VASP文献
- 格式:pdf
- 大小:179.26 KB
- 文档页数:5

VASP控制参数文件INCAR的简单介绍作者:elizerbeth文章来源:zilu@日月光华INCAR是决定how to do 的文件限于能力,只对部分最基本的一些参数(>,没有这个标志的参数都是可以不出现的) 详细说明,在这里只是简单介绍这些参数的设置,详细的问题在后文具体示例中展开。
部分可能会干扰VASP运行的参数在这里被刻意隐去了,需要的同学还是请查看VASP自带的帮助文档原文。
参数列表如下:>SYSTEM name of System 任务的名字 *** >NWRITE verbosity write-flag (how much is written) 输出内容详细程度 0-3 缺省2 如果是做长时间动力学计算的话最好选0或1(首末步/每步核运动输出) 据说也可以结合shell的tail或grep命令手动输出>ISTART startjob: restart选项 0-3 缺省0/1 for 无/有前次计算的WAVECAR(波函数) 1 'res tart with constant energy cut-off' 2 'restart with constant basis set' 3 'full restart inclu ding wave function and charge prediction' ICHARG charge: 1-file 2-atom 10-const De fault:if ISTART=0 2 else 0 ISPIN spin polarized calculation (2-yes 1-no) default 2 MAG MOM initial mag moment / atom Default NIONS*1 INIWAV initial electrwf. : 0-lowe 1 -rand Default 1 only used for start jobs (ISTART=0) IDIPOL calculate monopole/dipole and quadrupole corrections 1-3 只计算第一/二/三晶矢方向适于slab的计算 4 全部计算尤其适于就算孤立分子>PREC precession: medium, high or low(VASP.4.5+ also: normal, accurate) Default: M edium VASP4.5+采用了优化的accurate来替代high,所以一般不推荐使用 high。

侯柱峰-vasp计算晶体弹性常数引言晶体弹性常数是描述晶体材料力学性质的重要参数之一,对于理解材料的力学行为和设计新材料具有重要意义。
在材料科学领域中,计算晶体弹性常数的方法多种多样,其中基于第一性原理的计算方法得到了广泛的应用和认可。
本文将介绍侯柱峰等人在VASP软件包中计算晶体弹性常数的方法和步骤。
VASP简介VASP(Vienna Ab-initio Simulation Package)是一款基于密度泛函理论(DFT)的第一性原理计算软件包,由维也纳大学的J. Hafner教授及其团队开发。
VASP以固体物理和材料科学为核心,广泛应用于研究材料的电子结构、力学性质、热力学性质等方面。
VASP计算晶体弹性常数的方法1. 结构优化在计算晶体弹性常数之前,首先需要通过VASP进行结构优化。
结构优化的目的是找到晶体的平衡结构,使得能量最低。
在结构优化过程中,需要设定材料的晶格参数、原子种类和初始位置等参数,并设置计算的精度和收敛标准。
2. 弹性常数计算前的准备在进行弹性常数计算之前,需要对结构进行静力学计算,即计算晶体的内部应力状态。
为此,需要在INCAR文件中设置一些相关的参数,例如选用的泛函类型、截断能等。
3. 弹性常数计算在进行弹性常数计算之前,需要在INCAR文件中添加以下参数:ISTART = 1ICHARG = 2ENCUT = 520ISYM = 0ISMEAR = 0然后运行VASP进行弹性常数的计算。
计算完成后,可以得到弹性常数矩阵,其中包括36个元素,分别对应不同的弹性常数。
4. 弹性常数的后处理在得到弹性常数矩阵之后,需要进行一些后处理来得到弹性常数的具体数值。
这一步可以使用第三方软件进行,例如使用MATLAB来计算并提取需要的弹性常数。
结论侯柱峰等人在VASP软件包中提供了一种计算晶体弹性常数的方法,可以方便而准确地得到晶体的力学性质。
这种方法基于第一性原理,充分考虑了材料的电子结构和原子之间的相互作用,具有很高的可靠性和适用性。

个人非常好的VASP学习与总结VASP(Vienna Ab initio Simulation Package)是一种用于计算材料电子结构和材料性质的第一性原理软件包。
它是由奥地利维也纳大学的Peter Blöchl教授和Jürgen Hafner教授等人开发的。
VASP广泛应用于材料科学、凝聚态物理、表面科学、催化化学等领域,并且已成为当前计算材料科学研究中的重要工具。
我的VASP学习与总结主要包括以下几个方面:一、理论基础在学习VASP之前,我首先了解了从头计算的理论基础。
这包括了量子力学、自旋极化的密度泛函理论、平面波基组和赝势等关键概念。
我通过阅读相关文献和教材,深入理解了这些理论基础,并通过编程实现了一些基本的从头计算算法,如Hartree-Fock法和密度泛函理论。
二、VASP软件架构和输入文件学习VASP的过程中,我详细了解了VASP的软件架构和输入文件的格式。
VASP的软件架构分为主程序和一系列的预处理工具、后处理工具和与其他软件的接口。
对于输入文件,我了解了INCAR文件中的各种参数,如体系的描述、计算方法、收敛准则等;POSCAR文件中的晶体结构描述;KPOINTS文件中的k点网格描述等。
我还学习了如何使用VASP进行周期性边界条件下的能带计算、电子密度计算和弛豫力计算等。
三、VASP计算结果的解析和可视化VASP计算得到的结果需要进一步解析和可视化。
我学习了使用一些常用的后处理工具,如VASP可视化工具、VESTA和XCrysDen等,来分析和可视化VASP计算的结果。
这些工具可以帮助我理解晶体结构、电子能带结构以及电荷分布等。
四、VASP参数优化和计算效率为了得到准确的计算结果,我尝试了调整VASP计算中的一些参数,如波函数截断、k点密度、能量收敛准则等,以获得更准确的计算结果。
此外,我还学习了使用并行计算技术来提高VASP计算的效率,如MPI和OpenMP等,并了解了VASP在高性能计算集群上的使用方法。

Y-Fe系列化合物磁性的理论研究周薇;牟宏晶;杨路清;张辉;张桂玲【期刊名称】《四川师范大学学报(自然科学版)》【年(卷),期】2008(031)003【摘要】从第一性原理出发,使用VASP程序(Vienna ab initio simulation package)计算了Y-Fe系列化合物的磁性和态密度.结果表明所讨论的Y-Fe系列化合物都是亚铁磁性的;Y原子的负磁矩是由Y原子和Fe原子的d带电子之间的强共价相互作用引起的;除YFe5外,Y-Fe系列化合物中Fe的平均原子磁矩随着Fe含量的增加而增大.【总页数】5页(P332-336)【作者】周薇;牟宏晶;杨路清;张辉;张桂玲【作者单位】哈尔滨师范大学,化学系,黑龙江,哈尔滨,150080;哈尔滨理工大学,化学与环境工程学院,黑龙江,哈尔滨,150080;哈尔滨理工大学,化学与环境工程学院,黑龙江,哈尔滨,150080;哈尔滨理工大学,化学与环境工程学院,黑龙江,哈尔滨,150080;哈尔滨师范大学,化学系,黑龙江,哈尔滨,150080;哈尔滨理工大学,化学与环境工程学院,黑龙江,哈尔滨,150080【正文语种】中文【中图分类】O48【相关文献】1.晶场劈裂序参量导致稀土–硼十二化合物中磁性和比热反常的理论研究 [J], 胡靖三;顾建飞;章维益2.在"Ni(M)_4X_2型化合物光、热、磁性质"理论研究中的计算方法 [J], 周小清;邬云文;颜占先3.双亚点阵系统磁性理论研究与稀土过渡金属化合物磁性的有关进展 [J], 张志东;赵彤4.Ni(mpz)_4X_2(X=C1、Br、Ⅰ)型化合物中Ni^(2+)离子的光磁性质的理论研究[J], 周小清;颜占先;代薇;李翠莲5.GdMn_2Ge_2化合物的磁性和磁相变的分子场理论研究 [J], 郭光华;张海贝;张剑因版权原因,仅展示原文概要,查看原文内容请购买。

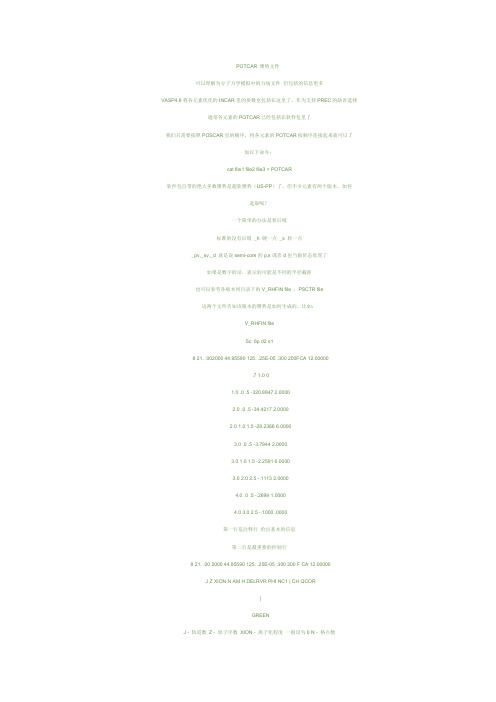
POTCAR 赝势文件可以理解为分子力学模拟中的力场文件但包括的信息更多VASP4.6将各元素优化的INCAR里的参数也包括在这里了,作为支持PREC的缺省选择通常各元素的POTCAR已经包括在软件包里了我们只需要按照POSCAR里的顺序,将各元素的POTCAR按顺序连接起来就可以了如以下命令:cat file1 file2 file3 > POTCAR软件包自带的绝大多数赝势是超软赝势(US-PP)了,但不少元素有两个版本,如何选取呢?一个简单的办法是看后缀标准的没有后缀_h 硬一点_s 软一点_pv,_s v,_d 就是说s emi-core的p,s或者d也当做价态处理了如果是数字的话,表示的可能是不同的半径截距也可以参考各版本同目录下的V_RHFIN file ,PSCTR file这两个文件告知该版本的赝势是如何生成的。
比如:V_RHFIN fileSc: 6p d2 s18 21. .002000 44.95590 125. .25E-05 .300 200FCA 12.00000.7 1.0 01.0 .0 .5 -320.88472.00002.0 .0 .5 -34.4217 2.00002.0 1.0 1.5 -28.2366 6.00003.0 .0 .5 -3.7944 2.00003.0 1.0 1.5 -2.2591 6.00003.0 2.0 2.5 -.1113 2.00004.0 .0 .5 -.2699 1.00004.0 3.0 2.5 -.1000 .0000第一行是注释行给出基本的信息第二行是最重要的控制行8 21. .00 2000 44.95590 125. .25E-05 .300 200 F CA 12.00000J Z XION N AM H DELR VR PHI NC1 | CH QCOR|GREENJ - 轨道数Z - 原子序数XION - 离子化程度一般设为0 N - 格点数AM - 原子质量H - 决定格点间距DELRVR - 自洽收敛标准PHI - 线性拟合参数NC1 - 最大自洽循环次数GREEN - 是否存在初始的势CH - 交换相关能(XC)类型Slater-XCHL Hedin Lundquist (1971)CA Ceperly and Alder parameterized by J.Perdew and Z ungerWI Wigner interpolationPB Perdew -Bec kePW Perdew -Wang 86LM Langreth-Mehl-Hu91 Perdew -Wang 91QCOR - 非价键电子数(core electrons)第三行开始是每个轨道的具体参数,依次为n l j(=l±1/2) 原子轨道能占有率PSCTR file of LDA/H1.25TITEL = US HLULTRA = T use ultras oft PP ?RWIGS = 0.57 nn distance ! Wigner-Seitz radiusRCLOC = .65NE = 100LCOR = .TRUE.QCUT = -1RMAX = 3.0 ! core radius for proj-operDescriptionl E TYP RCUT TYP RCUT(cutoff radi us)0 0 15 0.80 23 1.250 0.5 15 0.80 23 1.251 -0.2 15 0.80 23 1.25最重要的地方上面已经用颜色标出来啦:)说明一下,TYP是指赝势的类型,RCUT是半径截距,TYP可取的值如下:正则1 BH S2 TM3 VAN6 XNC7 RRKJ wave func tion possi bly with node15 RRKJ wav e function strictl y no node非正则+8最后一个问题是LDA or GGA。
VASP使用总结VASP(Vienna Ab initio Simulation Package)是一款基于密度泛函理论(DFT)的第一性原理计算软件,主要用于材料科学和凝聚态物理领域的计算。
它提供了丰富的功能和工具,可以用于模拟和研究各种材料的物理和化学性质。
以下是对VASP使用的总结:1.输入文件的准备在进行VASP计算之前,首先需要准备好输入文件。
VASP使用的输入文件包括POSCAR、INCAR、POTCAR等。
POSCAR文件用于定义晶体结构和原子坐标,INCAR文件用于定义计算参数和设置计算方法,POTCAR文件用于定义原子的赝势。
2.材料结构的优化VASP可以通过结构优化计算来确定材料的最稳定结构。
结构优化计算通过改变原子位置和晶胞大小,寻找最低能量的结构。
可以使用ISIF 参数来设置优化类型,如禁止移动原子、禁止改变晶胞大小等。
3.能带结构的计算VASP可以计算材料的能带结构,从而提供关于能带轨道和能带间隙的信息。
能带结构计算需要先进行结构优化计算,然后再进行自洽计算和能带计算。
可以通过设置KPOINTS和NBANDS参数来控制计算的精度和效率。
4.密度状态的计算VASP可以计算材料的密度状态,包括电荷密度、电荷分布和电子态密度等。
通过密度状态计算,可以了解材料的电子结构和性质。
可以通过设置LSORBIT、IALGO和NPAR等参数来控制计算的模式和效率。
5.势能面的计算VASP可以计算材料的势能面,并通过构建势能面图像来显示材料的稳定性和反应性。
势能面计算需要进行结构优化计算,然后通过改变原子位置和晶胞大小来势能面上的最低能量和结构。
6.热力学性质的计算VASP可以通过计算自由能、热容和热膨胀系数等热力学性质来了解材料的热稳定性和热响应。
热力学性质的计算需要进行结构优化计算和自洽计算,然后使用VASP提供的工具和脚本进行热力学性质的分析和计算。
7.计算结果的解析和可视化VASP提供了丰富的工具和脚本,可以用于解析和可视化计算结果。
MedeA-VASP优势1.VASP使用PAW方法或超软赝势,因此基组尺寸非常小,描述体材料一般需要每原子不超过100个平面波,大多数情况下甚至每原子50个平面波就能得到可靠结果。
2.磁性材料最精确的计算软件。
3.在平面波程序中,某些部分代码的执行是三次标度。
在VASP中,三次标度部分的前因子足可忽略,导致关于体系尺寸的高效标度。
因此可以在实空间求解势的非局域贡献,并使正交化的次数最少。
当体系具有大约2000个电子能带时,三次标度部分与其它部分可比,因此VASP可用于直到4000个价电子的体系。
4.VASP使用传统的自洽场循环计算电子基态。
这一方案与数值方法组合会实现有效、稳定、快速的Kohn-Sham方程自洽求解方案。
程序使用的迭代矩阵对角化方案(RMM-DISS和分块Davidson)可能是目前最快的方案。
5.VASP包含全功能的对称性代码,可以自动确定任意构型的对称性。
6.对称性代码还用于设定Monkhorst-Pack特殊点,可以有效计算体材料和对称的团簇。
Brillouin区的积分使用模糊方法或四面体方法。
四面体方法可以用Blöchl校正去掉线性四面体方法的二次误差,实现更快的k点收敛速度。
MedeA 2.5版本软件将材料设计领域的应用最广的工具VASP的最新版本5.2作为计算引擎,提供了更加丰富的计算功能和更高的稳定性能:.光学性质,特别是与介电函数相关的频率虚部和实部计算。
.增加外场和粒子位置相关的线性响应机制。
.大部分二阶响应函数,如内部应力张量、压电张量、Born有效电荷和原子间应力常数。
.准确的交换混合函数(PBE0)不仅支持Γ点而且支持整个k点。
因为目前的程序是基于波函数的对称性来执行的,所以k点是指IRZ(不可约布里渊区)。
计算量将随着增加很快,增加大约两个数量级。
.屏蔽交换能,COHSEX中的GW将得到支持。
.支持优化的有效势方法中的交换能确定。
.提高全频率GW方法计算的效率,如等离子体柱模型:并行效率非常高、Si 128能带、6×6×6 k点计算用双核Opteron机器需要500-1000秒。
Effects of pantoprazole and esomeprazole on platelet inhibition by clopidogrelJolanta M.Siller-Matula,MD,a Alexander O.Spiel,MD,a Irene ng,MD,b Gerhard Kreiner,MD,bGuenter Christ,MD,b and Bernd Jilma,MD a Vienna,AustriaBackground Clopidogrel is activated by CYP2C19,which also metabolizes proton pump inhibitors(PPI).As proton pump inhibitors are metabolized to varying degrees by CYP2C19,we hypothesized that the reported negative omeprazole-clopidogrel drug interaction may not be a class effect.Methods Responsiveness to clopidogrel was assessed by the vasodilator-stimulated phosphoprotein phosphorylation (VASP)assay and aggregometry(Multiplate Analyzer)in300patients with coronary artery disease(CAD)undergoing percutaneous coronary intervention(PCI).Results The mean platelet reactivity index(PRI,assessed by the VASP assay)was nearly the same in patients with(n=226; PRI=51%)or without PPI treatment(n=74;PRI=49%;P=.724).Likewise,the adenosine diphosphate–induced platelet aggregation did not differ significantly between patients with or without PPI treatment(45vs.41U;P=.619).Similarly,there was no difference in the PRI or the adenosine diphosphate–induced platelet aggregation between patients with pantoprazole(n= 152;PRI=50%;aggregation=47U),esomeprazole(n=74;PRI=54%;aggregation=42U),or without PPI(n=74;PRI=49%; aggregation=41U;P=.382).Conclusion In contrast to the reported negative omeprazole-clopidogrel drug interaction,the intake of pantoprazole or esomeprazole is not associated with impaired response to clopidogrel.(Am Heart J2009;157:148.e1-148.e5.)The antiplatelet effect of clopidogrel is not uniform in all patients and reduced platelet inhibition by clopidogrel is associated with an increased risk of cardiac events.1-4 The variability in the response to clopidogrel has been linked,at least in part,to its cytochrome P450–dependent metabolism steps including CYP2C19and CYP3A4.5-8 Proton pump inhibitors(PPIs),frequently used in patients receiving clopidogrel and aspirin,are also metabolized by CYP2C19and CYP3A4.9It has recently been reported that the PPI omeprazole decreases the antiplatelet effect of clopidogrel possibly due to the inhibition of the CYP2C19enzyme.10,11As all PPIs are metabolized by CYP2C19,12but to a varying degree,we hypothesized that the reported negative omeprazole-clopidogrel drug interaction may not be a class effect.Thus,we compared the responsiveness to clopidogrel with or without concomitant PPI treatment in300patients with coronary artery disease(CAD)undergoing percutaneous coronary intervention(PCI).To quantify the pharmacodynamic effect of clopidogrel with or without PPIs treatment,we performed the vasodilator-stimulated phosphoprotein (V ASP)phosphorylation assay and impedance aggrego-metry.13-15The V ASP assay is specific for clopidogrel and other P2Y12antagonists in the absence of cilostazol.13-18 It has been shown that adjusting the clopidogrel loading dose according to the platelet reactivity index in the V ASP assay may improve the clinical outcome in patients with decreased platelet inhibition by clopidogrel.19,20 MethodsStudy designThe study protocol was approved by the Ethics Committee of the Medical University of Vienna in accordance with the Declaration of Helsinki.Written informed consent was obtained from all study participants before the study entry.Three hundred consecutive patients with coronary artery disease (CAD)undergoing percutaneous coronary intervention(PCI) were enrolled.All patients received a clopidogrel loading dose (600mg)at the start of clopidogrel treatment.Patients had been on clopidogrel(75mg/d)and aspirin(100mg/d)treatment for 3months on average(5days at least)at the time of inclusion. Two different PPIs have been used in the study:pantoprazole and esomeprazole.Blood samples from patients were obtained from the arterial sheath(6F)in the catheterization laboratory immediately after PCI.Part of patients has been analyzed in our previous study.21From the a Department of Clinical Pharmacology,Medical University of Vienna,Vienna, Austria,and b Department of Cardiology,Medical University of Vienna,Vienna,Austria. This study was supported by a grant from the Jubiläumsfond of the Austrian National Bank (Nr.12565).Submitted August24,2008;accepted September25,2008.Reprint requests:Bernd Jilma,MD,Department of Clinical Pharmacology,Medical University of Vienna,Währinger Gürtel18-20,A-1090Vienna,Austria.E-mail:bernd.jilma@meduniwien.ac.at0002-8703/$-see front matter©2009,Mosby,Inc.All rights reserved.doi:10.1016/j.ahj.2008.09.017Analysis of VASP phosphorylation by flow cytometry To determine the V ASP(vasodilator stimulated phospho-protein)phosphorylation state of whole blood,we used a standardized flow cytometric assay(Platelet V ASP;BioCytex, Marseille,France).Blood samples collected in3.8%sodium citrate(BD Vacutainer;Becton Dickinson,Vienna,Austria) were incubated in vitro with adenosine diphosphate and/or prostaglandin E1(PGE1)before fixation.After10minutes, platelets were permeabilized,labeled with a primary mono-clonal antibody against serine239-phosphorylated V ASP(clone 16C2)or its isotype,followed by a secondary fluorescein isothiocyanate–conjugated polyclonal goat-antimouse antibody. All procedures were performed at room temperature.Geo-metric mean fluorescence intensity(GMFI)was determined using a flow cytometer(FACSCalibur System,BD Biosciences, Vienna,Austria).22The platelet population was identified by its forward and side scatter distribution,and10,000platelet events were gated and analyzed for GMFI.Platelet reactivity was expressed as platelet reactivity index(PRI)calculated as PRI%=[(GMFI(PGE1)−GMFI(PGE1+ADP)/GMFI(PGE1)]×100.The ratio is expressed as mean percentage platelet reactivity,which inversely correlates with the clopidogrel effect.The normal value of the PRI measurement using V ASP analysis is69%to100%.21,23The V ASP assay was performed within24hours after blood sampling.AggregometryADP-induced platelet aggregometry is a widely used method to measure the responsiveness to clopidogrel.24,25 Whole blood aggregation was determined using an impe-dance aggregometer(Multiple Platelet Function Analyzer, Dynabyte Medical,Munich,Germany).The system detects the electrical impedance change due to the adhesion and aggregation of platelets on two independent electrode-set surfaces in the test cuvette.26,27A2:1solution of whole blood anticoagulated with hirudin(200U/mL,Dynabyte Medical)and0.9%NaCl was stirred at37°C for3minutes in the test cuvettes,adenosine diphosphate([ADP]6.4μmol/L, Dynabyte Medical)was added,and the increase in electrical impedance was recorded continuously for6minutes.The mean values of the2independent determinations are expressed as the area under the curve of the aggregation tracing.The results measured by the Multiplate Analyzer are reproducible with less than6%variability.26The reference range for the test is29to118U.28Statistical analysisA sample size calculation of our study was based on the observed mean±SD(62±23)of the platelet reactivity index under clopidogrel and omeprazole treatment and the observed mean(50±16)of the platelet reactivity index under clopidogrel alone.11We calculated that we need to include72patients in each group to be able to detect such a 20%relative difference in platelet reactivity index with a power of95%and a2-sidedαvalue of.05.Stepwise multivariable logistic regression analysis was used to estimate possible associations between platelet reactivity index, platelet aggregation,and use of PPI.The logistic model included sex,use of statins(lipophilic versus hydrophilic), angiotensin-converting enzyme(ACE)inhibitors,calcium-channel blockers,diabetes mellitus,arterial hypertension, hypercholesterolemia,previous myocardial infarction,cause for hospitalization,and smoking.Data are reported as mean and95%confidence intervals.Statistical comparisons were performed with the Kruskal-Wallis analysis of variance,theχ2 test,and the Mann-Whitney U test.A2-tailed P value of b.05 was considered significant for the primary end point parameter(platelet reactivity index)between the PPI groups and patients without PPI.All statistical calculations were performed using commercially available statistical software (SPSS Version14.0;SPSS,Chicago,IL).ResultsPatient demographicsPatient demographics are shown in Table I.Most patients had high blood pressure and hyperlipidemia. Almost half of the patients had previous e of β-blockers and statins was high.There were fewer male patients in the pantoprazole(71%)or esomeprazole (80%)groups as compared to patients without any PPI (93%;P=.001;P=.046,respectively).The use of statins was higher in the pantoprazole(82%)or esomeprazole(87%)groups as compared to patients without any PPI(61%;P=.006;P=.001,respectively). The use of ACE inhibitors was higher in the esome-prazole(68%)group as compared to patients without any PPI(47%;P=.018).There were more patients hospitalized for myocardial infarction in the esomepra-zole group(39%)as compared to patients without PPI (20%;P=.002)and fewer patients with stable angina in the esomeprazole group(46%)compared to patients without PPI(66%;P=.008).Comparison of patients with any PPI vs.without PPI The platelet reactivity index(PRI,V ASP assay)was similar in patients with any PPI(n=226,mean51%; 95%CI48-54%)or without any PPI treatment(n=74; mean49%;95%CI43-55%;P=.724).As a consequence, the rate of decreased platelet inhibition by clopidogrel defined by a platelet reactivity index≥69%21was similar in both groups(25%vs20%).Likewise,the ADP-induced platelet aggregation did not differ significantly between patients with any PPI(mean45U;95%CI41-50U)or without any PPI treatment(mean=41U, 95%CI33-48U;P=.619).Comparison of patients with pantoprazole or esomeprazole vs without PPIThere was no difference in the platelet reactivity index or the ADP-induced platelet aggregation between patients with pantoprazole(n=152;PRI=50%;aggregation=47 U),esomeprazole(n=74;PRI=54%;aggregation=42U) or without PPI(n=74;PRI=49%;aggregation=41U; P=.382;Figures1and2).To exclude that minor differences in demographic data may have influenced the platelet reactivity index or the148.e2Siller-Matula et al American Heart JournalJanuary2009ADP-induced platelet aggregation,we performed a multivariable logistic regression analysis.Neither platelet reactivity index nor ADP-induced platelet aggregation were influenced by male sex,intake of statins,ACE inhibitors,or calcium-channel blockers.DiscussionThe intake of pantoprazole or esomeprazole was not associated with a reduced platelet inhibition by clopido-grel as compared to patients without PPI(Figures1and 2).The platelet reactivity index was49%in patients without PPI and,thus,similar to that in a previous study investigating the omeprazole-clopidogrel drug interaction (PRI=50%).11This demonstrates the external validity of the V ASP assay.Previous articles alerted the scientific community that concomitant treatment with omeprazole and clopidogrel may have negative effects.10,11The treating cardiologists, however,were left with the tantalizing question whether they should avoid omeprazole or any other PPI in patients receiving clopidogrel.Our data show that the reported negative effect of omeprazole on platelet function in patients receiving clopidogrel10,11is not seen in patientsTable I.Patient demographicsPatient demographics No PPI(n=74)Pantoprazole(n=152)Esomeprazole(n=74)Age73±1265±1262±13 Gender(male)(n[%])66(93)109(71)†59(80)⁎Cause forhospitalisation(n[%])Silent ischemia7(9)13(9)7(9) Stable angina49(66)87(57)33(45)†Unstable angina3(4)14(9)5(7) Myocardialinfarction15(20)38(25)29(39)†Risk factors/pastmedical history(n[%])Hypertension63(85)132(87)63(85) Smoking37(50)88(58)47(63) Family historyof CAD25(34)44(29)22(30)Diabetes mellitus23(31)53(35)23(31) Hyperlipidemia56(76)119(78)55(75) Prior myocardialinfarction23(31)52(34)24(32) Prior PCI36(49)80(53)38(51) PAOD8(11)20(13)8(11) CVD9(12)14(9)8(11) Laboratory dataWBC(G/L)8±2.57.9±2.87.8±2.9 Platelets(G/L)228±70226±68219±64 CRP(mg/dL) 1.2±2.7 1.3±2.9 1.8±2.6 Hb(g/dL)14±1.412.8±214.5±2.1 Fibrinogen(mg/dL)408±130421±120441±107 Creatinine(mg/dL) 1.3±1.2 1.3±1.2 1.7±1.3 Pre-PCI medications(n[%])ACE inhibitors35(47)73(48)51(68)⁎Calcium-channelblockers13(18)31(20)19(13)Statins45(61)124(82)†65(87)†β-Blockers51(69)122(80)59(80) ASA74(100)152(100)74(100) Clopidogrel74(100)152(100)74(100) PCI dataNumber of stentsper patient1.5±0.7 1.8±0.9 1.8±1.2 Total stent length29±1533±2133±25Data are reported as mean,SD,number of patients(n),or percentages.CVD,Cerebral vascular disease;CRP,C-reactive protein;Hb,hemoglobin;PAOD, peripheral arterial occlusive disease;WBC,white blood cells.⁎P b.05for pantoprazole or esomeprazole versus no PPI.†P b.01for pantoprazole or esomeprazole versus no PPI.Figure1Platelet reactivity index in the VASP phosphorylation assay in patients on clopidogrel with or without PPI:pantoprazole or esomeprazole. Data are presented as mean and95%CI.Figure2Adenosine diphosphate–induced platelet aggregation in patients on clopidogrel with or without PPI:pantoprazole or esomeprazole.Data are presented as mean and95%CI.Siller-Matula et al148.e3American Heart Journal Volume157,Number1treated with pantoprazole or esomeprazole.Therefore, the reported omeprazole-clopidogrel drug interac-tion10,11is probably not a class effect.A possible explanation for the reduced responsiveness to clopido-grel under omeprazole treatment could be the stereo-selective metabolism of omeprazole by CYP2C19,9,29 which might not be apparent for esomeprazole or other PPI.The lack of negative effects of concomitant treatment with pantoprazole or esomeprazole is an important finding because it may have an impact on clinical practice.Our study has97%power for pantoprazole and 88%for esomeprazole to exclude a20%difference of platelet reactivity index as compared to patients without PPI.The PRI was slightly(10%)higher in the esome-prazole group as compared to controls.However,this would require a sample size of762patients to definitely exclude such a drug-drug interaction with the same power(88%).These preliminary findings call for formal clinical trials investigating the effect of different PPIs on the pharmacodynamics and pharmacokinetics of clopido-grel.Moreover,it has to be evaluated if the reported interaction between PPI and clopidogrel has an impact on hard outcome parameters,as significant pharmaco-logical drug-drug interactions do not necessarily have clinical impact.30-32Similar to our study,another trial implicates that the PPI-clopidogrel interaction is not a class effect:con-comitant treatment with lansoprazole did not alter the pharmacokinetics or pharmacodynamics of clopido-grel.7This study also showed that increasing the gastric pH did not influence the platelet inhibitionby clopidogrel.7We selected2methods for evaluating PPI-clopidogrel drug-drug interaction:a very specific V ASP assay and a highly functional ADP-induced aggregometry.There are the following arguments for a combination of the two assays applied.Although the V ASP assay is highly specific for the effect of clopidogrel on the ADP receptor(P2Y12),V ASP is a biochemical marker which may not reflect certain aspects of platelet function: Firstly,activation of the P2Y12receptor by ADP initiates other signalling pathways,which are inde-pendent of V ASP phosphorylation.20Secondly,the antibody16C2used in the V ASP assay recognizes phosphorylation at a serine residue that is also phosphorylated by different cyclic guanosine mono-phosphate-dependent kinases that are not regulated by P2Y12.20Aggregometry is a functional assay based on the stimulation of platelet aggregation with ADP.26We used an impedance aggregometry in whole blood,which eliminates potential disadvantages of the light transmis-sion aggregometry:time-consuming centrifugation steps, variable reproducibility,large required sample volumes, and lengthy processing time.14A good correlation between impedance and light transmission aggregometry has been shown.25Therefore,combination of the V ASP assay and the ADP-induced aggregometry was reasonable.In summary,our study implies that in contrast to the reported negative omeprazole-clopidogrel drug interac-tion,the intake of pantoprazole or esomeprazole is not associated with impaired response to clopidogrel. LimitationsPossible imprecision in study results could have arisen from the nonrandomized study design.Although we adjusted for several variables in the multivariable logistic regression model,it is possible that residual confounding could affect results.Secondly,our study could not compare omeprazole with pantoprazole or esomepra-zole.Therefore,we could not examine whether the data from the previous trial are reproducible. References1.Snoep JD,Hovens MM,Eikenboom JC,et al.Clopidogrel non-responsiveness in patients undergoing percutaneous coronary inter-vention with stenting:a systematic review and meta-analysis.AmHeart J2007;154:221-31.2.Siller-Matula J,Schror K,Wojta J,et al.Thienopyridines incardiovascular disease:focus on clopidogrel resistance.ThrombHaemost2007;97:385-93.3.Angiolillo DJ,Guzman LA,Bass TA.Current antiplatelet therapies:benefits and limitations.Am Heart J2008;156:S3-9.4.Gladding P,Webster M,Ormiston J,et al.Antiplatelet drugnonresponsiveness.Am Heart J2008;155:591-9.5.Savi P,Pereillo JM,Uzabiaga MF,et al.Identification and biologicalactivity of the active metabolite of clopidogrel.Thromb Haemost2000;84:891-6.6.Pereillo JM,Maftouh M,Andrieu A,et al.Structure and stereo-chemistry of the active metabolite of clopidogrel.Drug Metab Dispos 2002;30:1288-95.7.Small DS,Farid NA,Payne CD,et al.Effects of the proton pumpinhibitor lansoprazole on the pharmacokinetics and pharmacody-namics of prasugrel and clopidogrel.J Clin Pharmacol2008;48:475-84.8.Lotfi A,Schweiger MJ,Giugliano GR,et al.High-dose atorvastatindoes not negatively influence clinical outcomes among clopidogrel treated acute coronary syndrome patients—a Pravastatin or Ator-vastatin Evaluation and Infection Therapy–Thrombolysis in Myocar-dial Infarction22(PROVE IT-TIMI22)analysis.Am Heart J2008;155:954-8.9.Li XQ,Andersson TB,Ahlstrom M,et parison ofinhibitory effects of the proton pump-inhibiting drugs omeprazole, esomeprazole,lansoprazole,pantoprazole,and rabeprazole on human cytochrome P450activities.Drug Metab Dispos2004;32: 821-7.10.Gilard M,Arnaud B,Cornily JC,et al.Influence of omeprazole on theantiplatelet action of clopidogrel associated with aspirin:therandomized,double-blind OCLA(Omeprazole CLopidogrel Aspirin) study.J Am Coll Cardiol2008;51:256-60.11.Gilard M,Arnaud B,Le Gal G,et al.Influence of omeprazol on theantiplatelet action of clopidogrel associated to aspirin.J ThrombHaemost2006;4:2508-9.148.e4Siller-Matula et al American Heart JournalJanuary200912.Ishizaki T,Horai Y.Review article:cytochrome P450andthe metabolism of proton pump inhibitors—emphasis onrabeprazole.Aliment Pharmacol Ther1999;13(Suppl3):27-36.13.Cairns JA,Eikelboom J.Clopidogrel resistance:more grist for the mill.J Am Coll Cardiol2008;51:1935-7.14.Gurbel PA,Becker RC,Mann KG,et al.Platelet function monitoring inpatients with coronary artery disease.J Am Coll Cardiol2007;50: 1822-34.15.Manolopoulos P,Glenn JR,Fox SC,et al.Acyl derivatives ofcoenzyme A inhibit platelet function via antagonism at P2Y1andP2Y12receptors:a new finding that may influence the design of anti-thrombotic agents.Platelets2008;19:134-45.16.Sudo T,Ito H,Kimura Y.Phosphorylation of the vasodilator-stimulatedphosphoprotein(VASP)by the anti-platelet drug,cilostazol,inplatelets.Platelets2003;14:381-90.17.Judge HM,Buckland RJ,Sugidachi A,et al.The active metabolite ofprasugrel effectively blocks the platelet P2Y12receptor and inhibits procoagulant and pro-inflammatory platelet responses.Platelets2008;19:125-33.18.Bonello L,Paganelli F,Arpin-Bornet M,et al.Vasodilator-stimulated phosphoprotein phosphorylation analysis prior topercutaneous coronary intervention for exclusion of postproce-dural major adverse cardiovascular events.J Thromb Haemost 2007;5:1630-6.19.Bonello L,Camoin-Jau L,Arques S,et al.Adjusted clopidogrelloading doses according to vasodilator-stimulated phosphoprotein phosphorylation index decrease rate of major adverse cardio-vascular events in patients with clopidogrel resistance:a multi-center randomized prospective study.J Am Coll Cardiol2008;51:1404-11.20.Kleiman NS.Will measuring vasodilator-stimulated phosphoproteinphosphorylation help us optimize the loading dose of clopidogrel?J Am Coll Cardiol2008;51:1412-4.21.Siller-Matula J,Lang I,Christ G,et al.Calcium channel blockersreduce the antiplatelet effect of clopidogrel.J Am Coll Cardiol2008;52:1557-63.22.Siller-Matula JM,Panzer S,Jilma B.Reproducibility and standardisedreporting of the vasodilator-stimulated phosphoprotein phosphor-ylation assay.Platelets2008;19:551-4.23.Morel O,Faure A,Ohlmann P,et al.Impaired platelet responsivenessto clopidogrel identified by flow cytometric vasodilator-stimulatedphosphoprotein(VASP)phosphorylation in patients with subacutestent thrombosis.Thromb Haemost2007;98:896-9.24.Seyfert UT,Haubelt H,Vogt A,et al.Variables influencing Multiplate(TM)whole blood impedance platelet aggregometry and turbidi-metric platelet aggregation in healthy individuals.Platelets2007;18: 199-206.25.Sibbing D,Braun S,Jawansky S,et al.Assessment of ADP-inducedplatelet aggregation with light transmission aggregometry andmultiple electrode platelet aggregometry before and after clopidogrel treatment.Thromb Haemost2008;99:121-6.26.Toth O,Calatzis A,Penz S,et al.Multiple electrode aggregometry:anew device to measure platelet aggregation in whole blood.Thromb Haemost2006;96:781-8.27.Penz SM,Reininger AJ,Toth O,et al.Glycoprotein Ibalpha inhibitionand ADP receptor antagonists,but not aspirin,reduce plateletthrombus formation in flowing blood exposed to atheroscleroticplaques.Thromb Haemost2007;97:435-43.28.Mueller T,Dieplinger B,Poelz W,et al.Utility of whole bloodimpedance aggregometry for the assessment of clopidogrel action using the novel Multiplate(R)analyzer-comparison with two flowcytometric methods.Thromb Res2007;121:249-58.29.Abelo A,Andersson TB,Antonsson M,Naudot AK,Skanberg I,Weidolf L.Stereoselective metabolism of omeprazole by humancytochrome P450enzymes.Drug Metab Dispos2000;28:966-72.u WC,Waskell LA,Watkins PB,et al.Atorvastatin reduces theability of clopidogrel to inhibit platelet aggregation:a new drug-drug interaction.Circulation2003;107:32-7.31.Saw J,Brennan DM,Steinhubl SR,et ck of evidence of aclopidogrel-statin interaction in the CHARISMA trial.J Am CollCardiol2007;50:291-5.32.Angiolillo DJ,Alfonso F.Clopidogrel-statin interaction:myth orreality?J Am Coll Cardiol2007;50:296-8.Siller-Matula et al148.e5American Heart Journal Volume157,Number1。