帕洛诺司琼(止若)
- 格式:pdf
- 大小:3.75 MB
- 文档页数:29
(一)甘利欣:适应症:适用于伴有谷丙氨基转移酶升高的急、慢性病毒性肝炎的治疗。
产品口号:用时省心、用完放心产品定位:各种原因所致肝损伤治疗的经典药物主要竞品:甘利欣;美能;阿拓莫兰;古拉定;易善复;凯西莱(二)天晴甘美:适应症:适用于慢性病毒性肝炎。
改善肝功能异常。
产品口号:快速抗炎,迅速恢复肝功能产品定位:天晴甘美注射剂,快速,强效抗炎,是住院期肝功能损伤患者治疗的第一选择(三)天晴甘平:适应症:适用于伴有谷丙氨基转移酶升高的急、慢性肝炎的治疗。
【产品优势】提高了甘草酸口服生物利用度,显著增强疗效;甘草酸与磷脂双效协同高效持久;安全性更高;长期治疗能达到持续抗炎,稳定肝功能、阻止肝纤维化进展之效;专利金奖产品,具有制剂、组合物两项专利。
产品口号:双效协同保肝,高效持久安全产品定位:持久抗炎,稳定肝功能---------病毒性肝炎;药物性肝病;酒精性肝病和脂肪肝(四)润众:适应症:本品适用于病毒复制活跃,血清转氨酶ALT持续升高或肝脏组织学显示有活动性病变的慢性成人乙型肝炎的治疗。
产品特点:强效、快速、低耐药产品优势:首家上市;润众与博路定同品同质;价格合理产品口号:恩润广众,让更多慢乙肝患者受益的恩替卡韦产品定位:慢乙肝初治患者首选用药;阿德福韦酯(ADV)应答不佳患者的最佳选择主要竞品:名正;代丁;贺维力;阿迪仙;贺普丁;博路定;素比伏;润众,和恩/和定(五)名正:适应症:适用于治疗有乙型肝炎病毒活动复制证据,并伴有血清氨基酸转移酶(ALT或AST)持续升高或肝脏组织学活动性病变的肝功能代偿的成年慢性乙型肝炎患者。
产品特点:持久低耐药,安全无交叉产品口号:名正言顺,言之有理的选择,顺利的进行抗病毒治疗。
主要竞品:博路定;素比伏;贺普丁;阿迪仙;贺维力;代丁;名正;(六)天晴复欣:适应症:用于慢性乙型病毒性肝炎及肿瘤放疗、化疗引起的白细胞低下和其它原因引起的白细胞减少症。
产品口号:植物干扰素产品定位:病毒性肝炎;肝炎肝硬化;免疫低下患者主要竞品:1) 恒迈-苦参素氯化钠注射液0.6g:100ml,36元,江苏恒瑞医药2) 博尔泰力-宁夏博尔泰力药业股份有限公司,2ml:200mg*10支/盒,80元。
帕洛诺司琼在胃肠癌化疗过程中止吐的临床分析摘要】目的探讨帕洛诺司琼在胃肠癌化疗过程中止吐效果。
方法选取本院2011年10月~2013年10月诊治的胃肠癌化疗患者104例,采用数字随机法分为两组,52例患者采用恩丹西酮治疗为对照组,52例患者采用帕洛诺司琼治疗为观察组,比较两组患者的止吐效果。
结果观察组患者急性呕吐的止吐总有效率(96.2%)、迟发性呕吐的止吐总有效率(94.2%)均明显高于对照组(82.7%)、(80.8%),差异有统计学意义(p<0.05)。
结论帕洛诺司琼在胃肠癌化疗过程中止吐效果显著,不仅起效快且作用时间长,值得临床推广使用。
【关键词】帕洛诺司琼胃肠癌化疗止吐恩丹西酮【中图分类号】R969 【文献标识码】A 【文章编号】2095-1752(2014)09-0259-02胃肠癌是临床常见的恶性肿瘤疾病,会明显影响到患者的饮食,大幅降低患者的生活质量,影响患者的预后[1]。
目前临床治疗胃肠癌的首选方案为手术治疗,但术后需要给予患者化疗,才能有效杀灭残留病灶,提高治疗效果,化疗也会引发不同程度的不良反应[2-3],呕吐就是最为常见的一种。
为了探讨帕洛诺司琼在胃肠癌化疗过程中止吐效果,本院选取2011年10月~2013年10月诊治的胃肠癌化疗患者104例,采用数字随机法分为两组,行恩丹西酮和帕洛诺司琼治疗,针对两组患者的止吐效果进行对比分析,现报告如下。
1.资料与方法1.1资料本院2011年10月~2013年10月诊治的胃肠癌化疗患者104例,经胃肠镜检查和病理组织学检查确诊,Karnofsky评分均高于60分,排除患有其他心肺疾病、肝肾疾病、血液性疾病、感染性疾病、免疫性疾病、精神疾病的患者。
采用数字随机法分为两组,52例患者采用恩丹西酮治疗为对照组,年龄为53~76岁,平均年龄为61.7±10.4岁,其中男性34例,女性18例。
52例患者采用帕洛诺司琼治疗为观察组,年龄为55~74岁,平均年龄为62.0±8.5岁,其中男性33例,女性19例。
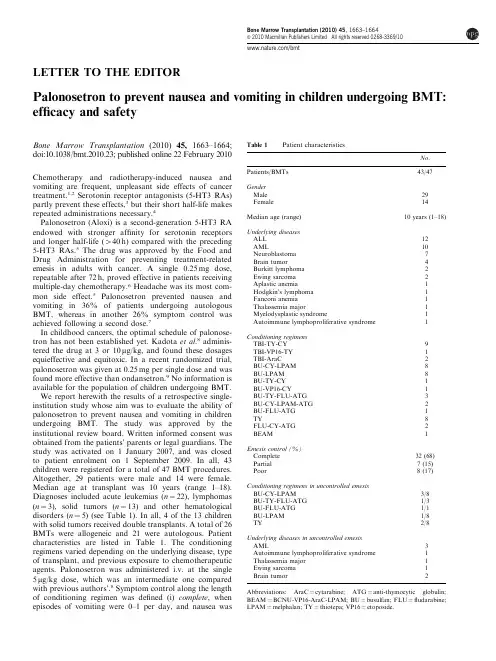
LETTER TO THE EDITORPalonosetron to prevent nausea and vomiting in children undergoing BMT: efficacy and safetyBone Marrow Transplantation(2010)45,1663–1664; doi:10.1038/bmt.2010.23;published online22February2010 Chemotherapy and radiotherapy-induced nausea and vomiting are frequent,unpleasant side effects of cancer treatment.1,2Serotonin receptor antagonists(5-HT3RAs) partly prevent these effects,3but their short half-life makes repeated administrations necessary.4Palonosetron(Aloxi)is a second-generation5-HT3RA endowed with stronger affinity for serotonin receptors and longer half-life(440h)compared with the preceding 5-HT3RAs.5The drug was approved by the Food and Drug Administration for preventing treatment-related emesis in adults with cancer.A single0.25mg dose, repeatable after72h,proved effective in patients receiving multiple-day chemotherapy.6Headache was its most com-mon side effect.5Palonosetron prevented nausea and vomiting in36%of patients undergoing autologous BMT,whereas in another26%symptom control was achieved following a second dose.7In childhood cancers,the optimal schedule of palonose-tron has not been established yet.Kadota et al.8adminis-tered the drug at3or10m g/kg,and found these dosages equieffective and equitoxic.In a recent randomized trial, palonosetron was given at0.25mg per single dose and was found more effective than ondansetron.9No information is available for the population of children undergoing BMT. We report herewith the results of a retrospective single-institution study whose aim was to evaluate the ability of palonosetron to prevent nausea and vomiting in children undergoing BMT.The study was approved by the institutional review board.Written informed consent was obtained from the patients’parents or legal guardians.The study was activated on1January2007,and was closed to patient enrolment on1September2009.In all,43 children were registered for a total of47BMT procedures. Altogether,29patients were male and14were female. Median age at transplant was10years(range1–18). Diagnoses included acute leukemias(n¼22),lymphomas (n¼3),solid tumors(n¼13)and other hematological disorders(n¼5)(see Table1).In all,4of the13children with solid tumors received double transplants.A total of26 BMTs were allogeneic and21were autologous.Patient characteristics are listed in Table 1.The conditioning regimens varied depending on the underlying disease,type of transplant,and previous exposure to chemotherapeutic agents.Palonosetron was administered i.v.at the single 5m g/kg dose,which was an intermediate one compared with previous authors’.8Symptom control along the length of conditioning regimen was defined(i)complete,when episodes of vomiting were0–1per day,and nausea was Table1Patient characteristicsNo. Patients/BMTs43/47 GenderMale29 Female14 Median age(range)10years(1–18) Underlying diseasesALL12AML10 Neuroblastoma7 Brain tumor4 Burkitt lymphoma2 Ewing sarcoma2 Aplastic anemia1 Hodgkin’s lymphoma1 Fanconi anemia1 Thalassemia major1 Myelodysplastic syndrome1 Autoimmune lymphoproliferative syndrome1 Conditioning regimensTBI-TY-CY9TBI-VP16-TY1TBI-AraC2BU-CY-LPAM8BU-LPAM8BU-TY-CY1BU-VP16-CY1BU-TY-FLU-ATG3BU-CY-LPAM-ATG2BU-FLU-ATG1TY8FLU-CY-ATG2 BEAM1 Emesis control(%)Complete32(68) Partial7(15) Poor8(17) Conditioning regimens in uncontrolled emesisBU-CY-LPAM3/8BU-TY-FLU-ATG1/3BU-FLU-ATG1/1BU-LPAM1/8TY2/8 Underlying diseases in uncontrolled emesisAML3 Autoimmune lymphoproliferative syndrome1 Thalassemia major1 Ewing sarcoma1 Brain tumor2 Abbreviations:AraC¼cytarabine;ATG¼anti-thymocytic globulin; BEAM¼BCNU-VP16-AraC-LPAM;BU¼busulfan;FLU¼fludarabine; LPAM¼melphalan;TY¼thiotepa;VP16¼etoposide.Bone Marrow Transplantation(2010)45,1663–1664&2010Macmillan Publishers Limited All rights reserved0268-3369/10/bmtscored o1according to the NCI Common Toxicity Criteria,version2.0,10(ii)partial,when vomiting episodes were2–5per day,but responded to dexamethasone, and(iii)poor,when vomiting episodes were45per day. Delayed vomiting that occurred after410days from starting the conditioning regimen was excluded from analysis,as it was considered possibly secondary to aplasia-related mucositis.Nausea and vomiting were completely controlled by a single palonosetron dose for32of47transplants(68%), and partially controlled for additional7(15%),all responsive to dexamethasone.Finally,symptoms were poorly controlled for the last eight transplants(17%),but receded after a second drug dose given on day5of the conditioning regimen.Efficacy of palonosetron did not correlate with the underlying disease,nor with conditioning regimen(see Table1).No adverse side effects attributable to the drug were reported.Our data suggest that palonosetron is a valuable option for preventing chemotherapy and radiotherapy-induced nausea and vomiting in children undergoing BMT. Compared with other5-HT3RAs,palonosetron was more easily manageable and cost-effective,as efficacy was achieved with fewer administrations of the drug.In our study,by using5m g/kg single-dose schedule,only17%of BMTs required a second drug dose,which was always effective and devoid of side effects.This is possibly the first report on testing palonosetron in children under-going BMTs.Its efficacy,associated with the feasibility of administration and safety,suggest the possibility of its widespread use for preventing nausea and vomiting in children undergoing intensive conditioning regimens for BMT.Further studies on larger pediatric series are warranted.Conflict of interestThe authors declare no conflict of interest. AcknowledgementsWe thank Dr Bruno De Bernardi and Ms Valerie Perricone for revising the paper,and Ms Alessandra Trocino for secretarial assistance.M Ripaldi1,R Parasole2,G De Simone1,MR D’Amico1,R Migliorati2,G Zanotta2,G Loffredo2,F Petruzziello2and V Poggi21BMT Unit,Department of Pediatric Hemato-Oncology,Santobono-Pausilipon Hospital,Napoli,Italy and2Department of Pediatric Hemato-Oncology,Santobono-Pausilipon Hospital,Napoli,ItalyE-mail:rparasol@libero.itReferences1Navari RM.Pharmacological management of chemotherapy-induced nausea and vomiting:focus on recent developments.Drugs2009;69:515–533.2Hesketh PJ,Kris MG,Grunberg SM,Beck T,Hainsworth JD, Harker G et al.Proposal for classification of the acute emetogenicity of cancer chemotherapy.J Clin Oncol1997;15:103–109.3Osoba D,Zee B,Warr D,Latreille J,Kaizer L,Pater J.Effect of post-chemotherapy nausea and vomiting on health related quality of life.Support Care Cancer1997;5:307–313.4The Antiemetic Subcommittee of the Multinational Associa-tion of Supportive Care in Cancer(MASCC).Prevention of chemotherapy-and radiotherapy-induced emesis results of the 2004Perugia International Antiemetic Consensus Conference.Ann Oncol2006;17:20–28.5Gralla R,Lichinitser M,Van Der Vegt S,Sleeboom H, Mezger J,Peschel C et al.Palonosetron improves prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy:results of a double-blind randomized phase III trial comparing single doses of palonosetron with ondansetron.Ann Oncol2003;14: 1570–1577.6Musso M,Scalone R,Bonanno V,Crescimanno A,Polizzi V, Porretto F et al.Palonosetron and dexamethasone for the prevention of acute and delayed nausea and vomiting in patients receiving multiple-day chemotherapy.Support Care Cancer2009;17:205–209.7Musso M,Scalone R,Crescimanno A,Bonanno V,Polizzi V, Porretto F et al.Palonosetron and dexamethasone for prevention of nausea and vomiting in patients receiving high-dose chemotherapy with auto-SCT.Bone Marrow Transplant 2010;45:123–127.8Kadota R,Shen V,Messinger Y.Safety,pharmacokinetics, and efficacy of palonosetron in pediatric patients:a stratified, double-blind,phase3,randomized study.Proc Am Soc Clin Oncol2007;25(Suppl18):S(abstract9570)p.543.9Sepu lveda-Vildosola AC,Betanzos-Cabrera Y,Lastiri GG, Rivera-Marquez H,Villasis-Keever MA,Wanzke del Algel V et al.Palonosetron hydrochloride is an effective and safe option to prevent chemotherapy-induced nausea and vomiting in children.Arch Med Research2008;39:601–606.10National Cancer Institute.Cancer Therapy Evaluation mon Toxicity Criteria Version2.0April30,1999..Letter to the Editor 1664Bone Marrow Transplantation。
核准日期:修改日期:盐酸帕洛诺司琼注射液说明书请仔细阅读说明书并在医师指导下使用。
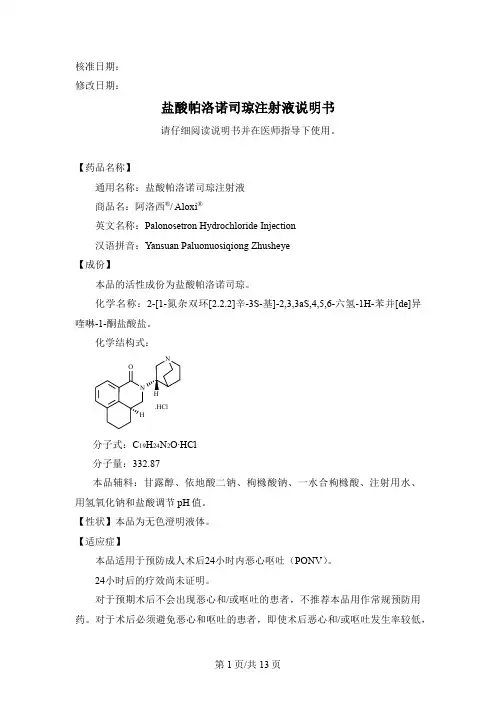
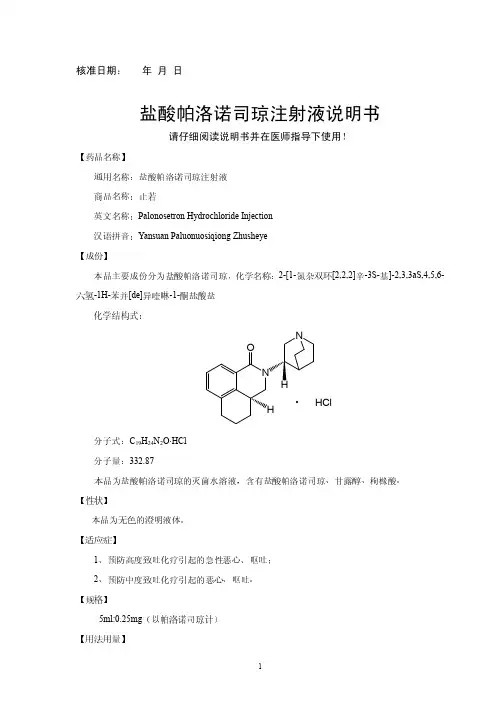
【药品名称】通用名称:盐酸帕洛诺司琼注射液商品名:阿洛西®/ Aloxi ®英文名称:Palonosetron Hydrochloride Injection汉语拼音:Yansuan Paluonuosiqiong Zhusheye【成份】本品的活性成份为盐酸帕洛诺司琼。
化学名称:2-[1-氮杂双环[2.2.2]辛-3S-基]-2,3,3aS,4,5,6-六氢-1H-苯并[de]异喹啉-1-酮盐酸盐。
化学结构式:.HClN OH分子式:C 19H 24N 2O∙HCl分子量:332.87本品辅料:甘露醇、依地酸二钠、枸橼酸钠、一水合枸橼酸、注射用水、用氢氧化钠和盐酸调节pH 值。
【性状】本品为无色澄明液体。
【适应症】本品适用于预防成人术后24小时内恶心呕吐(PONV )。
24小时后的疗效尚未证明。
对于预期术后不会出现恶心和/或呕吐的患者,不推荐本品用作常规预防用药。
对于术后必须避免恶心和呕吐的患者,即使术后恶心和/或呕吐发生率较低,也推荐使用本品。
【规格】1.5mL: 0.075mg(按C19H24N2O计)【用法用量】推荐剂量为:麻醉诱导前,单次静脉注射本品0.075mg(1支),注射时间应超过10秒。
本品浓度为0.05 mg/ml (50 mcg/ ml),可直接静脉给药。
本品不可与其他药物混合。
输液前和输液后应使用生理盐水冲洗输液管路。
在给药前应检查其中是否含有可见的颗粒物,以及是否变色。
特殊人群肾脏损害任何程度的肾功能损害患者均不需要调整剂量。
肝脏损害任何程度的肝功能损害患者均不需要调整剂量。
儿童用药尚未在儿科患者中确定预防术后恶心和呕吐的安全性和有效性。
老年用药用于老年患者的有效性尚未充分评估。
对老年患者无需调整剂量或特殊监护。
【不良反应】由于临床试验的实施条件差异很大,因此在一种药物的临床试验中观察到的不良反应率无法与另一种药物的临床试验中观察到的不良反应率进行直接比较,且不能反映临床实践中观察到的发生率。
盐酸帕洛诺司琼注射怎么用
关于《盐酸帕洛诺司琼注射怎么用》,是我们特意为大家整理的,希望对大家有所帮助。
盐酸帕洛诺司琼是临床医学上普遍服药,尤其是在大家犯恶心干呕的情况下,盐酸帕洛诺司琼的运用则十分普遍。
盐酸帕洛诺司琼对身体的治疗效果是较为显著的,可是在运用这类药的情况下也是有很多需要留意的地区。
除开功效,主要用途还要考虑到人体是不是可用。
那盐酸帕洛诺司琼注射如何使用?
1.主要用途
盐酸帕洛诺司琼是一种抑止恶心干呕药,归属于新式高可选择性、高亲和性5-HT3受体拮抗剂,它可阻隔呕吐反射面神经中
枢颈静脉神经细胞的神经递质前5-HT。
蛋白激酶的激动,并立即影响神经中枢系统内5-HT。
蛋白激酶激动造成的欲望根据交感神经传承前区的功效,阻隔肠胃中交感神经末梢神经,阻拦数据信号传送至5-HT。
蛋白激酶开启区,降低恶心想吐和呕吐的发病率。
临床医学上用以医治由中、中重度致吐性化疗药造成的亚急性、延迟时间性恶心想吐和呕吐。
因其具备功效高、毒副作用小、药物半衰期长(约40 h)、服药使用量小等特性而备受关注。
2.适用范围
防止高宽比致吐放疗造成的亚急性恶心想吐、呕吐。
防止轻中度致吐放疗造成的恶心想吐、呕吐。
禁止使用于己知对该药品或药品中一切双组分皮肤过敏的病人。
3.留意
盐酸帕洛诺司琼的过敏症状可能产生于对其他可选择性5-HT3受体拮抗剂过敏症状。
针对身患或可能发展趋势为心脏传输间期增加的患者,尤其是QTC 增加的患者应慎重应用帕洛诺司琼。
盐酸帕洛诺司琼注射液不可以跟别的药品混和。
孕妇及哺乳期间谨慎使用。
帕洛诺司琼结构特点
1. 帕洛诺司琼的结构可独特啦!就好像一个精密设计的小机器,每个部分都有着关键作用。
比如说在药物发挥作用的时候,它的结构就像是精准的导航仪,指引着药物去到该去的地方,这是不是超级厉害!
2. 你知道吗,帕洛诺司琼的结构特点就像是一个复杂但有序的拼图!每一块都恰到好处地拼在一起。
就如同在治疗疾病时,它的结构能完美契合,发挥出强大的效果,你说神奇不神奇!
3. 哎呀呀,帕洛诺司琼的结构特点真的超有趣!就仿佛是一个神秘的宝藏地图,指引着我们去探索它的奇妙之处。
当我们了解它的结构,不就像是找到了打开宝藏的钥匙吗!
4. 帕洛诺司琼的结构那可真是不一般!好比是一座坚固的城堡,各个部分紧密相连。
比如在应对不良反应的时候,它的结构就像坚实的城墙,牢牢守护着健康,是不是很了不起!
5. 喂喂喂,瞧瞧帕洛诺司琼的结构特点呀!就跟神奇的魔法道具一样。
当它工作起来的时候,就像是魔法生效了,效果出奇的好,这也太让人惊讶了吧!
6. 哇哦,帕洛诺司琼的结构可是有大讲究的哟!类似于一个高超的乐团,每个乐器都不可或缺。
而在发挥药效的过程中,它的结构就像完美的合奏,奏响健康的乐章,厉害吧!
7. 嘿,帕洛诺司琼的结构特点简直太特别啦!就如同是一辆超级赛车的设计图。
当药物奔跑在身体里的赛道时,它的结构让它风驰电掣般发挥作用,太酷了吧!
8. 帕洛诺司琼的结构真的很奇妙啊!就好像是宇宙中一颗独特的星星。
在医疗的天空中,它的结构特点让它闪闪发光,为人们带来希望!我觉得帕洛诺司琼真的是一种非常神奇且重要的药物,它的结构特点是其发挥强大作用的关键呢!。
盐酸帕洛诺司琼立题目的与依据3.1盐酸帕洛诺司琼概述盐酸帕洛诺司琼是一种新型高选择性、高亲和性的5-HT3受体拮抗剂, 临床上用于中到重度致吐性化疗药物引起的急性和延迟性恶心和呕吐。
盐酸帕洛诺司琼及其注射液剂型由瑞士Helsinn Healthcare公司研制开发,于2003年7月首次在美国上市时间,商品名为Aloxi,其主要特点是疗效高、毒副作用小、半衰期长、用药剂量小。
3.2国内外研究或生产使用情况3.2.1盐酸帕洛诺司琼的研究进程盐酸帕洛诺司琼由美国Syntex公司(现属瑞士罗氏生物技术公司)Berger, J等人在1991年合成,罗氏生物技术公司将开发和上市盐酸帕洛诺司琼的权利以及盐酸帕洛诺司琼的全球专利转让给了瑞士的Helsinn公司。
1996年,Helsinn Healthcare公司研发的盐酸帕洛诺司琼在进行II期临床时因故搁浅,2001年,Helsinn公司将美国和加拿大的独占权和地区销售权授予了MGI制药公司并和美国MGI公司结成合作伙伴继续对盐酸帕洛诺司琼的临床研究。
2000年4月起,在北美和欧洲的130多个医疗中心进行了盐酸帕洛诺司琼用于治疗化疗诱导恶心和呕吐的III期临床,有1800多名癌症患者参加。
该试验比较了静注盐酸帕洛诺司琼和应用当前市场上销售的5-HT3受体拮抗剂的效果,2002年中,Helsinn和MGI Pharma公司宣布盐酸帕洛诺司琼的核心III期临床试验完成,并开始进行数据分析工作。
III期临床先导试验结果的初步分析显示盐酸帕洛诺司琼比现在市售的5-HT3受体拮抗剂效果更好。
2002年第三季度,两公司依据从3个随机、双盲、安慰剂对照III期临床中得到的数据向美国FDA提出申请将盐酸帕洛诺司琼用于治疗化疗诱发的恶心和呕吐,2003年7月,盐酸帕洛诺司琼静脉注射剂型在美国获得批准,商品名为Aloxi,同年9月在美国首次上市。
3.2.2国外使用情况在美国,盐酸帕洛诺司琼由MGI公司以Aloxi为商品名进行销售,盐酸帕洛诺司琼上市后第二季度就被卫生界人士和癌症患者广泛接受,约有17.5万个剂量被应用,很快成为预防恶心和呕吐的首选药,本品上市当年即赢得了970万美圆的销售额,建立了12.5万人的患者群,2004年一季度创下了1860万美圆的销售额,占据了MGI公司一季度销售额的69%。
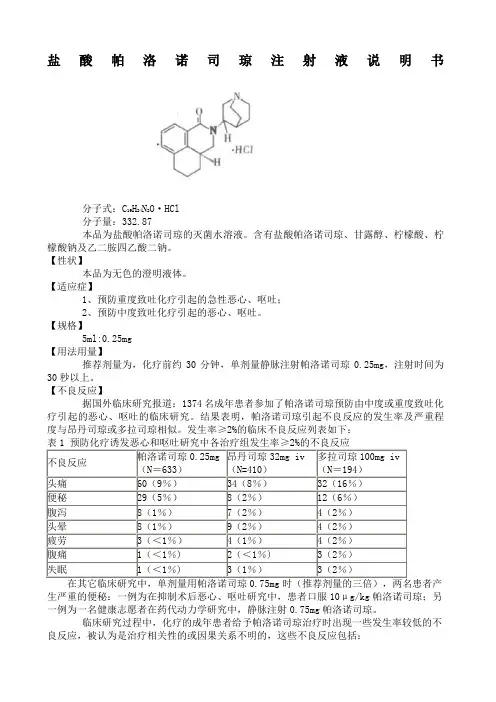
盐酸帕洛诺司琼注射液说明书分子式:C19H24N2O·HCl分子量:332.87本品为盐酸帕洛诺司琼的灭菌水溶液。
含有盐酸帕洛诺司琼、甘露醇、柠檬酸、柠檬酸钠及乙二胺四乙酸二钠。
【性状】本品为无色的澄明液体。
【适应症】1、预防重度致吐化疗引起的急性恶心、呕吐;2、预防中度致吐化疗引起的恶心、呕吐。
【规格】5ml:0.25mg【用法用量】推荐剂量为,化疗前约30分钟,单剂量静脉注射帕洛诺司琼0.25mg,注射时间为30秒以上。
【不良反应】据国外临床研究报道:1374名成年患者参加了帕洛诺司琼预防由中度或重度致吐化疗引起的恶心、呕吐的临床研究。
结果表明,帕洛诺司琼引起不良反应的发生率及严重程度与昂丹司琼或多拉司琼相似。
发生率≥2%的临床不良反应列表如下:不良反应帕洛诺司琼0.25mg(N=633)昂丹司琼32mg iv(N=410)多拉司琼100mg iv(N=194)头痛60(9%)34(8%)32(16%)便秘29(5%)8(2%)12(6%)腹泻8(1%)7(2%)4(2%)头晕8(1%)9(2%)4(2%)疲劳3(<1%)4(1%)4(2%)腹痛1(<1%)2(<1%)3(2%)失眠1(<1%)3(1%)3(2%)生严重的便秘:一例为在抑制术后恶心、呕吐研究中,患者口服10μg/kg帕洛诺司琼;另一例为一名健康志愿者在药代动力学研究中,静脉注射0.75mg帕洛诺司琼。
临床研究过程中,化疗的成年患者给予帕洛诺司琼治疗时出现一些发生率较低的不良反应,被认为是治疗相关性的或因果关系不明的,这些不良反应包括:心血管系统:发生率1%:间歇性的心动过速、心动过缓、低血压;发生率<1%:高血压、心肌缺血、期外收缩、窦性心动过速、窦性心律失常、室上性期外收缩、QT间期延长。
多数病例与帕洛诺司琼的关系不明确。
皮肤:发生率<1%:过敏性皮炎、出疹。
视力和听力:发生率<1%:运动病、耳鸣、眼刺激和弱视。