抗癌药物急性及亚急性毒性分级标准
- 格式:doc
- 大小:124.50 KB
- 文档页数:4
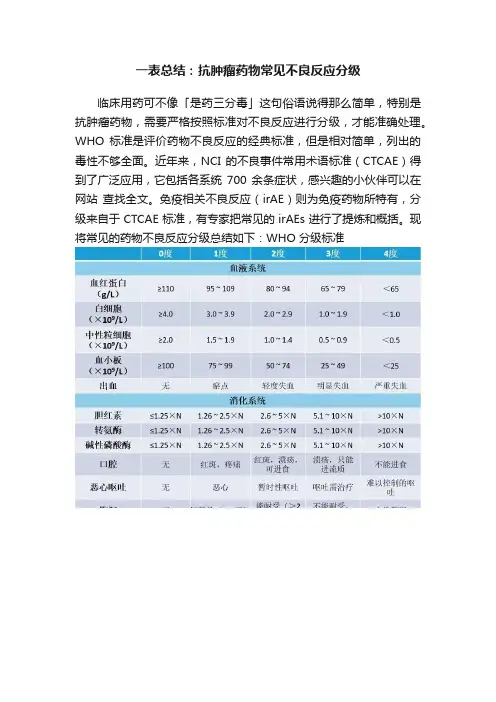
一表总结:抗肿瘤药物常见不良反应分级
临床用药可不像「是药三分毒」这句俗语说得那么简单,特别是抗肿瘤药物,需要严格按照标准对不良反应进行分级,才能准确处理。
WHO 标准是评价药物不良反应的经典标准,但是相对简单,列出的毒性不够全面。
近年来,NCI 的不良事件常用术语标准(CTCAE)得到了广泛应用,它包括各系统700 余条症状,感兴趣的小伙伴可以在网站查找全文。
免疫相关不良反应(irAE)则为免疫药物所特有,分级来自于 CTCAE 标准,有专家把常见的 irAEs 进行了提炼和概括。
现将常见的药物不良反应分级总结如下:WHO 分级标准
CTCAE 标准(4.0 版)
(5 级毒性为死亡,表中未列出)
LLN:正常下限;ULN:正常上限常见免疫相关不良反应。

高危药品的分级在医学领域中,药品的分类和管理是非常重要的一项工作。
其中,高危药品的分级更是至关重要,因为高危药品一旦使用不当,可能会对患者的健康造成重大危害。
因此,根据药品的毒性、副作用以及使用范围等因素,我们将高危药品分为三个等级:A级、B级和C级。
A级高危药品A级高危药品是指具有极高毒性和危险度的药品,误用或过量使用可能导致严重后果甚至危及生命。
这类药品一般用于治疗严重病症或手术中使用,必须在医生的指导下使用。
常见的A级高危药品包括强效止痛药、抗癌药物、麻醉药等。
在使用A级高危药品时,医务人员要格外谨慎,严格按照医嘱和用药要求来进行使用。
B级高危药品B级高危药品相对于A级来说毒性较低,但仍然具有一定的危险性,需要在专业人员的指导下合理使用。
这类药品可能会出现严重的副作用,对患者的健康造成损害。
常见的B级高危药品包括某些抗生素、激素类药物等。
在使用B级高危药品时,患者要注意严格遵守医嘱,避免自行停药或更改用药方案。
C级高危药品C级高危药品是相对安全性较高的一类药品,但在特定条件下使用时仍需谨慎。
这类药品可能会出现较轻的不良反应,但也有可能导致严重后果。
常见的C级高危药品包括一些抗生素、消炎药、镇痛药等。
在使用C级高危药品时,患者应严格按照药品说明书来使用,注意可能出现的不良反应,并及时向医生咨询。
综上所述,对高危药品进行科学合理的分级管理对于保障患者的安全和健康至关重要。
医务人员和患者在使用高危药品时都应当严格遵守相关规定,做到用药安全,最大限度地发挥药品的疗效,确保患者获得最佳治疗效果。
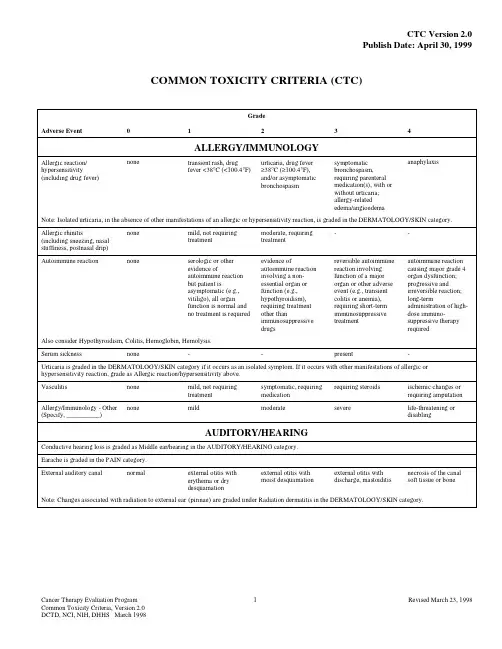
COMMON TOXICITY CRITERIA (CTC)GradeAdverse Event01234ALLERGY/IMMUNOLOGYAllergic reaction/ hypersensitivity (including drug fever)none transient rash, drugfever <38°C (<100.4°F)urticaria, drug fever≥38°C (≥100.4°F),and/or asymptomaticbronchospasmsymptomaticbronchospasm,requiring parenteralmedication(s), with orwithout urticaria;allergy-relatededema/angioedemaanaphylaxisNote: Isolated urticaria, in the absence of other manifestations of an allergic or hypersensitivity reaction, is graded in the DERMATOLOGY/SKIN category.Allergic rhinitis (including sneezing, nasal stuffiness, postnasal drip)none mild, not requiringtreatmentmoderate, requiringtreatment--Autoimmune reaction none serologic or otherevidence ofautoimmune reactionbut patient isasymptomatic (e.g.,vitiligo), all organfunction is normal andno treatment is required evidence ofautoimmune reactioninvolving a non-essential organ orfunction (e.g.,hypothyroidism),requiring treatmentother thanimmunosuppressivedrugsreversible autoimmunereaction involvingfunction of a majororgan or other adverseevent (e.g., transientcolitis or anemia),requiring short-termimmunosuppressivetreatmentautoimmune reactioncausing major grade 4organ dysfunction;progressive andirreversible reaction;long-termadministration of high-dose immuno-suppressive therapyrequiredAlso consider Hypothyroidism, Colitis, Hemoglobin, Hemolysis.Serum sickness none--present-Urticaria is graded in the DERMATOLOGY/SKIN category if it occurs as an isolated symptom. If it occurs with other manifestations of allergic or hypersensitivity reaction, grade as Allergic reaction/hypersensitivity above.Vasculitis none mild, not requiringtreatment symptomatic, requiringmedicationrequiring steroids ischemic changes orrequiring amputationAllergy/Immunology - Other (Specify, __________)none mild moderate severe life-threatening ordisablingAUDITORY/HEARINGConductive hearing loss is graded as Middle ear/hearing in the AUDITORY/HEARING category. Earache is graded in the PAIN category.External auditory canal normal external otitis witherythema or drydesquamation external otitis withmoist desquamationexternal otitis withdischarge, mastoiditisnecrosis of the canalsoft tissue or boneNote: Changes associated with radiation to external ear (pinnae) are graded under Radiation dermatitis in the DERMATOLOGY/SKIN category.Adverse Event01234Inner ear/hearing normal hearing loss onaudiometry only tinnitus or hearing loss,not requiring hearingaid or treatmenttinnitus or hearing loss,correctable with hearingaid or treatmentsevere unilateral orbilateral hearing loss(deafness), notcorrectableMiddle ear/hearing normal serous otitis withoutsubjective decrease inhearing serous otitis or infectionrequiring medicalintervention; subjectivedecrease in hearing;rupture of tympanicmembrane withdischargeotitis with discharge,mastoiditis orconductive hearing lossnecrosis of the canalsoft tissue or boneAuditory/Hearing - Other (Specify, __________)normal mild moderate severe life-threatening ordisablingBLOOD/BONE MARROWBone marrow cellularity normal for age mildly hypocellular or≤25% reduction fromnormal cellularity forage moderately hypocellularor >25 - ≤50%reduction from normalcellularity for age or >2but <4 weeks torecovery of normalbone marrow cellularityseverely hypocellular or>50 - ≤75% reductionin cellularity for age or4 - 6 weeks to recoveryof normal bone marrowcellularityaplasia or >6 weeks torecovery of normalbone marrow cellularityNormal ranges:children (≤18 years)90% cellularityaverageyounger adults (19-59)60 - 70%cellularity averageolder adults (≥60 years)50% cellularityaverageNote: Grade Bone marrow cellularity only for changes related to treatment not disease.CD4 count WNL<LLN - 500/mm3200 - <500/mm350 - <200/mm3<50/mm3 Haptoglobin normal decreased-absent-Hemoglobin (Hgb)WNL<LLN - 10.0 g/dL<LLN - 100 g/L<LLN - 6.2 mmol/L 8.0 - <10.0 g/dL80 - <100 g/L4.9 - <6.2 mmol/L6.5 - <8.0 g/dL65 - <80 g/L4.0 - <4.9 mmol/L<6.5 g/dL<65 g/L<4.0 mmol/LFor leukemia studies or bone marrow infiltrative/ myelophthisic processes, if specified in the protocol.WNL10 - <25% decreasefrom pretreatment25 - <50% decreasefrom pretreatment50 - <75% decreasefrom pretreatment≥75% decrease frompretreatmentHemolysis (e.g., immune hemolytic anemia, drug-related hemolysis, other)none only laboratoryevidence of hemolysis[e.g., direct antiglobulintest (DAT, Coombs’)schistocytes]evidence of red celldestruction and ≥2gmdecrease in hemoglobin,no transfusionrequiring transfusionand/or medicalintervention (e.g.,steroids)catastrophicconsequences ofhemolysis (e.g., renalfailure, hypotension,bronchospasm,emergencysplenectomy)Also consider Haptoglobin, Hemoglobin.Adverse Event01234Leukocytes (total WBC)WNL<LLN - 3.0 x 109 /L<LLN - 3000/mm3≥2.0 - <3.0 x 109 /L≥2000 - <3000/mm3≥1.0 - <2.0 x 109 /L≥1000 - <2000/mm3<1.0 x 109 /L<1000/mm3For BMT studies, if specified in the protocol.WNL≥2.0 - <3.0 X 109/L≥2000 - <3000/mm3≥1.0 - <2.0 x 109 /L≥1000 - <2000/mm3≥0.5 - <1.0 x 109 /L≥500 - <1000/mm3<0.5 x 109 /L<500/mm3For pediatric BMT studies(using age, race and sexnormal values), if specifiedin the protocol.≥75 - <100% LLN≥50 - <75% LLN≥25 - 50% LLN<25% LLNLymphopenia WNL<LLN - 1.0 x 109 /L<LLN - 1000/mm3≥0.5 - <1.0 x 109 /L≥500 - <1000/mm3<0.5 x 109 /L<500/mm3-For pediatric BMT studies(using age, race and sexnormal values), if specifiedin the protocol.≥75 - <100%LLN≥50 - <75%LLN≥25 - <50%LLN<25%LLNNeutrophils/granulocytes (ANC/AGC)WNL≥1.5 - <2.0 x 109 /L≥1500 - <2000/mm3≥1.0 - <1.5 x 109 /L≥1000 - <1500/mm3≥0.5 - <1.0 x 109 /L≥500 - <1000/mm3<0.5 x 109 /L<500/mm3For BMT studies, if specified in the protocol.WNL≥1.0 - <1.5 x 109 /L≥1000 - <1500/mm3≥0.5 - <1.0 x 109 /L≥500 - <1000/mm3≥0.1 - <0.5 x 109 /L≥100 - <500/mm3<0.1 x 109 /L<100/mm3For leukemia studies or bone marrow infiltrative/ myelophthisic process, if specified in the protocol.WNL10 - <25% decreasefrom baseline25 - <50% decreasefrom baseline50 - <75% decreasefrom baseline≥75% decrease frombaselinePlatelets WNL<LLN - 75.0 x 109 /L<LLN - 75,000/mm3≥50.0 - <75.0 x 109 /L≥50,000 - <75,000/mm3≥10.0 - <50.0 x 109 /L≥10,000 - <50,000/mm3<10.0 x 109 /L<10,000/mm3For BMT studies, if specified in the protocol.WNL≥50.0 - <75.0 x 109 /L≥50,000 - <75,000/mm3≥20.0 - <50.0 x 109 /L≥20,000 - <50,000/mm3≥10.0 - <20.0 x 109 /L≥10,000 - <20,000/mm3<10.0 x 109 /L<10,000/mm3For leukemia studies or bone marrow infiltrative/ myelophthisic process, if specified in the protocol.WNL10 - <25% decreasefrom baseline25 - <50% decreasefrom baseline50 - <75% decreasefrom baseline≥75% decrease frombaselineTransfusion: Platelets none--yes platelet transfusions andother measures requiredto improve plateletincrement; platelettransfusionrefractoriness associatedwith life-threateningbleeding. (e.g., HLA orcross matched platelettransfusions)For BMT studies, if specified in the protocol.none 1 platelet transfusion in24 hours2 platelet transfusions in24 hours≥3 platelet transfusionsin 24 hoursplatelet transfusions andother measures requiredto improve plateletincrement; platelettransfusionrefractoriness associatedwith life-threateningbleeding. (e.g., HLA orcross matched platelettransfusions)Also consider Platelets.Adverse Event01234 Transfusion: pRBCs none--yes-For BMT studies, if specified in the protocol.none≤2 u pRBC in 24 hourselective or planned3 u pRBC in 24 hourselective or planned≥4 u pRBC in 24 hours hemorrhage orhemolysis associatedwith life-threateninganemia; medicalintervention required toimprove hemoglobinFor pediatric BMT studies, if specified in the protocol.none≤15mL/kg in 24 hourselective or planned>15 - ≤30mL/kg in 24hours elective orplanned>30mL/kg in 24 hours hemorrhage orhemolysis associatedwith life-threateninganemia; medicalintervention required toimprove hemoglobinAlso consider Hemoglobin.Blood/Bone Marrow - Other (Specify, __________)none mild moderate severe life-threatening ordisabling CARDIOVASCULAR (ARRHYTHMIA)Conduction abnormality/ Atrioventricular heart block none asymptomatic, notrequiring treatment(e.g., Mobitz type Isecond-degree AVblock, Wenckebach)symptomatic, but notrequiring treatmentsymptomatic andrequiring treatment(e.g., Mobitz type IIsecond-degree AVblock, third-degree AVblock)life-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock)Nodal/junctional arrhythmia/dysrhythmia none asymptomatic, notrequiring treatmentsymptomatic, but notrequiring treatmentsymptomatic andrequiring treatmentlife-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock)Palpitations none present---Note: Grade palpitations only in the absence of a documented arrhythmia.Prolonged QTc interval (QTc >0.48 seconds)none asymptomatic, notrequiring treatmentsymptomatic, but notrequiring treatmentsymptomatic andrequiring treatmentlife-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock)Sinus bradycardia none asymptomatic, notrequiring treatment symptomatic, but notrequiring treatmentsymptomatic andrequiring treatmentlife-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock)Sinus tachycardia none asymptomatic, notrequiring treatment symptomatic, but notrequiring treatmentsymptomatic andrequiring treatment ofunderlying cause-Supraventricular arrhythmias (SVT/atrial fibrillation/ flutter)none asymptomatic, notrequiring treatmentsymptomatic, but notrequiring treatmentsymptomatic andrequiring treatmentlife-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock)Syncope (fainting) is graded in the NEUROLOGY category.Vasovagal episode none-present without loss ofconsciousness present with loss of consciousness-Adverse Event01234Ventricular arrhythmia (PVCs/bigeminy/trigeminy/ ventricular tachycardia)none asymptomatic, notrequiring treatmentsymptomatic, but notrequiring treatmentsymptomatic andrequiring treatmentlife-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock)Cardiovascular/ Arrhythmia - Other (Specify, ___________)none asymptomatic, notrequiring treatmentsymptomatic, but notrequiring treatmentsymptomatic, andrequiring treatment ofunderlying causelife-threatening (e.g.,arrhythmia associatedwith CHF, hypotension,syncope, shock) CARDIOVASCULAR (GENERAL)Acute vascular leak syndrome absent-symptomatic, but notrequiring fluid supportrespiratory compromiseor requiring fluidslife-threatening;requiring pressorsupport and/orventilatory supportCardiac-ischemia/infarction none non-specific T - waveflattening or changes asymptomatic, ST - andT - wave changessuggesting ischemiaangina without evidenceof infarctionacute myocardialinfarctionCardiac left ventricular function normal asymptomatic declineof resting ejectionfraction of ≥10% but<20% of baseline value;shortening fraction≥24% but <30%asymptomatic butresting ejection fractionbelow LLN forlaboratory or decline ofresting ejection fraction≥20% of baseline value;<24% shorteningfractionCHF responsive totreatmentsevere or refractoryCHF or requiringintubationCNS cerebrovascular ischemia is graded in the NEUROLOGY category.Cardiac troponin I (cTnI)normal--levels consistent withunstable angina asdefined by themanufacturer levels consistent with myocardial infarction as defined by the manufacturerCardiac troponin T (cTnT)normal≥0.03 - <0.05 ng/mL≥0.05 - <0.1 ng/mL≥0.1 - <0.2 ng/mL≥0.2 ng/mLEdema none asymptomatic, notrequiring therapy symptomatic, requiringtherapysymptomatic edemalimiting function andunresponsive to therapyor requiring drugdiscontinuationanasarca (severegeneralized edema)Hypertension none asymptomatic, transientincrease by >20 mmHg(diastolic) or to>150/100* if previouslyWNL; not requiringtreatment recurrent or persistentor symptomatic increaseby >20 mmHg(diastolic) or to>150/100* if previouslyWNL; not requiringtreatmentrequiring therapy ormore intensive therapythan previouslyhypertensive crisis*Note: For pediatric patients, use age and sex appropriate normal values >95th percentile ULN.Adverse Event01234Hypotension none changes, but notrequiring therapy(including transientorthostatic hypotension)requiring brief fluidreplacement or othertherapy but nothospitalization; nophysiologicconsequencesrequiring therapy andsustained medicalattention, but resolveswithout persistingphysiologicconsequencesshock (associated withacidemia and impairingvital organ function dueto tissue hypoperfusion)Also consider Syncope (fainting).Notes:Angina or MI is graded as Cardiac-ischemia/infarction in the CARDIOVASCULAR (GENERAL) category.For pediatric patients, systolic BP 65 mmHg or less in infants up to 1 year old and 70 mmHg or less in children older than 1 year of age, use two successive or three measurements in 24 hours.Myocarditis none--CHF responsive totreatment severe or refractory CHFOperative injury of vein/artery none primary suture repairfor injury, but notrequiring transfusionprimary suture repairfor injury, requiringtransfusionvascular occlusionrequiring surgery orbypass for injurymyocardial infarction;resection of organ (e.g.,bowel, limb)Pericardial effusion/ pericarditis none asymptomatic effusion,not requiring treatmentpericarditis (rub, ECGchanges, and/or chestpain)with physiologicconsequencestamponade (drainage orpericardial windowrequired)Peripheral arterial ischemia none-brief episode ofischemia managed non-surgically and withoutpermanent deficit requiring surgicalinterventionlife-threatening or withpermanent functionaldeficit (e.g.,amputation)Phlebitis (superficial)none-present--Notes:Injection site reaction is graded in the DERMATOLOGY/SKIN category.Thrombosis/embolism is graded in the CARDIOVASCULAR (GENERAL) category.Syncope (fainting) is graded in the NEUROLOGY category.Thrombosis/embolism none-deep vein thrombosis,not requiringanticoagulant deep vein thrombosis,requiring anticoagulanttherapyembolic event includingpulmonary embolismVein/artery operative injury is graded as Operative injury of vein/artery in the CARDIOVASCULAR (GENERAL) category.Visceral arterial ischemia (non-myocardial)none-brief episode ofischemia managed non-surgically and withoutpermanent deficitrequiring surgicalinterventionlife-threatening or withpermanent functionaldeficit (e.g., resection ofileum)Cardiovascular/General - Other (Specify, ______________)none mild moderate severe life-threatening ordisablingAdverse Event01234COAGULATIONNote: See the HEMORRHAGE category for grading the severity of bleeding events.DIC(disseminated intravascular coagulation)absent--laboratory findingspresent with nobleedinglaboratory findings andbleedingAlso consider Platelets.Note: Must have increased fibrin split products or D-dimer in order to grade as DIC.Fibrinogen WNL≥0.75 - <1.0 x LLN≥0.5 - <0.75 x LLN≥0.25 - <0.5 x LLN<0.25 x LLNFor leukemia studies or bone marrow infiltrative/ myelophthisic process, if specified in the protocol.WNL<20% decrease frompretreatment value orLLN≥20 - <40% decreasefrom pretreatment valueor LLN≥40 - <70% decreasefrom pretreatment valueor LLN<50 mgPartial thromboplastin time(PTT)WNL>ULN - ≤1.5 x ULN>1.5 - ≤2 x ULN>2 x ULN-Phlebitis is graded in the CARDIOVASCULAR (GENERAL) category.Prothrombin time (PT)WNL>ULN - ≤1.5 x ULN>1.5 - ≤2 x ULN>2 x ULN-Thrombosis/embolism is graded in the CARDIOVASCULAR (GENERAL) category.Thrombotic microangiopathy (e.g., thrombotic thrombocytopenic purpura/TTP or hemolytic uremic syndrome/HUS)absent--laboratory findingspresent without clinicalconsequenceslaboratory findings andclinical consequences,(e.g., CNS hemorrhage/bleeding or thrombosis/embolism or renalfailure) requiringtherapeutic interventionFor BMT studies, if specified in the protocol.-evidence of RBCdestruction(schistocytosis) withoutclinical consequencesevidence of RBCdestruction withelevated creatinine (≤3x ULN)evidence of RBCdestruction withcreatinine (>3 x ULN)not requiring dialysisevidence of RBCdestruction with renalfailure requiringdialysis and/orencephalopathyAlso consider Hemoglobin, Platelets, Creatinine.Note: Must have microangiopathic changes on blood smear (e.g., schistocytes, helmet cells, red cell fragments).Coagulation - Other (Specify, __________)none mild moderate severe life-threatening ordisabling CONSTITUTIONAL SYMPTOMSFatigue(lethargy, malaise, asthenia)none increased fatigue overbaseline, but notaltering normalactivitiesmoderate (e.g., decreasein performance statusby 1 ECOG level or20% Karnofsky orLansky) or causingdifficulty performingsome activitiessevere (e.g., decrease inperformance status by≥2 ECOG levels or 40%Karnofsky or Lansky) orloss of ability toperform some activitiesbedridden or disablingNote: See Appendix III for performance status scales.Adverse Event01234Fever (in the absence of neutropenia, where neutropenia is defined as AGC <1.0 x 109/L)none38.0 - 39.0°C (100.4 -102.2°F)39.1 - 40.0°C (102.3 -104.0°F )>40.0°C (>104.0°F ) for<24hrs>40.0°C (>104.0°F ) for>24hrsAlso consider Allergic reaction/hypersensitivity.Note: The temperature measurements listed above are oral or tympanic. Hot flashes/flushes are graded in the ENDOCRINE category.Rigors, chills none mild, requiringsymptomatic treatment(e.g., blanket) or non-narcotic medication severe and/orprolonged, requiringnarcotic medicationnot responsive tonarcotic medication-Sweating(diaphoresis)normal mild and occasional frequent or drenching--Weight gain<5% 5 - <10%10 - <20%≥20%-Also consider Ascites, Edema, Pleural effusion (non-malignant).Weight gain associated with Veno-Occlusive Disease (VOD) for BMT studies, if specified in the protocol.<2%≥2 - <5%≥5 - <10%≥10% or as ascites≥10% or fluid retentionresulting in pulmonaryfailureAlso consider Ascites, Edema, Pleural effusion (non-malignant).Weight loss<5% 5 - <10%10 - <20%≥20%-Also consider Vomiting, Dehydration, Diarrhea.Constitutional Symptoms -Other(Specify, __________)none mild moderate severe life-threatening ordisablingDERMATOLOGY/SKINAlopecia normal mild hair loss pronounced hair loss--Bruising(in absence of grade 3 or 4 thrombocytopenia)none localized or independent areageneralized--Note:Bruising resulting from grade 3 or 4 thrombocytopenia is graded as Petechiae/purpura and Hemorrhage/bleeding with grade 3 or 4 thrombocytopenia in the HEMORRHAGE category, not in the DERMATOLOGY/SKIN category.Dry skin normal controlled withemollients not controlled withemollients--Erythema multiforme (e.g., Stevens-Johnson syndrome, toxic epidermal necrolysis)absent-scattered, but notgeneralized eruptionsevere or requiring IVfluids (e.g., generalizedrash or painfulstomatitis)life-threatening (e.g.,exfoliative or ulceratingdermatitis or requiringenteral or parenteralnutritional support)Flushing absent present---Hand-foot skin reaction none skin changes ordermatitis without pain(e.g., erythema, peeling)skin changes with pain,not interfering withfunctionskin changes with pain,interfering withfunction-Injection site reaction none pain or itching orerythema pain or swelling, withinflammation orphlebitisulceration or necrosisthat is severe orprolonged, or requiringsurgery-Adverse Event01234Nail changes normal discoloration or ridging(koilonychia) or pitting partial or complete lossof nail(s) or pain innailbeds--Petechiae is graded in the HEMORRHAGE category.Photosensitivity none painless erythema painful erythema erythema withdesquamation-Pigmentation changes (e.g., vitiligo)none localized pigmentationchangesgeneralizedpigmentation changes--Pruritus none mild or localized,relieved spontaneouslyor by local measures intense or widespread,relieved spontaneouslyor by systemic measuresintense or widespreadand poorly controlleddespite treatment-Purpura is graded in the HEMORRHAGE category.Radiation dermatitis none faint erythema or drydesquamation moderate to briskerythema or a patchymoist desquamation,mostly confined to skinfolds and creases;moderate edemaconfluent moistdesquamation ≥1.5 cmdiameter and notconfined to skin folds;pitting edemaskin necrosis orulceration of fullthickness dermis; mayinclude bleeding notinduced by minortrauma or abrasionNote: Pain associated with radiation dermatitis is graded separately in the PAIN category as Pain due to radiation.Radiation recall reaction (reaction following chemotherapy in the absence of additional radiation therapy that occurs in a previous radiation port)none faint erythema or drydesquamationmoderate to briskerythema or a patchymoist desquamation,mostly confined to skinfolds and creases;moderate edemaconfluent moistdesquamation ≥1.5 cmdiameter and notconfined to skin folds;pitting edemaskin necrosis orulceration of fullthickness dermis; mayinclude bleeding notinduced by minortrauma or abrasionRash/desquamation none macular or papulareruption or erythemawithout associatedsymptoms macular or papulareruption or erythemawith pruritus or otherassociated symptomscovering <50% of bodysurface or localizeddesquamation or otherlesions covering <50%of body surface areasymptomaticgeneralizederythroderma ormacular, papular orvesicular eruption ordesquamation covering≥50% of body surfaceareageneralized exfoliativedermatitis or ulcerativedermatitisAlso consider Allergic reaction/hypersensitivity.Note: Stevens-Johnson syndrome is graded separately as Erythema multiforme in the DERMATOLOGY/SKIN category.Rash/dermatitis associated with high-dose chemotherapy or BMT studies.none faint erythema or drydesquamationmoderate to briskerythema or a patchymoist desquamation,mostly confined to skinfolds and creases;moderate edemaconfluent moistdesquamation ≥1.5 cmdiameter and notconfined to skin folds;pitting edemaskin necrosis or ulcera-tion of full thicknessdermis; may includespontaneous bleedingnot induced by minortrauma or abrasionRash/desquamation associated with graft versus host disease (GVHD) for BMT studies, if specified in the protocol.None macular or papulareruption or erythemacovering <25% of bodysurface area withoutassociated symptomsmacular or papulareruption or erythemawith pruritus or otherassociated symptomscovering ≥25 - <50% ofbody surface orlocalized desquamationor other lesionscovering ≥25 - <50% ofbody surface areasymptomaticgeneralizederythroderma orsymptomatic macular,papular or vesiculareruption, with bullousformation, ordesquamation covering≥50% of body surfaceareageneralized exfoliativedermatitis or ulcerativedermatitis or bullousformationAlso consider Allergic reaction/hypersensitivity.Note: Stevens-Johnson syndrome is graded separately as Erythema multiforme in the DERMATOLOGY/SKIN category.Adverse Event01234Urticaria(hives, welts, wheals)none requiring no medication requiring PO or topicaltreatment or IVmedication or steroidsfor <24 hoursrequiring IV medicationor steroids for ≥24hours-Wound-infectious none cellulitis superficial infection infection requiring IVantibioticsnecrotizing fasciitisWound-non-infectious none incisional separation incisional hernia fascial disruptionwithout evisceration fascial disruption with eviscerationDermatology/Skin - Other (Specify, ________)none mild moderate severe life-threatening ordisablingENDOCRINECushingoid appearance (e.g.,moon face, buffalo hump,centripetal obesity,cutaneous striae)absent-present--Also consider Hyperglycemia, Hypokalemia.Feminization of male absent--present-Gynecomastia none mild pronounced or painful pronounced or painfuland requiring surgery-Hot flashes/flushes none mild or no more than 1per day moderate and greaterthan 1 per day--Hypothyroidism absent asymptomatic,TSHelevated, no therapygiven symptomatic or thyroidreplacement treatmentgivenpatient hospitalized formanifestations ofhypothyroidismmyxedema comaMasculinization of female absent--present-SIADH (syndrome ofinappropriate antidiuretichormone)absent--present-Endocrine - Other (Specify, __________)none mild moderate severe life-threatening ordisablingGASTROINTESTINALAmylase is graded in the METABOLIC/LABORATORY category.Anorexia none loss of appetite oral intake significantlydecreased requiring IV fluids requiring feeding tubeor parenteral nutritionAscites (non-malignant)none asymptomatic symptomatic, requiringdiuretics symptomatic, requiringtherapeutic paracentesislife-threateningphysiologicconsequencesColitis none-abdominal pain withmucus and/or blood instool abdominal pain, fever,change in bowel habitswith ileus or peritonealsigns, and radiographicor biopsydocumentationperforation or requiringsurgery or toxicmegacolonAlso consider Hemorrhage/bleeding with grade 3 or 4 thrombocytopenia, Hemorrhage/bleeding without grade 3 or 4 thrombocytopenia, Melena/GI bleeding, Rectal bleeding/hematochezia, Hypotension.Constipation none requiring stool softeneror dietary modification requiring laxatives obstipation requiringmanual evacuation orenemaobstruction or toxicmegacolon。
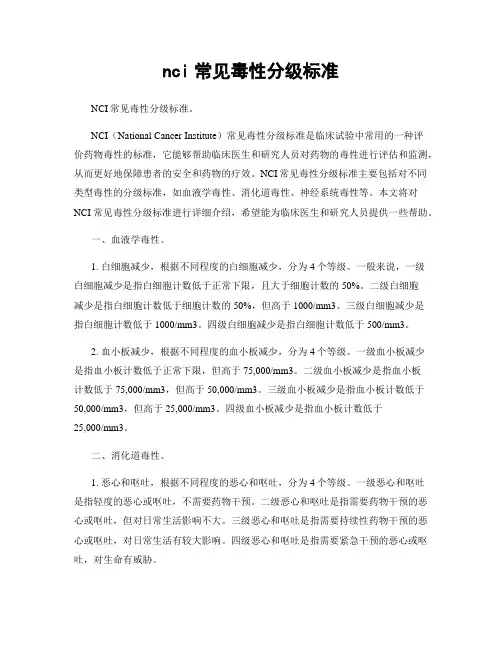
nci常见毒性分级标准NCI常见毒性分级标准。
NCI(National Cancer Institute)常见毒性分级标准是临床试验中常用的一种评价药物毒性的标准,它能够帮助临床医生和研究人员对药物的毒性进行评估和监测,从而更好地保障患者的安全和药物的疗效。
NCI常见毒性分级标准主要包括对不同类型毒性的分级标准,如血液学毒性、消化道毒性、神经系统毒性等。
本文将对NCI常见毒性分级标准进行详细介绍,希望能为临床医生和研究人员提供一些帮助。
一、血液学毒性。
1. 白细胞减少,根据不同程度的白细胞减少,分为4个等级。
一般来说,一级白细胞减少是指白细胞计数低于正常下限,且大于细胞计数的50%。
二级白细胞减少是指白细胞计数低于细胞计数的50%,但高于1000/mm3。
三级白细胞减少是指白细胞计数低于1000/mm3。
四级白细胞减少是指白细胞计数低于500/mm3。
2. 血小板减少,根据不同程度的血小板减少,分为4个等级。
一级血小板减少是指血小板计数低于正常下限,但高于75,000/mm3。
二级血小板减少是指血小板计数低于75,000/mm3,但高于50,000/mm3。
三级血小板减少是指血小板计数低于50,000/mm3,但高于25,000/mm3。
四级血小板减少是指血小板计数低于25,000/mm3。
二、消化道毒性。
1. 恶心和呕吐,根据不同程度的恶心和呕吐,分为4个等级。
一级恶心和呕吐是指轻度的恶心或呕吐,不需要药物干预。
二级恶心和呕吐是指需要药物干预的恶心或呕吐,但对日常生活影响不大。
三级恶心和呕吐是指需要持续性药物干预的恶心或呕吐,对日常生活有较大影响。
四级恶心和呕吐是指需要紧急干预的恶心或呕吐,对生命有威胁。
2. 腹泻,根据不同程度的腹泻,分为4个等级。
一级腹泻是指轻度的腹泻,不需要药物干预。
二级腹泻是指需要药物干预的腹泻,但对日常生活影响不大。
三级腹泻是指需要持续性药物干预的腹泻,对日常生活有较大影响。
抗癌药物常见不良反应分级标准(who)表格随着癌症发病率的增加,抗癌药物的使用也越来越广泛。
然而,抗癌药物也会带来一系列不良反应,这给患者的治疗带来了一定的挑战。
了解抗癌药物的不良反应分级标准对于医生和患者都至关重要。
WHO(世界卫生组织)制定了一套抗癌药物常见不良反应的分级标准,这些标准帮助医生对患者的不良反应做出及时的评估和处理。
下面将介绍抗癌药物常见不良反应的分级标准。
1. 血液系统不良反应(1)贫血:Ⅰ级:Hb(血红蛋白)下降≥30 g/L,但≤80 g/LⅡ级:Hb下降>80 g/LⅢ级:需要输血或Hb下降≤60 g/L(2)白细胞减少:Ⅰ级:WBC(白细胞计数)下降<3.0×10^9/LⅡ级:WBC下降<2.0×10^9/LⅢ级:WBC下降<1.0×10^9/L,或伴有发热或症状2. 消化系统不良反应(1)恶心与呕吐:Ⅰ级:轻度,不影响日常生活Ⅱ级:需要药物治疗Ⅲ级:需要静脉输液治疗(2)腹泻:Ⅰ级:每天增加小于4次Ⅱ级:每天增加4-6次Ⅲ级:每天增加7次以上3. 皮肤及其附件不良反应(1)脱发:Ⅰ级:头发量减少Ⅱ级:需要使用帽子或假发Ⅲ级:持续脱发(2)皮疹:Ⅰ级:局部红斑、瘙痒等Ⅱ级:需要用药治疗Ⅲ级:需要住院治疗4. 肝功能不良反应(1)ALT(丙氨酸氨基转移酶)升高:Ⅰ级:ALT升高1-2倍正常上限Ⅱ级:ALT升高3-5倍正常上限Ⅲ级:ALT升高>5倍正常上限(2)黄疸:Ⅰ级:TB(总胆红素)升高1.25-2.5倍正常上限Ⅱ级:TB升高2.6-5倍正常上限Ⅲ级:TB升高>5倍正常上限5. 肾功能不良反应(1)肌酐升高:Ⅰ级:Cr(肌酐)升高1.5-2倍基础水平Ⅱ级:Cr升高2-3倍基础水平Ⅲ级:Cr升高>3倍基础水平(2)血尿素氮(BUN)升高:Ⅰ级:BUN升高1.5-2.5倍基础水平Ⅱ级:BUN升高2.6-5倍基础水平Ⅲ级:BUN升高>5倍基础水平以上就是抗癌药物常见不良反应分级标准(WHO)表格。
抗肿瘤药物的分级原则及划分标准下载提示:该文档是本店铺精心编制而成的,希望大家下载后,能够帮助大家解决实际问题。
文档下载后可定制修改,请根据实际需要进行调整和使用,谢谢!本店铺为大家提供各种类型的实用资料,如教育随笔、日记赏析、句子摘抄、古诗大全、经典美文、话题作文、工作总结、词语解析、文案摘录、其他资料等等,想了解不同资料格式和写法,敬请关注!Download tips: This document is carefully compiled by this editor. I hope that after you download it, it can help you solve practical problems. The document can be customized and modified after downloading, please adjust and use it according to actual needs, thank you! In addition, this shop provides you with various types of practical materials, such as educational essays, diary appreciation, sentence excerpts, ancient poems, classic articles, topic composition, work summary, word parsing, copy excerpts, other materials and so on, want to know different data formats and writing methods, please pay attention!抗肿瘤药物的分级原则及划分标准在现代医学中,抗肿瘤药物是治疗肿瘤疾病的重要手段之一。
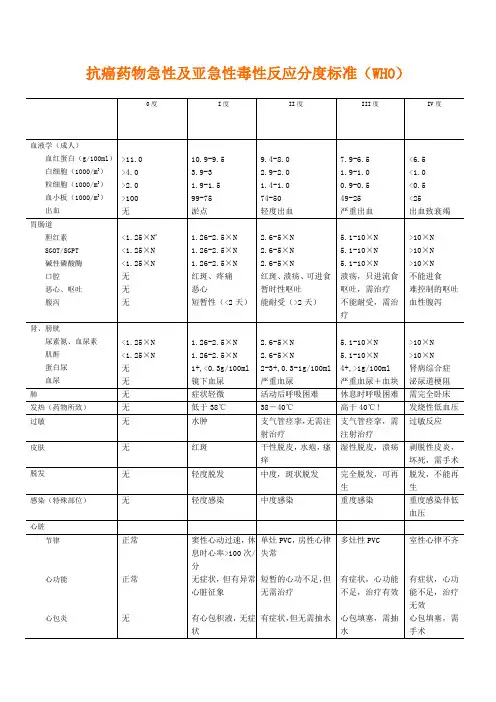
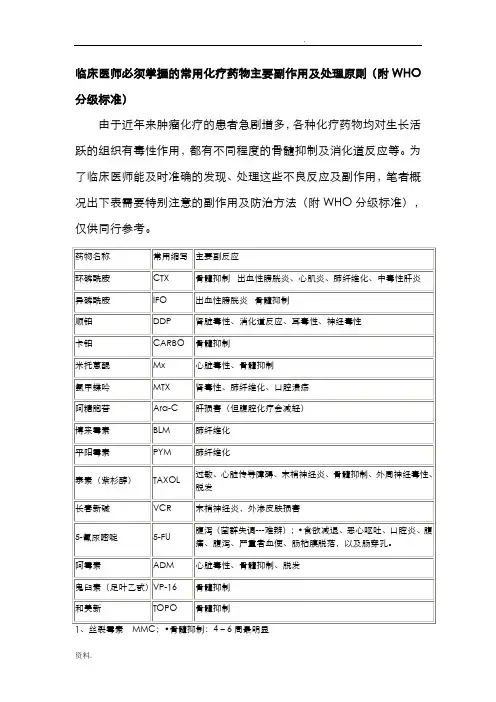
临床医师必须掌握的常用化疗药物主要副作用及处理原则(附WHO 分级标准)由于近年来肿瘤化疗的患者急剧增多,各种化疗药物均对生长活跃的组织有毒性作用,都有不同程度的骨髓抑制及消化道反应等。
为了临床医师能及时准确的发现、处理这些不良反应及副作用,笔者概况出下表需要特别注意的副作用及防治方法(附WHO分级标准),仅供同行参考。
2、博莱霉素BLM;•毒副作用:肺毒性:肺炎样症状、肺纤维化,皮肤反应:指趾关节皮肤肥厚,色素沉着。
发热:38度左右,可自行消退。
3、新一代铂类,包括:奥沙利铂、络铂、奈达铂高发生率不良反应有:周围神经毒性、骨髓抑制、腹泻经对症处理、减量、停药,基本可控制4、长春瑞宾NVB:从外周静脉给药时,刺激大,静脉炎发生率高,切勿外渗。
周围神经毒性:腱反射消失、指、趾麻木、四肢疼痛、肌肉震颤。
骨髓抑制:主要为中性粒细胞减少,但无剂量累积毒性。
5、依立替康:1)急性反应:乙酰胆碱综合征,表现为多汗、多泪、唾液分泌增多、视物模糊、痉挛性腹痛、“早期”腹泻;在用药24小时内出现,多可自行缓解,严重者给阿托品治疗;恶心呕吐常见。
2)亚急性反应:延迟性腹泻,剂量限制毒性,用药24小时后出现,水样便,可带血,发生率80%~90%,严重者占39%;大剂量易蒙停有效;骨髓抑制明显,亦为剂量限制毒性。
6、托泊替康:骨髓抑制明显;4度血小板降低发生率达26%,中位持续时间为5天,血小板降低至最低中位发生时间为15天。
7、草酸铂L-OHP:外周神经毒性:感觉迟钝、异常,遇冷加重,偶见可逆性急性咽喉感觉异常。
与依立替康合用可发生胆碱能综合征(腹痛、唾液分泌过多等)危险,阿托品可以预防。
护理措施:------四禁•禁止用N.S稀释•禁止用冰水漱口和冷食•禁止与碱性药物或溶液配伍输注•制备药液及输注时避免接触铝制品、避开离子8、掌握化疗药物的正确溶酶,保证药物有效性用N.S稀释的药物:氮芥、CTX、VDS、BLM、喜树碱、VP-16、DDP用G.S稀释的药物:MTX、CBP、草酸铂、秋水酰碱、THP、光辉霉素、抗癌锑等。
化疗后骨髓抑制分度及处理骨髓抑制概述骨髓抑制是指骨髓中的血细胞前体的活性下降。
血流里的红细胞和白细胞都源于骨髓中的干细胞。
血流里的血细胞寿命短,常常需要不断补充。
为了达到及时补充的目的,作为血细胞前体的干细胞必须快速分裂。
化学治疗(Chemotherapy)和放射治疗(radiation)、以及许多其它抗肿瘤治疗方法,都是针对快速分裂的细胞,因而常常导致正常骨髓细胞受抑。
广州医科大学附属肿瘤医院胸外科薛兴阳起因骨髓抑制是多数化疗药的常见毒性反应,大多数化疗药均可引起有不同程度的骨髓抑制,使周围血细胞数量减少,血细胞由多种成分组成,每一种成分都对人体起着不可缺少的作用,任何一种成分的减少都使机体产生相应的副反应.较常见的药物如:阿霉素,泰素,卡铂,异环磷酰胺,长春碱类等。
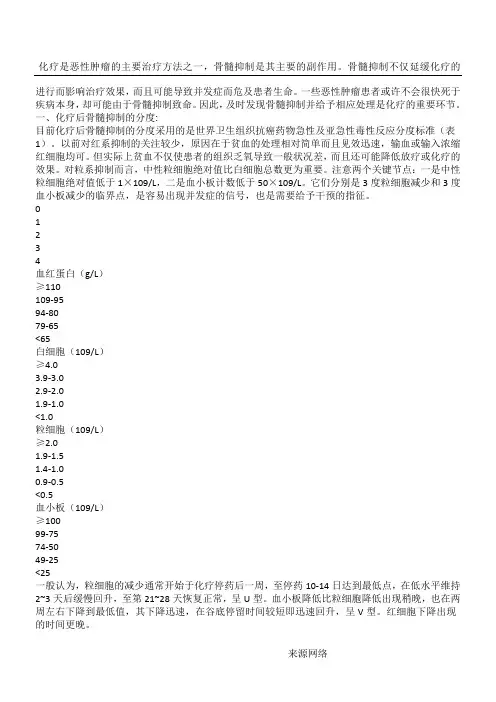
鉴别与诊断骨髓抑制的级别诊断:骨髓的抑制程度根据WHO分为0~Ⅳ级:0级:白细胞≥4.0×109/L,血红蛋白≥110g/L,血小板≥100×109/L,Ⅰ级:白细胞(3.0~3.9)×109/L,血红蛋白95~100g/L,血小板(75~99)×109/L,Ⅱ级:白细胞(2.0~2.9)×109/L,血红蛋白80~94 g/L,血小板(50~74)×109/L,Ⅲ级:白细胞(1.0~1.9)×109/L ,血红蛋白65~79 g/L,血小板(25~49)×109/L,Ⅳ级:白细胞(0~1.0)×109/L ,血红蛋白<65g/L,血小板<25×109/L。
骨髓抑制通常发生在化疗后。
因粒细胞平均生存时间最短,约为6-8小时,因此骨髓抑制常最先表现为白细胞下降;血小板平均生存时间约为5-7天,其下降出现较晚较轻;而红细胞平均生存时间为120天,受化疗影响较小,下降通常不明显。
多数化疗药物所致的骨髓抑制,通常见于化疗后1-3周,约持续2-4周逐渐恢复,并以白细胞下降为主,可有伴血小板下降,少数药如健择、卡铂、丝裂霉素等则以血小板下降为主。
ctcae分级标准CTCAE分级标准。
CTCAE(Common Terminology Criteria for Adverse Events)是美国国家癌症研究所(NCI)制定的一套用于评估临床试验中药物不良事件的标准。
CTCAE分级标准是临床研究中常用的一种评估药物毒性和不良事件的工具,对于临床试验的安全性评价和治疗方案的调整具有重要意义。
CTCAE分级标准主要分为五个等级,分别是1级、2级、3级、4级和5级,用于描述药物不良事件的轻重程度。
在临床研究中,医务人员会根据患者出现的不良事件的严重程度,按照CTCAE分级标准进行评定和记录,以便及时采取相应的干预措施。
1级不良事件通常是轻微的,对患者的生活质量影响较小,不需要特殊治疗措施。
比如,头痛、恶心、呕吐、轻度腹泻等。
2级不良事件会对患者的生活造成一定程度的影响,可能需要采取一些治疗措施。
比如,中度腹泻、轻度贫血、轻度疲劳等。
3级不良事件会对患者的生活造成较大影响,需要采取积极的治疗措施。
比如,重度腹泻、中度贫血、中度疲劳等。
4级不良事件会对患者的生命造成威胁,需要紧急治疗和监护。
比如,重度贫血、严重腹泻、严重呕吐等。
5级不良事件是最严重的,可能导致患者死亡。
比如,严重的心脏毒性、严重的肺毒性等。
在临床研究中,CTCAE分级标准的使用对于评估药物的安全性和毒性具有重要意义。
通过对患者出现不良事件的严重程度进行分级,可以及时采取相应的治疗措施,保障患者的安全。
同时,也可以为临床试验结果的准确评估提供重要依据。
因此,医务人员需要熟练掌握CTCAE分级标准,并在临床实践中加以应用。
总之,CTCAE分级标准是临床研究中不可或缺的工具,对于评估药物的安全性和毒性具有重要意义。
医务人员应当充分了解和掌握CTCAE分级标准,正确评定和记录患者出现的不良事件,以确保临床试验的安全性和有效性。
同时,也需要加强对患者的监测和护理,最大程度地保障患者的安全和利益。
第一节不良反应分类任何药物性治疗均会伴有---定程度的不良反应,不同的药物具有不同的毒性谱c对恶性肿瘤化疗的不良反应而言,除了最常见的血液毒性、消化道毒件之外,人体的许多脏器、许多组织均会受到抗癌药物不同程度地损伤而产生多种多样的不良反应。
一、近期反应和远期反应抗癌药物不良反应的分类方式很多,临床最为常用的是根据不良反应发生的时间分为四类(表1-1),或简化为近期反应和远期反应两类:11。
近期反应主要发生于给药后4 词以内,而远期反应则指在用药4周后发生,有时可长达数十年。
常见毒性反应的发生时间如表卜2[2)所示。
表1-1抗癌药物的不良反应分类即刻反应早期反敁中期反应后期反应过敏性休克恶心、呕吐骨髓抑制皮肤色素沉者心律不齐发热口炎承要器官损伤注射部位疼痛过敏反应流感样综合征膀胱炎腹泻脱发周围神经炎重要系统损伤牛殖系统毐性内分泌改变致畸胎作用反射消失肠麻痹肾毐性免疫抑制表1 一2抗肿癯药物毒性的发生时间抗肿瘤药物毒性的发生时间性类____________________________________________________________________________________发生时间 毒性种类 ____________________________用药当日H、动过速、心律失常、眩犛、发氣、血^痛:恶2-3日倦怠感、食欲不振、恶心、呕吐(迟发性) 7-14 日 口炎、腹泻、食欲不振、血液泰性14〜28日 脏器损害、膀咣炎、皮肤角化、色紊沉著、脱发、神经损害、免疫异常 2〜6个月 肺纤維化、允血性心功不全 5-6年继发性肿瘤二、急性、亚急性、慢性毐性通常在进行新药研究时,要求进行急性毒性、亚急性毒件和慢性毒n试验c1.急性毒性:指用药后1-2周内的#副作用,,2.急性毐性:指用药后2周至3个月的毒副作用.:3.慢性毒性:指超过3个月的毒性作坩…二、世界11生组织(WHO)分类1.急性和亚急性毐件:用药后3个月以内发牛的毒性…2.慢性和后期#性:发生fr:用药后3个月至数年。