超声引导下肝、肾活检
- 格式:pdf
- 大小:1.68 MB
- 文档页数:13
超声引导下肝穿刺活检术在慢性肝病诊治中的价值摘要目的探讨超声引导下肝穿刺活检术在慢性肝病诊治中的临床价值。
方法138例慢性肝病患者作为研究对象,在超声引导下采用BARD活检枪、16及18G活检针对患者肝脏进行穿刺,取肝组织进行病理学检测,观察穿刺成功率、炎症活动度、纤维化程度。
结果138例患者全部穿刺成功,穿刺成功率为100%,穿刺过程及完成后无一例患者产生并发症。
病理学结果:共穿刺178针,对标本进行HE染色,镜下观察炎症活动度、纤维化程度,其中G1S0 17例,G1S1 19例,G1~2S2 50例,G3S1~2 32例,G3~4S4 30例;1例胆管缺失,考虑硬化性胆管炎。
结论超声引导下肝穿刺活检具有较高的安全性与成功率,并且并发症发生率较低,是明确诊断、评估疾病程度及判定治疗效果的重要依据,值得在临床上推广应用。
关键词超声引导;肝穿刺活检;慢性肝病;诊治价值肝穿刺活体组织检查术简称为肝穿刺活检术,是采取肝组织标本的一种简易手段,是通过肝穿刺针获取少许肝组织进行病理组织学检查。
超声引导下肝穿刺活检术是利用超声穿刺架,或超声穿刺探头直视穿刺针前进方向,使超声穿刺针进针位置固定,针道固定。
避免损伤大血管及胆囊、胆道等,使其具有安全、简单、迅速特点[1,2]。
本次研究选取2012年5月~2016年10月本院接收诊治的138例慢性肝病患者进行研究分析,现报告如下。
1 资料与方法1. 1 一般资料选取本院2012年5月~2016年10月收治的138例慢性肝病患者,其中男86例,女52例,年龄9~56岁,慢性肝病诊断符合2000年全国第十次病毒性肝炎及肝病会议修订的标准[3],其中慢性慢性乙型肝炎(乙肝)126例,肝功异常病因不明12例。
1. 2 仪器与方法术前1~2 d患者进行常规肝脏生化检查,凝血4项、血常规、血小板、心电图、胸片检查,腹部超声观察肝脏大小、形态,肝内回声、肝表面是否光滑、肝内管道走行、肝静脉及门静脉系统,胆囊、脾脏有无改变。
超声引导下经皮肾组织穿刺活检术对肾脏疾病的应用探讨朱智勇;吕永聪【摘要】目的探讨超声引导下经皮肾组织穿刺活检术在肾脏疾病中应用效果.方法收集本院2015年5月~2018年8月间收治的46例肾内科住院患者,对临床资料回顾性分析,超声引导下行经皮肾组织穿刺活检术.观察取材成功率、术后并发症及病理结果 .结果46例患者中,取材成功率100%,其中42例(91.3%)1~2针取材成功,3例(6.5%)3~4针取材成功;术后,3例(6.5%)患者包膜下出现包膜下血肿,未经特殊护理,术后1周血肿吸收;2例(4.3%)出现肉眼血尿,2d内自行消失、1例(2.2%)患者因术前紧张,血压升高,服用降压药物血压控制、8例(17.4%)腰部疼痛明显,因长时间卧床所致,经按摩及定期翻身消失,未见其他严重并发症.病理结果显示,lgA肾病17例(36.9%)、系膜增生性肾小球肾炎14例(30.4%),所占比例最高,其次为微小病变性肾病4例(8.7%),局灶增生型紫癜性肾炎、高血压病肾损伤、糖尿病肾小球硬化症各2例(4.3%),坏死性肾小球肾炎、急性肾小管损伤、新月体性肾小球肾炎各1例(2.2%).结论超声引导下经皮肾组织穿刺活检术取材成功率及穿刺命中率均较高,并发症少,可获得多种病理结果,值得采用.【期刊名称】《中国医药科学》【年(卷),期】2019(009)007【总页数】3页(P137-139)【关键词】超声引导;肾脏组织穿刺活检术;肾脏疾病;成功率【作者】朱智勇;吕永聪【作者单位】广东省中西医结合医院超声诊断科,广东佛山 528200;广东省中西医结合医院超声诊断科,广东佛山 528200【正文语种】中文【中图分类】R692肾脏疾病同一临床表现会呈现不同病理类型,同一病理类型临床表现又多种多样,固定规律缺乏,增加了病理诊断难度。
经皮肾组织穿刺活检术(简称肾活检)在肾脏疾病诊断中应用日趋普遍,可以更为直观的对肾脏组织学变化进行观察,尤其是在使用免疫学技术及特殊染色技术后,可以使疾病诊断更为精准、客观,为后续治疗提供科学依据,是取得良好预后的关键[1-2]。
高风险诊疗技术项目1.超声引导下高风险诊疗技术项目包括实性脏器或肿块穿刺活检、肝、肾、卵巢囊肿抽液硬化治疗、脓肿置管引流、心包置管抽液、胸腔置管抽液、术后各种积液的置管抽液治疗、肠套叠超声引导下水压灌肠复位、浅表淋巴结超声引导下细针细胞学检查。
2.CT高风险诊疗技术项目包括CT增强扫描过敏反应。
3.介入高风险诊疗技术项目包括肺动脉灌注、心血管介入诊疗技术(冠脉支架置入术、心脏永久性起搏器置入术、射频消融术)、神经血管介入诊疗技术(脑血管造影、动脉瘤栓塞)、综合介入诊疗技术、外周血管介入诊疗技术(肝动脉插管栓塞灌注、子宫动脉栓塞、脾动脉栓塞、下肢静脉造影术)。
4.胃镜高风险诊疗技术项目包括食道支架植入术、幽门支架植入、十二指肠支架植入、结肠支架植入、内镜下食道息肉摘除术、胃十二指肠息肉摘除术、结肠息肉摘除术、取异物、ESD、EMR、POEM、食管静脉曲张套扎、胃底静脉曲张硬化剂注射、内镜下钛夹止血、内镜下黏膜注射、ERCP。
5.普外科高风险诊疗技术项目包括全胃切除术、胃癌扩大根治术、左右半肝切除术、肝左外侧叶切除及楔形切除、门静脉高压食管胃底血管断流术、胆道再次手术、甲状腺癌颈淋巴结廓清术、甲状旁腺切除术、腹腔内肿瘤联合3种以上脏器切除、新开展的各种手术、诊断不明确的探查术、巨脾切除术、恶性肿瘤的腹腔镜胃、结直肠切除及消化道重建手术。
6.妇产科高风险诊疗技术项目包括子宫癌根治术、卵巢癌根治术、复杂尿漏修补术、各种疑难阴式手术、各种人工成形术、新开展的各种手术(腹腔镜、宫腔镜)、诊断不明的探查术、凶险性前置胎盘的子宫切除术、复杂性会阴裂伤修补术。
7.骨科高风险诊疗技术项目包括截肢(指趾)术、骨肿瘤切除术、骨折骨不连+再次内固定术、大关节内骨折内固定术、全髋关节置换术、全关节人工关节置换术、颈椎前后路联合手术、髋臼前后路联合手术、椎间孔镜手术、关节镜下后交叉韧带重建手术、胫骨平台骨折内外后入路联合手术。

超声引导下不同方法肾脏组织活检对比分析梅红;刘卫侠;黄秀英【摘要】Objective Explore the clinical effect of different ultrasound-guided methods of kidney biopsy. Methods Analyzed the 42 patients clinical data from March 2009 to February 2010 adopted ultrasound-guided automatic cutting biopsy gun. Conclusions Kidney biopsy plays an important role in kidney disease treatment, and ultrasound-guided automatic cutting biopsy has advantages of real-time observation, accurate, less invasive, fewer complications, which is worthy of further clinical application.%目的探讨超声引导下不同方法肾脏组织活检的临床效果.方法回顾分析2009年03月~2010年02月间采用超声引导自动切割活检枪行经皮肾穿刺活检术42例患者的临床资料,并与2009年03月~2009年08月相同时间内采用超声引导负压抽吸活检术、盲法负压抽吸活检术、超声引导手动切割活检术3组各40例患者临床资料进行对比观察.结果超声自动切割组1次穿刺成功率与超声手动切割组、超声引导负压组比较,差异无统计学意义(P>0.05);但超声自动切割组1次穿刺成功率明显高于盲法负压组,差异有统计学意义(х2=14.64,P<0.01).超声自动切割组并发症发生率与超声手动切割组比较,差异无统计学意义(х2=0.40,P>0.05);但明显低于超声引导负压组,差异有统计学意义(х2=15.79,P<0.01);明显低于盲法负压组,差异有统计学意义(х2=46.26,P<0.01).经一般对症处理2~3天后可好转或消失.结论肾活组织检查对肾脏疾病诊断、病理分型、治疗起着重要的作用,而超声定位自动切割肾穿刺活检术,具有实时观察、准确、创伤小、并发症少等优点,值得临床进一步推广应用.【期刊名称】《中国医疗设备》【年(卷),期】2011(026)008【总页数】4页(P152-155)【关键词】超声诊断仪;自动活检枪;超声引导;肾脏组织;活组织检查【作者】梅红;刘卫侠;黄秀英【作者单位】青岛市中心医院,超声科,山东,青岛,266042;青岛市中心医院,超声科,山东,青岛,266042;青岛市中心医院,超声科,山东,青岛,266042【正文语种】中文【中图分类】R445.1近年来,随着实验病理学、免疫学技术和介入性超声技术在临床的广泛应用,肾活检成为确定肾实质病变病理类型和病变程度的必需手段。

CHINA MEDICINE AND PHARMACY Vol.9 No.7 April 20191372019年4月第9卷第7期·放射与影像·超声引导下经皮肾组织穿刺活检术对肾脏疾病的应用探讨朱智勇 吕永聪广东省中西医结合医院超声诊断科,广东佛山 528200[摘要] 目的 探讨超声引导下经皮肾组织穿刺活检术在肾脏疾病中应用效果。
方法 收集本院2015年5月~2018年8月间收治的46例肾内科住院患者,对临床资料回顾性分析,超声引导下行经皮肾组织穿刺活检术。
观察取材成功率、术后并发症及病理结果。
结果 46例患者中,取材成功率100%,其中42例(91.3%)1~2针取材成功,3例(6.5%)3~4针取材成功;术后,3例(6.5%)患者包膜下出现包膜下血肿,未经特殊护理,术后1周血肿吸收;2例(4.3%)出现肉眼血尿,2d 内自行消失、1例(2.2%)患者因术前紧张,血压升高,服用降压药物血压控制、8例(17.4%)腰部疼痛明显,因长时间卧床所致,经按摩及定期翻身消失,未见其他严重并发症。
病理结果显示,lgA 肾病17例(36.9%)、系膜增生性肾小球肾炎14例(30.4%),所占比例最高,其次为微小病变性肾病4例(8.7%),局灶增生型紫癜性肾炎、高血压病肾损伤、糖尿病肾小球硬化症各2例(4.3%),坏死性肾小球肾炎、急性肾小管损伤、新月体性肾小球肾炎各1例(2.2%)。
结论 超声引导下经皮肾组织穿刺活检术取材成功率及穿刺命中率均较高,并发症少,可获得多种病理结果,值得采用。
[关键词] 超声引导;肾脏组织穿刺活检术;肾脏疾病;成功率[中图分类号] R692 [文献标识码] A [文章编号] 2095-0616(2019)07-137-03Exploration on application of ultrasound-guided percutaneousrenal biopsy in renal diseasesZHU Zhiyong LV YongcongDepartment of Ultrasound Diagnosis, Guangdong Hospital of Integrated Traditional Chinese and Western Medicine, Guangdong, Foshan 528200, China[Abstract] Objective To explore the application effect of ultrasound-guided percutaneous renal biopsy in renal diseases. Methods 46 hospitalized patients who were admitted and treated in the department of nephrology in our hospital from May 2015 to August 2018 were selected and their clinical data were retrospectively analyzed. They were given ultrasound-guided percutaneous renal biopsy. The success rate of sampling, postoperative complications and pathological results were observed. Results In 46 patients, the success rate of sampling was 100%. Among them, 42 cases (91.3%) were successfully sampled with 1-2 stitches and 3 cases (6.5%) were successfully sampled with 3-4 stitches. After surgery, subcapsular hematoma was found in 3 patients (6.5%). Without special nursing, hematoma was absorbed in 1 week after surgery. Gross hematuria occurred in 2 cases (4.3%) and disappeared within 2 days. One patient (2.2%) took antihypertensive drugs to control blood pressure for elevated blood pressure due to preoperative progress. Eight patients (17.4%) had obvious lumbar pain, which was caused by prolonged bed rest. The lumbar pain disappeared after massage and regular turning over, and no other serious complications were found. Pathological results showed that there were17 cases (36.9%, the highest proportion) of lgA nephropathy, 14 cases (30.4%) of mesangial proliferative glomerulonephritis, 4 cases (8.7%) of minimally pathological nephropathy, 2 cases (4.3%) of focal proliferative purpuric nephritis, 2 cases (4.3%) of renal injury due to hypertension, 2 cases (4.3%) of diabetic glomerulosclerosis, 1 case (2.2%) of necrotizing glomerulonephritis, 1 case (2.2%) of acute tubular injury and 1 case (2.2%) of crescentic glomerulonephritis. Conclusion The success rates of sampling and puncture of ultrasound-guided percutaneous renal biopsy ware both relatively high. It has few complications and it can obtain a variety of pathological results, which is worthy of adoption.[Key words] Ultrasound-guided; Percutaneous renal biopsy; Renal diseases; Success rate肾脏疾病同一临床表现会呈现不同病理类型,同一病理类型临床表现又多种多样,固定规律缺乏,增加了病理诊断难度。
超声引导下对肾活检技术的临床应用价值及意义目的:探讨超声引导下肾活检技术的临床应用价值及意义。
方法:选取2013年7月-2015年7月本院收治的采用超声引导下经皮肾穿刺活检术的患者90例作为研究对象,回顾性分析穿刺取材成功率,病理结果及术后并发症情况。
结果:所有患者取材成功率为100%;病理结果显示:系膜增生性肾小球肾炎46例,伴肾小球硬化22例;局灶性阶段硬化性肾小球肾炎19例;IgA肾病12例;狼疮性肾炎5例;过敏性紫癜性肾小球肾炎6例;膜性肾病1例;微小病变性肾小球病1例。
术后出现并发症12例,其中6例自诉有腰酸和腰痛,2例患者出现肉眼血尿后自行消退,4例出现穿刺针处出血,并发症发生率为13.3%。
结论:超声引导下肾脏穿刺活检术是一种安全有效的辅助检查方法,具有成功率高,术后并发症少的优点,值得临床应用。
由于人体肾脏疾病类型十分复杂,且患者临床治疗方法及预防均取决其病理类型。
近年来,临床介入性超声技术得到了快速发展及应用。
然而各种肾脏疾病临床病理组织学诊断的金标准为肾穿刺活检术,同时临床诊断肾脏疾病时还需尽可能地反映出患者疾病性质及病情严重程度,从而为患者临床治疗及预后判断提供参考依据[1]。
应用超声引导下经皮穿刺活检术是目前临床检验及诊断的主要方法,该方法可获取患者肾脏活组织病理标本,同时还可较好地诊断肾脏疾病,为患者临床治疗方案选择提供参考。
同时随着定位方法和穿刺仪器的快速发展,超声引导下经皮穿刺活检技术也得到极大发展,并为肾脏疾病患者临床治疗提供重要指导价值,本研究通过回顾性分析本院90例肾脏病患者在超声引导下穿刺活检的临床资料,探讨其取材成功率、并发症发生率,旨在为今后超声引导下肾活检技术的临床应用提供思路,现报道如下。
1 资料与方法1.1 一般资料选取2013年7月-2015年7月本院收治的超声引导下经皮肾穿刺活检术的患者90例作为研究对象,其中男58例,女32例;年龄7~78岁,平均(30±6)岁;临床诊断:肾病综合征36例,慢性肾小球肾炎44例,系统性红斑狼疮5例,不明原因肾衰5例。
超声引导下肾脏穿刺活检的影响因素分析作者:刘莉王金荣来源:《中国卫生产业》 2013年第34期刘莉王金荣泰兴市人民医院超声科,江苏泰兴 225499[摘要] 目的探讨超声引导下肾脏穿刺活检术的影响因素,降低并发症。
方法分析97例超声引导下肾脏穿刺活检患者的临床、穿刺方法、是否出现并发症,对穿刺的准确性和并发症进行分析。
结果 97例病例中,穿刺成功97例,出现一过性血尿1例,肾包膜下血肿2例,未见严重并发症。
结论超声引导下肾脏穿刺活检术是一种安全有效的诊断方法,可为临床提供重要的诊断依据。
[关键词] 超声引导;肾脏活检;并发症[中图分类号] R446.8;R445.1[文献标识码] A[文章编号] 1672-5654(2013)12(a)-0108-02肾脏功能异常病因复杂,病变早期临床表现和实验室检查缺乏特异性,超声引导下肾脏穿刺活检可提供病理诊断依据,目前认为是确诊肾脏疾病病因的可靠方法,对临床分型和治疗方案的确定有重要意义。
超声引导可准确地确定穿刺方向和深度,减少并发症[1],有效提高了成功率。
1资料与方法1.一般资料选取2010年1月—2011年12月期间,在我院住院,行超声引导下肾穿刺活检的患者97例,临床表现为血尿、蛋白尿伴不同程度的眼睑或/和双下肢浮肿,临床诊断包括:肾小球肾炎,肾病综合征,高血压性肾病,糖尿病肾病,不明原因肾功能衰竭等。
其中男48例,女49例,年龄16~77岁。
穿刺前常规检查出凝血或凝血酶原时间,无肾脏穿刺活检绝对禁忌症。
2 仪器与方法2.1应用TOSHIBAnemio30型彩色多普勒超声诊断仪,凸阵探头,频率为3.5MHz,穿刺枪采用用美国巴德全自动活检穿刺枪及专用穿刺针(Tru-Cut内槽切割式活检针16G或18G)进行肾活检。
2.2穿刺方法患者俯卧,腹下垫一软硬适中枕头,首先超声观察肾脏大小、结构以及实质区厚度,本组病例均选取右肾下极作为穿刺部位,分别在肾脏下极长轴和短轴方向初步定位,取两者交叉点为穿刺点,作一标记,并测量穿刺点皮肤至肾表面距离。
超声引导下肾脏穿刺活检术46例临床观察摘要:目的:探讨超声引导下经皮肾脏穿刺活检术的操作,为临床肾穿活检术的开展提供依据.方法:选取我院在2012年1月~2012年5月期间收治的46例行超声引导下肾脏穿刺活检术的患者为研究对象,对其临床资料进行回顾性分析。
结果:本组研究的46例患者均顺利的完成了超声引导下肾脏穿刺活检术.术后无感染发生,无严重并发症经治疗后痊愈出院。
结论:超声引导下经皮肾脏穿刺活检术具有准确定位、操作简便、成功率高和并发症少等特点值得基层医院推广。
关键词:超声;肾脏穿刺活检术;临床观察【中图分类号】r692.3 【文献标识码】b 【文章编号】1672-3783(2012)06-0247-01肾活检进行组织病理检查是肾脏疾病最常用的诊断手段。
它不仅用于自体肾或移植肾的病理诊断。
此外,它还是临床研究的一个重要途径[1]。
但是肾穿刺活检术是一种有创性检查,可出现肾脏破裂、出血等严重并发症,现超声引导下肾脏穿刺活检术,大大的降低了上述风险。
选取我院(原阳县人民医院)在2011年12月~2012年5月期间收治的46例行超声引导下肾脏穿刺活检术的患者为研究对象, 对其临床资料进行回顾性分析,现报告如下:1 资料与方法1.1 仪器和材料:①采用日立hv900彩色超声诊断仪,探头配有穿刺引导架2-5mhz频率;②肾穿活检针1个;③无菌手套3双,碘伏,消毒棉球,胶布等;利多卡因针2支,刀片一个,剪刀1个,无菌治疗弯盘1个,500ml生理盐水1瓶,5ml注射器2个。
④沙袋一个,腹带一条。
⑤3个清洁的5ml标本瓶,一个加入光境固定液3ml(faa固定液:甲醛溶液10ml,冰醋酸5ml,95%乙醇85ml混均),盖塞紧后备用(以防乙醇挥发)。
一个加入冷电镜固定液3ml[2.5%成二醛10ml,双蒸馏水40 ml,混匀后再加ph{为7.4的磷酸缓冲液(pbs)50m1.冰箱内保存},一个标本空瓶置冰箱内备用,取一块纱布用生理盐水浸透,以拧不出水,而又潮湿为宜。
超声引导经皮肾穿刺活检操作技巧经验分析摘要:目的:分析超声引导经皮肾穿刺活检操作技巧,提升穿刺的成功率,为患者减少术后并发症的影响作用。
方法:选取我院2019年12月-2021年12月肾内科因肾病住院患者共计105例为研究对象,观察肾病患者的刺穿次数以及术后出现并发症和不良反应的情况。
结果:105例患者中进行刺穿手术的总次数为452次,其中刺穿成功患者为444例,肾活检取材成功率为98.2%,其中 4 例因肾小球数目< 10 个,不能满足病理诊断要求,剩余448例均有明确的病理结果。
4 例因肾小球数目< 10 个的患者出现明显的水肿现象,占总数的0.89%,并无明显并发症以及不良反应。
结论:超声引导经皮肾穿刺活检术是当前临床最常使用的一种刺穿技术,患者经过术后有明显的治疗效果,并发生和不良反应的发生率较小,但是手术仍旧存在一定的风险,在刺穿过程中出现不良反应需要及时处理,引起重视。
关键词:超声引导;皮肾穿刺活检术;操作技巧经验分析随着我国医疗水平的不断提升,超声引导经皮肾穿刺活检术已经成为当前临床最常使用的一种刺穿技术,通过对患者进行超声引导经皮肾穿刺活检能够帮助其快速的诊断肾脏方面的疾病。
使用超声引导能够帮助快速查到和监控,有效提升穿刺的成功率,但是在实际的操作过程中还存在一定的风险,可能会引发一些术后的并发症和不良反应[1]。
本研究主要针对我院105例患者的刺穿手术,观察患者在进行刺穿手术之后的成功率,以及术后出现不良反应以及并发症的情况,具体研究报告如下。
1资料与方法1.1一般资料选取我院2019年12月-2021年12月肾内科因肾病住院,进行刺穿活检患者共计105例为研究对象,其中男性为56例,女性为49例,患者的平均年龄为(45.2±11.8)岁,所有患者均对此次研究知情,且签署同意书。
1.2一般方法超声引导装置与设备:Aloka-Prosoundα 10 彩超仪,探头频率3.5MHz;SAG-16160半自动性活检针。
超声介入穿刺的护理要点超声介入穿刺是一种在多种医学领域中广泛应用的技术,包括肝脏、肾脏和甲状腺等器官的穿刺活检、射频消融和经内镜手术等。
它通常由放射科医生和护士共同进行,因此在进行超声介入穿刺时,护士起着至关重要的作用。
护士需要在术前、术中和术后为患者提供全面的护理。
下面将详细介绍超声介入穿刺的护理要点。
术前护理超声介入穿刺的术前护理十分重要,因为它能为患者的安全和舒适提供良好的准备。
下面是超声介入穿刺术前护理的要点:1.了解患者病情。
在进行任何治疗前,护士需要了解患者的病情,包括病史、过敏史、用药情况等,以确保术前的准备工作和操作的安全性。
2.术前指导。
术前要向患者详细说明超声介入穿刺的术前准备工作,包括禁食禁饮时间、洗净穿刺部位等,提醒患者在术前按照医嘱进行准备,以确保手术的顺利进行。
3.准备必备器械。
在术前需要将超声引导设备和穿刺器械准备齐全,确保设备的正常运转和无菌状态。
4.心理疏导。
术前护士需要对患者进行心理疏导,以缓解患者的紧张和焦虑情绪,通过耐心的沟通和鼓励,使患者能够配合医生的操作。
5.术前检查。
护士需要负责对患者进行术前检查,包括测量体温、血压、脉搏等生命体征,以确保患者的身体状况符合手术的要求。
6.签署知情同意书。
术前护士需要协助患者或患者家属签署手术知情同意书,确保患者了解手术的风险和可能产生的并发症。
术中护理超声介入穿刺的术中护理是保证手术成功的关键之一。
护士需要密切配合医生,为患者提供全面的护理,确保手术的顺利进行。
以下是超声介入穿刺术中护理的要点:1.协助患者入室。
护士需要协助患者入室,帮助患者脱掉衣物,穿上手术服,并检查患者的身份、手术部位等,确保手术的顺利进行。
2.协助术前准备。
在术前,护士需要帮助医生进行术前准备工作,包括监测患者的生命体征、放置监护仪器、做好无菌铺巾、擦拭消毒等工作。
3.维持患者舒适。
在手术过程中,护士需要密切观察患者的情况,及时疏导患者的情绪,确保患者的舒适和安全。
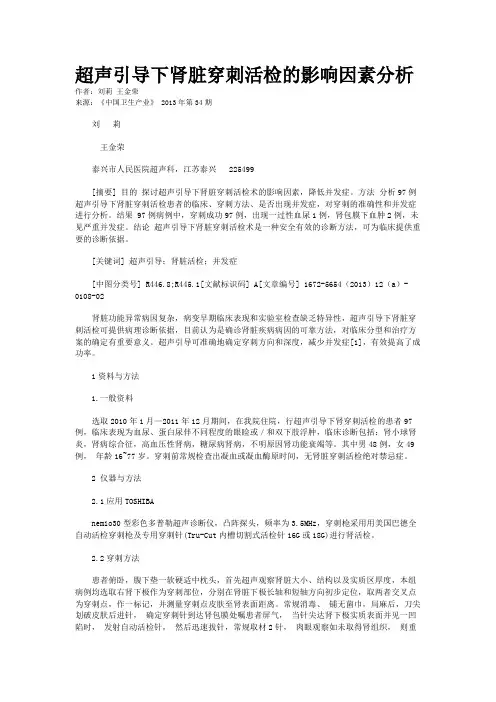
Ultrasound-Guided VisceralBiopsies:Renal and HepaticNirvikar Dahiya,MD ,William D.Middleton,MD ,Christine O.Menias,MD*The authors have provided several related videos at /.LIVER BIOPSY Ultrasound-guided percutaneous biopsy of vis-ceral organs in the abdomen has been in effect for many years.Paul Ehrlich is credited with per-forming the first percutaneous liver biopsy in1883in Germany.1Schu ¨pfer 2in 1907published the first liver biopsy series.Huard and Baronpopularized liver biopsy for general purposes in the1930s.Some of the more contemporary arti-cles reporting ultrasound-guided procedures were written in 1972by Goldberg and Pollack.3The basic approach to planning an ultrasound-guided biopsy is similar to performing any other in-terventional procedure.However,there are certain complexities specific to biopsy of the liver and kidney that are addressed in this article.Indications for a Liver Biopsy The indications for doing a liver biopsy are outlined in Box 1.A liver biopsy gives invaluable infor-mation regarding the staging,prognosis,and management even if clinical,laboratory,or imaging tests point to a specific focal or diffuse liver disease.Serial liver biopsies may help to monitor effects of specific therapy or to identify recurrence of disease.4Preparation for a Liver Biopsy The preparation of a liver biopsy constitutes the major portion of the work needed to execute a successful biopsy.The actual act of directing the needle to the target region and collecting the specimen only constitutes a small component of the procedure itself.A thorough history taking is imperative before the initiation of the biopsy.With this,the exact clinical question can be under-stood and the correct biopsy technique (fine-needle aspiration [FNA]vs core needle biopsy)determined;accordingly,the proper needle typeand gauge can be selected.For instance,inpatients with diffuse liver disease and a coexisting mass,it may be necessary to biopsy the mass (for diagnosis),the liver parenchyma (as part of preoperative surgical workup),or both depending Section of Abdomen Imaging,Mallinckrodt Institute of Radiology,Washington University,510South Kingshighway,St Louis,MO 63110,USA*Corresponding author.E-mail address:meniasc@KEYWORDSUltrasound Biopsy Renal Hepatic Perivascular Pseudoaneurysm KEY POINTSThe basic approach to planning an ultrasound-guided biopsy is similar to performing any other interventional procedure.Visceral organ biopsies are being routinely done these days with excellent diagnostic results. Ultrasound is a safe and reliable imaging modality to provide guidance for the vast majority of biopsies.With good technique,these procedures have a very low complication rate.Ultrasound Clin 7(2012)363–375doi:10.1016/j.cult.2012.03.0041556-858X/12/$–see front matter Ó2012Elsevier Inc.All rights reserved.ul t r a s o u n d .t h e c l i n i c s .c o mon the clinical situation.In patients with multiple livermasses,prior workup may point to specific lesions that are worrisome and others that are clearlybenign.If the patient had undergone positron emis-sion tomography/computed tomography (PET-CT)as part of the workup,it is important to make a good anatomic correlation between the hyper-metabolic lesion seen on the PET-CT and ultra-sound examination.Some of the newer ultrasound equipments allow for fusion imaging,whereby an overlaying of the CT,magnetic resonance imaging,or PET can be done with the ultrasound examination to accurately identify the target.5Once the clinical question has been understood,the prebiopsy workup includes evaluation of thebleeding profile of the patient and a detailed review of current medications taken by the patient.At our institution,we routinely obtain international normal-ized ratio (INR),platelet count,prothrombin time,and partial thromboplastin time (PTT).Our guide-lines include performing a biopsy when INR is less than 1.5and the platelet count is greater than70,000/m L.Some institutions take a count of plate-lets of 50,000/m L as the minimum requirement.6If the INR is greater than 1.5or if the platelets are less than 70,000/m L,a transfusion of platelets and/or fresh frozen plasma can be considered dependent on the clinical evaluation.The decision to proceedcan then be based on the location of the mass orthe general condition of the patient.Once the bleeding profile has been evaluated,it is important to review all the medications the patient is taking.Some patients may be on long-term antico-agulation or antiplatelet therapy,including aspirin,warfarin,clopidogrel bisulfate (PLAVIX;Bristol-Myers Squibb [New York,NY,USA]/Sanofi Phar-maceuticals [Bridgewater,NJ,USA]),and heparin.The referring physician must then determine if the risk of discontinuing the medicines is worse than the increased risk of bleeding related to the biopsy.If the medications are to be discontinued,wefollow the guidelines listed in Table 1to determinethe period of time they are withheld.Regardingsubcutaneous heparin,the liver biopsy can be per-formed if the PTT is within normal limits.Readers are advised to consult with their respective hema-tologic and clinical departments to ascertainguidelines for coagulation parameters and man-agement of time for holding anticoagulants before doing a biopsy.Many times such decisions are made on a case-by-case basis.An informed consent is obtained before pro-ceeding with the biopsy.An allergy history to latex gloves and lidocaine is established at this time.Allthe steps of the procedure are explained to thepatient in detail so that there are no surprisesduring the procedure itself.Procedure of Doing the Liver Biopsy A critical component of the procedure is choosing an approach for a liver biopsy.The ideal approach would be to find the shortest course to the target,avoiding lung,diaphragm,and all the vascular structures.However,this is not always possible.For a random liver biopsy,we prefer targeting the peripheral right hepatic lobe.This regionisDahiya et al364remote from the central hilar vasculature,and a tamponade effect can be achieved on comple-tion of the biopsy by having the patient to lie in right lateral decubitus position.If a good subcostal window is available,it is our first preference. However,in most cases an intercostal approach is performed,in which the needle traverses the diaphragm and pleural space.Care should be taken to avoid the aerated lung.For this reason, we generally position the needle inferior to the transducer,so that shadowing from the lung can be visualized and avoided before the needle is advanced into the liver.When using the intercostal approach,the needle is directed over the ribs as the vascular bundle courses along the inferior edge of the ribs(Fig.1).A random biopsy of the left hepatic lobe is per-formed when the right hepatic lobe is not feasible. In most cases,the lateral section of the left lobe is targeted in a manner such that the left portal vein and artery can be avoided.Color Doppler is used as a mapping tool for all our biopsies.Care is taken to minimize the risk of bleeding by trying to take the maximum length of the core tissue in the first pass.In cases in which the biopsy is of a target lesion within the liver,many have sug-gested choosing a biopsy path that courses through a part of the normal liver before reaching the target.Although there are no studies to prove it,this approach presumably helps with the tampo-nade effect if there is any bleeding from the target lesion after the biopsy(Fig.2).It also may have a role in preventing seeding.We believe that there may be some justification to this approach,but we do not hesitate to biopsy lesions on the surface of the liver if they are substantially easier to reach than the deeper lesions.Needles are categorized as aspiration-or suction-type needles(Menghini needle,Klatskin needle,Chiba needle,and Jamshidi needle)and cutting-type needles(Vim-Silverman needle and Tru-cut needle).The cutting-type needles can also be spring loaded.Most visceral core biopsies are now performed with spring-loaded needles. These needles can be further classified as side notch or end cutting(Figs.3–6).They can also be classified as automatic or semiautomatic.The semiautomatic needles allow one to manually advance the side-notch needle into the target.The biopsy is performed if the oper-ator is satisfied with the placement of the notch in the target.The automatic needle obtains the core without providing the option of manual advance-ment.With this type of needle,it is critical to make accurate measurements of the target size to select an appropriate predefined length for core biopsy.The end-cutting needles used in our department yield full core specimens at lengths of1.3,2.3,or3.3cm,whereas the semiautomatic side-notch needle yields a partial core specimen at a length of1or2cm.This can vary depending on the biopsy device manufacturers.If the biopsy device that is chosen has a loud clicking sound while performing the procedure,it is best to make patients aware of this so that they do not get startled during the procedure when they hear the sound.In terms of guidance,the choice is between using a mechanical guide attached to the transducer and freehand guidance.The free-hand technique requires more experience but has the distinct advantage of maneuverability, especially when subtle changes are required in direction or angle.Choice of transducer used to guide the needle is also important.Provided visualization of the target and adjacent vessels is adequate,phased array transducers have many advantages because they are small and easy to maneuver,especially when using an intercostal approach.Linear array transducers provide the advantage ofbetterFig.1.Liver biopsy technique.(A)Longitudinal view of the liver and lung interface showing the potential dangerof puncturing lung when performing biopsy via a superior approach.(B)Corresponding ultrasound image showsa bright reflection and dirty shadow arising from the aerated lung(L).Performing the biopsy from this trajectoryrisks potential lung puncture and pneumothorax.Arrows indicate the potential trajectories for liver mass biopsy.Ultrasound-Guided Visceral Biopsies365Fig.2.Liver biopsy technique.(A )Transverse view of the right lobe of the liver showing a large liver metastasis.(B )Magnified high-resolution view of the medial aspect of the lesion showing a preferred needle trajectory to traverse normal liver parenchyma before entering themass.Fig.3.Side-notch needle.(A )Side-notch needle in cocked position before biopsy of a focal lesion,(B )partially deployed position,and (C )fully deployedposition.Fig.4.Side-notch needles.(A )Side-notch needle in cocked position and (B )deployedposition.Fig.5.Full-core needle.(A )Full-core needle in cocked position,(B )partially deployed position,and (C )fully de-ployedposition.Fig.6.Full-core needle.(A )Full-core needle in cocked position and (B )fully deployed position.Dahiya et al366visualization if the target is superficial(ie,within approximately5cm of the skin surface).Curved array transducers provide an intermediate choice when lesions are too deep for a linear array,and visualization is inadequate with a phased array. The major disadvantage of curved arrays is their larger size,which makes them more clumsy to maneuver.Generally,we prefer lining up our biopsy needle along the side of the transducer, so that we can see the entire shaft of the needle as we approach the target(Fig.7).The sterile biopsy tray we use for a biopsy procedure includes1.10mL of1%lidocaine buffered with8.4%sodium bicarbonate2.25-gaugeÂ30-mm needle3.4Â4gauze pack4.Scalpel#11blade5.5-mL syringe6.25-gaugeÂ5/8-in needle for superficialanesthesia7.Applicator prep,gloves,and sterile drapes. We perform most of our biopsies under local anesthesia,using1%lidocaine mixed with sodium bicarbonate.The shorter25-gaugeÂ5/8-in nee-dle is used to inject lidocaine for superficial intra-dermal anesthesia after the patient has been cleaned and draped in a sterile manner.For deep-er anesthesia,we use the25-gaugeÂ30-mm needles to introduce more lidocaine.Deeper anes-thesia is injected under ultrasound guidance to determine the proper trajectory for the biopsy and to ensure that the anesthesia is injected deep enough to numb the capsule of the viscera, be it the liver or the kidney.Moderate sedation or conscious sedation is usually not necessary for routine liver biopsies; however,there are institutions that may typically use fentanyl(Sublimaze)and midazolam(Versed). If moderate sedation is used,special credentialing and privileging to perform sedation may be required.7It helps to give a little extra1%lidocaine at the capsule(Fig.8).At times,it helps to inject enough so as to cause a slight bump in the contour of the parietal peritoneum;this serves as a landmark for the entry point of the biopsy needle.Once the local anesthesia has been satisfacto-rily injected,we observe the relation between the biopsy target and the patient’s breathing to deter-mine if the biopsy will be done with the patient holding his/her breath in normal or deep inspiration or normal expiration.We usually ask the patient to practice a couple of breath-holds at this time to ascertain the best position of the target lesion for the biopsy.When possible,we prefer normal expi-ration because this is more reproducible than deep inspiration and it raises the location of lung paren-chyma.However,this expiration may not be possible in patients who are short of breath.For core biopsies,local anesthesia is followed by a small nick in the skin with a surgical blade. This is important because it can sometimes be difficult to advance core needles through the skin.The core needle we like to use is usually the spring-loaded18-gauge needle.For liver biopsies, we most often use the end-cutting needle that yields a full core specimen at lengths of1.3,2.3, or 3.3cm.When a focal lesion is near major vessels,a semiautomatic side-notch needle that yields a partial core specimen at a length of1or 2cm may be preferable.In both cases,the needle is introduced to the capsule surface;patients are then asked to hold their breath and the needleisFig.7.Freehand biopsy technique.Biopsy needle ispositioned in the plane of the image,immediatelynext to the side of the transducer.This allows for visu-alization of the needle tip and shaft throughout theprocedure.Fig.8.Liver capsule numbing.Needle shaft and tip(arrows)are positioned such that anesthesia adminis-tered is at the level of the liver capsule(arrowheads).Ultrasound-Guided Visceral Biopsies367introduced into the liver.In most cases,if the trajectory has been well planned and the needle is well visualized,the needle can be advanced to the lesion and a sample can be obtained on a single breath-hold.The throw of the needle depends on the location and size of the lesion and the distribution of adjacent vessels.It is important,however,to remember that a throw setting of 10or 13mm typi-cally results in a sample that is several millimeters shorter.So,if safe,it is best to avoid these short throws.For random liver biopsies,we mostly use the 3.3-cm throw.For FNA,we use either a 25-gauge spinal needle or a 23-gauge Chiba needle.In both cases,we prefer introducing the needle with the stylet inside to avoid contaminating the lumen with extraneous cells and to ensure that the needle has some tensile strength to maneuver.Once the needle tip has reached the target,the stylet can be removed and the process of taking the FNA sample can begin (Fig.9).Typically,we do the first aspiration without suction.Subsequent aspirations are performed with or without suction depending on the yield of the initial pass.Although we prefer making multiple separate passes,sometimes successful and consistent needle placement may be very difficult.In these cases,coaxial technique can be per-formed,7wherein an introducer is initially deployed into the target area and subsequent sampling can be done coaxially through it.Although a distinct advantage of the coaxial technique is the single puncture through the liver capsule,it is somewhat offset by the increased risk of capsule shearing or tearing as the needle stays in for a longer period while the patient breathes.The choice of performing an FNA biopsy or a core biopsy depends on the clinical scenario.In a patient with a known extrahepatic primary cancer in whom the only reason to perform a liver biopsy is to prove the presence of metastatic disease,we would do an FNA.If immediate on-site cytologic analysis is possible,aspirations are performed until a diagnostic sample is obtained.If the initial aspiration result is positive for malig-nancy and correlates with the primary tumor,no additional aspirations are required.If the initial specimens are negative for malignancy or suggest an alternative primary,then additional aspirations or core biopsies are obtained.If only semi-immediate off-site cytologic analysis is possible or if there is no cytologic support,several passes (3–6)should be obtained before terminating theprocedure.Fig.9.FNA.A 55-year-old woman with a history of pancreatic cancer.Small liver mass in the patient with a history of pancreatic cancer and a suspicious lesion seen on CT.(A )Contrast-enhanced CT scan of the liver showing a small low-attenuation lesion in the liver (arrow ).(B )Transverse sonogram of the liver shows a 9-mm solid hypoechoic lesion (cursors )corresponding to the lesion seen on CT.(C )Image obtained from a real-time cine clip taken during FNA shows the tip of a 25-gauge spinal needle (arrow )within the lesion.Needle shaft location (arrowheads )was more apparent during real-time imaging.Dahiya et al368Despite the presence of a known extrahepatic primary tumor,if immunohistochemical studies are anticipated,we typically do a core biopsy rather than an FNA.A core biopsy provides enough tissue for hematoxylin-eosin as well as immunohistochemical staining.Additional sec-tions can be taken from the paraffin block of the core biopsy to stain for immunohistochemistry markers such as estrogen receptor,progesterone receptor,and HER2/neu.If the clinical history or prior imaging results suggest a primary malignant or benign liver tumor, we generally perform core biopsies with an18-gauge needle(Fig.10).If hepatocellular cancer is confirmed,it is permissible to start with FNA and get preliminary analysis from the respective cytopathologist.If the diagnosis of hepatocellular cancer is con-firmed after1to3passes,no further aspirations are necessary.But if the initial aspiration results are negative or nondiagnostic,cores become nec-essary.In patients with suspected hepatocellular cancer and tumor thrombus of the portal or hepatic vein,it is possible to confirm the diagnosis and assist with staging by performing FNA of the tumor thrombus.8At times,referring hepatologists do not require a tissue diagnosis to confirm the presence of hepatocellular carcinoma if the cross-sectional imaging is consistent with hepato-cellular carcinoma and there is a correlative eleva-tion of a-fetoprotein level.The diagnostic accuracy of percutaneous nee-dle biopsy in lesions1cm or smaller has increased from79%(n524)in1987to87.5%(n524)in 1993and99%(n574)in1999.The use of a free-hand biopsy technique under ultrasound guidance is a common feature of all the series.9 ComplicationsLiver biopsies are relatively safe,with a complica-tion rate of0.2%to0.3%.10Hemorrhage is the most common complication and is more likely to occur in patients with underlying cirrhosis or ma-lignancy or bleeding diathesis.Most complications occur soon after completion of the biopsy.A linear color flow signal may at times be seen along the needle track immediately after the biopsy.11Kim and colleagues11evaluated the predictive role this signal played in the detection ofpostbiopsyFig.10.A61-year-old woman with a history of breast cancer.(A)Contrast-enhanced CT scan shows a small super-ficial low-attenuation lesion in the right lobe of the liver(arrow).(B)Oblique ultrasound image shows an18-gauge core needle(arrows)in position to obtain a core biopsy.(C)The needle is deployed(arrows)and traversesthe entire diameter of the lesion.Note that the throw in this case was selected at20mm to ensure sampling ofthe entire lesion.Ultrasound-Guided Visceral Biopsies369bleeding and referred to it as patent track sign.The investigators suggested that the postbiopsy bleeding events were significantly more likely when a patent track sign persisted on scans ob-tained5minutes after the biopsy(Fig.11). Ascites should not be considered a contraindica-tion to liver biopsy;however,in cases of moderate to large ascites,we prefer to have a paracentesis done before the biopsy.In cases in which patients are affected by significant coagulopathy,we recommend a transjugular hepatic biopsy. RENAL BIOPSYPercutaneous renal biopsy using an aspiration needle and with the patient in sitting position was first described by Iversen and Brun12in1951.In 1954,Kark and Muehrcke13described the use of the cutting Vim-Silverman needle in patients in the prone position,with a substantial improvement in the rate of success.The1961Ciba Foundation Symposium on renal biopsy marked the coming of age of this technique.14Recent advances in imaging,interventional,and cytologic techniques have enhanced the role of percutaneous biopsy in the diagnosis of renal masses.The incidental detection of benign and malignant renal masses has increased with increase in use of multidetector CT and magnetic resonance imaging.15In one study,25%of masses smaller than3cm were benign.16This factor has led to an increased demand for percutaneous renal biopsies for small-er masses.Biopsy of oncocytoma has been controversial.The reason lies in the difficulty pre-sented to differentiate benign cells from malignant cells on pathologic examination.Oncocytic cells can exist in various renal neoplasms,including renal oncocytoma and oncocytic renal cell carci-nomas,many of which are renal cell carcinomas of low metastatic potential.17These include gran-ular cell carcinoma,chromophobe renal cell carci-noma,and eosinophilic variant of papillary renal cell carcinoma.18–21In some cases,a diagnosis of oncocytoma can be strongly suggested on the basis of histochemical,immunocytochemical, and ultrastructural studies.Oncocytomascould Fig.11.A60-year-old man with chronic hepatitis C referred for an ultrasound-guided random liver biopsy.(A) Oblique view of the liver shows the core needle(arrows)in position obtaining a random liver biopsy.(B)Post-biopsy scan shows a patent tract(arrow)with detectable Doppler signal at the biopsy site.(C)Postbiopsy image obtained2hours after the procedure shows an acute hematoma surrounding the liver(arrows).This required Gelfoam embolization by an interventional radiologist.Dahiya et al370be confidently distinguished from oncocytic renal cell carcinoma using immunocytochemical anal-ysis.In a study done by Liu and Fanning,22all on-cocytomas were negative for vimentin,whereas only granular cell carcinoma and eosinophilic variant of papillary renal cell carcinoma were posi-tive for vimentin.Also,the2vimentin-negative neoplasms,oncocytoma and chromophobe renal cell carcinoma,could be distinguished by Hale colloidal iron stain,which was present in all chro-mophobe renal cancers but only focally or not at all in oncocytomas.Indications for a Renal BiopsyAs with the liver,kidney biopsies may be done either to evaluate an indeterminate focal lesion/ mass or to evaluate the cortex for a parenchymal disease process.A list of the more important indi-cations is presented in Box2.Preparation for Renal BiopsyThe issues related to preparation for the biopsy have already been discussed in the liver biopsy section and are essentially the same.The coagula-tion workup and the assessment for medications that interfere with clotting mechanisms are also similar.The fundamental difference comes in the approach to a kidney biopsy and the associated complications.As with hepatic biopsies,renal biopsies,whether focal or nonfocal,can be per-formed as outpatient procedures under ultrasound guidance.Focal mass lesion biopsyFor focal biopsies of a mass lesion,FNA and core biopsy can both be performed.Some institutions may perform both in the same sitting because a combination of the two may produce higher diagnostic yield.Whereas FNA may be performed using a22-or25-gauge needle,18-gauge needles are used for core biopsies.We do4to6passes for our FNA samples and2or more samples for our core biopsies.The patient is put in a posterior ob-lique or lateral decubitus position for most biop-sies.A towel or pillow may be put between the body and the bed to enhance the kyphosis.This helps in pushing the rib cage up and increasing the space available for doing the biopsy.We try to use the posterior axillary line as the point of entry.This posterolateral approach avoids the potential inadvertent injury to the colon.Some-times the location of the mass may prompt a more posterior approach in prone position (Fig.12).Once the mass has been visualized using ultrasound,anesthesia is administered in a manner similar to that described for liver biopsies. Nonfocal renal cortex(cortical)biopsy Nonfocal parenchymal biopsies are performed in whatever position provides optimal visualization of the kidney and avoids critical overlying struc-tures.The lower pole of either kidney is the preferred ually the left kidney is the first choice because it is lower in location than the right.The target is the cortical tissue from the lower pole of the kidney.Care is taken to avoid the medulla and the collecting system by direct-ing the needle into the superficial cortex in a rela-tively tangential manner.An onsite pathology service determines the adequacy of the sample (Fig.13).ComplicationsRenal biopsy is a relatively safe procedure,with loss of life extremely rare and major complications, mostly related to bleeding,occurring in only1%to 6%of procedures.23Renal biopsies have an over-all low mortality rate of0.031%.24Postbiopsy complications include hemorrhage, pseudoaneurysm,arteriovenous fistula,infection, pneumothorax,adjacent bowel or liver/spleen injury,and tumor seeding.Postbiopsy bleeding can occur in several places:into the collecting system,leading to microscopic or gross hematuria and possible ureteral obstruction;in a subcapsular location,leading to pressure tamponade and pain;or into the perinephric space,leading to retroperitoneal hematoma and possibly a drop in the serum hematocrit level(Fig.14).Mostclinically Ultrasound-Guided Visceral Biopsies371significant bleedings are recognized within 12to 24hours of the biopsy.25Mild perinephric hemorrhage is self-limiting and seen in 44%of the cases.26If there is a large retroperitoneal hematoma,the patient will have to be closely monitored and may even need other imaging modalities to assess the extent ofbleed.Fig.12.A 24-year-old man with a history of lymphoma.(A )Contrast-enhanced CT scan shows a low-attenuation lesion in the anterior aspect of the left kidney (arrows ).Other similar lesions were seen in both kidneys.(B )Trans-verse sonogram showing an 18-gauge core needle (arrowheads )within a hypoechoic solid renal mass (arrows )corresponding to the lesion shown on CT.Pathology from this biopsy was consistent withlymphoma.Fig.13.Status after renal transplant in a 45-year-old woman with elevated creatinine levels and concern for rejection.(A )Longitudinal view of the lower pole of the transplant.Identification of cortex without calyces and medullary components is important.(B )Transverse view of the lower pole of the transplant (arrowheads )shows the relationship of the transplant with the external iliac artery (arrow ).(C )Transverse view with needle in position showing the eccentric oblique orientation of the needle (arrows )used to obtain cortical tissue with little or no medullary component.Dahiya et al372。