4、Hepatitis B virus infection and B-cell non-Hodgkin’s lymphoma in a hepatitis B endemic areaa cas
- 格式:pdf
- 大小:70.46 KB
- 文档页数:7

The new england journal of medicinen engl j med 350;11 march 11, 20041118 mechanisms of diseaseHepatitis B Virus Infection — Natural Historyand Clinical ConsequencesDon Ganem, M.D., and Alfred M. Prince, M.D.From the Departments of Microbiologyand I mmunology and Medicine and theHoward Hughes Medical Institute, Univer-sity of California, San Francisco (D.G.); andthe Laboratory of Virology, Lindsley F. Kim-ball Research I nstitute, New York BloodCenter, and the Department of Pathology,New York University School of Medicine— both in New York (A.M.P.). Address re-print requests to Dr. Prince at the Laborato-ry of Virology, Lindsley F. Kimball ResearchInstitute, New York Blood Center, 310 E. 67thSt., New York, NY 10021, or at aprince@.N Engl J Med 2004;350:1118-29.Copyright © 2004 Massachusetts Medical Society. n the past 10 years, remarkable strides have been made in the understanding of the natural history and pathogenesis of hepatitis B virus (HBV)infection. In this article we will review these advances, with particular referencehepatitis in the decades after World War II. The groundbreaking studies of Krugmanand colleagues in 1967 firmly established the existence of at least two types of hepa-titis, 1 one of which (then called serum hepatitis, and now called hepatitis B) was parenter-ally transmitted. Links to the virus responsible for this form of hepatitis were derived by serologic studies conducted independently by Prince and colleagues 2-4 and byBlumberg and colleagues. 5 Blumberg and colleagues, searching for serum protein poly-morphisms linked to diseases, identified an antigen (termed Au) in serum from pa-tients with leukemia, leprosy, and hepatitis, though the relationship of this antigen tohepatitis was initially unclear. By systematically studying patients with transfusion-associated hepatitis, Prince and coworkers independently identified an antigen, termedSH, that appeared in the blood of these patients during the incubation period of thedisease, and further work established that Au and SH were identical. 6,7 The antigenrepresented the hepatitis B surface antigen (HBsAg). 8,9 These seminal studies madepossible the serologic diagnosis of hepatitis B and opened up the field to rigorous epi-Hepatitis B virus (HBV) is the prototype member of the Hepadnaviridae (hepatotropicDNA virus) family. Hepadnaviruses have a strong preference for infecting liver cells, butsmall amounts of hepadnaviral DNA can be found in kidney, pancreas, and mononu-clear cells. However, infection at these sites is not linked to extrahepatic disease. 10-13HBV virions are double-shelled particles, 40 to 42 nm in diameter (Fig. 1A), 14 withan outer lipoprotein envelope that contains three related envelope glycoproteins (orsurface antigens). 15 Within the envelope is the viral nucleocapsid, or core. 16 The corecontains the viral genome, a relaxed-circular, partially duplex DNA of 3.2 kb, and a po-lymerase that is responsible for the synthesis of viral DNA in infected cells. 17 DNA se-quencing of many isolates of HBV has confirmed the existence of multiple viral geno-types, each with a characteristic geographic distribution. 18In addition to virions, HBV-infected cells produce two distinct subviral lipopro-tein particles: 20-nm spheres (Fig. 1B) and filamentous forms of similar diameteri The New England Journal of Medicine as published by New England Journal of Medicine.Downloaded from on July 29, 2010. For personal use only. No other uses without permission.mechanisms of disease(Fig. 1A).16 These HBsAg particles contain only en-ABFigure 1. Structure of HBsAg-Associated Particles(Phosphotungstic Acid–Negative Stain).Panel A shows HBV virions (Dane particles) and fila-ments. Panel B shows 20-nm HBsAg particles.n engl j med 350;11 march 11 , 2004 The new england journal of medicine1120 identity of which remains unknown. After mem-brane fusion, cores are presented to the cytosol andtransported to the nucleus. There, their DNA ge-nomes are converted to a covalently closed circular(ccc) form, 26 which serves as the transcriptionaltemplate for host RNA polymerase II. This enzymegenerates a series of genomic and subgenomictranscripts. 27All viral RNA is transported to the cytoplasm,where its translation yields the viral envelope, core,and polymerase proteins, as well as the X and preC polypeptides. Next, nucleocapsids are assembled in the cytosol, and during this process a single mol-ecule of genomic RNA is incorporated into the as-sembling viral core. 28 Once the viral RNA is en-capsidated, reverse transcription begins. 28 TheEntry of HBVinto cell Vesicular transportto cell membraneBudding intoendoplasmicreticulumCore assembly andRNA packaging Core particleCore particle plusstrand synthesisCore particle minus strand synthesisHBVTranslationTranscriptionNucleusCytoplasmcccDNARepairRecyclingThe New England Journal of Medicine as published by New England Journal of Medicine.Downloaded from on July 29, 2010. For personal use only. No other uses without permission.mechanisms of diseasesynthesis of the two viral DNA strands is sequential. The first DNA strand is made from the encapsi-dated RNA template; during or after the synthesis of this strand, the RNA template is degraded and the synthesis of the second DNA strand proceeds, with the use of the newly made first DNA strand as a template.25,27,29 Some cores bearing the mature genome are transported back to the nucleus, where their newly minted DNA genomes can be convert-ed to cccDNA to maintain a stable intranuclear pool of transcriptional templates.26 Most cores, how-ever, bud into regions of intracellular membranes bearing the viral envelope proteins. In so doing, they acquire lipoprotein envelopes containing the viral L, M, and S surface antigens and are then exported from the cell.pathogenesis of hepatitis bThe HBV replication cycle is not directly cytotoxic to cells. This fact accords well with the observation that many HBV carriers are asymptomatic and have minimal liver injury, despite extensive and ongo-ing intrahepatic replication of the virus.30 It is now thought that host immune responses to viral anti-gens displayed on infected hepatocytes are the prin-cipal determinants of hepatocellular injury. This no-tion is consistent with the clinical observation that patients with immune defects who are infected with HBV often have mild acute liver injury but high rates of chronic carriage.31The immune responses to HBV and their role in the pathogenesis of hepatitis B are incompletely understood. Correlative clinical studies show that in acute, self-limited hepatitis B, strong T-cell re-sponses to many HBV antigens are readily demon-strable in the peripheral blood.32 These responses involve both major-histocompatibility-complex (MHC) class II–restricted, CD4+ helper T cells and MHC class I–restricted, CD8+ cytotoxic T lympho-cytes. The antiviral cytotoxic T-lymphocyte response is directed against multiple epitopes within the HBV core, polymerase, and envelope proteins; strong helper T-cell responses to C and P proteins have also been demonstrated in acute infection. By contrast, in chronic carriers of HBV, such virus-specific T-cell responses are greatly attenuated, at least as assayed in cells from the peripheral blood. However, anti-body responses are vigorous and sustained in both situations (although free antibodies against HBsAg [anti-HBs antibodies] are not detectable in carriers because of the excess of circulating HBsAg). This pattern strongly suggests that T-cell responses, es-pecially the responses of cytotoxic T lymphocytes, play a central role in viral clearance. Figure 3 sum-marizes the major types of cellular immune re-sponse to HBV.The mechanisms by which cytotoxic T lympho-cytes kill liver cells and cause viral clearance have been incisively investigated in transgenic mice that express viral antigens or contain replication-com-petent viral genomes in the liver.32,33 Because these mice harbor HBV genes in their germ-line DNA, they are largely tolerant to HBV proteins, and according-ly, clinically significant liver injury does not devel-op. However, if antiviral cytotoxic T lymphocytes of syngeneic animals are transferred into such mice, acute liver injury with many of the features of clini-cal hepatitis B develops.34 It is striking that, in this model, the number of hepatocytes killed by direct engagement between cytotoxic T lymphocytes and their targets is very small and clearly insufficient to account for most of the liver damage. This sug-gests that much of the injury is due to secondary antigen-nonspecific inflammatory responses that are set in motion by the response of the cytotoxic T lymphocytes. Presumably, much of the damage occurring in this context is due to cytotoxic by-prod-ucts of the inflammatory response, such as tumor necrosis factor (TNF), free radicals, and proteas-es. Other immune-cell populations, notably natu-ral killer T cells,35 probably also contribute to liver injury.Recent experiments suggest that some of the inflammatory by-products, notably interferon-g (IFN-g) and TNF-a, can have antiviral effects that do not involve killing the target cells. When cytotoxic T lymphocytes are transferred to mice that bear rep-licating HBV, viral DNA and RNA throughout the liver rapidly disappear, even from viable, uninjured hepatocytes — an effect that can be blocked by the administration of antibodies to TNF-a and IFN-g.34 Such noncytocidal antiviral effects may be impor-tant for viral clearance in natural infection. In fact, cytokine release triggered by unrelated hepatic in-fections in HBV-transgenic mice can have the same effect.36 This phenomenon may explain the sup-pression and occasional clearance of chronic HBV infection in patients with superimposed acute hep-atitis caused by unrelated viruses.natural historyPrimary HBV infection in susceptible (nonimmune) hosts can be either symptomatic or asymptomatic. The latter is more common than the former, espe-n engl j med 350;11 march 11 , 2004The new england journal of medicine1122 cially in young children. Most primary infections inadults, whether symptomatic or not, are self-lim-ited, with clearance of virus from blood and liverand the development of lasting immunity to rein-fection. 37,38 However, some primary infections inhealthy adults (generally less than 5 percent) do notresolve but develop into persistent infections. Insuch cases, viral replication continues in the liverand there is continual viremia, although the titersof virus in the liver and blood are variable. Persis-tent HBV infection may be symptomatic or asymp-tomatic. People with subclinical persistent infec-tion, normal serum aminotransferase levels, andnormal or nearly normal findings on liver biopsyare termed asymptomatic chronic H BV carriers;those with abnormal liver function and histologicfeatures are classified as having chronic hepatitis B.Cirrhosis, a condition in which regenerative nod-ules and fibrosis coexist with severe liver injury,develops in about 20 percent of people with chron-ic hepatitis B. The resulting hepatic insufficiency and portal hypertension make this process one of the most feared consequences of chronic HBV in-fection. Primary Infection In primary infection, HBsAg becomes detectable in the blood after an incubation period of 4 to 10weeks, followed shortly by antibodies against the HBV core antigen (anti-HBc antibodies), which ear-ly in infection are mainly of the IgM isotype. 38 Vire-mia is well established by the time HBsAg is detect-ed, and titers of virus in acute infection are very high — frequently 10 9 to 10 10 virions per milliliter. 39 Cir-culating HBeAg becomes detectable in most cases,and studies of chimpanzees and other animals with primary hepadnaviral infection show that 75 to 100percent of hepatocytes are infected when this anti-gen is evident. 40 Thus, it is not surprising that epi-demiologic studies consistently show high rates ofMHC class IMHCclass I Antigen-presenting cellMHCclass II Infected hepatocyte CD4+T cellCD8+T cell CD8+T cellHBVpeptidesHBVpeptidesHBV coresHBVantigens HBV DNAHBV RNA Down-regulation of viral replication TNF-aInterferon-g HBVHBsAgThe New England Journal of Medicine as published by New England Journal of Medicine.Downloaded from on July 29, 2010. For personal use only. No other uses without permission.mechanisms of diseaseboth vertical and horizontal transmissibility during acute HBV infection.41When liver injury does occur in primary infec-tion, alanine aminotransferase levels do not increase until after viral infection is well established, reflect-ing the time required to generate the T-cell–mediat-ed immune response that triggers liver injury. Once this response is under way, titers of virus in blood and liver begin to drop. The fact that infection can be cleared from virtually all hepatocytes without massive hepatic destruction (in most cases) is a tes-tament to the extraordinary power of the noncy-tolytic clearance mechanisms described above. With clearance of the infection, the viral antigens HBsAg and HBeAg disappear from the circulation, and free anti-HBs antibodies become detectable.Surprisingly, in self-limited infection, as defined by the disappearance of the viral antigens and the appearance of anti-H Bs antibodies, low levels of HBV DNA in the blood may persist for many years, if not for life.42 It is not known whether this DNA contains the entire HBV genome, or even whether it is contained in virions. However, inoculation of serum from three subjects with persistent H BV DNA into chimpanzees has not led to documented infectivity.42Persistent InfectionIn persistent HBV infection, the early events unfold as in self-limited infection, but HBsAg remains in the blood and virus production continues, often for life. However, levels of viremia in chronic infection are generally substantially lower than during pri-mary infection, although they can vary consider-ably from person to person. High titers of HBV in the blood are often indicated by the continued pres-ence of HBeAg. Typically, there are 107 to 109 virions per milliliter in the blood43 in such cases, which are highly infectious. But most people with persistent infection, especially those with anti-HBe antibod-ies, have somewhat lower levels of viremia.One feature of chronic HBV infection that is not widely appreciated is its dynamic natural history. Even though, in most cases, HBsAg remains detect-able for life, titers of viral DNA tend to decline over time. With the passage of time, there is also a ten-dency for HBeAg to disappear from the blood, along with seroconversion to positivity for anti-HBe anti-bodies — a progression that occurs at a rate of 5 to 10 percent per year in persistently infected peo-ple.39 Often, the disappearance of HBeAg is pre-ceded or accompanied by a transient rise in alanine aminotransferase levels, known as a flare, which suggests that the process reflects immune-mediat-ed destruction of infected hepatocytes. Reductions in the level of viremia as great as five orders of mag-nitude may accompany seroconversion to anti-HBe antibodies.44 Thus, the natural history of HBV per-sistence suggests that there is an ongoing immune attack on infected cells in the liver — an attack that is usually inadequate to eradicate infection alto-gether, but that does reduce the number of infected cells and thereby lowers the circulating viral load. Figure 4 shows typical patterns of serologic and molecular markers in both acute self-limited and chronic HBV infection.The widely held view that circulating viral DNA disappears when anti-HBe antibodies appear is in-correct; this idea reflects the fact that, for many years, HBV DNA was measured by relatively insen-sitive hybridization methods with a detection limit of 105 to 106 virions per milliliter. Thanks to the ad-vent of the polymerase-chain-reaction (PCR) meth-od, we now know that at least 70 to 85 percent of people with anti-HBe antibodies have detectable viral DNA in the circulation, typically in the range of 103 to 105 molecules per milliliter, and some-times higher.44 Although these levels of HBV DNA are relatively low, they are hardly negligible. (For reference, they are similar to levels of human im-munodeficiency virus [HIV] and HCV DNA in many patients with symptomatic acquired immunodefi-ciency syndrome or hepatitis C.) Given the short half-life of HBV virions (approximately one day),39 such levels can be sustained only by ongoing viral replication; therefore, the claim that HBV enters a so-called nonreplicative phase later in its course is not correct. For this reason, anyone who has a pos-itive test for HBsAg should be presumed to have some level of ongoing viremia. For example, when a decision must be made about immunoprophy-laxis after a needle stick involving blood from an HBsAg-positive patient, prophylaxis should be of-fered irrespective of that patient’s HBeAg status.HBeAg-negative carriers are a heterogeneous group. Most such carriers have low levels of viral DNA, relatively normal levels of alanine amino-transferase, and a good prognosis.30 However, par-ticularly in southern Europe and in Asia, at least 15 to 20 percent of such carriers have elevated levels of alanine aminotransferase and viral DNA in the blood.45 The virus in many such carriers harbors mutations in the preC region that prevent the pro-duction of HBeAg.46 It has been suggested that per-n engl j med 350;11 march 11 , 2004The new england journal of medicine1124 sistently abnormal levels of alanine aminotransfer-ase and elevated levels of viral DNA may denote asubgroup of HBeAg-negative carriers who shouldreceive active antiviral therapy. 47Hepatocellular Carcinoma Another feature of the natural history of HBV infec-tion is its link to primary hepatocellular carcinoma.Chronically infected subjects have a risk of hepato-cellular carcinoma that is 100 times as high as thatfor noncarriers 48 ; within the HBsAg-positive group,HBeAg-positive carriers have the highest risk ofhepatocellular carcinoma, but even carriers withanti-HBe antibodies have a substantial risk of can-cer. 49 (Although the role of HBV in provoking hep-atocellular carcinoma is undisputed, its cellularand molecular mechanisms remain incompletelyunderstood. 50-54 ) Given these facts, twice-a-yearscreening of chronically infected patients with mea-surements of serum alpha fetoprotein or hepaticultrasonography, or both, is warranted. 47 However,there is debate as to when such screening shouldbegin. Furthermore, screening is imperfect — alpha fetoprotein screening, for example, has an excel-lent negative predictive value, but its positive pre-47are a reduction in the level of viremia and ameliora-tion of hepatic dysfunction. Most clinical studies have focused on chronically infected patients with elevated aminotransferase levels and circulating HBeAg, in whom viral loads can be readily mea-sured even with first-generation DNA tests. There are clear indications for therapy in HBeAg-positive patients. They have an increased risk of early pro-gression to chronic active hepatitis and cirrhosis, 55 and they have a risk of hepatocellular carcinoma that is substantially higher than that for other carri-ers. 49 By contrast, asymptomatic HBeAg-negative chronic carriers with viral loads below 10 5 genomes per milliliter and normal alanine aminotransferaseThe New England Journal of Medicine as published by New England Journal of Medicine.Downloaded from on July 29, 2010. For personal use only. No other uses without permission.mechanisms of diseasevalues tend to have a relatively stable course, with low rates of clinical or pathological progression.30 At present, therapy is usually not offered to such persons. As noted above, some HBeAg-negative pa-tients have liver dysfunction and substantial vire-mia (>105 molecules per milliliter). Discussions of the treatment of such patients are rare in the pub-lished literature, but results of a recent trial suggest that many of these patients would also benefit from effective antiviral therapy.56 A recent clinical prac-tice guideline47 includes this group in its discus-sion of treatment; clearly, future clinical investiga-tions should focus more attention on this group.The usual markers of successful therapy are the loss of H BeAg, seroconversion to anti-H Be anti-bodies, and reduction of the circulating viral load. These are useful indicators, since patients with sta-ble seroconversion to anti-HBe–positive status typ-ically have improved histologic findings in the liv-er, and this improvement tends to be maintained over the long term.57 True cure of infection (loss of HBsAg and complete disappearance of viremia, as measured by stringent PCR assays) is achieved only infrequently (in 1 to 5 percent of patients) with cur-rent regimens, although the increasing numbers of active antiviral drugs might lead to an upward revi-sion of this figure in the future. In the case of pa-tients with HBeAg-negative chronic hepatitis, there is no information about which markers best mea-sure the response to therapy. Quantitation of vire-mia by PCR assays would seem a logical starting place, but there have been no systematic studies to guide the clinical interpretation of results. interferonFor many years, administration of interferon alfa (5 million to 10 million units subcutaneously three times per week, for at least three months) was the mainstay of therapy. About 30 percent of patients who tolerated this regimen had a successful re-sponse, defined as a loss of HBeAg, the develop-ment of anti-HBe antibodies, and a decline in se-rum alanine aminotransferase levels.58 With HBe seroconversion and normalization of alanine ami-notransferase levels, improvement is usually sus-tained well after therapy has been discontinued.58 Interferon alfa treatment of chronic HBV infections in patients with cirrhosis has even been reported to reduce the risk of hepatocellular carcinoma.59 However, the side effects of therapy with inter-feron alfa (fever, myalgias, thrombocytopenia, and depression) make it a difficult treatment for many patients. Moreover, in many patients a flare of liver injury occurs during administration of interferon alfa, often just before or during clearance of HBeAg. This phenomenon may reflect the immunomodu-latory activity of interferon alfa, which, in addition to impairing HBV replication, can also cause up-reg-ulation of MHC class I antigens on hepatocytes and thereby augment the recognition of infected cells by cytotoxic T lymphocytes. Although sometimes disquieting to patients and physicians alike, these flares are intrinsic to the therapy and, as markers of enhanced antiviral immune responsiveness, often presage a successful outcome. However, treatment with interferon alfa is generally contraindicated in very advanced liver disease, since in such cases the flares may precipitate overt liver failure. Moreover, patients with advanced cirrhosis and splenomeg-aly usually have base-line leukopenia and throm-bocytopenia, which can be exacerbated by the drug. antiviral drugsLamivudineIn the past decade, therapy for HBV has been revo-lutionized by the advent of drugs that directly block replication of the HBV genome. All these drugs (to date) are nucleoside or nucleotide analogues that selectively target the viral reverse transcriptase. The first successful drug, lamivudine, emerged from screening for inhibitors of the HIV reverse trans-criptase and was introduced into clinical practice for the management of HIV infection. Carriers of HIV who are also infected with HBV had substan-tial declines in HBV viremia when treated with la-mivudine,60 and such declines were also observed in patients with chronic hepatitis B who did not have HIV infection.61 In general, treatment with la-mivudine results in a reduction of 3 to 4 log in circu-lating levels of HBV DNA in the first three months of therapy; this decline is associated with more rap-id loss of HBeAg, seroconversion to anti-HBe–pos-itive status, and improvement in serum aminotrans-ferase levels. The drug is usually well tolerated, a factor that has led to the rapid displacement of in-terferon alfa from the roster of first-line therapies for HBV. Lamivudine is not immunomodulatory and can be used in patients with decompensated cir-rhosis.62 Even polyarteritis nodosa associated with H BV has been shown to respond dramatically to treatment with lamivudine plus plasma exchange.63 Although lamivudine is not an immunomodu-lator, there is strong evidence that successful treat-ment with lamivudine relies to some extent on ann engl j med 350; march 11, 2004The new england journal of medicine1126adequate host immune response. This evidenceemerged from a retrospective examination of sub-groups of patients with optimal responses to ther-apy, which revealed a strong correlation betweenHBeAg clearance and elevated pretreatment val-ues for alanine aminotransferase.64 HBeAg sero-conversion occurred in 65 percent of cases in whichpretreatment values for alanine aminotransferasewere more than five times the upper limit of thenormal range, as compared with only 26 percentin patients with elevations in alanine aminotrans-ferase values that were two to five times the upperlimit of the normal range. Only 5 percent of pa-tients with pretreatment alanine aminotransferasevalues that were less than twice the upper limit ofthe normal range had clearance of H BeAg — arate similar to that for the spontaneous loss of thismarker. This finding suggests that by reducing theviral load, lamivudine allows the immune and in-flammatory responses to deal more effectively withthe remaining infected hepatocytes in the host.The principal limitation of lamivudine mono-therapy is the development of drug resistance,which is mediated largely by point mutations atthe YMDD motif at the catalytic center of the viralreverse transcriptase. The resulting mutants areslightly less fit than wild-type HBV in the absenceof the drug, but they are strongly selected for in itspresence.65 Viral resistance emerges much moreslowly in HBV infection than in HIV infection, forcomplex reasons beyond the scope of this review.By the end of one year of therapy, 15 to 20 percentof patients have resistant variants in the circula-tion; the figure rises to 40 percent by two years, andto 67 percent by the fourth year.66The clinical significance of the development ofresistance is still being debated. Clearly, in manypatients, resistance presages a return of higher-level viremia, and in some of these patients furtherliver injury develops. However, although the levelof viremia rises, in many patients it may still remainbelow pretreatment levels — perhaps as a resultof the reduced fitness of the variants. In addition,some patients continue to undergo conversion fromHBeAg-positive status to H BeAg-negative status,even after the appearance of lamivudine-resistantmutants in the circulation; by the end of four yearsof therapy, 40 to 50 percent of patients treated withlamivudine have undergone such conversion. There-fore, some experts favor the continuation of lamiv-udine therapy in patients with resistant variants but no evidence of overt clinical failure, especially since transient exacerbations of liver injury devel-op in some patients when antiviral therapy is with-drawn.67 (Such postwithdrawal flares are not lim-ited to lamivudine but have also been observed with other anti-H BV regimens.56,68) Now that newer anti-HBV drugs are available, additional options exist for patients with resistant strains of HBV .Other Nucleotide Analogues Recently, the Food and Drug Administration (FDA)approved a second antiviral drug, adefovir, to treat HBV infection. Adefovir, a nucleotide (adenosine monophosphate) analogue, is a prodrug that un-dergoes two intracellular phosphorylations to yield the active drug, an inhibitor of the viral polymer-ase. Initially developed as an inhibitor of HIV re-verse transcriptase, it proved nephrotoxic in the dos-es that were required for effective inhibition of HIV replication. However, in lower doses (10 mg per day)it has shown little nephrotoxicity and retains good efficacy against HBV in HBeAg-positive patients,with a reduction of 3 to 4 log in viremia; the fre-quency of HBeAg seroconversion is enhanced, and there is histologic improvement in the liver.68 Simi-lar efficacy was documented in HBeAg-negative pa-tients with abnormal liver function and elevated lev-els of viral DNA.56 Moreover, the drug effectively inhibits the replication of lamivudine-resistant HBV mutants, both in vitro and in vivo.69,70 Clear evi-dence of the emergence of adefovir-resistant HBV mutants has not been found in the clinical trials performed to date,56,68,71 although this issue re-mains open now that large numbers of patients will be using the drug.Tenofovir, another adenine nucleotide analogue that was approved by the FDA for the treatment of HIV , also has activity against the HBV polymerase.In recent trials in HIV carriers who were positive for HBeAg, treatment with standard doses of tenofovir led to a reduction of 4 log in circulating HBV DNA levels, even in patients who had evidence of lamiv-udine-resistant virus.72,73 H owever, the FDA has not yet approved tenofovir for use in patients with HBV infection. Several investigational drugs are now in ad-vanced stages of clinical trials. Entecavir is a guan-osine analogue that, unlike the drugs discussed above, is highly selective for the HBV polymerase and has no activity against HIV . It is extremely po-tent on a molar basis, and doses as low as 0.1 mg perThe New England Journal of Medicine as published by New England Journal of Medicine.Downloaded from on July 29, 2010. For personal use only. No other uses without permission.。

Acta virologica 57: 389 – 396, 2013 doi:10.4149/av_2013_04_389Hepatitis B virus-induced hepatocellular carcinoma: The role of thevirus x proteinM. MOTAVAF1, S. SAFARI1,2, M. SAFFARI JOURSHARI1,2 , S. M. ALAVIAN1,3*1Department of Molecular Hepatology, Middle East Liver Disease Center, Tehran, Iran; 2Department of Anesthesiology, Tehran University of Medical Sciences, Tehran, Iran; 3Baqiyatallah Research Center for Gastroenterology and Liver Diseases, BaqiyatallahUniversity of Medical Sciences, Tehran, IranReceived March 4, 2013; accepted October 4, 2013Summary. – Hepatocellular carcinoma (HCC) is one of the most common malignant diseases and has thefourth highest mortality rate worldwide. Chronic hepatitis B virus (HBV) infection has been identified as a majorrisk factor in HCC. Currently available evidence support a critical role of hepatitis B virus x (HBx) gene andprotein in the pathogenesis of HBV-induced HCC. HBx protein is a multifunctional regulator that modulatescellular signal transduction pathways, transcriptional regulations, cell cycle progress, DNA repair, apop-tosis, and genetic stability by interacting with different host factors. This review describes the currentstate of knowledge about the biological roles of this protein in the development of HCC.Keywords: hepatitis B x protein; hepatitis B virus; hepatocellular carcinoma; apoptosis; nuclear excisionrepair; epigenetic modificationsContents:1. Introduction2. HBV-specific mechanisms involved in HCC develop-ment3. HBx gene and HBx protein4. Different roles of HBx protein in hepatocarcinogenesis 4.1 Effects of HBx protein on epigenetic modifications 4.2 Effects of HBx protein on apoptosis4.2.1 A nti-apoptotic effects of HBx protein4.2.2 P ro-apoptotic effects of HBx protein4.3 Effects of HBx protein on DNA repair4.4 Effects of HBx protein on signal transduction andtranscription regulation5. Conclusion*Corresponding author. E-mail: alavian@thc.ir; phone: +98-2188945186.Abbreviations: DNMTs = DNA methyltransferases; HBV = hepa-titis B virus; HBx = hepatitis B x protein; HCC = hepatocellular carcinoma; MMP = matrix metalloproteinase; MTA = metastasis-associated protein; RAR-β2 = retinoic acid receptor β2; TSGs = tu-mor suppressor genes; XPB = xeroderma pigmentosum B1. IntroductionWith an annual incidence of more than 500,000 in the year 2000, HCC is considered to be one of the ma-jor malignant diseases in the world today (Motavaf and Alavian, 2012). Overall, 75–80% of global HCC cases are attributable to persistent viral infections with either HBV (50–55%) or hepatitis C virus (HCV) (25–30%) (Lu et al., 2006; Motavaf et al., 2012). Although this evidence indicates that HBV is a major etiologic factor in HCC (Alavian, 2011), the association of chronic HBV infection with HCC remains obscure. The hepatocarcinogenesis of HBV infection has been extensively analyzed, and multiple factors appear to play a role. Much of the evidence available supports the role of HBx gene and its expression product in the pathogenesis of HBV-related HCC. It is demonstrated that HBx gene is often included, and remains functionally active, in the HBV-DNA that is frequently integrated into cellular DNA during hepatocellular carcinogenesis. Several putative mechanisms by which HBx protein may contrib-ute to the development of HCC have been investigated. While the specific mechanisms are still unknown, its criti-390 MOTAV AF , M. et al.: MINIREVIEWcal role in hepatocarcinogenesis has been demonstrated by different in vivo and in vitro studies. Here, we attempt to summarize the current knowledge about carcinogenic pathways in HBV-induced HCC, with a focus on the role of HBx protein.2. HBV-specific mechanisms involved in HCCdevelopment Chronic HBV infection is the primary risk factor for the development of HCC (Mahboobi et al ., 2010). After decades of chronic hepatitis, about 30–40% of patients progress into liver cirrhosis, and of them, around 1–5% subsequently develop HCC (Liu and Kao, 2007).Intensive research has focused on the role of HBV in hepatocarcinogenesis for the past decades. Current evidence points to two major HBV-specific mechanisms that contrib-ute to the development of HCC. The first mechanism is the integration of HBV-DNA into host cellular DNA, which is observed in approximately 85% of HBV-associated tumors and is crucial during HBV chronic infection. Integration of HBV-DNA causes cis-effects, which by direct act in the genome disrupt or promote expression of cellular genes that are important in cell growth and differentiation. The second mechanism involves the expression of trans-activating fac-tors encoded by HBV genome, which have the potential to influence intracellular signal transduction pathways and alter host gene expression indirectly. Several HBV trans-activating factors such as the HBx protein, the PreS2 activators, and a novel spliced transcript of HBV , referred to as the hepatitis B spliced protein (HBSP) have been found to be implicated in hepatocarcinogenesis (Su et al ., 2008). An increasing number of studies suggest that HBx protein may contribute to the development of HCC by interfering with differentcellular activities.Fig. 1Scheme of various targets of HBx protein in the cellMOTAV AF, M. et al.: MINIREVIEW3913. HBx gene and HBx proteinThe HBV genome is a 3.2 kb circular, partially double-stranded DNA molecule with four overlapping open reading frames (ORFs), which code for the viral envelope (pre-S1/ pre-S2/S), core proteins (pre-C/C), viral polymerase, and HBx protein. Among the proteins originating from the HBV genome, the HBx protein has drawn much attention for its pleiotropic functions as a viral trans-activator playing dif-ferent roles in the development of HCC. The HBx gene that codes the HBx protein is phylogenetically highly conserved among all mammalian hepadnaviruses, strongly suggesting that it plays a critical role in viral life cycle. This gene com-prises 452 nucleotides that encode HBx protein. The protein is 154 aa long with a molecular mass of 17 kDa. HBx protein operates as a multifunctional regulator that can modulate various cellular processes, including signal transduction cascades, transcriptional pathways, cell cycle progress, DNA repair, apoptosis, cell proliferation and genetic stability by interacting with different host factors. Currently available evidence supports multiple roles for the HBx protein in the pathogenesis of HBV-induced HCC (Fig. 1).4. Different roles of HBx protein in hepatocarcinogenesis4.1 Effects of HBx protein on epigenetic modificationsEpigenetic modifications refer to alterations in gene ex-pression with no underlying changes in the genetic sequence itself. These alterations can switch genes on or off and de-termine which proteins are transcribed. Within cells, there are three systems that epigenetically silence the genes: DNA methylation, histone modifications, and RNA-associated silencing. Disrupting any of these three systems can cause abnormal activation or silencing of genes. Such disruptions have been associated with different disorders including cancer, syndromes involving chromosomal instabilities, and mental retardation. DNA methylation plays an important role for epigenetic gene regulation in development and dis-ease. It is catalyzed by a family of DNA methyltransferases (DNMTs), including DNMT1, DNMT3a, and DNMT3b (Be-stor et al., 1988; Okano et al., 1998). DNMT1 is responsible for the maintenance of DNA methylation after each round of replication. DNMT3a and DNMT3b are the main players involved in de novo methylation during early development. This family catalyzes the transfer of a methyl group to the C-5 position of cytosine in CpG dinucleotide, using S-adenosyl methionine as the methyl donor. The increased expression of DNMT1 and DNMT3a has been shown to be associated with increased cell proliferation, tumorigenesis, and tumor progression. Thus, elucidation of the mechanism for DNMT1 and DNMT3a up-regulation may provide an important clue for the understanding of epigenetic alterations in tumors. Studies indicated that DNMT1 and DNMT3a expres-sion is significantly higher in HCC when compared with non-neoplastic liver tissues (Saito et al., 2001). HBx protein has been contributed to the up-regulation of DNMT1 and DNMT3a expression at both the mRNA and protein levels (Jung et al., 2007). By virtue of this ability, HBx protein is suggested to be involved in epigenetic modifications during hepatocarcinogenesis.DNA in CpG rich islands (genomic regions that contain a high frequency of GC dinucleotide) in the promoter re-gions of the TSGs is a common target for methylation by DNMT1. One of the important results of this methylation is inactivation of TSGs, leading to tumor development by eliminating negative regulatory proteins. The observation of methylation in 82% of at least one TSG promoter dur-ing hepatocarcinogenesis demonstrates the importance of this mechanism in HCC development (Yang et al., 2003). Methylation of the p16INK4A promoter, a potent TSG is an important early event in carcinogenesis. It has been demonstrated that up-regulation of DNMT1 and DNMT3a by HBx protein is one of the leading causes of p16INK4A promoter methylation resulting in its inactivation (Zhu et al., 2010). P16INK4A is one of the cyclin-dependent kinase inhibitors (CDKIs) and acts as a negative cell cycle regulator. Its functional inactivation is shown to be one of the most frequent alterations in HCC.By inducing DNMT1 transcription, HBx protein also represses the expression of the E-cadherin gene (Lee et al., 2005). E-cadherin plays a well-established role in cell-cell adhesion, ensuring that cells within tissues are bound to-gether. The adhesive function of E-cadherin is dependent on its binding to the cytoplasmic α- and β-catenin proteins, two components of adherence junctions, which serve as a link between E-cadherin and the cytoskeleton. In a variety of cancers, including HCC, reduced expression of E-cadherin has been correlated with disruption of cell-cell contacts and enhanced cancer cell invasion. Binding of E-cadherin to β-catenin also suppresses cell growth and transformation. In addition, β-catenin plays an essential role in the Wnt signaling pathway. Activation of the Wnt signaling pathway leads to nuclear translocation of β-catenin where it func-tions as transcriptional regulator. Suppression of E-cadherin has important ramifications upon β-catenin function and consequently Wnt signaling pathway. Normally by binding to β-catenin, E-cadherin sequesters it at the membrane and keeps it away from the nucleus resulting in inhibition of β-catenin/Wnt signaling pathway. When E-cadherin expres-sion is suppressed, β-catenin is released and translocates to the nucleus. Excessive accumulation of β-catenin in nucleus induces overactivation of β-catenin/Wnt signaling pathway, which results in enhanced cell growth and malignant cel-392 MOTAV AF, M. et al.: MINIREVIEWlular transformation. This suggests that HBx protein may promote elevated β-catenin/Wnt signaling, in part, by down-regulation of E-cadherin.By up-regulating DNMTs expression, HBx protein also induces methylation of the insulin-like growth factor binding protein 3 (IGFBP-3) promoter, which suppresses IGFBP-3 expression (Park et al., 2007). IGFBP-3 is an anti-proliferative, pro-apoptotic, and anti-tumor protein. Thus, its suppression can be associated with cancer progression. The ankyrin-repeat-containing, SH3-domain-containing, and proline-rich-region-containing protein1 (ASPP1) and ASPP2 family of proteins regulate apoptosis through inter-action with p53 and enhancing its binding to promoters of pro-apoptotic genes. The expression of ASPP2 and ASSP1 genes is frequently down-regulated by DNA methylation via increased DNMT expression in HBV-positive HCC, which may play important role in the development of HCC. (Samuels-Lev et al., 2001; Zhao et al., 2010).HBx modulates the function of retinoic acid (RA) with up-regulation of retinoic acid receptor (RAR) β. RA regulates important biological processes such as cell proliferation, cell differentiation and cell death. It has been reported that RA acts as inhibitor of carcinogenesis by blocking the promotion of cell-transformation via induction of apoptosis, inhibition of further growth of abnormal cells and induction of abnor-mal cells to re-differentiate back to normal. Their signal can be transduced through two families of receptors including RAR (alpha, beta and gamma) and retinoid X receptor (RXR). HBx protein has been shown to induce promoter methylation of RAR-β2 via up-regulation of DNMT1 and DNMT3a resulting in down-regulation of its expression in human HCC cells. Because RAR-β2 is a major executor of the anti-tumor activity of retinoic acid, its down-regulation is likely to be an important event in HCC (Jung et al., 2010). Methylation also abolishes the potential of retinoic acid to down-regulate levels of G1-checkpoint regulators including p16, p21, and p27. This leads to activation of transcription factor E2F1, which plays a crucial role in the control of cell. As a result, in the presence of HBx protein, cells are less susceptible to RA-induced growth inhibition.It has recently been demonstrated that HBx protein is able to deregulate cellular micro-RNA expression. miRNAs are small noncoding RNA molecules that inhibit gene expression by interacting with target mRNAs. miRNAs have been shown to exhibit regulatory functions in numerous cellular proc-esses, including proliferation, differentiation, and apoptosis. They can function as either oncogenes or tumor suppressors through the suppression of protein-coding genes involved in cancer development and progression. Different studies pro-vide evidence for the ability of HBx protein to deregulate cel-lular miRNAs expression (Wang et al., 2010; Xu et al., 2013). Although the function of many of these miRNAs remains largely unknown, but functional studies illustrated the role of a number of them in hepatocarcinogenesis. For instance miRNA let-7, a negative regulator of cellular proliferation is one of these miRNAs, which expression was shown to be down-regulated by HBx protein (Wang et al., 2010).4.2 Effects of HBx protein on apoptosisMaintenance of normal tissue homeostasis mainly de-pends on the balance between cell proliferation and pro-grammed cell death (apoptosis). Apoptosis is responsible for the removal of infected, damaged, cancerous cells and cells that are simply in the wrong place during development. Apoptosis can be mediated through various extrinsic or intrinsic signal pathways, with activation of caspases and the possible involvement of mitochondria. The effect of HBx protein on apoptosis is one of the most fully documented mechanisms by which it contributes to the development of HCC. These effects are complex, because HBx protein has both anti-apoptotic and pro-apoptotic effects.4.2.1 Anti-apoptotic effects of HBx proteinA number of ways in which HBx protein may induce anti-apoptotic effects have been described in different studies. HBx protein has been demonstrated to function as inhibitor of p53-mediated apoptosis. The main role of p53 is maintain-ing the integrity of the genome in response to stress signals including oxidative stress, metabolic stress, and DNA dam-age by inducing growth arrest, or apoptosis. In response to these stress signals, p53 is imported into the nucleus, where it induces cell cycle arrest, allowing for repair of damage or p53-dependent apoptosis (Ellis et al., 1991). It is suggested that HBx protein reduces the concentration of nuclear p53 by cytoplasmic sequestration of this apoptosis inducer (Wang et al., 1995). One consequence of this effect is the failure of p53 to up-regulate genes involved in apoptosis (Feitelson, 2006). p53 also plays a role in induction of apoptosis via binding to the xeroderma pigmentosumB (XPB) and XPD compo-nents of the transcriptional factor II H (TFIIH), which are involved in induction of apoptosis. Binding of HBx protein to the C-terminal of p53 and inhibiting its binding to XPB and XPD, may disrupt p53 induced apoptosis.HBx protein can also exert anti-apoptotic functions in-dependently of p53 via modulating activities of the serine protease hepsin and up-regulation of survivin (Zhang et al., 2005b). Survivin is a member of the apoptosis-inhibitor protein family, which is implicated in both the control of cell division and the inhibition of apoptosis. By inhibiting apoptosis and stimulating mitosis, survivin simplifies cancer cell survival and growth. Furthermore, survivin can form complexes with HBx-interacting protein (HBxIP), a cellular protein which was originally recognized for its association with HBx protein. Survivin-HBxIP complexes bind to pro-caspase 9, preventing its recruitment to apoptotic proteaseMOTAV AF, M. et al.: MINIREVIEW393activating factor 1 (Apaf1), and thereby suppressing initiated mitochondrial apoptosis pathway. HBx protein is able to interact with such complexes and suppress caspase activa-tion in a surviving-dependent way. Findings show that HBx protein is a potent caspases-3 inhibitor as well (Gottlob et al., 1998). HBx protein may inhibit apoptosis by activating methionine-adenosyltransferase II alpha (MAT2A) expres-sion through NF-κB and cAMP-response-element-binding protein (CREB) signaling pathways, resulting in the decrease of S-adenosyl-methionine production (Liu et al., 2011).4.2.2 Pro-apoptotic effects of HBx proteinIn addition to its anti-apoptotic effects, HBx protein may also induce apoptosis by different mechanisms such as deregulating Fas/FasL death receptor pathway, Bax/Bcl-2 family-induced mitochondrial pathway, activity of cFADD-like interleukin-1 beta-converting enzyme (cFLICE), expression of heat shock protein 60 (HSP60) and HSP70, expression of DNA damage-binding protein 1 (DDB1) and activity of NF-κB (Kim et al., 2008; Kim and Seong, 2003; Kim et al., 2005). It is demonstrated that the HBx protein sensitizes cells to apoptotic killing when expressed during viral replication. Cells that were resistant to apoptotic killing by high doses of TNFα were made sensitive to very low doses of TNFα by HBx protein (Su and Schneider, 1997). Produc-tion of TNFα is often part of the immune responses associ-ated with liver damage during HBV infection. HBx protein sensitizes cells to TNFα killing by prolonged stimulation of n-myc (a proto-oncogene) and the stress-mediated mitogen-activated-protein kinase kinase 1 (MEKK1) pathway, but it has no effect on regulation of TNFα receptors. Interaction of HBx protein with mitochondria, which is associated with the abnormal aggregation of mitochon-drial structures in the cell (Takada et al., 1999) is another possible mechanism underlying HBx-related apoptotic cell death. It is also indicated that by causing the loss of mitochondrial membrane potential, HBx protein induces mitochondria-dependent apoptosis (Shirakata and Koike, 2003). Furthermore, HBx protein can form a complex with mitochondrial proteins, HSP60 and HSP70 that exerts effects on mitochondria-dependent apoptosis (Zhang et al., 2005a). HBx protein also may alter mitochondrial function by asso-ciation with a member of the family of human mitochondrial voltage-dependent anion channel (HVDAC3) (Rahmani et al., 2000). Such functional roles of HBx protein, resulting in mitochondrial dysfunction and structural changes, have implications for HBV-induced liver injury and the develop-ment of HCC.4.3 Effects of HBx protein on DNA repairDNA repair systems are fundamental to the maintenance of genomic integrity through the recognition and repair of damaged or altered DNA. The nucleotide excision repair (NER) pathway is responsible for the repair of a number of DNA lesions. DNA repair is achieved by the collaboration of the products of as many as 30 genes. The transcriptional fac-tor II H, which includes XPB and XPD subunits, is involved in NER. It is thought that by interacting with XPB/XPD and inhibiting their translocation from sites of damaged DNA, p53 stabilizes the formation of repair complexes. Both in vitro and in vivo studies have shown that HBx protein can bind and disrupt the p53 binding to XPB and XPD. The binding domain of p53 for interaction with HBx protein has been mapped between aa 293–393 (Abdel-Hafiz, 2011), which also binds to XPB and XPD. Thus HBx protein may interfere with the NER pathway by covering this domain and blocking p53 from binding to XPB and XPD.HBx protein in liver cells is also able to down-regulate XPB and XPD expression in specificity protein 1 (Sp1)-dependent manner. Sp1 is one of the transcription factor responsive elements that are present in both XPB and XPD promoters. Sp1 has been shown to be a specific target for HBx protein resulting in impairment of its DNA binding properties and down-regulation of XPB and XPD.4.4 Effects of HBx protein on signal transduction and transcription regulationThe HBx protein is known as a dual-specificity trans-activator exerting both in the cytoplasm, via modulating intracellular signal transduction cascades, and in the nucleus, via interfering directly with transcription factors. Nuclearly localized HBx protein has been shown to up-regulate the expression of a number of cellular and viral genes including the HBV enhancers, RPB5 subunit of RNA polymerase II, TATA-binding protein, and proto-oncogenes such as c-jun, c-fos, and c-myc. Furthermore, HBx protein has been shown to activate transcriptional factors such as NF-κB, activator protein 1 (AP-1), AP-2, and activating transcription factor (ATF)/ CREB (Balsano et al., 1991; Chirillo et al., 1996; Kim et al., 2010; Twu et al., 1993). HBx protein also activates promoters of cellular genes associated with cell proliferation, such as IL-8, TNF, TGF-β1, and early growth response factor (EGRF) (Andrisani and Barnabas, 1999). TGF-β1 signaling involves phosphorylation of Smad3 at serine residues 208 and 213 in the linker region (Smad3L) and serine residues 423 and 425 in the C-terminal region (Smal3C). Smad3C pathway inhibits growth of cells in vivo, but Smad3L-mediated signaling promotes tumor cell proliferation by up-regulating c-myc oncoprotein. It has been observed that HBx protein shifts hepatocytic TGF-β1 signaling from the tumor-suppressive pSmad3C pathway to the oncogenic pSmad3L pathway in early carcinogenesis (Murata et al., 2009). HBx protein localized in the cytoplasm, has been shown to activate signal transduction pathways such as394 MOTAV AF, M. et al.: MINIREVIEWRas-Raf-mitogen-activated protein kinase (MAPK) pathway (Benn and Schneider, 1994), JAK/STAT pathway (Lee and Yun, 1998), the cell stress-induced MEKK1-p38-c-Jun N-terminal kinase (JNK) pathway (Benn et al., 1996). HBx protein may also contribute to tumorigenesis in HCC through modulation of the angiogenesis pathway. It is demonstrated that HBx protein up-regulates the transcrip-tion of vascular endothelial growth factor (VEGF), a potent angiogenic factor, by stabilizing or even up-regulating the hypoxia inducible factor 1 (HIF-1) (Lee et al., 2000). HIF-1 is also the main transcriptional activator of carbonic an-hydrase 9 (CA9). CA9 is involved in pH regulation, which helps tumor cells overcome intracellular acidosis and sur-vive extended periods of time in hypoxic conditions. Thus, increased expression of CA9 results in the development of HCC by contributing to the survival of hepatocytes infected with HBV in the fibrotic liver parenchyma (Holotnakova et al., 2010). Moreover, HBx protein plays an important role in facilitating invasion and metastasis by enhancing cellular migration through up-regulation of transcription of matrix metalloproteinase 2 (MMP-2), MMP-9, MMP-3, MMP14, MT1-MMP, and cyclooxygenase-2 (COX-2) (Lara-Pezzi et al., 2002; Liu et al., 2010b; Ou et al., 2007). MMPs degrade extracellular matrix components, thereby contributing to physiological events (wound healing, and angiogenesis) and pathological conditions (cancer and arthritis).HBx protein has been shown to induce the expression of metastasis-associated protein 1 (MTA1) co-regulator, via NF-κB signaling in hepatic cells. It is a component of the nuclear remodeling and histone deacetylase complex involved in carcinogenesis. MTA1 is a positive regulator of inducible nitric oxide synthase (iNOS) transcription as well (Bui-Nguyen et al., 2010). The HBx/MTA1 complex stimu-lates the production of nitric oxide (NO°), by stimulation of iNOS expression in an NF-κB-dependent manner. NO° is a free radical, producing many reactive intermediates that account for NO°-mediated DNA damage or inhibition of DNA repair.HBx protein has also been shown to up-regulate the expression and activity of human telomerase reverse transcriptase (hTERT) (Liu et al., 2010a; Zou et al., 2004), which is the one of the primary mechanisms underlying the proliferation, differentiation and tumorigenesis. hTERT is a catalytic subunit of the enzyme telomerase that maintains DNA telomere ends. Telomerase activity is associated with the number of times a cell can divide playing an important role in the immortality of cancerous cell lines.5. ConclusionHCC is one of the most prevalent and lethal cancers worldwide. Considerable efforts are currently aimed at unraveling the underlying molecular mechanisms of HCC in order to design better treatments, or even to prevent the disease. Chronic HBV infection is a major risk factor for HCC, but the pathogenesis of HBV-mediated HCC is not completely understood. Evidence suggests that the HBx pro-tein plays a crucial role in hepatocarcinogenesis. Although further research is needed, these data give us insight into un-derstanding the cell-transforming potential of HBx protein. Elucidating the role of HBx protein in hepatocarcinogenesis may ultimately lead to novel therapeutic strategies in the management of patients with HCC.ReferencesAbdel-Hafiz H (2011): Role of Hepatitis B virus X protein in DNA repair during hepatocellular carcinoma development. J.Carcinogen. Mutagen. S 3, 37–39.Alavian SM (2011): New globally faces of hepatitis B and C in the world. Gastroenterol. Hepatol. Bed Bench 4. Andrisani OM, Barnabas S (1999): The transcriptional function of the hepatitis B virus X protein and its role in hepatocar-cinogenesis (Review). Int.l J. Onc. 15, 373–379. Balsano C, Avantaggiati ML, Natoli G, De Marzio E, Will H, Per-ricaudet M, Levrero M (1991): Full-length and truncatedversions of the hepatitis B virus (HBV) X protein (pX)transactivate the cmyc protooncogene at the transcrip-tional level. Biochem. Bioph. Res. Co. 176, 985–992./10.1016/0006-291X(91)90379-L Benn J, Schneider RJ (1994): Hepatitis B virus HBx protein activates Ras-GTP complex formation and establishes a Ras, Raf,MAP kinase signaling cascade. PNAS USA 91, 10350–10354. /10.1073/pnas.91.22.10350 Benn J, Su, F, Doria M, Schneider RJ (1996): Hepatitis B virus HBx protein induces transcription factor AP-1 byactivation of extracellular signal-regulated and c-JunN-terminal mitogen-activated protein kinases. J. Virol.70, 4978–4985.Bestor T, Laudano A, Mattaliano R, Ingram V (1988): Cloning and sequencing of a cDNA encoding DNA methyltransferaseof mouse cells. The carboxyl-terminal domain of themammalian enzymes is related to bacterial restrictionmethyltransferases. J. Mol. Biol. 203, 971–983. http:///10.1016/0022-2836(88)90122-2Bui-Nguyen TM, Pakala SB, Sirigiri DR, Martin E, Murad F, Kumar R (2010): Stimulation of inducible nitric oxide by hepa-titis B virus transactivator protein HBx requires MTA1coregulator. J. Biol. Chem. 285, 6980–6986. http://dx.doi.org/10.1074/jbc.M109.065987Chirillo P, Falco M, Puri PL, Artini M, Balsano C, Levrero M, Natoli G (1996): Hepatitis B virus pX activates NF-kappaB-dependent transcription through a Raf-independentpathway. J. Virol. 70, 641–646.Ellis RE, Yuan J, Horvitz H (1991): Mechanisms and functions of cell death. Ann. Rev. Cell Biol. 7, 663–698. http://dx.doi.org/10.1146/annurev.cb.07.110191.003311。
Hepatitis B virus and hepatocellular carcinomaJordi Bruix *,Josep M.LlovetBCLC Group,Liver Unit,Digestive Disease Institute,Hospital Clı´nic,IDIBAPS,University of Barcelona,Villarroel 170,08036Barcelona,Spain1.IntroductionThe development of hepatocellular carcinoma (HCC)is a major global health problem [1,2].Its incidence has increased worldwide and nowadays it constitutes the 5th most frequent cancer representing around 5%of all cancers worldwide [2].More than 500,000new cases are diagnosed per year and it represents the third cause of cancer-related death and the first cause of death amongst cirrhotic patients [3–5].HCC incidence has striking geographical differences [1].In North America,Europe and Australia the age-adjusted incidence is less than 2/100,000per year.This increases in the South European and Mediterranean countries and reaches the highest scores (.50/100,000)in Sub-Sahara Africa and South East Asia [1].This geographic pattern overlaps with the distribution of risk factors and probably also reflects genetic characteristics inherited or acquired through oncogenic agents.While in some high risk areas the incidence has decreased as a result of a better health care of the population,the HCC incidence in several areas such as US and South Europe has increased.This may be due both to an increased disease awareness with a higher diagnostic capability,but also to the emergence of risk factors which up to now would have had a minor dissemi-nation and thus,no impact.This is probably the case for hepatitis C virus (HCV)-related HCC that should represent the final step of the HCV epidemic that spread in some Western countries after the second world war,while in Asia it could have appeared decades before.The most relevant oncogenic agent for HCC development is chronic hepatitis B virus (HBV)or HCV infection [1,6].Their prevalence is known to vary largely among the world population.Not unexpectedly,areas with high prevalence of viral infection have high HCC rates [1].This association allowed the establishment of the relationship between HBVinfection and HCC.Other risk factors such as alcoholism or hemochromatosis are also relevant,but have not yet reached the epidemiological and clinical importance of viral infec-tion.In most cases,HCC development complicates an underlying chronic liver disease,but in all etiological categories the tumor may occur in the absence of cirrhosis or when minimal histologic changes have taken place.The present chapter reviews the evidence that links HCC development with HBV infection,summarizes the mech-anisms that may be involved in the HBV carcinogenic pathway and finally provides the guidelines to achieve early diagnosis and effective therapy.2.Epidemiological relationship between HBV infection and HCCData linking HBV with HCC were raised soon after the discovery of the ‘Australia Antigen’(corresponding to the hepatitis B surface antigen –HBsAg).Several epidemio-logical surveys demonstrate the geographic coincidence between HBV endemicity and HCC prevalence [7].In South-East Asia the prevalence of HBV infection reaches 10–15%and the HCC rate ranges between 10and 25/100,000population [1,8,9].In all areas the prevalence of serological markers of past or present HBV infection is higher in HCC patients than in those without this tumor.Figures may vary according to the background rate in the global population and may depend on the techniques employed to assess the existence of viral infection.HBV DNA might be found in the tumor and non-tumor liver tissue of HCC patients in whom serological markers may be negative or only positive for anti-HBc [10].Accordingly,both in low and high incidence areas,the role of HBV in HCC development is very relevant.In addition to cross-sectional studies,cohort studies have established that chronic HBV infection carries an increased HCC risk and thus,of cancer related death [6,8].Again,big differences0168-8278/03/$30.00q 2003European Association for the Study of the Liver.Published by Elsevier B.V.All rights reserved.doi:10.1016/S0168-8278(03)00140-5Journal of Hepatology 39(2003)S59–S63/locate/jhep*Corresponding author.Fax:þ34-4-227-9803.E-mail address:jbruix@clinic.ub.es (J.Bruix).have been observed depending on the geographic area and the presence or absence of an underlying liver disease.In the seminal study by Beasley et al.including more than22,000 Taiwanese men the risk in chronic HBV carriers was100 times higher than in non-infected individuals[11].A Japanese study performed also in males found afifty-fold increased risk in HBV infected individuals[12].Studies performed in Alaska[13],Europe[3,14]and Canada[15] have established that the increased risk applies world-wide. However,while in Asian patients the tumor appears more frequently in an otherwise normal liver,in the Caucasian population HCCs mostly develop in patients with chronic liver disease,namely cirrhosis.Patients with HCC in a normal liver are usually younger and this may support the role of age at infection.The coexistence of additional oncogenic agents in those areas where the infection is acquired perinatally or during childhood may also be rele-vant.This might be the case for aflatoxin,a carcinogen that contaminates food stored in humid conditions[16].It induces a unique missense mutation of codon249of the p53 gene[17].While this is observed at early HCC stages in Asian patients,this genetic signature is rarely observed in Western tumors.The annual HCC incidence in chronic HBV carriers in Asia ranges between0.4and0.6%.This figure is lower in Alaskan natives(0.26%/year)and even lower in Caucasian HBV carriers.The incidence in cirrhotics exceeds2%in all areas.Male sex,advanced age (a potential surrogate for the disease duration)and increased alphafetoprotein(AFP)are associated with higher risk[6].Thefinal demonstration of the role of HBV in the development of HCC comes from the preventive effect of vaccination.In Taiwan this has prompted a reduction of the prevalence of HBV infection in children from15to1% and also a60%reduction of HCC during childhood[18]. Considering that more than70%of HCC in developing countries is attributable to HBV,the current challenge is to ensure the availability of the vaccine in all these countries. Other preventive measures should be addressed at public health campaigns to reduce food contamination by fungi, as well as to modulate the metabolism of aflatoxins once ingested,as has been proposed by the use of oltipraz.Dosage and schedule parameters for its administration have been described in a phase II study in Qidong,China[19,20],where HCC is the leading cause of death and exposure to dietary aflatoxins is widespread.However,long-term outcome of randomized controlled trials(RCTs)are not yet available.3.Oncogenic mechanismsThe oncogenic mechanisms of HBV are not fully understood[9,21,22].HBV DNA may integrate into the genome of the hepatocytes[23]and this may cause several hits leading to transformation.However,HBV DNA integration is random and involves always different parts of the viral genome.The viral X gene may have an important role as it is a powerful transactivator for transcription of oncogenes such as c-myc and c-jun.Additional events that may be triggered by HBV DNA integration and X gene expression deregulation include DNA repair impairment, increased cytokine production and growth factors,inhibition of apoptosis and increased expression of angiogenic agents such as vascular endothelial growth factor and nitric oxide [9,21].This last agent may act as a potent mutagen[24]and can be induced both by HBV infection or the inflammation associated to chronic hepatitis.Recent human studies suggest that HBV positive HCC are characterized by higher chromosomal instability leading to loss of heterozygosity as compared to tumors related to HCV[25].However,there is no clear-cut HBV related genetic profile leading to HCC[26].As mentioned above,in most cases HCCs appear in a cirrhotic liver after many years of inflammation,cellular necrosis and regeneration that define a microenvironment that is characterized by the release of several cytokines, growth factors and other mediators.This may affect the hepatocytes,promote oxidative stress and prompt the appearance of a critical genetic damage irrespective of the virus itself.4.Early detection and diagnostic confirmationMortality from HCC may decrease due to effective implementation of preventive strategies and,less impor-tantly,early detection and effective treatment.Prevention will be achieved by vaccination and by drugs that eradicate the virus prior to irreversible hepatic and/or genetic damage. In patients with chronic hepatitis B,interferon-a lamivu-dine,adefovir and other antiviral agents will reduce the incidence of cirrhosis,and also of HCC.If cirrhosis is established there is no agent that has been proven to diminish the HCC risk[6,27,28].Therefore,in this setting the only option to decrease cancer related deaths will be early detection.Early detection might be achieved by surveillance of the population at risk and its cost-effectiveness will depend on successful therapy.Thus,careful selection of patients for surveillance is mandatory.HCC meets most of the accepted criteria to establish surveillance[29].It is a frequent event in the population at risk.This can be identified and the disease causes significant morbidity or mortality.The population should accept the surveillance strategy and this has to have a high detection and diagnostic accuracy.Abnormal results have to be clearly defined and the investigations necessary must be well established.Finally,effective therapy should be available.There are no RCTs demonstrating a survival benefit of surveillance.The available evidence is derived from cohort studies showing that the proportion of patients diagnosed at an early stage,and thus amenable for effective treatment, is increased as compared to patients not included intoJ.Bruix,J.M.Llovet/Journal of Hepatology39(2003)S59–S63 S60surveillance[5,6].Cost-effectiveness has been assessed from cohort studies and multistage transition modelling [5,30,31].An adequate relationship is achieved if surveil-lance is performed in patients with significant risk and if all treatments with positive impact are available and properly indicated to achieve the best possible outcome.Based on the incidence of HCC in patients with HBV cirrhosis,surveillance is indicated irrespective of the racial background.In non-cirrhotics the evidence is controversial. The0.4–0.6%yearly risk of Asian HBV carriers justifies their surveillance.The very low risk in Caucasians, however,results in a low number of detected HCCs and a reduced cost-effectiveness[6].It is important to stress that only those individuals who could be treated should enter the program while those who are not candidates for curative therapy should be excluded.Therefore,the ideal target population are patients with normal liver function or with Child-Pugh A cirrhosis.Child-Pugh C cirrhotics should be evaluated for liver transplan-tation in the absence of an HCC.If this option is not feasible,there will be no benefit from surveillance.Child-Pugh B cirrhotics are a controversial group.Without liver transplantation it is very unlikely that any therapy will offer a significant survival benefit and hence,they should probably not become a target group for surveillance.4.1.Surveillance for HCCThe growth of small HCC from undetectable to2cm takes about4–12months[6].Aiming to detect tumors smaller than3cm in diameter,a6-month interval has been set for surveillance.Patients with increased risk do not require shorter intervals,because increased risk does not mean faster growth.The surveillance tools are AFP and ultrasonography(US).AFP is not a very good screening test.Its sensitivity is39–64%,its specificity 76–91%and its positive predictive value9–32%[6,15, 32,33].AFP as the only tool for surveillance has not been properly investigated and this has maintained it in most surveillance is a more effective tool.As a screening test in HBsAg carriers,it has a sensitivity of 71%and a specificity of93%,with a reduced positive predictive value of14%[15].US should be conducted by an experienced operator.If US or AFP are abnormal,the patients should be referred to a comprehensive cancer unit offering the most updated human and technical resources[6].4.2.Recall procedures and diagnostic confirmationThis is an area of clinical research.There are no pros-pective studies assessing the efficacy of different strategies. In the recent EASL Monothematic Conference on HCC a panel of experts proposed a set of guidelines depicted in Fig.1[6].The US discovery of a hypo-or hyperechoic nodule during follow-up should raise a HCC suspicion,depending on size.Pathological studies have shown that 50%of nodules,1cm are not malignant[34]and the available diagnostic techniques do not allow proper classification.Therefore,US control of the nodules every 3months is recommended until disappearance or progres-sive growth to.1cm.Even a true HCC may remain stable for more than1year and thus,absence of growth during the follow-up period does not exclude malignancy.For lesions.1cm HCCs are more likely and diagnostic confirmation is required.A positivefine needle biopsy (tissue sample for cytology and histology)was felt mandatory for nodules,2cm because the imaging techniques are not sufficiently accurate.By contrast,in cirrhotic patients,the incidentalfinding of a hepatic nodule .2cm showing arterial hypervascularization in at least two imaging techniques(US,CT,angiography and magnetic resonance imaging)may suffice to establish the diagnosis(Table1)[34].In fact,with these characteristics, a negative biopsy will not rule out an HCC and thus,this result will not change the clinical diagnosis.AFP.400ng/ ml may also establish the diagnosis,if coinciding with a highly suspicious hepatic nodule in a cirrhotic liver[6,33]. However,transient AFP increases might be observed coinciding with inflammatoryflares[35]and thus,care should be taken to properly characterize the hepatic nodules through imaging techniques.In any case,the request for a diagnostic biopsy should take into account the impact of the result on the clinical decision making and the balance between the potential risks of biopsyand Fig.1.Surveillance and recall strategy[6].(Reproduced from Bruix et al.[6],with permission.)Table1Diagnostic criteria for HCC[6]X Cyto-histological criteriaX Non-invasive criteria(cirrhotic patients)1.Radiological criteria:two coincidental imaging techniques a–Focal lesion.2cm with arterial hypervascularizationbined criteria:one imaging technique associated to AFP–Focal lesion.2cm with arterial hypervascularization–AFP levels.400ng/mla Four techniques considered:US,Spiral CT,MRI and angiography.J.Bruix,J.M.Llovet/Journal of Hepatology39(2003)S59–S63S61the risk of invasive treatments(i.e.transplantation)to be applied thereafter.There are no robust data to define the recall policy for patients who present an increased AFP value.In the absence of a coincidental nodule on US a triple phase CT scan may be needed to rule out an HCC.If negative,a persistently increased AFP classifies the patient as a high risk individual for HCC development[6].Applying this surveillance strategy40–80%of the detected HCC are solitary,but only half of them are suitable for curative treatment after careful evaluation[5,6].5.Treatment of HCCPatients diagnosed with early stage HCC benefit from radical options(surgery,percutaneous ablation)that provide a high rate of complete responses according to oncologic criteria[6,36,37].An untreated control arm to test the impact of these options is not ethical and the survival benefits from treatment have been derived from cohort studies.By contrast,the absence of effective therapies for advanced HCC has allowed the conduction of several RCTs comparing some of the available alternatives versus no treatment[6,36].5.1.Treatment of early HCCThere are no studies comparing the available curative treatment options–resection,liver transplantation and percutaneous ablation–against no treatment or amongst themselves.Thus,there are no data to establish thefirst-line treatment in patients with HCC in compensated cirrhosis. Each group,center and country should establish the pre-ferred schedule taking into account the results of cohort studies and the available resources[6,36].However,in patients with early HCC in decompensated liver disease,the outcome after transplantation is clearly superior to other alternatives.Surgical resection is considered for single asymptomatic HCC in patients with preserved liver function.The Child-Pugh classification is not adequate to select surgical candi-dates,since even Child-Pugh A may include relevant functional impairment and minor ascites.Indocyanine green retention rate or the selection of patients with normal bilirubin and no portal hypertension identify the candidates that will achieve a70%5-year survival[36,38].Vascular invasion,satellites and poor differentiation are associated with an increased risk of recurrence of up to more than70% within5years and no effective prevention of recurrence [36–38].The optimal candidates for transplantation are patients with early HCC(single lesion,5cm or up to three lesions ,3cm)with a70%5-year survival and a recurrence rate below15%[36,37].Transplantation is not available world-wide and there is a severe shortage of donors.Antitumoral treatments upon listing may benefit some patients,but there are no RCTs to prove their efficacy.One of the major risks after transplantation is the re-infection of the graft.Hyper-immune globulin and new antiviral agents discussed else-where in this issue markedly reduce this risk and allow optimal graft and patient survival.Percutaneous ethanol injection(PEI)under US guidance achieves a complete response in70–80%of solitary tumors ,3cm.Child-Pugh A cirrhotics may achieve a50%5-year survival.By contrast,survival benefits of PEI in Child-Pugh B class patients are controversial.PEI is inexpensive and carries almost no treatment related mortality.Hence,it constitutes the standard technique against which new options have to be compared[36–38].5.2.Treatment of intermediate/advanced HCCThe survival benefits of palliative options are highly controversial due to the low number of RCTs.Chemo-embolization has been extensively evaluated[36,37]and recent Western[39]and Eastern[40]investigations have provided positivefindings that support a beneficial effect. Tamoxifen administration has no efficacy[36]and other options such as systemic chemotherapy,octreotide,internal radiation,proton beam radiation,antiandrogens and immunotherapy have been assessed in single investigations including a limited number of patients and/or lacking an untreated control arm.Unfortunately,some of them lack any antitumoral effect and/or are associated to relevant toxicity [36,37].In summary,HCC is a major complication of chronic HBV infection representing one of the most frequent causes of death.Universal vaccination will eventually eradicate this infection and thus,diminish the incidence of liver cancer.Effective antiviral therapy may prevent cirrhosis and ultimately cancer.However,if cirrhosis is already estab-lished,the only chance for long-term HCC cure will come from early detection and effective treatment. AcknowledgementsDr.Llovet is a recipient of a contract from Programa “Ramon y Cajal”(Ministerio de Ciencia y Tecnologı´a). References[1]Bosch FX,Ribes J,Borras J.Epidemiology of primary liver cancer.Semin Liver Dis1999;19:271–85.[2]Parkin DM,Bray F,Ferlay J,Pisani P.Estimating the world cancerburden:Globocan2000.Int J Cancer2001;94:153–6.[3]Fattovich G,Giustina G,Schalm SW,Hadziyannis S,Sanchez-TapiasJ,Almasio P,et al.Occurrence of hepatocellular carcinoma and decompensation in western European patients with cirrhosis typeB.The EUROHEP Study Group on Hepatitis B Virus and Cirrhosis.Hepatology1995;21:77–82.J.Bruix,J.M.Llovet/Journal of Hepatology39(2003)S59–S63 S62[4]Degos F,Christidis C,Ganne-Carrie N,Farmachidi JP,Degott C,Guettier C,et al.Hepatitis C virus related cirrhosis:time to occurrence of hepatocellular carcinoma and death.Gut2000;47:131–6.[5]Bolondi L,Sofia S,Siringo S,Gaiani S,Casali A,Zironi G,et al.Surveillance programme of cirrhotic patients for early diagnosis and treatment of hepatocellular carcinoma:a cost-effectiveness analysis.Gut2001;48:251–9.[6]Bruix J,Sherman M,Llovet JM,Beaugrand M,Lencioni R,Burroughs AK,et al.Clinical Management of Hepatocellular carcinoma:conclusions of the Barcelona-2000EASL Conference.J Hepatol2001;35:421–30.[7]Beasley RP.Hepatitis B virus as the etiologic agent in hepatocellularcarcinoma.Hepatology1982;2:21–26s.[8]Chang MH,Chen DS.Prospects for hepatitis B virus eradication andcontrol of hepatocellular carcinoma.Baillieres Best Pract Res Clin Gastroenterol1999;13:511–7.[9]Okuda K.Hepatocellular carcinoma.J Hepatol2000;32:225–37.[10]Brechot C,Thiers V,Kremsdorf D,Nalpas B,Pol S,Paterlini-BrechotP.Persistent hepatitis B virus infection in subjects without hepatitis B surface antigen:clinically significant or purely‘occult’?Hepatology 2001;34:194–203.[11]Beasley RP,Hwang LY,Lin CC,Chien CS.Hepatocellular carcinomaand hepatitis B virus.A prospective study of22,707men in Taiwan.Lancet1981;2:1129–33.[12]Sakuma K,Saitoh N,Kasai M,Jitsukawa H,Yoshino I,YamaguchiM,et al.Relative risks of death due to liver disease among Japanese male adults having various statuses for hepatitis B s and e antigen/ antibody in serum:a prospective study.Hepatology1988;8:1642–6.[13]McMahon BJ,Bulkow L,Harpster A,Snowball M,Lanier A,Sacco F,et al.Screening for hepatocellular carcinoma in Alaska natives infected with chronic hepatitis B:a16-year population-based study.Hepatology2000;32:842–6.[14]Fattovich G,Brollo L,Giustina G,Noventa F,Pontisso P,Alberti A,et al.Natural history and prognostic factors for chronic hepatitis typeB.Gut1991;32:294–8.[15]Sherman M,Peltekian KM,Lee C.Screening for hepatocellularcarcinoma in chronic carriers of hepatitis B virus:incidence and prevalence of hepatocellular carcinoma in a North American urban population.Hepatology1995;22:432–8.[16]Jackson PE,Groopman JD.Aflatoxin and liver cancer.Baillieres BestPract Res Clin Gastroenterol1999;13:545–55.[17]Ozturk M.p53mutation in hepatocellular carcinoma after aflatoxinncet1991;338:1356–9.[18]Chang MH,Chen CJ,Lai MS,Hsu HM,Wu TC,Kong MS,et al.Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children.N Engl J Med1997;336: 1855–9.[19]Kensler TW,He X,Otieno M,Egner PA,Jacobson LP,Chen B,et al.Oltipraz chemoprevention trial in Qidong,People’s Republic of China:modulation of serum aflatoxin albumin adduct biomarkers.Cancer Epidemiol Biomarkers Prev1998;7:127–34.[20]Wang JS,Shen X,He X,Zhu YR,Zhang BC,Wang JB,et al.Protective alterations in phase1and2metabolism of aflatoxin B1by oltipraz in residents of Qidong,People’s Republic of China.J Natl Cancer Inst1999;91:347–54.[21]Brechot C,Gozuacik D,Murakami Y,Paterlini-Brechot P.Molecularbases for the development of hepatitis B virus(HBV)-related hepatocellular carcinoma(HCC).Semin Cancer Biol2000;10: 211–31.[22]Chen PJ,Chen DS.Hepatitis B virus infection and hepatocellularcarcinoma:molecular genetics and clinical perspectives.Semin Liver Dis1999;19:253–62.[23]Shafritz DA,Shouval D,Sherman HI,Hadziyannis SJ,Kew MC.Integration of hepatitis B virus DNA into the genome of liver cells in chronic liver disease and hepatocellular carcinoma.Studies in percutaneous liver biopsies and post-mortem tissue specimens.N Engl J Med1981;305:1067–73.[24]Halliwell B.Oxygen and nitrogen are pro-carcinogens.Damage toDNA by reactive oxygen,chlorine and nitrogen species:measure-ment,mechanism and the effects of nutrition.Mutat Res1999;443: 37–52.[25]Laurent-Puig P,Legoix P,Bluteau O,Belghiti J,Franco D,Binot F,et al.Genetic alterations associated with hepatocellular carcinomas define distinct pathways of hepatocarcinogenesis.Gastroenterology 2001;120:1763–73.[26]Buendia MA.Genetics of hepatocellular carcinoma.Semin CancerBiol2000;10:185–200.[27]Baffis V,Shrier I,Sherker AH,Szilagyi e of interferon forprevention of hepatocellular carcinoma in cirrhotic patients with hepatitis B or hepatitis C virus infection.Ann Intern Med1999;131: 696–701.[28]Camma C,Giunta M,Andreone P,Craxi A.Interferon and preventionof hepatocellular carcinoma in viral cirrhosis:an evidence-based approach.J Hepatol2001;34:593–602.[29]Prorok PC.Epidemiologic approach for cancer screening.Problems indesign and analysis of trials.Am J Pediatr Hematol Oncol1992;14: 117–28.[30]Sarasin FP,Giostra E,Hadengue A.Cost-effectiveness of screeningfor detection of small hepatocellular carcinoma in western patients with Child-Pugh class A cirrhosis.Am J Med1996;101:422–34. [31]Collier J,Sherman M.Screening for hepatocellular carcinoma.Hepatology1998;27:273–8.[32]Sherman M.Alphafetoprotein:an obituary.J Hepatol2001;34:603–5.[33]Trevisani F,D’Intino PE,Morselli-Labate AM,Mazzella G,AccogliE,Caraceni P,et al.Serum alpha-fetoprotein for diagnosis of hepatocellular carcinoma in patients with chronic liver disease: influence of HBsAg and anti-HCV status.J Hepatol2001;34:570–5.[34]Nakashima T,Kojiro M.Pathologic characteristics of hepatocellularcarcinoma.Semin Liver Dis1986;6:259–66.[35]Lok AS,Lai CL.Alpha-Fetoprotein monitoring in Chinese patientswith chronic hepatitis B virus infection:role in the early detection of hepatocellular carcinoma.Hepatology1989;9:110–5.[36]Bruix J,Llovet JM.Prognostic prediction and treatment strategy inHCC.Hepatology2002;35:519–24.[37]Befeler AS,Di Bisceglie AM.Hepatocellular carcinoma:diagnosisand treatment.Gastroenterology2002;122:1609–19.[38]Arii S,Yamaoka Y,Futagawa S,Inoue K,Kobayashi K,Kojiro M,et al.Results of surgical and non-surgical treatment for small-sized hepatocellular carcinomas:a retrospective and nationwide survey in Japan.Hepatology2000;32:1224–9.[39]Llovet JM,Real MI,Montanya X,Planas R,Coll S,Aponte AJ,et al.Arterial embolization,chemoembolization versus symptomatic treat-ment in patients with unresectable hepatocellular carcinoma:a randomized controlled ncet2002;359:1734–9.[40]Lo CM,Ngan H,Tso WK,Liu CL,Lam CM,Poon RT,et al.Randomized controlled trial of transarterial lipiodol chemoemboliz-ation for unresectable hepatocellular carcinoma.Hepatology2002;35: 1164–71.J.Bruix,J.M.Llovet/Journal of Hepatology39(2003)S59–S63S63。

中华人民共和国传染病防治法Law of the PRC on the Prevention and Treatment of Infectious Diseases 第一条为了预防、控制和消除传染病的发生与流行,保障人体健康,制定本法。
Article 1. This Law is enacted in order to prevent, control and eliminate the occurrence and epidemic of infectious diseases and to ensure the health of the people.第二条国家对传染病实行预防为主的方针,防治结合,分类管理。
Article 2. The state shall implement a policy of putting the emphasis on prevention, combining prevention with treatment and classified management with respect to infectious diseases.第三条本法规定管理的传染病分为甲类、乙类和丙类。
Article 3. The infectious diseases governed by this Law shall be divided into Classes A, B, and C.甲类传染病是指:鼠疫、霍乱。
A Class infectious diseases shall include plague and cholera.乙类传染病是指:病毒性肝炎、细菌性和阿米巴性痢疾、伤寒和副伤寒、艾滋病、淋病、梅毒、脊髓灰质炎、麻疹、百日咳、白喉、流行性脑脊髓膜炎、猩红热、流行性出血热、狂犬病、钩端螺旋体病、布鲁氏菌病、炭疽、流行性和地方性斑疹伤寒、流行性乙型脑炎、黑热病、疟疾、登革热。

Hepatitis B virus-induced oncogenesisJoachim Lupberger;Eberhard Hildt【期刊名称】《世界胃肠病学杂志:英文版》【年(卷),期】2007(13)1【摘要】Hepatocellular carcinoma (HCC) is one of the most com- mon cancers in the world with an annual incidence of more than 500 000 in the year 2000. Its incidence is rising in many countries. Recently, it has been estimated that about 53% of HCC cases in the world are related to hepatitis B virus (HBV). The epidemiological association of HBV with HCC is well established. In recent studies, it was revealed that HBsAg carriers have a 25-37 times increased risk of developing HCC as compared to non-infected people. At present, HBV-associated carcinogenesis can be seen as a multi-factorial process that includes both direct and indirect mechanisms that might act synergistically. The integration of HBV DNA into the host genome occurs at early steps of clonal tumor expansion. The integration has been shown in a number of cases to affect a variety of cancer- related genes and to exert insertional mutagenesis. The permanent liver inflammation, induced by the immune response, resulting in a degeneration and regeneration process confers to the accumulation of critical mutations in the host genome. In addition to this, the regulatory proteins HBx and the PreS2 activators that can be encoded by the integrate exert a tumor promoter-like function resulting in positiveselection of cells producing a functional regulatory protein. Gene expression profiling and proteomic techniques may help to characterize the molecular mechanisms driving HBV-associated carcino- genesis, and thus potentially identify new strategies in diagnosis and therapy.【总页数】8页(P74-81)【关键词】乙型病毒肝炎;治疗;临床;肿瘤发生【作者】Joachim Lupberger;Eberhard Hildt【作者单位】Department of Internal Medicine II, Hugstetter Str. 55, D-79106 Freiburg, Germany【正文语种】中文【中图分类】R512.62【相关文献】1.Hepatitis C virus-induced prion protein expression facilitates hepatitis C virus replication [J], Huixia Zhang;Shanshan Gao;Rongjuan Pei;Xinwen Chen;Chaoyang Li2.Hepatitis C virus-induced prion protein expression facilitates hepatitis C virus replication [J], Huixia Zhang;Shanshan Gao;Rongjuan Pei;Xinwen Chen;Chaoyang Li;;;3.Hepatitis B and C virus-induced hepatitis: Apoptosis, autophagy, and unfolded protein response [J], Behzad Yeganeh;Adel Rezaei Moghadam;Javad Alizadeh;Emilia Wiechec;Seyed MoayedAlavian;Mohammad Hashemi;Bita Geramizadeh;Afshin Samali;Kamran Bagheri Lankarani;Martin Post;Payam Peymani;Kevin M Coombs;SaeidGhavami4.Application of the woodchuck animal model for the treatment of hepatitis B virus-induced liver cancer [J], Manasa Suresh;Stephan Menne5.Contributions of transgenic mouse studies on the research of hepatitis B virus and hepatitis C virus-induced hepatocarcinogenesis [J], Shogo Ohkoshi;Haruka Hirono;Kazuhiko Watanabe;Katsuhiko Hasegawa;Masahiko Yano因版权原因,仅展示原文概要,查看原文内容请购买。
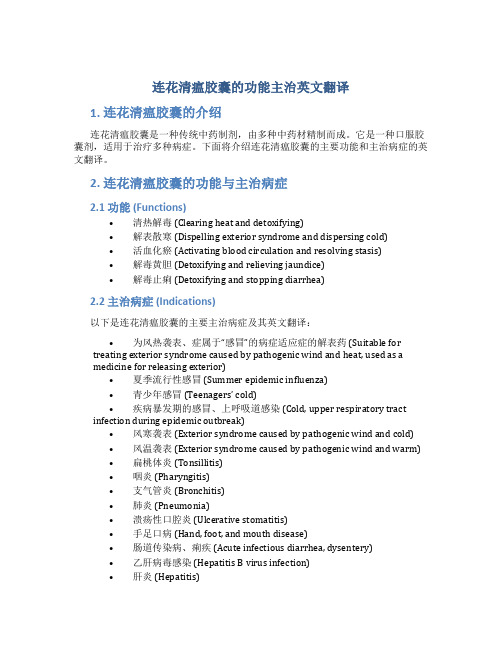
连花清瘟胶囊的功能主治英文翻译1. 连花清瘟胶囊的介绍连花清瘟胶囊是一种传统中药制剂,由多种中药材精制而成。
它是一种口服胶囊剂,适用于治疗多种病症。
下面将介绍连花清瘟胶囊的主要功能和主治病症的英文翻译。
2. 连花清瘟胶囊的功能与主治病症2.1 功能 (Functions)•清热解毒 (Clearing heat and detoxifying)•解表散寒 (Dispelling exterior syndrome and dispersing cold)•活血化瘀 (Activating blood circulation and resolving stasis)•解毒黄胆 (Detoxifying and relieving jaundice)•解毒止痢 (Detoxifying and stopping diarrhea)2.2 主治病症 (Indications)以下是连花清瘟胶囊的主要主治病症及其英文翻译:•为风热袭表、症属于“感冒”的病症适应症的解表药 (Suitable for treating exterior syndrome caused by pathogenic wind and heat, used as amedicine for releasing exterior)•夏季流行性感冒 (Summer epidemic influenza)•青少年感冒(Teenagers’ cold)•疾病暴发期的感冒、上呼吸道感染 (Cold, upper respiratory tract infection during epidemic outbreak)•风寒袭表 (Exterior syndrome caused by pathogenic wind and cold)•风温袭表 (Exterior syndrome caused by pathogenic wind and warm)•扁桃体炎 (Tonsillitis)•咽炎 (Pharyngitis)•支气管炎 (Bronchitis)•肺炎 (Pneumonia)•溃疡性口腔炎 (Ulcerative stomatitis)•手足口病 (Hand, foot, and mouth disease)•肠道传染病、痢疾 (Acute infectious diarrhea, dysentery)•乙肝病毒感染 (Hepatitis B virus infection)•肝炎 (Hepatitis)2.3 用法用量 (Dosage and Administration)连花清瘟胶囊的用法用量如下:•成人每次2粒,每日3次 (Adult: take 2 capsules per time, 3 times daily)•18岁以下的未成年人按体重适量减量 (For individuals under 18 years old, dosage should be reduced according to body weight)注:请按照医生或药师的指导使用。
HIV感染者乙肝丙肝梅毒感染情况调查与分析摘要】目的:研究HIV感染者合并感染乙肝病毒、丙肝病毒、梅毒的情况,为HIV感染防治和治疗提供科学依据。
方法:我院于2014年5月至2017年5月共有27144名受检者进行进行HIV、乙肝、丙肝以及梅毒四项检查,比较HIV感染者合并其他病毒感染的情况。
结果:其中HIV(1+2)抗体阳性并经艾滋病确证实验室确证为艾滋病感染者共171例,在171例HIV感染者中,合并乙肝表面抗原阳性的为17例(5.89%);合并丙肝抗体阳性的为3例(1.75%);合并梅毒螺旋体抗体阳性的为37例(21.64%),即HIV感染者中合并梅毒阳性感染率明显高于合并乙肝、合并丙肝感染率。
合并乙肝、丙肝的为1例(0.58%);合并乙肝、梅毒阳性的为4例(2.34%);合并丙肝、梅毒阳性的为2例(1.17%);合并乙肝、丙肝、梅毒阳性的为1例(0.58%),合并单个病毒感染率明显高于合并双重病毒感染率、合并多重病毒感染率,合并双重病毒感染率明显高于合并多重病毒感染率。
结论:在HIV感染者中,往往合并乙肝、丙肝、梅毒的双重或者多重感染,且合并梅毒有较高的感染率,即在HIV感染者治疗的过程中,应当多注意患者的双重或者多重感染,有助于改善患者病情,改善预后。
【关键词】HIV感染者;乙肝;丙肝;梅毒;双重感染;多重感染;调查分析【中图分类号】R511 【文献标识码】A 【文章编号】1007-8231(2018)06-0011-02【Abstract】Objective To study the HIV infection of hepatitis b virus, hepatitis c virus (HCV), syphilis, provided the scientific basis for prevention and control of HIV infection and treatment method of our hospital from May 2014 to May 2014 a total of 27144 subjects of HIV, hepatitis b, hepatitis c and syphilis four examination, comparedto other virus infection of HIV merger results of HIV antibody positive (1+2) and were confirmed by AIDS laboratory confirmed for a total of 171 cases of people infectedwith HIV, in 171 cases of HIV infection, the merger of hepatitis b surface antigen positive for 17 cases (5.89%). Three cases (1.75%) were positive for HCV. In 37 cases (21.64%), the positive infection rate of syphilis was significantly higher than that of hepatitis b combined with hepatitis c. One case (0.58%) was combined with hepatitis b and hepatitis c. There were 4 cases of hepatitis b and syphilis (2.34%). Two cases(1.17%) were combined with hepatitis c and syphilis. With hepatitis b, hepatitis c, positive for syphilis 1 case (0.58%), the single virus infection rate is significantly higher than the combining dual infection rates, merge multiple virus infections, double infection rates significantly higher than the combining multiple virus infection. Conclusion In people living with HIV, often merge double or multiple infection of hepatitis b, hepatitis c, syphilis, and merger syphilis have higher infection rates, namely in the process of people living with HIV treatment, patients should pay more attentionto the double or multiple infections, help to improve the patients, improve the prognosis.【Key words】HIV infected; Hepatitis b; Hepatitis c; Syphilis; Double infection; Multiple infection, Investigation and analysis.艾滋病病毒与丙型肝炎病毒、乙型肝炎病毒、梅毒螺旋体等具有相似的传染源和传播途径[1]。
《2024年世界卫生组织慢性乙型肝炎患者的预防、诊断、关怀和治疗指南》推荐意见要点艾小委,张梦阳,孙亚朦,尤红首都医科大学附属北京友谊医院肝病中心,北京 100050通信作者:尤红,******************(ORCID:0000-0001-9409-1158)摘要:2024年3月世界卫生组织(WHO)发布了最新版《慢性乙型肝炎患者的预防、诊断、关怀和治疗指南》。
该指南在以下方面进行了更新:扩大并简化慢性乙型肝炎治疗适应证,增加可选的抗病毒治疗方案,扩大抗病毒治疗预防母婴传播的适应证,提高乙型肝炎病毒诊断,增加合并丁型肝炎病毒的检测等。
本文对指南中的推荐意见进行归纳及摘译。
关键词:乙型肝炎,慢性;预防;诊断;治疗学;世界卫生组织;诊疗准则Key recommendations in guidelines for the prevention,diagnosis,care and treatment for people with chronic hepatitis B infection released by the World Health Organization in 2024AI Xiaowei, ZHANG Mengyang, SUN Yameng, YOU Hong.(Liver Research Center, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, China)Corresponding author: YOU Hong,******************(ORCID: 0000-0001-9409-1158)Abstract:In March 2024, the World Health Organization released the latest version of guidelines for the prevention, diagnosis,care and treatment for people with chronic hepatitis B infection. The guidelines were updated in several aspects,including expanding and simplifying the indications for chronic hepatitis B treatment,adding alternative antiviral treatment regimens,broadening the indications for antiviral therapy to prevent mother-to-child transmission,improving the diagnosis of hepatitis B virus,and adding hepatitis D virus (HDV)testing. This article summarizes and gives an excerpt of the recommendations in the guidelines.Key words:Hepatitis B, Chronic; Prevention; Diagnosis; Therapeutics; World Health Organization; Practice Guideline近年来,慢性乙型肝炎(CHB)在预防、诊断、治疗等方面取得重要进展。
木仓医学考研复试SCI长难句肝胆胃肠外科第一章-肝细胞恶性肿瘤Hepatocellular carcinoma(HCC)is the third leading cause of cancer--related deaths worldwide,and hepatitis B virus(HBV)infection is one of its leading causes.During the past several years,next-generation sequencing studies using bulk tumor samples have revealed considerable intratumor molecular and genetic heterogeneity in HCC.Such intratumor heterogeneity poses a great challenge for tumor characterization and therapeutic management of HCC patients.As is well known,tumor initiation and evolution are mediated by sequential genetic alterations in single cells.Single-cell sequencing has the potential to provide new insights into cancer bio-logical diversity that were difficult to resolve in genomic data from bulk tumor samples.在全球范围内导致癌症相关死亡的原因中,肝细胞癌(HCC)位列第三,而乙型肝炎病毒感染是其重要病因之一。
孕妇产检项目明细(Details of pregnancy test items)What does a pregnant woman have for 5 months? What kind of inspection items do you have? Next to understand together:Inspection and inspection project1 、 B ultrasoundUsually the doctor will ask pregnant mother in the early pregnancy, middle and late for a comprehensive B ultrasound, as long as the diagnostic dose of B ultrasound examination, the fetus is not affected. This month B, the main purpose is for screening for fetal brain abnormalities such as major malformations (hydrocephalus, no brain...... ) limb deformities, fetal edema, etc.. In addition, the B-mode ultrasound can tell the sex of the fetus.2 、 amniotic fluid diagnosisAmniocentesis: the detection of an abnormal fetus, preferably performed at 16~20 weeks of gestation (except for exceptional conditions), can examine all abnormalities in the number and shape of chromosomes. Amniotic fluid diagnosis is risky. Therefore, amniotic fluid diagnosis is limited to chromosomal or genetic disorders at high risk in pregnant women. For other pregnant women, ultrasound and serological screening tests have been able to give excellent indicators.Understanding of pregnant women 5 months, what the inspection, the following describes the general pregnancy inspection required to do the inspection content:First, the early pregnancy inspection content1, record the past medical history, drug sensitivity, family history, menstrual history, pregnancy history, and so on, to know if there are any diseases or abnormalities affecting pregnancy;3, gynecological examination: the location of the uterus, size, and determine whether the pregnancy month is quite, and pay attention to whether genital inflammation, deformity and tumor;2, physical examination: blood pressure, weight, height, heart, lungs, liver, spleen, thyroid, breast, etc., to understand the development and nutritional status of pregnant women;4, blood routine, urine routine, liver function, hepatitis B surface antigen, syphilis screening and ECG examination.Two, mid pregnancy inspection content1, each physical examination measure blood pressure, body weight, uterine height, abdominal circumference, fetal heart rate, and noted that there is no lower extremity edema;2 、 15~20 weeks gestation, we should do serological screening for Down syndrome and neural tube defect;3, review blood routine, timely detection of pregnancy associated anemia, review urine routine, timely screening ofpregnancy induced hypertension syndrome;4, 20~24 weeks pregnant, it is recommended to do B screening fetal body surface abnormalities;5, 24~28 weeks pregnant, recommended pregnancy associated diabetes screening (50g glucose screening test).Three, late pregnancy inspection content1, count and record the movement; suggestions for regular monitoring of fetal heart rate;2, continue to pay attention to check the physical examination in mid pregnancy, fetal position, such as abnormal timely correction;3, prenatal ultrasound examination, observation of fetal growth and development, placenta location and maturity, amniotic fluid and so on.The above describes the pregnant women 5 months, what inspection and specific inspection content, and I hope to help mothers, if you still have questions,The obstetric expert answered, "the gestational age is calculated from the first day of the last menstrual period, and the seven day is one week.". Below, for you to introduce the next few months pregnant women to do the birth check, as well as the time of each birth inspection, you can refer to understand:The first inspection: (13 weeks ago) the establishment of "Dongguan City Maternal and Child Health Handbook": urine HCG, gynecological examination, blood routine, urine routine, ECG, ultrasound, hemoglobin electrophoresis test (screening of thalassemia)Second check (16-18 weeks): obstetric examination (including fetal Doppler), blood group (ABO, Rh), blood routine, urine routine, renal function, liver function (3) (5), two pairs of semi hepatitis B, hepatitis C virus antibody, syphilis antibody in serum, blood glucose;The third examination: (20-24 weeks) obstetrical examination, urine routine examination and color B ultrasonic examinationFourth examinations: (24-28 weeks) obstetric examination, urinalysis, and blood glucose screeningFifth examinations: (28-30 weeks) obstetrical examination, urine routine examination and ABO antibody testThe sixth examination: (30-32 weeks) obstetrical examination, routine blood test, urine routine examination and B ultrasonic examinationSeventh examinations: (32-34 weeks) obstetric examination and urinalysisEighth examinations: (34-36 weeks) obstetric examination, fetal monitoring and urinalysisThe ninth examination: 37 weeks obstetrics examination, urine routine, B ultrasonic examination, routine blood test, liver and kidney function, fetal monitoringTenth examinations: 38 weeks obstetric examination, fetal monitoring and urinalysisThe eleventh examination: 39 weeks obstetrics examination, urine routine, B ultrasound, fetal monitoringTwelfth examinations: 40 weeks obstetric examination, fetal monitoring and urinalysisPregnant women go to the doctor for a few months, and they are the concerns of pregnant women. Xuzhou Ruibo hospital obstetric experts suggest that the majority of pregnant women, positive time to go to the hospital check, to ensure the healthy growth of babies. From the first three months of pregnancy to the hospital for a pregnancy check and then to childbirth, the hospital is where all expectant mothers have to go.Xuzhou expert reminder: pregnant, looking forward to the arrival of new life, is a sweet and long hard road, regular check in the body weight, blood pressure, urine, urine protein, uterine height and abdominal circumference size, although the simple but very important, can help physicians understand the conditions associated with pregnant women is good. In addition, to maintain a good cheerful mood, listen to melodies, beautiful music, but also an indispensable topic of prenatal education.Prenatal examination schedule is how to arrange the expert, Xuzhou Ruibo said general hospital, prenatal examination including: seven months pregnant 28 weeks ago: once every 4 weeks. Pregnant for eight to nine months [29-35 weeks], once every two weeks. After tenth months [36 weeks], once a week.Prenatal examination itemsGeneral items [inspection of each prenatal examination]Height and weight were measuredFunction: height, first check once. The doctor will be through the height and weight ratio to estimate if your weight is overweight or underweight, and the size of the pelvis.Body weight is a mandatory test for each pregnancy. Through the weight of pregnant women can indirectly detect fetal growth. Weight gain was approximately 12.5 kg throughout gestation, followed by an increase of 350g to 500g per week. Increase too much, prone to complications, the heart burden is too heavy; too little increase will lead to fetal absorption of nutrients is not enough, affecting the normal growth of the fetus.Measurement of uterine height and abdomenThe relationship between the size of mother during pregnancy uterine height and abdominal circumference and the birth of the baby is very close. In the early and middle trimester of pregnancy, there is a certain standard of growth per month. How much the circumference of a pregnancy needs to know. And laterthrough the measurement of uterine height and abdominal circumference, can also be estimated fetal weight. So, do prenatal examination every time to measure the height of uterine fundus and abdominal circumference, to estimate the intrauterine fetal growth, at the same time according to the curve in order to understand the high palace pregnancy intrauterine fetal growth retardation, whether or macrosomia.Measuring blood pressureEffect: blood pressure is a must test item during pregnancy. In general, standard values should not exceed 130/190mmHg, or increase by no more than 30/15mmHg compared with baseline blood pressure (pre pregnancy BP). High blood pressure is one of the symptoms of pregnancy induced hypertension. It usually happens 20 weeks later. It affects the development of the fetus. So check blood pressure every time and see if there is an increase in basal blood pressure to predict or see if a pregnant woman has a pregnancy induced hypertension.Urine testFunction: enter the obstetric examination, urine test to check every time. Check whether there is protein, sugar and ketone bodies in the urine, and check the red blood cells and white blood cells, especially the detection of the protein, which can indicate the occurrence of diseases such as pregnancy, hypertension and so on. Problems may be dealt with in a timely manner. If have hematuria circumstance, need to be checked further, be kidney stone, bladder stone?.Blood testFunction: blood test, usually in the first check the most detailed, including many projects, such as liver function, renal function, blood group (ABO), cytomegalovirus and rubella virus and Toxoplasma infection, syphilis screening, if you want to keep the cord blood to do HIV examination, namely hiv. Pregnancy tests are also, to some extent, a health examination,A lot of times, the mother does not feel at all, but it inadvertently affects the fetus, and has an impact on the delivery and continuing pregnancy. In order to eugenics, it is necessary to do these checks.Edema examinationRole: after pregnancy, especially 5~6 months later, because of the increase in the fetus and amniotic fluid increase, the body of the lower limb vascular compression, the lower extremity blood circulation is not smooth, resulting in increased pulse pressure, lower limbs prone to edema. This is not a disease. But edema is also one of the manifestations of hypertensive disorders in pregnancy, so it is important to distinguish between pregnancy edema and pregnancy induced hypertension. If the swelling is serious, diuretic treatment is necessary.B-mode ultrasonographyEffects: generally do 3 times. For the first time between 16~20 weeks of pregnancy, the emphasis is on dislocation.Second check in about 23 weeks of gestation, will do a 9 screening inspection screening structure is deformed, look at the fetal cerebellum, superior, kidney, kidney, stomach bubble, heart four cavity, abdominal wall, bladder and femoral bone of acer.Third times in the pregnancy after 36 weeks, and see if there is blood, umbilical cord around the neck of the cerebral arteries, determine fetal position.electrocardiogramFunction: the electrocardiogram is performed separately at first visit and 32~34 weeks after pregnancy. First visit, mainly to understand the pregnant mommy's heart function, exclude heart disease, to confirm whether pregnant Mommy can bear childbirth, if there is a problem, to enter the medical treatment in time. In addition, the burden on the heart during pregnancy will experience the two peak, the first peak is between 32 ~ 34 weeks, the second peak is at the time of delivery, so the first peak to do electrocardiogram, see the heart burden.Special inspection4-6 weeks pregnantPregnancy TestDetermine pregnancy or not. When necessary, urinalysis, blood test in chorionic gonadotropin. General menstruation expires a week [gravid fifth weeks] can examine.ABO blood groupDetermine the blood type of pregnant women.Rh blood groupA Rh negative pregnant woman who has a positive Rh blood group may have a hydrops fetus. Rh negative blood type pregnant women should pay attention to: 1, need to test Rh antibody, if there is Rh antibody, should pay close attention to fetal edema. 2, pregnancy bleeding, and after abortion or production, need to be injected within 72 hours of immunoglobulin. 3, it is best to produce Rh negative blood reserve.Complete blood countMeasure hemoglobin, red cell size, white blood cell count, red blood cell count, and platelet count. Anemia to supplement iron and pay attention to nutrition, so as not to affect the risk of fetal development and production of. The average red blood cell volume of pregnant women is less than 80fl during the first examination. They may be Mediterranean anemia or iron deficiency anemia, and spouses should also receive an average red blood cell volume test. If the spouse is less than 80fl, the pregnant woman and his spouse should be referred for further examination. If the couple is the same type of thalassemia with fetal 1/4, the risk of severe thalassemia, need further chorionic villus sampling or amniocentesis for fetal gene diagnosis. Platelets less than 150000mm and clotting problems should be examined further.Syphilis serum test VDRLVDRL positive may have syphilis. TPHA is required to confirm the diagnosis. Determination of syphilis in pregnant women infected with the fetus may have congenital syphilis infection and deformity, must be treated as soon as possible, so as not to cause abortion, stillbirth and deformity. Syphilis infected pregnant women need to be treated with antibiotics, the fetus should undergo ultrasound examination and follow-up, and consider fetal umbilical cord blood test.German measles IgG antibodyThe positive person indicated that once infected German measles, has the lifelong immunity. A negative person who has not been infected with German measles should avoid infection during pregnancy and may consider vaccination after birth. German measles infection during pregnancy, should immediately see a doctor to confirm the diagnosis, twenty weeks of pregnancy before infection, fetal congenital rubella syndrome and malformation rate is higher,Consider stopping pregnancy or pregnancy, twenty-two weeks after fetal umbilical cord blood test, and a detailed ultrasound examination. After twenty weeks of pregnancy, a detailed ultrasound examination should be performed.UrinalysisHigh glucose may have diabetes, high urine protein renaldysfunction. Excessive white blood in the urine indicates urinary tract infection or genital tract infection, and excessive red blood cells in the urine may lead to urinary tract infection, urinary tract bleeding or vaginal bleeding.Hepatitis B antigenHepatitis B surface antigen positive patients are hepatitis B carriers. All fetuses need to be given a hepatitis vaccine on time. E antigen positive infection is more powerful, newborns need to be injected within 24 hours of birth globulin. Prenatal hepatitis certificate is required for vaccination. Hepatitis B pregnant women still breastfeeding.8-10 weeks pregnantGo back to the results of the examination and make a further examination. If necessary, perform a basic physical examination, including cardiac auscultation, heart murmur, and irregular pulse. Pelvic examination - size of uterus and ovary, size of pelvic cavity. PAP - cervical cancer screening. Breast exams - breast cancer screening and breast feeding.16-18 weeks pregnantAmniocentesisPerformed at 196-18 weeks gestation. Examine fetal chromosomes and diagnose abnormalities in the structure or number of fetal chromosomes, such as Down's syndrome. More than 35 year old pregnant women who had given birth to children who havecongenital anomalies, family genetic diseases, fetal malformation may, had fetal chromosomal abnormalities, maternal serum screening for high risk group, or parental chromosome abnormality, the probability of fetal chromosome abnormality is higher, should do the amniotic membrane puncture. About 2-3 weeks later, the result is that if the fetus has severe chromosomal abnormalities, the pregnancy can be aborted. Amniocentesis, unlike chorionic villus sampling, does no harm to the fetus itself and only slightly raises the odds of miscarriage [0.5%].Maternal blood Down syndrome screeningThe mother is older, the probability of fetal Down syndrome is higher, the probability of pregnant women over the age of 35 is about 1/270, can be considered accepted amniocentesis, pregnant women under the age of 34 of the consideration is low, but it is still possible to have fetal Down syndrome, should do maternal serum screening for down syndrome. Maternal blood was taken at 16-18 weeks after pregnancy for Down's screening. Serum alpha fetoprotein and chorionic gonadotropin in serum were measured. Calculate the odds of fetuses with Down's syndrome depending on the number of weeks of pregnancy, age, and weight. Pregnant women who are high risk groups need to have an ultrasound examination and amniocentesis if necessary. Screen 60% "rate.20-22 weeks pregnantUltrasound fetal screeningAt 20-22 weeks, the fetal organs were developed and most clearly visible. Check fetal patterns and organs. The abdominal surface of the pregnant woman was examined by an ultrasonic scanner. Examine the size of the fetus, brain, spine, face, lips, heart, stomach, kidneys, bladder, abdominal wall, limbs, sex, umbilical cord blood vessel, placenta position and amniotic fluid volume, etc.. A fetus with severe abnormalities may consider aborting pregnancy 24 weeks earlier. Fetuses suspected of chromosomal abnormalities may receive amniocentesis or cord blood tests. The gestational age can be estimated accurately by the measurement of the fetal head.24-28 weeks pregnantGestational diabetes screeningApproximately one percent to three of pregnant women have gestational diabetes mellitus, if not found, may cause fetal macrosomia or even endanger the fetus or mother. This screening can examine the possibility of gestational diabetes mellitus. In the absence of fasting conditions, an hour to eat 50 grams of glucose powder, measuring blood glucose concentration, if greater than 140gm%, further 100 grams of glucose tolerance test, fasting and taking 100 grams of sugar per hour, a total of four times the blood sugar value, if the four is two times more than the standard value you can confirm the diagnosis. Indeed, pregnant women with gestational diabetes mellitus should be instructed by a dietitian to control their diet. If the blood sugar is still high, insulin injections are required.32-34 weeks pregnantUltrasound evaluation of fetal growthFetal growth rate was evaluated. At the end of the pregnancy if it is not lying when,A clear understanding of the position of the fetus's hands and feet and the body in the uterus so as to determine the mode of production early. Fetal growth retardation may be caused by factors such as the mother, placenta, or fetus. If there is no specific reason, the fetus should also undergo regular follow-up and perform an examination of the physiological function of the ultrasound. A large fetus may endanger the mother and the fetus itself.Pregnant for more than 41 weeksFetal fetal heart examinationOnce or twice a week. Two times a week. Check if placental function is sound. Change with fetal monitor detect the presence of fetal and fetal fetal heartbeat. If your reaction may be bad for fetal heart rate, fetal distress, oxytocin stimulation test should be done, if it is fetal distress, fetal output should be as soon as possible.The experts described in detail the maternity examination schedule, specifically what? I hope it will help you, if you have any previous questions,!。
Jpn. J. Cancer Res.93, 471–477, May 2002471Hepatitis B Virus Infection and B-Cell Non-Hodgkin ’s Lymphoma in a Hepatitis B Endemic Area: A Case-control StudyJee Hyun Kim,1 Yung-Jue Bang,1,2,7 Byung Joo Park,3 Taiwoo Yoo,4 Chul Woo Kim,2,5Tae-You Kim,1,2 Dae Seog Heo,1,2 Hyo-Suk Lee 1,6 and Noe Kyeong Kim 11Department of Internal Medicine, 2Cancer Research Institute, 3Department of Preventive Medicine,4Department of Family Medicine, 5Department of Pathology and 6Liver Research Institute, Seoul National University College of Medicine, 28 Yongon-Dong, Chongno-Gu, Seoul 110-744, South Korea Several studies have reported a higher prevalence of chronic hepatitis C virus (HCV) infection in patients with B-cell non-Hodgkin ’s lymphoma and suggested a pathogenic role for HCV , but studies on hepatitis B virus (HBV) infection and non-Hodgkin ’s lymphoma are limited. To determine the association between HBV infection and non-Hodgkin ’s lymphoma, we performed a case-control study in Korea, a hepatitis B endemic area. We recruited 222 patients newly diagnosed with non-Hodgkin ’s lymphoma at Seoul National University Hospital between January 1997 and December 1998 as cases. Four age- and sex-matched controls were selected for each case, and the control groups comprised of 439 patients with non-hematological malignancy (control group 1) and 444subjects with non-malignant conditions (control group 2). Relative risk of developing non-Hodgkin ’s lymphoma among individuals tested positive for hepatitis B surface antigen was calcu-lated after controlling for other potential risk factors of lymphoma, such as smoking, alcohol drinking, transfusion history and HCV infection. Hepatitis B surface antigen was positive in 28 of 222 patients (12.6%) with non-Hodgkin ’s lymphoma compared with 32 of 439 (7.3%) in control group 1, and 21 of 444 (4.7%) in control group 2 (P =0.001). The crude odds ratio for B-cell non-Hodgkin ’s lymphoma among the HBV carriers was 2.54 (1.46–4.45) and the adjusted odds ratio was 3.30 (1.69–6.45) by multivariate analysis. The present study suggests that the risk of B-cell non-Hodgkin ’s lymphoma is increased in HBV carriers and warrants further investigation of the possible role of hepatitis B virus in the pathogenesis of B-cell non-Hodgkin ’s lymphoma.Key words: Case-control study — Non-Hodgkin ’s lymphoma — Hepatitis B — Risk factorThe incidence of non-Hodgkin ’s lymphoma is increas-ing rapidly in many countries, such as the USA, UK, and Scandinavia.1) Many factors such as immunodeficiencies,various chemical or radiation exposures and transfusion have been suggested to be risk factors, but the cause of non-Hodgkin ’s lymphoma remains uncertain.Several studies in Italy and Southern California have reported a higher prevalence of chronic hepatitis C virus (HCV) infection in B-cell non-Hodgkin ’s lymphoma patients, ranging from 9% to 32%.2–4) In addition, it has been hypothesized that chronic antigenic stimulation by HCV may induce the clonal expansion of immunoglobulin secreting cells and eventually lead to malignant B-cell neoplasm.5) Like HCV , hepatitis B virus (HBV) can repli-cate in various extrahepatic tissues including the lymph nodes and the bone marrow.6–8) Several studies have reported a high prevalence of HBV infection in patients with non-Hodgkin ’s lymphoma, ranging from 3% to 30%.9–14) However, most of these studies were performed as case series studies without control groups.South Korea is one of the endemic areas of chronic HBV infection, the prevalence of hepatitis B surface anti-genemia being 8.0% and 6.2% for adult males and females, respectively.15) In comparison, the prevalence of HCV infection in the general population, in terms of anti-HCV antibody positivity, is 1.7%, which compares to that of developed countries.16) To determine the association between HBV infection and non-Hodgkin ’s lymphoma, we conducted a case-control study involving a large number of patients in Korea.MATERIALS AND METHODSParticipants All 233 patients newly diagnosed with non-Hodgkin ’s lymphoma at Seoul National University Hospi-tal (SNUH) between January 1997 and December 1998were evaluated for the study. Pathology reports were scru-tinized in all cases to confirm the diagnosis. Of the initial 233 patients, 11 patients who were not tested for HBV sur-face antigen (HBsAg) were excluded. All of the remaining 222 patients were histopathologically classified according to the Working Formulation.17) Immunophenotypic analy-sis for surface B and T lymphocytic markers was per-formed in 194 patients.For each case, four controls were selected, two from patients with non-hematologic malignancy who were diag-nosed at SNUH during the same period (control group 1),7To whom correspondence should be addressed.E-mail: bangyj@plaza.snu.ac.krJpn. J. Cancer Res. 93, May 2002472and two from patients with non-malignant conditions attending SNUH during the same period (control group 2).Controls were individually matched to the lymphoma cases by age, sex, and date of admission. Patients closest in age to the case were selected. If there were more than two candidates, those who attended the hospital on the date closest to the date of case admission were selected.Control group 1 consisted of 401 patients with gastric can-cer and 38 with various sarcomas including osteosarcoma,rhabdomyosarcoma, Ewing ’s sarcoma, primitive neuroec-todermal tumor, malignant fibrous histiocytoma and was selected from 1847 gastric cancer patients and 158 sar-coma patients. Control group 2 consisted of 315 visitors and 129 patients with fracture, and was selected from 1348 visitors to the Center for Health Promotion and 238patients who were admitted to the department of Orthope-dic Surgery with the diagnosis of fracture. All visitors to the Center for Health Promotion and all the patients at the orthopedic ward received a routine check, which included a complete blood count, blood chemistry, urinalysis, fecal occult blood test, chest X-ray and electrocardiogram. Only those who were free of malignant diseases by history,physical examination and screening laboratory tests were enrolled.In SNUH, routine viral marker screening is performed for all in-patients of the department of internal medicine and for all in-patients undergoing surgical procedure.Cases and controls were tested for HBsAg, antibodies to HBsAg, anti-HCV antibody and anti-human immunodefi-ciency virus (HIV) antibody by second-generation enzyme-linked immunosorbent assay using a Behring ELISA processor III (Behringwerke AG, Diagnostics, Marburg,Germany). A liver panel including total protein, serum albumin, serum alkaline phosphatase, total bilirubin,alanine aminotransferase, and aspartate aminotransferase was also obtained for all patients. Tests were performed with fresh samples on admission or during the first visit to the outpatient clinic, before any treatment, including blood transfusion or cancer chemotherapy. We reviewed medical records for information on occupation, alcohol consumption, smoking habits, previous diseases and trans-fusion history. For those who tested positive for HBsAg,we recorded the dates on which patients were first diagnosed as HBV carriers.Statistical methods The χ2 test was used to assess the significance of differences in distribution of characteristics between cases and controls. Logistic regression analyses were performed to test the hypothesis that HBV infection may independently influence the occurrence of non-Hodgkin ’s lymphoma, after controlling for confounders.Confounders were used in the model if they were risk fac-tors for non-Hodgkin ’s lymphoma or showed a significant association with HBV infection. Specific potential con-founders were also included in the model if they hadbiological plausibility as risk factors for non-Hodgkin ’s lymphoma. The appropriate odds ratios and their 95%confidence intervals were calculated as estimates of the association between HBV infection and non-Hodgkin ’s lymphoma. Statistical analysis was performed using SPSS for Windows, version 9.0 (SPSS, Inc., Chicago, IL).RESULTSA total of 222 cases and 883 controls were enrolled in the study. The cases consisted of 132 men (59.5%) and 90 women (40.5%) and their demographic characteristics are summarized in Table I. The cases and controls were similar with respect to sex, age, smoking, and transfusion history.HBsAg was positive in 28 of 222 patients (12.6%) with non-Hodgkin ’s lymphoma, as opposed to 32 of 439patients (7.3%) in control group 1 and 21 of 444 subjects (4.7%) in control group 2. A higher risk of non-Hodgkin ’s lymphoma was found in HBsAg-positive carriers than in the HBsAg-negative subjects. The odds ratios were 1.84(1.07–3.14) versus control group 1 and 2.91 (1.61–5.25)versus control group 2. The relation of several potential confounders to non-Hodgkin ’s lymphoma was assessed by logistic regression analysis (Table II). The association between HBV infection and non-Hodgkin ’s lymphoma remained significant after controlling for age, sex, transfu-sion history, smoking, alcohol drinking and HCV infection (Table III).HBsAg carrier status was not associated with any par-ticular histologic subtypes of non-Hodgkin ’s lymphoma,and the HBsAg-positive rate was 13.3%, 12.9%, and 10.0% in patients with low-grade, intermediate-grade, and high-grade lymphoma. The HBsAg-positive rate was higher in B-cell lymphoma patients (14.0%) than in T-cell lym-phoma patients (6.9%) in the 194 patients immunopheno-typed. Subgroup analysis revealed that HBsAg-positive carriers had a higher risk of B-cell non-Hodgkin ’s lym-phoma, but not T-cell lymphoma. The corresponding odds ratios were 2.07 (1.13–3.78) versus control group 1, and 3.27 (1.70–6.29) versus control group 2 (Table III).Eighty-two percent of B-cell non-Hodgkin ’s lymphoma patients had extranodal involvement and 8.1% had hepatic involvement. There was no significant difference in hepatic involvement in HBsAg-positive and -negative patients; 10.0% vs. 7.4% (P =0.65), respectively.The HBsAg-positive rate was consistently higher for non-Hodgkin ’s lymphoma patients in every age group. It was highest among the younger age groups, showing a peak prevalence of 23.8% in the 20 to 29 age group,then declined with increasing age. Risk of B-cell non-Hodgkin ’s lymphoma was most evident in the younger HBsAg-positive groups. The odds ratios of B-cell non-Hodgkin ’s lymphoma were 4.66, 3.01 and 1.94 in the 29-HBV Infection and B-Cell NHL473Table I.Characteristics of Non-Hodgkin ’s Lymphoma Cases and Their Age-, Sex-matched Controls, Seoul National University Hospital, Korea, 1997–1998CharacteristicsCases (n =222)Control 1a )(n =439)Control 2b )(n =444)P value c )Median age (range), yr.52 (14–85)52 (13–82)52 (13–84) 1.0Age, n (%) 1.0≤199 (4.1)13 (3.0)18 (4.1)20–2921 (9.5)40 (9.1)42 (9.5)30–3934 (15.3)70 (15.9)68 (15.3)40–4935 (15.8)70 (15.9)70 (15.8)50–5952 (23.4)104 (23.7)105 (23.6)60–6943 (19.4)86 (19.6)84 (18.9)≥7028 (12.6)56 (12.8)57 (12.8)Sex0.974Male, n (%)132 (59.5)258 (58.8)264 (59.5)Female, n (%)90 (40.5)181 (41.2)180 (40.5)Smoking0.078Ever, n (%) 69 (31.1)167 (38.0)186 (41.9)Never, n (%)130 (58.6)245 (55.8)235 (52.9)Unknown, n (%)23 (10.4)27 (6.2)23 (5.2)Alcohol drinking 0.038Yes, n (%)60 (27.0)161 (36.7)169 (38.1)No, n (%)139 (62.6)246 (56.0)251 (56.5)Unknown, n (%)23 (10.4)32 (7.3)24 (5.4)Transfusion history 0.171Yes, n (%)26 (11.7)36 (8.2)52 (11.7)No, n (%)157 (70.7)341 (77.7)342 (77.0)Unknown, n (%)39 (17.6)62 (14.1)50 (11.3)a )Control group 1: patients with non-hematologic malignancy, SNUH, 1997–1998.b )Control group 2: subjects with non-malignant conditions, SNUH, 1997–1998.c )Pearson ’s χ2 test.Table II.Odds Ratios for the Association between Risk Factors and Non-Hodgkin ’s Lymphoma in Cases and Controls, Seoul National University Hospital, Korea, 1997–1998CharacteristicsControl 1Control 2Crude OR a )95%CICrude OR b )95%CISmoking Ever 0.780.55–1.110.670.47–0.95Never 1.00 1.00Alcohol Ever 0.660.46–0.950.640.45–0.92Never 1.00 1.00Transfusion ≥1 pint 1.570.92–2.69 1.090.66–1.81Never 1.00 1.00HBsAg Positive 1.84 1.07–3.14 2.91 1.61–5.25Negative 1.00 1.00Anti-HCV Ab Positive 2.020.70–5.85 1.200.47–3.10Negetive1.001.00a )Risk of non-Hodgkin ’s lymphoma using control group 1 as a reference group.b )Risk of non-Hodgkin ’s lymphoma using control group 2 as a reference group.Jpn. J. Cancer Res. 93, May 2002474year-old or younger, 30–49, and 50-year-old or older age groups, respectively (Table IV).Antibody to HBsAg (anti-HBsAb) was positive in 131(59.0%) out of 222 patients with lymphoma, 287 (65.7%)out of 437 patients in control group 1, and 282 (63.5%)out of 444 subjects in control group 2. Anti-HCV antibody was detected in 7 (3.3%) out of 214 patients with lym-phoma, 7 (1.6%) out of 426 patients in control group 1,and 12 (2.7%) out of 439 subjects in control group 2. No significant differences were found in the anti-HBsAb and anti-HCV antibody-positive rates for the three groups (P =0.15, P =0.65, respectively). Three patients were found to be positive for both HBsAg and anti-HCV antibody.None tested positive for anti-HIV antibody.Data on the date of detection of HBV carrier status were available for ten out of 28 HBsAg-positive patients with non-Hodgkin ’s lymphoma. All ten of these patients were diagnosed as carriers prior to being diagnosed with non-Hodgkin ’s lymphoma and the mean interval between detection of carrier status and diagnosis of non-Hodgkin ’s lymphoma was 100 months (2 to 223 months).DISCUSSIONThe results of this case-control study suggest that HBsAg carrier status is associated with B-cell non-Hodgkin ’s lymphoma. Compared with HBsAg-negative subjects, the risk of developing B-cell non-Hodgkin ’s lym-phoma was increased in HBsAg-positive carriers by two to threefold. This association was independent of age, sex,transfusion history, smoking, alcohol drinking and HCV infection.A high prevalence of HBV infection among patients with non-Hodgkin ’s lymphoma has been reported by sev-eral investigators. Liang et al. reported a high positive rate of 22% for HBsAg in their study on 484 non-Hodgkin ’s lymphoma patients in Hong Kong.9) The same authors also reported a high prevalence of 27% among 100 patients with non-Hodgkin ’s lymphoma in their prospective study.10) Kumagai et al. and Markovic et al. reported the prevalence of HBsAg carriers to be 3.2% in Japan and Slovenia, which is lower than that of Hong Kong, but still higher than the general population in those countries.11,12)Table III.HBsAg-positive Rates and Odds Ratios for the Association between HBV Infection and Non-Hodgkin ’s Lymphoma According to ImmunophenotypesImmuno-phenotypeHBsAg (+)n (%)Control 1Control 2Crude OR a ) (95%CI)Adjusted OR b ) (95%CI)Crude OR c ) (95%CI)Adjusted OR b ) (95%CI)Total 28 (12.6) 1.84 1.99 2.91 3.85(n =222)(1.07–3.14)(1.05–3.75) (1.61–5.25)(1.87–7.92)B-Cell 19 (14.0) 2.07 2.43 3.27 4.57(n =136)(1.13–3.78)(1.17–5.01)(1.70–6.29)(2.03–10.29)T-Cell 4 (6.9)0.940.55 1.490.96(n =58)(0.32–2.77)(0.12–2.48)(0.49–4.51)(0.21–4.47)a )Risk of specified immunopheotype of lymphoma among HBV carriers using control group 1 as a reference group.b )Adjusted for age, sex, smoking, alcohol drinking, transfusion history, and anti-HCV antibody.c )Risk of specified immunopheotype of lymphoma among HBV carriers using control group 2 as a reference group.Table IV .HBsAg-positive Rate of B-Cell Non-Hodgkin ’s Lymphoma Patients and Controls, According to Age Groups, with Odds Ratios of B-Cell Non-Hodgkin ’s Lymphoma among HBsAg-positive Patients and Their 95% Confi-dence Intervals within Specified Age GroupsAge (yr.)Cases Control 1Control 2OR a )(95%CI)nb )%nb )%nb )%≤294/1723.52/53 3.85/608.3 4.66 (1.20–18.10)30–497/3718.911/1407.99/138 6.5 3.01 (1.18–7.71)≥508/829.819/2467.77/246 2.8 1.94 (0.85–4.44)a )Risks of B-cell non-Hodgkin ’s lymphoma among HBsAg-positive patients within specified age groups using both control groups 1 and 2 as reference groups.b )Number of patients tested positive for HBsAg within the specified age group/total number of patients within the specified age group.HBV Infection and B-Cell NHL475The most recent studies performed in Romania and Japan also reported a strikingly higher prevalence of HBV and HCV infection among non-Hodgkin ’s lymphoma patients,29.5% and 30.8%, and 6.9% and 8.1%, respectively.13,14)However, most of these studies were conducted without controls and the HBsAg-positive rate was compared to that of the general population.Three likely explanations have been proposed for the association between HBV infection and non-Hodgkin ’s lymphoma. One hypothesis is that the risk of viral infec-tion or reactivation increases due to the direct immunosup-pressive effect of the lymphoma. The second hypothesis is that HBV carrier status itself might be responsible for lymphomagenesis. Based on the findings that HBV-spe-cific nucleic acid sequences have been detected in periph-eral blood mononuclear cells and in the hematopoietic tumor cells in HBsAg-positive patients,18–20) it could be hypothesized that persistence of HBV in the peripheral blood mononuclear cells, like HCV , may result in chronic stimulation of B-cells which may lead to malignant B-cell lymphoma. The third hypothesis is that another unknown virus with a mode of transmission similar to HBV might be responsible for the lymphomagenesis. Viruses can con-tribute to the development of human tumors, as evidenced by Epstein-Barr virus and HTLV-1, which have been found to be associated with Burkitt ’s lymphoma and adult T cell leukemia-lymphoma.21)The results of our case-control study support the second or third hypothesis, namely, that viral infection, possibly by HBV , might play a pathogenic role in the development of malignant lymphoma. Of the 28 non-Hodgkin ’s lym-phoma patients, at least ten patients were diagnosed as carriers prior to being diagnosed with non-Hodgkin ’s lym-phoma with a mean duration of 100 months. These ten patients had been chronic carriers before the immunosup-pressive effect of lymphoma could have influenced them.Although reactivation of hepatitis B has been reported in HBsAg-negative, anti-hepatitis B core antibody-positive patients receiving immunosuppressive therapy,22,23) no spon-taneous reactivation has been reported in non-Hodgkin ’s lymphoma patients without concomitant immunosuppres-sive therapy. Our findings firmly oppose the first hypothesis.Moreover, our result that only B-cell and not T-cell non-Hodgkin ’s lymphoma is associated with HBV infection also support the second hypothesis. The fact that the risk of B-cell non-Hodgkin ’s lymphoma was higher in the younger age groups calls for special attention. We observed that the HBsAg-positive rate was highest in the youngest age group, then decreased linearly with aging in lymphoma patients in contrast to the control groups (Fig.1). Liang et al. also observed that HBsAg-positive non-Hodgkin ’s lymphoma patients are younger than HBsAg-negative patients; the mean and median ages of the HBsAg-positive and -negative patients were 46.5 and 52.6years, and 48 and 53 years, respectively.9,10) The natural decline of HBsAg-positive rate with aging and the short-ened life expectancy of HBV carriers have been suggested as possible mechanisms,9) but these cannot explain the similar HBsAg-positive rate across the age groups in controls.In HBV endemic countries, most infection occurs dur-ing childhood by perinatal transmission and is followed by chronic carriage of HBV .24) Perinatally acquired HBV undergoes an immune tolerance phase, which permits active viral replication without hepatitis for 2 to 3 decades,and then enters a virus clearance phase.25) Younger age groups are more likely to be infected with actively repli-cating HBV represented by high HBV DNA titer and pos-itive HBeAg (hepatitis B e antigen), which in turn, are more likely to stimulate B cell proliferation. Based on our results, we support the second hypothesis that actively rep-licating HBV may induce B-cell proliferation by chronic antigenic stimulation and play a pathogenic role in non-Hodgkin ’s lymphoma, especially in younger patients. The possibility of unidentified virus contributing to lymphoma-genesis remains. There may be a viral infection which shares the same mode of infection as HBV which would have contributed to lymphomagenesis. Epstein-Barr virus (EBV) could be one candidate. Viral shedding of EBV in salivary gland excretions permits early infections, usually within the first year of life, in developing countries and EBV persists in the infected host throughout life.21)We performed immunohistochemical staining to detect HBsAg and HBcAg (hepatitis B core antigen) in the paraf-fin-embedded, formalin-fixed lymphoma tissues of 28HBsAg-positive patients and 15 HBsAg-negative controlsbut failed to identify HBsAg in any of the lymphoma orFig. 1.HBsAg-positive rate in patients with B-cell non-Hodgkin ’s lymphoma versus controls, according to age groups.Striped bars represent HBsAg-positive rate in patients with B-cell non-Hodgkin ’s lymphoma; white bars represent HBsAg-pos-itive rate in controls. ∗ P =0.038. ∗∗ P =0.026.Jpn. J. Cancer Res. 93, May 2002476control specimens. Although we failed to prove the etio-logic role of HBV , this may also support our hypothesis that an etiologic role of HBV is confined to a relatively small proportion of lymphoma patients, and we believe that this aspect warrants further study.Our study subjects showed no significant differences in anti-HCV antibody-positive rate. South Korea is endemic area for HBV infection, whereas the prevalence of HCV infection in the general population is, in terms of anti-HCV antibody positivity, 1.7%, which resembles that of developed countries. The prevalence of anti-HCV positiv-ity remains below 1% till the 4th decade, then increases steadily with aging, up to 5.7% in the seventies. Chronic carriage of HCV and therefore chronic antigenic stimula-tion by HCV infection would be less likely, which would have contributed to the lack of association between HCV infection and non-Hodgkin ’s lymphoma in this study.Several methodological limitations should be men-tioned. The most serious disadvantage of a case-control study concerns the temporal ambiguity between exposure and the disease occurrence. Although we found a higher prevalence of HBV carriers among non-Hodgkin ’s lym-phoma patients, it cannot be deduced whether this higher prevalence was a cause or an effect of lymphoma. Another limitation is the lack of information on other potential con-founders. Most of the information was taken by reviewing medical records rather than by questionnaire or interview,resulting in many missing values. Thirdly, there may have been selection bias in choosing control groups. We used two control groups (hospital and community) in order toreduce the selection bias. The hospital controls would have similar risk of acquiring HBV infection to the case patients, owing to more frequent exposures to blood prod-ucts and invasive procedures. We chose one homogenous group of gastric cancer patients as control group 1 to reduce other potential confounding variables, and because gastric cancer is the most common cancer in Korea. Given that the association was strongest in young patients, it may be possible that the choice of young controls was biased in some way. Due to differences in the age distribution of the lymphoma patients and control populations, young con-trols were mainly chosen from patients with sarcoma and fractures.To our knowledge, this is the first case-control study on the association between HBV infection and non-Hodgkin ’s lymphoma, using two groups of age- and sex-matched controls. Our results suggest that chronic HBV infection might play a pathogenic role in lymphomagenesis in a cer-tain subset of patients, especially in the younger age groups. Our findings warrant further investigation, includ-ing a prospective cohort study and molecular studies to examine the role of HBV in the pathogenesis of non-Hodgkin ’s lymphoma.ACKNOWLEDGMENTSThis study was supported in part by the 1999 BK21 project for Medicine, Dentistry and Pharmacy.(Received January 11, 2002/Revised February 28, 2002/Accepted March 4, 2002)REFERENCES1)Devesa, S. S. and Fears, T. Non-Hodgkin ’s lymphoma timetrends: United States and international data. Cancer Res.,52 (Suppl.), 5432s –5440s (1992).2)Ferri, C., Caracciolo, F., Zignego, A. L., La Civita, L.,Monti, M., Longombardo, G., Greco, F. and Capochiani, E.Hepatitis C virus infection in patients with non-Hodgkin ’s lymphoma. Br. J. Haematol., 88, 392–394 (1994).3)Silvestri, F., Pipan, C., Barillari, G., Zaja, F., Fanin, R.,Infanti, L., Russo, D., Falasca, E., Botta, G. A. and Baccarani, M. Prevalence of hepatitis C virus infection in patients with lymphoproliferative disorders. Blood , 87,4296–4301 (1996).4)Zuckerman, E., Zuckerman, T., Levine, A. M., Douer, D.,Gutekunst, K., Mizokami, M., Qian, D. G., Velankar, M.,Nathwani, B. N. and Fong, T.-L. Hepatitis C virus infec-tion in patients with B-cell non-Hodgkin ’s lymphoma. Ann.Intern. Med., 127, 423–428 (1997).5)Ferri, C., Monti, M., La Civita, L., Longombardo, G.,Greco, F., Pasero, G., Gentilini, P., Bombardieri, S. and Zignego, A. L. Infection of peripheral blood mononuclear cells by hepatitis C virus in mixed cryoglobulinemia.Blood , 82, 3701–3704 (1993).6)Yoffe, B., Burns, D. K., Bhatt, H. S. and Combes, B.Extrahepatic hepatitis B virus DNA sequences in patients with acute hepatitis B infection. Hepatology , 12, 187–192(1990).7)Mason, A., Wick, M., White, H. and Perrillo, R. HepatitisB virus replication in diverse cell types during chronic hep-atitis B virus infection. Hepatology , 18, 781–789 (1993).8)Stoll-Becker, S., Repp, R., Glebe, D., Schaefer, S., Kreuder,J., Kann, M., Lampert, F. and Gerlich, W. H. Transcription of hepatitis B virus in peripheral blood mononuclear cells from persistently infected patients. J. Virol., 71, 5399–5407 (1997).9)Liang, R. H. S., Lok, A. S. F., Lai, C. L., Chan, T. K.,Todd, D. and Chiu, E. K. W. Hepatitis B infection in patients with lymphomas. Hematol. Oncol., 8, 261–270(1990).10)Lok, A. S. F., Liang, R. H. S., Chiu, E. K. W., Wong, K. L.,Chan, T. K. and Todd, D. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy. Report of a prospective study. Gastroenterology , 100, 182–188(1991).11)Kumagai, K., Takagi, T., Nakamura, S., Sawada, U., Kura,HBV Infection and B-Cell NHL477Y., Kodama, F., Shimano, S., Kudoh, I., Nakamura, H.,Sawada, K. and Ohnoshi, T. Hepatitis B virus carriers in the treatment of malignant lymphoma: an epidemiological study in Japan. Ann. Oncol., 8 (Suppl. 1), S107–S109(1997).12)Markovic, S., Drozina, G., Vovk, M. and Fidler-Jenko, M.Reactivation of hepatitis B but not hepatitis C in patients with malignant lymphoma and immunosuppressive ther-apy. A prospective study in 305 patients. Hepatogastroen-terology , 46, 2925–2930 (1999).13)Cucuianu, A., Patiu, M., Duma, M., Basarab, C., Soritau,O., Bojan, A., Vasilache, A., Mates, M. and Petrov, L.Hepatitis B and C virus infection in Romanian non-Hodgkin ’s lymphoma patients. Br. J. Haematol., 107, 353–356 (1999).14)Kuniyoshi, M., Nakamuta, M., Sakai, H., Enjoji, M.,Kinukawa, N., Kotoh, K., Fukutomi, M., Yokota, M., Nishi,H., Iwamoto, H., Uike, N., Nishimura, J., Inaba, S., Maeda,Y., Nawata, H. and Muta, K. Hepatitis B or C virus infec-tions and non-Hodgkin ’s lymphoma. J. Gastroenterol.Hepatol., 16, 215–219 (2001).15)Ann, Y. O., Kim, Y. S., Lee, M. S. and Shin, M. H. Hepa-titis B virus infection rate among Koreans. Seoul J. Med.,33, 105–114 (1992).16)Kim, Y. S., Pai, C. H., Chi, H. S., Kim, D. W., Min, Y. I.and Ann, Y. O. Prevalence of hepatitis C virus antibody among Korean adults. J. Kor. Med. Sci., 7, 333–336(1992).17)The Non-Hodgkin ’s Lymphoma Pathologic Classification Project. National Cancer Institute sponsored study of classi-fications of non-Hodgkin ’s lymphomas: summary anddescription of a working formulation for clinical usage.Cancer , 49, 2112–2135 (1992).18)Pontisso, P., Poon, M. C., Tiollais, P. and Brechot, C.Detection of hepatitis B virus DNA in mononuclear blood cells. Br. Med. J., 288, 1563–1566 (1984).19)Yoffe, B., Noonan, C. A., Melnick, J. L. and Hollinger, F.B. Hepatitis B virus DNA in mononuclear cells and analy-sis of cell subsets for the presence of replicative intermedi-ates of viral DNA. J. Infect. Dis., 153, 471–477 (1986).20)Galun, E., Ilan, Y., Livni, N., Ketzinel, M., Nahor, O.,Pizov, G., Nagler, A., Eid, A., Rivkind, A., Laster, M., Ron,N., Blum, H. E. and Shouval, D. Hepatitis B virus infection associated with hematopoietic tumors. Am. J. Pathol., 145,1001–1007 (1994).21)Hausen, H. Z. Viruses in human cancers. Science , 254,1167–1173 (1991).22)Nagington, J., Cossart, Y. E. and Cohen, B. J. Reactivation of hepatitis B after transplantation operations. Lancet , i ,558–560 (1977).23)Blanpain, C., Knoop, C., Delforge, M. L., Antoine, M.,Peny, M. O., Liesnard, C., Vereerstraeten, P., Cogan, E.,Adler, M. and Abramowicz, D. Reactivation of hepatitis B after transplantation in patients with pre-existing anti-hepa-titis B surface antigen antibodies: report on three cases and review of the literature. Transplantation , 66, 883–886(1998).24)Kane, M. Global programme for control of hepatitis B infection. Vaccine , 13 (Suppl. 1), S47–S49 (1995).25)Chen, D.-S. Natural history of chronic hepatitis B virus infection: new light on an old story. J. Gastroenterol.Hepatol., 8, 470–475 (1993).。