心内护理查房模板
- 格式:pptx
- 大小:7.83 MB
- 文档页数:10
心血管内科护理查房查房时间:2022.10.12 查房地点:病房患者: 住院号:202231450 性别:男年龄:61岁民族:汉族入院时间:2022年10月08日11:05婚姻状况:已婚记录时间:2022年10月08日13:28职业:退(离)休人员病史叙述者:患者本人主持人:今天心内科全体实习生进行一次护理查房,目的使实习生掌握高血压冠心病患者的护理既往史:患者既往身体状况一般,否认肝炎、疟疾史、结核史,否认高血压史,冠心病史,否认糖尿病史、脑血管病、精神病史,否认手术史,外伤史、输血史,否认食物及药物过敏史,预防接种史不详。
主诉:反复胸痛1+年,复发20天初步诊断:1.胸痛2.冠状动脉粥样硬化3.睡眠障碍现病史:患者入院前1+年无诱出现胸痛,位于心前区,持续1-2小时,呈隐痛不适,当时于华西医院住院行冠脉造影结果提示左前降支开口狭窄20%,余未见狭窄,当时心脏彩超提示室间隔增厚,出院后建议患者服用降脂药、阿司匹林肠溶片,患者出院后未坚持规律服用。
患者因寻求胸痛原因先到成都市第二人民医院及重庆中医医院治疗,上述,症状有缓解。
入院前20天,患者再次出现心前区胸痛不适,持续1-2小时,呈隐痛不适,且后出现左肩背部疼痛、剑突下疼痛,左下肢大腿疼痛不适,无明显活动后气促不是适,无心悸、黑朦,无咳嗽、咳痰,无夜间阵发性呼吸困难,无下肢水肿,现为进一步治疗来我科住院。
患者自患病以来精神状态一般,食欲食量一般,睡眠情况较差,每天睡眠时间不到2小时,体重无明显变化,大便正常,小便正常。
个人史:生于四川省资阳市安岳县,久居本地生活环境一般否认嗜酒史、吸烟史,职业:退(离)休人员,工作条件良好,无工业毒物、粉尘、放射性物质接触史,无血吸虫疫水接触史。
无冶游史。
发病前14天内无病例报告社区的旅居史或居住史;发病前14天内无与新型冠状病毒感染的患者或无症状感染者有接触时;发病前是14天未曾接触过自有病例报告社区的发热或,有呼吸道症状的患者;无聚性性发病(2周内小范围内如家庭、办公室、学校班级等场所出现两例以上发热和/或呼吸道症状的病例)。

心内科查房记录模板范文英文回答:Heart Department Ward Round Template.Date: [Date]Patient Name: [Patient Name]MRN: [Medical Record Number]Attending Physician: [Attending Physician]Introduction:Today, I conducted a ward round on [Date] for [Patient Name], who is admitted to the Heart Department under my care. The purpose of this ward round was to assess the patient's current condition, review test results, discuss treatment options, and address any concerns or questionsthe patient may have.Subjective Assessment:During the ward round, I had a detailed conversation with the patient to gather subjective information about their symptoms, medical history, and overall well-being. The patient reported experiencing occasional chest pain, shortness of breath, and fatigue. They also mentioned feeling anxious and worried about their condition. Additionally, the patient shared that they have a family history of heart disease.Objective Assessment:After obtaining subjective information, I proceeded with the objective assessment. I reviewed the patient's vital signs, including blood pressure, heart rate, respiratory rate, and temperature. I also examined the patient's heart sounds, checked for any abnormal murmurs, and assessed their peripheral pulses. Furthermore, I reviewed the results of the patient's recent cardiac tests,including an electrocardiogram (ECG) and echocardiogram.Assessment and Plan:Based on the subjective and objective assessment, I have formulated the following assessment and plan:1. Diagnosis:The patient is diagnosed with coronary artery disease (CAD) based on their symptoms, family history, and abnormal cardiac test results.Further investigations, such as a stress test or coronary angiography, may be required to confirm the diagnosis and assess the severity of the disease.2. Treatment:The patient will be started on a combination of medications, including antiplatelet agents, beta-blockers, and statins, to manage their CAD and reduce the risk ofcardiovascular events.Lifestyle modifications, such as regular exercise, a heart-healthy diet, smoking cessation, and stress management, will be strongly encouraged.3. Follow-up:The patient will be scheduled for regular follow-up appointments to monitor their progress, adjust medications if needed, and address any concerns or questions.Education regarding the signs and symptoms of cardiac emergencies will be provided to the patient and their family members.Conclusion:In conclusion, during today's ward round, I assessed and diagnosed [Patient Name] with coronary artery disease.I have initiated appropriate treatment and lifestyle modifications to manage the condition and reduce the riskof complications. The patient will be closely monitored and provided with necessary education and support. I will continue to follow up with the patient to ensure theirwell-being and address any further needs.中文回答:心内科查房记录模板。

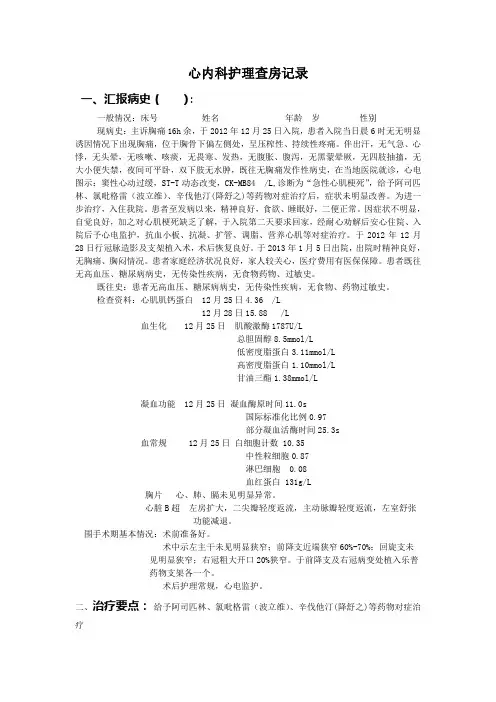
心内科护理查房记录一、汇报病史():一般情况:床号姓名 年龄 岁性别现病史:主诉胸痛16h余,于2012年12月25日入院,患者入院当日晨6时无无明显诱因情况下出现胸痛,位于胸骨下偏左侧处,呈压榨性、持续性疼痛。
伴出汗,无气急、心悸,无头晕,无咳嗽、咳痰,无畏寒、发热,无腹胀、腹泻,无黑蒙晕厥,无四肢抽搐,无大小便失禁,夜间可平卧,双下肢无水肿,既往无胸痛发作性病史,在当地医院就诊,心电图示:窦性心动过缓,ST-T动态改变,CK-MB84 /L,诊断为“急性心肌梗死”,给予阿司匹林、氯吡格雷(波立维)、辛伐他汀(降舒之)等药物对症治疗后,症状未明显改善。
为进一步治疗,入住我院。
患者至发病以来,精神良好,食欲、睡眠好,二便正常。
因症状不明显,自觉良好,加之对心肌梗死缺乏了解,于入院第二天要求回家,经耐心劝解后安心住院、入院后予心电监护,抗血小板、抗凝、扩管、调脂、营养心肌等对症治疗。
于2012年12月28日行冠脉造影及支架植入术,术后恢复良好。
于2013年1月5日出院,出院时精神良好,无胸痛、胸闷情况。
患者家庭经济状况良好,家人较关心,医疗费用有医保保障。
患者既往无高血压、糖尿病病史,无传染性疾病,无食物药物、过敏史。
既往史:患者无高血压、糖尿病病史,无传染性疾病,无食物、药物过敏史。
检查资料:心肌肌钙蛋白 12月25日4.36 /L12月28日15.88 /L血生化 12月25日肌酸激酶1787U/L总胆固醇8.5mmol/L低密度脂蛋白3.11mmol/L高密度脂蛋白1.10mmol/L甘油三酯1.38mmol/L凝血功能 12月25日凝血酶原时间11.0s国际标准化比例0.97部分凝血活酶时间25.3s血常规 12月25日白细胞计数 10.35中性粒细胞0.87淋巴细胞 0.08血红蛋白 131g/L胸片心、肺、膈未见明显异常。
心脏B超左房扩大,二尖瓣轻度返流,主动脉瓣轻度返流,左室舒张功能减退。
心内科护理查房模板范文英文回答:Good morning everyone, it's time for our daily ward round in the cardiology department. Let's start by checking in on our patients and reviewing their progress.Patient 1: Mr. Smith, how are you feeling today? Have you been experiencing any chest pain or shortness of breath?Patient 2: Mrs. Johnson, how is your blood pressure today? Have you been taking your medications as prescribed?Patient 3: Mr. Lee, have you been following your diet and exercise plan? How is your weight and fluid intake?Now let's review the vital signs and lab results for each patient to ensure they are stable and progressing as expected.中文回答:大家早上好,现在是我们心内科的每日查房时间。
让我们开始检查我们的病人,并回顾他们的进展情况。
病人1,史密斯先生,你今天感觉怎么样?你有没有出现胸痛或气短的情况?病人2,约翰逊女士,你今天的血压怎么样?你有按照处方服药吗?病人3,李先生,你有按照饮食和运动计划吗?你的体重和液体摄入情况如何?现在让我们回顾每位病人的生命体征和实验室结果,确保他们的情况稳定,并按预期进展。
心内科护理查房模板范文一、查房时间。
[具体日期],[上午/下午/晚上][具体时间]二、查房地点。
心内科[病房号]病房。
三、参加人员。
1. 护士长:[护士长姓名]2. 责任护士:[责任护士姓名]3. 其他护士:[列出其他参与护士的姓名]四、查房目的。
1. 了解患者病情进展及护理措施的落实情况。
2. 针对患者现存的护理问题进行讨论,制定或调整护理计划。
3. 提高护士对心内科疾病护理的专业知识和技能。
五、病例介绍。
# (一)基本信息。
患者姓名:[患者姓名],性别:[男/女],年龄:[X]岁,住院号:[住院号],床号:[床号]。
# (二)简要病史。
患者因“[主要症状,如心悸、胸闷、胸痛等] [持续时间]”入院。
既往有[列出既往病史,如高血压病史X年、冠心病病史X年等],否认[与疾病相关的特殊病史,如过敏史等]。
患者日常生活习惯为[简单描述患者吸烟、饮酒、运动、饮食等方面的习惯]。
# (三)入院诊断。
1. [主要诊断,如冠心病、不稳定型心绞痛等]2. [其他诊断,如有则列出]# (四)治疗经过。
入院后,医生给予患者[列出主要治疗措施,如抗血小板聚集(阿司匹林、氯吡格雷)、调脂(他汀类药物)、改善心肌供血(硝酸酯类药物)等治疗]。
同时完善了一系列检查,包括[列举检查项目,如心电图、心脏彩超、心肌酶谱等],检查结果显示[简要说明检查结果中的关键信息]。
六、护理评估。
# (一)生命体征。
体温:[体温数值]℃,脉搏:[脉搏数值]次/分,呼吸:[呼吸数值]次/分,血压:[血压数值]mmHg。
# (二)症状评估。
1. 胸痛。
疼痛部位:[描述疼痛具体部位,如心前区、胸骨后等]。
疼痛性质:[如压榨性、闷痛、刺痛等]。
疼痛程度:采用[疼痛评估工具,如数字评分法(NRS)]评估为[疼痛评分数值]。
疼痛发作频率:[多久发作一次],每次持续时间:[具体时长]。
疼痛诱发因素:[如劳累、情绪激动等],缓解因素:[如休息、含服硝酸甘油等]。