JCAD Study
- 格式:pdf
- 大小:412.90 KB
- 文档页数:7

第1篇一、开场白及自我介绍1. 题目:- Good morning/afternoon, Professor [Last Name]. Thank you forjoining us today. To start, could you please introduce yourself and provide a brief overview of your academic background?参考答案:- Good morning/afternoon, everyone. It's a pleasure to be here today. My name is [Your Name], and I am currently an Associate Professor at [Your University/Institution]. I specialize in [Your Field of Study],and my research focuses on [Brief Description of Your Research Focus]. I have been teaching at [Your University/Institution] for [Number of Years] years, and during this time, I have developed a strong passion for both teaching and research.2. 题目:- Can you tell us about your most significant academic achievement or publication?参考答案:- One of my most significant academic achievements is the publication of my book, "Title of the Book," which was released in [Year]. This book explores [Topic of the Book] and has been well-received by both academics and the general public. It has been cited in several research papers and has contributed to the advancement of knowledge in my field.二、专业知识及研究3. 题目:- Can you describe a recent research project that you have been involved in? What was the goal of the project, and what were the key findings?参考答案:- I recently led a research project titled "Project Title," which aimed to investigate [Objective of the Project]. The project involved [Description of Methods Used], and the key findings were [Summary of Findings]. Our research has provided new insights into [Area of Study] and has the potential to influence [Relevant Field or Practice].4. 题目:- How do you incorporate the latest developments in your field into your teaching and research?参考答案:- I stay updated with the latest developments in my field through continuous reading, attending conferences, and collaborating with other scholars. In my teaching, I ensure that my courses are current and that I incorporate recent research findings and case studies. This not only keeps my students engaged but also equips them with the most up-to-date knowledge in their field.三、教学经验及方法5. 题目:- Can you describe a teaching method that you have found particularly effective in your classroom?参考答案:- One teaching method that I have found particularly effective is the use of problem-based learning (PBL). In PBL, students are presented with real-world problems that they must work on in groups. This approach encourages critical thinking, teamwork, and the application of theoretical knowledge to practical situations. It has been very successful in engaging students and promoting deeper understanding of the subject matter.6. 题目:- How do you assess student performance in your courses?参考答案:- I use a variety of assessment methods to evaluate student performance, including written exams, presentations, research papers, and practical assignments. These assessments are designed to test a range of skills, from theoretical knowledge to practical application. I also provide feedback on student work to help them understand their strengths and areas for improvement.四、学术交流与合作7. 题目:- Can you tell us about a collaborative project you have been involved in with another academic or institution?参考答案:- I have been involved in a collaborative project with Professor [Collaborator's Name] from [Collaborator's Institution] titled "Project Name." This project aimed to [Objective of the Project]. We worked together to [Description of Collaboration], and the outcomes have been [Summary of Outcomes]. This collaboration has been mutually beneficial and has enhanced both our research and teaching efforts.8. 题目:- How do you stay motivated to continue producing high-quality research and teaching?参考答案:- Staying motivated is crucial in both research and teaching. I find inspiration in the potential impact of my work, both on the academic community and in the broader context. The passion for my field, the enthusiasm of my students, and the support of my colleagues and institution all contribute to my motivation. Additionally, I set clear goals and timelines for my research and teaching activities, which helps me stay focused and productive.五、未来规划及贡献9. 题目:- What are your future research plans, and how do you envision contributing to your field?参考答案:- My future research plans include [Description of Future Research Directions]. I aim to [Goals of Future Research]. I believe that by addressing these questions, I can contribute to the advancement of [Your Field of Study] and provide practical solutions to [Specific Challenges or Issues]. I am also committed to mentoring young scholars and passing on my knowledge and experience.10. 题目:- How do you think you will contribute to the academic community at our institution?参考答案:- I am excited about the opportunity to contribute to the academic community at your institution. I plan to actively engage in interdisciplinary research, collaborate with faculty members across departments, and contribute to the development of new courses and programs. I also intend to mentor graduate students and junior faculty, helping them to grow professionally and academically.六、总结11. 题目:- Is there anything else you would like to add that we haven't discussed yet?参考答案:- Yes, I would like to emphasize my enthusiasm for joining your institution and contributing to its academic excellence. I amparticularly interested in the opportunities for collaboration and the supportive environment that I have observed here. I am confident that myresearch and teaching experiences will be valuable assets to your institution, and I am looking forward to making a positive impact.This concludes the interview. Thank you for your time and consideration.---The above response templates are designed to provide a comprehensive guide for an Associate Professor's English interview. The actual content should be tailored to the individual's specific experiences, research, and teaching philosophy.第2篇Introduction:The following set of questions is designed to assess the candidate’s qualifications, expertise, teaching philosophy, research interests, and ability to contribute to the academic community. The questions are categorized into different sections to provide a comprehensive evaluation of the candidate’s suitability for the position of Associate Professor in English Language and Literature.Section 1: Background and Qualifications1. Academic Background:- Can you describe your academic journey from undergraduate to doctoral studies?- What inspired you to pursue a career in English Language and Literature?2. Research Experience:- What are your primary research interests within English Language and Literature?- Can you provide an overview of your research methodology and findings?- How have your research projects contributed to the field?3. Teaching Experience:- What teaching roles have you held in your academic career?- Describe your teaching philosophy and approach to student engagement.- How do you assess student learning and provide feedback?4. Publications and Presentations:- Can you list your recent publications and the impact they have had?- What role do conferences and workshops play in your academic development?- How do you stay updated with the latest trends and developments in your field?Section 2: Teaching and Pedagogical Skills5. Course Development:- What courses have you taught or are you interested in teaching at this institution?- How do you approach the development of new courses or the revision of existing ones?6. Student Engagement:- How do you create an inclusive and supportive learning environment for diverse student populations?- Can you provide an example of a successful student engagement strategy you have used?7. Technology in Teaching:- How do you incorporate technology into your teaching practices?- What are your thoughts on the use of online platforms and virtual learning in higher education?8. Assessment and Evaluation:- What methods do you use to assess student performance in your courses?- How do you ensure that assessments are fair, valid, and reliable?Section 3: Research and Scholarship9. Current Research Projects:- What are you currently working on in terms of research?- How do you plan to continue your research at this institution?10. Collaboration and Mentorship:- How do you collaborate with colleagues on research projects?- What is your approach to mentoring graduate students and postdoctoral researchers?11. Research Impact:- How do you measure the impact of your research on the field and beyond?- What strategies do you employ to disseminate your research findings?Section 4: Contribution to the Academic Community12. Service to the University:- How have you contributed to the academic community within your current institution?- What roles have you played in university governance and committees?13. Community Engagement:- How do you engage with the local community through your academic work?- Can you provide an example of a community-based project orinitiative you have led or participated in?14. Professional Development:- What professional development activities do you engage in to enhance your teaching and research?- How do you stay connected with the broader academic community?Section 5: Future Plans and Vision15. Long-Term Goals:- What are your long-term career goals as an Associate Professor?- How do you envision your research and teaching evolving over the next decade?16. Institutional Fit:- Why are you interested in joining this particular institution?- How do you see your work contributing to the mission and values of the university?17. Closing Questions:- Is there anything else you would like to share with us about your qualifications or experiences that we have not covered?- How do you see yourself contributing to the English Language and Literature department at this institution?Conclusion:This comprehensive set of interview questions is designed to provide a thorough assessment of the candidate’s suitability for the position of Associate Professor in English Language and Literature. It aims to evaluate their academic background, teaching and research skills, contributions to the academic community, and their vision for the future. The candidate’s responses will be car efully considered to determinetheir potential to excel in this role and to further the academic excellence of the institution.第3篇一、自我介绍1. 请简要介绍您的个人信息,包括姓名、年龄、籍贯、教育背景等。

尼可地尔联合麝香保心丸对冠心病心绞痛患者高敏C反应蛋白及基质金属蛋白酶-9的影响张洪霞;李文杰【摘要】目的:观察尼可地尔联合麝香保心丸对冠心病心绞痛患者血清中高敏C 反应蛋白(hs-CRP)及基质金属蛋白酶-9(MMP-9)的影响。
方法选择60例经确诊为冠心痛心绞痛的患者,分为2组,对照组给予正规西药治疗;治疗组在正规西药治疗的基础上加尼可地尔及麝香保心丸治疗。
所有患者均于入院时以及治疗后8周测高敏C反应蛋白(hs-CRP)、基质金属蛋白酶-9(MMP-9)。
结果治疗组治疗后hs-CRP为(114.99±31.84)mg/L、MMP-9为(188.04±121.01)ng/mL,各项水平明显低于对照组(P<0.05)。
结论尼可地尔联合麝香保心丸通过抗炎机制与西药联合对冠心痛心绞痛的治疗具有肯定的疗效。
%Objective To observe the effect of nicorandil combined with Shexiang Baoxin Pill on coronary heart disease angina pectoris of serum C reactive protein (hs-CRP) and matrix metalloproteinase-9 (MMP-9) effect.Methods 60 cases of hospitalized patients with -12 in the Department of internal medicine in January 2013 were selected. Diagnosed as coronary heart disease and angina pectoris weredivided into two groups, the control group was given regular treatment of Western medicine; treatment group given regular western medicine plus nicorandil and musk to guarantee the heart pill treatment. All patients on admission and 8 weeks after treatment test of high sensitive C reactive protein (hs-CRP), matrix metalloproteinase -9 (MMP-9).Results After treatment, the hs-CRP was (114.99±31.84)mg/L, MMP-9 was (188.04±121.01)ng/mL, and the levels were significantly lower thanthose in the control group (P<0.05).Conclusion Nicorandil musk protecting heart pill by anti-inflammatory mechanism and Western medicine combined with the crown heartache has a positive role in treatment of angina pectoris.【期刊名称】《当代医学》【年(卷),期】2016(000)005【总页数】2页(P144-145)【关键词】心绞痛;尼可地尔;麝香保心丸;C反应蛋白;基质金属蛋白酶-9【作者】张洪霞;李文杰【作者单位】辽宁 110003 沈阳市第七人民医院辽宁中医药大学附属第一医院;辽宁 110003 沈阳市第七人民医院辽宁中医药大学附属第一医院【正文语种】中文当今社会人口逐渐趋于老龄化,冠心病已成为人类最显见的心血管系统疾病,严重危害着人类身心健康。

陕西省校本研修30问(英文版)philosophy of school-based research is to promote the nal development of teachers and XXX。
school-based research should be based on the actual needs of the school and the teachers。
Third。
school-based research should be XXX。
with the support of the school leadership.4.What are the benefits of school-based research?School-based research can improve the quality of n。
promote the nal development of teachers。
XXX development of the school。
It can also promote curriculum reform。
balance basic n resources。
and XXX.5.How can school-based research be carried out?School-based research can be carried out through us methods。
such as n research。
case studies。
experimental research。
XXX。
The key is to ensure that the research is based on the actual needsof the school and the teachers。
and that it is XXX.6.What are the challenges of school-based research?The challenges of school-based research include the lack of research skills among teachers。


尼可地尔治疗冠心病慢性心力衰竭疗效观察周温【摘要】Objective To observe the clinical effect of Nicorandil on heart failure caused by coronary heart disease. Methods 228 patients of heart failure caused by coronary heart disease were randomly divided into the study group (n=108) and the control group (n=120). Patients in the control group were given conventional treatment, while those in the study group were given Nicorandil on the basis of conventional treatment. The variation of Brain Natriuretic Peptide (BNP) one month after treatment, and left ventricular ejection fraction (LVEF), ventricular septal thickness (TVS), left ventricular posterior wall thickness (LVP), left ventricular end diastolic diameter (LVEDD) and left ventricular end systolic diameter (LVESD) five months after treatment were compared between the two groups. Results Compared with the control group, the decrease of BNP, IVS, LVP, LVEDD and LVESD in the study group after treatment was more significantly (P<0.05), and the increase of LVEF in the study group was more significantly (P<0.05). Conclusion Nicorandil can treat heart failure caused by coronary heart disease effectively and improve the cardiac function.%目的观察尼可地尔治疗冠心病慢性心力衰竭的临床疗效.方法选取在我院住院的冠心病慢性心力衰竭患者228例,随机分成实验组和对照组,对照组予常规治疗,实验组在对照组治疗方案的基础上加用尼可地尔治疗,以1个月为一个疗程,出院后随访观察5个月,观察治疗1个月后两组患者脑钠肽(BNP)值的变化以及随访5个月后左室射血分数(LVEF值)、室间隔厚度(IVS)、左室后壁厚度(LVP)、左室舒张末期内径(LVEDD)、左室收缩末期内径(LVESD)的变化.结果实验组BNP值、IVS、LVP、LVEDD、LVESD值较对照组治疗后降低明显,LVEF值较对照组治疗后升高明显(P<0.05).结论尼可地尔可以治疗冠心病慢性心力衰竭,改善患者症状的心功能.【期刊名称】《海南医学》【年(卷),期】2012(023)004【总页数】3页(P18-20)【关键词】尼可地尔;冠心病;心力衰竭;脑钠肽;左室射血分数【作者】周温【作者单位】海口市秀英区海秀卫生院普通内科,海南海口570311【正文语种】中文【中图分类】R541.4冠状动脉粥样硬化性心脏病(Coronary atherosclerotic heart disease)简称冠心病,是指冠状动脉粥样硬化使血管腔狭窄或阻塞或(和)冠状动脉功能性或器质性病变(痉挛)导致心肌缺血缺氧或坏死而引起的心脏病[1]。
Studying in College: A Journey of Discoveryand GrowthCollege life is an exciting and transformative phase of one's academic journey. It marks a significant transition from the familiar environment of high school to the world of independent learning and exploration. As students step onto the college campus, they embark on a new adventure filled with challenges, opportunities, and personal growth. **Embracing the Challenge of Independence**One of the most significant aspects of college life is the独立自由 it affords. Unlike high school, where students often have a more structured schedule and routine, college expects them to take charge of their own learning. This independence requires students to manage their time effectively, balance学术学业与其他responsibilities, and make informed decisions about their educational path.**Exploring a Wide Range of Courses**Colleges offer a diverse array of courses, allowing students to explore their interests and passions. Whetherit's delving into the mysteries of science, understandingthe intricacies of humanities, or learning about the global perspectives in international relations, college courses provide the perfect platform for intellectual curiosity. These courses not only enhance students' knowledge and skills but also help them discover new interests and hobbies.**Developing Critical Thinking Skills**College is not just about acquiring knowledge; it's also about developing critical thinking skills. In college, students are encouraged to question assumptions, analyze complex problems, and evaluate information critically. This process of critical thinking helps them become more discerning consumers of knowledge and effective communicators in various settings.**Connecting with Peers and Mentors**College is also a time for making meaningful connections with peers and mentors. Students have the opportunity to meet people from diverse backgrounds and perspectives, creating a rich and diverse learning environment. These relationships not only enhance theirsocial life but also provide valuable support and guidance during their academic journey.**Preparing for the Future**Finally, college serves as a launching pad forstudents' future careers. It provides them with the necessary skills, knowledge, and experience to succeed in their chosen fields. Whether it's through internships, extracurricular activities, or networking opportunities, college helps students build a strong foundation for their future success.**大学学习的探索与成长之旅**大学生活是学术旅程中令人兴奋且充满变革的一个阶段。
高尿酸血症与急性冠脉综合征的相关性彭民安;刘传垠;万凤福;王雪樵;易志强【摘要】目的:探讨高尿酸血症与急性冠脉综合征之间的相关性.方法:对178例冠心病患者进行血尿酸测定,并与正常对照组比较;同时将冠心病组患者分为急性冠脉综合征组和稳定性心绞痛组,进行血尿酸水平比较.结果:冠心病组血尿酸水平显著高于正常对照组(P<0.05);高尿酸血症患者的冠心病发生率明显高于正常尿酸者;急性冠脉综合征组血清尿酸水平显著高于稳定性心绞痛组(P<0.05).结论:高尿酸血症与急性冠脉综合征发生密切相关.【期刊名称】《赣南医学院学报》【年(卷),期】2013(033)003【总页数】3页(P358-360)【关键词】高尿酸血症;急性冠脉综合征;血尿酸【作者】彭民安;刘传垠;万凤福;王雪樵;易志强【作者单位】江西省吉安市中心人民医院,江西吉安343000;江西省吉安市中心人民医院,江西吉安343000;江西省吉安市中心人民医院,江西吉安343000;江西省吉安市中心人民医院,江西吉安343000;江西省吉安市中心人民医院,江西吉安343000【正文语种】中文【中图分类】R541.4尿酸是核酸代谢的产物,尿酸生成过多和(或)排泄减少均可致高尿酸血症。
自1951年Gertler[1]等首次提出尿酸与心血管疾病之间可能存在复杂的相互作用以来,国内外学者围绕这一问题展开了大量研究。
目前大量国外资料表明高尿酸症与冠心病在流行病学、发病机制及治疗上密切相关,受到临床重视。
本研究旨在探讨高尿酸血症与急性冠脉综合征的相关性。
1 资料与方法1.1 一般资料研究对象为于2010年1月至2012年8月在我院经冠状动脉造影检查确诊为冠心病的178例冠心病患者,其中男97例,女81例,平均年龄(59.8±11.3)岁。
选择同期门诊体检无明显冠心病病史的180例患者(无典型心绞痛症状及普通心电图和活动平板试验均无心肌缺血改变)作为对照组,其中男98例,女82例,平均年龄(54.3±10.1)岁;冠心病组中又分为急性冠脉综合征组和稳定性心绞痛组,其中急性冠脉综合征组92例,稳定性心绞痛组86例。
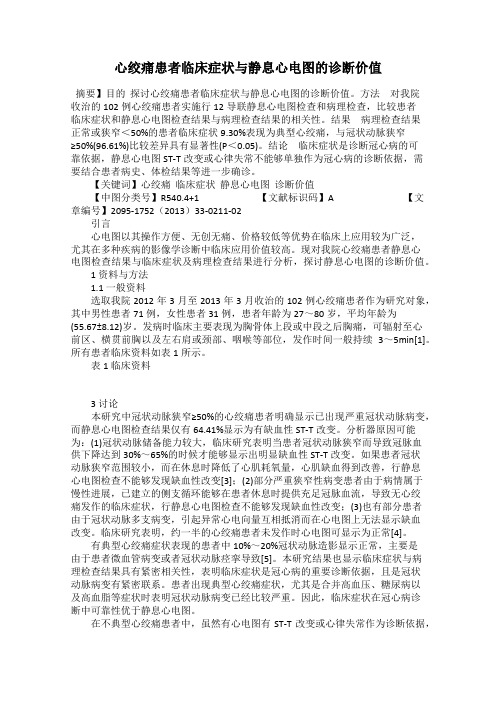
Circulation Journal Vol.73, May 2009Circ J 2009; 73: 885 – 891ince Klein et al reported the relation between uric acid (UA) level and coronary artery disease (CAD) in1973,1 the question of whether high UA is a risk factor for arteriosclerosis and CAD has remained con-troversial. Although a correlation between UA level and cardiovascular events was not observed in the Framinghamstudy,2 it has been demonstrated in studies of hypertensive patients in the worksite,3 in the PIUMA4 and SHEP studies,5 and in the Syst-China Trial.6 Moreover, it was recently reported that UA level may be a new predictor of athero-sclerosis.7,8 In Japan, a study of an employee cohort 9 anda long-term follow-up survey of atomic bomb survivors 10demonstrated that high UA was an independent predictor for cardiovascular disease. However, no study has been con-ducted on the correlation in patients with higher cardiovas-cular risk, such as CAD.This study was a subanalysis of data from the JapaneseCoronary Artery Disease Study,11 to examine whether ele-vated UA is an independent predictor of all events including cardiovascular events and all-cause mortality. The study was a 3-year follow-up of high-risk patients who had coronary artery stenosis ≥75% according to the classification of the American Heart Association.MethodsStudy PatientsA total of 13,812 patients who were diagnosed as having stenosis ≥75% (American Heart Association classification) by coronary angiography in at least 1 branch of the coronary arteries were enrolled in the Japanese Coronary Artery Disease Study between April, 2000 and March, 2001.This subanalysis targeted 8,832 patients (6,781 men, 2,051 women; mean age 65.5±9.7 years) whose UA data were available at registration and after 6 months.Study DesignThe details of the Japanese Coronary Artery DiseaseStudy have been published.11,12 Briefly, all follow-up data were collected in a database over the internet and all the information was entered by the study investigators. The information collected at registration consisted of medica-tion, established CAD risk factors, the underlying condition,(Received August 28, 2008; revised manuscript received January 5, 2009; accepted January 6, 2009; released online March 31, 2009)Department of Integrated Medicine and Informatics, Ehime University Graduate School of Medicine, Ehime, *Department of Clinical Epide-miology and Systems, **Translational Research for Health Care and Clinical Science and †Cardiovascular Medicine, Graduate School of Medicine, Faculty of Medicine, The University of Tokyo, Tokyo, Japan Mailing address: Takafumi Okura, MD, Department of Integrated Medicine and Informatics, Ehime University Graduate School of Medi-cine, Toon, Ehime 791-0295, Japan. E-mail: okura@m.ehime-u.ac.jp All rights are reserved to the Japanese Circulation Society. For permis-sions, please e-mail: cj@j-circ.or.jpElevated Serum Uric Acid is an Independent Predictorfor Cardiovascular Events in Patients WithSevere Coronary Artery StenosisSubanalysis of the Japanese CoronaryArtery Disease (JCAD) StudyTakafumi Okura, MD; Jitsuo Higaki, MD; Mie Kurata, MD; Jun Irita, MD; Ken-ichi Miyoshi, MD;Tsutomu Yamazaki, MD*; Doubun Hayashi, MD**; Takahide Kohro, MD**;Ryozo Nagai, MD † for the JCAD Study InvestigatorsBackground: The association of elevated serum uric acid (UA) with cardiovascular events in patients with severe coronary artery stenosis was examined.Methods and Results: Patients with stenosis ≥75% (n=8,832) were followed for “all events” (cardiovascular events and all-cause mortality) for 3 years. The group was divided into quartiles based on baseline UA level. The incidence rate of all events was significantly different among quartiles (58.3, 56.5, 61.2, 76.3/1,000 patients-year, P<0.001). Cox’s proportional hazard regression analysis showed that the hazard ratio (HR) for all events was 1.25 [95% confidence interval (CI): 1.07–1.45, P<0.01] in the highest quartile (UA ≥6.8 mg/dl). The group in which UA increased ≥1.0 mg/dl after 6 months had significantly higher cardiovascular events rate than the group in which UA did not change (70.6 vs 58.8/1,000 patients-year, P=0.042). Propensity score matching was performed and 4,206 patients were divided into the highest quartile and the rest. High UA remained an independent predictor of all events (HR 1.25, 95%CI 1.06–1.43). However, no significant difference was observed between the group with increased UA ≥1.0 mg/dl and the group with unchanged UA level.Conclusions: Elevated UA is an independent predictor of cardiovascular events and all-cause mortality com-bined in patients with coronary artery stenosis. (Circ J 2009; 73: 885 – 891)Key Words: Cardiovascular events; JCAD study; Uric acidSORIGINAL ARTICLE Epidemiology886OKURA T et al.Circulation Journal Vol.73, May 2009887Uric Acid and CAD in Japan Circulation Journal Vol.73, May 2009the medical history (disease and treatment), the site and degree of stenosis, and medical procedures undertaken after coronary angiography. The information on CAD risk factors and clinical laboratory values was collected at registration and every 6 months thereafter for 3 years.The primary endpoint was “all events”, defined as cardio-vascular events and all-cause mortality. Detailed informa-tion was collected regarding cardiovascular events, all-cause mortality, treatment, and outcome. All events registered in the database were defined by all-cause mortality and cardio- and cerebrovascular events. Angiographic restenosis found during routine coronary angiography without symptoms was excluded.We divided the 8,832 patients into quartiles based on baseline UA level and compared the incidence of all events and cardiac events among the 4 groups. Study patients were placed in a quartiles regardless of hyperuricemic medica-tion. The group was also divided into 2 subgroups according to the changes in UA at 6 months after registration. The increased UA group included patients with a UA increasing by more than 1.0 mg/dl and the non-increased UA group included those whose UA did not change or increased by <1.0 mg/dl.To reduce the effect of medications that directly affect serum UA level, we also conducted propensity score match-ing. A propensity score for each patient was calculated by multivariate logistic regression analysis, taking into account the CAD risk factors and medications that directly affect the serum UA level, including α1-blockers, calcium-channel blockers, angiotensin-converting enzyme inhibitors, diuretics, losartan, uricosuric drugs, and UA synthesis inhibitors. We then divided 4,206 patients into the highest quartile (UA ≥6.8 mg/dl) and the rest, and compared the results.Statistical AnalysisFor patient baseline characteristics, the difference in percentage was evaluated among the 4 groups by χ2 test. Continuous variables are expressed as mean ± standard deviation, and the difference among the 4 groups was evalu-ated by Kruscal-Wallis test. Cumulative incidence of events was estimated by the Kaplan-Meier product-limit methodand compared by log-rank test in the events. The multivari-ate analysis was performed using the Cox hazard ratio (HR) model, and expressed with 95% confidence intervals (CI). Statistical analysis was performed with SAS version 8.02 (SAS Institute Inc, Cary, NC, USA).ResultsBaseline Patient CharacteristicsBaseline patient characteristics were compared among the 4 groups (Table 1): there were significant differences among the quartiles in age, sex, the number of stenoses, hypertension, hyperlipidemia, impaired glucose tolerance, obesity, smokers, alcohol users, and congestive heart failure (CHF). However, there was no difference in the rate of CAD familial history and left main CAD (LMT).Incidence Rates of EventsTable 2 shows the association between baseline UA and subsequent events by sex and each endpoint. The total inci-dence rates of all events were significantly different among the 4 groups (58.3, 56.5, 61.2, 76.3/1,000 patients-year, P< 0.001). Cardiac mortality and morbidity for total and female patients were significantly different among quartiles, but not for male patients. When the cardiac events were divided into CAD events (ie, acute myocardial infarction, unstable angina pectoris, and coronary artery bypass graft) and other events (ie, arrhythmia, CHF, and cardiopulmonary arrest on arrival), the incidence of CAD events was not significantly different among quartiles. However, other events were sig-nificantly different. On the other hand, the incidence rate of cerebral death and events did not differ among the 4 groups.Cumulative Incidence of EventsThe cumulative incidence of all events and cardiac events that occurred during the 3 years in the quartiles was com-pared with a Kaplan-Meier curve (Figure 1). The HRs were significantly different among quartiles (1.00, 0.99, 1.06, 1.31, P<0.001). The results by sex showed a similar trend (Figures 2a ,b ).The cumulative incidence of all events in thepatientsFigure 1. Comparison of cumulative inci-dence of cardio-and cerebrovascular events including all-cause death among quartiles with uric acid ≥6.8 mg/dl (gray broken line), 5.8–6.7 mg/dl (gray solid line), 4.8–5.7 mg/dl (black broken line), and <4.7 mg/dl (black solid line). HR, hazard ratio; CI, confidence interval.888OKURA T et al.Circulation Journal Vol.73, May 2009with UA increasing by ≥1.0 mg/dl after 6 months compared with those with unchanged UA is shown by Kaplan-Meier curve (Figure 3a ). The event rate in the increased UA group was 70.6, vs 58.8/1,000 patient-years in the group with no increase (P=0.042).Association of UA With Risk for All EventsThe HR for all events, including cardiac and cerebrovas-cular events, and all-cause mortality was 1.25 (1.07–1.45, P<0.01) in the highest quartile when adjusted for sex, age, hyperlipidemia, impaired glucose tolerance, hypertension, obesity, smoking, drinking, CAD familial history, CHF, LMT, and the number of stenoses, suggesting that elevated serum UA was an independent predictor for cardiovascular events (Table 3).Propensity Score AnalysisBaseline patient characteristics adjusted by propensity score analysis were compared between the 2 groups (Table 4). Even after adjustment for CAD risk factors and medicationsdirectly affecting serum UA level, the incidence rate of all events was significantly higher in the highest quartile than in the others (Table 5). When analyzed by each endpoint, results were similar to that of all events, except for mortality. The HR calculated by the Cox HR model was 1.23 (95%CI 1.06 –1.43, P<0.01), which was similar to that of all patients (Table 6). However, the cumulative incidence of all events in the patients with UA increased ≥1.0 mg/dl after 6 months was not significantly different from that of patients with unchanged UA (Figure 3b ).DiscussionThe Japanese Coronary Artery Disease Study 11 targeted patients who had a severe stenosis in their coronary arteries diagnosed by coronary angiography, which conferred an equivalent risk of CAD as in Western patients. We per-formed a subanalysis of cardio- and cerebrovascular events and all-cause mortality among quartiles based on baseline UA. The UA of the highest quartile was >6.8 mg/dl. TheFigure 2. Comparison of cumulative incidence of cardio- and cerebrovascular events includ-ing all-cause death by quartiles of uric acid ≥6.8 mg/dl (gray broken line), 5.8–6.7 mg/dl (gray solid line), 4.8–5.7 mg/dl (black broken line), and <4.7 mg/dl (black solid line) in (a ) male and (b ) female patients. HR, hazard ratio;CI, confidence interval.889Uric Acid and CAD in Japan Circulation Journal Vol.73, May 2009incidence of cardio- and cerebrovascular events and all-cause mortality was higher in the highest quartile than in the others. The results demonstrate that elevated UA was an important risk factor for cardio- and cerebrovascular events and all-cause mortality combined in patients who had severe coro-nary artery stenosis. Cox’s proportional hazard regression analysis showed that the HR for all events was 1.25 (95%CI 1.07–1.45, P<0.01) in the highest quartile (UA ≥6.8 mg/dl). It showed that UA was still an independent predictor for all events, including all-cause death and cardio–cerebrovas-cular events.A similar relationship between elevated UA and cardio-vascular events, such as myocardial infarction and stroke, has been demonstrated in numerous large-scale clinicalstudies. In the NHANES I Study,13 a high level of UA was an independent predictor for cardiovascular disease in both men and women. The incidence of cardiac death increased in men with UA >7.0 mg/dl, and in women with UA >5.6 mg/dl. Bickel et al reported similar findings to the Japanese Coro-nary Artery Disease Study in patients with CAD diagnosedFigure 3. Comparison of cumulative incidence of cardio- and cerebrovascular events includ-ing all-cause death in patients with change in uric acid (UA) level ≥1.0 mg/dl (gray line) and <1.0 mg/dl (black line) before (a ) and after (b ) propensity score matching. HR, hazard ratio; CI, confidence interval.890OKURA T et al.Circulation Journal Vol.73, May 2009by coronary angiography. The HR for death in their reportwas 1.30 in women and 1.39 in men,14 suggesting that ele-vated UA is an independent risk factor for death. Accord-ing to our study results, the HR for cardiac events of 1.25 (95%CI 1.07–1.45, P<0.01) in Japanese patients was compa-rable to the HR for death of patients in Western countries.In Japan, Tomita et al’s employee survey 9 found that in patients with UA >8.5 mg/dl, the HR for death from CAD and for cerebrovascular death increased to 1.7 and 2.6, respectively. In our study, the highest quartile showed the same tendency when we focused only on the endpoint of cardiac events. However, the HR did not increase for cere-bral events. Although the incidence of cerebral events is greater than that of cardiac events in the Japanese general population, patients with severe coronary stenosis were tar-geted in the Japanese Coronary Artery Disease Study, which may be reflected in our results that the incidence of cardiac events was much greater than that of cerebral events.When the cardiac events were divided into CAD events and other events, for other events only there was a signifi-cant difference among baseline UA quartiles in terms of both mortality and morbidity. Strasak et al reported similarresults in their cohort study of 83,683 male patients.15 In the present study, CHF accounted for approximately 75% of other events. Recent in vitro and in vivo findings suggest that UA contributes directly to endothelial dysfunction by inducing antiproliferative effects and impairing nitric oxideproduction,16 thus causing a deterioration of CHF. Sakai et al 17 recently demonstrated that in patients with mildto891Uric Acid and CAD in Japan Circulation Journal Vol.73, May 2009severe CHF, not only high plasma concentrations of B-type natriuretic peptide but also high UA concentrations were likely to be independent predictors of mortality. They con-cluded that monitoring both of these parameters may be important in the management of CHF patients.In the present study, the UA level was not significantly associated with the incidence of CAD, which is consistent with the findings of previous studies including theFramingham Heart Study,2 Wannamethee et al,18 and theARIC study.19 On the other hand, it has been reported that human atherosclerotic plaque contains a considerable amount of UA, and hyperuricemia may promote thrombus forma-tion via purine metabolism.20,21 Strasak et al 22 reported that UA is an independent predictor for acute and subacute forms of CAD, so we cannot conclude that there is no association between UA and CAD. However, UA may have a stronger effect on dysfunction of the heart than CAD.When analyzed by sex, the association of UA with event risk was higher in female patients than in male patients. In the NHANES I Study 13 and ARIC study 19 the cut-off value increasing CAD risk was higher by approximately 1 mg/dl in male patients compared with female patients. In the present study, we assumed that the incidence rate of female patients was high because we used the UA cut-off value of 6.8 mg/dl to divide patients into quartiles, regardless of sex.According to the Japanese guidelines, hyperuricemia is de- fined as UA ≥7.0 mg/dl and the target UA level is <6.0 mg/dl, which may be reasonable, because in the present study the incidence rate of events increased in male patients with UA ≥6.8 mg/dl.In this analysis, the group in which UA increased more than 1.0 mg/dl after 6 months had more events than the other group, regardless of the UA level. Hakota et al 10 reported that a 1.0 mg/dl increase in UA increased the HR of myocar-dial infarction to 1.17 in men and 1.23 in women. However, in our propensity score analysis, taking into account CAD risk factors and medications directly affecting serum UA level, no difference was observed between patients with UA change ≥1.0 mg/dl and UA change <1.0 mg/dl after 6 months. We assumed that the presence of complications and medi-cations affecting serum UA level caused cardiovascular events. Because we can only control complications, but not completely cure them, management of serum UA level by medication is important for reducing cardiovascular events.Study LimitationsThis study was observational and although confounding factors were adjusted by multivariate Cox regression analy-sis, and the results were still consistent after propensity score matching, an interventional study must be conducted to examine the effect of UA lowering treatment on cardiovas-cular disease.In conclusion, hyperuricemia is an independent predictor of cardiovascular events and all-cause mortality combined in patients with severe coronary artery stenosis.AcknowledgmentThis study was supported by the Japan Heart Foundation.References1. Klein R, Klein BE, Cornoni JC, Maready J, Cassel JC, Tyroler HA.Serum uric acid: Its relationship to coronary heart disease risk factorsand cardiovascular disease, Evans County, Georgia. Arch Intern Med 1973; 132: 401 – 410.2. Culleton BF, Larson MG, Kannel WB, Levy D. Serum uric acid and risk for cardiovascular disease and death: The Framingham heart study. Ann Intern Med 1999; 131: 7 – 13.3. Alderman MH, Cohen H, Madhavan S, Kivlighn S. Serum uric acid and cardiovascular events in successfully treated hypertensive patients. Hypertension 1999; 34: 144 – 150.4.Verdecchia P, Schillaci G, Reboldi G, Santeusanio F, Porcellati C, Brunetti P. Relation between serum uric acid and risk of cardiovascu-lar disease in essential hypertension: The PIUMA study. Hypertension 2000; 36: 1072 – 1078.5.Franse LV, Pahor M, Bari MD, Shorr RI, Wan JY, Somes GW, et al. Serum uric acid, diuretic treatment and risk of cardiovascular events in the systolic hypertension in the elderly program (SHEP). J Hyper-tens 2000; 18: 1149 – 1154.6.Wang J, Staessen JA, Fagard RH, Birkenhäger WH, Gong L, Liu L. Prognostic significance of serum creatinine and uric acid in older Chinese patients with isolated systolic hypertension. Hypertension 2001; 37: 1069 – 1074.7. Tseng CH. Sex difference in the distribution of atherosclerotic risk factors and their association with peripheral arterial disease in Taiwanese type 2 diabetic patients. Circ J 2007; 71: 1131 – 1136.8. Song SH, Kwak IS, Kim YJ, Kim SJ, Lee SB, Lee DW, et al. Can γ-glutamyltransferase be an additional marker of arterial stiffness. Circ J 2007; 71: 1715 – 1720.9. Tomita M, Mizuno S, Yamanaka H, Hosoda Y, Sakuma K, Matuoka Y, et al. Does hyperuricemia affect mortality? A prospective cohort study of Japanese male workers. J Epidemiol 2000; 10: 403 – 409.10.Hakoda M, Masunari N, Yamada M, Fujiwara S, Suzuki G, Kodama K, et al. Serum uric acid concentration as a risk factor for cardiovas-cular mortality: A long term cohort study of atomic bomb survivors. J Rheumatol 2005; 32: 906 – 912.11.Japanese Coronary Artery Disease (JCAD) Study Investigators. Current status of the background of patients with coronary artery disease in Japan: The Japanese coronary artery disease study. Circ J 2006; 70: 1256 – 1262.12. Kohro T, Hayashi D, Okada Y, Yamazaki T, Nagai R, JCAD Investi-gators. Effects of medication on cardiovascular events in the Japanese coronary artery disease (JCAD) study. Circ J 2007; 71: 1835 – 1840.13. Fang J, Alderman MH. Serum uric acid and cardiovascular mortality: The NHANES epidemiologic follow-up study. JAMA 2000; 283: 2404 – 2410.14.Bickel C, Rupprecht HJ, Blankenberg S, Rippin G, Hafner G,Daunhauer A, et al. Serum uric acid as an independent predictor of mortality in patients with angiographically proven coronary artery disease. Am J Cardiol 2002; 89: 12 – 17.15.Strasak A, Ruttmann E, Brant L, Kelleher C, Klenk J, Concin H, et al. Serum uric acid and risk of cardiovascular mortality: A prospective long-term study of 83683 Austrian men. Clin Chem 2008; 54: 273 – 284.16. Kanellis J, Kang DH. Uric acid as a mediator of endothelial dysfunc-tion, inflammation, and vascular disease. Semin Nephrol 2005; 25: 39 – 42.17.Sakai H, Tsutamoto T, Tsutsui T, Tanaka T, Ishikawa C, Horie M. Serum level of uric acid, partly secreted from the failing heart, is a prognostic marker in patients with congestive heart failure. Circ J 2006; 70: 1006 – 1011.18. Wannamethee SG, Shaper AG, Whincup PH. Serum urate and the risk of major coronary hear disease events. Heart 1997; 78: 147 – 153.19.Moriarity JT, Folsom AR, Iribarren C, Javier Nieto F, Rosamond WD. Serum uric acid and risk of coronary heart disease: Atheroscle-rosis risk in communities (ARIC) study. Ann Epidemiol 2000; 10: 136 – 143.20.Suarna C, Dean RT, May J, Stocker R. Human atherosclerotic plaque contains both oxidized lipids and relatively large amounts of alpha-tocopherol and ascorbate. Arterioscler Thromb Vasc Biol 1995; 15: 1616 – 1624.21.Visy JM, Le Coa P, Chadefaux B, Fressinaud C, Woimant F, Marquiet J, et al. Homocystinuria due to 5, 10-methylenetetrahydofolate reduc-tase deficiency revealed by stroke in adult siblings. Neurology 1991; 41: 1313 – 1315.22.Strasak AM, Kelleher CC, Brant LJ, Rapp K, Ruttmann E, Concin H, et al. Serum uric acid is an independent predictor for all major forms of cardiovascular death in 28,613 elderly women: A prospective 21-year follow-up study. Int J Cardiol 2008; 125: 232 – 239.。