幽门螺杆菌感染机制
- 格式:pdf
- 大小:122.45 KB
- 文档页数:10

幽门螺旋杆菌是人类胃肠道的一种常见细菌。
它是一种螺旋状的革兰氏阴性菌,能在人类胃黏膜上生长繁殖,是导致慢性胃炎、消化性溃疡、胃癌等疾病的主要病因之一。
近年来,随着人们的生活水平不断提高,胃癌和胃肠道疾病的患病率也在不断上升,因此,了解的发病机制、诊断和治疗方法,对于控制和预防该类疾病具有重要的实际意义。
一、的发现和结构最初是由澳大利亚的两位科学家独立发现的。
在1982年,澳大利亚研究人员罗宾·沃伦发现在许多患有胃炎和消化性溃疡的患者胃内均存在这种细菌,随后,在同一年,澳大利亚的马歇尔也发现了类似的情况,并通过自己吞食了培养细菌的试管证明了细菌导致胃炎、消化性溃疡和胃癌的关系,从而赢得了诺贝尔生理学或医学奖。
随着技术的不断进步,人们对的结构和特性也有了较为深入的了解。
的外壳是由多种不同结构的蛋白质和糖类分子形成的。
其中,血型抗原是其最重要的成分之一。
通过这些抗原在胃黏膜上形成稳定的结构,以抵抗胃液和黏液的侵蚀,从而生存和繁殖。
同时,的细胞壁还含有大量的脂质DNA,这些脂质DNA可以与宿主胃黏膜细胞的核酸结合,并将致癌物质注入宿主细胞内,引发细胞发生癌变。
二、的发病机制会释放毒素和炎症因子,引发宿主胃黏膜发生炎性反应,造成慢性胃炎。
长期的胃炎可以导致胃黏膜萎缩和溃疡形成。
除此之外,还可以刺激宿主产生大量的胃酸,进一步破坏胃黏膜,加速病情的恶化。
而且,慢性胃炎的高风险人群和长期患病者有患胃癌的风险。
三、的检测方法感染并不一定引起症状,因此,很多人并不知道自己感染了。
对于有感染风险的人群,如长期使用类固醇或非甾体类药物、曾经患有胃病、胃肠道手术史以及家族中有慢性胃炎或胃癌患者等人群,应该定期进行的检测。
的检测方法包括呼气试验、血清学检测和胃镜检查等。
其中,呼气试验是一种安全、无痛和非创伤性的检测方法,可用于初步筛查感染。
血清学检测通过检测血液中存在的特异性抗体水平来诊断感染。
胃镜检查是一种准确、可靠的检测方法,能够直接观察胃粘膜的病理改变,并采用组织学等方法进行的检测。

幽门螺杆菌感染与儿童胃肠道疾病的关系随着医学研究的不断发展,我们对于儿童胃肠道疾病的认识和理解也越来越深入。
其中,幽门螺杆菌感染被认为是一种常见的病原因素,在儿童胃肠道疾病的发病机制中起到重要的作用。
本文将就幽门螺杆菌感染与儿童胃肠道疾病的关系展开讨论,并对相关研究进行梳理与归纳。
一、幽门螺杆菌感染及其病因幽门螺杆菌(Helicobacter pylori)是一种生活在人类胃黏膜中的革兰氏阴性菌。
该菌的感染主要通过口腔-口腹道传播途径进行,其中儿童和成人之间的感染率存在一定的差异。
传播途径主要包括飞沫传播、食物与水源传播以及人际接触传播等。
研究表明,幽门螺杆菌感染与胃病、十二指肠溃疡、胃癌等胃肠道疾病密切相关。
幽门螺杆菌通过其可运动性的鞭毛积极化附着于胃黏膜上皮细胞的表面,并释放出多种毒力因子,如细菌毒素、酶和炎性因子等,导致慢性胃炎和其他相关疾病的发生。
二、 1. 慢性胃炎儿童幽门螺杆菌感染常导致慢性胃炎的发生。
研究显示,儿童幽门螺杆菌感染率普遍较高,而感染程度与年龄呈正相关。
在幼儿群体中,幽门螺杆菌感染率尤为突出。
慢性胃炎表现为胃痛、腹泻、恶心、食欲不振等症状,严重时可伴随溃疡形成,影响儿童生长发育。
2. 其他胃肠道疾病除了慢性胃炎,幽门螺杆菌感染还与其他儿童胃肠道疾病的发生密切相关,如反流性食管炎、功能性腹痛等。
反流性食管炎表现为胃酸回流至食管,导致食管黏膜受损,幽门螺杆菌感染被认为是其发病因素之一。
功能性腹痛则是指排除其他明确原因后依然存在的腹痛,幽门螺杆菌感染可能与其发病机制有关。
3. 幽门螺杆菌感染与儿童胃肠道微生态近年来的研究发现,幽门螺杆菌感染与儿童胃肠道微生态的变化密切相关。
幽门螺杆菌感染会引起胃肠道菌群失衡,导致有益菌数量减少,病原菌数量增加,进而导致儿童胃肠道疾病的发生。
这为深入研究幽门螺杆菌感染与儿童胃肠道疾病之间的关系提供了新的思路。
三、幽门螺杆菌感染的诊断和治疗早期发现和诊断儿童幽门螺杆菌感染至关重要。

幽门螺杆菌杆菌试题幽门螺杆菌(H. pylori)是一种常见的胃肠道细菌,它存在于大约一半以上的人体内。
幽门螺杆菌感染与胃炎、胃溃疡和胃癌等胃部疾病密切相关。
针对幽门螺杆菌感染的诊断与治疗,以下是一些试题供参考。
试题一:幽门螺杆菌感染的传播途径幽门螺杆菌主要通过哪些途径传播?请简要描述其传播途径。
另外,列举一些可能存在传染风险的情况。
试题二:幽门螺杆菌感染的致病机制幽门螺杆菌感染胃部组织后,通过哪些机制导致炎症反应和胃部病变?请从细菌特性、毒素产物、免疫反应等方面进行论述。
试题三:幽门螺杆菌感染的临床表现描绘幽门螺杆菌感染常见的临床表现,包括但不限于胃部不适、疼痛、恶心等症状。
并简述为何部分人感染后无明显症状。
试题四:幽门螺杆菌感染的检测方法列举常用的检测方法,包括非侵入性和侵入性方法,并简要说明各自的适用情况、优缺点及操作原理。
试题五:幽门螺杆菌感染的治疗策略针对幽门螺杆菌感染,请简述常见的治疗策略,包括抗生素联合治疗、药物选择、治疗方案等,并对治疗过程中的注意事项进行说明。
试题六:幽门螺杆菌感染的预防措施针对幽门螺杆菌感染的传播,提出一些预防措施。
例如,个人卫生习惯、食品安全要求以及公共场所的卫生管理等方面的措施。
试题七:幽门螺杆菌感染与胃癌的关联幽门螺杆菌感染与胃癌的关系备受关注。
请简要阐述二者之间的关联,包括幽门螺杆菌感染增加胃癌风险的机制等。
试题八:幽门螺杆菌感染在特殊人群中的处理针对孕妇、儿童、老年人等特殊人群中的幽门螺杆菌感染处理,提出适用的诊断和治疗策略。
请从安全性、疗效和特殊情况等角度进行讨论。
总结:通过以上试题,我们从不同的角度探讨了幽门螺杆菌感染的相关问题,包括传播途径、病理机制、临床表现、检测方法、治疗策略、预防措施以及特殊人群的处理等。
对于幽门螺杆菌感染的认识和掌握,有助于提高对该疾病的防治水平,为患者的健康保驾护航。

幽门螺杆菌感染的相关研究现状幽门螺杆菌(Helicobacter pylori)是一种能够寄生在胃黏膜上的螺旋形细菌,是人类胃部最常见的感染源之一。
多年以来,幽门螺杆菌感染与许多胃疾病如胃溃疡、慢性胃炎和胃癌等密切相关。
针对幽门螺杆菌感染的研究已经取得了许多重要发现,本文将就幽门螺杆菌感染的相关研究现状进行探讨。
一、幽门螺杆菌感染的传播途径根据广泛临床观察和实验室研究,人类主要通过口-口接触和食物-口接触途径感染幽门螺杆菌。
这意味着亲密接触(如家庭成员之间)、不洁食品及水源会增加感染的风险。
此外,虫媒也被认为是其中一种可能的传播途径。
母体传播也是导致婴儿和儿童幽门螺杆菌感染的常见原因。
二、幽门螺杆菌感染的致病机制幽门螺杆菌感染主要通过其特有的致病因子引起。
其中最为重要的是尿素酶(urease)和细胞毒素(cytotoxin-associated gene A,简称CagA)。
尿素酶可以将胃内尿素分解为氨和二氧化碳,从而中和胃酸,提供适宜的生存环境给细菌。
CagA则可以通过进入寄主上皮细胞并与其相互作用来引发一系列生物学效应,并介导肠上皮细胞炎症反应。
此外,还有其他一些致病因子如细菌表面黏附分子(adhesins)、组蛋白变构酶等也参与了幽门螺杆菌感染过程。
这些致病因子协同作用引发的产物,如氧化应激、促炎性因子和错过免疫反应等,均对宿主组织产生直接或间接的损害。
三、幽门螺杆菌感染与消化系统疾病1. 胃溃疡:多数胃溃疡患者(超过80%)被证实为幽门螺杆菌感染。
细菌通过破坏胃粘膜抵御感染,引起黏膜屏障功能紊乱,从而导致胃酸和消化酶对黏膜产生直接损害。
2. 慢性胃炎:幽门螺杆菌引起的慢性胃炎是最常见的胃部疾病之一。
感染后,机体会产生炎性细胞浸润和局部免疫反应,释放大量促炎因子和氧自由基等,导致黏膜组织发生变性、坏死以及纤维化。
3. 胃癌:幽门螺杆菌感染是胃癌发展的重要诱导因素之一。
细菌引起的持久慢性肠上皮炎症可导致DNA突变、细胞增殖异常以及凋亡抑制等,从而增加了癌前期阶段及早期癌变的风险。

幽门螺杆菌致病机制的研究进展幽门螺杆菌(H. pylori)是一种嗜酸杆菌,是胃十二指肠黏膜上最主要的细菌。
它已经被证实是导致胃炎、胃溃疡、胃癌等多种胃肠道疾病的重要致病因素之一。
虽然已经有很多研究关注幽门螺杆菌的致病机制,但至今为止,与其相关的致病机制仍然需要重新审视和评估。
本文将从幽门螺杆菌的生物学特性入手,全面探讨幽门螺杆菌的致病机制的最新研究进展。
1. 幽门螺杆菌的基础生物学特性1.1 菌体形态幽门螺杆菌的菌体呈螺旋状,约为3-5微米长,约0.5微米宽。
1.2 适应环境幽门螺杆菌适应在胃肠道环境中生长。
它可以在pH为1.5-8的范围内生存,并且适应气体浓度较低的环境。
它还可以耐受胆盐、胃酸和消毒剂等。
1.3 遗传学特性幽门螺杆菌是一种高变异性细菌,其基因组由1.6到1.8兆碱基组成。
它具有一种特殊的DNA修复机制,可以在高氧环境下修复自身的DNA。
1.4 感染途径幽门螺杆菌感染主要通过口腔或胃肠道进行。
2. 幽门螺杆菌的致病机制2.1 细菌致病因素2.1.1 细菌粘附幽门螺杆菌的菌体表面有许多不同类型的粘附分子,包括血凝素、鲨烷醇、血清透明质酸和蛋白酶切割产物等。
这些分子可以粘附到胃肠道上皮细胞表面的不同分子上,例如细胞膜蛋白和MUC5AC粘液等,从而形成生物膜。
2.1.2 毒素分泌幽门螺杆菌可以分泌出毒素,包括细胞毒素、炎症毒素、溶血素和外毒素。
细胞毒素和炎症毒素可以杀死胃上皮细胞和白细胞,并可能导致胃肠道炎症。
溶血素可以产生毒性,可能导致胃肠道炎症和黏膜损伤。
外毒素可以刺激胃黏膜释放粘液,从而抑制正常的胃消化功能。
2.1.3 上皮细胞的免疫干扰幽门螺杆菌感染会导致胃肠道上皮细胞对免疫系统的免疫抗性降低。
它可以通过抑制胃上皮细胞的抗氧化酶活性,减少胃上皮细胞对自由基的清除能力,从而影响上皮细胞的生长和功能。
此外,幽门螺杆菌还可以通过酪氨酸酶的作用,在氢气过氧化物和氧气的存在下导致氧释放,从而影响上皮细胞的生长和功能。
2024年幽门螺杆菌致病机制的最新进展一、黏附与定植机制幽门螺杆菌(Helicobacter pylori,简称H. pylori)对胃黏膜的黏附与定植是其致病的首要步骤。
近年来的研究表明,H. pylori通过其表面的多种黏附素,如尿素酶、血凝素、脂多糖等,与胃黏膜上皮细胞表面的受体相结合,实现紧密黏附。
这些黏附素不仅增强了细菌在胃黏膜上的定植能力,还通过激活信号通路诱导细胞损伤。
此外,H. pylori还能通过调节自身运动性和趋化性,在胃黏膜上寻找并定植于合适的微环境。
二、炎症与免疫反应H. pylori感染后,胃黏膜会发生慢性炎症,伴随着免疫反应的发生。
这种炎症反应主要由H. pylori的多种毒力因子引起,如细胞毒素相关蛋白(CagA)、空泡毒素(VacA)等。
这些毒力因子能够激活宿主细胞内的信号通路,诱导炎症反应和免疫应答。
同时,H. pylori 还能触发Th1/Th2/Th17等细胞因子的产生,导致胃黏膜的免疫损伤。
三、毒力因子与致病性H. pylori的毒力因子在其致病过程中发挥着关键作用。
其中,CagA和VacA是最具代表性的两种毒力因子。
CagA能够通过T4SS (Type IV Secretion System)系统注入宿主细胞,干扰细胞内的信号转导,导致细胞损伤和凋亡。
而VacA则能形成空泡,破坏宿主细胞的正常结构,引起细胞功能障碍。
此外,H. pylori还表达多种其他毒力因子,如尿素酶、过氧化氢酶等,共同参与了其致病过程。
四、基因突变与耐药性随着抗生素的广泛使用,H. pylori的耐药性问题日益严重。
近年来的研究表明,H. pylori的基因突变是导致其耐药性的重要原因。
这些突变主要发生在抗生素作用靶点相关的基因上,如23SrRNA基因、尿素酶基因等。
这些基因突变使得H. pylori能够逃避抗生素的杀灭作用,从而导致治疗失败。
五、宿主遗传因素与易感性宿主遗传因素在H. pylori感染及其相关疾病的发生发展中起着重要作用。
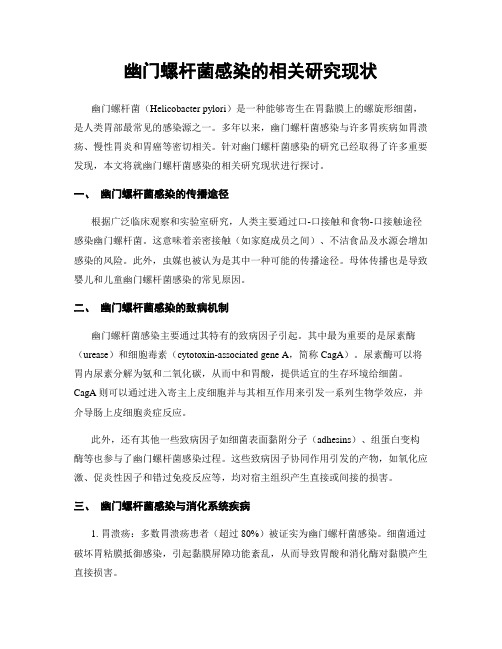
Molecular and Cellular Biochemistry 253: 207–215, 2003.© 2003 Kluwer Academic Publishers. Printed in the Netherlands.Molecular mechanism of action of major Helicobacter pylori virulence factorsSuman Kumar Dhar,1 Rajesh K. Soni,1 Bimal K. Das 2 and Gauranga Mukhopadhyay 11Special Centre for Molecular Medicine, Jawaharlal Nehru University, New Delhi; 2Department of Microbiology, All India Institute of Medical Sciences, New Delhi, IndiaAbstractAlthough Helicobacter pylori infects 50% of the total human population, only a small fraction of the infected people suffer from severe diseases like peptic ulcers and gastric adenocarcinoma. H. pylori strains, host genotypes and environmental fac-tors play important role in deciding the extent and severity of the gastroduodenal diseases. The bacteria has developed a unique set of virulence factors to survive in the extreme ecological niche of human stomach. Together these virulence factors make H.pylori one of the most successful human pathogenic bacteria colonizing more than half of the human population. Understand-ing the mechanism of action of the major H. pylori virulence factors will shed light into the molecular basis of its pathogenic-ity. (Mol Cell Biochem 253: 207–215, 2003)Key words : Helicobacter pylori , virulence factors, type IV secretion system, VacA, PAIntroductionHelicobacter pylori are Gram-negative spiral shaped bacte-ria that infect more than 50% of humans globally [1]. The in-fection normally takes place through faecal-oral pathways.It is now generally accepted that H. pylori causes gastric and duodenal ulcer diseases. Additionally, H. pylori is associatedsified H. pyloridisease die since it is mostly diagnosed at the advance stage.Though H. pylorienvironmental factors [4].Several aspects ofH. pylori infection and of the host re-actions have been uncovered so far. Current research is un-dergoing to clarify the molecular mechanisms of action of H.pylori virulence factors. A number of factors contribute to the development of severe gastroduodenal diseases. Among them, the most important ones are the virulence factors pro-duced by the pathogenic strains. Pathogenic strains contain cytotoxin (V H. pylori bacterial flagella [6], lipopolysaccharides (LPS) [7] , Lewis x,y antigen [8], IceA [9], PicB [10] and several other outer mem-brane proteins.In this review, primarily we will discuss about the recent advances in molecular basis of pathogenesis caused by ma-jor H. pylori cations of these virulence factors in human immune response will also be discussed.Address for offprints : S.K. Dhar, Special Centre for Molecular Medicine, Jawaharlal Nehru University, New Delhi, India (E-mail: skdhar2002@yahoo.co.in)208Urease: A key component for buffering stomach pHtaining seven genes is responsible for the biosynthesis of the enzyme urease [11, 12]. These genes encode for UreA (26.5 kDa) and UreB (60.3 kDa) and five other proteins re-quired for the uptake of Ni +2, the cofactor required for its activity [12, 13]. Crystal structure of urease reveal that the two subunits (α and β) first form a αβ heterodimer. Three αβheterodimer form a trimeric assembly (αβ)3 with 3 fold sym-metry. (αβ)3 units of H. pylori urease further assemble to form a unique supramolecular dodecameric assembly, ((αβ)3)4,which is organized as a double ring of 13 nm in diameter [14].Urease hydrolyses urea and generates ammonia that buff-ers the cytosol and periplasm and helps forming a neutral layer around the bacterial surface. The uptake of urea by H.pylori takes place through a proton-gated channel which is open only at lower pH [15]. This is an excellent way of main-taining intracellular and extracellular pH. At neutral pH, the tion.Stingl et al . recently proposed a model in favour of the high cytoplasmic urease activity of H. pylori [16]. This activity is essential for maintaining the cytoplasmic pH of this organ-ism at a value close to neutral under extreme low pH condi-tions. This mechanism involves the formation of ammonium ions (combining NH 3 released by urea and H + ions present in the cytoplasm) followed by the electrogenic export of ammonium ions from the cytoplasm via a yet to be discov-ered transport system (Fig. 1). The authors also propose that the extracytoplasmic urease activity creates a cloud of am-monia around the cells leading to the formation of a micro-environment of neutral pH.Urease is found both in the cytosol and surface of the bac-teria. It is synthesized and accumulated mainly in the cytosol together with a heat shock protein HspB. These proteins are released from the cytosol following bacterial autolysis and are adsorbed on the surface of the live bacteria. So far this is the only acceptable mechanism of surface expression of ure-ase since no leader sequence has been found in urease which can export it from the cytoplasm to the bacterial surface. This mechanism may ensure survival of the population at the ex-Fig. 1.Overview on H. pylori -host cell interactions. Major adhesins, BabA, SabA and corresponding host cell surface antigens are indicated. Translocation of CagA through the type IV secretion system into host cell and its fate has been marked. Perturbation of host cell signaling pathway and up regulation of actin cytoskeletal rearrangement and inflammatory response by phosphorylated CagA are shown. Type IV secretion system is shown by thick arrow. Neu-tralization of cytoplasmic acid by ammonia generated by the action of H. pylori enzyme urease on urea is indicated.209of the H. pyloriUrease defectiveH. pylori . However, urease activity may also contribute to toxicity by the production of ammonia which is toxic to thecells. Ammonia may also react with the reactive intermedi-H. pyloriin vitropresence of ammonium chloride, V acA rapidly induces forma-tion of larger vacuoles in HeLa cells compared to the vacuolesgenerated by Vurease-stimulated mononuclear phagocytes may play a cen-tral role in the development of H. pyloribacterial motility and attachment to the host cellsTo avoid prolonged exposure to acid and getting dischargedin the intestine, H. pylorinize the stomach suggesting that flagellar movement is es-sential for the bacteria to cross the mucous barrier [27].OnceH. pylori reach the stomach epithelial cells under the mucous layer, it adheres strongly to gastric cells. This bindingsurface molecules have been shown to be responsible for binding. Out of them BabA, the Leb blood group antigenbinding adhesin, an outer membrane protein of H. pyloribinds to Lewis B type antigen of human cells [28, 29]. Re-cently, Mahdavi et al Lewis x antigens expressed during chronic inflammation,might also contribute to virulence (Fig. 1). H. pylori AlpB, required for H. pylori adherence to gastric epithelialcells were identified recently. The pattern of AlpAB-depend-ent adherence of H. pylori to the gastric epithelial surface showed a clear difference to the BabA2-mediated adherence to Lewis, suggesting the involvement of a different receptor [33]. An H. pylori lectin binds to the sialic residues of laminin [34]. Additional bacterial proteins also help establishing con-tact with the host cells [35, 36]. It is unlikely that mutation in a single gene can create an adhesion defective mutant bac-teria incapable of making contacts with the host cells.Binding of the bacteria to the host cells is followed by the rearrangement of the plasma membrane below the contact area. The plasma membrane changes its shape and extends in order to increase the bacterial surface area of contact [37].H. pylori ated with the presence of a 40 kb pathogenicity island contain-ing more than thirty genes [38]. Depending on the presence or absence of this region, H. pylori strains are termed as cag +or cag –. The origin of pathogenicity island is not understood clearly so far. It is assumed that it has been acquired from another species or even genus since the GC content of this region is different from the rest of the genome [39].In Mongolian gerbil models, cag – bacteria cause mild in-flammation of the stomach whereas the cag + strains cause severe inflammation, gastric ulcers and tumors. This result strongly support the data obtained from the epidemiological studies showing that severe gastric diseases are always as-sociated with cag + strains [40]. Although the reports from East Asian and Indian populations do not show strong correlation between disease status and the presence of cag + strains [41–43]. It is possible that East Asian strains may contain some virulence factor(s) other than CagA. Though the role of CagA in pathogenicity is shown by Mongolian gerbil model, the exact molecular mechanism behind the severe inflammation and the occurrence of gastric cancer is still not clear.Genes in the pathogenicity island are involved in differ-ent pathogenic process including the induction of host cells intracellular signaling [44].128 kDa protein. CagA is always present in H. pylori strains associated with the more severe form of the disease. The exact function of CagA is not clearly understood so far. CagA pro-tein is injected from the attached H. pylori into host cells using the type IV secretion system [10]. Upon transfer into the host cells, CagA is tyrosine phosphorylated [45, 46].Introduction of cagA +210sine phosphatase has been identified as an intracellular tar-get of H. pylori CagA protein (Fig. 1). CagA formed a physi-cal complex with the SH2-containing tyrosine phosphatase SHP-2 in a phosphorylation dependent manner and stimulated the phosphatase activity leading to the dephosphorylation of some cellular proteins. Wild-type but not phosphorylatrion-resistant, CagA induced a growth factor like response in gas-tric epithelial cells. Deregulation of SHP-2 by CagA may induce abnormal proliferation and movement of gastric epi-thelial cells, promoting the acquisition of a cellular trans-formed phenotype [48].Two members of the src kinases family, c-Src and Lyn,account for most of the CagA-specific kinase activity in host cell lysates [49, 50]. Tyrosine phosphorylation of CagA is restricted to a repeated sequence called D1 located in the C-terminal half of the protein. It contains the five-amino-acid motif EPIYA, which is amplified by duplications in a large fraction of clinical isolates. Tyrosine phosphorylation at the EPIYA motifs may lead to the cytoskeletal rearrangements,cell elongation and increased cellular motility. CagA shows sequence diversity among differentH. pylori strains. The phosphorylation domain ‘EPIYA’ is located within the repeatregion of CagA. Therefore, the number and sequence poly-be found useful to elucidate the clinical outcome of infection by different cagA +H. pylori strains [48].The vacuolating cytotoxin A (VacA)In cultured cells, H. pylori vacuolating cytotoxin (VacA)forms large cytoplasmic vacuoles, which eventually fill up the entire cytosol [51]. The molecular mass of VacA is 95 kDa and it is present in half of the H. pylori isolates. It is one of the major virulence factor of H. pylori which is a strong immuno-VacA gene encodes a protoxin approximately 140 kDa in mass. An amino terminal signal sequence and a carboxy-terminal fragment are proteolytically cleaved to produce a ~ 88 kDa mature toxin [51]. Mature toxin molecules are ei-ther secreted in the extracellular space or it may be retained in bacterial surface [53]. Mature VacA may further undergo cleavage leading to the formation of N-terminal 34 kDa (p37)and C-terminal 54 kDa (p58) fragments which remain non-β-pleated sheets. This region contains a 32-residue hydrophobic segment with a propen-sity to insert into membrane [54]. p58 is predicted to contain two domains separated by a flexible segment of variable length.The first domain is highly conserved whereas the second domain is genetically diverse. VacA is purified as a large oligomeric complex (> 900 kDa), which under electron mi-croscope is appeared as ‘flower’ like structure with 30 nm in diameter [55, 56]. These structures are thought to be com-posed of one or two rings each comprised of 6–7 VacA monomer. The oligomeric complex is disassembled in monomers when exposed to acidic or basic pH. Monomeric forms show increased cytotoxocity than oligomers [57].VacA is released and placed in between the mucus layer and the apical domain of the stomach epithelial cells. Using radioactive VacA, a number of non-saturable low-affinity receptors were found on the surface of HeLa cells suggest-ing that VacA may not need specific receptors on the cell surface. Upon insertion into the plasma membrane, VacA forms anion specific channels of low conductance [58]. These channels release bicarbonate and organic anions from the cell cytosol to support bacterial growth. The toxin channels are slowly endocytosed and finally reach late endosomal com-partments. The presence of vacuolar ATPase proton pump on the membrane of the endosome increases hydrogen ion con-centration inside the lumen of the endosome. These proton pumps are essential for the formation of the vacuoles. In the presence of weak bases like ammonia generated by the H.pylori urease, osmotically active acidotropic NH4+ ions are accumulated inside the endosome. This leads to water influx and vesicle swelling leading to the vacuole formation. By an unknown mechanism, VacA alters the tight junctions and increases the permeability of iron and nickel ions through the paracellular route. These nutrients are essential for H. pylori growth. VacA may mediate this activity by specific interac-tion with recently identified cytosolic protein VIP54 [59].Apart from vacuolar ATPase, several cellular enzymes are required for vacuole development and maintenance. These include small GTP binding proteins Rab7 [60] and Rac1 [61].Rab7 may be needed to support membrane deposition and homotypic fusion between late endosomes, and Rac1 may control cytoskeletal elements affecting membrane trafficking.Purified and activated VacA applied externally to cells in-duce cytochrome c release into the cytosol. In order to find out specific role of p37 and p58 in VacA mediated cytosolic cytochrome c release, HEp-2 cells were transfected with DNAs encoding either the N-terminal (p37) or the C-termi-nal (p58) fragment of VacA. p37 was found to be localized specifically to mitochondria, whereas p58 was cytosolic.Incubated in vitro with purified mitochondria, VacA and p37but not p58 translocated into the mitochondria. p37-GFP or VacA-GFP transfected HeLa cells induced the release of cytochrome c from mitochondria and activated the caspase 3, a key enzyme for apoptosis. This was determined by the tochondria-dependent apoptotic signals. This clearly sug-gests that p37 is specifically targeted to mitochondria followed by the induction of apoptosis in cultured cells [62]. However,211it is interesting to note that externally applied toxin failed to induce a significant apoptosis.Increased levels of apoptosis have been well documented in the gastric epithelium of patients colonized by H. pylori [63]. Therefore, the increased occurrence of cell death prob-ably plays a role in the appearance of atrophic gastritis, an[63].antigens in the antigen-processing compartment of antigenpresenting cells [64]. As a result, it inhibits the stimulation of T-cell clones specific for epitopes generated in the anti-gen-processing compartment.H. pylori inhibits the local immune response as evidenced by the low frequency of VacA specific CD4+ T cells found in the stomach mucosa. Persist-ent H. pylori infection also down regulates specific CD8+cytotoxic T cell response suggesting that H. pylorimay take this strategy for prolonged survival leading to the chronic infection of the human stomach.In conclusion, although many aspects of VacA function have been elucidated so far, several important aspects are still missing. Presently two models have been postulated for VacA function. In the first model, V acA is an A/B toxin and its toxic activity requires either p37 or the entire protein which is translocated in the cytoplasm and then acts on an intracellu-lar target(s). The other model proposes that active VacA binds to targets on the cell plasmamembrane followed by forma-tion of transmembrane anion selective channels. Membrane associated VacA molecules are endocytosed and accumulate in endo-lysosomal compartments leading to the vacuole for-mation. These two models may be alternative or complemen-tary to each other.Helicobacter pylori neutrophil activating proteinInfection with H. pylori induces a state of chronic inflamma-tion which often leads to gastric or duodenal ulcers or more rarely to gastric adenocarcinoma or mucosa-associated lym-phoid tissue (MALT) lymphoma. H. pylori induced inflamma-tion is associated with the infiltration of phagocytes (mainly neutrophils) to the gastric mucosa. The tissue damage may be attributed to the combined effects of bacterial factors and host inflammatory mediators. Recently, a protein capable of promoting neutrophil infiltration and adhesion to endothe-lial cells was identified. The purified protein was termed as HP-NAP. It is a 150-kDa dodecameric (composed of 15 kDa subunits) iron-binding protein that promotes adhesion of oxidase as- (ROS) viaa cascade of intracellular activation events including an in-crease in cytosolic calcium ion concentration and phospho-rylation of proteins. HP-NAP is less powerful than PMA with respect to neutrophil activation. It has been suggested that HP-NAP induces moderate inflammation, which alters the epithelial tight junction leading to the release of nutrients from the mucosa [67].of mice with HP-NAP induced protection against H. pylori challenge. This is consistent with the finding of HP-NAP specific antibodies present in the majority of H. pylori in-fected patients [69]. Therefore, HP-NAP is a virulence fac-tor important for the H. pylori pathogenic effects at the site of infection and a candidate antigen for vaccine development.Type IV secretion systemH. pylori type I strains are characterized by the presence of cag pathogenicity island (PAI) which contains 31 open read-ing frames. Some of these ORFS share significant homology with the virulence (vir ) genes virB4, virB7, virB8, virB9,virB10, virB11, and virD4 of the so-called VirB/D complex of type IV secretion systems known from Agrobacterium tumefaciens and Bordetella pertussis [46, 70]. Generally type IV secretion systems are involved in conjugative DNA trans-fer of prokaryotes and in the delivery of bacterial virulence factors into the eukaryotic cells (Fig. 1).CagA is the only protein known so far to be injected by H.pylori into host cells (Fig. 1). This is the first evidence of a functional secretion apparatus in H. pylori . In recent studies,each gene in the cag-PAI was deleted without causing polar effect on the expression of the downstream genes. Seventeen out of 27 genes including the VirD homologue were found to be absolutely essential for translocation of CagA into host cells [71]. This clearly suggests that an intact type IV secre-tion system is required for the translocation of CagA. Attach-ment of the type I H. pylori strains to host cells induces the production and secretion of chemokines such as interleukin-8 (IL-8) [44]. The mechanism of this chemokine induction is not clearly understood. Several genes of the cag-PAI or components of the type IV secretion apparatus seem to be involved in this process by activation of AP-1 [72] and NF κB [10] leading to the induction of chemokines. Inactivation of VirD4 homologue which affected CagA translocation had no effect on IL-8 secretion. This clearly suggests that CagA translocation and IL-8 secretion may take place independent212to each other. VirD4 is thought to be an adapter protein guid-ing CagA into the transport channel. Both CagA transloca-tion and IL-8 secretion require intact type IV secretion system since inactivation of VirB4 which does not allow functional assembly of transporter affect both the activities. IL-8 secre-tion may take place either due to the transportation of an yet another unidentified molecule through the type IV secretion system or by binding of the transporter itself to relevant cell surface receptors (receptor hypothesis) followed by activa-tion of cellular signaling mechanism.Overall biological effectsWe have discussed the cellular effects of major H. pylori virulence factors in details (Fig. 1). Multiple virulence fac-tors modulate host in different ways giving rise to H. pylori pathogenicity. It is important to note that host factors also play important roles in determining the extent and severity of the damage of the host tissues. Biological effects of H. pylori on the host cells include cellular proliferation, inflammation and apoptosis.H. pylori infection is associated with enhanced cellular pro-liferation of host cells. However, the mechanism behind the proliferation is not clearly understood. Expression of vari-ous cell cycle markers associated with the proliferation was checked in the host cells following co-culture of gastric epi-thelial cells with bacteria. In a recent report, Cyclin D1 tran-scription in gastric cancer (AGS) cells was enhanced by co-culture with H. pylori [73]. This activation of cyclin D1was partly dependent on the cag pathogenicity island but not on vacA . Among various cyclins, cyclin D1 regulates passage through the restriction point and entry into the S phase. Fur-thermore, cyclin D1 overexpression shortens the G 1 phase and increases the rate of cellular proliferation. Co-culture of H.pylori with epithelial cells was reported to reduce expression of the cell-cycle regulatory protein p27, which leads to epi-thelial-cell G 1 arrest [74]. Cell proliferation may also be in-duced by H. pylori as a result of host response to bacteria.Production of gastrin by mucosal G cells increases in the presence of H. pylori . In vitro , gastrin enhances the prolifera-tion of gastric epithelial cells. Transgenic mice overexpressing gastrin yielded gastric adenocarcinoma more frequently and in less time in the presence of H. pylori than in the absence of bacteria suggesting that high gastrin level andH. pyloricolonization may cooperatively enhance the incidence of gastric cancer [75].H. pylori also causes inflammation. Pro-inflammatoryits expression in the gastric epithelial cells is increased when co-cultured with H. pylori [76]. Phospholipase A 2, a keyenzyme catalysing the formation of the prostaglandin precur-H. pylori and in vivo [77, 78]. In the presence of H. pylori , activated neutrophils may also induce inflam-age.H. pylori level of apoptosis depending on the host. In vitro , H. pylori by itself and purified urease and VacA induces apoptosis in gastric epithelial cells. T H 1 cytokines induced by H. pylori ,such as IFN-γ, might induce epithelial-cell apoptosis through a Fas-mediated pathway. Expression of Fas receptors on the surface of epithelial cells increase in the presence of H. py-lori. In vitro , H. pylori may also induce apoptosis by activat-ing NF-κB [79]. There should be a delicate balance between apoptosis and cell proliferation. Increased rates of apoptosis could result in formation of atrophic gastritis, with a concomi-tant increased risk of distal gastric adenocarcinoma. Whereas,reduced rates of apoptosis, accompanied by hyperproliferation,could lead to the development of gastric cancer.Host factors and onset of gastric cancerWe have discussed the effects of H. pylori virulence factors.Several host factors are also associated with the onset of gastric cancer. Th1 type of immune response is induced in humans by H. pylori whereas Helicobacter felis can induce same type of immune response in mice [80]. Gastric atrophy initiated by H. felis can be reduced by Th2 immune response [81].H. pylori infected individuals show differential level of IL-1β secretion within the gastric mucosa [82]. IL-1β gene pro-moter contains several polymorphic regions affecting protein expression. The chances of getting gastric atrophy and gas-tric adenocarcinoma are higher in H. pylori infected indi-viduals with higher IL-1β secretion than average [83]. In Mongolian gerbil models, gastric acid production is reduced with increasing IL-1β secretion after 6–12 weeks following infection. IL-1β, the proinflammatory cytokine could play a major role in the formation of gastric adenocarcinoma [84].Polymorphism of the TNF-α promoter is associated with increased risk of gastric cancer [85]. TNF-α expression is in-creased in H. pylori infected mucosa as a result of Th1 im-mune response. It has been reported recently that mutation in RAS together with increased level of TNF-α may cause carcinogenesis in genetically susceptible hosts [86].Some major histocompatibility complex (MHC) genotype may also play some role in H. pylori induced gastric cancer.Class II MHC molecules expressed on gastric epithelial cells are upregulated in the presence of H. pylori suggesting that213Host cells and H. pylori constantly exchange signals with each other leading to a formation of dynamic equilibrium. In most cases the equilibrium is unchanged whereas in some cases the equilibrium is shifted causing disease depending on the host and bacterial characteristics. This might explain why some people get disease and majority don’t get affected by H. pylori. Individuals infected with Cag+H. pylori strain and with high level of IL-1βand TNF-α expression due to genetic polymorphism in host are at more risk than individuals in-fected with either Cag– strain or low expression of IL-1βand TNF-α in the host.Therefore, the onset of gastric cancer may be the net re-sult of bacterial strain variation, host genotype and environ-mental factors.Development of vaccinesTo date, H. pylori is one of the most common infections of mankind. Infection usually occurs during childhood, and when left untreated results in lifelong colonization of the stomach. Antimicrobial therapy is currently the method of choice for the treatment. However, complex dosing, inconsistent efficiency, development of antibiotic resistance, costs and side effectsH. pylorisince it will be both effective and economic in use. Natural in-fection with H. pylori usually results in a strong inflammatory Th1-type CD4(+)T-cell response that does not seem to have any protective effects. A Th2-type response is required for pro-tection. Unfortunately, the exact mechanisms involved in pro-tective immunization are still poorly understood.H. pylori virulence factors like Urease, CagA, VacA, HP-NAP are major antigens in the human immune response to H. pylori infection [52]. Introduction of these antigens in animal models, result in induction of immune response which may either protect the animals from infection (prophylactic vaccines) or eradicate an already existing infection (therapeu-tic vaccine). Both oral and systemic immunization should be considered in this regard. Although commercial development of vaccines for clinical trial is underway, many important is-sues, such as lack of a suitable mucosal adjuvant, and pre-vention of potential side effects, such as postimmunization gastritis, need to be resolved. If a suitable vaccine against H. pylori is found, elimination of a common pathogen which has been living in human for such a long time will be made pos-sible.AcknowledgementSKD acknowledges the University Grant Commission, India for support.References1.Parsonnet J: The incidence of H. pylori infection. Ailment PharmacolTher 9:(suppl 2) 45–51, 19952.Peek RM, Blaser MJ: Helicobacter pylori and gastrointestinal tractadenocarcinomas. Nature Rev Cancer 2: 28–37, 20023.Correa P: Helicobacter pylori and gastric cancer: State of the art. Can-cer Epidemiol Biomarkers Prev 5: 477–481, 19964.Go MF: What are the host factors that place an individual at risk forHelicobacter pylori-associated diseases? Gastroenterology 113: S15–S20, 19975.Montecucco C, Papini E, de Bernard M, Zoratti M: Molecular andcellular activities of Helicobacter pylori pathogenic factors.FEBS Lett 452: 16–21 19996.Suerbaum S: The complex flagella of gastric Helicobacter species.Trends Microbiol 3: 168–170, 19957.Moran AP, Linder E, Walsh EJ: Structural characterization of the li-pid A component of Helicobacter pylori rough- and smooth-form lipopolysaccharides. J Bacteriol 179: 6453–6463, 19978.Appelmelk BJ, Negrini R, Moran AP, Kuipers EJ: Molecular mimicrybetween Helicobacter pylori and the host. Trends Microbiol 5: 70–73, 19979.Peek RM Jr, Thompson SA, Donahue JP, Tham KT, Atherton JC, BlaserMJ, Miller GG: Adherence to gastric epithelial cells induces expres-sion of a Helicobacter pylori gene, iceA, that is associated with clini-cal outcome. Proc Assoc Am Physicians 110: 531–544, 199810.Censini S, Lange C, Xiang Z, Crabtree JE, Ghiara P, Borodovsky M,Rappuoli R, Covacci A: Cag, a pathogenicity island of Helicobacter pylori, encodes type I-specific and disease-associated virulence fac-tors. Proc Natl Acad Sci USA 93: 14648–14653, 199611.Hu LT, Mobley HLT: Purification and N-terminal analysis of ureasefrom Helicobacter pylori. Infect Immun 58: 992–998, 1990bigne A, Cussac V, Courcoux P: Shuttle cloning and nucleotide se-quences of Helicobacter pylori genes responsible for urease activity.J Bacteriol 173: 1920–1931, 199113. Achtman M, Suerbaum S (eds): In: Helicobacter pylori: Molecular andCellular Biology. Horizon Scientific, Norfolk, 200114.Ha NC, Oh ST, Sung JY, Cha KA, Lee MH, Oh BH: Supramolecularassembly and acid resistance of Helicobacter pylori urease. Nat Struct Biol 8: 505–509, 200115.Weeks DL, Eskandari S, Scott DR, Sachs G: A H+-gated urea channel:The link between Helicobacter pylori urease and gastric colonization.Science 287: 482–485, 200016.Stingl K, Altendorf K, Bakker EP: Acid survival of Helicobacter py-lori: How does urease activity trigger cytoplasmic pH homeostasis?Trends Microbiol 10: 70–74, 200217.Phadnis SH, Parlow MH, Levy M, Ilver D, Caulkins CM, Connors JB,Dunn BE: Surface localization of Helicobacter pylori urease and a heat shock protein homolog requires bacterial autolysis. Infect Immun 64: 905–912, 199618.Dunn BE, Vakil NB, Schneider BG, Miller MM, Zitzer JB, Peutz T,Phadnis SH: Localization of Helicobacter pylori urease and heat shock protein in human gastric biopsies. Infect Immun 65: 1181–1188, 1997 19.Eaton KA, Brooks CL, Morgan DR, Krakowka S: Essential role of ure-ase in pathogenesis of gastritis induced b y Helicobacter pylo ri in gnoto-biotic piglets. Infect Immun 59: 2470–2475, 199120.Megraud F, Neman-Simha V, Brugmann D: Further evidence of thetoxic effect of ammonia produced by Helicobacter pylori urease on human epithelial cells. Infect Immun 60: 1858–1863, 199221.Suzuki M, Miura S, Suematsu M, Fukumura D, Kurose I, Suzuki H,Kai A, Kudoh Y, Ohashi M, Tsuchiya M: Helicobacter pylori-associ-ated ammonia production enhances neutrophil-dependent gastric mu-cosal cell injury. Am J Physiol 263: G719–G725, 1992。