以腹胀、双下肢水肿、气促为表现的POEMS综合征1例及文献复习
- 格式:pdf
- 大小:1.07 MB
- 文档页数:8

-428-四川医学2021年4月第42卷(第4期)Sihuan Meghal Joumal#2021#Vol.42#No.4 df:10.16252/kP ion1004-0501-2021.04.024POEMS综合征1例报告潘纬榕J张红智2,孙思娴2,欧阳志英2,陈涛2,韩志宏2,朱旭莹2△(1.上海市静安区中医医院心病科,上海200072;2.上海中医药大学附属曙光医院神经内科,核医学科,病理科,上海200021)1临床资料患者,女,33岁,因进行性双下肢乏力7个月余,加重1个月入院。
患者2019年2月无明显诱因下出现双下肢乏力,伴小腿后侧及足底酸痛麻木,行走不稳,于外院神经内科,完善相关检查后诊断为“格林巴利综合征”,予人免疫球蛋白及甲强龙治疗,病情略有好转,可拄拐行走,出院后口服强的松3周后逐渐减量至停药。
4月起自觉体毛增多,月经周期不规律。
6月时出现双足底麻木伴轻微针刺感,就诊于外院,考虑“格林巴利综合征恢复期”,予加巴喷丁治疗,服药后出现双眼睑水肿、头晕头痛、腹泻等症状,遂停药。
7月始出现双下肢乏力进行性加重,至反复跌倒,同时伴双手指麻木,再次就诊于外院神经科,未予特殊治疗。
9月时患者偶有小便失禁,继续就诊于外院,予醋酸泼尼松40 mg口服,1次/d,共14d,症情未见好转。
2019年10月初因双下肢乏力反复跌倒,双下肢痛觉过敏,双手指及足底麻木,左侧)部疼痛,偶有小便失禁,就诊我院神经内科门诊,收入住院治疗。
查体:体毛增多,双上肢肌张力正常,双下肢肌张力略减弱,双上肢腱反射略减弱,双下肢腱反射消失,双上肢肌力及双下肢远端肌力V级,双下肢近端肌力n级,双上肢针刺觉正常,双下肢痛觉过敏。
实验室检查:骨髓细胞学镜检:骨髓浆细胞占2.5%,形态无特殊;骨髓有核细胞增生明显活跃,粒红比稍高)免疫固定电泳:异常条带4-9%,IgG可见异常条带,LAMDA 轻链可见异常条带。
VEGF:730.69pg/mi(上海新培晶医学检验所,参考值0~142pg/mi)。

POEMS综合征文献复习(附1例临床报道)POEMS综合征是一种与浆细胞病有关的多系统病变,进行性多发性神经病变(Polyneuroparhy,P)、器官(肝脾)肿大(Organomegaly,O)、内分泌紊乱(Endocrinopathy,E)、M蛋白增高(M protein,M)、皮肤改变(skin changes , S)并常伴有全身凹陷性水肿、胸腹水、杵状指(趾)和心衰等症状,取其头一个字母组合并命名为POEMS综合征。
我院2005年收治1例报道如下并作文献复习。
1 病例介绍患者,男,50岁,农民。
以双下肢无力半年,胸闷气短不能行走半月于2005年12月入院。
半年前四肢无力,进行性加重,当时无活动不灵,半月前气短胸闷,双下肢麻木,活动不灵伴有肢体肿胀,站立时手指发紫。
发病后皮肤渐黑。
查体:T36 6℃P80次/min R 16次/min BP 120/80mmHg。
神清,慢性病容,消瘦体质,全身皮肤颜色发黑,双侧颈部可触及肿大淋巴结3~4枚,直径1~2cm,触痛阴性。
乳房发育,乳晕色黑,胸骨无压痛,双肺呼吸音清,心率80次/min,律齐,肝脾肋下未及,双下肢指压痕阳性。
四肢末端凉。
四肢远端痛觉减退。
实验室检查:血常规:Wbc 8 24×109HB131g/LPLT 338×109 血沉22cmH2O/第1小时,C反应蛋白0 56mg/dlIgG 19 8g/LIgA 4 48g/LIgM 1 74g/L 、24小时尿蛋白定量024 g/L、免疫电泳可见M峰,心脏彩超:少量心包积液,双上肢静脉和肱静脉血栓,肌电图:左下肢周围神经原损害,骨髓:未见浆细胞比例增高。
2 讨论本病病因及发病机制不清,临床发现POEMS综合征常与多种浆细胞瘤伴发摘要[1]摘要如骨硬化性骨髓瘤,未定性单克隆免疫球蛋白病及原发性巨球蛋白血症,因此有学者认为本病可能也是一种浆细胞病,浆细胞异常增生产生异常球蛋白血症致多系统损害。
POEMS综合征误诊1例报告发表时间:2011-02-17T13:52:55.547Z 来源:《中外健康文摘》2010年12月第34期供稿作者:蔡树生[导读] 近3个月腹胀及膨隆加重、消瘦、乏力,活动后心悸、气短、头晕,视物模糊。
蔡树生(辽宁省朝阳市第二医院内科辽宁朝阳 122000)【中图分类号】R73 【文献标识码】A 【文章编号】1672-5085(2010)34-0272-021 病例患者,女,36岁,8个月前无诱因感到上腹闷胀不适,渐感腹胀加重,膨隆,当地医院诊为“结腹”予抗痨治疗半个月无好转而停药。
近3个月腹胀及膨隆加重、消瘦、乏力,活动后心悸、气短、头晕,视物模糊。
当地医院经胸腹部CT等检查后,以“肝硬化”“肾炎”治疗,病情无好转,遂住入中日友好医院消化科诊治。
既往史:5岁时患甲型肝炎治愈。
查体:慢性病容,营养差,消瘦体型,步态欠稳。
皮肤无黄染、无出血点及皮下瘀斑,无肝掌,甲状腺不大、双肺下野叩略变浊,左肺下野闻及少许细湿罗音,心音纯、律齐。
腹膨隆、肝脾触摸不清、肝区无叩痛,双肾区叩痛阳性,移动性浊音阳性,肠鸣音存在。
双下肢胫前凹陷性浮肿。
四肢肌张力Ⅵ级,病理征未引出,共济失调可疑阳性。
入院诊断:腹水原因待查,结腹?柏—查综合征?需要除外妇科肿瘤、肾病或慢性肾炎。
实验室及特殊检查:FBS3.9mmol/L、ESR60mm/1h、尿Rt pro++、血K5.60mmol/L、BUN12.28mmol/L、Cr221.6μmol/L、T3.121nmol/L、T4.53nmol、TSH.5.13nmol,乙肝6项均(-)。
自身抗体ENA谱(-)、免疫球蛋白:IgG.1.440g/L、IgA.0.761g/L、IgM.0.169g/L、IgD100IU/ml、IgE.300.5IU/L。
血清K轻链1.130g/L,λ轻链1.110g/L。
腹水检查:未查到肿瘤细胞及抗酸杆菌。
沉渣见大量浆细胞。

POEMS综合征:1例报告并文献复习张科技;杨丽;杨长青【摘要】POEMS综合征是一种与浆细胞有关的多系统病变,临床上以进行性多发性周围神经病变(P)、脏器(肝脾)肿大(O)、内分泌紊乱(E)、M蛋白增高(M)和皮肤改变(S)为特征,常伴有全身凹陷性水肿、胸腹水、杵状指(趾)和心力衰竭等症状。
我们报道1例男性38岁患者,因“腹胀、双下肢水肿2年,四肢远端麻木2月”入院,经临床各种检查被诊断为该病。
我们复习了有关POEMS综合征的临床特征和诊治进展。
【期刊名称】《实用肝脏病杂志》【年(卷),期】2013(000)006【总页数】2页(P563-564)【关键词】POEMS综合征;病例报道;文献复习【作者】张科技;杨丽;杨长青【作者单位】315800 浙江省宁波市北仑区第二人民医院内科;同济大学附属同济医院消化科;同济大学附属同济医院消化科【正文语种】中文POEMS综合征是一种与浆细胞有关的多系统病变,临床上以进行性多发性周围神经病变(Polyneuropathy)、脏器(肝脾)肿大(Organomegaly)、内分泌紊乱(Endocrinopathy)、M 蛋白增高(M-protein)和皮肤改变(Skin-Changes)为特征,常伴有全身凹陷性水肿、胸腹水、杵状指(趾)和心力衰竭等症状。
1956年由Crow等首次报道,1968年Fukase将其作为一个独立的综合征提出,因此,亦称Crow-Fukase综合征。
1980年Bardwick取本病的五大临床特征的英文首字母将其命名为POEMS综合征[1]。
本病在日本报道较多[2],我国近年也有多例报道。
我院消化科最近收治1例,现报告如下。
病例摘要患者男,38岁,山西省晋城市人,中学教师。
因“腹胀、双下肢水肿2年,四肢远端麻木2月”于2010年5月14日收住我院。
于2008年5月起出现中上腹胀、双下肢轻度水肿,经当地医院检查诊断为“甲状腺功能低下症”,给予左甲状腺激素钠(优甲乐)100μg/d替代治疗,水肿症状稍好转。

以双下肢水肿为首发表现的POEMS综合征1例杨元;陶涛;袁正洲;李作孝【期刊名称】《广东医学》【年(卷),期】2014(035)024【摘要】患者,女,51岁,因双下肢水肿、麻木1年,皮肤色素沉着、四肢无力7个月于2014年4月17日入院。
2013年5月患者无明显诱因开始出现双下肢凹陷性水肿、伴远端麻木。
尿常规:红细胞(+),24 h尿蛋白定量0.159 g/24h;考虑诊断为"肾炎综合征?"。
给予利尿、抗炎等对症处理,症状缓解不明显自动出院。
2013年10月,患者出现腹胀、纳差、颜面部及四肢皮肤发黑、粗糙,伴双下肢疼痛乏力,自认为是药物中毒。
【总页数】1页(P3931)【作者】杨元;陶涛;袁正洲;李作孝【作者单位】泸州医学院附属医院神经内科四川泸州646000;泸州医学院附属医院神经内科四川泸州646000;泸州医学院附属医院神经内科四川泸州646000;泸州医学院附属医院神经内科四川泸州646000【正文语种】中文【相关文献】1.以双下肢水肿为首发表现的肝豆状核变性一例 [J], 袁红英;李玲2.以甲状腺功能减退症合并全身性水肿、肺动脉高压为首发表现的POEMS综合征1例报道 [J], 成玮;蒋瑛;张维佳;李晓华;徐艳红;贝鹏剑3.以脑梗死为首发表现的POEMS综合征1例并文献复习 [J], 徐伟;陈琛;杨晶;王成美4.以腹胀、双下肢水肿、气促为表现的POEMS综合征1例及文献复习 [J], ZHANG Jiayi;OUYANG Zeying;LI Rong;LENG Aiming;LIU Ting5.顽固性腹水、淋巴结肿大、肝脾肿大为首发表现的POEMS综合征1例 [J], 王珍香;陈叶青;何泉;周国华因版权原因,仅展示原文概要,查看原文内容请购买。
POEMS综合征1例报告患者男性,1951年生人。
于2007年7月因“双下肢水肿、乏力1年余,加重伴四肢乏力1月”入院。
入院1年前无明显诱因渐出现双下肢水肿,乏力,轻度凹陷性水肿,伴走路不稳,踩棉感,肢体沉重感,无头痛、头晕,无意识障碍及肢体抽搐,无大小便功能障碍。
曾到济南各大医院就诊,行肌电图示神经源性病变(2006年11月),腰穿示脑脊液蛋白1.58g/L,白细胞(-),寡克隆区带(-)(2006.12)。
应用B族维生素及中药等药物治疗,效果欠佳。
既往史:有多次晕厥病史,持续时间短暂,存在短暂意识丧失,无肢体抽搐及大小便障碍。
否认高血压、糖尿病等病史。
无烟酒嗜好。
20岁结婚,育有2女1子,均体健,否认遗传病史。
查体:肝脏体积略大,肋下可扪及,全身皮肤色素沉着,双下肢凹陷性水肿,颅神经(-),四肢肌张力正常,肌力双上肢IV级,双下肢III-IV级,四肢腱反射消失,双侧Babinski征(-),Chaddock征(-)。
四肢末端痛觉减退,共济运动尚可,劲软,双侧Kernig征(-)。
入院后辅助检查:(2007年7月)化验血清叶酸、维生素B12水平正常,铁蛋白、CEA、AFP正常,血沉9mm/H,风湿系列、肝炎六项正常,检查免疫球蛋白水平示IgG、IgM、IgA均处于正常水平,尿本周蛋白阴性,腹部B超示肝大,肝脏最大斜径15.5cm,形态饱满,实质回声均质,脾脏厚度3.5cm,实质回声均质,脾静脉不宽。
肌电图示双侧胫神经、腓总神经运动传导未引出动作电位,右侧正中神经、尺神经运动传导速度减慢,波幅降低,双侧正中神经及右侧尺神经感觉传导速度减慢,波幅降低,双侧胫前肌呈完全失神经支配,右侧拇短展肌呈神经源性损害,右侧正中神经F波潜伏期延长,波形离散,结论为四肢神经源性损害(周围神经病变)。
骨穿结果示正常骨髓象。
腰穿示初压120mmH2O,末压70mmH2O,蛋白1073mg/L,CSF常规示无色透明,潘氏试验(+),细胞学、寡克隆区带均未见异常。
1例POEMS综合征患者临床特征分析赵敦勇;肖云月;汤旭东;陈磊;陈文生【期刊名称】《检验医学与临床》【年(卷),期】2018(015)016【总页数】2页(P2523-2524)【关键词】POEMS综合征;内分泌系统疾病;临床特征【作者】赵敦勇;肖云月;汤旭东;陈磊;陈文生【作者单位】中国人民解放军陆军军医大学附属第一医院全军消化病研究所 ,重庆400038;中国人民解放军陆军军医大学附属第一医院全军消化病研究所 ,重庆400038;中国人民解放军陆军军医大学附属第一医院全军消化病研究所 ,重庆400038;中国人民解放军陆军军医大学附属第一医院全军消化病研究所 ,重庆400038;中国人民解放军陆军军医大学附属第一医院全军消化病研究所 ,重庆400038【正文语种】中文【中图分类】R597POEMS综合征,又称为骨硬化性骨髓瘤、Crow-Fukase综合征、PEP综合征或Takatsuki综合征[1-3],是继发于单克隆浆细胞病的多系统疾病。
POEMS是几个主要症状英文单词首字母的缩写:周围神经病(P)、脏器肿大(O)、内分泌疾病(E)、单克隆浆细胞增殖性疾病(M)和皮肤改变(S)[4]。
主要临床特征是以运动功能障碍为主的进行性多发性神经疾病。
虽然发病率低,但误诊率和漏诊率高。
本科近期收治1例以多浆膜腔积液为表现的患者,现报道如下。
1 临床资料患者为中年男性,因“腹胀伴双下肢水肿2月”入院。
既往1年前诊断为格林巴利综合征,服用醋酸泼尼松,50 mg/d。
甲状腺功能减退11月,间断服用优甲乐治疗。
无乙肝、丙肝等慢性肝炎病史,无长期大量饮酒史。
体格检查:精神差,颜面水肿,甲床苍白。
腹部轻度肌紧张,肝脏未扪及,脾脏轻度肿大,移动性浊音阳性。
双下肢Ⅰ度水肿。
四肢肌张力降低,肌反射减弱,病理征未引出。
辅助检查:腹水常规及生化提示漏出液。
腹水脱落细胞学检查见大量组织细胞及少量间皮细胞。
尿本周氏蛋白定性检查阴性。
POEMS 综合征4 例临床分析并文献复习摘要】目的探讨POEMS 综合征的临床特征及治疗方法。
方法对4 例POEMS 综合征患者临床资料、相关检查及治疗方法进行回顾性分析。
结果 4 例患者均有多发性神经病、异常球蛋白血症及内分泌异常,其他症状还有水肿、肝脾大等。
结论 POEMS 综合征是一种少见的多脏器损害疾病,较难诊断。
临床上对可疑病例需进行密切观察及必要的检查,以免误诊。
治疗并无特效药物,尚处于探讨阶段。
【关键词】POEMS 综合征;诊断;治疗POEMS syndrome in 4 cases and literature review.[Abstact] Objective To investigate the clinical features of POEMS syndrome and treatment. Methods clinical data,related examinations and treatment about 4 cases of POEMS syndrome were retrospectively analyzed. Results 4patients had polyneuropathy,abnormal hypergammaglobulinemia and endocrine abnormalities, there are other symptoms of edema, hepatosplenomegaly and so on. Conclusion POEMS syndrome is a rare disease with multipleorgan damage, more difficult to diagnose. Clinically suspected cases are need close observation and inspection necessary to avoid misdiagnosis. drug treatment is no effects and is still in the exploratory stage.[Keywords] POEMS syndrome; diagnosis; treatmentPOEMS 综合征是一种病因和发病机制均未明了的疾病。
以全身水肿和色素沉着为主要表现P OE MS综合征一例报告陈文丽,樊毫军,高红梅,张永青,张健鹏(武警总医院呼吸科,北京 100039)[关键词] P OE MS综合征/并发症;水肿/病因学;色素沉着过多/病因学;病例报告[文献类型] 患者男性,57岁,农民,因间断性全身水肿7个月加重伴腹胀1个月于2005年11月20日入院。
患者于2005年4月中旬无诱因出现双足水肿,在当地医院给予利尿治疗后水肿稍有好转。
同年10月中旬出现全身水肿、腹胀、胸闷气短,并出现全身色素沉着,全身皮肤呈黑褐色,为进一步诊治,入住本科。
2003年11月曾患面神经炎,留有右眼睑下垂,偶有面肌抽搐。
自诉近半年来性欲减退,患病以来一直无发热。
查体:T36℃,神志清,眼睑水肿,巩膜无黄染,皮肤黏膜未见出血点、肝掌及蜘蛛痣,全身浅表淋巴结未触及肿大,全身皮肤呈黑褐色,皮肤增厚,触之呈橡皮样。
双下肺可闻及湿性罗音,心率88次/ m in,律齐,各瓣膜听诊区未闻及杂音。
腹部膨隆,无静脉曲张,腹壁僵硬,揉面样感觉,未扪及包块,墨菲征(-),肝脾触诊不满意,移动性浊音(+)。
阴囊色素沉着,水肿明显,面部及四肢重度凹陷性水肿。
四肢腱反射减低。
眼科检查:双视乳头水肿,右眼屈光不正,右眼睑痉挛。
入院检查:T30142ng/m l、T4 45142ng/m l、TSH1116μI U/m l、I gG2913g/L(升高)、I g M2166 g/L(升高)、补体C31105g/L,抗双链DNA、E NA抗体谱、ANA 均为阴性,AS O正常,RF8917I U/m l,CRP3816mg/L,蛋白电泳Ga mma3416,余均正常,肝炎方面检查未见异常。
尿酸516μmol/L,肌酐及尿素正常,餐后1h、2h血糖正常,餐后3h血糖7172mmol/L(升高),睾酮1416ng/dl,皮质醇613ng/m l。
尿I g轻链K AP2196mg/dl(升高),尿I g轻链LAM01566mg/dl (升高),胸腹部CT双侧少量胸腔积液,心包积液及腹水,彩超示脾大。
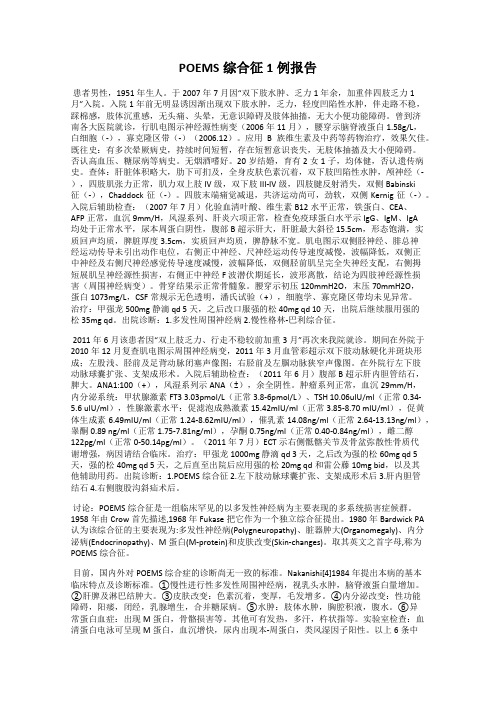
中南大学学报(医学版)J Cent South Univ (Med Sci)2019, 44(6) htt p://706POEMS syndrome presenting with abdominal distension, lower limb edema and shortness of breath: A case reportand literature reviewZ HANG Jiayi 1, OUYANG Zeying 1, LI Rong 2, LENG Aiming 1, LIU Ting 1( 1. Department of Gastroenterology, Xiangya Hospital, Central South University, Changsha 410008;2. Department of Gastroenterology, Second Xiangya Hospital, Central South University, Changsha 410011, China )ABSTRACTP OEMS syndrome is a rare paraneoplastic disorder. A 60-year-old female patient was admitt ed to the Department of Gastroenterology, Xiangya Hospital of Central South University (Changsha, China), complaining of abdominal distension, severe edema of both lower limbs and shortness of breath for more than 1 year. Aft er intensive and careful medical investigations, the patient manifested with polyneuropathy, M-proteinemia, splenomegaly, lymphadenopathy, hypothyroidism, extravascular volume overload, sclerotic bone lesions, elevated VEGF and pulmonary hypertension. According to the latest diagnostic criteria of POEMS syndrome, this patient met two mandatory major criteria, two other major criteria and three minor criteria, the diagnosis was clear aft er ruling out differential diagnosis. The patient was treated with dexamethasone and lenalidomide, which relieved her clinical symptoms. The pathogenesis of POEMS syndrome is not fully understood; however, increased levels of vascular endothelial growth factor may contribute to most of the clinical manifestations. This patient had been in physical discomfort for more than 14 months, which seriously aff ected her quality of life. Clinically, the awareness of early diagnosis and treatment of POEMS syndrome should be improved.KEY WORDSP OEMS syndrome; vascular endothelial growth factor; pulmonary hypertension; edema; Castleman’s diseaseDate of reception: 2018-11-13First author: ZHANG Jiayi, Email: 168112161@, ORCID: 0000-0002-3776-4683Corresponding author: LIU Ting, Email: liuting818@, ORCID: 0000-0001-7083-1238Foundation item: Th is work was supported by the fund from Changsha Science and T echnology Bureau (1701090) and Hunan Provincial Natural Science Foundation (2018JJ2664), China.DOI:10.11817/j.issn.1672-7347.2019.06.015htt p:///xbwk/fileup/PDF/201906706.pdf·CASE ANALYSES · ·临床病例讨论·POEMS syndrome presenting with abdominal distension, lower limb edema and shortness of breath: A case report and literature review ZHANG Jiayi , et al 707POEMS syndrome is a rare paraneoplastic disorder which involve multiple symptoms, including polyneuropathy, organomegaly, endocrinopathy, M-proteinemia and skin changes. Not all patients have all of these symptoms [1]. POEMS syndrome is associated with an underlying clonal plasma cell dyscrasia [2], but the mechanism by which plasma cells cause POEMS syndrome is not fully understood. Vascular endothelial growth factor (VEGF) is a major diagnostic criterion for POEMS syndrome, and may be responsible for many clinical presentations of the syndrome. The incidence of POEMS syndrome is low, but the misdiagnosis rate and mortality rate are high. It takes an average of 18 months from the onset of symptoms to a definitive diagnosis [3], and by the time the diagnosis is made, patients have developed multiple systemic impairments, and common causes of death include cardiopulmonary failure, coagulation disorders, long-term use of glucocorticoids and infections caused by immunosuppressive agents [1]. Therefore, early identification of this disease is very important due to its distinctive manifestations, difficult diagnosis and high mortality rate. We report a successful diagnosis of POEMS syndrome in a female patient. Lenalidomide and dexamethasone therapy was initiated after diagnosis. The patient had a good prognosis and was subsequently discharged from hospital.以腹胀、双下肢水肿、气促为表现的POEMS 综合征1例及文献复习张嘉怡1,欧阳泽颖1,李荣2,冷爱民1,刘霆1(中南大学 1. 湘雅医院消化内科,长沙 410008;2. 湘雅二医院消化内科,长沙 410011)[摘要] POEMS 综合征是一种少见的副肿瘤性疾病。
中南大学湘雅医院消化内科收治1例60岁女性POEMS 综合征患者,其腹胀病史超过1年,并伴有严重的双下肢水肿及气促;检查结果提示多发性周围神经病变、M 蛋白血症、脾肿大、淋巴结肿大、甲状腺功能减退、血管外容量负荷超载、硬化性骨病变、VEGF 升高和肺动脉高压。
根据POEMS 综合征的最新诊断标准,患者满足2个强制性主要标准、2个其他主要标准和3个次要标准,排除鉴别诊断后POEMS 综合征诊断明确。
患者接受地塞米松及来那度胺治疗,临床症状得到明显改善。
POEMS 综合征的发病机制尚不完全清楚,VEGF 水平的升高可能与上述临床表现有关。
该患者病史超过14个月,严重影响其生活质量,临床上应提高对POEMS 综合征早期诊断和早期治疗的意识。
[关键词] POEMS 综合征;血管内皮生长因子;肺动脉高压;水肿;Castleman 病1 Case reportOn November 9, 2017, a 60-year-old female patient was admitted to the Department of Gastroenterology, Xiangya Hospital of Central South University (Changsha, China), complaining of abdominal distension, severe edema of both lower limbs and shortness of breath. Her past medical history showed that she had type 2 diabetes for more than 4 years. She had no history of coronary heart disease, hypertension, hypercholesterolemia, alcohol consumption, cigarette smoking or drug abuse, and her family history was unremarkable.On admission, body temperature was 36.6 ℃; respiration rate, 14 min –1; heart rate, 86 min –1; and blood pressure, 15.7/10.4 kPa. Physical examination revealed severe edema of both lower limbs, and soft lymph nodes were palpable in the supraclavicular fossa, infraclavicular fossa and axillary fossa. Abdominal examination identified generalized tenderness without rebound tenderness. The patient’s body mass had decreased by 2 kg in the past year.Laboratory data on admission demonstrated a decrease in red blood cells (3.05×1012/L),hemoglobin (85 g/L) and platelets (116×109/L), which suggested moderate anemia. However, liver function, serum tumor markers, NT-proBNP, blood glucose, markers of viral hepatitis, and cardiac enzymes were within normal中南大学学报(医学版), 2019, 44(6) 708limits. Renal function test indicated increased uric acid. The HIV antibody was negative. Blood coagulation tests showed increased activated partial thromboplastin time and increased plasma D-dimer. Analysis of endocrine hormones revealed decreased free triiodothyronine, free tetraiodothyronine and increased thyroid stimulating hormone, which was suggestive of hypothyroidism. Serum VEGF was significantly increased (660.41 pg/mL, normal range: 0–142 pg/mL), which supported the diagnosis of POEMS syndrome and indicated the disease activity[4-6]. Serum immunofixation electrophoresis revealed increased production of M-protein, λ light chains and IgA.An electromyogram revealed motor and sensory polyneuropathy, with typical demyelination at the proximal and distal ends of peripheral nerves in all four limbs. Electrocardiography was normal. An abdominal color Doppler ultrasonography scan showed splenomegaly, ascites and multiple enlarged lymph nodes in the abdominal cavity. Echocardiography showed enlarged left atria, moderate tricuspid regurgitation, mild mitral regurgitation, pulmonary hypertension (systolic pulmonary artery pressure≈7.2 kPa), and pericardial effusion. Right heart catheterization showed moderate pulmonary hypertension(pulmonary arterial pressure = 6.0 kPa). Bone scanning revealed bone metabolism abnormality in the right sixth rib. CT scanning showed the signs of infection in the lungs, pulmonary hypertension, abdominal cavity, pelvic cavity and pericardial effusions, abdominal wall edema, and splenomegaly. Ventilation/ perfusion lung scanning, spirometry results and arterial blood gas analysis were normal. The patient also exhibited lymphadenopathy in the retroperitoneal, abdominal cavity and bilateral inguinal regions. The patient’s lymph node next to the right external iliac artery was obtained by biopsy (Figure 1) and immunohistochemistry revealed dysplasia of plasma cells which were positive for CD38, CD138, Ki-67 and kappa light chain, and negative for CD20 and CD21.According to the 2017 update on the diagnosis of POEMS syndrome[7], the patient was diagnosed with POEMS syndrome. Most studies have showed that in patients with POEMS syndrome, autologous stem cell transplantation and long-term thalidomide therapy can cause underlying connective tissue disease and neurological complications. However, lenalidomide is effective and safe and has some neurological benefit in patients with POEMS syndrome, as it can alleviate neurological symptoms and decrease plasma VEGF level[7]. Considering the patient’s physical condition, we opted for low-dose steroid treatment (oral dexamethasone, 10 mg/d) and oral lenalidomide treatment (10 mg/d). Her condition was stable, and the symptoms of abdominal distension, lower limb edema and shortness of breath improved after treatment.Dispenzieri proposed widely accepted diagnostic criteria in 2017 in an attempt to standardise the various features and investigation findings necessary to make a diagnosis of POEMS syndrome[7]. The diagnosis is definite when both the polyneuropathy and monoclonal gammopathy are present in combination with one of the other three major criteria (Castleman’s disease, sclerotic bone lesions and increased levels of VEGF), and one of the six minor criteria (organomegaly, endocrinopathy, extravascular volume overload, skin changes, papilloedema, thrombocytosis/polycythemia). The clinical features of this patient included splenomegaly, lymphadenopathy, hypothyroidism, extravascular volume overload, sclerotic bone lesions, and pulmonary hypertension. Her laboratory examination presented a λ-type IgA monoclonal gammopathy and elevated VEGF; electromyogram manifested motor and sensory polyneuropathy, with typical demyelination at the proximal and distal ends of peripheral nerves in all four limbs. Our patient fulfilled two mandatory major criteria, two other major criteria and three minor criteria. The diagnosis was confirmed after excluding other differential diagnoses. Liver cirrhosis can be characterized by hepatosplenomegaly and ascites, our patient’s liver function is normal and there is no history of hepatitis B virus infection or other causes of cirrhosis. Therefore, the above symptoms caused by liver cirrhosis are not considered. Although Guillain Barre Syndrome has the characteristics of symmetrical lower limb motor neuron paralysis and separation of cerebrospinal fluid protein cells, it should not be accompanied by organomegaly and skin changes, and the determination of serum M protein can be helpful for identification. In addition, connective tissue disease also has urinary protein, hematologic disorder and dysimmunity, but accompanied by peripheral nerve damage and organomegaly is uncommon.POEMS syndrome presenting with abdominal distension, lower limb edema and shortness of breath: A case report and literature review ZHANG Jiayi, et al709 Figure 1 HE staining showing the lymph node next to the right external iliac artery with abnormal proliferation of plasma cellsA: ×100; B: ×2002 DiscussionPOEMS syndrome can be traced back to 1958 when it was described by Crow for the first time. In 1980, the first systematic study of POEMS syndrome was reported by Bardwick et al[8], who suggested that the main characteristics of POEMS syndrome were polyneuropathy, organomegaly, endocrinopathy, M-proteinemia and skin changes. He used acronyms of these characteristics and named them the POEMS syndrome. POEMS syndrome is also called Crow-Fukase syndrome[9] or Takatsuki syndrome[10]. Most studies[9-10] have been carried out in Japan; however, over the past decades, the incidence of POEMS syndrome has increased worldwide, including the United States, C hina, India and France[3, 11-12]. Although the pathogenesis of POEMS syndrome is not completely understood, many scholars hold the view that abnormal cytokine hyperproduction may be responsible for this disease, such as interleukin (IL)-6, IL-8, tumor necrosis factor-α (TNF-α) and VEGF[13-14]. The clinical manifestations of POEMS syndrome are extremely variable and nonspecific; therefore it is difficult to establish an accurate diagnosis quickly. However, detailed history and physical examination combined with appropriate laboratory tests can help differentiate this syndrome from other diseases.POEMS syndrome is believed to be related to a number of clinical symptoms. Several clinical studies have shown that almost all patients have multiple peripheral neuropathy (PN), and the incidence rates of other manifestations are: organomegaly (45%–85%), Castleman’s disease (11%–25%), endocrinopathy (67%–84%), diabetes (3%–36%), hypothyroidism (9%–67%), abnormal proliferation of monoclonal plasma cells (100%), M-proteinemia (24%–54%) and skin changes (68%–89%)[7, 15].In this case, severe edema in patient’s both lower limbs was one of the classic symptoms, and the possibility of nephrogenic, hepatogenic, cardiogenic, endocrine and autoimmune edema should be also considered. In addition, the patient had mild hypothyroidism, which could explain her severe edema of the lower limbs, but it was difficult to explain the patient’s accompanying multiple serous cavity hydrops, organomegaly and multiple lymphadenopathies. Our patient did not have a history of heart disease or hepatic disease. Since there are no sufficient diagnostic criteria for nephrotic syndrome or nephritis, lower limb edema was unlikely to be due to cardiac, hepatogenic, or nephrogenic diseases. Following thyroid hormone replacement therapy, the patient's edema did not significantly improve, and the diagnosis of POEMS syndrome was confirmed by lymph node biopsy and immunohistochemistry. Some studies have shown that increased VEGF and decreased serum erythropoietin induced functional alterations in the vessel wall that lead to increased permeability and edema[6, 16-17].Pulmonary arterial hypertension (PAH) is an interesting clinical manifestation in this case. PAH is characterized by an elevated mean pulmonary artery pressure of ≥3.3 kPa, with a normal pulmonary artery wedge pressure. This serious disease results in progressive right-sided heart failure and ultimately death[18]. Our patient had no evidence of portal hypertension on liver ultrasound, biologic data on renal and hepatic functionsA B中南大学学报(医学版), 2019, 44(6) 710were within normal limits, and chronic thromboembolic pulmonary hypertension was excluded after ventilation/ perfusion lung scan. Pulmonary hypertension caused by lung diseases or hypoxia were also excluded based on spirometric results and arterial blood gas analysis. No specific PAH gene mutations were identified. The patient had obvious chest tightness and shortness of breath, and right heart catheterization showed moderate pulmonary hypertension, and serum VEGF was markedly increased which may explain the occurrence of PAH. According to a retrospective study of 137 patients with POEMS syndrome carried out in the United States, 25% of patients also had pulmonary disease[19], in particular, pulmonary hypertension, and severe pulmonary hypertension could cause right heart failure or death. The pathogenesis of POEMS syndrome-associated pulmonary hypertension is currently unclear; however, excessive production of immune mediators in POEMS syndrome with pulmonary hypertension has been reported by Feinberg et al[20]. Increased baseline levels of VEGF, TNF-α, IL-6, abnormally low levels of sIL-6R and HHV-8 infection appear to be associated with the pathogenic manifestations of POEMS syndrome with PAH[21-23].Overproduction of serum VEGF was another meaningful presentation in this patient. Data from several reports have identified increased VEGF level as a useful biomarker for POEMS syndrome, which may also assess disease activity and correlate with therapeutic response[14, 24-25]. Fulfillment of the diagnostic criteria together with other findings prompted the diagnosis of POEMS syndrome in this patient. VEGF is expressed by osteoblasts, macrophages, tumor cells[14], plasma cells[26-27], and megakaryocytes/platelets[28]. VEGF targets endothelial cells, leads to a fast and irreversible increase in neovascularization and vasopermeability which may trigger symptoms of POEMS syndrome, such as angiomata, pleural effusion, edema, polyneuropathy, and organomegaly. Plasma cells and platelets both release VEGF in POEMS syndrome, and due to the secretion of VEGF from platelets in vitro during serum processing, serum VEGF level is higher than plasma VEGF level. The plasma VEGF critical value is 200 pg/mL (specificity: 95%; sensitivity: 68%)[6], the serum VEGF critical value is 1 920 pg/mL (specificity: 98%; sensitivity: 73%)[29]. However, overexpression of VEGF in serum can also be observed in other diseases, such as rheumatoid arthritis, systemic lupus erythematosus and multiple myeloma. Wang et al revealed a correlation between N-terminal propeptide of type I collagen and POEMS syndrome. They demonstrated that N-terminal propeptide of type I collagen was a new biomarker for the diagnosis of POEMS syndrome and the best threshold of this biomarker in the diagnosis of POEMS syndrome is 70 ng/mL (specificity: 91.5%; sensitivity: 80%)[29].Castleman’s disease is currently considered to be an unexplained reactive lymphoproliferative disorder[30], and is one of three other major criteria in the diagnosis of POEMS syndrome[7]. Castleman’s disease or Castleman-like histology occurs in 11%–30% patients with POEMS syndrome[31]. Castleman’s disease is classified into two major types: unicentric CD (UCD) and multicentric CD (MCD). A subset of multicentric CD (MCD) is caused by human herpesvirus-8 (HHV-8) (HHV-8-associated MCD), while HHV-8-negative MCD cases remain idiopathic (iMCD)[32]. Castleman’s disease and HIV also have strong relationships[33]. Castleman’s disease is a diagnosis of exclusion, and the ultimate investigation is a pathological diagnosis made by excisional biopsy of affected lymph node tissue, it can be classified into three types based on pathological characteristics: hyaline vascular type (HV), plasma cell type (PC) and mixed type[34]. In the hyaline-vascular subtype, the centers of the huge folliculus lymphaticus are atrophied, numerous hyalinized blood vessels are increased, and a portion have an “onion-skinning” appearance[35-36]. In the plasmacytic subtype, the lymphoid follicles are variably characterized by germinal centers which are hyperplastic or regressive[34], and the plasma cells are mainly spread throughout the interfollicular areas[37]. In the mixed type, it has the typical histology of the mixed form, and there are numerous immunoblasts. In this case, our patient without any pathological features of increased numbers of hyalinized blood vessels, hyperplastic or regressive changes in the follicles of involved lymph nodes, or obvious “onion-like skin” appearance, and the patient’s laboratory examinations showed that the HIV antibody was negative. So our patient could not be diagnosed as Castleman’s disease. VEGF is the most consistently elevated cytokine of POEMS syndrome, in contrast to POEMS syndrome, IL-6 is the major abnormally overexpressed cytokine of Castleman’s disease[7]. In CD, the PN is less frequent, more subtle, and more sensory than that of POEMS patients. Only patientsPOEMS syndrome presenting with abdominal distension, lower limb edema and shortness of breath: A case report and literature review ZHANG Jiayi , et al 711(ASCT) and the use of drugs, such as alkylators, corticosteroids, bevacizumab, rituximab, bortezomib, and thalidomide [55-56]. Radiotherapy doses in patients with fewer than three bone lesions, no bone-marrow involvement and no medullar infiltration, should be 40 Gy or more [57-58]. ASCT is effective in POEMS syndrome [59-60], although it seems to be accompanied by a worrying number of complications [61]. Dexamethasone, thalidomide and lenalidomide are also beneficial in patients with POEMS syndrome [62-63].In conclusion, POEMS syndrome is rare, delayed diagnosis combined with advanced stage lead to a poor prognosis; therefore, recognition and early diagnosis of this syndrome are crucial. This case will contribute to an improved understanding of the clinical presentation and laboratory indicators of POEMS syndrome. With further research, a more comprehensive recognition and scientific basis of the disease will provide the best treatment strategies in the future.References[1]Dispenzieri A, Kyle RA, Lacy MQ, et al. POEMS syndrome: definitions and long-term outcome[J]. Blood, 2003, 101(7): 2496-2506.[2]Dispenzieri A. POEMS syndrome: update on diagnosis, risk-stratification, and management[J]. Am J hematol, 2015, 90(10): 951-962.[3]Li J, Zhou DB, Huang Z, et al. Clinical characteristics and long-term outcome of patients with POEMS syndrome in China[J]. Ann Hematol, 2011, 90(7): 819-826.[4]Scarlato M, Previtali SC, Carpo M, et al. Polyneuropathy in POEMS syndrome: role of angiogenic factors in the pathogenesis[J]. Brain, 2005, 128(Pt 8): 1911-1920.[5]Goto H, Nishio M, Kumano K, et al. Discrepancy between disease activity and levels of vascular endothelial growth factor in a patient with POEMS syndrome successfully treated with autologous stem-cell transplantation[J]. Bone Marrow Transplant, 2008, 42(9): 627-629.[6]D ’Souza A, Hayman SR, Buadi F, et al. The utility of plasma vascular endothelial growth factor levels in the diagnosis and follow-up of patients with POEMS syndrome[J]. Blood, 2011, 118(17): 4663-4665.[7]Dispenzieri A. POEMS syndrome: 2017 Update on diagnosis, risk stratification, and management[J]. Am J Hematol, 2017, 92(8): 814-829.[8]Bardwick PA, Zvaifler NJ, Gill GN, et al. Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skinwith PN and a plasma cell clone can be diagnosed with POEMS syndrome, and if a patient has other POEMS symptoms, but without these two features, the patient can be classified as having Castleman’s disease.PN is one of the mandatory major criteria, and it is normally depicted as a ascending, peripheral, symmetrical, and demyelinating on ner ve conduction studies (NCS)[38-39]. POEMS syndrome should be differentiated from other neuropathies associated with monoclonal gammopathies such as monoclonal gammopathy of undetermined significance (MGUS)[40-42]. The presence of a λ-type IgA or IgG monoclonal gammopathy is required for the diagnosis of the POEMS syndrome. In MGUS-associated neuropathy the paraprotein is IgM more generally [43-44]. The most typical presentation in IgM MGUS is distal acquired demyelinating symmetric neuropathy [45], which manifests slowly progressive sensory neuropathy with predominantly distal numbness, ataxia, and mild to no weakness. IgM isotype is also associated with Waldenström’s macroglobulinemia (WM), a lethal lymphoproliferative disease characterized by a monoclonal lymphoplasmacytosis within the bone marrow and/or the peripheral lymphatic tissue accompanied by an elevated serum IgM M protein [46-47], and most of patients have myelin-associated glycoprotein (MAG) antibodies on serologic testing [48]. Although WM and POEMS syndrome may both have neuropathy and papilloedema [49], a bone marrow biopsy is effective to distinguish the two diseases [50-51]. PN is a usual presentation of primary amyloidosis (AL), which is a multisystemic disease characterized by widespread amyloid deposition. The PN in AL is typically a progressive, distal, symmetric sensory neuropathy with autonomic dysfunction. The main clinical features of AL included loss of light touch and temperature sensation, painful dysesthesia, and marked autonomic involvement [52-53]. The diagnosis depends on the histological confirmation, which can be accomplished through Congo red staining or mass spectrometry of biopsied tissue. The histological examination demonstrates the amyloid deposits in tissue obtained from involved organs [53]. POEMS syndrome and AL can be differentiated by bone marrow findings and the plasma or serum VEGF level [7, 54].Due to the rarity of the disease, prospective therapeutic clinical trials are rare. To date, treatment strategies for POEMS syndrome include radiation, chemotherapy, autologous stem cell transplantation中南大学学报(医学版), 2019, 44(6) 712changes: the POEMS syndrome. Report on two cases and a review ofthe literature[J]. Medicine, 1980, 59(4): 311-322.[9] Nakanishi T, Sobue I, Toyokura Y, et al. The Crow-Fukase syndrome:a study of 102 cases in Japan[J]. Neurology, 1984, 34(6): 712-720.[10] Takatsuki K, Sanada I. Plasma cell dyscrasia with polyneuropathy andendocrine disorder: clinical and laboratory features of 109 reportedcases[J]. Jpn J Clin Oncol, 1983, 13(3): 543-555.[11] Kulkarni GB, Mahadevan A, Taly AB, et al. Clinicopathologicalprofile of polyneuropathy, organomegaly, endocrinopathy, M proteinand skin changes (POEMS) syndrome[J]. J Clin Neurosci, 2011,18(3): 356-360.[12] Zhang B, Song X, Liang B, et al. The clinical study of POEMSsyndrome in China[J]. Neuro Endocrinol Lett, 2010, 31(2): 229-237.[13] Gherardi RK, Belec L, Soubrier M, et al. Overproduction ofproinflammatory cytokines imbalanced by their antagonists inPOEMS syndrome[J]. Blood, 1996, 87(4): 1458-1465.[14] Soubrier M, Dubost JJ, Serre AF, et al. Growth factors in POEMSsyndrome: evidence for a marked increase in circulating vascularendothelial growth factor[J]. Arthritis Rheum, 1997, 40(4): 786-787.[15] Gandhi GY, Basu R, Dispenzieri A, et al. Endocrinopathy in POEMSsyndrome: the Mayo Clinic experience[J]. Mayo Clin Proc, 2007,82(7): 836-842.[16] Hashiguchi T, Arimura K, Matsumuro K, et al. Highly concentratedvascular endothelial growth factor in platelets in Crow-Fukasesyndrome[J]. Muscle Nerve, 2000, 23(7): 1051-1056.[17] Soubrier M, Guillon R, Dubost JJ, et al. Arterial obliteration inPOEMS syndrome: possible role of vascular endothelial growthfactor[J]. J Rheumatol, 1998, 25(4): 813-815.[18] Rubin LJ. Primary pulmonary hypertension[J]. N Engl J Med, 1997,336(2): 111-117.[19] Allam JS, Kennedy CC, Aksamit TR, et al. Pulmonary manifestationsin patients with POEMS syndrome: a retrospective review of 137patients[J]. Chest, 2008, 133(4): 969-974.[20] Feinberg L, Temple D, de Marchena E, et al. Soluble immunemediators in POEMS syndrome with pulmonary hypertension: casereport and review of the literature[J]. Crit Rev Oncog, 1999, 10(4):293-302.[21] Lesprit P, Godeau B, Authier FJ, et al. Pulmonary hypertension inPOEMS syndrome: a new feature mediated by cytokines[J]. Am JRespir Crit Care Med, 1998, 157(3 Pt 1): 907-911.[22] Dorfmuller P, Perros F, Balabanian K, et al. Inflammation inpulmonary arterial hypertension[J]. Eur Respir J, 2003, 22(2): 358-363.[23] Humbert M, Monti G, Brenot F, et al. Increased interleukin-1 andinterleukin-6 serum concentrations in severe primary pulmonaryhypertension[J]. Am J Respir Crit Care Med, 1995, 151(5): 1628-1631.[24] Misawa S, Sato Y, Katayama K, et al. Vascular endothelial growthfactor as a predictive marker for POEMS syndrome treatmentresponse: retrospective cohort study[J]. BMJ Open, 2015, 5(11):e009157.[25] Misawa S, Sato Y, Katayama K, et al. Safety and efficacy ofthalidomide in patients with POEMS syndrome: a multicentre,randomised, double-blind, placebo-controlled trial[J]. LancetNeurol, 2016, 15(11): 1129-1137.[26] Endo I, Mitsui T, Nishino M, et al. Diurnal fluctuation of edemasynchronized with plasma VEGF concentration in a patient withPOEMS syndrome[J]. Intern Med, 2002, 41(12): 1196-1198. [27] Nakano A, Mitsui T, Endo I, et al. Solitary plasmacytoma withVEGF overproduction: report of a patient with polyneuropathy[J].Neurology, 2001, 56(6): 818-819.[28] Koga H, Tokunaga Y, Hisamoto T, et al. Ratio of serum vascularendothelial growth factor to platelet count correlates with diseaseactivity in a patient with POEMS syndrome[J]. Eur J Intern Med,2002, 13(1): 70-74.[29] Wang C, Zhou YL, Cai H, et al. Markedly elevated serum totalN-terminal propeptide of type I collagen is a novel marker for thediagnosis and follow up of patients with POEMS syndrome[J].Haematologica, 2014, 99(6): 78-80.[30] Dispenzieri A, Armitage JO, Loe MJ, et al. The clinical spectrum ofCastleman's disease[J]. Am J Hematol, 2012, 87(11): 997-1002. [31] Naddaf E, Dispenzieri A, Mandrekar J, et al. Clinical spectrum ofCastleman disease-associated neuropathy[J]. Neurology, 2016,87(23): 2457-2462.[32] Fajgenbaum DC, Uldrick TS, Bagg A, et al. International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathicmulticentric Castleman disease[J]. Blood, 2017, 129(12): 1646-1657.[33] Dong Y, Wang M, Nong L, et al. C linical and laboratorycharacterization of 114 cases of Castleman disease patients froma single centre: paraneoplastic pemphigus is an unfavourableprognostic factor[J]. Br J Haematol, 2015, 169(6): 834-842. [34] Szalat R, Munshi NC. Diagnosis of Castleman disease[J]. HematolOncol Clin North Am, 2018, 32(1): 53-64.[35] Talat N, Belgaumkar AP, Schulte KM. Surgery in Castleman's disease:a systematic review of 404 published cases[J]. Ann Surg, 2012,255(4): 677-684.[36] Schaefer IM, Gunnel H, Schweyer S, et al. Unicentric Castleman’sdisease located in the lower extremity: a case report[J]. BMCCancer, 2011, 11: 352.[37] Wang HW, Pittaluga S, Jaffe ES. Multicentric Castleman disease:Where are we now?[J]. Semin Diagn Pathol, 2016, 33(5): 294-306.[38] Dispenzieri A. POEMS syndrome: 2014 update on diagnosis, risk-stratification, and management[J]. Am J hematology, 2014, 89(2):214-223.[39] Nasu S, Misawa S, Sekiguchi Y, et al. Different neurologicaland physiological profiles in POEMS syndrome and chronicinflammatory demyelinating polyneuropathy[J]. J Neurol Neurosurg。