meta分析教程
- 格式:pdf
- 大小:307.34 KB
- 文档页数:5

meta分析教程Step 1: Formulate your research questionBefore conducting a meta-analysis, it is crucial to clearly define your research question or objective. This will help guide your search for relevant studies and determine the criteria for including or excluding studies from your analysis.The next step is to perform an extensive literature search to identify all relevant studies on your research question. This can be done by searching electronic databases, such as PubMed or Google Scholar, using specific keywords and inclusion/exclusion criteria. Additionally, it may be helpful to review the reference lists of selected articles to find additional studies that were missed during the initial search.Step 3: Screen and select studiesStep 4: Extract data from selected studiesStep 5: Assess study quality and risk of biasTo evaluate the quality and risk of bias of the included studies, a critical appraisal should be conducted. This involves assessing factors such as study design, sample size, blinding, randomization, and potential sources of bias. Various tools and checklists, such as the Cochrane Collaboration's Risk of Bias Tool, can be used to systematically assess the quality of individual studies.Step 6: Analyze the dataStep 7: Assess heterogeneityHeterogeneity refers to the variability in effect sizes across studies. It is important to assess and quantify heterogeneity using statistical tests, such as the Q test or I² statistic. If significant heterogeneity is present, subgroup analyses or sensitivity analyses may be conducted to explore potential sources of heterogeneity.Step 8: Publication bias assessmentPublication bias occurs when studies with statistically significant results are more likely to be published, while studies with nonsignificant or negative findings remain unpublished. To assess publication bias, funnel plots can be used to visually examine the symmetry of the distribution of effect sizes. Statistical tests, such as Egger's regression or Begg's rank correlation, can also be applied to quantify the degree of asymmetry.Step 9: Interpret and report the findingsFinally, the results of the meta-analysis should be interpreted and reported in a clear and concise manner. The findings should be discussed in light of the research question, the characteristics of the included studies, and the limitationsof the analysis. Conclusions should be drawn based on the strength of evidence provided by the meta-analysis.。
meta分析原理与流程下载温馨提示:该文档是我店铺精心编制而成,希望大家下载以后,能够帮助大家解决实际的问题。
文档下载后可定制随意修改,请根据实际需要进行相应的调整和使用,谢谢!并且,本店铺为大家提供各种各样类型的实用资料,如教育随笔、日记赏析、句子摘抄、古诗大全、经典美文、话题作文、工作总结、词语解析、文案摘录、其他资料等等,如想了解不同资料格式和写法,敬请关注!Download tips: This document is carefully compiled by theeditor. I hope that after you download them,they can help yousolve practical problems. The document can be customized andmodified after downloading,please adjust and use it according toactual needs, thank you!In addition, our shop provides you with various types ofpractical materials,such as educational essays, diaryappreciation,sentence excerpts,ancient poems,classic articles,topic composition,work summary,word parsing,copy excerpts,other materials and so on,want to know different data formats andwriting methods,please pay attention!Meta 分析是一种统计学方法,用于综合多个研究结果,以提供更全面、更可靠的结论。

Meta分析的实施步骤简介Meta分析是一种通过综合多个独立研究结果来获得更准确和可靠的结论的统计方法。
它可以解决单个研究可能无法得出一致结论的问题,还可以提供更大样本量和更广泛范围的评估。
本文将介绍meta分析的实施步骤,并以列点的方式给出详细说明。
实施步骤1.明确研究目的:–确定要分析的研究问题和目标。
–确定研究领域和主题,以便确定适当的文献检索策略。
2.文献检索和筛选:–制定文献检索策略,包括选择适当的数据库和关键词。
–检索和筛选符合研究目的和标准的相关文献,如纳入和排除标准。
3.数据提取:–建立数据提取表格或工具,包括提取的变量和相关数据。
–独立提取数据,并双重检查以确保准确性。
4.质量评估:–评估纳入研究的质量和偏倚风险。
–使用适当的工具、量表或评估标准进行评估。
5.效应量的计算:–根据研究设计和数据类型选择适当的效应量测量方法。
–计算每个研究的效应量和标准误差。
6.数据合并:–使用统计软件进行meta分析的数据合并。
–选择合适的模型(例如,固定效应模型或随机效应模型)进行合并。
7.统计分析和解释:–分析合并效应量,并计算相应的置信区间和p值。
–进行敏感性分析和亚组分析,以探究可能的异质性和系统误差。
8.结果报告和解释:–撰写meta分析报告,包括研究背景、方法、结果和讨论等部分。
–解释结果的实际意义和潜在影响,讨论研究结果的局限性和不确定性。
9.提出结论:–总结meta分析的主要结论和发现。
–提出未来研究的建议和方向。
总结通过执行上述meta分析的实施步骤,研究者可以综合多个独立研究的结果,提供更准确和可靠的结论。
这种方法对于整合和综合现有证据,获得更具统计学意义的结论具有重要意义。
然而,执行meta分析时需要详细考虑文献检索、数据提取、质量评估等关键步骤,并以透明和系统的方式进行分析和报告。
meta分析数据处理流程方法
Meta分析是一种统合多个研究结果以得出综合结论的统计分析方法。
进行meta分析的数据处理流程大致可以分为以下几个步骤:
1.明确研究问题与纳入标准:首先,需要明确meta分析的目标和
研究问题。
基于这个目标,制定包括纳入和排除研究的标准。
2.文献搜索与筛选:通过系统性地搜索电子数据库和其他资源来识
别相关研究,使用事先定义的纳入和排除标准来筛选研究。
3.数据提取与管理:对于筛选后纳入的研究,提取关键信息和数据,
如样本大小、干预措施和结果等。
可能需要使用电子表格或专门的软件来管理这些数据。
4.质量评估:评估纳入研究的质量,识别可能的偏倚风险。
这可以
通过使用标准化的评估工具来完成。
5.统计分析:使用meta分析的统计方法来综合研究结果。
这通常
涉及计算效应量的合并估计值和进行异质性测试。
可能会使用固定效应或随机效应模型,具体取决于研究间异质性的程度。
6.解释结果与报告:对分析结果进行解释,并考虑异质性的来源、
研究质量、可能的偏倚等因素。
最后,编写报告或发表文章,详细描述meta 分析的方法、结果和结论。
7.灵敏度分析:进行灵敏度分析来检查结果的稳健性,即改变一些
分析假设(如纳入标准、效应量模型等)对结果的影响。
8.评估发表偏倚:使用统计方法((如漏斗图和Egger测试)来评估
是否存在发表偏倚,即未发表的负面或无显著结果研究可能对综合结果的影响。
完成以上步骤后,meta分析可以为某一领域的研究提供一个全面和客观的综述,帮助科研人员和决策者更好地理解和应用现有证据。


meta基本步骤
Meta分析是一种统计分析方法,用于综合多项研究的结果以评估某一问题或干预的效果。
进行Meta分析的基本步骤如下:
1. 确定研究问题:明确Meta分析的研究目标和问题,包括研究的类型、研究对象、干预措施等。
2. 制定纳入和排除标准:设定明确的标准来决定哪些研究应该被包括在分析中,哪些应该被排除。
这些标准应基于研究设计、样本大小、发表状态等因素。
3. 文献检索和筛选:系统地检索数据库和其他来源,找到所有相关的研究。
根据纳入和排除标准筛选出符合条件的研究。
4. 数据提取:从选定的研究中提取关键信息和数据,包括研究特征、参与者特征、干预措施、结果指标等。
5. 质量评估:评估所选研究的质量和偏倚风险。
可以使用不同的工具来评估随机对照试验和非随机研究的质量。
6. 数据分析:使用统计软件对提取的数据进行分析。
这包括计算效应量、进行异质性检验、探索亚组分析或敏感性分析等。
7. 解释结果:解释Meta分析的结果,包括效应量的大小和方向、异质性的可能来源、研究质量对结果的影响等。
8. 报告和讨论:撰写报告,详细描述Meta分析的方法、结果和结论。
讨论研究的局限性、未来研究方向和临床实践的意义。
9. 更新Meta分析:随着新研究的出现,定期更新Meta分析,确保其结果保持最新和相关性。
通过遵循这些步骤,研究者可以确保Meta分析的系统性和透明度,从而提供可靠的证据支持决策制定。

Meta分析的步骤Meta分析是一种通过合并多个独立研究的结果来获得更准确、可靠的结论的统计分析方法。
它可以帮助研究者总结和评估大量相关研究的结果,从而提供更全面的证据支持决策和政策制定。
下面将介绍Meta分析的完整步骤。
第一步:明确研究问题在进行Meta分析之前,需要明确研究的目的和问题。
这将有助于确定所需的研究类型和选择适当的研究策略。
第二步:收集相关研究第三步:筛选研究第四步:提取数据在提取数据时,研究者应根据预先设计的数据提取表,从每个纳入研究中提取所需的数据。
这些数据可以包括研究特征、样本大小、效应量(如均值、标准差、相对风险等)和其他相关变量。
第五步:评估研究质量评估研究质量是Meta分析的关键步骤之一、研究者可以使用一些评估工具,如Cochrane协作网络(Cochrane Collaboration)提供的工具来评估纳入研究的质量。
这些工具通常包括随机对照试验的风险偏倚评估工具和观察研究的质量评估工具。
第六步:进行统计分析在进行统计分析之前,研究者需要对纳入研究的数据进行预处理。
这可能包括转换效应量、计算合适的权重和调整相关的不一致性。
然后,根据研究设计和变量特征,选择合适的统计模型进行分析。
常用的统计模型包括固定效应模型和随机效应模型。
固定效应模型假设所有研究的效应量相同,而随机效应模型允许研究之间存在异质性。
第七步:进行效应量合并在进行效应量合并之前,需要考虑研究之间的异质性。
如果研究之间的异质性较小,则可以使用固定效应模型进行合并。
如果研究之间的异质性较大,则应使用随机效应模型进行合并。
研究者还可以使用森林图或漏斗图等图形来显示合并效应量和置信区间。
第八步:评估结果的稳健性在评估结果的稳健性时,研究者可以进行敏感性分析和亚组分析。
敏感性分析是通过排除一些研究或改变分析方法来检验结果的稳健性。
亚组分析是将研究按照一些特定特征进行分类,然后比较不同亚组间的效应量。
这可以帮助研究者了解不同因素对结果的影响。
meta分析教程Meta分析是一种系统性的分析方法,用于综合多个研究的结果,以获得更为准确和可靠的结论。
在进行Meta分析时,需要按照以下步骤进行:1. 研究收集:收集与所要研究的问题相关的研究文献。
可以通过检索学术数据库、查找文献引用、联系领域专家等途径进行。
2. 文献筛选:根据预先设定的纳入和排除标准,对收集到的文献进行筛选。
通常会根据文献的标题和摘要进行初步筛选,只保留符合研究问题的文献。
3. 数据提取:从筛选出的文献中提取相关数据。
这些数据可以是研究的参与者特征、研究设计、结果等。
4. 数据分析:结合收集到的数据,进行统计分析。
常见的分析方法包括计算效应量、绘制森林图、计算加权平均效应量等。
5. 结果解释:根据分析结果,进行结果解释和探讨。
可以结合研究的目的和问题,对结果进行解读,并分析可能的研究偏倚和不确定性。
在进行Meta分析时需要注意一些常见的问题:1. 研究异质性:由于研究设计、样本特征等因素的不同,研究结果可能存在一定的异质性。
在进行Meta分析时,可以使用统计方法(如Cochrane's Q统计量和I^2指数)来评估异质性,并考虑采用随机效应模型进行分析。
2. 研究偏倚:由于公开发表结果可能存在选择性报道和发表偏倚,Meta分析也可能受到研究偏倚的影响。
可以通过绘制漏斗图和进行敏感性分析等方法来评估研究偏倚的影响。
3. 数据质量评估:在进行Meta分析时,需要对包含的研究进行质量评估。
可以使用工具(如Cochrane Risk of Bias工具)对研究的内部有效性进行评估,并根据评估结果进行结果解释和结论推断。
综上所述,Meta分析是一种有效的综合研究结果的方法,能够更全面地了解某一研究问题。
在进行Meta分析时,需要对研究进行收集、筛选、数据提取、数据分析和结果解释等步骤,并需要注意研究异质性、研究偏倚和数据质量等问题。
谁总结的meta分析教程,太全了meta分析系列001期荟萃分析一般步骤002期浅谈meta分析的选题和写作注意事项003期系统综述和荟萃分析优先报告的条目:PRISMA声明004期 Revman实现单个率的荟萃分析005期荟萃分析在急危重症中的应用006期什么荟萃分析容易发表007期一图读懂:meta分析异质性008期 SCI教程meta系列:动物实验meta的学习网站009期系统评价新的评价工具:ROBIS010期累积meta分析原理以及软件的实现011期高影响因子的meta分析应该是这样的012期如何利用meta分析寻找危险因素013期 Step by step 完成meta分析014期中药方剂如何发meta,纳入文献全是中文哦!动心不?015期简单粗暴的meta选题016期 SCI思路篇:meta分析速成要点017期 Meta分析:老年人打太极降压效果堪比一线降压药物018期累积meta分析实例讲解019期核心期刊系列:中药meta范文欣赏020期想在BMJ上的发表meta分析吗,点进去?021期 R软件系列:实现二分类数据的Meta分析(2)022期如何使用Revman产生文献筛选流程图023期 Meta分析时,傻傻分不清楚的效应量指标的选择024期 R软件系列:实现连续数据的Meta分析025期 Power and Precision和G*Power软件实现Meta分析统计效能计算(2)026期 Power and Precision和G*Power软件实现Meta分析统计效能计算(1)027期如何在stata中添加meta模块从这里开始点击标题0..期028期诊断性meta分析报告规范:不知道规矩还怎么玩029期文献解读:原来meta分析如此简单030期 Medcalc:如何完成meta分析031期所有的meta分析,都可以参考这个模板032期如何采用RevMan 5.3 软件实现单核苷酸多态性数据的Meta 分析033期 SCI思路篇:meta分析速成要点034期诊断性meta分析——R语言教程035期 EXCEL用于诊断性meta分析缺失数据的提取036期诊断性meta分析质量评价037期 PRISMA:meta分析结构化写作举例说明038期 R语言实现累积meta分析039期 Meta分析常用教程之连续性变量:R语言教程040期SNP(单核苷酸多态性)Meta分析:史上最全通熟易懂教程041期做meta分析,再也不用担心发表偏倚如何检测了042期 Meta分析常用教程:R语言043期考克兰组织告诉你一篇干预性meta分析,应该如何提取数据044期临床科研轶事:meta回归小记关于惊喜那些事首发促销活动中,原价250元,现价仅为99元网易云课堂链接/course/introduction/1004860024.htmshare=2&shareId=400000000355020课程目标帮助临床医生,循证医学爱好者,研究生,快速掌握Meta分析的基本知识以及选题技巧,并且能够独立完成Meta文章的撰写。
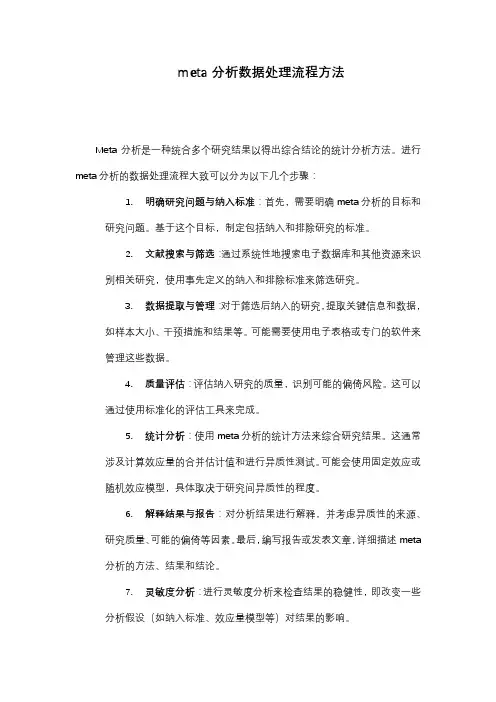
Leukemia Research 34 (2010) 1596–1600Contents lists available at ScienceDirectLeukemiaResearchj o u r n a l h o m e p a g e :w w w.e l s e v i e r.c o m /l o c a t e /l e u k r esMTHFR C677T polymorphisms and childhood acute lymphoblastic leukemia:A meta-analysisJing Wang a ,Ping Zhan b ,Bing Chen a ,Rongfu Zhou a ,Yonggong Yang a ,Jian Ouyang a ,∗a Department of Hematology,the Affiliated DrumTower Hospital of Nanjing University Medical School,321Zhongshan Road,Nanjing 210008,Jiangsu PR China bDepartment of Respiratory Medicine,Nanjing Chest Hospital,Nanjing,PR Chinaa r t i c l e i n f o Article history:Received 4January 2010Received in revised form 19March 2010Accepted 20March 2010Available online 20 April 2010Keywords:MTHFR polymorphismsAcute lymphoblastic leukemia Meta-analysisa b s t r a c tTo date,case–control studies on the association between methylenetetrahydrofolate reductase (MTHFR)C677T and childhood acute lymphoblastic leukemia have provided either controversial or inconclusive results.To clarify the effect of MTHFR C677T on the risk of childhood acute lymphoblastic leukemia,a meta-analysis of all case–control observational studies was performed.Heterogeneity (I 2=65%,P <0.0001)for C677T among the studies was extreme.The random effects (RE)model showed that the 677T allele was not associated with a decreased susceptibility risk of childhood acute lymphoblastic leukemia compared with the C allele [OR =0.96,95%confidence interval (CI)(0.88–1.04),P =0.34].The contrast of homozygotes,recessive model and dominant model produced the same pattern of results as the allele contrast.Although MTHFR C677T was associated with increased risks of colorectal cancer,leukemia,and gastric cancer,our pooled data suggest no evidence for a major role of MTHFR C677T in the carcinogenesis of childhood acute lymphoblastic leukemia.© 2010 Elsevier Ltd. All rights reserved.1.IntroductionAcute lymphoblastic leukemia (ALL)is the most common malig-nancy affecting children,constituting about 30%of all cancers among children [1,2].Although significant improvements in both ALL diagnosis and treatment have been made over the past decades,the etiology of most cases of ALL remains unknown due to proba-ble multifactorial mechanisms of pathogenesis [3].Pediatric acute leukemias are likely influenced by both the genetic background and the environment of the patient [4,5].Methylenetetrahydrofolate reductase (MTHFR)plays an important role in folate metabolism by catalyzing the irre-versible conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate [4].A common polymorphism at the nucleotide 677,C677T (Ala →Val),in the gene for the enzyme MTHFR,results in a less stable version of the enzyme [6].MTHFR C677T has been associated with an increased risk of colorectal cancer,leukemia,and gastric cancer [7].The role of MTHFR polymorphisms in the development of childhood ALL has been investigated in the past decade,with conflicting results.Sev-eral studies have previously suggested an association between the MTHFR C677T polymorphism and a decreased risk of acute lymphoblastic leukemia (ALL)[8,9].However,other studies have∗Corresponding author.Tel.:+862583105211;fax:+862583105211.E-mail address:ouyang211@ (J.Ouyang).failed to confirm such an association [10,11].Moreover,two meta-analyses [12,13]investigating the same hypothesis,quite similar in methods and performed almost at the same time,yielded different conclusions.The exact relationship between genetic polymorphisms of MTHFR C677T and susceptibility to childhood ALL has not been entirely established.To clarify the effect of MTHFR C677T on the risk of childhood ALL,our study undertakes a meta-analysis of all published case–control observational studies.2.Methods2.1.Publication searchThe electronic databases PubMed,Embase,Web of Science,and CNKI (China National Knowledge Infrastructure)were searched for studies to include in the present meta-analysis,using the terms:“Methylenetetrahydrofolate Reductase,”“genotype,”“Leuk(a)emia,”“Acute lymphocytic,”“Acute lymphoblastic,”“Child-hood,”“P(a)ediatric,”“polymorphism,”“MTHFR,”“C677T,”“folate,”and “mutation.”An upper date limit of August 30,2009was applied;we used no lower date limit.The search was conducted without any restrictions on language but focused on stud-ies that had been conducted on human subjects.We also reviewed the Cochrane Library for relevant articles.The reference lists of reviews and retrieved articles were hand-searched simultaneously.Only published studies with full text articles were included.When more than one instance of the same patient population was included in several publications,only the most recent or complete study was used in this meta-analysis.2.2.Data extractionThe following information was extracted from each study:first author,year of publication,ethnicity of study population,genotyping method,and the num-ber of cases and controls for the C677T genotype.We did not define any0145-2126/$–see front matter © 2010 Elsevier Ltd. All rights reserved.doi:10.1016/j.leukres.2010.03.034J.Wang et al./Leukemia Research34 (2010) 1596–16001597Table1Study characteristics.Studyfirst author Country Source of controls No.of cases/controls Leukemia characteristicsFranco et al.[8]Brazil Population71/7177%B-ALL and23%T-ALLWiemels et al.[10]United Kingdom Population216/20036%were TEL-AML1and64%were hyperdiploid leukemiasBalta et al.[11]Turkey Population142/18552%B-ALL,28%non-B-ALL,and20%undeterminedKarjinovic et al.[14]Canada Hospital270/30085%pre B-ALL,11%T-ALL,and4%undeterminedJiang et al.[9]China Population29/67Immunophenotype not describedChatzidakis et al.[18]Greece Population52/8887%B-ALL and13%T-ALLOliveira et al.[16]Portugal Population103/111Immunophenotype not describedSchnakenberg et al.[17]Germany Population443/37977.7%B-ALL,18.3%T-ALL,0.9%biphenotype,and3.2%undetermined Thirumaran et al.[15]Germany Population453/1448Immunophenotype not describedZanrosso et al.[19]Brazil Population165/19894.9%B-ALL and5.1%T-ALLKim et al.[22]Korea Population66/100Immunophenotype not describedReddy et al.[21]India Population135/142Immunophenotype not describedYu et al.[20]China Population51/5372.5%B-ALL and27.5%T-ALLPetra et al.[24]Slovenia Hospital68/25875%B-ALL,11.8%T-ALL,13.2%biphenotype,and3.2%undetermined Kamel et al.[23]Egypt Population88/311B-ALLGiovannetti et al.[25]Indonesia Population71/44Immunophenotype not describedAlcasabas et al.[26]Philippines Population189/394Immunophenotype not describedLiu et al.[27]China Population83/83Immunophenotype not describedde Jonge et al.[28]Netherlands Population243/49675%B-ALL and25%T-ALLKim et al.[29]Korea Population107/1700Immunophenotype not describedYeoh et al.[30]Singapore Population318/34589.4%B-ALL,7.8%T-ALL and2.8%infant ALLThree studies[9–11]were excluded from this meta-analysisminimum number of patients as a criterion for a study’s inclusion in our meta-analysis.2.3.Statistical analysisThe meta-analysis examined the overall association for the allele contrasts,the contrast of homozygotes,and the recessive and dominant models.The effect of the association was indicated as an odds ratio(OR)with its corresponding95%confi-dence interval(CI).Pooled OR was estimated usingfixed effects and random effects models.Heterogeneity between studies was tested using the Q statistic.Such het-erogeneity was considered statistically significant if P<0.10.Heterogeneity was quantified using the I2metric,which is independent of the number of studies in the meta-analysis(I2<25%no heterogeneity;I2=25–50%moderate heterogene-ity;I2>50%large or extreme heterogeneity).An estimate of potential publication bias was carried out by the funnel plot,in which the standard error of log(OR) of each study was plotted against its log(OR).An asymmetric plot suggests a possible publication bias.Funnel plot asymmetry was assessed by the method of Egger’s linear regression test,a linear regression approach for measuring fun-nel plot asymmetry on the natural logarithm scale of the OR.The significance of the intercept was determined by the t-test suggested by Egger(P<0.05indicated a statistically significant publication bias).All calculations were performed using ReviewManage5.0.3.Results3.1.Study characteristicsWe found21published articles addressing the relation-ship between MTHFR C677T and childhood acute lymphoblastic leukemia(Table1).The studies were published between1999and 2009.In all studies,the cases were histologically confirmed,and the control groups were free of ALL and were matched for age and gender.Studies were conducted in various populations of dif-ferent ethnicities:nine were conducted in populations of Asian regions[9,20–22,25–27,29,30],and eight studies looked at Euro-peans[10,11,15–18,24,28].Table2Distribution of methylenetetrahydrofolate reductase(MTHFR)C677T genotypes and allelic frequency.Studyfirst author(year)Distribution of C677T MTHFR genotype Frequency of C677T MTHFR alleles Hardy–Weinbergequilibrium(HWE)PvalueCC CT TT C TCases,n Controls,n Cases,n Controls,n Cases,n Controls,n Cases,n Controls,n Cases,n Controls,nFranco et al.(2001)[8]362228366131008040620.796Wiemels et al.(2001)[10]9889917927322872571451430.047Balta et al.(2004)[11]71906087118202267821030.020Karjinovic et al.(2004)[14]11212612712831463513801892200.159Jiang et al.(2004)[9]1518144108447714570.039Chatzidakis et al.(2005)[18]31321847398011124650.169Oliveira et al.(2005)[16]484550575914114760750.120 Schnakenberg et al.(2005)[17]19518420115247435915203042380.179Thirumaran et al.(2005)[15]19960019568159167593188131310150.210Yu et al.(2006)[20]30201423710746328430.466Zanrosso et al.(2006)(W)[19]4359355081012116851700.896Zanrosso et al.(2006)(nW)[19]5337213251012710631520.462Kim et al.(2006)[22]1724385511217210360970.313Reddy et al.(2006)[21]517977587517921691680.148Petra et al.(2007)[24]301123311053693334431820.287Kamel et al.(2007)[23]3915642135720120447561750.195Liu et al.(2008)[27]343823362699111275540.914Giovannetti et al.(2008)[25]512611630113581760.558Alcasabas et al.(2008)[26]14532241663633171047780.227de Jonge et al.(2009)[28]1302199322322543536611373310.805Kim et al.(2009)[29]295405186327297109194310514570.132Yeoh et al.(2009)[30]18416311115023324794761572140.7651598J.Wang et al./Leukemia Research34 (2010) 1596–1600Fig.1.Forest plot of the OR of T allele vs.C allele.The size of the squares reflects each study’s relative weight and the diamond (♦)represents the aggregate OR and 95%CI.The studies provided 3358cases and 6961controls for C677T.The variant genotype and allele frequencies of C677T in the indi-vidual studies are shown in Table 2.For case groups,the frequency of C677T polymorphism among CC-homozygous individuals was 48.9%;while 40.9%of CT-heterozygous individuals and 10.2%of TT-homozygous individuals displayed C677T polymorphism.In control groups,the frequencies of C677T polymorphism among CC-homozygous individuals,CT-heterozygous individuals,and TT-homozygous individuals were 43.1%,45.0%,and 12.1%,respectively.The 677T allelic frequencies in the case and control groups were 30.8%and 34.5%,respectively.In three studies [9–11]of the C677T polymorphism,the distribution of genotypes in the control group was not in HWE (P <0.05),indicating genotyping errors and/or pop-ulation stratification (Table 2).These three studies were excluded from this meta-analysis to clarify the effect of MTHFR C677T on the risk of childhood ALL.3.2.Meta-analysis resultsTable 3lists the main results of this meta-analysis.Overall,the 677T allele was not associated with the risk of childhood ALL compared with the C allele (OR =0.93;95%CI =0.82–1.07,Fig.1).Contrasting homozygotes (TT ),the recessive model,and the dominant model produced the same pattern of results as the allele contrast.In the analysis stratified by ethnicity and region,no sig-nificant associations were found between childhood ALL and the various genetic models.There was extreme heterogeneity (I 2=65%,P <0.0001)among the 18studies.To eliminate heterogeneity,we divided the 18studies into subgroups as far as possible;subse-quently,heterogeneity only decreased for subgroups of white and European subjects,which revealed that most of the studies could not be grouped helpfully according to ethnicity and region.3.3.Publication biasBegg’s funnel plot and Egger’s test were performed to assess the publication bias of literatures.Evaluation of publication bias for 677T allele versus C allele showed that the Egger test was not significant (P =0.346).These results did not indicate a potential forpublication bias.For TT versus CC,the publication bias was also not found (P =0.356).4.DiscussionIt is well recognized that individual susceptibility to the same kind of cancer can vary,even with identical environmental expo-sures.Host factors,including polymorphism in the genes involved in carcinogenesis may account for this difference.Therefore,genetic susceptibility to cancer has been the focus of research in the scientific community.Recently,genetic variants of the MTHFR gene have been subject to increasing attention in the etiology of leukemia.This meta-analysis summarized all the available data on the association between MTHFR C677T and childhood acute lymphoblastic leukemia,including a total of 3358cases and 6961controls.Our results indicated no evidence for a major protective role of MTHFR C677T in the carcinogenesis of childhood acute lym-phoblastic leukemia.Additionally,white ethnicity and European region were not found to be significantly associated with any of the genetic models.Although in Caucasians,no significant associa-tions were found for the genetic models examined,heterogeneity disappeared when that population was viewed as a separate group,which suggested that the effect of T allele on the risk of pediatric ALL may differ by ethnicity.Population stratification is an area of concern,and it can lead to spurious evidence for the association between the genetic marker and the disease,suggesting a possible role of ethnic differences in genetic backgrounds and environments [31].In an effort to shed some light on the impact of MTHFR C677T on pediatric ALL,data was pooled from available published trials for meta-analysis.However,two previous meta-analyses [12,13]per-formed almost at the same time came to different conclusions from one another.One of these previously published meta-analyses [12]drew on four fewer publications than the other [13].Of these four missed/excluded publications,two examined adult ALL [32,33]and two evaluated childhood ALL [15,19].In fact,electronic searches by Zintzaras et al.were carried out solely using Medline [12].The use of this database alone is not sufficient for literature searches [34].Previous research assessing different electronic databases hasJ.Wang et al./Leukemia Research34 (2010) 1596–16001599Table3Odds ratios(ORs)and heterogeneity results for the genetic contrasts of MTHFR gene C677T polymorphisms for childhood acute lymphoblastic leukemia.Population OR I2(%)P value Q testFixed effects(95%CI)Random effects(95%CI)Alleles(T vs.C)All0.95(0.89–1.02)0.93(0.82–1.07)65<0.0001 Non-White 1.02(0.91–1.15) 1.03(0.80–1.31)730.0001 White0.91(0.84–1.00)0.87(0.76–1.01)510.04 European0.93(0.84–1.03)0.89(0.75–1.05)540.05 Asian 1.05(0.92–1.20) 1.09(0.83–1.43)720.0007 East Asian a0.96(0.82–1.11)0.97(0.68–1.39)790.0007TT to CC All0.91(0.78–1.07)0.87(0.68–1.11)440.02 Non-White 1.08(0.82–1.42) 1.05(0.67–1.67)550.02 White0.84(0.68–1.02)0.80(0.62–1.02)210.25 European0.88(0.70–1.10)0.85(0.65–1.12)170.30 Asian 1.18(0.88–1.58) 1.20(0.72–2.01)570.02 East Asian 1.11(0.81–1.52) 1.07(0.56–2.06)720.006TT to(CT+CC)All0.98(0.84–1.14)0.95(0.76–1.18)380.05 Non-White 1.19(0.93–1.54) 1.16(0.78–1.72)480.04 White0.87(0.72–1.06)0.87(0.72–1.07)30.41 European0.93(0.75–1.15)0.94(0.76–1.17)00.43 Asian 1.26(0.96–1.65) 1.25(0.80–1.96)520.04 East Asian 1.24(0.93–1.64) 1.20(0.68–2.14)710.009TT+CT to CC All0.93(0.84–1.02)0.91(0.76–1.08)65<0.0001 Non-White 1.00(0.85–1.16) 1.00(0.73–1.38)720.0002 White0.89(0.79–1.00)0.84(0.69–1.03)550.02 European0.89(0.78–1.02)0.85(0.67–1.07)590.03 Asian 1.03(0.86–1.22) 1.07(0.75–1.53)720.0008 East Asian0.82(0.67–1.01)0.85(0.58–1.23)600.04a East Asian is composed of Chinese and Korean.demonstrated that a single search engine does not provide all of the pertinent articles,and combining more databases yields greater coverage of possible articles[35].Conference proceedings and jour-nal supplements should also be searched to ensure that relevant remaining reports are identified.However,additional assessments of databases other than PubMed and EMBASE should be analyzed with caution,due to a potential lack of quality in study design. Although the other meta-analysis included more publications in its analysis,one study may not suitable for the subgroup analysis according to age[36].In this study,cases and controls were not matched for age and gender(P<0.05).Krajinovic et al.found a protective effect of MTHFR polymor-phisms in children born before1996(about the time that Health Canada recommended folate supplementation during pregnancy) but not in children born later[14].More conceivable would be the relation between folate status and genotype in adult ALL,where folate status might be more conditional on the subject’s own geno-type and folate intake.In studies of breast cancer risk,high folate intake may be more protective in women with the polymorphism than in those with the wild type[37,38].Thesefindings demon-strate that the risks associated with the MTHFR677TT genotype vary depending on folate status.Genetic and/or environmental exposures are required for cancer to develop.None of the studies to date has assessed dietary folate intake to evaluate whether overall folate status may have modified the relation between having the MTHFR genotype and one’s risk of developing leukemia.We cannot rule out the possibility that the C677T variant plays a major role in risk modulation in pediatric ALL for populations with inadequate folate intake.Considering some limitations of this meta-analysis,our results should be interpreted with caution.Firstly,heterogeneity is a potential problem when interpreting the results from any meta-analysis.We minimized the likelihood of encountering het-erogeneity problems by performing a careful search for published studies and using explicit criteria for study inclusion,precise data extraction,and strict data analysis.Significant between-study heterogeneity existed in almost each comparison.Heterogene-ity can result from study differences in the selection of controls, age distribution,lifestyle factors,and so on.There are major differences of genetic background within the Asian population studied,and it should be stratified to add moreflavor to the subject.Secondly,only published studies were included in this meta-analysis.The presence of publication bias indicates that non-significant or negativefindings may be stly,our results were based on unadjusted estimates,while a more pre-cise analysis should be conducted using individual data if they were available,which would allow researchers to adjust covari-ates including age,ethnicity,family history,environmental factors, and lifestyle.In conclusion,although studies investigating the association between MTHFR C667T polymorphism and the risk of childhood ALL arrive at different conclusions,this meta-analysis suggests that MTHFR C667T polymorphism is not associated with childhood ALL.Conflict of interestWe declare that we have nofinancial and personal relationships with other people or organizations that can inappropriately influ-ence our work,there is no professional or other personal interest of any nature or kind in any product,service and company that could be construed as influencing the position presented in,or the review of,the manuscript.AcknowledgementsContributions.JW,PZ and JO conceived and designed the study. JW,PZ and BC did the electronic search,data collection,abstrac-tion,hand-search of journals,and data entry;RZ and YY were responsible for the quality assessment of trials and quality scores; JW and PZ were statistical advisers;JW,BC,RZ and JO were responsible for the overall direction of the text and discus-sion.1600J.Wang et al./Leukemia Research34 (2010) 1596–1600References[1]Chen CL,Liu Q,Pui CH,Rivera GK,Sandlund JT,Ribeiro R,et al.Higher frequencyof glutathione Stransferase deletions in black children with acute lymphoblas-tic leukemia.Blood1997;89(5):1701–7.[2]Sinnett D,Krajinovic M,Labuda D.Genetic susceptibility to childhood acutelymphoblastic leukemia.Leuk Lymphoma2000;38(5–6):447–62.[3]Gilliland DG.Molecular genetics of human leukemia.Leukemia1998;12(Suppl.1):S7–12.[4]Smith MT,McHale CM,Wiemels JL,Zhang L,Wiencke JK,Zheng S,et al.Molec-ular biomarkers for the study of childhood leukemia.Toxicol Appl Pharmacol 2005;206(2):237–45.[5]Cnattingius S,Zack MM,Ekbom A,Gunnarskog J,Kreuger A,Linet M,et al.Prenatal and neonatal risk factors for childhood lymphatic leukemia.J Natl Cancer Inst1995;87(12):908–14.[6]Frosst P,Blom HJ,Milos R,Goyette P,Sheppard CA,Matthews RG,et al.Acandidate genetic risk factor for vascular disease:a common mutation in methylenetetrahydrofolate reductase.Nat Genet1995;10(1):111–3.[7]Dong LM,Potter JD,White E,Ulrich CM,Cardon LR,Peters U.Genetic sus-ceptibility to cancer:the role of polymorphisms in candidate genes.JAMA 2008;299(20):2423–36.[8]Franco RF,Simões BP,Tone LG,Gabellini SM,Zago MA,Falcão RP.Themethylenetetrahydrofolate reductase C677T gene polymorphism decreases the risk of childhood acute lymphocytic leukaemia.Br J Haematol 2001;115(3):616–8.[9]Jiang H,Gu LJ,Xue HL.Methylenetetrahydrofolate reductase gene polymor-phism of childhood acute lymphocytic leukaemia.Zhonghua Xue Ye Xue Za Zhi2004;25(7):439–40.[10]Wiemels JL,Smith RN,Taylor GM,Eden OB,Alexander FE,Greaves MF.Methylenetetrahydrofolate reductase(MTHFR)polymorphisms and risk of molecularly defined subtypes of childhood acute leukemia.Proc Natl Acad Sci USA2001;98(7):4004–9.[11]Balta G,Yuksek N,Ozyurek E,Ertem U,Hicsonmez G,Altay C,et al.Character-ization of MTHFR,GSTM1,GSTT1,GSTP1,and CYP1A1genotypes in childhood acute leukemia.Am J Hematol2003;73(3):154–60.[12]Zintzaras E,Koufakis T,Ziakas PD,Rodopoulou P,Giannouli S,Voulgarelis M.A meta-analysis of genotypes and haplotypes of methylenetetrahydrofolatereductase gene polymorphisms in acute lymphoblastic leukemia.Eur J Epi-demiol2006;21(7):501–10.[13]Pereira TV,Rudnicki M,Pereira AC,Pombo-de-Oliveira MS,Franco RF.5,10-Methylenetetrahydrofolate reductase polymorphisms and acute lym-phoblastic leukemia risk:a meta-analysis.Cancer Epidemiol Biomark Prev 2006;15(10):1956–63.[14]Krajinovic M,Lamothe S,Labuda D,Lemieux-Blanchard E,Theoret Y,MoghrabiA,et al.Role of MTHFR genetic polymorphisms in the susceptibility to childhood acute lymphoblastic leukemia.Blood2004;103(1):252–7.[15]Thirumaran RK,Gast A,Flohr T,Burwinkel B,Bartram C,Hemminki K,et al.MTHFR genetic polymorphisms and susceptibility to childhood acute lym-phoblastic leukemia.Blood2005;106(7):2590–1.[16]Oliveira E,Alves S,Quental S,Ferreira F,Norton L,Costa V,et al.The MTHFRC677T and A1298C polymorphisms and susceptibility to childhood acute lym-phoblastic leukemia in Portugal.J Pediatr Hematol Oncol2005;27(8):425–9.[17]Schnakenberg E,Mehles A,Cario G,Rehe K,Seidemann K,Schlegelberger B,et al.Polymorphisms of methylenetetrahydrofolate reductase(MTHFR)and susceptibility to pediatric acute lymphoblastic leukemia in a German study population.BMC Med Genet2005;6:23.[18]Chatzidakis K,Goulas A,Athanassiadou-Piperopoulou F,Fidani L,Koliouskas D,Mirtsou V.Methylenetetrahydrofolate reductase C677T polymorphism:asso-ciation with risk for childhood acute lymphoblastic leukemia and response during the initial phase of chemotherapy in Greek patients.Pediatr Blood Can-cer2006;47(2):147–51.[19]Zanrosso CW,Hatagima A,Emerenciano M,Ramos F,Figueiredo A,Félix TM,et al.The role of methylenetetrahydrofolate reductase in acute lymphoblastic leukemia in a Brazilian mixed population.Leuk Res2006;30(4):477–81.[20]Yu H,Jin RM,Bai Y.The relationship between the methylenetetrahydrofo-late reductase C677T gene polymorphism and acute lymphocytic leukemia in children.Lin Chuang Xue Ye Xue Za Zhi2006;19(4):205–9.[21]Reddy H,Jamil K.Polymorphisms in the MTHFR gene and their possible associ-ation with susceptibility to childhood acute lymphocytic leukemia in an Indian population.Leuk Lymphoma2006;47(7):1333–9.[22]Kim NK,Chong SY,Jang MJ,Hong SH,Kim HS,Cho EK,et al.Associa-tion of the methylenetetrahydrofolate reductase polymorphism in Korean patients with childhood acute lymphoblastic leukemia.Anticancer Res 2006;26(4B):2879–81.[23]Kamel AM,Moussa HS,Ebid GT,Bu RR,Bhatia KG.Synergistic effect of methyl-tetrahydrofolate reductase(MTHFR)C677T and A1298C polymorphism as risk modifiers of pediatric acute lymphoblastic leukemia.J Egypt Natl Canc Inst 2007;19(2):96–105.[24]Petra BG,Janez J,Vita D.Gene–gene interactions in the folate metabolic path-way influence the risk for acute lymphoblastic leukemia in children.Leuk Lymphoma2007;48(4):786–92.[25]Giovannetti E,Ugrasena DG,Supriyadi E,Vroling L,Azzarello A,de Lange D,et al.Methylenetetrahydrofolate reductase(MTHFR)C677T and thymidylate synthase promoter(TSER)polymorphisms in Indonesian children with and without leukemia.Leuk Res2008;32(1):19–24.[26]Alcasabas P,Ravindranath Y,Goyette G,Haller A,Del Rosario L,Lesaca-MedinaMY,et al.5,10-Methylenetetrahydrofolate reductase(MTHFR)polymorphisms and the risk of acute lymphoblastic leukemia(ALL)in Filipino children.Pediatr Blood Cancer2008;51(2):178–82.[27]Liu JX,Chen JP,Lin DX.Polymorphisms in the MTHFR gene and their possibleassociation with susceptibility to acute lymphocytic leukemia.Jie Fang Jun Za Zhi2008;33(11):1291–3.[28]de Jonge R,Tissing WJ,Hooijberg JH,Jansen G,Kaspers GJ,Lindemans J,et al.Polymorphisms in folate-related genes and risk of pediatric acute lymphoblas-tic leukemia.Blood2009;113(10):2284–9.[29]Kim HN,Kim YK,Lee IK,Yang DH,Lee JJ,Shin MH,et al.Association betweenpolymorphisms of folate-metabolizing enzymes and hematological malignan-cies.Leuk Res2009;33(1):82–7.[30]Yeoh AE,Lu Y,Chan JY,Chan YH,Ariffin H,Kham SK,et al.Genetic sus-ceptibility to childhood acute lymphoblastic leukemia shows protection in Malay boys:results from the Malaysia–Singapore ALL Study Group.Leuk Res 2010;34(3):276–83.[31]Hirschhorn JN,Lohmueller K,Byrne E.A comprehensive review of genetic asso-ciation studies.Genet Med2002;4:45–61.[32]Deligezer U,Akisik E,Dalay N.Genotyping of the MTHFR gene polymor-phism,C677T in patients with leukemia by melting curve analysis.Mol Diagn 2003;7(3–4):181–5.[33]Gemmati D,Ongaro A,Scapoli GL,Della Porta M,Tognazzo S,Serino ML,etmon gene polymorphisms in the metabolic folate and methylation pathway and the risk of acute lymphoblastic leukemia and non-Hodgkin’s lymphoma in adults.Cancer Epidemiol Biomarkers Prev2004;13(5):787–94.[34]Shuman AL.For literature searches,is Medline enough?Perception of an ade-quate literature b Anim(NY)2004;33(2):15–6.[35]Brand-de Heer DL.A comparison of the coverage of clinical medicine providedby PASCAL BIOMED and MEDLINE.Health Info Libr J2001;18(2):110–6. [36]Chiusolo P,Reddiconto G,Cimino G,Sica S,Fiorini A,Farina G,et al.Methylenetetrahydrofolate reductase genotypes do not play a role in acute lymphoblastic leukemia pathogenesis in the Italian population.Haematologica 2004;89(2):139–44.[37]Chen J,Gammon MD,Chan W,Palomeque C,Wetmur JG,Kabat GC,et al.One-carbon metabolism,MTHFR polymorphisms,and risk of breast cancer.Cancer Res2005;65(4):1606–14.[38]Shrubsole MJ,Gao YT,Cai Q,Shu XO,Dai Q,Hébert JR,et al.MTHFR poly-morphisms,dietary folate intake,and breast cancer risk:results from the Shanghai Breast Cancer Study.Cancer Epidemiol Biomark Prev2004;13(2): 190–6.。