main
- 格式:pdf
- 大小:851.99 KB
- 文档页数:15

main 方法首先,让我们来看一下 main 方法的基本语法。
在Java中,main 方法是程序的入口点,它的语法格式如下:```java。
public class Main {。
public static void main(String[] args) {。
// 在这里编写你的程序代码。
}。
}。
```。
在这段代码中,我们定义了一个名为 Main 的类,并在其中定义了一个名为main 的方法。
该方法被声明为 public(公共的),static(静态的)和 void(无返回值)。
它接受一个类型为 String 数组的参数 args。
在 main 方法中,我们可以编写我们的程序代码,以实现我们想要的功能。
接下来,让我们来看一下 main 方法的作用。
作为程序的入口,main 方法是程序开始执行的地方。
当我们运行一个 Java 程序时,虚拟机会自动查找并执行名为main 的方法。
因此,我们可以将 main 方法看作是程序的起点,所有的程序逻辑都将从这里开始执行。
除了作为程序的入口,main 方法还可以接受命令行参数。
在上面的语法中,我们可以看到 main 方法接受一个类型为 String 数组的参数 args。
这些参数可以在程序运行时从命令行传入,我们可以根据这些参数来定制程序的行为。
在实际应用中,我们经常会用到 main 方法来执行一些初始化操作,比如初始化变量、加载配置文件等。
此外,我们还可以在 main 方法中调用其他方法,实现程序的逻辑功能。
总之,main 方法是程序的核心,它承担着程序执行的重要任务。
在使用 main 方法时,我们需要注意一些细节。
首先,main 方法必须被声明为public 和 static,这是因为虚拟机需要通过这个方法来启动程序。
其次,main 方法的参数类型必须是 String 数组,这是因为命令行参数都以字符串的形式传入。
最后,main 方法没有返回值,它的返回类型被声明为 void。

main方法中入参用法
在Java中,`main`方法是程序的入口点。
它接受一个字符串数组作为参数,这个数组代表命令行参数。
这些命令行参数允许你在运行程序时传递信息给程序。
以下是一个简单的例子:
```java
public class Main {
public static void main(String[] args) {
// 获取第一个命令行参数
String firstArg = args[0];
("第一个命令行参数是: " + firstArg);
// 获取所有命令行参数
for (String arg : args) {
(arg);
}
}
}
```
在这个例子中,我们通过`args[0]`获取第一个命令行参数,并通过一个for-each循环打印所有命令行参数。
如果你从命令行运行这个程序,像这样:
```bash
java Main arg1 arg2 arg3
```
那么输出将是:
```makefile
第一个命令行参数是: arg1
arg1
arg2
arg3
```
请注意,`args`是一个字符串数组,因此你可以像操作任何其他数组一样操作它。
例如,你可以使用``来获取命令行参数的数量,或者使用`args[i]`来获取特定索引的参数(请注意,索引是从0开始的)。

main()方法声明中各部分的含义在Java语言中,main()方法是一个特殊的方法,它是程序的起点。
当我们执行一个Java程序时,程序会从main()方法开始执行,这也是程序的入口。
main()方法的声明包括以下几个部分:1. public:表示该方法是公开的,可以被其他类访问。
Java程序必须含有一个公开的main()方法,作为程序的入口。
2. static:表示该方法为静态方法。
静态方法可以直接通过类名调用,而无需创建该类的对象。
3. void:表示该方法没有返回值。
main()方法被执行后,并不返回执行结果。
4. main:方法名。
main()方法是Java程序的入口,它的名称必须为main。
5. (String[] args):方法参数。
main()方法可以接受一个String数组作为参数,这个参数通常用于接收命令行参数。
下面对main()方法的各部分进行详细解释:1. public修饰符:public是一个访问修饰符,表示该方法是公开的,可以被其他类访问。
如果main()方法没有被public修饰符修饰,则只能在同一个包内的类中访问。
通常情况下,main()方法需要被public修饰符修饰,以便可以从命令行执行。
2. static修饰符:static是一个关键字,表示该方法是静态方法。
静态方法可以直接通过类名调用,而无需创建该类的对象。
main()方法通常被定义为静态方法,以便可以从命令行执行。
静态方法可以在被定义的类加载时就被调用,而不需要实例化类对象。
3. void关键字:void是一个关键字,用于表示该方法没有返回值。
main()方法被执行后,并不返回执行结果。
因为main()方法是程序的入口点,程序执行后并不需要返回结果,因此它的返回类型被定义为void。
4. main方法名:main()方法是一种约定俗成的命名规范,表示Java程序的入口。
Java程序在执行时,会从main()方法开始执行。
一、main函数的参数我们经常用的main函数都是不带参数的。
因此main 后的括号都是空括号。
实际上,main函数可以带参数,这个参数可以认为是main函数的形式参数。
C语言规定main函数的参数只能有两个,习惯上这两个参数写为argc和argv。
因此,main函数的函数头可写为:main (argc,argv)C语言还规定argc(第一个形参)必须是整型变量,argv( 第二个形参)必须是指向字符串的指针数组。
加上形参说明后,main函数的函数头应写为:main (argc,argv)int argv;char *argv[];或写成:main (int argc,char *argv[])由于main函数不能被其它函数调用,因此不可能在程序内部取得实际值。
那么,在何处把实参值赋予main函数的形参呢? 实际上,main函数的参数值是从操作系统命令行上获得的。
当我们要运行一个可执行文件时,在DOS提示符下键入文件名,再输入实际参数即可把这些实参传送到main的形参中去。
DOS提示符下命令行的一般形式为:C:\>可执行文件名参数参数……; 但是应该特别注意的是,main 的两个形参和命令行中的参数在位置上不是一一对应的。
因为,main的形参只有二个,而命令行中的参数个数原则上未加限制。
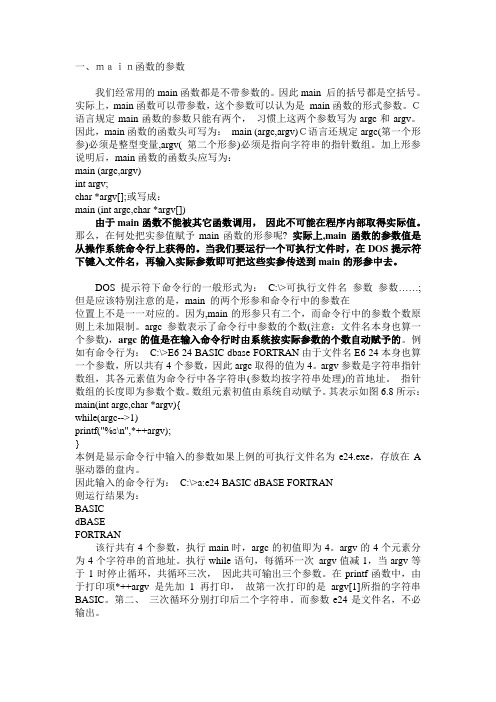
argc参数表示了命令行中参数的个数(注意:文件名本身也算一个参数),argc的值是在输入命令行时由系统按实际参数的个数自动赋予的。
例如有命令行为:C:\>E6 24 BASIC dbase FORTRAN由于文件名E6 24本身也算一个参数,所以共有4个参数,因此argc取得的值为4。
argv参数是字符串指针数组,其各元素值为命令行中各字符串(参数均按字符串处理)的首地址。
指针数组的长度即为参数个数。
数组元素初值由系统自动赋予。
其表示如图6.8所示:main(int argc,char *argv){while(argc-->1)printf("%s\n",*++argv);}本例是显示命令行中输入的参数如果上例的可执行文件名为e24.exe,存放在A 驱动器的盘内。

main的最高级
“main”这个词在英语中并没有比较级和最高级的形式,因为它通常被用作形容词来描述事物的主要或最重要的特征。
然而,如果我们想要表达“main”的某种程度上的增强或比较,我们可以使用其他词汇或短语来达到类似的效果。
如果我们想要表达“更加主要的”或“最主要的”,我们可以使用“more main”或“the most main”,但这些表达并不常见,因为“main”本身已经具有强调的含义。
更常见的做法是使用其他相关的词汇或短语来表达这种比较或强调,例如:
•“More important”或“the most important”来强调某事物的重要性。
•“Primary”或“primary objective”来描述主要的目标或重点。
•“Chief”或“chief concern”来表示主要的关注点或问题。
总之,虽然“main”没有明确的比较级和最高级形式,但我们可以通过使用其他相关的词汇或短语来表达类似的意义。

main 怎么读
“Main”是一个英文单词,发音为英[meɪn],美[meɪn]。
它主要有名词和形容词两种词性,含义丰富多样。
作为名词时,“main”通常指“主要部分”或“主干”,是整体中最为重要或显著的部分。
例如,在河流中,“main river”指的是河流的主干流,是河流系统中最为重要和显著的部分。
而作为形容词时,“main”则用来描述某物或某事是“主要的”、“最重要的”或“首要的”。
例如,“main idea”表示文章或谈话中的中心思想或主要观点;“main entrance”指的是建筑物的主要入口,是人们通常进出的地方。
在日常生活和工作中,“main”是一个非常常用的单词。
我们可以说“main road”来指代主要的道路,可以说“main point”来强调某个关键点,还可以说“main reason”来解释某个现象或决策的主要原因。
总之,“main”是一个简单但非常实用的单词,通过掌握其发音和基本释义,我们能够更好地理解和运用它,丰富我们的语言表达。
main的用法总结大全(学习版)编制人:__________________审核人:__________________审批人:__________________编制学校:__________________编制时间:____年____月____日序言下载提示:该文档是本店铺精心编制而成的,希望大家下载后,能够帮助大家解决实际问题。
文档下载后可定制修改,请根据实际需要进行调整和使用,谢谢!并且,本店铺为大家提供各种类型的经典范文,如英语单词、英语语法、英语听力、英语知识点、语文知识点、文言文、数学公式、数学知识点、作文大全、其他资料等等,想了解不同范文格式和写法,敬请关注!Download tips: This document is carefully compiled by this editor.I hope that after you download it, it can help you solve practical problems. The document can be customized and modified after downloading, please adjust and use it according to actual needs, thank you!In addition, this shop provides various types of classic sample essays, such as English words, English grammar, English listening, English knowledge points, Chinese knowledge points, classical Chinese, mathematical formulas, mathematics knowledge points, composition books, other materials, etc. Learn about the different formats and writing styles of sample essays, so stay tuned!main的用法总结大全main的意思main的简明意思adj. 主要的;最重要的n. 干线;总管道;[pl](水、煤、电)供应系统;大海英式发音 [meɪn] 美式发音 [meɪn]main的详细意思在英语中,main不仅具有上述意思,还有更详尽的用法,main 作形容词 adj. 时具有主要的;全力的,尽力的;最重要的,重要的;有力的;完全的,充分的;尽量的;相当大的;关键的,压轴的;主导的;相近的,相接的;辽阔的等意思,main作名词 n. 时具有干线,输电干线;总管道,污水总管道,主管道;主要部分;体力,力量;要点;大陆,本土;总管;大海,海洋;水源,煤气源,电源;供应系统;下水道系统;美因河(德国南部河流)等意思,main作副词 adv. 时具有非常,极端等意思,main作动词 v. 时具有把注射进静脉;把…路加宽,把…加宽为大路等意思,main的具体用法用作形容词 adj.main的基本意思是“主要的”“最重要的”,指某事或某物是整体中最主要或最明显的,或在大小、潜力或重要性方面优于同类事物的。
C语言中main的含义简介在C语言中,`m ai n`是一个特殊的函数,是程序执行的起点和入口。
本文将深入探讨`mai n`函数的含义,以及它在C语言程序中的作用。
`main`函数的定义与声明在C语言中,`m ai n`函数的定义和声明如下所示:i n tm ai n(vo id){//执行程序的代码r e tu rn0;}`main`函数的参数无参数形式`m ai n`函数的无参数形式声明如下:i n tm ai n(vo id)这表示`ma in`函数不接收任何参数。
带参数形式`m ai n`函数的带参数形式声明如下:i n tm ai n(in ta rg c,c h ar*a rg v[])其中,`ar gc`表示命令行参数的个数,`a rg v`是一个指向字符串数组的指针,每个字符串表示一个命令行参数。
程序入口与起点在执行C语言程序时,操作系统会首先调用`ma in`函数作为程序的入口和起点。
`ma in`函数是程序与操作系统之间的桥梁,通过`ma in`函数,程序开始执行并产生相应的结果。
`main`函数的返回值`m ai n`函数的返回值是一个整数,表示程序的终止状态。
根据惯例,返回值为0表示程序正常终止,而非零值则表示程序异常终止,可以用于表达程序的执行结果。
`main`函数的执行过程`m ai n`函数的执行过程可以分为三个阶段:初始化阶段、执行阶段和清理阶段。
初始化阶段在初始化阶段,操作系统会完成一些必要的准备工作,例如为程序分配内存空间、加载库函数等。
执行阶段在执行阶段,程序会按照`m ai n`函数中编写的代码逐行执行,实现程序的功能和逻辑。
清理阶段在执行阶段结束后,操作系统会清理程序运行所占据的内存空间,释放系统资源。
`main`函数的常见用法执行简单程序`m ai n`函数可以用于执行简单的程序,例如打印"H el lo,W o rl d!"等。
#i nc lu de<s td io.h>i n tm ai n(vo id){p r in tf("He ll o,Wor l d!\n");r e tu rn0;}处理命令行参数通过带参数形式的`m a in`函数,我们可以处理命令行参数,实现程序的灵活性和可配置性。
main函数的返回值
在C和C++编程中,main函数是程序的入口点。
这个函数可以返回一个整数值,这个值通常被操作系统用来判断程序是否成功地执行了。
一般来说,如果main函数成功地执行了,那么它应该返回0。
这是一个约定俗成的规则,虽然操作系统实际上不会对返回值做任何处理(除了将其视为程序是否成功运行的标志)。
如果main函数返回一个非零值,通常表示程序遇到了某种错误。
这个值可以被操作系统或其他调用这个程序的代码作为错误代码进行处理。
例如:
```c
int main() {
// 程序代码
return 0; // 成功执行,返回0
}
```
或者:
```c
int main() {
// 程序代码
return 1; // 遇到错误,返回非零值
}
```
需要注意的是,返回值的范围在不同的系统和编译器中可能会有所不同。
在某些系统中,返回值可能只有8位,所以非零值的范围是1-255。
在其他系统中,返回值可能是32位或64位,那么非零值的范围就会更大。
c语⾔中main函数⽤法及知识点总结1、main函数是C程序的⼊⼝函数,即程序的执⾏从main函数开始,其他函数的调动也直接或间接地在main函数中调⽤。
2、main函数的返回值⽤于解释程序的退出状态。
若返回0,则表⽰程序正常退出。
返回其他数字的含义由系统决定。
通常返回⾮零代表程序异常退出。
实例#include <stdio.h>#include <string.h>int main(int argc, char **argv) {int i = 0;printf("The program name is %s\n", argv[0]);printf("The command line has %d argument: \n", argvc - 1);for (i = 1; i < argc; i++) {printf("%s ", argv[i]);}return 0;}知识点扩充:每⼀C程序都必须有⼀main()函数,可以根据⾃⼰的爱好把它放在程序的某个地⽅。
有些程序员把它放在最前⾯,⽽另⼀些程序员把它放在最后⾯,⽆论放在哪个地⽅,以下⼏点说明都是适合的。
在Turbo C2.0启动过程中,传递main()函数三个参数:argc,argv和env。
* argc:整数,为传给main()的命令⾏参数个数。
* argv:字符串数组。
char* argv[],我们可以看出,argv的类型是char* [],即是⼀个指向字符数组的指针,所以我们还可以写作:char** argv。
在DOS 3.X版本中,argv[0]为程序运⾏的全路径名;对DOS 3.0以下的版本,argv[0]为空串("")。
argv[1]为在DOS命令⾏中执⾏程序名后的第⼀个字符串;argv[2]为执⾏程序名后的第⼆个字符串;...argv[argc]为NULL。
ARTICLE Generalized Arterial Calcification of Infancyand Pseudoxanthoma Elasticum Can Be Causedby Mutations in Either ENPP1or ABCC6Yvonne Nitschke,1,27Genevie`ve Baujat,2,27Ulrike Botschen,1Tanja Wittkampf,1Marcel du Moulin,1 Jacqueline Stella,1Martine Le Merrer,2Genevie`ve Guest,3Karen Lambot,4Marie-Frederique Tazarourte-Pinturier,5Nicolas Chassaing,6,7Olivier Roche,8Ilse Feenstra,9Karen Loechner,10Charu Deshpande,11Samuel J.Garber,12Rashmi Chikarmane,13Beat Steinmann,14 Tatevik Shahinyan,15Loreto Martorell,16Justin Davies,17Wendy E.Smith,18Stephen G.Kahler,19 Mignon McCulloch,20Elizabeth Wraige,21Lourdes Loidi,22Wolfgang Ho¨hne,23Ludovic Martin,24 Smaı¨l Hadj-Rabia,25Robert Terkeltaub,26and Frank Rutsch1,*Spontaneous pathologic arterial calcifications in childhood can occur in generalized arterial calcification of infancy(GACI)or in pseu-doxanthoma elasticum(PXE).GACI is associated with biallelic mutations in ENPP1in the majority of cases,whereas mutations in ABCC6are known to cause PXE.However,the genetic basis in subsets of both disease phenotypes remains elusive.We hypothesized that GACI and PXE are in a closely related spectrum of disease.We used a standardized questionnaire to retrospectively evaluate the phenotype of92probands with a clinical history of GACI.We obtained the ENPP1genotype by conventional sequencing.In those patients with less than two disease-causing ENPP1mutations,we sequenced ABCC6.We observed that three GACI patients who carried biallelic ENPP1mutations developed typical signs of PXE between5and8years of age;these signs included angioid streaks and pseu-doxanthomatous skin lesions.In28patients,no disease-causing ENPP1mutation was found.In14of these patients,we detected path-ogenic ABCC6mutations(biallelic mutations in eight patients,monoallelic mutations in six patients).Thus,ABCC6mutations account for a significant subset of GACI patients,and ENPP1mutations can also be associated with PXE lesions in school-aged children.Based on the considerable overlap of genotype and phenotype of GACI and PXE,both entities appear to reflect two ends of a clinical spectrum of ectopic calcification and other organ pathologies,rather than two distinct disorders.ABCC6and ENPP1mutations might lead to alter-ations of the same physiological pathways in tissues beyond the artery.IntroductionGeneralized arterial calcification of infancy(GACI[MIM 208000])is a rare autosomal-recessive disorder character-ized by calcification of the internal elastic lamina,fibrotic myointimal proliferation of muscular arteries,and resul-tant arterial stenosis.1Affected patients suffer from severe congestive cardiac failure,hypertension,and myocardial ischemia.In the past,few patients survived the neonatal period,2–4whereas more recently,patients treated with bisphosphonates have experienced a more favorable out-come.5,6Radiological studies reveal diffuse vascular and1Department of General Pediatrics,Mu¨nster University Children’s Hospital,Albert-Schweitzer-Campus1,Gbde.A1,D-48149Mu¨nster,Germany; 2Department of Genetics,Centre de reference des maladies osseuses constitutionnelles,Necker Hospital,Universite´Paris Descartes,149rue de Se`vres, 75743Paris cedex15,France;3Nephrology Unit,Necker Hospital,Universite´Paris Descartes,149rue de Se`vres,75743Paris cedex15,Paris,France; 4Department of Radiology,Necker Hospital,Universite´Paris Descartes,149rue de Se`vres,75743Paris cedex15,Paris,France;5Pediatrics Unit,Centre Hos-pitalier de Montreuil,56Boulevard de la Boissiere,93100Montreuil,France;6Department of Medical Genetics,CHU Toulouse,F31400Toulouse,France; 7EA-4555,Toulouse III Paul-Sabatier University,F31400Toulouse,France;8Department of Ophtalmology,Centre de Re´fe´rence des Maladies Rares en Oph-talmologie,Necker Hospital,Universite´Paris Descartes,149rue de Se`vres,75743Paris cedex15,Paris,France;9Department of Human Genetics,Radboud University Nijmegen Medical Centre,Geert Grooteplein10,6525GA Nijmegen,The Netherlands;10NC Pediatric Osteoporosis Clinic,Pediatric Endocrine Unit,University of North Carolina Chapel Hill,3341Medical Biomolecular Research Building CB#7039103,Mason Farm Road,NC27599,USA; 11Department of Clinical Genetics,Guy’s and St.Thomas’NHS Foundation Trust,7thfloor,Borough Wing,Guy’s Hospital,Great Maze Pond,London SE19RT,UK;12Division of Neonatology,Department of Pediatrics,Children’s Hospital of Philadelphia,University of Pennsylvania School of Medicine, 34th St.and Civic Center Blvd.,Philadelphia,PA19104,USA;13Institute of Medical Genetics,St.Peter’s University Hospital,254Easton Avenue,New Brunswick,NJ08901,USA;14Division of Metabolism and Molecular Pediatrics,University Children’s Hospital,Steinwiesstrasse75,CH-8032Zurich, Switzerland;15Arabkir Joint Medical Centre,Mamikonyants St.,30Building,0014Yerevan,Armenia;16Department of Genetics,Hospital Sant Joan de De´u,Calle de San Juan de Dios2,08950Esplugues de Llobrega,Barcelona,Spain;17University of Wales College of Medicine Heath Park,CF44XN Cardiff,UK;18Division of Genetics,Maine Pediatric Specialty Group,Barbara Bush Children’s Hospital,Maine Medical Center,887Congress Street, Suite320,Portland,ME04102,USA;19Division of Medical Genetics,Arkansas Children’s Hospital,Slot512-22,One Children’s Way,Little Rock, AR72202,USA;20Department of Pediatric Nephrology,Evelina Children’s Hospital,Guy’s and St.Thomas’NHS Foundation Trust,St.Thomas’Hospital, Westminster Bridge Road,London SE17EH,UK;21Department of Pediatric Neurology,Evelina Children’s Hospital,Guy’s and St.Thomas’NHS Foundation Trust,St.Thomas’Hospital,Westminster Bridge Road,London SE17EH,UK;22Unidad de Medicina Molecular,Fundacio´n Pu´blica Galega de Medicina Xeno´mica,Hospital Clı´nico Universitario,Choupana SN,E-15706Santiago de Compostela,Spain;23Department of Biochemistry,Charite´University Medicine,Oudenarder Strasse16,Haus A,Aufgang9,13347Berlin,Germany;24Department of Dermatology,Angers University Hospital,4rue Larrey, F-49933Angers cedex9,France;25Department of Dermatology,Centre de reference des Maladies Ge´ne´tiques a`Expression Cutane´e,Necker Hospital, Universite´Paris V Descartes,49rue de Se`vres,75743Paris cedex15,France;26Department of Rheumatology,Allergy and Immunology,VA Medical Center, University of California San Diego,3350La Jolla Village Drive,San Diego,CA92161,USA27These authors contributed equally to this work*Correspondence:rutschf@ukmuenster.deDOI10.1016/j.ajhg.2011.11.020.Ó2012by The American Society of Human Genetics.All rights reserved.periarticular soft-tissue calcifications.Some patients may also develop hypophosphatemic rickets,a presentation associated with a milder phenotype.6–10Inactivating muta-tions in ENPP1(MIM173335),encoding ecto-nucleotide pyrophosphatase/phosphodiesterase1(NPP1),have been identified as the underlying defect in about75%of the cases of GACI.6,11NPP1generates PP i,a major physiologic inhibitor of calcification that exerts its effects by,among other things,inhibiting hydroxyapatite crystal growth.12 Moreover,effects of NPP1on adenosine metabolism also could modulate arterial calcification.13 Pseudoxanthoma elasticum(PXE[MIM264800])wasfirst described in1881,14and its prevalence is estimated to be1 in25,000.15It is known as an autosomal-recessive disorder, but autosomal-dominant inheritance has been proposed in rare PXE cases.16,17PXE is characterized by ectopic mineral-ization and fragmentation of elasticfibers of connective tissues,including skin,vascular walls,and the eyes.18The main dermatological features are yellowish papules or pla-ques of coalesced papules on the neck and inflexural areas that have typical histological abnormalities.The presence of fragmented basophilic elasticfibers in the upper and middle reticular dermis and calcifications of elasticfibers are characteristic histologicfindings of this disorder. Cardiovascular involvement includes decreased peripheral pulses,vascular calcifications,and endocardial thick-ening.19–21Angioid streaks seen in fundoscopy reflect disruption of the so-called Bruch’s membrane,which consists of elasticfibers between the pigmented retinal epithelium and the choroidea.22Additionally,PXE can manifest with gastrointestinal haemorrhage and abnormal tissue mineralization in different organs,including the liver,kidneys,spleen,breast,and testes.23,24Classic PXE results from mutations in the ABCC6 (ATP-binding cassette subfamily C number6)gene(MIM 603234).25The ABCC6-transported substrate or substrates, which modulate arterial calcification and other phenotypic changes of PXE,are not known,and hepatic abnormalities that have effects on calcification-regulating plasma proteins such as fetuin have been suggested to at least partially mediate pathogenesis of PXE.26In this context, PXE-likefindings have also been found in patients with b-thalassemia(MIM613985)27and have been found to accompany deficiency of the vitamin-K-dependent clotting factors.28In2007,mutations in GGCX(MIM137167)were reported in several cases with PXE-like cutaneous lesions and deficiency of vitamin-K-dependent clotting factors.29 GGCX encodes a gamma-glutamyl carboxylase essential for activation of hepatic coagulation factors and of the ectopic calcification inhibitor matrix gla protein(MGP).29 Most recently,our group reported on a family with two sons;the older son presented with PXE and mutations in ABCC6,and the younger one died of GACI at the age of 15months.30Mutation analysis was not performed in the younger brother.However,retrospective analysis of the living family members was negative for mutations in ENPP1.On the basis of these observations,we hypothe-sized that GACI and PXE might be more closely related than previously thought.Here we report on three patients with GACI caused by biallelic mutations in ENPP1.These patients developed typical signs of PXE in childhood.We also present the results of the clinical and mutational analysis of14patients who have GACI but do not have disease-causing mutations in ENPP1and in whom ABCC6mutations were identified.Patients and MethodsPatientsFor this study,we used clinical data and DNA material from our international GACI registry.6This registry is an ongoing system-atic collection of phenotypic and genotypic data from patients with the clinical diagnosis of GACI and currently contains data from92GACI patients of85unrelated families(Figure S1,avail-able online).Diagnosis of GACI was based on the presence of cardiovascular symptoms associated with evidence of arterial calci-fications with or without stenoses as seen on X-ray or ultrasound in infancy,periarticular calcifications detected on radiological studies,or typical histologicalfindings.Patient history and clinical data were gathered through a standardized questionnaire,which was sent to the referring physician or geneticist.All patients in the registry were screened for mutations in ENPP1as part of the routine diagnostic analysis.Clinical and mutational data on a subset of55of these patients have been published before.6The clinical course of GACI is exem-plified by a case report on patients1,2,and8(Supplemental Data). When available,clinical data on signs of PXE were evaluated(for detailed case reports,see Supplemental Data).PXE diagnostic criteria included characteristic skin involvement,characteristic histopathologic features of lesional skin,31and angioid streaks of the retina.32The study protocol was approved by the Mu¨nster University Hospital Ethical Committee and other participating institutional peer-review human-subject committees.The parents of all subjects involved in this study gave informed written consent. Mutation AnalysisGenomic DNA was extracted from whole blood.When blood was unavailable,patient DNA was extracted from formalin-fixed tissue blocks.DNA from92patients of85unrelated families with clinically proven GACI was subjected to mutation analysis of ENPP1.Poly-merase chain reaction(PCR)with24primer pairs was used for amplification of the25exons and theflanking splice sites in ENPP1(RefSeq accession number NG_008206.1),as previously described.7Primer sequences are available upon request.In those patients with less than two biallelic coding-region or splice-site mutations in ENPP1,ABCC6(RefSeq accession number NG_007558.2)mutation analysis was performed with previously described ABCC6-specific primers so that all31exons and the exon/intron boundaries would be amplified.33,34Previously re-ported sequences35were used for synthesis of intron-derived primers specific for PCR amplification of ABCC6exons1–9.We investigated splice-site mutations and aberrant splicing by sequencing the ABCC6cDNA.Primer sequences are available on request.PCR products were directly sequenced bidirectionally withan ABI3730Genetic Analyzer and a BigDye Terminatorv3.1Cycle Sequencing Kit according to the protocol provided by the manufacturer (Applied Biosystems,Foster City,California,USA).Mutations were compared with the dbSNP ,HGMD,and ENSEMBL polymorphism databases.The recurrent large deletion of exons 23–29(c.2996_4208del)of ABCC6was screened by PCR with a previously described set of nested primers.36For segregation analysis,parental DNA was analyzed with the aim of excluding the occurrence of two mutations on the same allele.Multiplex Ligation-Dependent Probe AmplificationThe specific synthetic probe set for multiplex ligation-dependent probe amplification (MLPA)analysis of ABCC6,covering 23of the 31exons,was used (SALSA MLPA kit P092ABCC6,MRC-Holland,Amsterdam,The Netherlands).The construction of the kit precludes the generation of signals from the ABCC6pseudo-genes.MLPA reactions were performed with the reagents and recommendations of the ABCC6MLPA reagent kit and with 100ng of genomic DNA.The PCR products were separated by capillary electrophoresis on an ABI 3730Genetic Analyzer (Applied Biosystems,Foster City,CA,USA).The Peak ScannerTM Software v1.0(Applied Biosystems,Foster City,CA,USA)was used for peak identification and fragment sizing.Data analysis was carried out according to the manufacturer’s recommenda-tions.All samples were tested in duplicate.Splice-Site PredictionFor analysis of the splice-site mutation of patient #2,there was no RNA available.Thus,the software NetGene2v.2.4(Center for Bio-logical Sequence Analysis,Technical University of Denmark DTU)was used for in silico prediction of aberrant splicing.ResultsCumulatively,we identified biallelic pathogenic mutations in ENPP1in 62of 92affected patients (data not shown).Three of these patients developed typical signs of PXE in childhood (Table 1).Of the remaining 30GACI patients,28patients showed neither splice-site nor coding-region mutations in ENPP1,and 14patients were found to carry ABCC6mutations (Figure S1).Two unrelated probands of our cohort carried only one pathogenic ENPP1mutation on one allele.Genomic DNA derived from these probands was also subjected to ABCC6mutation analysis.None of these probands carried a potentially pathogenic mutation in ABCC6.Clinical Features of GACI Patients Who Have PXE and Carry Mutations in ENPP1Of the 92patients of our study cohort,three unrelated patients,two boys and one girl (patients 1,2,and 3)who had generalized arterial calcification of infancy (Table 1;for detailed case reports on patients 1and 2see Supple-mental Data )presented with clinical features of PXE in later childhood.In the first male patient (patient 1),who was born to consanguineous parents and presented with extensive calcifications of large and medium-sized arteries,the diagnosis of GACI was already established in the neonatal period and led to early bisphosphonateT a b l e 1.C l i n i c a l a n d M u t a t i o n a lD a t a o f P a t i e n t s w i t h G A C I a n d P XE P h e n o t y p e C a r r y i n g M u t a t i o n s i n E N P P 1F a m i l y P a t i e n t S e xG e o -g r a p h i c O r i g i n C o n s a n -g u i n i t y A f f e c t e d /N o n a f f e c t e d S i b l i n g s (G A C I )A r t e r i a l C a l c i -fic a t i o n sP e r i -a r t i c u l a r C a l c i -fic a t i o n sC a r d i o -v a s c u l a r C o m p l i -c a t i o n sA d d i t i o n a l A b n o r m a l i t i e sA g e a t D a t a C o l l e c t i o n P X E F e a t u r e sB i s p h o s -p h o n a t e T h e r a p yH i s t o l o g y D N A C h a n g e i n E N P P 1A m i n o A c i d C h a n g e i n E N P P 1R e f .11m F r a n c ey e s 1/0a ,c h i p s ,a n k l e s ,w r i s t s ,s h o u l d e r sh y p e r -t e n s i o n i n n e o n a t a l p e r i o df u s i o n o f v e r t e b r a l b o d i e s C 3-C 5,h y p o p h o s p h a t e m i c r i c k e t s ,s t a p e d o v e s t i b u l a r a n k y l o s i s l e a d i ng t oh e a ri n g l o s s ,a n g i o -m a t o u s s k i n l e s i o n s9y e a r s p s e u d o -x a n t h o m a t o u s l e s i o n s o n t h e n e c kc l od r o n a te p .o .c a l c i fic a t i o n of e l a s t i c fib e r s i n t h e d e r m i s o f p s e u d o -x a n t h o m a t o u s l e s i o nc .[1612G >C ];[1612G >C ]p .[A s p 538H i s ];[A s p 538H i s ]22f F r a n c e n o 1/0e n d o -c a r d i u m ,a ,p p a i n f u l w r i s t c a l c i fic a t i o n s i n t h e n e o n a t a l p e r i o d h y p o p h o s -p h a t e m i c r i c k e t s S t a p e d o v e s t i b u l a r a n k y l o s i s l e a d i n g t o h e a r i n g l o s s5y e a r sa n g i o i d s t r e a k s i n t h e B r u c h ’s m e mb r a n e n oc .[795þ1G >A ];[1756G >A ]p .[a l t e r e d s p l i c i n g ];[G l y 586A r g ]33mG r e a tB r i t a i nn o 2/1a n ol e f t v e n t r i c u l a r h y p e r t r o p h y ,a r t e r i a l h y p e r -t e n s i o n‘‘m i d d l e a o r t i c s y n d r o m e ,’’p r o g r e s s i v e h e a r i n g l o s s9y e a r sp s e u d o -x a n t h o m a t o u sp e r i u m b i l i c a l a n d c e r v i c a l l e s i o n sn o c a l c i fic a t i o n o f e l a s t i c fib e r s i n t h e d e r m i s o f p s e u d o -x a n t h o m a t o u s l e s i o nc .[783C >G ];[878_879de l A A ]p .[T y r 261*];[L y s 293f s *4]8A b b r e v i a t i o n s a r e a s f o l l o w s :A ,a o r t a ;c ,c o r o n a r y a r t e r i e s ;d ,d i v e r s e a r t e r i e s ;p ,p u l m o n a r y a r t e r y ;a n d r ,r e n a l a r t e r i e s .treatment.At the age of 8yr,this patient developed pseu-doxanthomatous skin lesions,which were proven histo-logically to reflect calcifications of elastic fibers in the dermis,as are typical for PXE (Figure 1).Also,the mother of this proband showed yellowish papules.The female patient (patient 2),who presented with painful periarticu-lar calcifications in infancy,showed angioid retinal streaks suggestive of PXE at the age of 5yr.At that time,wide-spread calcifications of the heart and the proximal great arteries were noted on computed tomography.She had not received bisphosphonate therapy.Interestingly,both patients developed hypophosphatemic rickets as well as deafness due to stapedo-vestibular ankylosis.Additionally,both patients showed capillary angiomas on different parts of the skin (Supplemental Data ),which had not been described previously in patients with GACI or PXE.The third patient (patient 3)presented with left ventricular hypertrophy in the neonatal period.At 14months of age,arterial hypertension was noted,and angiography revealed severe arterial stenosis of the celiac artery,the superior mesenteric artery,renal arteries,and both internal and external carotid arteries.Mutation analysis of ENPP1in this boy was performed when the mother had a second pregnancy,which resulted in a stillbirth at 31weeks of gestation;the fetus showed fetal hydrops and aortic root calcification,suggestive of GACI.A detailed case report on the two siblings was recently published.8Most recently,starting at the age of 8yr,the surviving boy developed pseu-doxanthomatous skin lesions around his umbilicus and on his neck,and these were histologically proven to be typical PXE lesions.Mutations in ENPP1in Three Patients with GACI and PXEThe homozygous missense mutation c.1612G >C (p.Asp538His)was detected in exon 16of ENPP1in patient 1.Both parents were shown to be heterozygous carriers of the mutation.This amino acid change affects a conserved residue located within the catalytic domain of NPP1and is therefore predicted to affect enzyme activity (Table 2upper panel,Figure 2).In patient 2,the mutation c.795þ1G >A was detected on the maternal allele,and c.1756G >A (p.Gly586Arg)was detected on the paternal allele.The mutation c.795þ1G >A is located at the exon-intron boundary of exon 7and is predicted to affect a splice donor site (NetGene2v.2.4,Center for Biological Sequence Anal-ysis,Technical University of Denmark DTU)and therefore to lead to abnormal splicing.The mutation c.1756G >A (p.Gly586Arg)leads to a change of the conserved polar amino acid glycine to the polar charged amino acid argi-nine in the catalytic domain of the NPP1protein and thus most likely affects NPP1enzymatic activity.Patient 3was compound heterozygous for the two nonsense muta-tions c.783C >G (p.Tyr261X)in exon 7and c.878_879delAA (p.Lys293fsX4)in exon 8,8both of which are pre-dicted to lead to a severely truncated protein.Sequence analysis of the exons and flanking intronic regions of ABCC6in each of the three patients did not show any aber-ration.Clinical Features of GACI Patients Carrying ABCC6Mutations30patients with GACI and with less than two coding regions or splice-site mutations in ENPP1were screened for mutations in ABCC6.Mutations in ABCC6were de-tected in 14of these patients (Table 3).Homozygous muta-tions were found in two patients,compound heterozygous mutations in six,and in six patients only one mutation could be identified.37,38The eight patients carrying biallelic ABCC6mutations were of different ethnic backgrounds and presented in early infancy with widespread calcifications of the aorta and medium-sized arteries,including coronary arteries and renal arteries (Table 3).Four of these patients (patients 4,5,7,and 11)were severely affected and died of myocar-dial infarction and cardiac failure within the first three months of life.Autopsy performed in one patient (patient 4)revealed the typical histological features consisting of calcification of the internal elastic lamina,myointimal proliferation in the coronary arteries,and consequent severe arterial stenosis (Figure 3D).Interestingly,in one patient,generalized arterial stenoses were demonstrated without any evidence of arterial calcification (patient #5).This patient died of myocardial infarction at the age of 8weeks.Another patient (patient 8)presented with periar-ticular calcifications of the shoulder joints and the hip joints (Figures 3A and 3B).This patient also developed diffuse cerebral white matter disease leading to cystic ence-phalomalacia,which is quite uncommon inGACI.Figure 1.Manifestation of GACI and PXE Associated with ENPP1MutationsPatient 1,who suffered from generalized arterial calcification in infancy.X-ray showing extensive peri-articular calcification of the right shoulder (A)and abdominal CT scan showing a ring-like calcification of the abdominal aorta (B,arrow)in the neonatal period.Yellowish papules,located on the frontal part of the neck when the patient was 9years old,were suggestive of PXE (C),which was histologically proven by the presence of dermal calcium deposits associated with elastic fibers (D)(Von Kossa staining,310).In six additional patients we were able to detect only one potentially pathogenic mutation in ABCC6.One of these patients was the recipient twin of a twin-to-twin transfusion syndrome.He died of myocardial ischemia at the age of5months,whereas the donor twin survived.6,7,39,40The other patients had a more favorable clinical course;for example,one female proband who pre-sented with GACI41developed epilepsy at the age of20yr and was31yr old at the time of this study(Table3,patient 14).Information on dermal elastorrhexis or retinal changes on this patient was not available.Mutations in ABCC6in Patients with GACIThirteen different mutations in ABCC6were identified in patients with GACI.These included six missense mutations (c.1064T>G[p.Leu355Arg], c.1171A>G[p.Arg391Gly], c.1769C>T[p.Ser590Phe], c.3340C>T[p.Arg1114His], c.3662G>A[p.Arg1221His,and c.3940C>T[p.Arg1314Trp]), two nonsense mutations(c.1552C>T[p.Arg518*], c.3421C>T[p.Arg1141*]),one small deletion(c.3105_3107 delCTT[p.Phe1036del]),one small insertion leading to a frameshift(c.450_451insC[p.Ala151Argfs*45),two splice-site mutations(c.2787þ1G>T[p.Arg929fs*1], c.3736-1G>A[p.Ala1246fs*26]),and one large deletion (c.2996_4208del[p.Ile1000Trpfs*60]).Of these,11muta-tions have been previously described as disease-causing in patients with PXE(p.Leu355Arg,25,42p.Arg391 Gly,25,42,43p.Arg1114His,25,42,44p.Arg1221His,42,45p.Arg 1314Trp,25,34,42,46p.Arg518*,25,42p.Arg1141*,25,33,34,47 p.Phe1036del,25p.Arg929fs*1,25,42p.Ala1246fs*26,25,42,47Table2.Functional Consequences of Mutations in ENPP1and ABCC6Exon DNA Change Amino Acid Change Patient Functional Consequences References ENPP17 c.783C>G p.Tyr261*3truncated protein6,8,11 IVS7 c.795þ1G>A Loss of splice site2predicted loss of donor splice site,aberrantsplicingnew8 c.878_879delAA p.Lys293fs*43truncated protein6,8,1116 c.1612G>C p.Asp538His1affects conserved aa in catalytic domain,negatively charged aa changedto neutral/positively charged aanew18 c.1756G>A p.Gly586Arg2affects conserved aa in catalytic domain,polar aa changed to polar,positivelycharged aanew ABCC64 c.450_451insC p.Ala151Argfs*455truncated protein new9 c.1064T>G p.Leu355Arg14affects conserved aa in transmembranedomain,non-polar aa changed into polar,positively charged aa25,429 c.1171A>G p.Arg391Gly9,15,16affects conserved aa in intracellulardomain,polar,posively chargedaa changed into polar aa25,42,4312 c.1552C>T p.Arg518*6,10truncated protein25,4213 c.1769C>T p.Ser590Phe12affects aa in transmembrane domain,conserved in bovine,chicken and fungusnewIVS21 c.2787þ1G>T p.Arg929fs*14truncated protein25,4223 c.3105_3107delCTT a p.Phe1036del6loss of one conserved aa in intracellulardomain 25(c.3106delTTT p.Phe1036del)24 c.3340C>T p.Arg1114Cys13affects conserved aa in intracellulardomain,polar charged aa changedinto non-polar aa,possible formationof incorrect disulfide bonds25,42,4424 c.3421C>T p.Arg1141*11truncated protein25,33,34,4726 c.3662G>A p.Arg1221His7affects conserved aa in intracellular domain42,45IVS26 c.3736-1G>A p.Ala1246fs*264truncated protein25,42,4728 c.3940C>T p.Arg1314Trp5,8,17affects conserved aa in ATP-binding domain25,34,42,4623-29 c.2996_4208del p.Ile1000Trpfs*609truncated protein36a The mutation p.Phe1036del is already known,25although the known DNA change is c.3106_3108delTTT.The DNA change c.3105_3107delCTT leading to the same amino acid change,p.Phe1036del,is not described in the literature.and p.Ile1000Trpfs*6036).Only four mutations,namely p.Arg391Gly,p.Arg518*,p.Arg1141*,and p.Arg1314Trp,were found in more than one patient;all other mutations occurred only once.All mutations that led to amino acid exchanges involved amino acids located within cytosolic or transmembrane domains of ABCC6,reflecting the potential importance of these regions in terms of protein function.Localization of mutations in the ABCC6protein is visualized in Figure 4.The missense mutations p.Leu355Arg,p.Arg391Gly,p.Ser590Phe,p.Arg1114His,and p.Arg1221His are pre-dicted to result in alterations of the ABCC6conformation.Some of these alterations might affect the function more than others,and the effect might be particularly strong at conserved positions.For the second ATP-binding domain,where the mutation p.Arg1314Trp of the current study is located,it is known that mutations are able to completely abolish the transport activity of the ABCC6protein.48The missense mutations cause amino acid substitutions that lead to the introduction of a residue with different phys-ical-chemical properties (Table 2,lower panel).Multiple sequence alignment of ABCC6across species showed changes in highly conserved amino acids,exceptfor the mutation p.Ser590Phe,which is conserved in bovines,chicks,and fungus (Figure 5).The nonsense mutations (p.Arg518*and p.Arg1141*),the frameshift mutation (p.Ala151Argfs*45),and the large deletion of exons 23–29(p.Ile1000Trpfs*60)are predicted to result in the production of a truncated protein.These polypeptides are devoid at least of an intact second ATP-binding domain and are therefore predicted to be nonfunctional.It should be noted that the mutation p.Phe1036del has been described before in PXE patients as being caused by the DNA change c.3106_3108delTTT.25The patient presented here,however,carried the mutation c.3105_3107delCTT,which led to the same in-frame dele-tion of phenylalanine at position 1036.The splice-site mutations c.2787þ1G >T and c.3736-1G >A have been predicted to alter splicing.34,47To deter-mine the effect of these two mutations on the protein,we sequenced cDNA from our patients.Both splice-site muta-tions lead to a new splice site and aberrant splicing (Supple-mental Data ).This causes a frameshift and results in an abnormal and truncated protein.Two disease-associated ABCC6mutations are presented here.The DNA change c.1769C >T (p.Ser590Phe)was found in a heterozygous state in a patient with only one mutation.It is located in the transmembrane domain of the protein.The DNA change c.450_451insC (p.Ala151Argfs*45)was also found in a heterozygous state in one patient.This small insertion leads to a frame-shift and to generation of an abnormal and truncated protein.These two mutations were not present on 200alleles from 100individuals from corresponding ethnic backgrounds and could therefore be excluded as polymorphisms.Type and severity of the ABCC6muta-tions identified in our cohort of GACI patients did not differ from those previously found to be associated with PXE.DiscussionPXE and GACI have been considered to be two distinct enti-ties in the past and have been primarily linked to ABCC6and ENPP1,respectively.In the current study,we showed that biallelic mutations in ABCC6account for a substantial number of typical GACI cases,which involve typical disease manifestations such as widespread arterial calcifica-tions,arterial stenosis,peri-articular calcifications,and,occasionally,hypophosphatemic rickets (patient 12).Addi-tionally,in six patients with clinical GACI,we detected mono-allelic ABCC6mutations.These patients,from a clin-ical point of view,do not significantly differ from the patients carrying biallelic ABCC6mutations.Although MLPA failed to detect large deletions on the other allele in these patients,it is possible that the ABCC6mutation on the allele in trans in these patients was missed by our exon-based sequencing approach,e.g.,mutations in regula-tory untranslated regions of ABCC6could be present,2Transmembranedomaindomains catalytic domainNuclease-likedomainFigure 2.Schematic Representation of Human NPP1Shows Mutations Identified in GACI Patients with PXE Features in the Current StudyAmino acid positions in functional domains according to spP22413(SwissProt)¼Q5T9R6(UniProtKB/TREMBL)for human NPP1.。