmiddlecerebralarterybloodflowspectruminthediagnosisofpregnancy ̄inducedhypertensionsyndromeHAOXiaoyingꎬGAOBingꎬRENYuꎬWANXiaomeiDepartmentofUltrasoundꎬZigongMaternalandChildHealthHospitalꎬZigong643000ꎬP.R.ChinaʌAbstractɔ㊀Objective㊀Toexplorethevalueofbloodflowspectrumofuterinearteryꎬfetalumbilicalartery(UA)andmiddlecerebralartery(MCA)inthediagnosisofpregnancy ̄inducedhypertensionsyndrome(PIH).Methods㊀Atotalof219pregnantwomenwhowereexaminedinourhospitalfromMay2017toFebruary2019wereselectedforuterinearteryꎬfetalumbilicalarteryꎬandmiddlecerebralarterybloodflowspectrumdetection.Pregnantwomenweredividedintostudygroups(PIHpregnantwomen)basedonclinicaldiagnosisꎬ(41cases)andthecontrolgroup(normalpregnantwomenꎬ178cases).Thediagnosticvalueofpul ̄sationindex(PI)ꎬresistanceindex(RI)ꎬandsystolicanddiastolicflowrate(S/D)ofuterinearteryꎬfetalUAꎬandMCAbloodflowspectrumwerecompared.Results㊀ThePIꎬRIꎬandS/Doftheuterinearteryinthestudygroupweresignificantlyhigherthanthoseinthecontrolgroup.ThePIꎬRIꎬS/DꎬandV ̄notchwavepositiveratesinthestudygroupweresignificantlyhigherthanthoseinthecontrolgroupꎬandthedifferenceswerestatisticallysignificant(P<0.05)ꎻROCcurveanalysisshowedthattheAUCforPIHdiagnosisofPIꎬRIꎬS/DꎬandV ̄notchwavepositiverateswere0.935ꎬ0.905ꎬ0.899ꎬand0.920ꎬrespectively.ThesensitivityandspecificitywerePIpositiverates.Thepositiverateswere92.7%ꎬ94.4%ꎬRIpositiverateswere87.8%ꎬ93.3%ꎬS/Dpositiverateswere85.4%ꎬ94.4%ꎬandV ̄notchwavepositiverateswere90.2%ꎬ93.8%.ThePIꎬRIꎬandS/DoftheUAinthestudygroupweresignificantlyhigherthanthoseofthecontrolgroupꎬandthePIꎬRIꎬandS/DoftheMCAandMCA/UAinthestudygroupweresignificantlylowerthanthoseofthecontrolgroupꎬandthedifferenceswerestatisticallysignifi ̄cant(P<0.05).ROCcurveanalysisshowedthattheAUCofPIꎬRIꎬandS/DforMCA/UAdiagnosisofPIHwere0.995ꎬ0 955ꎬand0.867ꎬrespectively.Thesensitivityandspecificitywere:PIwas100%ꎬ93.3%ꎬandRIwas90.2%ꎬ92.7%ꎬS/Dwas65.9%ꎬ90.4%.Conclusion㊀UltrasounddetectionofbloodflowspectrumofuterinearteriesꎬUAandMCAcanpredictPIHearlyandprovidereferenceforclinicaldiagnosisandtreatment.ʌKeywordsɔ㊀UterinearteryꎻUmbilicalarteryꎻMiddlecerebralarteryꎻBloodflowspectrumꎻPregnancy ̄inducedhypertensionsyndrome作者简介:郝晓英(1979 ̄)ꎬ女ꎬ四川自贡人ꎬ毕业于泸州医学院ꎬ本科学历ꎬ主治医师ꎬ主要从事胎儿超声影像诊断工作㊀㊀妊娠高血压综合征(pregnancyinducedhyper ̄tensionꎬPIH)是指在妊娠期特有的疾病[1]ꎬPIH孕0741妇胎盘绒毛血管痉挛㊁梗塞㊁水肿ꎬ使绒毛血管狭窄ꎬ可导致子宫动脉阻力升高ꎬ使子宫 ̄胎盘循环阻力增加ꎬ脐带及胎儿各脏器血流量下降ꎬ从而增加中央动脉阻力ꎬ最终使血压升高[2 ̄3]ꎮ采用彩色多普勒诊断仪检测的子宫动脉㊁胎儿脐动脉(umbilicalarteryꎬUA)和大脑中动脉(middlecerebralarteryꎬMCA)血流频谱ꎬ可客观㊁直接反应血流阻力ꎮ本文以PIH孕妇和正常孕妇作为研究ꎬ分析子宫动脉㊁胎儿UA㊁MCA血流频谱的搏动指数(pulsatilityindexꎬPI)㊁阻力指数(resistanceindexꎬRI)㊁收缩期与舒张期流速比(systolictodiastolicvelocityratioꎬS/D)对PIH的诊断价值ꎮ1㊀资料与方法1.1㊀一般资料选取2017年5月~2019年2月在我院产检的孕妇219例ꎬ根据临床诊断将孕妇分为研究组(PIH孕妇)41例和对照组(正常妊娠孕妇)178例ꎮ研究组:年龄17~39岁ꎬ平均年龄28岁ꎬ孕周早孕期1例ꎬ中孕期26例ꎬ晚孕期14例ꎮ对照组:年龄26~38岁ꎬ平均年龄32岁ꎬ孕周早孕期2例ꎬ中孕期113例ꎬ晚孕期63例ꎮ比较两组的年龄㊁孕周等各项资料ꎬ差异无统计学意义(P>0.05)ꎬ有研究比较的价值ꎮ1.2㊀检查方法采用GE ̄8和Philips ̄Q5彩色多普勒诊断仪ꎬ选择腹部探头ꎬ频率2.5~5MHzꎬ选择胎儿中晚孕检测模式ꎮ子宫动脉检测:孕妇平卧平静呼吸ꎬ在子宫宫颈和宫体交界处进行子宫动脉的频谱多普勒检测ꎬ取样时使血管长轴与声束方向平行或减小角度ꎮ探头置于子宫下段肌壁外侧缘ꎬ启动CDFI找到髂外血管和子宫动脉的交叉ꎬ取样容积置于相交点远端1cm处子宫动脉上ꎬ角度小于30ʎꎬ取样容积大小约等于血管的宽度ꎮ获得连续性稳定满意的多普勒频谱进行测量ꎮ正常子宫动脉频谱(图1)ꎮ胎儿UA检测:选择脐带游离段ꎬ超声声束尽可能的平行于血管ꎬ避开胎儿呼吸样运动时进行测量ꎬ选取平稳规则的频谱波形进行测量记录分析ꎬUA频谱(图2)ꎮ胎儿MCA检测:选择靠近探头一侧的大脑中动脉检测ꎬ将多普勒取样门放在大脑中动脉与颈内动脉分支处ꎬ保持超声束和血管长轴之间角度为0ꎮ在胎儿平静状态下检测ꎬ取频谱波形平稳规则进行测量分析ꎬ正常MCA频谱(图3)ꎮ1.3㊀观察指标比较两组子宫动脉㊁UA㊁MCA㊁MCA/UA的PI㊁RI㊁S/Dꎬ以及子宫动脉的PI㊁RI㊁S/D㊁有V型缺口波阳性率ꎬ并采用ROC曲线分析子宫动脉的PI㊁RI㊁S/D㊁有V型缺口波阳性率ꎬMCA/UA的PI㊁RI㊁S/D的诊断价值ꎮ1.4㊀统计学方法所有数据均采用SPSS22.0软件处理分析ꎬ计量资料符合正态分布ꎬ以均数ʃ标准差( xʃs)表示ꎬ血流频谱PI㊁RI㊁S/D比较采用独立样本t检验ꎮ诊断价值评估采用ROC曲线分析ꎬ曲线下面积(ar ̄eaundercurveꎬAUC)<0.5时不具诊断价值ꎬAUC为0.7~0.9则诊断准确性较好ꎬ>0.9时诊断准确性高ꎮ以P<0.05为差异有统计学意义ꎮ2㊀结果2.1㊀子宫动脉血流频谱相关参数及对PIH的诊断价值研究组子宫动脉的PI㊁RI㊁S/D与对照组比较明显较高ꎬ研究组的PI阳性率㊁RI阳性率㊁S/D阳性率㊁有V型缺口波阳性率与对照组比较明显较高ꎬ差异有统计学意义(P<0.05)ꎬ见表1ꎮROC曲线分析显示ꎬ子宫动脉的PI㊁RI㊁S/D㊁有V型缺口波阳性率诊断PIH的AUC分别为0.935㊁0.905㊁0 899㊁0.920ꎬ敏感度和特异度分别为:PI阳性率为92.7%㊁94.4%ꎬRI阳性率87.8%㊁93.3%ꎬS/D阳性率为85.4%㊁94.4%ꎬ有V型缺口波阳性率为90 2%㊁93.8%ꎮ表1㊀两组子宫动脉血流频谱相关参数及对PIH的诊断价值比较 xʃsꎻn(%)组别例数PIRIS/DPI阳性率RI阳性率S/D阳性率有V型缺口波阳性率研究组411.13ʃ0.370.57ʃ0.172.63ʃ0.4738(92.68)36(87.8)35(85.37)37(90.24)对照组1780.77ʃ0.110.45ʃ0.172.10ʃ0.2510(5.62)12(6.74)10(5.62)11(6.18)t值11.0924.07510.104147.604127.956129.815137.604P值0.0010.0010.001<0.001<0.001<0.001<0.0011741表2㊀两组UA㊁MCA㊁MCA/UA血流频谱比较( xʃs)组别例数UAPIRIS/DMCAPIRIS/DMCA/UAPIRIS/D研究组411.23ʃ0.170.77ʃ0.112.97ʃ0.251.45ʃ0.041.11ʃ0.183.24ʃ0.191.31ʃ0.061.35ʃ0.181.09ʃ0.23对照组1780.93ʃ0.130.55ʃ0.152.15ʃ0.311.58ʃ0.031.39ʃ0.264.06ʃ0.481.59ʃ0.081.89ʃ0.251.75ʃ0.49t值12.5278.85215.78719.5676.53810.73121.07213.0628.403P值0.0010.0010.0010.0010.0010.0010.0010.0010.001图1Aꎬ1B㊀正常左右侧子宫动脉频谱(28岁孕28w)㊀图2㊀UA频谱ꎮ图2A正常频谱ꎮ图2B异常频谱ꎬ舒张期频谱消失㊀图3㊀正常MCA频谱㊀图4㊀子宫动脉PI㊁RI㊁S/D㊁有V型缺口波阳性率诊断PIH的ROC曲线㊀图5㊀MCA/UA的PI㊁RI㊁S/D㊁有V型缺口波阳性率诊断PIH的ROC曲线2.2㊀UA㊁MCA㊁MCA/UA血流频谱研究组UA的PI㊁RI㊁S/D与对照组比较明显较高ꎬ研究组MCA㊁MCA/UA的PI㊁RI㊁S/D与对照组比较明显较低ꎬ差异有统计学意义(P<0.05)ꎬ见表2ꎮROC曲线分析显示ꎬMCA/UA的PI㊁RI㊁S/D诊断PIH的AUC分别为0.995㊁0.955㊁0.867ꎬ敏感度和特异度分别为:PI为100%㊁93.3%ꎬRI为90 2%㊁92 7%ꎬS/D为65.9%㊁90.4%(图4ꎬ5)ꎮ3㊀讨论㊀㊀超声检查是目前产科首选的影像检查方法ꎬ应用彩色多普勒检测手段对孕高症患者多血管检测是可靠可重复性无创性的检测方法ꎬ可直接准确的判断胎儿血流循环的特点及变化ꎬ监测胎盘功能和胎儿宫内状况ꎬ可以早期发现胎儿宫内低氧状态ꎬ指导临床对监测中有异常指标的孕妇进行高危管理和随访复查ꎬ做好预防措施和发生预案ꎬ在危及孕妇和胎儿时紧急采取适当的救治措施ꎮPIH在妊娠20周后临床症状常表现为水肿㊁尿蛋白㊁高血压ꎬ随着病情的发展易发生子痫ꎬ对母婴结局均造成不良影响ꎮ多数研究表明ꎬPIH的基本病理改变为血液浓缩㊁全身小动脉痉挛型收缩㊁血容量减少ꎬ对肝脏㊁心脏㊁脑部㊁血液供应造成不同程度的损伤ꎬ从而影响胎儿发育和母体健康[4 ̄6]ꎮPIH前期还表现出子宫动脉血流动力学异常ꎬ从而影响对胎儿氧气㊁营养物质等的输送ꎬ严重时可导致胎儿窒息[7 ̄8]ꎮ在非妊娠期和妊娠早期ꎬ子宫动脉血流频谱呈现高阻力状态ꎬ舒张早期伴有V型切迹[9]ꎮ随着孕周的增加子宫动脉管腔增粗㊁增大ꎬ血液供应增多ꎬ血流频谱阻力逐渐降低ꎬ舒张早期V型切迹逐渐变浅或消失ꎬ使子宫动脉血流频谱逐渐变为低阻力状态[10]ꎮ当发生PIH病变时ꎬ子宫螺旋动脉出现重塑障碍ꎬ使滋养细胞入侵受阻ꎬ导致螺旋动脉得不到充分扩张ꎬ增加了子宫 ̄胎盘 ̄胎儿的循环阻力[11 ̄12]ꎮ本文研究中ꎬ研究组子宫动脉的PI㊁RI㊁S/D明显高于对照组ꎬ研究组的PI㊁RI㊁S/D㊁有V型缺口波阳性率明显高于对照组ꎬ可见PIH孕妇子宫动脉血流频谱会出现异常ꎬ呈高阻力状态ꎮ进一步的ROC曲线分析显示ꎬPI㊁RI㊁S/D㊁有V型缺口波阳性率诊断PIH的AUC分别为0.935㊁0.905㊁0.899㊁27410 920ꎬ敏感度和特异度分别为:PI阳性率为92.7%㊁94.4%ꎬRI阳性率87.8%㊁93.3%ꎬS/D阳性率为85 4%㊁94.4%ꎬ有V型缺口波阳性率为90.2%㊁93 8%ꎮ结果表明PI㊁RI㊁S/D㊁有V型缺口波阳性率对PIH均具有诊断价值ꎬ其中PI的诊断价值最高ꎮ正常妊娠期RI随着孕周的增加而降低ꎬ舒张末期血流增高ꎬ当出现胎盘发育不全时ꎬ胎盘内血管血流阻力和UA血流阻力增高ꎬ表现为多普勒超声波形异常如舒张末期血流消失或反向ꎬ多普勒血流参数异常ꎬ如PI㊁RI㊁S/D增高[13 ̄14]ꎮ随着孕周的增长ꎬMCA血流阻力降低ꎬ血流速度增高ꎬ在胎儿出现缺氧和贫血时ꎬMCA血流阻力降低ꎬ出现脑保护效应ꎬ这一生理改变可通过多普勒超声检测表现为收缩期峰速及舒张末期血流速度增高ꎬPI㊁RI㊁S/D比值均降低ꎮ本文中ꎬ研究组UA的PI㊁RI㊁S/D明显高于对照组ꎬ研究组MCA㊁MCA/UA的PI㊁RI㊁S/D明显低于对照组ꎬ可见PIH孕妇UA㊁MCA血流频谱均会出现异常ꎬUA呈高阻力状态ꎬMCA呈低阻力状态ꎮ进一步的ROC曲线分析显示ꎬMCA/UA的PI㊁RI㊁S/D诊断PIH的AUC分别为0.995㊁0.955㊁0 867ꎬ敏感度和特异度分别为:PI为100%㊁93.3%ꎬRI为90.2%㊁92.7%ꎬS/D为65.9%㊁90.4%ꎮ结果表明MCA/UA的PI㊁RI㊁S/D对PIH均具有诊断价值ꎬ其中PI的诊断价值最高ꎮ综上所述ꎬ采用超声检测子宫动脉㊁UA㊁MCA的血流频谱ꎬ可早期预测PIHꎬ为临床诊断和治疗提供参考ꎮ本文的不足在于样本数量较小ꎬ有一定的局限性ꎬ今后有待于进一步增加样本数量ꎬ使其更具广泛性和适用性ꎮ参考文献:[1]沈银ꎬ黎萍.妊娠高血压综合征患者肾脏三维超声参数与血管内皮功能的相关分析[J].医学研究杂志ꎬ2019ꎬ48(4):100 ̄103.[2]刘畅ꎬ刘庆ꎬ李红艳ꎬ等.腰硬联合麻醉在PIH产妇剖宫产术中的应用及其对血流动力学和血液流变学的影响[J].山东医药ꎬ2019ꎬ59(16):79 ̄81.[3]房振亚ꎬ张美华.妊娠高血压综合征患者免疫功能与内分泌相关性分析[J].国际免疫学杂志ꎬ2018ꎬ41(3):274 ̄278. [4]SharmaRꎬMagoonRꎬChoudharyRꎬetal.Anaesthesiaforemer ̄gencycaesareansectioninamorbidlyobeseachondroplasticpa ̄tientwithPIH:feasibilityofNeuraxialanaesthesia[J].2017ꎬ61(1):77.[5]张蕊ꎬ黄丹萍ꎬ刘晓芳ꎬ等.M型血流传播速度评价妊娠高血压孕妇的胎儿心室舒张功能的价值[J].山西医药杂志ꎬ2018ꎬ47(13):1502 ̄1504.[6]徐蕙ꎬ朱璇.妊娠期血脂变化对妊娠高血压综合征的影响研究[J].中国继续医学教育ꎬ2017ꎬ9(24):164 ̄166. [7]EswarappaMꎬRakeshMꎬSonikaPꎬetal.Spectrumofrenalin ̄juryinpregnancy ̄inducedhypertension:experiencefromasinglecenterinIndia[J].SaudiJournalofKidneyDiseasesandTrans ̄plantation:AnOfficialpublicationoftheSaudiCenterforOrganTransplantationꎬSaudiArabiaꎬ2017ꎬ28(2):279 ̄284. [8]陈志伟ꎬ阳建军.超声检测母体子宫动脉及胎儿脐动脉血流参数对妊娠期高血压的诊疗价值[J].中国计划生育学杂志ꎬ201ꎬ26(6):517 ̄519.[9]罗晓婷ꎬ晁玥ꎬ尚小轶ꎬ等.孕早㊁中㊁晚期子宫动脉频谱对预测妊娠高血压的价值[J].贵州医药ꎬ2019ꎬ43(7):418 ̄421. [10]宫婷ꎬ潘艳艳.孕11~13+6周子宫动脉频谱与不明原因胎儿宫内生长受限相关性研究[J].陕西医学杂志ꎬ2019ꎬ48(8):1049 ̄1051.[11]BanooSꎬMakhdoomiTAꎬMirSꎬetal.Incidenceofhelpsyn ̄dromeinseverepregnancyinducedhypertensionanditsimpactonmaternalandfetaloutcome[J].2017ꎬ14(3):443 ̄450. [12]徐欣然ꎬ王妍平ꎬ崔洪艳.胎盘外泌体在子宫螺旋动脉重铸不全相关妊娠并发症中的作用[J].国际妇产科学杂志ꎬ2019ꎬ46(3):288 ̄292.[13]韩秋云.马新武.彩超诊断妊娠高血压综合征的临床应用价值[J].医学影像学杂志ꎬ2004ꎬ24(8):660 ̄660.[14]王立平ꎬ马新武ꎬ骆瑾.彩色多普勒超声测量脐动脉血流㊁胎儿四项指标预测胎儿生长受限[J].医学影像学杂志ꎬ2006ꎬ16(6):648 ̄649.(收稿日期:2019 ̄12 ̄13)3741。

经颅多普勒在颈内动脉颅外段重度狭窄或闭塞中的诊断价值刘菊华(高州市人民医院神经电生理室,广东525200)扌!要:目的:探讨经颅多普勒超声(TCD)在颈内动脉颅外段(ICAex)重度狭窄或闭塞中的诊断价值%方法:选取2020年3月-2020年9月我院经过数字减影血管造影检查确诊患有单侧ICAex重度狭窄或闭塞的60例患者作为观察组,另外选取同期经检查证实ICAex无明显病变的60例健康人员作为对照组0两组均行TCD检查%结果:TCD检查结果显示:对照组双侧MCA、ACA、PCA血流速度相近(P>0.05);频谱形态陡直,频窗明显&PI相近;双侧OA血流呈正向频移,频谱形态为外周血管高阻力波%观察组患侧MCA及ACA血流速度明显降低,健侧(MCA)、ACA、PCA的PI均高于患侧(P<0.05);前交通都开放患侧ACA血流方向逆转&MCA及ACA频谱呈低平圆钝状;眼动脉侧支开放患侧OA血流方向逆转,频谱形态颅内化,呈低搏动性改变%观察组和对照组健侧、患侧MAC、ACA、PCA的PSV和PI比较均有统计学意义(P<0.05)%TCD诊断ICAex重度狭窄的敏感性为85.71%,特异性为90.91%,阳性预测值为97.67%,阴性预测值为58.82%&有效性为86.67%;诊断ICAex闭塞的敏感性为90.91%,特异性为87.76%,阳性预测值为62.50%,阴性预测值为97.73%,有效性为88.33%%结论:TCD在ICAex重度狭窄或闭塞中的诊断价值较高%关键词:经颅多普勒;颈内动脉颅外段重度狭窄或闭塞;诊断;临床研究中图分类号:R445.1;R543.4文献标识码:B D0I:10.3969/j.issn.1001-0270.2021.02.10The Diagnostic Value of Transcranial Doppler in Severe Stenosis or Occlusion of theExtracranial Segment of Internal Carotid ArteryLIU Ju-hua(Department of Neurophysiology,The People's Hospital of Gaozhou,Guangdong525200,China) Abstract:Objective:To explore the diagnostic value of TCD in severe ICAex stenosis or occlusion.Methods:Select60patients diagnosed with severe unilateral ICAex stenosis or occlusion in our hospital from March2020to September2020as the observation group.In addition,60healthy people who had no obvious lesions in ICAex during the same period were selected as the control group. Both groups were performed TCD check.Results:TCD examination results showed that the blood flow velocities of bilateral MCA,ACA,and PCA in the control group were similar(P>0.05);the spectrum shape was steep,the frequency window was obvious,and the bandwidth was similar;the blood flow of bilateral OA showed a positive frequency shift.The frequency spectrum is a high resistance wave of peripheral blood vessels.The blood flow velocity of MCA and ACA on the affected side of the observation group was significantly reduced,and the PI of MAC,ACA and PCA on the unaffected side were higher than those of the affected side(P<0.05);The front traffic is open to reverse the direction of收稿日期:2021-02-07the ACA blood flow on the affected side,and the MCA and ACA spectrum are low,flat and round;The collateral branches of the ophthalmic artery were open to reverse the direction of the blood flow of the affected side OA,the blood flow speed increased,and the spectral shape was intracranial,showing low-pulsation changes.The PSV and PI of the healthy side and the affected side of the observation group and the control group were statistically significant(P<0.05).The sensitivity of TCD in diagnosing ICAex severe stenosis was85.71%,the specificity was90.91%,the positive predictive value was97.67%,the negative predictive value was58.82%,and the validity was86.67%;The sensitivity for diagnosing ICAex occlusion was90.91%,the specificity was87.76%,the positive predictive value was62.50%, the negative predictive value was97.73%,and the validity was88.33%.Conclusion:TCD has a higher diagnostic value for severe ICAex stenosis or occlusion.Key words:Transcranial Doppler;severe stenosis or occlusion of the extracranial segment of the internal carotid artery;diagnosis;clinical research颈内动脉颅外段(Extracranial internal carotid artery,ICAex)重度狭窄或闭塞是缺血性脑卒中发生的重要病因,其当前防治措施主要有控制危险因素、药物治疗以及颈动脉内膜剥脱术、颈动脉支架植入术等治疗方式%1-3&'因此,临床上对于颈动脉狭窄程度及部位的准确判断对脑卒中病因正确诊断具有非常重要的意义⑷。
回旋支医学缩写回旋支医学缩写是指在医学领域中常用的回旋支相关的缩写词。
回旋支是人体中的一个重要器官,对于人体的功能和健康起着至关重要的作用。
下面将介绍一些常见的回旋支医学缩写及其含义。
1. MCA:Middle Cerebral Artery(大脑中动脉)大脑中动脉是人体大脑中的一支主要动脉,负责供应大脑的侧面区域。
当大脑中动脉发生狭窄或者阻塞时,可能导致中风等严重后果。
2. ACA:Anterior Cerebral Artery(大脑前动脉)大脑前动脉是人体大脑中的一支主要动脉,负责供应大脑的前部区域。
当大脑前动脉发生狭窄或者阻塞时,可能导致认知功能障碍等问题。
3. PCA:Posterior Cerebral Artery(大脑后动脉)大脑后动脉是人体大脑中的一支主要动脉,负责供应大脑的后部区域。
当大脑后动脉发生狭窄或者阻塞时,可能导致视力问题、记忆力减退等症状。
4. BA:Basilar Artery(基底动脉)基底动脉是人体大脑中的一条主要动脉,负责供应脑干和大脑的后部。
基底动脉供应的区域涉及到许多重要的脑功能,当基底动脉发生问题时,可能导致严重的神经系统疾病。
5. SAH:Subarachnoid Hemorrhage(蛛网膜下腔出血)蛛网膜下腔出血是指动脉破裂导致血液进入脑室和蛛网膜下腔的一种情况。
这种出血常常是突然发生的,症状严重,可能导致昏迷、颅内压增高等危险情况。
6. TIA:Transient Ischemic Attack(短暂性脑缺血发作)短暂性脑缺血发作是指脑血液供应暂时中断导致的短暂性症状,一般持续时间较短,通常在几分钟到一小时之间。
短暂性脑缺血发作是中风的前兆,需要及时识别和处理。
7. ICA:Internal Carotid Artery(颈内动脉)颈内动脉是供应大脑血液的重要动脉之一,负责向大脑提供大部分血液。
当颈内动脉受损时,可能导致中风等严重后果。
8. CVA:Cerebrovascular Accident(脑血管意外)脑血管意外是指脑血管发生病变或者损伤导致的突发事件,包括中风、脑出血等。
Time: 120 minsDirection: There is only one correct answer from the answer list. Choose the correct answer and blacken the corresponding letter on your answer sheet with your pen or pencil.1. Transient ischemic attack (TIA) in general does not exceed ( B ) A. 30 minutes B. 60 minutes C. 2 hours D. 3 hours2. A patient is cerebral infarction with the language barrier, characterized by could not understand what is said to him. His spontaneous speech is fluent. What is kind of aphasia in this patient? ( B )A. Broca ’s aphasiaB. Wernicke ’s aphasiaC. conduction aphasiaD. global aphasia3. In general, epilepsy patients could consider to reduce or stop the antiepileptic drugs (AEDs) in any of the following situations: ( C )A. Seizure stops after 6 monthsB. takes drugs after 2 yearsC. seizure stops after 4 yearsD. all above is not4. The cause of subarachnoid hemorrhage can be ( B )A. AmyloidosisB. aneurysmC. arterial thrombosisD. viral encephalitis5. The main cause of cerebral hemorrhage is ( A )A. High blood pressureB. pneumoniaC. diabetesD. coronary heart disease6. Female, 65 years old, suddenly coma for 3 hours. The head CT shows the low density shadow in the right frontal cortex. The most likely diagnosis is ( C ) A. s yncope B.cerebral hemorrhage C.cerebral embolism D. hypertensive encephalopathy7. The most accurate diagnosis of intracerebral hemorrhage is based on ( C )A. over 60 years of ageB. hemiplegiaC. sudden hemiplegia, and head CT see high density near the basal gangliaD.meningeal irritationS t u d e n t N o .: N a m e : A d m i s s i o n Y e a r (C l a s s ): M a j o r :8.If the lesion can cause the right face palsy, and left limbs weakness, then it locate in the ( B )A.right mesencephalonB. right ponsC. left mesencephalonD. left pons9.Which of the following test is not associated with myasthenia gravis? ( D )A.Jolly testB. Tensilon testC. Neostigmine testD. Romberg test10.Male, 25 years old, right ptosis, weakness of four limbs, AChR(+), diagnosis with myasthenia gravis. Which of the following treatment is not correct? ( A )A.AspirinB. corticosteroidsC. acetylcholinesterase inhibitorsD. thymectomy11.Patients with global aphasia, his blood vessel which is most likely to block? ( C )A.anterior cerebral arteryB. anterior spinal arteryC. middle cerebral arteryD. posterior cerebral artery12.Which of the following is not part of the brain stem? ( A )A.CerebellumB. medulla oblongataC. ponsD. mesencephalon13.Male, 50 years old, right ptosis, dilated pupil, The most likely diagnosis is ( B )A.Myasthenia gravisB. oculomotor nerve impairedC. abducent nerve impairedD. facial nerve impaired14.Which of the following symptoms could not present in the cerebellar lesions. ( C )A.Intention tremorB. cerebellar ataxiaC. weakness of limbsD. nystagmus15.Which of the following is not the disturbance of the level of consciousness? ( B )A.SomnolenceB. confusionC. stuporD. coma16.Male, 65 years old, a history of hypertension for 3 years, now has a sudden of speech disorder, a skewed corner of the mouth, and left limbs movement disorder for 3 days. Which of the following tests do you think is most appropriate? ( D )A. Lumbar puncture CSF examinationB. Cerebral angiographyC. EEG examinationD. head CT scanCase: male, 10 years old, Sudden loss of consciousness, twitching of extremities, foaming in the mouth, stopping convulsions after 3 minutes.17.The most likely diagnosis is ( C )A.StrokeB. migraineC. epilepsyD. TIA18.Which of the following is the most helpful for diagnosis? ( C )A.Head CTB. head MRIC. ElectroencephalogramD. Lumbar puncture CSF examinationCase: female, 45 years old, sudden weakness of right upper and lower limbs, no consciousness disturbance. The attack occurred 5 times in total, and the attack duration was about 20 minutes.19.The most likely diagnosis is ( D )A.EpilepsyB. cerebral embolismC. vertebrobasilar system TIAD. internal carotid artery system TIA20.The lesions are most likely at ( B )A.basilar artery blood supply areaB. left middle cerebral artery blood supply areaC. right middle cerebral artery blood supply areaD. left anterior cerebral artery blood supply are21.To confirm the etiology, which test is preferred? ( D )A.Head CTB. blood lipids examinationC. blood glucose examinationD. cardiac B ultrasoundCase: female, 25 years old, bilateral peripheral facial paralysis, difficulty swallowing, flaccid paralysis of the extremities.22.The most likely diagnosis is ( A )A.GBSB. myasthenia gravisC. facial neuritisD. Acute myelitis23.What is the feature about this disease? ( A )A.Increased CSF albumin with absence of cellular reactionB. AChR-Ab (+)C. Electromyography suggests facial nerve conduction disordersD. MRI suggests spinal cord thickeningCase: male, 20 years old, right ptosis, respiratory failure, Jolly test is positive.24.The most likely diagnosis is ( B )A.GBSB. myasthenia gravisC. oculomotor nerve impairedD. stoke in midbrain25.Which drugs is appropriate? ( C )A.Vitamins BB. aspirinC. pyridostigmineD. potassium chlorideII. Explanation of Nouns (19 scores):26.What is the definition of status epilepticus? (5 scores)Answers: Status epilepticus is a clinical or electrical seizure lasting at least 30 minutes, or aseries of seizures without complete recovery over the same period of time.27.What is the coordination test consist of? (5 scores)Answers: finger-to-nose, rapid alternating movements, rebound, Heel-knee-shin, Romberg’s test.28.What is the motor symptoms of Parkinson’s disease? (4 scores)Answers: static tremor, rigidity, bradykinesia, postural instability. ( tremor at rest, rigidity, bradykinesia-hypokinesia, flexed posture, loss of postural reflexes, freezing phenomenon.)29.What is the definition of migraine? (5 scores)Answers: migraine is a chronic neurovascular disorder characterized by a recurrent, unilateral, and throbbing headache which usually lasts 4-72 hours, associated with nausea and vomiting. It is often aggravated by light (photophobia) and voice (phonophobia), and alleviated by rest and sleep.III. Short-answer Questions (31 scores):30.Please describe the grades muscle strength. (6 scores)Answers: it is total 6 grades. Grade 0 means no muscular contraction detected; grade 1 means a barely detectable trace of contraction; grade2 means active movement with gravity eliminated; grade 3 means active movement against gravity; grade 4 means active movement against gravity and some resistance; grade 5 means active movement against full resistance.31.Please describe how to differential intracranial hemorrhage from cerebral infarction. (6 scores)Answers: often, the distinction between ischemic and hemorrhagic events cannot be made solely on the basis of clinical information. Intracranial hemorrhage-hemorragic stroke is more likely to present with severe headache, fluctuating levels of consciousness, and meningeal signs (2 scores), a history of hypertension (1 score). Ischemic vascular events are more likely to involve a singular vascular territory, and the patient’s status may improve early in the course of the event (1score). CT is able to identify intracerebral hemorrhages and most subarachnoid hemorrhages (2 scores).32.What are the crisis subtypes in myasthenia gravis? Please answer the causes of crises and how to identify them. (9 scores)Answer: (1) Myasthenia crisis: due to cholinergic deficiency ( insufficient amount of anticholinesterase), Tensilon test is positive, the symptoms improved; (2) Cholinergic crisis: due to the excess cholinergic (overdose of anticholinesterase), after Tensilon test, the symptoms become worse; (3) Brittle crisis: The anticholinesterase drug is not sensitive, sothe Tensilon test has no response.33.Please describe the characteristic of Wallenberg syndrome (including the lesions). (10 scores)Answers: it is also called lateral medullary syndrome. The syndrome is characterized by: (1) contralateral sensory deficits affecting the trunk and extremities and ipsilateral sensory deficits affecting the face and cranial nerves (damage to spinal trigeminal tract or nucleus of spinal trigeminal tract, and spinothalamic tract); (2) dysphagia, dysarthria palatal paralysis and absent gag reflex (damage to nucleus ambiguous, glossopharyngeal nerve and vagus nerve); (3) ipsilateral ataxia (damage to corpus restiforme, spinocerebellar tract or cerebellum); (4) vertigo, nystagmus and vomiting (vestibular nucleus); (5) Horner syndrome (descending fibers of sympathetic nerve). It usually occurs in obstruction of the vertebral artery, posterior inferior cerebellar artery or lateral medullary arteries.。
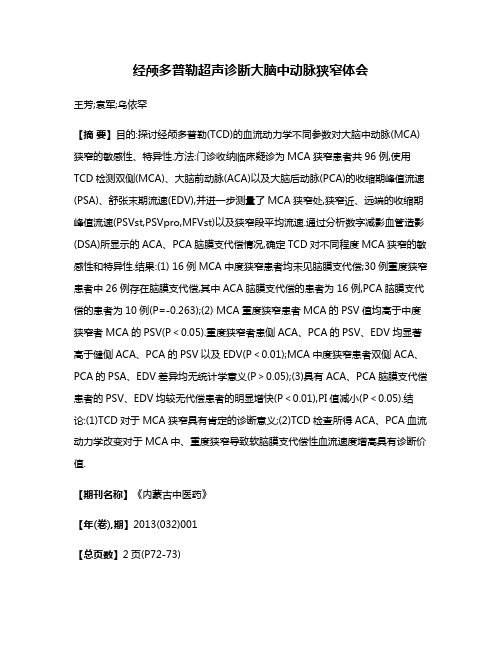
Diagnosis of Middle Cerebral Artery Stenosis by Transcranial Color-Coded Real-TimeSonographyKazumi Kimura,Masahiro Yasaka,Kuniyasu Wada,Kazuo Minematsu,Takenori Yamaguchi,andRyoichi OtsuboBACKGROUND&PURPOSE:This study was performed to determine the usefulness of transcranial color-coded real-time sonography(TCCS)in detecting stenosis in the horizontal portion of the middle cerebral artery(MCA).METHODS:Using TCCS and the incident angle correction technique,we measured the peak-systolic flow velocity in bilateral MCAs in45consecutive patients in whom cerebral angiography was carried out within1week before or after TCCS.Three patients had a stenosis of75%or greater and four had a unilateral occlusion of the extracranial internal carotid artery (ICA)(the ICS and ICO groups,respectively).Eight patients had a stenosis of50%or greater (one bilateral and seven unilateral)(the M1S group).Four patients had unilateral distal occlusion of the horizontal portion of the MCA(the M1O group).Twenty-six patients had no significant extra-or intracranial stenosis on the ipsilateral or contralateral side(the control group).RESULTS:Mean peak-systolic flow velocity on the affected side was83.0؎20.8cm/s in the ICS group,59.8؎23.2cm/s in the ICO group,and62.3؎33.7cm/s in the M1O group.In the control group,the mean peak-systolic flow velocity was116.0؎31.5cm/s.In the M1S group, however,the mean peak-systolic flow velocity(334.2؎35.7cm/s)on the affected side always exceeded180cm/s(mean value؎2SD in the control group),and was significantly higher than that in the other groups.The mean peak-systolic flow velocity in the M1S group increased with the grade of stenosis.CONCLUSION:The M1S group members could easily be distinguished from the other group members by their peak-systolic flow velocity in excess of180cm/s.Measurement of the peak-systolic flow velocity of the MCA by TCCS may help to identify a significant stenosis in the horizontal portion of the MCA.Since1982,when Aaslid et al(1)demonstrated Doppler signals from the arteries at the skull base through the temporal window,transcranial Doppler (TCD)sonography has been widely used to evaluate intracranial hemodynamic alterations,vasospasm af-ter subarachnoid hemorrhage,intracranial arterial stenosis,and arteriovenous malformations(2–4).In the early1990s,a new method,transcranial col-or-coded real-time sonography(TCCS)was intro-duced,and added real-time B-mode imaging and color coding of the Doppler signal to conventional TCD sonography(5–7).As a result of the B-mode and color-coded Doppler facilities,one can more readily and confidently identify a particular vascular structure with TCCS than is the case with TCD.Ad-ditionally,TCCS allows the investigator to measure the angle of insonation and to obtain flow velocities that are closer to true value than is possible with TCD. The peak-systolic flow velocity is considered to be useful for grading arterial stenosis because it in-creases with the progression of an arterial stenosis (8).Therefore,we set out to investigate whether it was possible to detect a significant stenosis in the horizontal portion of the middle cerebral artery (MCA)with TCCS by measuring peak-systolic flow velocity.Received March17,1998;accepted after revision July1.Supported in part by research grants for Cardiovascular Diseases(8-C4,9A-2,9A-3,9A-8)and for Comprehensive Research onAging and Health from the Ministry of Health and Welfare ofJapan,and by the Special Coordination Funds for Promoting Sci-ence and Technology(Strategic Promotion System for Brain Sci-ence)from the Science and Technology Agency of Japan.From the Cerebrovascular Division,Department of Medicine,National Cardiovascular Center,5–7–1Fujishirodai,Suita,Osaka565–8565,Japan.Address reprint requests to Kazumi Kimura,MD.©American Society of NeuroradiologyAJNR Am J Neuroradiol19:1893–1896,November19981893MethodsBetween April1,1997,and August30,1997,47patients had TCCS examinations within1week before or after cerebral angiography.Two patients with MCA occlusion at its origin were excluded because flow images of the MCA could not be obtained.Thus,45patients(37men and eight women;mean age,59Ϯ12years)were included in the study.On the basis of angiographic findings,we divided the45 patients into the following five groups:the internal carotid artery(ICA)stenosis(ICS)group,consisting of three patients with unilateral extracranial ICA stenosis(Ն75%);the ICA occlusion(ICO)group,containing four patients with a unilat-eral extracranial ICA occlusion;the MCA stenosis(M1S) group,including seven patients with unilateral and one with bilateral stenosis(Ն50%)of the horizontal portion of the MCA;the MCA occlusion(M1O)group,made up of four patients with a unilateral distal occlusion of the horizontal portion of the MCA;and the control group,which included52 vessels in26patients with no stenotic lesions(Ͻ50%)in the bilateral carotid systems.In the ICS,ICO,M1S,and M1O groups,19patients had atherothrombotic infarction in the carotid system,one had a lacunar infarction,and one had had a transient ischemic attack. In the control group,11patients had lacunar infarction,eight had cardioembolic infarction,four had had transient ischemic attacks,two had brain hemorrhage,and one had epilepsy. The equipment used included a commercially available TCCS system and a transducer that operated at2to3MHz for B-mode imaging and Doppler functions.The pulse repetition frequency was mainly3700Hz(range,3700to10,000Hz),and the low-pass filter was50Hz.The cerebral angiogram was imported into a computer sys-tem and an image of the MCA on the angiogram was magnified about three times to enable accurate measurement.Then,the percentage of stenosis was calculated by measuring the diam-eter at the stenotic lesion and at an adjacent intact portion. We routinely obtained color Doppler flow images and mea-sured flow velocity at MCAs on both sides by pulsed Doppler. The subjects were examined first in the left and then in the right lateral decubitus position.Blood flow velocity and direc-tion were displayed in real time as color signals within a sub-sector of the black-and-white image through a temporal bone window.Particular care was taken to obtain a long-axis view of the aimed vessel,especially of the horizontal portion of the MCA,by means of tilting,rotating,or shifting the transducer. Range-gated pulsed Doppler imaging,with a sample volume of2mm,was used to measure the blood flow velocity in the MCA.The sample volume was moved slowly from proximal to distal of the horizontal segment of the MCA,displayed as color flow on B-mode images,and the highest flow velocities during five consecutive cardiac cycles were obtained.We calculated the mean value of measured peak-systolic flow velocities corrected with an incident angle.Particular care was taken to keep the incident angle between the MCA and the beam at60°or less.The patients’age and flow velocity data were expressed as meanϮSD.For the analysis of velocity data among the five groups,we used the one-way factorial ANOVA.The regression analysis was performed using Cricket Graph software(version 1.3.2)between a peak-systolic flow velocity and percentage of stenosis by angiographic measurements in the M1S group.A value of PϽ.05was accepted as a significant difference.ResultsThe peak-systolic flow velocity on the affected side was83.0Ϯ20.8cm/s in the ICS group,59.8Ϯ23.2 cm/s in the ICO group,62.3Ϯ33.3cm/s in the M1O group,and116.0Ϯ31.5cm/s in the control group.All values were less than180cm/s(mean valueϩ2SD in the control group).There was no difference among the four groups.In the M1S group,however,the peak systolic flow velocity(334.2Ϯ35.7cm/s)on the affected side was significantly higher than that in the other four groups (PϽ.0001)(Figs1and2).The values always ex-ceeded180cm/s.Therefore,patients in the M1S group could accurately be distinguished from those in the other groups by their peak-systolic flow velocities above180cm/s.The peak-systolic flow velocities in the M1S group increased with the grade of stenosis(rϭ.87,Pϭ.001).DiscussionIn this study,patients in the M1S group had a significantly higher peak-systolic flow velocity than did those in the other groups.A stenosis of the hor-izontal portion of the MCA greater than50%could be distinguished perfectly from stenoses in any of the other groups by a cutoff point of peak-systolic flow velocity of180cm/s.TCD recordings of flow velocity were reported to be useful for evaluating intracranial occlusive arterial lesions(4,9–15).The TCD technique,however,has several problems.Precise placement of the sample volume as well as angle correction are not possible in the conventional TCD technique,and therefore it cannot be used for measuring absolute flow velocities. On the other hand,TCCS can be used to image the horizontal portion of the MCA and to measure absolute flow velocity(7),making this a more useful technique than TCD for assessing hemodynamics of the MCA.In previous studies,application of TCD to the di-agnosis of a stenosis of the horizontal portion of the MCA was based on increased peak systolic and mean flow velocities,spectral broadening,low-frequency bi-directional signals during systole,and arterial wall covibrations(9–11).It has been reported that the sensitivity of TCD in detecting MCA stenosis (Ն50%)ranged from75%to86%,and its specificity exceeded93%(9,10).The elevation of peak-systolic flow velocities ranged from150to250cm/s in stenotic lesions of the horizontal portion of the MCA(9–11). In TCD examinations,the angle between the Doppler beam and the horizontal portion of the MCA is as-sumed to range from0°to30°,so its cosine would vary between1.00and0.86(12).When a velocity of150 cm/s measured by TCD is corrected with a cosine of 30°,it would become173cm/s.This value,150cm/s, for a stenosis of the horizontal portion of the MCA as measured with TCD perhaps coincides with our cut-off value of180cm/s,measured with TCCS.Our study indicates an excellent correlation be-tween flow velocity and grade of stenosis on cerebral angiography.In previous TCD studies,an increased flow velocity corresponding to the grade of stenosis in the MCA has been described(13).However,Bray et al(9)reported that it was not uncommon to find similar flow velocities among patients with different degrees of MCA stenosis.These discrepant TCD1894KIMURA AJNR:19,November1998findings are probably attributable to inaccurate mea-surements of MCA flow velocity by TCD.ConclusionRecently,we reported that end-diastolic flow ve-locity as measured with TCCS might help to identify the site of occlusion in the horizontal portion of the MCA (16).In this study,we demonstrated that peak-systolic flow velocity may be useful to quantitate the degree of stenosis in the horizontal portion of the MCA.We conclude that in any evaluation of occlu-sive lesions in the MCA with TCCS,it is important to measure both the peak-systolic and end-diastolic flow velocities.References1.Aaslid R,Markwalder TM,Nornes H.Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries.J Neurosurg 1982;57:769–7742.Lindegaard KF,Bakke SJ,Grolimund P,Aaslid R,Huber P,Nornes H.Assessment of intracranial hemodynamic in carotid artery disease by transcranial Doppler ultrasound.J Neurosurg 1985;63:890–8983.Aaslid R,Huber P,Nornes H.Evaluation of cerebrovascular spasm with transcranial Doppler ultrasound.J Neurosurg 1984;60:37–414.Wechsler LR,Ropper AH,Kistler JP.Transcranial Doppler in cerebrovascular disease.Stroke 1986;17:905–9125.Bogdahn U,Becker G,Winkler J,Greiner K,Perez J,Meurers B.Transcranial color-coded real-time sonography in adults.Stroke 1990;21:1680–16886.Martin PJ,Evans DH,Naylor AR.Transcranial color-coded sonog-raphy of the basal cerebral circulation.Stroke 1994;25:391–3967.Tsuchiya T,Yasaka M,Yamaguchi T,Kimura K,Omae T.ImagingF IG parison of peak-systolic flow velocity among the groups.In the M 1S group,the peak-systolic flow velocity was significantly higher than that in the ICS,ICO,M 1O,and control groups (P Ͻ.0001).Dotted line indicates the mean ϩ2SD value of the peak-systolic flow velocity (180cm/s)in the control group.ICS,stenosis (Ͼ75%)of the extracranial ICA;ICO,occlusion of the extracranial ICA;M 1S,stenosis (Ն50%)of the horizontal portion of the MCA artery;M 1O,occlusion of the horizontal portion of the MCA artery;and Control,no significant arterial lesions in the carotidsystem.F IG 1.A representative case of MCA stenosis evaluated with cerebral angiography and transcranial color-coded real-time sonography.A ,Left carotid angiogram,anteroposterior view,shows a 50%stenosis in the left MCA (arrow ).B .Transcranial color-coded real-time sonogram shows the MCA (in red ),indicating flow toward the transducer.The sample volume is situated in the MCA.The angle between the Doppler beam and the vessel is adjusted (48°).C ,Doppler waveforms of the left MCA show the peak-systolic flow velocity is 281cm/s.AJNR:19,November 1998MIDDLE CEREBRAL ARTERY STENOSIS 1895of the basal cerebral arteries and measurement of blood velocity in adults by using transcranial real-time color flow Doppler sonogra-phy.AJNR Am J Neuroradiol1991;12:497–5028.Can U,Furie KL,Suwanwela N,Southern JF,et al.TranscranialDoppler ultrasound criteria for hemodynamically significant inter-nal carotid artery stenosis based on residual lumen diameter cal-culated from en bloc endarterectomy specimens.Stroke1997;28: 1966–19719.Bray JM,Joseph PA,Jeanvoine H,Maugin D,Dauzat M,PlassardF.Transcranial Doppler evaluation of middle cerebral artery ste-nosis.J Ultrasound Med1988;7:611–61610.Ley-Pozo J,Ringelstein EB.Noninvasive detection of occlusivedisease of the carotid siphon and middle cerebral artery.Ann Neurol1990;28:640–64711.Hennerici M,Rautenberg W,Schwartz A.Transcranial Dopplerultrasound for the assessment of intracranial arterial flow velocity, part2.Surg Neurol1987;27:523–53212.DeWitt LD,Rosengart A,Teal PA.Transcranial Doppler ultra-sonography:normal values.In:Babikan VL,Wechsler LR,eds.Transcranial Doppler Ultrasonography.St Louis:Mosby-Year Book;1993:29–3813.Lindegaard KF,Bakke SJ,Aaslid R,Hornes H.Doppler diagnosisof intracranial artery occlusive disorders.J Neurol Neurosurg Psy-chiatry1986;49:510–51814.Mattle H,Grolimund P,Huber P,Sturzenegger M,Zurbrugg HR.Transcranial Doppler sonographic findings in middle cerebral artery disease.Arch Neurol1988;45:289–29515.Kaps M,Damian MS,Teschendorf U,Dorndorf W.TranscranialDoppler ultrasound findings in middle cerebral artery occlusion.Stroke1990;21:532–53716.Kimura K,Hashimoto Y,Hirano T,Uchino M,Ando M.Diagnosisof middle cerebral artery occlusion with transcranial color-coded real-time sonography.AJNR Am J Neuroradiol1996;17:895–8991896KIMURA AJNR:19,November1998。