坐骨神经阻滞xjq
- 格式:ppt
- 大小:958.50 KB
- 文档页数:12
坐骨神经阻滞麻醉的小知识人体最粗大的神经便是坐骨神经,人们在足部手术及膝关节下部手术过程中可利用坐骨神经麻醉阻滞技术,单一利用坐骨神经麻醉阻滞能让患者的小腿内部及足部内侧面区域麻醉,整体麻醉效果较为理想。
坐骨神经阻滞属于一种局麻方法,将麻醉药物注入到坐骨神经旁,暂时阻滞坐骨神经传导功能,使坐骨神经支配的区域感受不到疼痛,坐骨神经作为人体最为粗大的神经,自梨状肌大孔出骨盆,在臀大肌深面,自股骨大转子及坐骨结节下降至大腿后侧,能支配人体小腿及足部,在麻醉阻滞过程中还需把握坐骨神经的影响范围,采取侧卧位坐骨神经阻滞及平卧位坐骨神经阻滞。
坐骨神经阻滞适应症该麻醉方式在坐骨神经痛、梨状肌损伤引发的综合征诊断及治疗中应用,对治疗坐骨神经根性痛及坐骨神经干性痛具有一定价值。
坐骨神经阻滞在足外侧及内侧脚趾手术中具有应用价值,也能在下肢麻醉手术中广泛应用。
坐骨神经阻滞禁忌症针对没有明确诊断的患者,无法利用坐骨神经阻滞麻醉,一旦对患者进行阻滞,可能导致患者实际病情被掩盖,无法及时诊断患者疾病,甚至发生误诊问题。
不能良好配合的患者也不能采取坐骨神经阻滞。
针对需要注射的位置,皮肤会诱发感染,或者引发全身性炎症,患者谨慎展开坐骨神经阻滞,针对全身感染的患者也要慎重进行坐骨神经阻滞。
部分患者合并出血倾向,此类患者无法使用坐骨神经阻滞。
心肺功能不全的患者禁忌坐骨神经阻滞。
也有一些患者对麻醉药物过敏,此类患者需明确过敏原,部分患者无法采取坐骨神经阻滞。
坐骨神经阻滞麻醉相关技术①后入路阻滞:麻醉阻滞患者应当保持侧卧,使阻滞侧在上方,身体保持屈膝及屈髋的状态。
股骨大转子及髂后上侧划线,将各个中点连接成为一条垂直线,通过股骨大转子及骶裂孔划一条直线,找到两条线的交点,这两个点便是麻醉阻滞穿刺点。
穿刺针经过穿刺点垂直进入,直到患者有异样的感受。
若在穿刺后患者没有感到异样,但碰触到患者骨质,此时穿刺针应当适当倾斜偏进内侧后进针,直到划过骨面,找到坐骨神经所在位置。
坐骨神经阻滞的临床应用徐旭仲温州医学院附属第一医院麻醉科区域神经阻滞具有全身影响小和术后镇痛时间长等优点。
坐骨神经阻滞难度较大,近年随着研究的深人,涌现出许多改良的简明有效的穿刺方法,特别是辅助技术如神经刺激器,影像学技术的发展,使其成功率大大提高,逐渐应用于临床。
现就应用解剖,穿刺径路及辅助技术应用等进行综述。
1.应用解剖坐骨神经是全身最粗大,最长的神经,起始段最宽可达2cm,经梨状肌下孔出盆腔后,位于臀大肌深面,在坐骨结节与大转子之间下行至股后区,继而在股二头肌深面下行,一般在腘窝上方分为胫神经和腓总神经两大终支。
胫神经较腓总神经粗大,神经束间的结缔组织较多,排列较疏松。
在坐骨神经自起始至股部的胫神经和腓总神经之间有较厚结缔组织相隔,没有任何神经纤维的交通支往来,胫神经位于内后侧, 腓总神经位于前外侧[1]。
坐骨神经干的表面投影:自坐骨结节和大转子之间连线中点,向下至股骨内,外侧踝之间中点连线,此线上2/3段,为其投影。
2.穿刺径路2.1 腘窝侧路:患者仰卧,膝关节完全伸展,足与水平面成90度,在股二头肌与股外侧肌之间的凹槽,股骨上髁最突点往头端约7cm处为穿刺点,平行进针,抵到股骨后退针至皮下,穿刺针与水平面成30度再进针。
2.2腘窝后路:患者俯卧,膝关节完全伸展,取在股二头肌腱与半腱肌腱之间的中点,腘窝摺痕上约7cm处为穿刺点,垂直进针。
2.3 经典前路:连接髂前上棘与耻骨结节称上线,并将其三等分,然后由股骨大转子作一平行线称下线,由上线中内1/3交界处作一垂线,该垂线与下线交点为穿刺点。
垂直进针直至抵到股骨,调整方向略向内侧以越过股骨再进针约2-3cm。
2.4 改良前路:画髂前上棘与耻骨联合的连线,经过此线中点画一垂线,第二条线向尾8cm处为穿刺点,垂直进针约10.5cm。
还有一种方法为在小转子水平下4 cm 穿刺,垂直进针。
2.5 经典后路: 画髂后上棘至大转子的连线,经过此连线中点作一垂线并向下延伸4cm处为穿刺点。

Levobupivacaine 0.2% or 0.125% for continuous sciatic nerve block: a prospective, randomized, double-blind comparison with 0.2% ropivacaine.0.2%或0.125%的左旋布比卡因用于连续坐骨神经阻滞与0.2%罗哌卡因的比较(前瞻、随机、双盲实验)Casati A, Vinciguerra F, Cappelleri G, Aldegheri G, Grispigni C, Putzu M, Rivoltini P.Department of Anesthesiology, IRCCS H San Raffaele, Via Olgettina 60, 20132 Milan, Italy. casati.andrea@hsr.itIn 60 patients receiving elective hallux valgus repair, we compared the efficacy of continuous popliteal sciatic nerve block produced with 0.2% ropivacaine (n = 20), 0.2% levobupivacaine (n = 20), or 0.125% levobupivacaine (n = 20) infused with a patient-controlled system starting 3 h after a 30-mL bolus of the 0.5% concentration of the study drug and for 48 h (baseline infusion rate, 6 mL/h; incremental dose, 2 mL; lockout time, 15 min; maximum incremental doses per hour, 3). No differences were reported in the intraoperative efficacy of the nerve block. The degree of pain was similar in the three groups throughout the study period, both at rest and during motion. Total consumption of local anesthetic solution during the first 24 h was 148 mL (range, 144-228 mL) with 0.2% ropivacaine, 150 mL (range, 144-200 mL) with 0.2% levobupivacaine, and 148 mL (range, 144-164 mL) with 0.125% levobupivacaine (P = 0.59). The volume of local anesthetic consumed during the second postoperative day was 150 mL (range, 144-164 mL) with 0.2% ropivacaine, 154 mL (range, 144-176 mL) with 0.2% levobupivacaine, and 151 mL (range, 144-216 mL) with 0.125% levobupivacaine (P = 0.14). A smaller proportion of patients receiving 0.2% levobupivacaine showed complete recovery of foot motor function as compared with 0.2% ropivacaine and 0.125% levobupivacaine, both at 24 h (35% vs 85% and 95%; P = 0.0005) and at 48 h (60% vs 100% and 100%; P = 0.001). We conclude that sciatic infusion with both 0.125% and 0.2% levobupivacaine provides adequate postoperative analgesia after hallux valgus repair, clinically similar to that provided by 0.2% ropivacaine; however, the 0.125% concentration is preferred if early mobilization of the operated foot is required.Nerve stimulator-assisted evoked motor response predicts the latency and success of a single-injection sciatic block.神经刺激器帮助下引起的运动反应可以预见单次注射坐骨神经阻滞的潜伏和成功Sukhani R, Nader A, Candido KD, Doty R Jr, Benzon HT, Yaghmour E, Kendall M, McCarthy R.Department of Anesthesiology, Northwestern University/Feinberg School of Medicine, 251 E. Huron Street, F5-704, Chicago, IL 60611, USA. radhasukhani@Variable onset latency of single-injection sciatic nerve block (SNB) may result from drug deposition insufficiently close to all components of the nerve. We hypothesized that this variability is caused by the needle tip position relative to neural components, which is objectified by the type of evoked motor response (EMR) elicited before local anesthetic injection. One-hundred ASA I-II patients undergoing reconstructive ankle surgery received infragluteal-parabiceps SNB using 0.4 mL/kg (maximum 35 mL) of levobupivacaine 0.625%. The end-point for injection was the first elicited EMR: inversion (I), plantar flexion (PF), dorsiflexion (DF), or eversion (E) at 0.2-0.4 mA. The frequencies of the EMRs were: I 40%, PF 43%, E 14%, and DF 3%. SNB was considered complete if both tibial and common peroneal nerves were blocked and failed if either analgesia to pinprick was not observed at 30 min or anesthesia at 60 min. Patients with an EMR of I demonstrated shorter mean times (+/-95% confidence interval [CI]) to complete the block with 8.5 (95% CI, 6.2-10.8) min compared to 27.0 (95% CI, 20.6-33.4) min after PF (P < 0.001) and 30.4 (95% CI, 24.9-35.8) min after E (P < 0.001). No rescue blocks were required in group I compared with 24% (P = 0.001) and 71% (P < 0.001) of patients in groups PF and E, respectively. We conclude that EMR type during nerve stimulator-assisted single-injection SNB predicts latency and success of complete SNB because the observed EMR is related to the positioning of the needle tip relative to the tibial and common peroneal nerves.3.Reg Anesth Pain Med. 2003 Jul-Aug;28(4):294-303.Levobupivacaine versus ropivacaine for sciatic nerve block in the rat.鼠坐骨神经阻滞实验中左旋布比卡因与罗哌卡因的比较Sinnott CJ, Strichartz GR.Pain Research Center, Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women's Hospital, 75 Francis Street, Boston, MA 02115, USA.BACKGROUND AND OBJECTIVES: Ropivacaine and levobupivacaine, both single S- enantiomers, are being promoted as safer alternatives to racemic bupivacaine. To determine whether levobupivacaine produces a more potent and longer lasting peripheral nerve block than ropivacaine, we compared functional blockade of sciatic nerve in the rat at several doses with these 2 agents. METHODS: Percutaneous sciatic nerve blocks were performed in 6 groups of rats (n = 8) with 0.1 mL of 0.0625%, 0.125%, and 0.25% of levobupivacaine or ropivacaine, with and without 1:200,000 epinephrine. In the 2 different hindlegs of the same 8 rats, we measured the degree and duration of deficit of 3 functions of peripheral nerve (proprioception, motor function, nociception) effected by the 2 respective drugs at the same concentration, using a blinded cross-over design. RESULTS: In general, both degree and duration of functional deficits produced by levobupivacaine were slightly greater than those from ropivacaine at the same dose. At the lowest concentration (0.0625%), no functions were completely blocked and the only significant difference was a longer motor impairment by levobupivacaine. At the highest concentration (0.25%), all formulations completely blocked the 3 functions, all of which lasted longer with levobupivacaine than ropivacaine. There were no significant differences in degree and duration of deficits between the 2 drugs at midconcentration (0.125%). The actions of both drugs were generally potentiated by epinephrine, but the rank order of potency was not altered. CONCLUSIONS: At the lowest concentration (0.0625%), levobupivacaine produces a greater degree of motor impairment and a longer duration of proprioceptive impairment relative to ropivacaine. At the middle concentration (0.125%), there no differences between the 2 drugs. At the higher concentration (0.25%), which is within the range used clinically for peripheral nerve block (0.25%-0.5%), levobupivacaine produces approximately a 30% longer duration of complete block in each modality compared with that by ropivacaine.4.J Clin Anesth. 2002 Mar;14(2):111-4.Clinical properties of levobupivacaine or racemic bupivacaine for sciatic nerve block.坐骨神经阻滞中左旋布比卡因与消旋布比卡因临床性质的比较Casati A, Chelly JE, Cerchierini E, Santorsola R, Nobili F, Grispigni C, Di Benedetto P, Torri G.Vita-Salute University, Department of Anesthesiology, IRCCS H. San Raffaele, Milan, Italy. casati.andrea@hsr.itSTUDY OBJECTIVE: To compare the intraoperative and postoperative clinical properties of the sciatic nerve block performed with either 0.5% bupivacaine or 0.5% levobupivacaine for orthopedic foot procedures. DESIGN: Randomized, double-blind study. SETTING: Inpatient unit of a university-affiliated hospital. PATIENTS: 30 ASA physical status I and II patients undergoing elective hallux valgus repair under regional anesthesia. INTERVENTIONS: After administering intravenous (IV) midazolam premedication (0.05 mg/kg), a femoral nerve block was performed with 15 mL of mepivacaine 2%. Patients were then randomly allocated to receive, in a double-blind fashion, a sciatic nerve block with 20 mL of either 0.5% bupivacaine (n = 15) or 0.5% levobupivacaine (n = 15). MEASUREMENTS AND MAIN RESULTS: An observer who was blinded to the study drug recorded the onset time, quality, and duration of the sciatic nerve block. Postoperative analgesia consisted of 100 mg IV ketoprofen every 8 hours, with the first administration given at the patient's request. Mean (+/-SEM) onset time of the sciatic nerve block was 35 +/- 5 minutes for bupivacaine and 31 +/- 6 minutes for levobupivacaine (p = not significant [NS]). The duration of motor and sensory blocks with bupivacaine was 761 +/- 112 minutes and 790 +/- 110 minutes, respectively, and 716 +/- 80 minutes and 814 +/- 73 minutes, respectively, with levobupivacaine (p = NS). The first pain medication was requested after 844 +/- 96 minutes with bupivacaine and 872 +/- 75 minutes after levobupivacaine (p = NS). No differences in the quality of nerve block and patient satisfaction were reported between the two groups. CONCLUSIONS: A dose of 20 mL of 0.5% levobupivacaine induces sciatic nerve block of similar onset, duration, and intensity as the block produced by the same volume and concentration of the racemic solution of bupivacaine.5.Anesth Analg. 2002 Apr;94(4):987-90,A double-blinded, randomized comparison of either 0.5% levobupivacaine or 0.5% ropivacaine for sciatic nerve block.0.5%左旋布比卡因与0.5%罗哌卡因用于坐骨神经阻滞的比较(双盲、随机)Casati A, Borghi B, Fanelli G, Cerchierini E, Santorsola R, Sassoli V, Grispigni C, Torri G.Department of Anesthesiology, Vita-Salute University, IRCCS H. San Raffaele, Milan, Italy. casati.andrea@hsr.itTo compare intraoperative and postoperative clinical properties of levobupivacaine and ropivacaine for sciatic nerve block, 50 ASA physical status I and II patients undergoing hallux valgus repair received a femoral nerve block with 15 mL of 2% mepivacaine. They were then randomly allocated in a double-blinded fashion to receive a sciatic nerve block with either 0.5% levobupivacaine (n = 25) or 0.5% ropivacaine (n = 25). An independent blinded observer evaluated the onset time of surgical anesthesia as well as the quality of the surgical block and postoperative analgesia. The median (range) onset time of surgical block at the sciatic nerve distribution was 30 min (5-60 min) with levobupivacaine and 15 min (5-60 min) with ropivacaine (P = 0.63). Four patients (two patients in each group) received a supplementary ankle block by the surgeon just before the beginning of surgery. All four patients also received IV fentanyl supplementation, but in three of them, propofol infusion was required to complete surgery (two in the Levobupivacaine group [8%] and one in the Ropivacaine group [4%]; P = 0.99). In six patients of the Levobupivacaine group (24%) and five patients of the Ropivacaine group (20%), IV fentanyl supplementation was required to complete surgery (P = 0.99). No differences in the time to recovery of sensory and motor function were observed between the two groups, whereas median (range) duration of postoperative analgesia was 16 h (8-24 h) with levobupivacaine and 16 h (8-24 h) with ropivacaine (P = 0.83). We conclude that 0.5% levobupivacaine and 0.5% ropivacaine provide comparable surgical anesthesia and postoperative analgesia. IMPLICATIONS: No studies have compared the clinical properties of levobupivacaine with those of ropivacaine when providing sciatic nerve block for hallux valgus repair. Results from this prospective, randomized, double-blinded study demonstrate that 20 mL of either 0.5% levobupivacaineor 0.5% ropivacaine provide comparable surgical block with prolonged postoperative analgesia.。
坐骨神经阻滞麻醉的小知识坐骨神经阻滞是局部麻醉之一,将局部麻醉药物注射到坐骨神经旁,让坐骨神经传导功能暂时受到限制,确保在手术过程中不会产生疼痛感。
坐骨神经由腰4至骶3前支组成,也是人体内最大、最粗的神经,主要支配小腿和足。
在膝关节、足部手术时会应用到坐骨神经阻滞麻醉,效果良好,不会产生疼痛感。
1坐骨神经解剖坐骨神经来自骶神经丛(L4-S3),神经根出发后在梨状肌前方这一层次形成坐骨神经,位于梨状肌正下方水平,从坐骨大孔从骨盆,在坐骨结节和股骨大转子间下行。
在大腿上中2/3,一直走在大腿后方一般到下1/3处,分层了胫神经和腓总神经。
股骨大转子的顶点与坐骨结节连线的中点,它与腘窝上极这个点的连线可反映出坐骨神经在大腿后方的行径。
臀大肌下坐骨神经体表定位的步骤具体如下:患者在病床上呈侧卧位,由专业医师描绘出股骨大转子的半圆形轮廓,并标记出股骨大转子的中点,用手触摸的方式确定髂后上脊,由该两中点作一条直线,测量并做好标记,在中点处做一条垂直线,下放5cm位置就是臀大肌下坐骨神经在体表的行走位置。
在确定腘窝坐骨神经时,患者呈俯卧位,膝盖略微弯曲,在膝盖后方皮肤褶皱上的7-9cm处画出一条连接股二头肌肌腱外侧面和半膜肌肌腱内侧面的直线,这条连接线的中点就是腘窝坐骨神经体表位置。
坐骨神经感觉支配的区域包括股后侧皮神经、腓总神经、腓深神经、腓浅神经、腓肠神经、足底外侧神经、足跟神经、足底内侧神经。
当完全阻滞股神经及坐骨神经时,基本可以完全阻滞所有下肢感觉神经,因此可以满足下肢手术的需求。
2坐骨神经阻滞麻醉的适应症(1)坐骨神经阻滞麻醉适用于坐骨神经疼痛、梨状肌受伤后的治疗诊断,在坐骨神经根性疼痛、干性痛方面价值非常突出;(2)如果患者足外侧以及足部第三、第四、第五趾的手术,可以应用坐骨神经阻滞麻醉,如果配合阻滞股神经应用,可让下肢手术顺利开展。
3坐骨神经阻滞麻醉的禁忌症(1)诊断结果不明确的患者,不能使用坐骨神经阻滞麻醉,避免出现掩盖病情的情况;(2)无法配合这种麻醉方式的患者;(3)注射局部麻醉药物的皮肤出现感染,或是患者本身有炎症性病灶,一定要慎用坐骨神经阻滞麻醉;对于全身感染症状严重的患者,要经过专业医生的评估之后才可使用;(4)对于心肺功能不全、有出血倾向的患者,不能使用坐骨神经阻滞麻醉;(5)部分患者体质比较特殊,对麻醉药物十分敏感,这类患者不能使用坐骨神经阻滞麻醉。
坐骨神经阻滞定位方法
坐骨神经阻滞是一种用于治疗坐骨神经痛的常见治疗方法。
以下是常用的坐骨神经阻滞定位方法:
1. 传统方式:患者平躺,并将骶尾部抬高。
医生通过手指触摸找到患者的骶尾肌和坐骨结节。
然后在坐骨结节的外上方约2-3cm处用酒精消毒,然后用针头注射麻药。
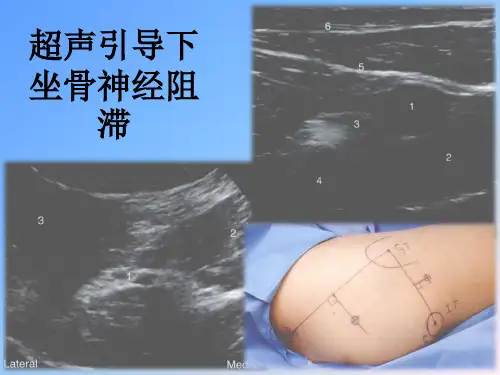
2. 超声引导:医生使用超声波仪器定位坐骨神经和相关解剖结构,然后进行阻滞注射。
这种方法可以提高定位的准确性和安全性。
3. CT或X光引导:在一些复杂情况下,医生可能使用CT或X光引导以更准确地定位坐骨神经。
无论使用哪种定位方法,医生在进行坐骨神经阻滞前应仔细检查患者的病史和进行体格检查,以确保患者适合接受该治疗。
此外,需要使用无菌操作,并密切监测患者在治疗过程中的情况。

坐骨神经阻滞麻醉,你了解的知识有多少坐骨神经是人体中尤为粗大的一类神经结构,通常会在膝部以下以及足手术时应用到坐骨神经阻滞技术,其技术的应用能够麻醉手术的区域形成一定的疼痛缓解效果,暂时抑制坐骨神经传导功能,使得病患在手术的过程中不会感到疼痛感。
在该篇科普文中主要针对坐骨神经阻滞麻醉的适应症、禁忌症以及相应的坐骨神经阻滞麻醉技术进行分析。
一、坐骨神经阻滞麻醉的适应症当坐骨神经受到压迫或损伤时,会引起腰部、臀部、腿部和脚部的疼痛。
坐骨神经阻滞麻醉可以单独使用或与其他麻醉技术结合使用。
坐骨神经阻滞麻醉通常会被应用到梨状肌损伤以及坐骨神经疼痛等的治疗诊断工作中,其在坐骨神经干性痛等方面具有的医疗价值极高。
二、坐骨神经阻滞麻醉的适应症禁忌症1.病患心肺功能不全,存在出血倾向。
2.无法主动配合坐骨神经阻滞麻醉方式的病患。
3.病患身体体质较为特殊,对于麻醉药物的敏感度较高。
4.病患在注射局部麻醉药物时,会产生皮肤过敏、感染等的症状,病患自身存在炎症性病灶,需要谨慎使用坐骨神经阻滞麻醉技术。
5.病患诊断结果不明确,不可应用坐骨神经阻滞麻醉技术,防止其技术在应用之后影响到病患病情的诊断,掩盖患者病情。
三、坐骨神经阻滞麻醉技术第一,臀下入路阻滞技术。
该技术主要会被投用至肥胖病患群体之中,在进行下肢手术时使用其技术,同时配合应用单次隐神经阻滞以及连续腰从阻滞等技术,病患要以侧卧姿势接受穿刺,确认并标记病患坐骨结节以及股骨大转子的位置,连线坐骨结节以及股骨大转子,在连线中心点的位置朝下方做出垂直线,不断延伸该垂直线,让其长度延展至四厘米左右后,触摸皮肤凹陷位置,其被当做穿刺点。
病患皮肤要和穿刺针保持80度的角度,在回抽实验无血后,将局部麻醉药物缓慢推注肌肉,其剂量要控制在20至30毫升范围。
第二,传统后侧入路。
病患侧卧,保持屈膝屈髋的状态,在髂后上棘以及股骨大转子位置连线,由二者连线中点做垂直线,并在病患骶裂孔以及股骨大转子位置做连线,二者连线相交位置为穿刺点。

坐骨神经阻滞麻醉定位器坐骨神经阻滞是一种常见的麻醉技术,广泛应用于手术和疼痛管理领域。
为了确保坐骨神经准确地被阻滞,麻醉定位器的使用变得越来越重要。
本文将介绍坐骨神经阻滞麻醉定位器的原理、应用、优势以及未来的发展。
1. 坐骨神经阻滞麻醉定位器的原理坐骨神经阻滞是通过向坐骨神经周围注射麻醉药物来生成局部麻醉作用,从而实现疼痛的缓解或患者手术需要。
麻醉定位器是一种用于辅助医生准确定位坐骨神经位置的设备。
该定位器通常由超声设备、神经电刺激器和针道导航系统组成。
超声设备可以为医生提供实时、清晰的影像,以帮助他们确定坐骨神经的位置。
神经电刺激器则可以通过电刺激坐骨神经,以判断是否已经准确找到了该神经。
针道导航系统能够帮助医生准确地将针头导入到坐骨神经周围。
2. 坐骨神经阻滞麻醉定位器的应用坐骨神经阻滞麻醉定位器广泛应用于以下几个方面:2.1 手术麻醉在全麻下进行手术过程中,坐骨神经阻滞可以减少手术部位的疼痛,同时还可以降低全麻药物的使用量,减少全麻引起的副作用和并发症。
麻醉定位器的使用可以确保手术医生准确地找到坐骨神经,从而提供更好的麻醉效果。
2.2 疼痛管理坐骨神经阻滞也广泛用于疼痛管理领域。
对于患有坐骨神经痛或其他与坐骨神经相关的疾病的患者,坐骨神经阻滞可以提供持久的疼痛缓解效果。
麻醉定位器的使用可以准确地定位坐骨神经,从而确保麻醉药物准确地注射到目标区域。
3. 坐骨神经阻滞麻醉定位器的优势坐骨神经阻滞麻醉定位器相对于传统的手动定位方法具有以下优势:3.1 提高准确性传统的手动定位方法依赖于医生的经验和技巧,存在一定的主观性和误差。
而麻醉定位器借助超声设备和神经电刺激器的辅助,提高了定位的准确性,减少了误差。
3.2 缩短手术时间通过使用麻醉定位器,医生可以更快地找到坐骨神经,减少了手术中定位的时间,进而缩短了手术时间。
这对于需要迅速进行手术的患者来说尤为重要。
3.3 增强安全性麻醉定位器的使用可以降低误伤周围组织和血管的风险。
坐骨神经阻滞的治疗方法有哪些很多人,特别是对于一整天就坐着的办公室一族来说,坐骨神经阻滞是常见的事情,所以我们也是不用过分担心的,但是也是需要适当的调整的。
对于坐骨神经阻滞来说,中医治疗是相对较多的,一般都是有很多种治疗方法,我们可以放心。
食物疗法(1)生姜鸡:用刚刚开叫的公鸡1只,生姜100~250g,切成小块,在锅中爆炒焖熟,不放油盐。
会饮酒者可放少量酒,1天内吃完,可隔1周或半月吃1次。
用于关节冷痛,喜暖怕寒者。
(2)鹿茸鸡:以当年的公鸡1只,鹿茸3~6g,在锅内焖熟,不放油盐。
吃肉喝汤,两天吃完。
可根据情况每隔1周或半月吃1次。
夏天及关节红肿疼痛者勿用。
(3)赤小豆粥:赤小豆30g,白米15g,白糖适量。
先煮赤小豆至熟,再加入白米作粥加糖,能除湿热。
(4)苡米粥:苡米30g、淀粉少许、砂糖、桂花适量。
先煮苡米,米烂熟放入淀粉少许,再加砂糖、桂花。
作早餐用,能清利湿热,健脾除痹。
(5)防风苡米粥:防风10g,苡米30g。
水煮,每日1次,连服1周,能清热除痹。
(6)川断25克,杜促30克,与1条猪尾共煮,调味服用。
(7)桑寄生15克与1个鸡蛋,煲熟服用。
(8)老桑枝6克,与500克重的雌鸡共炖,饮汤食用。
(9)粟子粥:粟子15枚,猪腰l对,粳米30克。
先将栗子炒香(用沙炒),后去壳,与粳米加水适量同煮粥。
或将栗子风干,磨粉,以栗粉30克,粳米20克,猪肾1对,同煮粥亦可,每次1小碗,每日1次。
本方有补肾强筋、健脾养胃之功,可用于坐骨神经痛脾肾亏虚证。
推拿治疗1、揉法。
沿腰背部顺行向下至小腿进行揉摩,以放松身体,舒通经络使气血得以畅通。
2、点按法。
点按双侧腰肌,以改变腰肌紧张状态。
3、弹筋法。
弹拨腰肌,以兴奋肌肉.恢复肌纤维组织弹性。
4、推法。
用双手掌根沿脊拄两侧自背部开始推至臀部,以调达气血、疏通经络,使腰背肌肉得以调整。
5、按揉法。
沿受累的神经路线重点按揉至小腿,以松解肌肉,改善受累区血受累区血液循环,恢复麻木区的神经组织。
坐骨神经阻滞
一概述
坐骨神经阻滞具有对血流动力学影响小,术后并发症少,镇痛时间长,利于术后患者恢复等诸多优点,是一种可供选择的较好的麻醉方法。
适用于老年患者急诊足踝部手术。
二术前准备
患者需在麻醉前建立静脉通路。
清空膀胱。
三适应证
1.适用于坐骨神经痛,梨状肌损伤综合征的治疗与诊断、鉴别诊断。
尤其对坐骨神经根性、干性痛有鉴别诊断价值。
2.高浓度局麻药行坐骨神经阻滞麻醉,可用于足外侧和第3、4、5趾手术,如同时阻滞股神经,可用于下肢手术麻醉。
四禁忌证
1.未明确诊断者忌行神经阻滞以免掩盖病情。
2.不合作患者。
3.注射部位皮肤或深部有感染、炎性病灶者禁用。
或全身感染者。
4.有出血倾向者。
5.严重心肺功能不全者
6.局麻药过敏者。
五麻醉方法
旁路坐骨神经阻滞法:患者取仰卧位,股骨大转子上缘向头侧再向背
侧 1. 5 ~ 2. 5 cm 处为穿刺点,用长100 mm 穿刺针并连接神经刺
激仪,设定神经刺激仪的刺激电流为1 m A,频率为 2 Hz。
当刺激坐
骨神经时出现足的跖屈或背屈,降低电流至0. 3 m A 时仍有肌肉颤搐,说明定位准确,回抽无回血,缓慢推注麻醉药。
六麻醉风险
尿潴留及腰部酸痛等并发症。
七注意事项
坐骨神经粗大,局麻药用药量较大,给药过程中应注意回抽注射器以
避免引起局麻药中毒。
坐骨神经阻滞,您了解多少相关麻醉知识?坐骨神经阻滞是一种区域阻滞麻醉的方法,也是一种以神经阻滞为基础的麻醉。
其特点是既能达到麻醉的效果,又能保证足够的安全性。
该技术最早在20世纪80年代开始应用于临床,随后,其应用范围逐渐扩大,现在已经广泛用于骨科麻醉、疼痛科等多种疾病的治疗。
那么关于坐骨神经阻滞麻醉,还有哪些事是我们还不知道的?接下来,就让我一一向大家介绍。
1.坐骨神经阻滞麻醉的简介坐骨神经阻滞即在局麻药作用于坐骨神经后,在坐骨神经周围形成一个浸润包裹,通过影响神经纤维传导疼痛信号产生麻醉效果。
这种麻醉方式不会影响脊柱,因此不会引起脊柱侧弯或弯曲。
此外,由于药物不通过血脑屏障,因此对大脑意识没有影响。
2.坐骨神经阻滞麻醉的适应症坐骨神经阻滞麻醉适应症广泛,包括但不限于以下几个方面:(1)各种慢性疼痛的治疗,如腰腿痛、坐骨神经痛、足跟痛等。
(2)下肢手术麻醉需要。
(3)改善坐骨神经周围血液循环。
(4)其他疼痛疾病的鉴别诊断。
坐骨神经阻滞麻醉可以用于小儿骨外科手术的麻醉,但因其操作相对复杂,因此临床应用需要超声引导。
3.坐骨神经阻滞麻醉的禁忌症(1)脊柱骨折和畸形的患者:椎体骨折、先天性脊柱畸形、下肢感觉异常、严重脊髓疾病等,是禁忌的。
(2)穿刺部位感染。
(3)对局麻药过敏的患者:坐骨神经阻滞麻醉中使用的局麻药对某些药物过敏,这是不适合使用的。
(4)全身情况差:由于全身情况较差,不能耐受或无法耐受麻醉方法,因此不适合使用坐骨神经阻滞麻醉。
4.坐骨神经阻滞麻醉的麻醉药物坐骨神经阻滞麻醉时局麻药常混合低浓度使用,常用的酰胺类局麻药包括利多卡因、罗哌卡因和布比卡因。
利多卡因是一种中效局麻药,也是唯一具有抑制心率失常的麻醉药物,应用广泛。
罗派卡因是一种长效类局麻药,低浓度具有感觉和运动分离效应。
安全范围大,常联合利多卡因低浓度应用于坐骨神经阻滞。
布比卡因也是长效局麻药,性能稳定,由于其心脏毒性大,应低剂量使用,应用于坐骨神经阻滞使用较少。