中心静脉穿刺图解
- 格式:doc
- 大小:168.00 KB
- 文档页数:8
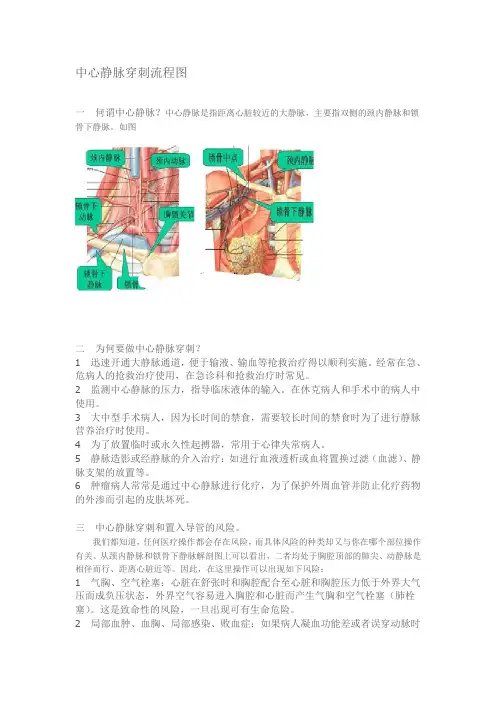
中心静脉穿刺流程图分享一何谓中心静脉?中心静脉是指距离心脏较近的大静脉,主要指双侧的颈内静脉和锁骨下静脉。
如图二为何要做中心静脉穿刺?1迅速开通大静脉通道,便于输液、输血等抢救治疗得以顺利实施。
经常在急、危病人的抢救治疗使用,在急诊科和抢救治疗时常见。
2监测中心静脉的压力,指导临床液体的输入。
在休克病人和手术中的病人中使用。
3大中型手术病人,因为长时间的禁食,需要较长时间的禁食时为了进行静脉营养治疗时使用。
4为了放置临时或永久性起搏器,常用于心律失常病人。
5静脉造影或经静脉的介入治疗:如进行血液透析或血将置换过滤(血滤)、静脉支架的放置等。
6肿瘤病人常常是通过中心静脉进行化疗,为了保护外周血管并防止化疗药物的外渗而引起的皮肤坏死。
三中心静脉穿刺和置入导管的风险。
我们都知道,任何医疗操作都会存在风险,而具体风险的种类却又与你在哪个部位操作有关。
从颈内静脉和锁骨下静脉解剖图上可以看出,二者均处于胸腔顶部的肺尖、动静脉是相伴而行、距离心脏近等。
因此,在这里操作可以出现如下风险:1气胸、空气栓塞:心脏在舒张时和胸腔配合至心脏和胸腔压力低于外界大气压而成负压状态,外界空气容易进入胸腔和心脏而产生气胸和空气栓塞(肺栓塞)。
这是致命性的风险,一旦出现可有生命危险。
2局部血肿、血胸、局部感染、败血症:如果病人凝血功能差或者误穿动脉时会因为动脉压力高或血液不容易凝固进入胸腔或皮下而形成血胸和皮下血肿,时间长了会出现感染导致败血症的发生。
3穿刺不成功:因为局部解剖变异或体位不恰当或选择穿刺点和进针角度不合适可以造成穿刺不成功,而多次多点多角度穿刺又可以增加上述风险出现的机率。
故不主张以增加上述风险出现的机率为代价行多次多点多角度穿刺,有时换一个人穿刺时反而更容易成功而且不以增加风险的出现机率。
通过上述的介绍,我们可以了解到,中心静脉穿刺术前同意书的内容就是这么来的。
由此,也可以类推其他医疗操作的风险由来。
我相信:没有任何一个医生会有意夸大穿刺等操作的风险,而且也没有哪一个医生有这份闲心杜撰一份危言耸听的文书来吓唬病人和家属四哪些医生应该掌握中心静脉穿刺?中心静脉穿刺是一项非常重要的专科性穿刺,尤其在遇到急救病人时,这根中心静脉导管将会成为一根救命的导管。

ICU深静脉插管技术详解——简单易懂,告别国内教科书分享首次分享者:ルヽ羔羊医生已被分享4232次评论(0)复制链接分享转载举报ICU深静脉插管技术详解——简单易懂,告别国内教科书来自美国旧金山加利福尼亚大学的培训资料,彻底告别国内不专业的文献以及教科书。
深静脉插管主要适应症:. 给予药物-很多药物(升压药、化疗药、全胃肠外营养等)因为具有刺激性,不适合经浅静脉导管给药,故需要经中心静脉导管给药。
. 血液动力学检测-检测中心静脉压;. 血浆过滤、血浆置换术、血液透析、持续静脉-静脉血液滤过。
次要适应症:. 浅静脉通路困难;. 容量复苏。
绝对禁忌症:∙Cellulitis over the vein site (must pick alternative location) ∙Peripheral IV access is adequate for the clinical needs of the patient∙Operator inexperience (unless supervised by an experienced practitioner)∙Uncooperative or combative patients∙Infection over catheter site∙Clot in the selected vein相对禁忌症:部位选择:你的病人能够忍受相应的并发症吗?解剖:The IJ vein travels with the carotid artery; the vein typically lies anterolateral to the carotid artery. It runs under the medial portion of the upper part of the sternocleidomastoid muscle and travels under the apex of the triangle formed by the sternal and clavicular heads of the sternocleidomastoid muscle and the clavicle.easily found in almostevery patient, and acatheter in thesubclavian vein is morecomfortable for thepatient than one placed inthe internal jugularvein.As the subclavian veincrosses behind the firstrib, it lies posterior tothe medial third of the clavicle, and has a diameter of 1-2 cm. At this point, the subclavian artery lies superior and posterior to the vein. As these vessels continue laterally, they both drop caudally to enter the axillary region. The right side is often preferred for line insertions as the dome of the pleura of the lung may extend above the first rib on the left, but rarely extends this far on the right. Insertion on the right also avoids the risk of damage to the thoracic duct on the left.ConsentAlways obtain consent prior to the procedure.Be sure to inform the patient of the reason for the procedure, the proposed benefits, its major risks and the potential management of these complications (including insertion of a chest tube, surgery or cardioversion). It is also best to walk the patient through the stepsof the procedure to minimize their anxiety.Step-by-Step Procedures GuideEquipmentBefore you begin, you should be familiar with the kit. One should gather all needed materials before starting the procedure. In addition to a central venous access kit, you will need the following supplies:∙Insertion Checklist∙Sterile gloves, gown, cap, mask with face fluid shield for each member of the insertion team∙Chloraprep (if extra desired, provided in the kit)∙Large sterile drape∙Lidocaine 1% (in the kit, but it doesn’t hurt to have some extra just in case)∙Tegaderm∙Central line kit (cordis, triple or quad lumen kit)Before starting, be sure all of your materials are within reach and familiarize yourself with the kit you will be using.* Bold items are IHI guidelines and have been proven to reduce central line infections.Complications1.Venous Hematoma2.Arterial Dilitation3.Hemothorax4.Bleeding - arterial puncutre or injury: approximately 3% with theinternal jugular approach5.Pneumothorax: approximately 3% with the subclavian approach6.Infection: Insertion site infection, thrombophlebitis,bacteremia, sepsis, cellulitis7.Embolization of clot, air, guidewire or catheter8.Arrhythmia9.Phlebitis or thrombosis of veins10.Pericardial tamponade11.Injury to neighboring nerves (phrenic, recurrent laryngeal)12.DeathEvaluator Checklist for safe central line placement - Click Here Preventing Complications of Central Venous Catheterization- Click Here∙Coagulopathy and thrombocytopenia (relative goal plateletsare >50k and INR >1.5, but linescan be placed if these goals are not reached depending on the case) ∙Injury or previous surgery to superior vena cava (e.g., superior vena cava syndrome)∙Complications that can belife threatening (i.e pneumothorax or bleed). Do not put asubclavian line in a patient with a coagulopathy or in patient with severe parenchymal lungdisease and respiratory failure with little respiratory reserve) ∙Coagulopathy and thrombocytopenia (relative goal plateletsare >50k and INR >1.5, but linescan be placed if these goals are not reached depending on the case) ∙Injury or previous surgery to superior vena cava (e.g., superior vena cava syndrome)∙Complications that can belife threatening (i.e pneumothorax or bleed). Do not put asubclavian line in a patient with a coagulopathy or in patient with severe parenchymal lungdisease and respiratory failure with little respiratory reserve)。