椎弓根钉置入技术讲座PPT课件
- 格式:ppt
- 大小:863.50 KB
- 文档页数:59

手术技术:钉道的徒手胸椎椎弓根螺钉置入技术 - 丁香园
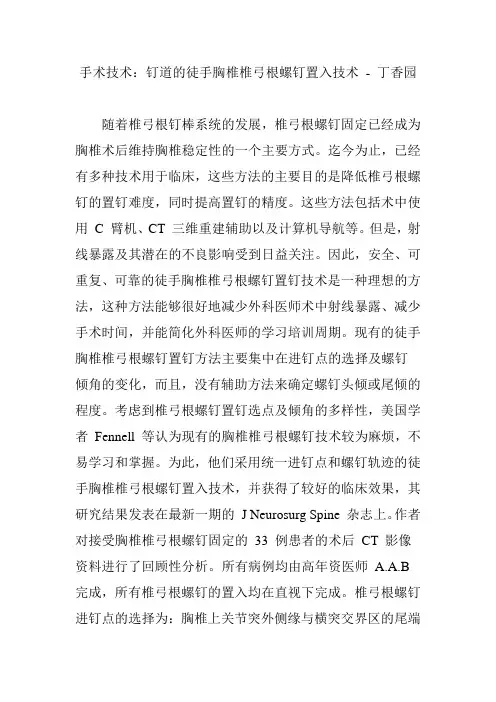
随着椎弓根钉棒系统的发展,椎弓根螺钉固定已经成为胸椎术后维持胸椎稳定性的一个主要方式。迄今为止,已经有多种技术用于临床,这些方法的主要目的是降低椎弓根螺钉的置钉难度,同时提高置钉的精度。这些方法包括术中使用 C 臂机、CT 三维重建辅助以及计算机导航等。但是,射线暴露及其潜在的不良影响受到日益关注。因此,安全、可重复、可靠的徒手胸椎椎弓根螺钉置钉技术是一种理想的方法,这种方法能够很好地减少外科医师术中射线暴露、减少手术时间,并能简化外科医师的学习培训周期。现有的徒手胸椎椎弓根螺钉置钉方法主要集中在进钉点的选择及螺钉倾角的变化,而且,没有辅助方法来确定螺钉头倾或尾倾的程度。考虑到椎弓根螺钉置钉选点及倾角的多样性,美国学者 Fennell 等认为现有的胸椎椎弓根螺钉技术较为麻烦,不易学习和掌握。为此,他们采用统一进钉点和螺钉轨迹的徒手胸椎椎弓根螺钉置入技术,并获得了较好的临床效果,其研究结果发表在最新一期的 J Neurosurg Spine 杂志上。作者对接受胸椎椎弓根螺钉固定的 33 例患者的术后 CT 影像资料进行了回顾性分析。所有病例均由高年资医师 A.A.B
完成,所有椎弓根螺钉的置入均在直视下完成。椎弓根螺钉进钉点的选择为:胸椎上关节突外侧缘与横突交界区的尾端约 3mm 处(图 1.),矢状面螺钉轨迹 / 方向与椎体所在平面的生理曲线垂直,沿这一通道将螺钉直接置入。图 1. 进钉点:胸椎上关节突外侧缘与横突交界区的尾端约 3mm
处。显露成功后,以高速磨钻去除标识好的进钉点处骨皮质,参照术前 CT 扫描结果,以专用开路器沿椎弓根方向开路,直至适当深度,以头端为球形的椎弓根探子确认通道安全后,选择合适规格的椎弓根螺钉置入。术中无需使用椎弓根标记(markers),先进行穿刺进针 10-15mm、而后探查、最后确定螺钉通道的常用做法是没有必要的,而且会增加手术时间。作者仅在手术定位及置钉完成后进行正侧位透视,所有患者术后均行 CT 扫描,并对所有位置满意的螺钉的平均内倾角进行测量,并由 2 名医师独立进行评估,螺钉位于椎弓根外侧超过 25% 视为穿破椎弓根壁。结果共有 219 枚胸椎椎弓根螺钉得到评估,置钉准确率为 96%。本研究需要植入胸椎椎弓根螺钉的脊柱疾病包括:创伤(61%)、感染(12%)、肿瘤(18%)、畸形(9%)(见图 2)。螺钉位置分布如下:T1:23 枚(10.5%)、T2: 27 枚(12.3%)、T3:11 枚(5%)、T4: 13 枚(5.9%)、T5: 10 枚(4.6%)、T6: 8 枚(3.7%)、T7: 15 枚(6.8%)、T8: 23 枚(10.5%)、T9: 23 枚(10.5%)、T10: 25 枚(11.4%)、T11: 19 枚(8.7%)、T12: 22

中国组织工程研究与临床康复第J2眷第22 2008—05—27出版 Journal ofClinical Rehabilitative Tissue Engineering Research May 27,2008 Vo1.12,No.22 Cli,l c口f cf,le
ADStl aCt BACKGRoUND:The characteristics of cervical anatomy and pedicle screw.operational specification.and individual screw implantation are the key factors of a successful implantation treatment. OBJECTIVE:This study was designed to investigate the cervical pedicle screw and host response as well as the recovery of spinal nerve functions during the surgery and follow—uD period of cervical spine fracture—dislocation. DESIGN:A case analysis. SETTING:Department of Orthopaedics,General Hospital of Shenyang Military Area Command of Chinese PLA,Shenyang, Lianning Province,China. PARTICIPANTS:A total of 4 l patients with cervical spine fracture—dislocation,who have complete follow。up data,were admiued to the Department of Orthopaedics.General Hospital of Shenyang Military Area Command of Chinese PLA between February 2OH02 and February 2006.Of the included patients.1 8 were complicated by spinal cord injury(according to Frankel classification system,6were gradedasA,l asB,4asC.and 7 asD. M THoDS:Forty—one patients with cervical spine fracture—dislocation were treated by implanting a screw through the cervical pedicle and fixing it.Prior to surgery,all patients were subjected to X—ray,CT and MRI examinations.According to measurements.each cervical pedicle screw was individually implanted.The entire surgery was accomplished by Xiang Liang—bi,chief physician,whose qualification corresponds to the responsibilities. MAIN oUTCoM MEASURES:Material and host response during and after screw implantation as well as in the follow—uD period.Recovery of spinal nerve function after screw implantation. RESUI S:AU patients were followed uD for 6—12 months and all incisions were healed primarily.Material and host response during the process of screw implantation:A total of 2l8 screws were implanted.After initial implantation.12 screws were loosened.and such a phenomenon disappeared in ll screws by adjusting inserting point and inserting direction or/and increasing screw diameter or length.The remaining l screw was stabilized by increasing the fixed segments.After drilling.poles of l0 screws bled much and treated by hemostasis.C1—2 venous plexus hemorrhage was caused in 3 patients and stopped by compression.and Apofix internal fixation was used in l of 3 patients due to unclear surgical visual field. Material and host response after surgery and during the follow—up:A total of 2l8 screws were inserted.Of the 2l8 screws. 196 were in correct position.and 22 were deviated to diferent degrees.Deviation of l screw caused injury to nerve root and that of another screw led to injury to blood vesse1.Thirty—eight patients acquired satisfactory reduction and bone union.Three patients presented with symptoms of nerve root irritation due to incomplete reduction in the old fracture—dislocation.Among the 3 patients,1 was subjected to anterior approach due to screw removed,and neither injury to vertebral artery,spinal cord, and nerve root nor internal fixation destroy was found in any other patients.Recovery of spinal nerve function after implantation:Among the 18 patients complicated with spinal cord injury,6 patients,who were assessed as grade A spinal cord injury,did not exhibit improvement in spinal cord function.while the remaining l2 presented with l or 2 grades of improvement. CoNCLUSIoN:There is a lower probability for biocompatibility reaction,and spinal nerve function recovers better after implantation of cervical pedicle screw.So implantation of a cervical pedicle screw system is an effective and relatively safe method for treatment of cervical spine fracture—dislocation.

让你秒懂的骶椎椎⼸根钉固定技术详解
作者:雷伟医学博⼠,脊柱外科专家,教授、主任医师,博⼠研究⽣导师,西京⾻科医院副院长,西外科学教研室常务副主任。出处:《脊柱内固定应⽤指南》权限:《⾻今中外》已获得作者对本⽂的转载授权。
⼀、骶椎椎⼸根的相关数据(图1ABCD)
骶⾻椎⼸根和骶⾻翼处的⾻量相对较少,因为骶⾻为⽚状⾻,骶⾻椎⼸根螺钉可以从标准的前
内侧⽅向拧⼊骶⾻体或⾻岬部,或者从前外⽅进⼊骶⾻翼。对于任何外侧骶⾻螺钉的放置,最
重要的是注意防⽌发⽣医源性损伤神经⾎管结构。S1椎⼸根⾼度平均值:左侧
(2.26±0.27)cm,右侧(2.22±0.21)cm,应⽤的螺钉直径达0.7cm,螺钉亦不易穿出椎⼸根
上、下缘。骶⾻前⽅的神经⾎管和脏器解剖的特点决定S1螺钉放置时可能的最⼤危险性是损伤
腰骶神经⼲、髂内静脉和骶髂关节,S1螺钉放置的区域以前内侧最为安全。除⾮特殊情况,⼀
般不进⾏S1节段的固定。
⼆、骶椎椎⼸根螺钉进钉点的定位(图2)
对于S1由于解剖上的变异,螺钉可以从不同的点、不同的⽅向进⼊,主要决定于器械和⾻骼的
质量。在骶椎上不同的位置⾻密度有着较⼤的差异,软⾻下⾻最硬,⽽骶⾻侧块相当疏松,有
时甚⾄是空的。
⼀般的说,骶椎椎⼸根的进钉点为上关节的外缘切线与上关节下缘⽔平线的交点。
三、骶椎椎⼸根螺钉的进钉⾓度(图3)
植⼊⾓度为内倾25°或者在骶⾻翼外侧成⾓35°。俯卧位时向头侧偏斜25°-30°,瞄向骶⾻岬,
进⼊软⾻下⾻。四、骶椎椎⼸根螺钉的进钉深度:⼀般情况下为30-35mm深度。
五、骶椎椎⼸根螺钉的直径选择:最常选⽤的螺钉直径为6.5-7.0mm。
六、⼿术操作步骤(具体操作步骤及注意事项见腰椎椎⼸根钉技术)
1、确认进钉点
2、预备螺钉钉道
a.去除⽪质⾻(图4)
b.钻孔(图5)
c.定位(图6)
3、螺钉的植⼊(图7)
七、标准椎⼸根螺钉的影像学(图8ABCDEF)

1/8 椎弓根钉使用指南
一颈椎
1、解剖特点
2、进针点
C2:枢椎椎板上缘水平线下5mm与椎管内侧缘外7mm垂直线交点;
C3-6:侧块背面中上1/4水平线与中外1/4垂直线交点;
C7:侧块背面中上1/4水平线与中点垂直线交点稍偏上。
3、角度 2/8 C2:矢状面内倾30度,水平面上倾20度;
C3-6:矢状面内倾40-45度,水平面与终板平行;
C7:矢状面内倾40-45度,水平面与终板平行。
4、螺钉直径(mm):3.5皮质骨螺钉
5、进钉深度(mm):18-20,进钉不超过80%
6、经验总结
(1)颈椎椎弓根钉植入方法有盲打法、椎弓根直视探查法和计算机导航植入法。但现行的进钉方法均存在不同程度的穿钉失败率,即使直视下穿钉也有相当的穿出率,考虑到个体差异和畸形,单纯依靠解剖标志定位的方法不能完全解决。螺钉植入的安全问题,应特别引起注意。术者应根据对颈椎解剖及椎弓根钉技术的掌握情况来选择相应的方法。
(2)在C3-C6节段内使用侧块螺钉固定较椎弓根螺钉固定简单安全。 3/8 (3)工具不能穿破椎弓根外壁,否则会损伤邻近的神经和血管。
(4)进钉的角度应随着椎弓角度的变化而变化。
(5)应避免穿透椎体前面的皮质骨。
(6)术中透视能准确地定位椎体及椎间隙,准确地植入螺钉,防止拧入椎间隙及椎管。
二胸椎
1、解剖特点
2、进针点:上关节突外缘垂线与横突中点水平线交点。
3、角度
矢状面角度:T1:25度;T2:20度;T3:15度;T4-9:10度;T10:5度;T11-12:0度;
水平面角度:与终板平行。
4、螺钉直径(mm):T1-5:3.5-4;T6-10:4-5;T11-12:5.5-6.5
5、进钉深度(mm):35-40(椎弓根到椎体前缘40-42,进钉不超过80%) 4/8
三腰椎
1、解剖特点
2、进针点
方法一:上关节突外缘垂线与横突中点水平线交点;
方法二:人字嵴进钉法,以副突嵴和峡部嵴为定位标志。 横突缺如、过大、过小、关节突关节增生、内聚,既往手术中已被咬除,会影5/8 响进钉点的定位,人字嵴进钉法,位置恒定,容易显露及辨认。