(完整word版)出院病历质控记录
- 格式:doc
- 大小:13.02 KB
- 文档页数:1
病历质量环节质控方法及质控点一、病历质控环节根据医疗质量检查流程和可行性,把病历质控环节分解为3级。
一级环节:病历质量监控分为病案首页、住院志、病程记录、医嘱和医嘱单,重点检查有无严重缺项。
二级环节:1、病案首页:主要分为病人一般情况,门(急)诊诊断,入院时情况,入院诊断,入院确诊日期,出院诊断,医院感染名称,病理诊断,损伤、中毒原因,诊疗效果转归、诊断符合情况,抢救及抢救成功标准,住院诊断治疗、手术各诊断符合性等。
2、住院志:书写形式(入院记录、再次或多次入院记录、24小时内入院记录、24小时内入院死亡记录)分为主诉、现病史、既往史、个人史及婚育史(月经及婚姻史)、家庭史、体格检查、辅助检查、诊疗计划、诊断等。
3、病程记录:分为首次病程记录、日常病程记录、上级医师查房记录、疑难病例讨论记录、交(接)班记录、转科记录、阶段小结、抢救记录、会诊记录、术前小结、术前讨论记录、麻醉记录、手术记录、手术护理记录、术后首次病情记录、出院记录(小结)、死亡记录、死亡病例讨论记录等,其他记录包括手术同意书、麻醉同意书、特殊检查(治疗)同意书等。
三级环节:将二级分解内容再次细化,如主诉中迫使病人就诊的主要诊断及时间描述的准确性,词语使用是否恰当,现病史中与本次疾病有关的主要诱因,起病情况,伴随症状,有鉴别意义的症状及体征描述等,三级分解是在二级基础上进一步细化,直至直接记录,主要看能否体现出病历内涵质量及医疗水平。
制定检查表格:根据质量控制办公室发现日常检查存在的主要隐患,如核心制度落实情况不力,针对性制定三级医师查房制度检查表、手术患者病历检查表、危重疑难病历管理检查表,每次查房针对一个问题进行检查,计算达标率。
二、质控方法1、重点对象:新入院病人、病危及疑难重症病人、手术病人、急症病人、特殊治疗病人。
2、重点岗位:门诊人流术、产科、新生儿科、ICU、骨科、麻醉科等。
3、重点环节:(1)时限控制点,针对整个医疗过程中诊断医疗质量关键要素,采用能够体现医疗时效性指标进行控制。
医疗质控记录范文模板第1篇1、分级管理及考核:(1)、各级医疗质量管理组织定期检查考核,对医疗、护理、医技、药品、病案、医院感染管理等的质量进行监督检查、考核、评价,提出改进意见及措施。
(2)、职能部门药定期下科室进行质量检查,重点检查医疗卫生法律、法规和规章制度执行情况,上级医师查房指导能力,住院医师“三基”能力和“三严”作风。
(3)、分管院长应组织职能部门和相关科室负责人,进行节假日前检查,突击性检查及夜查房,督促检查质量管理工作。
(4)、院医疗质量检查小组要定期和不定期组织科室交叉检查、考核。
(5)各科室医疗质控小组应每月对本科室医疗质量工作进行自查、总结、上报。
2、职能部门及各临床、医技、药剂科室、质控小组要制定切实可行的质量管理措施及评价方法。
要建立健全各种医疗质量记录及登记。
对各种质量指标做好登记、收集、统计,定期分析评价。
3、建立质量管理效果评价及双向反馈机制。
(1)、科室医疗质控小组每月自查自评,认真分析讨论,确定应改进的事项及重点,制定改进措施,并每月有医疗质控办上报业务工作月报表和科室当月的质控工作总结。
(2)、医疗质量管理委员会定期向临床医技等科室下发医疗质量管理评价表,进行交叉评价,经职能部门汇总分析,在临床、医技等科室主任联系会上通报。
(3)、医务科、护理部、质控办、信息科、院感办等职能部门应将检查考核结果、医疗质量指标等,分析后提出整改意见,及时向临床、医技等科室质控小组反溃科室质控小组应根据整改建议制定整改措施,并上报相关职能部门。
(4)、医疗质量管理委员会应定期召开全体会议,评价质量管理措施及效果分析,讨论存在的问题,交流质量管理经验,讨论、制定整改计划及措施。
医疗质控记录范文模板第2篇质控小组活动记录外科质控小组职责一、外科科质控小组组成。
组长;副组长;成员二、科室是医疗质量管理体系的重要组成部分,科主任是科室医疗质量的第一责任者。
三、结合本专业特点及发展趋势,制定及修订本科室疾病诊疗常规、药物使用规范并组织实施,责任落实到个人,与评优评先挂钩。
科室每月病历质控记录范文模板英文回答:Monthly Medical Record Quality Control Report Template for Department.Introduction:The monthly medical record quality control report is an essential document for monitoring and evaluating thequality of medical records in our department. It helps identify any deficiencies or areas of improvement in documentation, ensuring that patient information is accurately recorded and maintained. This template aims to provide a structured format for recording and reporting the results of the quality control process.Section 1: General Information.Department Name: [Insert department name]Month and Year: [Insert month and year of the report]Section 2: Data Collection.Total number of medical records reviewed: [Insert total number of medical records reviewed]Methodology: [Briefly describe the methodology used for data collection, such as random sampling or reviewing all records]Section 3: Findings.Overall Compliance Rate: [Insert percentage of medical records found to be compliant with documentation standards]Key Findings:Incomplete or missing patient demographics: [Provide specific details and percentage of records affected]Inadequate documentation of medical history: [Provide specific details and percentage of records affected]Lack of proper documentation of treatment plans: [Provide specific details and percentage of records affected]Inaccurate or incomplete medication records: [Provide specific details and percentage of records affected]Other significant findings: [Provide any other significant findings and their impact on patient care]Section 4: Recommendations.Based on the findings, the following recommendations are proposed to improve the quality of medical records:1. Implement regular training sessions on proper documentation practices for healthcare providers.2. Develop standardized templates for documentingpatient demographics, medical history, treatment plans, and medication records.3. Strengthen the use of electronic health records to ensure accurate and complete documentation.4. Establish a system for regular internal audits to monitor compliance with documentation standards.5. Encourage open communication and feedback among healthcare providers to address any documentation-related concerns.Section 5: Action Plan.An action plan will be developed based on the recommendations and will include specific timelines, responsible individuals, and measurable outcomes.Section 6: Follow-up.A follow-up report will be prepared in the next monthlyquality control review, highlighting the progress made in implementing the action plan and any further recommendations.Conclusion:The monthly medical record quality control report is a vital tool for ensuring the accuracy and completeness of patient documentation in our department. By identifying areas of improvement and implementing appropriate measures, we can enhance the quality of medical records andultimately improve patient care.中文回答:科室每月病历质控记录范文模板。
word格式病例,出院记录(含五篇)第一篇:word 格式病例,出院记录***人民医院出院记录姓名:性别:年龄科室:病室:床位:住院号:住院天入院日期:2013 年 06 月日出院日期:2013 年 06 月日入院情况(简要病史、体格检查及主要辅助检查):患者,48 岁,女性,已婚。
因“外伤致左手背部及右膝关节疼痛一天”入院。
患者于昨日下午下雨时坐车回家路上不慎跌倒,致左手背部疼痛流血,右膝关节疼痛难忍;立即于当地诊所清创缝合止血包扎后,自行回家,今日感疼痛加重,前来我院门诊就诊,并行左手 X 线检查示:未见异常。
自受伤至今左手肿胀明显,无明显呕吐,精神,饮食,睡眠欠佳,查体:T:37.0℃ P:80 次/分 R:20 次/分BP:130/80mmHg。
神志清楚,精神差,头颅、五官端正,眼结膜无充血、水肿,巩膜无黄染,双侧瞳孔等大等圆;双肺呼吸音能清晰,心前区无隆起,腹平坦,无压痛,无反跳痛。
专科情况:换药可见左手掌及掌背侧肿胀明显,两处皮肤裂口以缝合共俩针,局部无渗出,明显触压痛,右膝关节下方胫骨平台处皮肤挫裂伤,局部少许液性分泌物。
辅助检查:左手 X 线检查无异常。
入院诊断:诊疗经过(包括手术日期和手术名称):患者入院后给予进一步完善相关检查,抗炎对症支持治疗,今日好转,患者要求出院出院。
出院诊断:出院情况:患者诉无不适。
精神差、饮食不佳、睡眠差,大小便正常。
查体:T:36.6℃ 120/68 mmHg.神志清楚,双肺呼吸音清,心音清,左侧腰部压痛,叩击痛。
BP出院医嘱:1、2、1、注意休息,按时服药。
2、不适随诊。
上级医师签名: 2013 年 06 月日住院医师签名: 2013 年 06 月日第二篇:儿科病例出院小结新生儿出院记录X线片号: MRI/CT号:~~,女,24/30月出生于2013年第1胎第1产,胎龄39周在某医院剖宫产,出生体重3.7kg,出生时无宫内窘迫,羊水较多,无胎膜早破,脐带正常,胎盘正,Apgar评分:1min9分,5min10分、10min 10分。
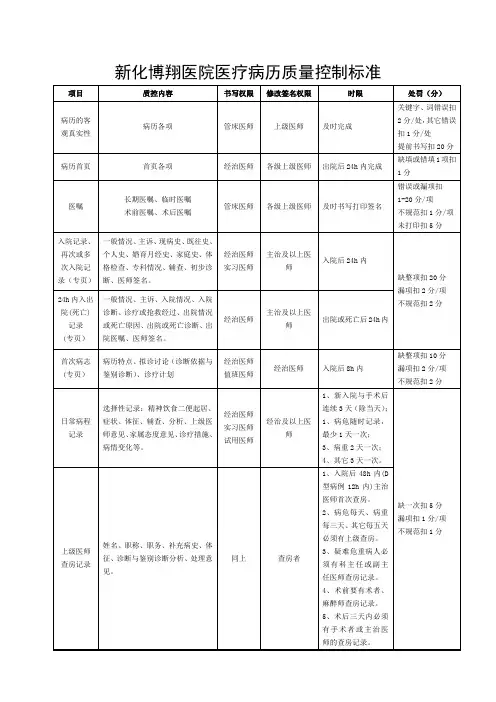
出院病历质量检查质控标准出院病历质量检查质控标准十、出院病历质量检查质控标准项目编号项目分值基本要求内容编号缺陷内容扣分标准01病案首页:10分准确填写首页各项,不能有空项01首项医疗信息未填写502传染病漏报503缺科主任或副主任医师以上人员签名304缺主治医师签名205缺住院医师签名206门(急)诊诊断未填写107入院诊断未填写208入院诊断填写有缺陷0.5/项09出院诊断未填写210出院诊断填写有缺陷0.5/项11院内感染栏未填写212手术操作名称未填写213手术操作名称填写有缺陷0.5/项14有病理报告,病理诊断未填写115病理诊断填写有缺陷0.516药物过敏栏空白或填写错误217除单列项目外的某项未填写或填写有缺陷0.2/项02入院记录:20分1、在24小时内由住院医师完成2、一般项目填写齐全3、主诉体现症状+部位+时间;能导出第一诊断4、现病史必须与主诉相关、相符;能反映本次疾病起始、演变、诊疗过程;要求重点突出、层次分明、概念明确、运用术语准确;有鉴别诊断资料5、既往史、个人史、月经生育史、家庭史齐全6、体格检查项目齐全;要求全面系统地进行记录7、有专科或重点检查01缺入院记录(实习医师代写,无住院医师修改签字视为缺入院记录)1002未在患者入院24小时内完成入院记录503未按规定书写再次或多次入院记录104患者一般项目填写不全0.2/项05缺主诉506主诉描述有缺陷207缺现病史508主诉与现病史不符209现病史发病原因描述不清110现病史主要疾病发展变化过程描述不清211缺与本次入院有关的重要阴性症状记录212发病后诊治情况记述不清113症状描述不全(如疼痛五要素)114缺既往史215既往史中有重要缺陷116缺个人史217个人史中与主要诊断相关的内容有重要缺陷118缺婚育史119缺家族史220家族史中与主要诊断相关的内容有重要缺陷121缺体格检查522体格检查遗漏主要阳性体征323体格检查缺有鉴别意义的阴性体征224体格检查顺序颠倒125体格检查记录有缺陷126表格病历体格检查记录的漏项0.5/项27需写专科情况的病历缺专科情况328专科情况记录的缺陷129辅助检查缺项230缺初步诊断531初步诊断书写有缺陷1/项32缺住院医师签名303病程记录:40分1、首次病程记录在病人入院8小时内完成,内容包括病例特点、初步诊断、疹断依据及鉴别诊断、诊疗计划四个部分2、日常病程记录要求:病危患者每天至少记一次;病重患者至少二天记一次;病情稳定患者至少三天记一次。