药理学笔记整理之糖皮质激素
- 格式:docx
- 大小:100.56 KB
- 文档页数:5
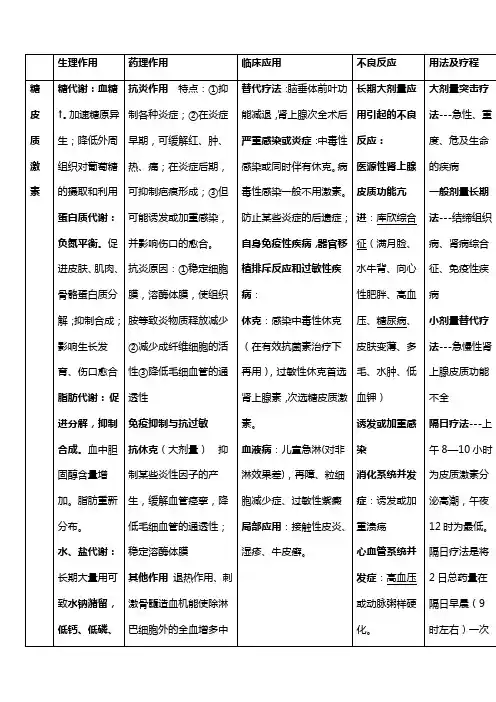
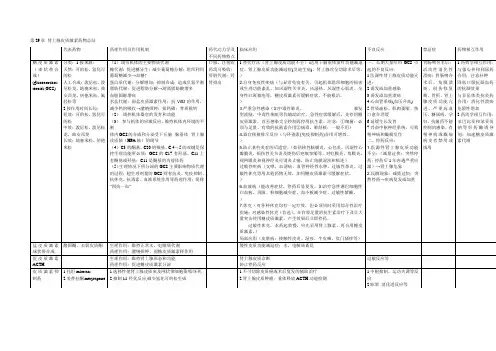
第29章肾上腺皮质激素药物总结代表药物药理作用及作用机制药代动力学及不同药物特点临床应用不良反应禁忌症药物相互作用糖皮质激素(束状带合成)(glucocorticos teroids,GCS) 分类:1.按来源:天然:可的松,氢化可的松人工合成:泼尼松,泼尼松龙,地塞米松,曲安西龙,倍他米松,氟轻松等2.按作用时间长短:短效:可的松,氢化可的松中效:泼尼松,泼尼松龙,曲安西龙长效:地塞米松,倍他米松(1)调节机体的主要物质代谢糖代谢:促进糖异生;减少葡萄糖分解;组织利用葡萄糖减少→血糖↑蛋白质代谢:分解增加;抑制合成;造成负氮平衡脂肪代谢:促进脂肪分解→游离脂肪酸增多血胆固醇增高水盐代谢:弱盐皮质激素作用;抗VitD的作用,减少钙的吸收→潴钠排钾;排钙磷;骨质脱钙(2)调控机体器官的发育和功能(3)参与机体的应激反应,维持机体内环境的平衡体内GCS的合成和分泌受下丘脑--腺垂体--肾上腺皮质轴(HPA轴)的调节(4)C3的酮基、C20的羰基、C 4-5的双键是保持生理功能所必须;GCS的C17有羟基、C11上有酮基或羟基;C11是酮基的为前体药(5)生理情况下所分泌的GCS主要影响物质代谢的过程;超生理剂量的GCS则有抗炎、免疫抑制、抗休克、抗毒素、血液系统作用等药理作用;简称“四抗一血”口服,注射给药均可吸收;肝脏代谢;经肾排出1.替代疗法(肾上腺皮质功能不全):适用于脑垂体前叶功能减退症、肾上腺皮质功能减退症(艾迪生病)、肾上腺次全切除术后等。
)2.自身免疫性疾病(与异常免疫有关,引起机体组织细胞的损害或生理功能紊乱。
如风湿性关节炎、风湿热、风湿性心肌炎、全身性红斑狼疮等,糖皮质激素可缓解症状,不能根治。
)3.严重急性感染(如中毒性肺炎、暴发型流脑、中毒性痢疾等作辅助治疗。
急性症状缓解后,先停用糖皮质激素,直至感染完全控制再停用抗生素。
注意:①细菌:必须与足量、有效的抗菌素合用②病毒、肺结核:一般不用)4.器官移植排斥反应(与环孢素(免疫抑制药)合用可增效。

药理学基础知识点:利尿药糖皮质激素化学治疗药物抗恶性肿瘤药基础知识化学治疗药物Give people the power to change the futureThe basic knowledge of pharmacology in 2015: the basic knowledge and chemical treatment of antimalignant neoplastic drugs in the drug of diuretic glucocorticoiddiuretic(1) effective diuretics: furthrice; In his acid; Bumetanide.[action mechanism]ACTS on the pulp loops rise a thick section, specificity to compete with Cl -, Na + -k + - 2 Cl - common Cl - combining parts of the transport system, inhibition of NaCl reuptake and act as a powerful diuretic effect.[diuresis] rapid, powerful, transient, individual differences【 clinical application 】 severe edema; Acute pulmonary edema; Brain edema; Treatment of acute renal failure (early urination); To promote the excretion of poisons.(2) effective diuretic drugs: thiazine diuretics;【】 pharmacological activities and mechanisms 1.Diuretic effect: features: mild, lasting working part: pulp loops rise a thick section of the cortex of distal convoluted tubules (start) effect: inhibition of K +, Na + - 2 cl - common transport systems; To promote Na plus minus K plus exchange; Effect of inhibiting carbonic anhydride enzyme. The reduction of blood pressure by diuresis and blood volume in the early stage. Antidiuresis (antidiuresis)A. clinical application 】【 edema: 1. The mind edema preferred medicine 2. Renal edema, renal function disorder disabled or careful with 3. Liver cirrhosis ascites: appropriate and spironolactone share b. hypertension c. diabetes insipidus【 poor response 】 1 electrolyte disorder 2 hyperuria 3 metabolic changes: high blood sugar, hyperlipemia. 4 an allergic reaction(3) inefficient diuretic drugs: snails, aminophenylate, amilloli[diuresis and mechanism] features: slow effect, weak effect, lasting, not losing potassium. Site: distal convoluted tubule and assembly-tube intracellular aldosterone receptor. Way: the aldosterone receptor for aldosterone. Result: suppress Na + -k + exchange, row Na + leave K +【 clinical application 】 the persistent edema of aldosterone increases. It is commonly used in combinationwith strong effect and medium effect diuretic medicine, enhances diuretic effect and can complement K +【 adverse reaction 】 1 long use cause high blood potassium: kidney function bad person to disable. 2 sex hormone response: male breast female, sexual dysfunction, women's polytrichosis.Pharmacology basic knowledge: glucocorticoidglucocorticoidsGlucocorticoid has a powerful anti-inflammatory effectthat inhibits the inflammatory response from multiple causes. At the beginning of the inflammation, can heighten blood vessels of tension, relieve congestion, reduce MAO vascular permeability, inhibition of leukocyteinfiltration and devour reaction at the same time, reduce inflammation factors. It can relieve the symptoms of red swelling and fever. Late in inflammation, glucocorticoid through inhibition of capillaries and fibroblasts proliferation, inhibit the synthesis of collagen and glycosaminoglycan and granulation tissue hyperplasia, prevention and control of adhesion and scar formation, reduce sequelae.[clinical significance](1) severe acute infection: adjuvant therapy with glucocorticoids while treating infection with effective antimicrobial agents. Because of its ability to increasethe tolerance of the harmful stimulation of the body, itis beneficial to buy time and rescue. (2) the sequelae of anti-inflammatory treatment and the prevention and control of certain inflammation: if inflammation occurs in vital organs of the human body, it will cause severe dysfunction. Therefore, early application of glucocorticoid to reduce inflammatory infiltration and reduce the excessive hyperplasia and adhesion of the fibers in the healing process, prevent the sequelae from occurring.[pharmacological action]A, anti-inflammatories B, anti-immune function, especially in cell immune-c, anti-shock action D, and anti-toxicity, can improve the body's tolerance to bacterial endotoxin. E, the stimulation of the blood and hematopoietic system, G, can induce the increase of gastric acid and pepsin[clinical use]A, alternative treatment B, and severe infection are used as adjuvant therapy C, antishock D, autoimmune disease and allergic disease E, hematopathy and tumor treating F,anti-local inflammation[adverse reaction]Hyperactivity syndrome adrenocortical function 1, 2, 3 induce and aggravate the infection, the digestive system complication 4, 5, and other complications can cause movement system aberrations 6, drug withdrawal reaction:(1), drug-induced cortical dysfunction (2), the bounce phenomenonPharmacology basic knowledge point: chemical treatment medicinechemothermyThe mechanism of antimicrobial action:(1) inhibit bacterial cell wall synthesisThe function of the cell wall is to maintain the normal form and osmotic pressure of the bacteria and maintain the normal function of the bacteria. Antimicrobial drugs can cause bacterial cell wall defects, water is infiltrated by the outside, and the cell expands and deforms, causing the cell to dissolve and dissolve and die.Applied to the cytoplasm: cycloserine, phosphodomycinApplied to cytoplasm: vancomycin, bacillusApplied to the cytoplasm: penicillin, cephalosporin(2) the permeability of the cell membrane:The cytoplasm is increased, protein, nucleotide, sugar, salt, and bacterial death(3) inhibit the synthesis of bacterial proteinsThecombination of the tetracycline and aminoglycoside antibioticsCombined with the 50s: erythromycin, chloramphenicol, and lincomycinAffect the whole process of protein synthesis: amino glycoside antibiotics(4) affect folate and nucleic acid metabolism? Folic acid is the precursor of synthetic nucleic acid? Sulfamide and methoxybenzine (TMP) can inhibit the enzyme and dihydrofolate reductase, which inhibits folic acid metabolism and inhibits the growth and reproduction of bacteria.Pharmacology basics: chemotherapy drugs (2)chemothermyBacterial resistance mechanism(1) it produces an inactivated enzyme that causes the antibiotic to be inactivatedThese inactivated enzymes can be expressed by plasmid and chromosomal genesA) hydrolyzed enzymes - antibiotics for beta-lactamB) passivating enzymes - aimed at aminoglycoside antibioticsC) other(2) the target changes of antimicrobial agentsA) changes the structure of the target protein, reducing the affinity with antibioticsRFP resistant bacteria change the substructure of the RNA polymeraseB) increase the number of target proteins and maintain normal form and function when the drug is presentEnterococcus is an antibiotic for beta-lactamC) the new synthesis function is normal and the target protein of antibiotic affinity lowThe bacterium produces penicillin binding protein PBP2a, which is extremely low to methoxillin(3) reducing the permeability of the outer membrane of the bacteriaAfter exposure to antibiotics, by changing the nature of the channel proteins and to reduce the bacteria number of membrane permeability to prevent antibiotic into thebacteria in the body and produce acquired drug resistance(4) to enhance active external system activity(5) bacteria change their metabolic pathwaysThe reason that the bacterium is resistant to sulfonamide is:There was a rise in aminobenzoic acidDrug-resistant strains make direct use of exogenous folic acidThe basic knowledge of pharmacology: the basic knowledge of anti-malignant tumor medicine【 introduction 】 in public institution to test network to provide medical and health professional knowledge, the following bring every candidates based on knowledge points - anti tumor medicine pharmacology foundation knowledge related content, for everybody to study for.The relationship between the proliferation cycle of the tumor and the drug of chemotherapyTumor cell proliferation cycle:1, the proliferative cell group 2, the non-proliferative cell group 3, the non-proliferative cell group (G1, S, G2, M)Periodic nonspecific drugs: the cells that can inhibit or destroy the cycle of the proliferation cycle, even G0. Alkanes, antibiotics.Cyclically specific drugs: only one issue of the cycle is stronger.The mechanism and classification of anti-malignant tumor drugs:Drugs that inhibit the synthesis of nucleic acids (DNA, RNA) : antimetabolitics(1) the steric acid synthase inhibitor, preventing pyrimidine nucleotide formation: 5-fluorouracil(2) DNA polymerase inhibitors: abglycoside(3) nucleotide reductase inhibitors: hydroxylurea(4) dehydrofolic acid reductase inhibitor: methylamineDrugs that damage DNA directly and stop it from being copied: alkylation, certain anti-cancer antibiotics, and cisplatin.The drugs that interfere with the transcription process to block the synthesis of RNA: acidomycin, roerythromycin, and amycin.4, the drugs that affect the synthesis of proteins: changchun alkaloids, taxol.Drugs that affect the hormonal balance of cancer: corticosteroids, androgens, and estrogen.。
巧记糖皮质激素,一看就懂!口诀巧记糖皮质激素!作者|格地章来源|医学界呼吸频道先来看看下面这副美图......认识吗?似曾相识的感觉有没有?朦朦胧胧当中...依稀记得......读书时在某本书上看见过,但是非要说出它是啥吧......额......不好意思,确实是不知道啊......(有一首歌是这么唱的:我们好像在哪见过,我记得你,记得那是一个夏天盛开如花......)那么,它到底是啥呢?揭晓答案......肾上腺皮质激素类药物的基本结构甾体母核!此时此刻,一种“山重水复疑无路,柳暗花明又一村”的畅快油然而生有没有?细讲一下肾上腺皮质激素类药物共同的结构特点:1、保持其生理功能所必须结构:甾核A环的C3的酮基、C4-5的双键、C20的羰基。
2、糖皮质激素结构特点:甾核D环的C17上,C11上有= O或-OH→→→糖代谢的影响及抗炎等作用较强,而对水、盐代谢作用较弱。
3、盐皮质激素结构特点:甾核D环的C17上无α-OH,C环C11上无O或有O与C18相联→→→水、盐代谢作用较强,对糖代谢作用很弱。
糖皮质激素(GC)是一种肾上腺皮质中束状带分泌的一种甾体激素,具有调节糖、脂肪、蛋白质的生物合成和代谢的作用,还具有抑制免疫应答、抗炎、抗毒、抗休克等作用。
现于临床上广泛使用。
该类药物作用广泛,随剂量不同而不同:■生理情况下:主要影响物质代谢过程,缺乏时将引起代谢失调,甚至死亡;■应激状态下:通过允许作用等,使机体能够应对内外环境变化产生的刺激;■ 超生理剂量(药理剂量):除影响物质代谢以外,还有抗炎、免疫抑制等作用。
1常用糖皮质激素药物药物名称半衰期(h)抗炎等效剂量(mg)短效类氢化可的松可的松8~128~122025中效类泼尼松泼尼松龙甲泼尼松龙曲安西龙帕拉米松氟泼尼松龙12~3612~3612~3612~36----554421.5长效类倍他米松地塞米松36~5436~540.60.752巧记来啦★药理作用四抗一抑制一允许一其他,升糖解蛋分脂百代水电。
第二十二单元糖皮质激素一、A11、长期应用糖皮质激素引起类肾上腺皮质功能亢进的表现是A、高血钾B、低血钠C、低血压D、高血脂E、低血糖2、小剂量糖皮质激素替代疗法用于治疗A、肾上腺皮质癌B、肾病综合征C、肾主腺嗜铬细胞瘤D、垂体肿瘤E、垂体前叶功能减退3、下列关于糖皮质激素对血液与造血系统作用的叙述,错误的是A、使血小板增多B、使红细胞和血红蛋白含量增加C、降低纤维蛋白原浓度D、嗜中性粒细胞数增多E、血中淋巴细胞减少答案部分一、A11、【正确答案】 D【答案解析】糖皮质激素具有轻微的盐皮质激素即醛固酮的作用,故有保钠排钾作用,能提高血钠水平降低血钾,引发低血钾;同时糖皮质激素可以促进脂肪分解提高血脂,并增加糖原分解提高血糖。
【该题针对“糖皮质激素的应用、不良反应和禁忌证”知识点进行考核】2、【正确答案】 E【答案解析】糖皮质激素可用于肾上腺皮质功能不全,小剂量替代疗法适用于腺垂体功能减退症、肾上腺皮质功能减退症(艾迪生病)、肾上腺危象和肾上腺次全切除术后。
【该题针对“糖皮质激素的应用、不良反应和禁忌证”知识点进行考核】3、【正确答案】 C【答案解析】糖皮质激素能刺激骨髓造血功能,使血液中红细胞和血红蛋白含量增加,大剂量亦使血小板和纤维蛋白原增多,缩短凝血时间。
刺激骨髓中的中性粒细胞释放入血而使嗜中性粒细胞增多,但降低其游走、吞噬等功能。
亦可使淋巴组织退化,抑制淋巴细胞分裂,使血中淋巴细胞减少。
此外,也能减少血中单核细胞和嗜酸性粒细胞,这可能是由于细胞转移至肺、脾、肠等组织的缘故。
【该题针对“糖皮质激素的分类及常用药、糖皮质激素的药理作用”知识点进行考核】。
药考证,找润德,医药培训第一品牌
糖皮质激素知多少
本文由润德教育整理
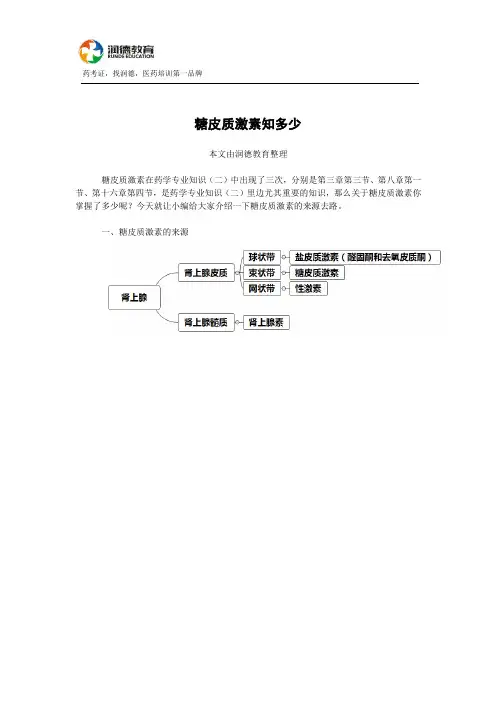
糖皮质激素在药学专业知识(二)中出现了三次,分别是第三章第三节、第八章第一节、第十六章第四节,是药学专业知识(二)里边尤其重要的知识,那么关于糖皮质激素你掌握了多少呢?今天就让小编给大家介绍一下糖皮质激素的来源去路。
一、糖皮质激素的来源
药考证,找润德,医药培训第一品牌二、糖皮质激素的药理作用
药考证,找润德,医药培训第一品牌
【习题演练】
1.下列哪项不属于糖皮质激素的药理作用的是
A.抗休克
B.免疫抑制作用
C.抗外毒素
D.抗炎
E.升高血糖
2.下列关于糖皮质激素对血液和造血系统作用描述不正确的是
A.血小板增多
B.纤维蛋白原浓度增高
C.淋巴细胞增多
D.嗜酸细胞减少
E.红细胞和血红蛋白含量增加
3.糖皮质激素免疫抑制作用的机制是
A.抑制巨噬细胞吞噬功能
B.稳定溶酶体膜
C.增强心肌收缩力
D.使细胞内cAMP明显升高
E.直接扩张支气管平滑肌
【答案】CCA。

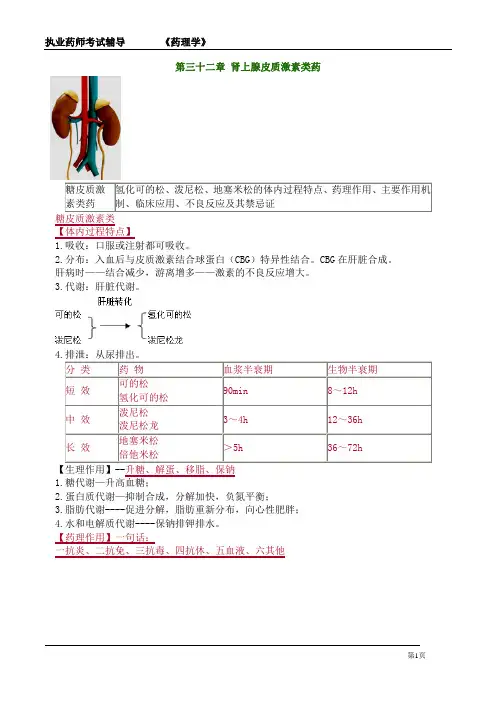
第三十二章肾上腺皮质激素类药糖皮质激素类药氢化可的松、泼尼松、地塞米松的体内过程特点、药理作用、主要作用机制、临床应用、不良反应及其禁忌证糖皮质激素类【体内过程特点】1.吸收:口服或注射都可吸收。
2.分布:入血后与皮质激素结合球蛋白(CBG)特异性结合。
CBG在肝脏合成。
肝病时——结合减少,游离增多——激素的不良反应增大。
3.代谢:肝脏代谢。
分类药物血浆半衰期生物半衰期短效可的松氢化可的松90min8~12h中效泼尼松泼尼松龙3~4h12~36h长效地塞米松倍他米松>5h36~72h【生理作用】--升糖、解蛋、移脂、保钠1.糖代谢—升高血糖;2.蛋白质代谢—抑制合成,分解加快,负氮平衡;3.脂肪代谢----促进分解,脂肪重新分布,向心性肥胖;4.水和电解质代谢----保钠排钾排水。
【药理作用】一句话:一抗炎、二抗免、三抗毒、四抗休、五血液、六其他1.抗炎作用(1)抗炎强大、迅速、凡炎皆抗,对感染性、非感染性(过敏性、机械性、化学性)炎症均有效——“万能灵药”。
(2)对炎症不同阶段均有抑制作用:①早期——渗出减少,改善症状;②后期:延缓肉芽组织生成,防止粘连及瘢痕形成,减轻后遗症。
【抗炎实质】实质:提高了机体对炎症的反应性;不足——降低了机体的防御机能。
激素的抗炎是“穿着石棉衣站在火里”——不怕火烧——但不救火、也不灭火。
【注意!】感染扩散、创面愈合延迟。
(3)抗炎机制——略。
①抑制磷脂酶A2(PLA2),减少前列腺素(PGs)和白三烯(LTs)等炎性介质合成;②抑制细胞黏附分子表达和有关细胞因子基因的转录;③稳定肥大细胞膜和溶酶体膜,减少组胺释放;④抑制肉芽组织形成,防止粘连及瘢痕形成。
2.免疫抑制作用(抗免疫)不同剂量作用有异——【记忆】“小细大体。
”大剂量:抑制体液免疫。
3.抗毒作用——不是抗病毒!TANG对抗毒素对机体的刺激性反应,缓解毒血症症状。
抗毒机制:抑制NO(一氧化氮)合酶,降低NO水平。
肾上腺皮质激素类药物
概述:肾上腺素激素是肾上腺皮质所分泌的激素的总称,其基本结构为甾体类化合物。
糖皮质激素类
药物分类:
短效——可的松→氢化可的松
中效——泼尼松→泼尼松龙
长效——地塞米松、倍他米松
体内过程:
1.口服、注射均可吸收。
2.可的松和泼尼松在肝内转化为氢化可的松和泼尼松龙而生效,严重肝功能不全者只宜用氢化可的松或泼
尼松龙。
药理作用:
1.对物质代谢的影响 (生理剂量)
①糖代谢:升高血糖
②蛋白质代谢:促分解,抑合成,负氮平衡
③脂肪代谢:增高血浆胆固醇,促使皮下脂肪分解,形成向心性肥胖,表现为“满月脸,水牛背”。
④水和电解质代谢:保钠排钾
——长期应用能促进钙、磷排泄,骨质脱钙。
归纳:
2. 抗炎作用:
抗炎作用强大、非特异性,对感染性、非感染性(过敏性、机械性、化学性)炎症均有效
(凡炎皆抗,“万能灵药” )。
利:早期——渗出减少,改善症状;
后期——延缓肉芽组织生成,防止粘连及瘢痕形成,减轻后遗症。
弊:降低了机体的防御机能。
3.免疫抑制与抗过敏作用(抗免疫)
(1)对免疫系统的抑制作用:抑制免疫细胞功能,对免疫反应的多个环节均有抑制作用;
小剂量:抑制细胞免疫;
大剂量:抑制体液免疫。
激素四大生理作用
升糖解蛋分脂保钠
抗炎不抗菌,
抗炎不抗因,
治标不治本
(2)抗过敏作用:减少过敏介质的产生,抑制因过敏反应而产生的病理变化。
4.抗休克作用:
大剂量,常用于严重休克,特别是感染中毒性休克的治疗。
①扩张痉挛收缩的血管,加强心肌收缩;
②降低血管对某些收缩血管活性物质的敏感性;
③稳定溶酶体膜,减少心肌抑制因子的形成
④提高机体对内毒素的耐受力,但对外毒素无效。
5.其他作用
(1)退热作用
严重的中毒性感染
降低体温调节中枢对体内致热原的敏感性
(2)血液与造血系统(一少五多)
①淋巴细胞减少
②红细胞、血红蛋白、血小板、中性粒细胞、纤维蛋白增多
(3)中枢神经系统
提高中枢的兴奋性,引起欣快、激动、失眠等,偶可诱发精神失常、癫痫及小儿惊厥的发作。
(4)骨骼
长期应用本类药物时可出现骨质疏松,特别是脊椎骨,其机制可能是糖皮质激素抑制成骨细胞的活力,减
少骨中胶原的合成,促进胶原和骨基质的分解,使骨质形成发生障碍。
骨质疏松——自发性骨折。
(5)心血管系统
增强血管对其他活性物质的反应性,诱发高血压——允许作用。
(6)消化系统
促进胃酸和胃蛋白酶的分泌,抑制黏液的分泌,可诱发或加重溃疡病。
(7)允许作用:
糖皮质激素对有些组织细胞虽无直接活性,但可给其他激素发挥作用创造有利条件。例如糖皮质激素可增
强儿茶酚胺的血管收缩作用和胰高血糖素的升血糖作用。
临床应用:
1.严重感染或炎症(辅助治疗)
(1)严重急性感染:主要用于中毒性感染或伴有休克者,如中毒性菌痢、暴发型流脑及败血症等
足量有效的抗菌药物+皮质激素(先停皮质激素后停糖皮质激素)
病毒性感染一般不用
(2)抗炎治疗及防止某些后遗症(早期应用)
对脑膜炎、心包炎、关节炎、角膜炎、视神经炎、睾丸炎及(Ⅱ、Ⅲ度)烧伤后瘢痕挛缩等。
2.免疫相关疾病
A.自身免疫性疾病
如严重风湿热、风湿性心肌炎、风湿性及类风湿性关节炎、全身性红斑狼疮、自身免疫性贫血和肾病综合
征等。
多发性皮肌炎为首选。
不宜单用,采用综合疗法。
B.过敏性疾病
如荨麻疹、血管神经性水肿、支气管哮喘和过敏性休克等。
主要用肾上腺素和抗组胺药。
C.器官移植排斥反应
应用糖皮质激素预防。
若已经发生排斥反应,治疗时采用大剂量氢化可的松静脉滴注,排斥反应控制后再逐步减少剂量至最小维
持量,并改为口服。
3.抗休克治疗
感染中毒性休克 首选 在有效的抗菌药物治疗前提下,可及早、短时间突击使用大剂量糖皮质激素
过敏性休克 糖皮质激素为次选药,与首选药肾上腺素合用
低血容量性休克 在补液补电解质或输血后效果不佳者,可合用超大剂量的皮质激素。
4.血液病
儿童急性淋巴细胞性白血病(疗效较好),再障、粒细胞减少症、血小板减少症和过敏性紫癜等的治疗(停
药后易复发)
5.局部应用
1)一般性皮肤病,湿疹、牛皮癣、接触性皮炎等(可局部外用)
2)宜用氢化可的松、泼尼松龙或氟轻松
6.替代疗法
急、慢性肾上腺皮质功能不全者
脑垂体前叶功能减退
肾上腺次全切除术后
不良反应:
1.长期大剂量应用引起的不良反应
(1)医源性肾上腺皮质功能亢进综合征
物质代谢和水盐代谢紊乱所致。
满月脸、水牛背、向心性肥胖、痤疮、浮肿、低血钾、高血压、糖尿病等(停药后低盐、低糖、高蛋白饮
食)
(2)诱发或加重溃疡
刺激胃酸、胃蛋白酶分泌,减弱胃粘膜的保护作用
(3)诱发或加重感染
免疫抑制作用,结核病患者合用抗结核药
(4)心血管系统并发症
水钠潴留、高血脂引起高血压和动脉粥样硬化
(5)骨质疏松、肌肉萎缩、伤口愈合迟缓、抑制生长发育等
促蛋白质Pr分解,抑合成,增加钙磷排泄
(6)糖尿病
糖皮质激素促进糖原异生,降低组织对葡萄糖的利用,抑制肾小管对葡萄糖的重吸收作用。
(措施:在控制原发病的基础上,尽量减少糖皮质激素的用量,最好停药;如不能停药,应酌情给予口服
降糖药或注射胰岛素治疗。)
(7)精神失常
有癫痫或精神病史者禁用或慎用。
2.停药反应
(1)医源性肾上腺皮质功能不全
由于长期大剂量使用糖皮质激素,反馈性抑制垂体-肾上腺皮质轴致肾上腺皮质萎缩所致。
(2)反跳现象
其发生原因可能是患者对激素产生了依赖性或病情尚未完全控制,突然停药或减量过快而致原病复发或恶
化。
禁忌症:
长期大剂量应用出现的不良反应归纳:
A.肾上腺皮质功能亢进综合征
B.诱发或加重感染
C.消化系统并发症(溃疡)
D.运动系统并发症(骨质疏松、肌肉萎缩、伤口愈合延迟)
E.诱发或加重心血管疾病(高血压和动脉粥样硬化)
F.诱发或加重精神疾病(精神病或癫痫病
(1)肾上腺皮质功能亢进症
(2)抗菌药不能控制的感染
(3)病毒感染(麻疹、水痘)
(4)活动性消化性溃疡、角膜溃疡
(5)新近胃肠吻合术、骨折、创伤修复期
(6)糖尿病、高血压
(7)有严重的精神病和癫痫病史者
(8)孕妇
用法与疗程:
1.大剂量冲击疗法
——用于急性、重度、危及生命的疾病的抢救。
严重感染、中毒性休克及各种休克。
氢化可的松静滴,首剂200-300mg,疗程3-5天
2.一般剂量长期疗法
结缔组织病、肾病综合征和顽固性支气管哮喘
泼尼松10-30mg口服,显效后逐渐减量直至最小维持量,疗程6-12个月。
3.小剂量替代疗法
垂体前叶功能减退、肾上腺皮质次全切除术后及原发性、继发性肾上腺皮质功能不全。
一般维持量,口服 可的松12.5-25mg/d
氢化可的松10-20mg/d
糖皮质激素分泌的昼夜规律:
基于糖皮质激素分泌的昼夜规律的维持量用法:
1) 每日晨给药法:即每晨7-8时一次给药,用短时间作用的可的松、氢化可的松等;
2) 隔日晨给药法:即每隔一日,早晨7-8时给药一次。此法应当用中效的泼尼松、泼尼松龙,而不用长
效的糖皮质激素,以免引起对下丘脑-垂体-肾上腺轴的抑制。
在长时间使用糖皮质激素治疗过程中,遇下列情况之一者,应撤去或停用糖皮质激素:
1) 维持量已减至正常基础需要量
2) 因治疗效果差,不宜再用糖皮质激素,应改药者;
3) 因严重副作用或并发症,难以继续用药者。
隔日疗法
将一日或两日的总药量在隔日早晨一次给予
长期疗法,适合于病情较轻或慢性病者,用泼尼松、泼尼松龙。
分泌高峰:每日上午8-10时
分泌低潮:午夜12时