全国医药客户资料(2015)
- 格式:xls
- 大小:74.50 KB
- 文档页数:14
最新医药市场调研报告范文3篇如何做好医院市场,在一定程度上决定了医药营销的成败,同时也是医药营销的主要内容.下面就是小编给大家带来的医药市场调研报告范文3篇,希望大家喜欢!医药市场调研报告范文一专家指出,中国医药市场远未饱和,但竞争业已开始.目前,中国每年人均医疗消费水平只是美国人的1/130,当一般发达国家年人均医疗卫生消费支出达到2015美元、美国人均突破4000美元的时候,中国年人均医疗卫生消费支出只有31美元.但在另一方面,国内医疗用品的销售量持续增加,在今后3~5年的时间里每年将以12%的速度增长.2015年的中国医药,面对的将是一个蓬勃发展和惨烈竞争共存的局面.这是值得每一个医药人认真思考的问题.医院市场分析如何做好医院市场,在一定程度上决定了医药营销的成败,同时也是医药营销的主要内容.我在实践中摸索到推销药品的窍门,那就是必须打点好一些关键人物 .第一是医生,他们手里有处方权,用哪种药,用多少,全由他们说了算;第二是医院的库房,从医药公司进药全由他们负责:第三是药房,他们有一个小账本 ,每个医生用了多少药,该得多少提成,全是由他们提供给我的;第四是医药公司,医院从他们那里进药,我凭药款拿提成医药行业市场调研报告范文.打点这些人的方法也简单,不过是根据各人的重要性给予不同档次的提成.有些人难打发,那么就给他多送点礼,多请他吃几次饭.推销同一种药品的医药代表是竞争对手,常常互相刺探军情 ,如果哪家公司给医生的提成高,另一家公司的医药代表就会向上汇报,要求提高给医生的提成.OTC市场或社区医药市场分析OTC市场或社区医药市场的开发,已经成为了现代医药营销的一个新的经济增长点.社区治疗的疾病,购买感冒药的比例在所有购买的药品类别中居首位,其次为咳嗽、咽喉疼痛、发烧及心血管病等疾病随着OTC市场和社区医疗市场的逐渐壮大,使得广告、店员成为影响消费者购药的主要因素,店员的作用仅次于电视广告.医药代表工作的总体思路由于医药代表工作对象的特殊性,决定了医药代表的专业知识水平及个人素质都比普通推销员要求更高.善于运用推销之术,对医药代表工作的顺利开展有着至关重要的作用.学会自我推介,赢得客户真诚、友好的合作.良好的自我推介,是让对方接纳你和你的产品的首要条件.要保持充沛的精神与活力,以整洁得体的仪容,彬彬有礼而不卑恭的形象面对自己的客户,并不断塑造自身良好的气质与稳健的风度;其次,培养真诚、友善、豁达、乐观的生活态度,磨炼自己的意志;再次,树立不断学习的思想,努力涉足包括医药专业在内的各种知识,不断提高自己的知识含量与专业化水准.实事求是展示企业形象,增加客户的信任度医药代表的工作不是独立的,而是企业整合营销的有机组成部分.企业与品牌在医生心目中形象的好与坏,很大程度上决定于产品的使用程度.医药代表在充分推介产品的同时,实际上也在从另一个角度推介企业.必须全方位深入了解自己的企业,充分理解企业的经营理念、经营原则与价值取向;其次,认真分析、提炼、归纳企业的优势,同时不回避劣势,正确对待企业的不足;再次,认清自己的工作目标,了解企业对员工的期望,充分利用企业所能提供的支持与帮助;最后,对企业充满信心,时刻觉得自己的企业是最棒的.只有对自己的企业充满信心,才能通过你的言行由衷地感染对方.利用新产品的全新概念感染客户.医药代表推销的药品一般是新药,另有部分是新剂型或老药新用,围绕这些具有学术理论及新概念的产品,完整准确地推介是让医生接纳产品的关键.介绍新品种的功效理论、研发背景以及该药与相关药品的临床发展历史;其次,恰当介绍新药品在临床应用中的效果和在实际应用中的具体情况.只有熟练掌握新药品的功效和临床知识,才能从各方面回答医生可能的提问.医药代表必须将扎实的医药基础知识充分应用于药品的推广活动之中.结束语根据以上调研分析,在完成了药品招标工作后,关键是对医院和医药公司进行业务公关,尤其是对医院的重点公关,力争在最大程度上赢得药品订购合同,以最终实现公司的经济效益和社会效益.在与他们打交道的时候,必须树立从药品订单的收集、药品运输的执行、公共关系的维护以及货款回笼的监控的全程服务的意识,兢兢业业地做好公司的药品销售工作.现代医药销售的实践告诉我们,只有切实地把医院的临床用药需求和疾病治疗的发展趋势掌握好,才能有针对性地开展医药代表的实际工作.具体的说,就是通过医药代表的努力,使医生完成从尝试用药、保守用药、二线用药一直到首选用药这样一个认知和用药过程.总之,每一个医药代表在具体的医药销售中,不仅要做好药品的销售,而且还要加强学习医药知识,并且用后者来指导自己的药品销售,努力改变过去那种光卖不管的被动文工作报告.医药市场调研报告范文二药品分类管理是国际上普遍认可与采用的管理模式.世界上第一个创建药品分类管理制度的国家是美国,这是由于当时(20世纪30-40年代)发生了几起严重的药害事件,使其必须加强对药品安全性和有效性的管理,通过立法,严格划分处方药与非处方药,至50年代建立起分类管理制度.50年代以后主要发达国家都相继建立了这一制度.目前,多数发展中国家与地区,包括我国,东南亚国家以及香港、台湾地区都建立了这一制度,东欧国家也在近几年逐步推行这一制度.我国在20**年启动药品分类管理工作,之后全面展开.为促进做好处方药与非处方药分类管理实施工作,国家局于20**-20**年连续发布了《实施处方药与非处方药分类管理20**-20**年工作计划》和《关于做好处方药与非处方药分类管理实施工作的通知》,同时,于近期先后召开了两次药品分类工作会议,国家实施药品分类管理的决心可见一斑.推进药品分类管理有利于保障人民用药安全,处方药的严格使用,可以减少滥用带来的许多不良反应和机体耐受性及耐受性带来的治疗困难,非处方药的合理使用,能够增强人们的自我保健、自我药疗意识,促进我国人人享受初级卫生保健目标的实现;有利于医药卫生事业健康发展,推动医药卫生制度改革;有利于逐步与国际上通行的药品管理模式接轨,有利于国际间合理用药的学术交流,提高用药水平.推进药品分类管理势在必行一、我市流通领域药品分类的现状和问题**市局一直把药品分类作为全局工作的重点,通过几年来的规范管理,全市药品流通领域药品分类逐渐完成阶段性目标,实现了三个转变.1、药品陈列转变100%的药品经营企业的药品陈列由原来的混放转变为如今的把药品与非药品、处方药与非处方药、内服与外用、功效或剂型相同进行分开摆放的方式,各摆放区都配有相应的标识.2、药品的销售转变现在的药品经营者把药品的销售分为两大部分:非处方药销售和处方药销售.处方药的销售经历了直售式、询售式、凭售式三个阶段的转变,同时非处方药销售也随着由利润驱动到信誉驱动的观念变化向疗效合理性转变.3、药品的咨用转变药品经营企业的用药咨询的变化较快,由原来的50%药店只配有一名兼职药士到现在100%的药店都配备了专职的药师、从业药师、执业药师作为驻店药师,药品零售企业的审核处方、指导合理用药的工作有的长足进展.通过对市区百余家的药品零售企业的现场调查,我们发现药品分类工作面临的问题也比较多,概括为三个不能.1、驻店药师不能保证始终在岗调查的120家药店,12%驻店药师长期不在岗;40%的驻店药师由于各种原因离岗;36家药店未挂停售处方药的标志;29家药店药师不在岗继续销售处方药.2、处方药不能完全凭医师处方销售在40%的驻店药师在岗的药品经营企业中,有近三成未能尽到审核处方的职责,形同虚设,有的不看处方,只盖章;有的只指导,不审核;甚者不闻不问.3、分类摆放不能做到完全分开60%的被调查的药店处方药与非处方药分类未能完全分开,个别药品混放,具体表现在没有标识的非处方药混放在处方药区;处方药存放不集中,与非处方药交叉存放;个别非药品混放于药品中.二、我市药品流通领域药品分类的问题分析对于以上存在的问题,我们分别从处方来源、人员素质、顾客心态、监管措施等几个方面做以调查和分析.(一)处方来源缺乏从处方方式的调查情况看,许多医院运用计算机网络管理,患者挂号时先买卡,医生在计算机上开处方,患者拿着卡去交款、取药,根本看不到处方.有的医院没有条件上电脑,居然给药品编号,医生开处方不写药名写编号.小规模的诊所普遍采取先扎针、后开方的做法,有的甚至扎完针也不开方.医院大多是公立性的,药品收入是医院的主营收入,所以医院不愿意让处方流向社会药店.据卫生部不完全统计,20**年全国医疗卫生机构的总收入达4000多亿元,其中42%是药品收入,利润至少达500亿元,而商业流通领域利润率只有0.5%~0.7%.虽然药品收入所中比例已出现逐年递减的状况,但医疗机构和药店之间药品价格差距还很大,因此,医疗机构控制处方外流的原因不言自明.(二)消费人群意识淡薄广大消费者对凭处方销售处方药不理解、不习惯.在调查时遇到一位正在药店购药的老者,他说,注射一个疗程的精制刺五加,在药店买,到社区诊所注射,300元钱就够了;如果到医院注射一个疗程,800元也下不来,药价低而且质量也不差.但当药店向他索要医生处方时,他不但不给,还拄着棍子大发脾气.消费者对药品分类管理的意义不懂,产生抵触情绪,客观上也促使药店顺水推舟违法销售处方药.尽管目前中国医药行业发展很快,但是中国人口基数大,现有的发展水平根本不能完全满足人们的就医和用药需求.在不少医院尤其是医疗水平很高的医院,人满为患、医生服务不到位、病人折腾半天依然看不上病,买不上药的现象并不少见.所以,很多病人只要不是大病,一般不愿去医院就医,而却愿意选择就近的药店购药.消费者已经习惯到药店买药不凭处方的方式,如果凭借处方意味着还得走医院程序.此外,广大消费人群对处方药滥用的危害性还没有深刻的认识,头痛脑热,就吃抗菌素、打点滴的情况已成自然,殊不知药品的不良反应、习惯性的耐药可能危及生命.(三)某些医疗机构责任差据有关资料报道,我国抗菌药物的消费85%发生在医疗机构,住院患者中抗菌药物使用率已高达80%,其中使用广谱抗菌药和联合使用两种以上抗菌药就占58%,远远高于30%的国际水平.目前,滥用抗菌药物现象表现在以下几个方面:一是联合应用抗菌药不当引起或加重不良反应;二是有不少医生给患者看病不做药敏试验,光凭经验就使用抗菌药;三是少数医生受利益驱动,不顾病情需要,大量使用价贵、先进的抗菌药;四是有的医生缺乏专业知识,不管需不需要使用抗菌药.在医生开出的抗生素中,不合理的处方就占四至五成左右.滥用抗菌药物,不仅给病人增添了额外的经济负担,浪费了有限的医疗资源,更严重的是加快了人体内耐药菌的产生,给临床治疗带来了困难;医生习惯性应用则会因势利导,患者则把应用抗菌素当成必要.(四)药品咨用人员素质差许多药店在人员责质、管理制度、设备设施等软硬件建设上还不能适应药品分类管理的要求.特别是在人员素质方面,差距更大.实施药品分类管理要求药店配备驻店执业药师.我国的执业药师数量本来严重不足,还多数在管理岗位上,不可能担任驻店执业药师.即使配备驻店药师,人数也不能满足要求.更重要的是,相当一部分药师对药品知识的熟悉程度和审方能力尚未达到驻店药师的要求.(五)规范措施不尽完善现行的处方药与非处方药分类摆放原则是偏重把非处方要单独存放,即OTC标识的药品标志清晰、分柜摆放.这样摆放给消费者的印象好象是非处方药作为一种需要特别管理的药品,而不是处方药,相反,无标识的处方药和暂无标识的非处方较难分开.因此,可以想到我们规范管理过程的许多亟待完善各项工作.例如:如何鉴别处方的真伪的管理方法等.三、我市药品流通领域药品分类的解决措施1、加强药品零售企业处方审核人员驻店注册、培训管理工作,充分发挥药学技术人员用药指导作用加强药师的队伍建设.为解决执业药师数量不足的矛盾,药监部门要采取有效方式,在保证人员素质的前提下,促进扩大了执业药师的数量,同时为弥补执业药师数量不足,加强对从业药师的再教育工作.要积极促进本地区从业人员的素质建设,从政策上鼓励从药人员进行再教育,从措施上完善从药人员的再培训.提高人员数量和质量,确保指导用药水平得到提高,满足本地区需求.加强药师的在岗情况的检查.一是严把审查关.对新开办药品零售企业进行现场检查验收时,对药师的资格、实际水平、是否兼职、外地人员能否保证在药店行使职责等进行严格把关.二是实行值班药师签到制.要求企业提前做好值班药师的工作安排,药师上班必须签到,保证药师在职在岗,充分履行对顾客购药咨询、用药指导、处方审核、质量把关等工作职责.三是要求挂牌明示.药师在营业时间上岗时,应佩带标明其姓名、技术职称、岗位等内容的胸卡,便于群众监督.如药师临时不在岗,应在凭处方销售药品专柜明显处,摆放药师不在岗暂停处方药销售的告示牌.四是开展药师在岗专项检查.加强对药师在职在岗监督检查,对连续多次检查发现药师不在职在岗的,将依照《药品管理法》第七十九条进行处罚.2、积极开展药品分类的宣传工作,引导广大群众改变用药习惯和正确使用药品首先,要通过科学的宣传教育,逐步增加公众合理用药知识,改变公众传统的用药习惯.要通过对加快推进药品分类管理的重要性和迫切性的宣传,让公众了解有关药品分类管理的相关政策性规定以及药品分类管理阶段性目标的主要内容,从思想上意识到药物滥用的危害.同时,还要加大对一些常见病的基本判断常识和推荐用药范围、常用非处方药的适应证等知识的宣传,采用媒体宣传与印发资料等多种宣传方式,着力解决公众在使用非处方药进行自我诊疗时所面临的合理用药知识缺陷,增加公众的自我保护意识,使其养成合理用药的习惯.其次,要通过积极有效的宣传,引导药品零售企业积极开展药学服务.零售药店及其从业人员是执行药品分类管理的最终端环节,只有把握住终端出口,药品分类管理的阶段性目标才有可能实现.因而药品监管部门要通过广泛宣传,让药品零售企业正确处理经济效益和社会效益的关系,通过高质量的药学服务,促进企业的发展,认真执行分类管理的相关要求与规定.第三,在宣传手段上应注重贴近性和多样性.通过手机短信向社会广作宣传;与媒体联动,将为群众解决问题的过程、结果公之于众,都起到了较好的宣传效果.要不拘形式,避免单一的灌输式教育.公众合理用药意识的养成不是一朝一夕的事,分类管理的宣传也不能停留在一阵风的阶段,而应探索长效的、持久的、深度的宣传方式和手段,并充分发挥相关协会、学会在推进药品分类管理方面的宣传、培训和正面推动作用.3、大力加强药品分类管理的监管和规范工作,积极稳妥促进药品分类对药店的监管.一是加强药品零售企业处方药与非处方药分柜摆放情况和专有标识规范情况的检查,积极促进药品零售企业达到药品分类管理的要求.二是加强驻店执业药师配备及在岗情况,以及处方审核制度落实情况的检查.结合GSp 认证工作,进一步完善驻店执业药师配备制度和处方审核制度.三是对已明确药品零售企业不得经营的药品,要加强监督检查.对违规经营的,按《药品管理法》、《药品管理法实施条例》等有关法律法规的规定进行处理.四是对已明确必须凭处方销售的药品,要加强对药品零售企业执行凭处方销售规定情况的检查.对药品零售企业违规销售处方药的行为,要及时予以纠正,并根据《药品流通监督管理办法》给予警告处罚;情节严重或经警告后仍违规销售的,除给予警告外,还应并处罚款.五是各级药品监管部门要结合医疗和药品广告整顿工作,加强对处方药和非处方药广告的监督和检查,特别要加大处方药在大众媒体违规发布广告和非处方药在大众媒体扩大宣传的检查力度.六是把药品分类管理工作的要求与零售药店的审批、变更、认证及监督检查有机结合,对达不到分类管理要求的,按照有关规定处理.对医疗机构的监管.加强抗菌药物监管,促进合理用药是一个系统工程,需要药监、卫生、工商等部门的共同监管,药品监督管理部门在推进合理用药的进程中应发挥主导作用.制止滥用抗菌药的关键是从源头抓,用制度来规范.相关部门应制定一个明确的制度,规范医生的处方行为.首先,抓医生的职业道德教育和业务技能培训;其次,医院药剂师可以参与临床医生查房,指导临床用药;三是建立健全规范用药、合理用药制度;四是真正发挥药品招标采购的作用,纠正从使用药品中获取利益的行为.四、我市药品流通领域药品分类的初步设想1、推进自我药疗计划,有步骤的引导群众习惯性使用非处方药品顾名思义,自我保健、自我药疗是在没有医生或其他医务工作者指导的情况下,恰当地使用非处方药物,用以缓解轻度的、短期的症状及不适,或者用以治疗轻微的疾病.由此可见,自我药疗是自我保健的一项重要内容.自我保健和自我药疗古已有之,几千年来,我国人民在与疾病作斗争中积累了丰富的经验,随着经济、文化、卫生事业的飞速发展,世界卫生组织(WHO)在**年提出到20**年人人享有卫生保健的宏伟目标.结合国情,我国政府提出了到20**年基本实现人人享有初级卫生保健.与此同时,WHO还提出人们有权利也有责任以个体和集体的方式参与他们的卫生保健的计划和实施.我国政府也提出做好卫生保健工作应以国家、集体为主,其他社会力量和个人为补充.由上可知,现代卫生保健的概念已经发生了根本改变,由过去单纯依赖国家转变为是个人的权利和责任,由被动转为主动积极参与,自我保健和自我药疗成为社会和个人共同关注的事业.非处方药的出现大大促进了自我药疗的发展,并在现实生活中有着非常重要的作用.我们应该注重对自我药疗的宣传,引导群众自觉使用非处方药,远离药物滥用,推行自我保健.2、探求解决处方来源的有效方法,促进处方的有序流动探索医疗机构药房商业化转型,实行医药分家,把门诊药房从医院剥离出来,建成独立核算的单体药店.严格执行处方药凭处方销售的要求,建立药品分类管理的试点,形成把医疗机构商业化药房作为处方药源头的模式,把分类管理经验全面推开,促进规范化建设.把发给许可证的医疗机构的药房作为完全实行分类管理的示范点,形成处方来源网,进一步解决处方来源和按处方购买药、凭处方售药还不适应的问题,推进药品经营企业的分类管理纵深发展.医药市场调研报告范文三中国是个农业大国,农村人口占到全国人口的70%.改革开放以来,农村形势发生了巨大的变化,农村经济出现了令人触目的成就.但是农村医药市场的情况却并不让人乐观. 根据国家统计局的有关资料, 今年上半城镇居民人均可支配收入3424元,比上年同期实际增长5.5%,同比增幅降低0.9个百分点;农村居民人均现金收入1063元, 实际增长4.2%,同比提高2.1个百分点 .国家统计局的统计资料还同时指出 ,上半年全国城镇居民家庭人均医疗保健消费169.2元,占全部消费性支出的6.65%,而农民人均医疗保健消费45.3元,占全部生活消费现金支出的6.82%.剔除其中的一些不可比因素,仍然可以看出,医疗消费在城乡人均消费构成中的比重差距并不大.农村居民人数基本是城镇居民人数的二倍以上,如按实际数字计算双方医药销售金额应当大致相近.但是今年上半年,由于多种因素,全国医药市场销售额723亿元,而其中农村销售额35.5亿元,仅占全国销售额的 4.9%.城乡医药市场消费差距之大,确实应该令人思索.笔者认为农民缺医少药的问题从某种角度讲还依然存在.这与快速发展的农村经济极不相适应.医。

竭诚为您提供优质文档/双击可除咽喉类药品市场调查报告篇一:咽喉类用药市场分析老品牌打造江山新品牌竞争乏力————咽喉类用药市场分析SFDA南方医药经济研究所广州时普医药信息有限公司咽喉病属常见病和多发病,分急性咽喉炎和慢性咽喉炎,慢性咽炎主要是由于急性咽炎治疗不彻底而反复发作,转为慢性。
慢性咽喉炎的患者比急性咽喉炎的患者要多,且难彻底根治,发病人群广。
1、市场增长性分析从五城市零售药店数据显示(见表1),咽喉产品市场2004年上半年比2003年上半年的市场规模增长4%,北京和上海的增长幅度较大,而其它三城市呈负增长。
咽喉产品市场较为成熟,消费者忠诚度较高,故市场空间增长幅度有限。
表1销售额对比(单位:万元)北京上海广州武汉成都2、各类别产品市场构成对慢性咽喉炎有较好疗效的中成药占据80%以上的咽喉产品市场,而化学药的成份多为西地碘、地奎氯胺、盐酸氯乙啶等,可消除症状,对急性咽喉炎患者有较好的疗效。
对于保健产品,可起到预防作用,吸引着反复发作慢性咽喉炎及注重保健的消费者。
至于食品类的咽喉产品更注重清除口腔异味、令喉部清凉舒爽,提神醒脑,对咽喉炎并无明显疗效,受到追求口感的时尚年青人的追捧。
表2:品类比较3、重点城市市场竞争格局在北京,保健品类的京都念慈菴枇杷糖由03年第5名上升到2004年第2名,其份额上长升了1.06,食品类的泰诺甘草怡喉爽也飚升至前十名。
而风靡一段时间的亿利甘草良咽片由于自身定位的不准确,导致产品诉求群体与实际消费人群出现偏差,退出前十名的竞争。
在上海,本地品牌信可舒与西瓜霜润喉片和金嗓子喉宝呈三足鼎立之局势,三大巨头的竞争较为激烈。
在广州,市场格局变化多端,特别是在三线品牌之间,本地品牌喉疾灵胶囊抢占了金嗓子喉宝的份额,上升到9.40%,而同属于广西桂林三金药业和西瓜霜润喉片和西瓜霜喷剂,在2004年上半年,喷剂型更受到消费者的欢迎;云南盘龙云海的灵丹草颗粒在03年红红火火地销售一段时间后,在2004年前十名品牌中已不见其踪迹,在产品功效同质化的今天,可见消费者对云南盘龙云海的高价策略并不受落。
【报告名称】:2010-2015年中国医药零售行业现状及发展前景报告【关键字】:医药零售药店连锁网上药店连锁药店医药零售市场前景【出版日期】:2010年5月【报告页码】:315页【图表数量】:207个【报告格式】:PDF电子版或纸介版【交付方式】:Email发送或EMS快递【中文价格】:印刷版8000元电子版8500元印刷版+电子版9100元【报告说明】: 本报告为中商情报网原创,近期我公司发现北京一些不良子公司(个人)将中商情报网的报告目录原样或改头换面后挂在其网站或一些博客网站进行宣传销售,对不明情况的客户进行欺诈(如:付款后迟迟收不到或收不全产品、收到的产品与网上公布目录明显不符等,识别报告请重点识别图表目录)。
为避免对您的市场决策带来重大损失!购买报告请直接与中商情报网市场部联系,谨防上当受骗!本报告订购后2小时内交付客户。
如目录及图表目录与内容不一样,均可全额退款。
【报告描述】:目前,我国医药行业产业链是从上游的医药制造企业生产出药品,通过各种渠道(主要包括医药商业公司、厂家直销或个体集贸市场等渠道)销售到医院、药店和乡镇卫生院等销售终端,作为最终用户的消费者主要通过这3个地方购买药品。
在我国医药零售主要是指药品以药店为渠道的销售行为。
2009年4月6日正式公布的新医改案对药品零售行业带来不小的冲击。
国家基本药物制度的实施意味着大量的基本药物目录药品的需求将转移到基础医疗单位,医药零售企业的市场份额将被挤压。
公立医院改革将打破医院药品的价格体系,使得医院药品价格将出现大幅下降,挤压零售药店的生存空间。
但是新医改中只是强调“降低基本药物采购价格”,而并不是指所有药品。
因此,中商情报网分析师建议医药零售企业可以通过调整药品销售结构,缓解新医改带来的市场竞争压力。
随着社区医院的基础设施和医疗水平的不断提升,消费者逐渐接受到社区医疗机构处理常见病症,社区医疗机构在药品销售中的地位在提升,这必然会使一部分消费者从零售药店转向社区医疗。
计算机管理系统首营企业建档操作程序1.目的:制定《计算机管理系统首营企业建档操作程序》,使采购员在计算机管理系统(以下简称“系统”)内规范首营企业资料的基础数据录入。
2.范围:适用于计算机管理系统首营企业资料的基础数据录入过程。
3.职责:质量负责人、质量管理员、采购员对本程序负责。
公司采供部各分组采购人员应当收集供货企业资料,在计算机管理系统内规范企业资料的录入。
经质量管理员审核合格后在系统中建立档案;4.内容:公司有采购职能的各分组收集到需建档的企业资料(首营企业规范填写《首营企业审批表》),在计算机管理系统内规范录入,经质量管理员审核合格后,在系统内中建立企业资料档案。
4.2质量管理员收到采购人员规范录入需建档的企业资料申请单后,登陆主管部门网站,核实资料的真实性、合法性,并在使用自己的工作用户名登陆系统,进入到“资料管理”→“客商信息”→“首营品种质量审批单”对该企业申请单进行审核;4.3系统内企业资料为基础数据,不得在数据库内直接建档;在企业信息录入时须对以下项目进行规范的填写:4.3.1客户类型:是指“生产企业”或“经营企业”;使用下拉菜单选择4.3.2客户名称:是指主管部门所颁发的证书(如营业执照、药品生产或经营许可证)上标注的企业名称;4.3.3助记码:由系统根据所建企业“企业名称”每个字汉语拼音首个字母按顺序生成。
4.3.4营业执照:《营业执照》复印件及其上一年度企业年度报告公示情况4.3.4.1营业执照号:为注册的15位数字;4.3.4.2执照效期:根据企业每年度上一年度企业年度报告在国家工商行政管理总局的“全国企业信用信息公示系统”(网址/)公示该企业年度报告的公示情况。
为每年的6月30日。
4.3.4.3注册地址:是指营业执照上“住所”栏标注的地址;4.3.4.4法人代表:是指营业执照上“法人代表人姓名”栏标注的姓名;4.3.5药品许可证:为药品生产许可证或药品经营许可证;4.3.5.1药品许可证号:为药品生产或经营许可证上编号(如川2012xxxx);4.3.5.2证照效期:为药品生产或经营许可证上有效期至(如2015年x月x 日);4.3.5.3经营方式:采用下拉菜单选择“生产销售”或“批发”;4.3.5.4仓库地址:为药品生产或经营许可证上的生产地址或经营仓库地址;4.3.5.5经营受控范围:根据药品生产许可证或经营许可证的生产或经营范围勾选对应的受控范围4.3.6GMP证书:为药品生产质量管理规范认证证书;4.3.6.1GMP证书号:为药品生产质量管理规范认证证书编号(如CNxxxxxxxx);4.3.6.2GMP证书效期:为药品生产质量管理规范认证证书有效期(如2018年x月x日);4.3.6.3生产范围:为药品生产质量管理规范认证范围(如片剂、颗粒剂、口服溶液剂等);4.3.7GSP证书:为药品经营质量管理规范认证证书;4.3.7.1GSP证书号:为药品经营质量管理规范认证证书编号(如A-SCxx-xxxx或SC**-**-201*****)4.3.7.2证书效期:为药品经营质量管理规范认证证书有效期(如2018年x 月x日)4.3.8法人委托书:为加盖有供货单位公章原印章和法定代表人印章或签名的授权书及加盖有供货单位公章原印章的销售人员身份证复印件;4.3.8.1被委托人:为供货单位销售人员;4.3.8.2身份证号码:为供货单位销售人员身份证号码(为第二代身份证);4.3.8.3签发日期:为授权书签发生效日期(如2014年1月1日);4.3.8.4委托书有效期:为授权书失效日期(如2014年12月31日);4.3.8.5特殊药品委托书有效期:4.3.8.6联系:为供货单位销售人员联系;4.3.9组织机构代码证:4.3.9.1代码证号:4.3.9.2证照效期:4.3.10账税号:4.3.10.1税号:4.3.10.2开户银行及账号:4.3.11医疗器械许可证:4.3.11.1许可证号:4.3.11.2证照效期:期限为五年;4.3.11.3范围:4.3.12医疗机构执业许可证:4.3.12.1许可证号:4.2.12.2证照效期:4.3.13食品流通许可证:4.3.13.1许可证号:4.3.13.2证照效期:期限为三年;4.3.13.3保健食品、乳制品、婴幼儿配方乳粉、预包装食品4.3.15质量保证协议有效期:一般为一年,到期将自动锁定4.3.16维护员:4.3.17终止妊娠药:是指用于终止妇女妊娠的药品;4.3.18含特殊药品复方制剂:是指含麻黄碱复方制剂、复方地芬诺酯片、复方甘草片、复方甘草口服溶液、氨酚曲马多片(胶囊)、桔梗可待因片等。
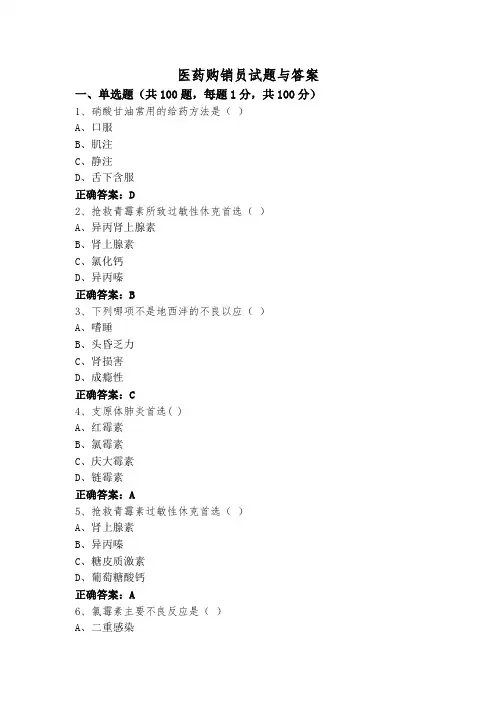
医药购销员试题与答案一、单选题(共100题,每题1分,共100分)1、硝酸甘油常用的给药方法是()A、口服B、肌注C、静注D、舌下含服正确答案:D2、抢救青霉素所致过敏性休克首选()A、异丙肾上腺素B、肾上腺素C、氯化钙D、异丙嗪正确答案:B3、下列哪项不是地西泮的不良以应()A、嗜睡B、头昏乏力C、肾损害D、成瘾性正确答案:C4、支原体肺炎首选( )A、红霉素B、氯霉素C、庆大霉素D、链霉素正确答案:A5、抢救青霉素过敏性休克首选()A、肾上腺素B、异丙嗪C、糖皮质激素D、葡萄糖酸钙正确答案:A6、氯霉素主要不良反应是()A、二重感染B、肾脏损害C、骨髓抑制D、胃肠道反应正确答案:C7、具有抗结核及超广谱抗菌作用的药物是()A、异烟肼B、利福平C、PAS-NaD、乙胺丁醇正确答案:B8、职业生活中的服务态度、礼貌行为主要依靠()来调节A、行政纪律B、领导指令C、道德规范D、法律条款正确答案:C9、药品验收时,抽样比例为( )A、每批在50件货50件以下抽取4件B、每批在50件或50件以下抽取一件C、每批在50件货50件以下抽取两件D、每批在50件货50件以下抽取3件正确答案:C10、下列何药禁用于支气管哮喘()A、普萘洛尔B、异丙肾上腺素C、氨茶碱D、肾上腺素正确答案:A11、进口药品检验报告书由()颁发A、国务院药品监督管理部门授权的口岸药品检验所B、市级药品检验所C、省级药品检验所D、国家药品检验所正确答案:A12、卡托普利降压的作用机制是()A、抑制血管紧张素转换酶B、兴奋中枢α受体C、阻断外周α受体D、阻断外周β受体正确答案:A13、下列何药过量可致高铁血红蛋白症()A、布洛芬B、乙酰水杨酸C、水杨酸钠D、对乙酰氨基酚正确答案:D14、抗药金葡菌感染应选()A、苄青霉素B、苄星青霉素C、普鲁卡因青霉素D、新青霉素II正确答案:D15、首营品种审核涉及的责任人包括企业主要责任人、质量管理人员、物价人员及()A、药品购进人员B、财务人员C、检验人员D、物流人员正确答案:A16、医药销售企业通常采用()客户档案A、数字式B、表格式C、文字式D、字符式正确答案:B17、关于注射剂的特点描述不正确的是()A、不能产生延长药效的作用B、适用于不宜口服的药物C、药效迅速疗效可靠D、适用于不能口服给药的患者正确答案:A18、糙皮病应选用()防治A、维生素DB、维生素AC、烟酸D、维生素C正确答案:C19、商品盘点前要做到“三清两符”,即票证数清,()、往来手续结清,会计记帐与柜组账相符,账簿有关单据相符。

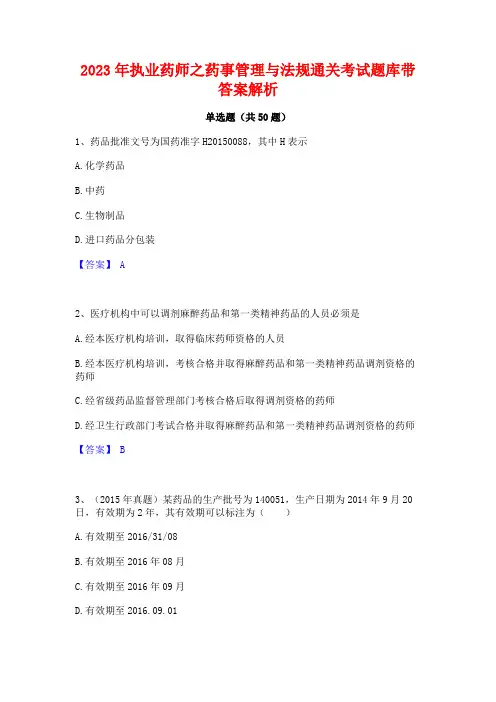
2023年执业药师之药事管理与法规通关考试题库带答案解析单选题(共50题)1、药品批准文号为国药准字H20150088,其中H表示A.化学药品B.中药C.生物制品D.进口药品分包装【答案】 A2、医疗机构中可以调剂麻醉药品和第一类精神药品的人员必须是A.经本医疗机构培训,取得临床药师资格的人员B.经本医疗机构培训,考核合格并取得麻醉药品和第一类精神药品调剂资格的药师C.经省级药品监督管理部门考核合格后取得调剂资格的药师D.经卫生行政部门考试合格并取得麻醉药品和第一类精神药品调剂资格的药师【答案】 B3、(2015年真题)某药品的生产批号为140051,生产日期为2014年9月20日,有效期为2年,其有效期可以标注为()A.有效期至2016/31/08B.有效期至2016年08月C.有效期至2016年09月D.有效期至2016.09.01【答案】 B4、全国药品召回的管理工作A.药品生产企业B.药品生产企业、药品经营企业和使用单位C.药品经营企业和使用单位D.国家药品监督管理部门【答案】 D5、药品类易制毒化学品生产企业建立的药品类易制毒化学品的专用账册保存期限是A.自药品有效期满之日起不少于5年B.自药品有效期满之日起不少于2年C.5年D.3年【答案】 B6、对药品生产企业、药品经营企业和医疗机构之间的互联网药品交易提供服务的企业进行审批的部门是A.国家药品监督管理部门B.省级药品监督管理部门C.市级药品监督管理部门D.信息产业主管部门【答案】 A7、至少配备一名主管中药师以上专业技术人员的是A.一级医院B.二级医院C.三级医院D.个体诊所【答案】 B8、下列品种可以委托生产的是A.葡萄糖氯化钠注射液B.阿奇霉素原料药C.地西泮注射液D.白蛋白注射液【答案】 A9、根据《化学药品和治疗用生物制品说明书规范细则》,使用某药品需观察过敏反应的内容应列在A.【适应证】B.【不良反应】C.【药物相互作用】D.【注意事项】【答案】 D10、(2019年真题)药品生产企业作出二级召回决定后,应当在规定时间内通知有关药品经营企业、使用单位停止销售和使用。
Technical guide for the ELABORATION OF MONOGRAPHSEuropean Pharmacopoeia7th Edition2015European Directorate for the Quality of Medicines & HealthCareEnglish version2015 Making copies of this file for commercial purposes or posting it on a websitefor which access is charged is strictly prohibited. Re-use of the file, in whole or in part, requires that the sourcebe clearly cited and the EDQM(@edqm.eu)be informed.European Directorate for the Qualityof Medicines & HealthCare (EDQM)Council of Europe7, allée KastnerCS 30026F-67081 STRASBOURGFRANCE Cover image: © EDQM - Council of Europe Director of the Publication: Dr S. KeitelPage layout: EDQMwww.edqm.eu© Council of Europe, 2015TECHNICAL GUIDE FOR THE ELABORATION OF MONOGRAPHS7th Edition – 2015TABLE OF CONTENTSI.INTRODUCTION (1)I.1.PURPOSE OF THE GUIDE (1)I.2.TEST PROCEDURES (1)I.3.EQUIPMENT (2)I.4.QUANTITIES (2)I.5.REAGENTS (4)MERCIAL NAMES (4)I.7.REFERENCE STANDARDS (4)II.MONOGRAPH ON A SUBSTANCE FOR PHARMACEUTICAL U SE (5)II.1.TITLE (5)II.2.DEFINITION (6)binations (7)II.2.2.Content (7)II.3.CHARACTERS (8)II.3.1.Appearance (8)II.3.2.Taste (9)II.3.3.Odour (9)II.3.4.Solubility (9)II.3.5.Stability factors (10)II.3.6.Hygroscopicity (10)II.3.7.Solid-state properties (10)II.3.8.Other characteristics (10)II.3.9.Behaviour in solution (11)II.4.IDENTIFICATION (11)II.4.1.General (11)II.4.2.Second Identification series (12)II.4.3.Infrared absorption spectrophotometry (13)II.4.4.Ultraviolet and visible absorption spectrophotometry (13)II.4.5.Melting point, freezing point and boiling point (14)II.4.6.Specific optical rotation (15)II.4.7.Thin-layer chromatography (15)II.4.8.Gas chromatography and liquid chromatography (16)II.4.9.Chemical reactions (16)II.5.TESTS (16)II.5.1.General (16)II.5.2.Title of tests (17)II.5.3.Solution S (18)II.5.4.Appearance of solution (19)II.5.4.1. Clarity and degree of opalescence (2.2.1.) (19)II.5.4.2. Degree of coloration (2.2.2.) (19)II.5.5.pH and Acidity or alkalinity (20)II.5.6.Optical rotation (2.2.7.) (21)II.5.7.Absorption spectrophotometry (ultraviolet and visible) (2.2.25.) (22)II.5.8.Related substances (23)II.5.8.1. Thin-layer chromatography (TLC) (2.2.27.) (27)II.5.8.2. Liquid chromatography (LC) (2.2.29.) (28)II.5.8.3. Gas-liquid chromatography (GC) (2.2.28.) (33)II.5.8.4. Capillary electrophoresis (CE) (2.2.31.) (33)II.5.9.Readily carbonisable substances (34)II.5.10.Foreign anions and/or cations (35)II.5.11.Heavy metals – Elemental Impurities (35)II.5.12.Loss on drying (2.2.32.) (36)II.5.13.Thermogravimetry (2.2.34.) (36)II.5.14.Semi-micro determination of water (2.5.12.) – (volumetric Karl Fischer) (37)II.5.15.Micro determination of water (2.5.32.) – (coulometric Karl Fischer) (37)II.5.16.Gas chromatographic determination of water (37)II.5.17.Determination of water by distillation (2.2.13.) (38)II.5.18.Sulfated ash (2.4.14.) (38)II.5.19.Residue on evaporation (38)II.5.20.Residual solvents (2.4.24.) (38)II.5.21.Bacterial endotoxins (38)II.6.ASSAY (39)II.6.1.Ultraviolet and visible spectrophotometry (2.2.25.) (40)II.6.1.1. Direct measurement (40)II.6.1.2. Measurement after a colour reaction (40)II.6.2.Volumetric analysis (40)II.6.3.Chromatography (41)II.6.4.Determination of nitrogen by sulfuric acid digestion (2.5.9.) (41)II.7.STORAGE (41)BELLING (42)II.9.IMPURITIES (42)II.10.FUNCTIONALITY-RELATED CHARACTERISTICS (43)III.ANALYTICAL VALIDATION (44)III.1.DEFINITIONS AND TERMINOLOGY (44)III.1.1.Introduction (44)III.1.2.Types of analytical procedures to be validated (44)III.1.3.Validation characteristics and requirements (45)III.1.4.Glossary (46)III.2.METHODOLOGY (47)III.2.1.Introduction (47)III.2.2.Specificity (48)III.2.2.1. Identification (48)III.2.2.2. Assays and impurity tests (49)III.2.3.Linearity (49)III.2.4.Range (50)III.2.5.Accuracy (51)III.2.5.1. Assay (51)III.2.5.2. Impurities (quantification) (51)III.2.5.3. Recommended data (51)III.2.6.Precision (51)III.2.6.1. Repeatability (52)III.2.6.2. Intermediate precision (52)III.2.6.3. Reproducibility (52)III.2.6.4. Recommended data (52)III.2.7.Detection limit (52)III.2.7.1. Based on visual evaluation (52)III.2.7.2. Based on signal-to-noise ratio (52)III.2.7.3. Based on the standard deviation of the response and the slope (53)III.2.7.4. Recommended data (53)III.2.8.Quantitation limit (53)III.2.8.1. Based on visual evaluation (53)III.2.8.2. Based on signal-to-noise ratio (53)III.2.8.3. Based on the standard deviation of the response and the slope (54)III.2.8.4. Recommended data (54)III.2.9.Robustness (54)III.2.10.System suitability testing (55)III.3.SPECIFIC APPLICATION TO METHODS USED IN THE PH. EUR. (55)III.3.1.Optical rotation (2.2.7.) (55)III.3.1.1. Introduction (55)III.3.1.2. Identification (55)III.3.1.3. Tests (55)III.3.2.Ultraviolet spectrophotometry (2.2.25.) (56)III.3.2.1. Identification (56)III.3.2.2. Limit test (56)III.3.2.3. Assay (56)III.3.3.Non-instrumental limit tests (57)III.3.3.1. Appearance of solution (2.2.1. and 2.2.2.) (57)III.3.3.2. Acidity or alkalinity (57)III.3.3.3. Limit tests for anions/cations (2.4.) (57)III.3.4.Atomic absorption spectrometry (2.2.23.) (58)III.3.4.1. Specificity (58)III.3.4.2. Calibration (58)III.3.4.3. Matrix effects (59)III.3.4.4. Detection and quantification limit (based on the standard deviation of the blank) (59)III.3.5.Separation techniques (59)III.3.5.1. Thin-layer chromatography (2.2.27.) (59)III.3.5.2. Liquid chromatography (2.2.29.) (60)III.3.5.3. Gas chromatography (2.2.28.) (62)III.3.6.Semi-micro determination of water (2.5.12.) (63)III.3.7.Volumetric titrations (2.5.11. - 2.2.19. - 2.2.20.) (64)III.3.8.Peptide identification by nuclear magnetic resonance spectrometry (2.2.64.) (66)I.INTRODUCTIONI.1.PURPOSE OF THE GUIDEThis document is a guide for the authors of monographs and also a means of communicating the principles for the elaboration of monographs to the users of the European Pharmacopoeia (Ph. Eur.), especially industry, licensing authorities and official medicines control laboratories. Since the principles applied and guidance given for the elaboration of monographs should be the same as those applied by licensing authorities, the Technical Guide may also serve as a guideline in the elaboration of specifications intended for inclusion in licensing applications.It is necessary to bear in mind that a monograph will be a mandatory standard and must be applicable in licensing procedures in all Member States of the Convention on the Elaboration of a European Pharmacopoeia.I.2.TEST PROCEDURESThe methods chosen for the identification tests, purity tests and assay(s) constituting the bulk of a pharmacopoeial monograph are preferably those already described and utilised in the Ph. Eur.. In this context, the author of a monograph is referred not only to the General Methods of the Ph. Eur.. but also to published monographs on similar materials. The above considerations aim at ensuring a reasonable degree of harmonisation within the Ph. Eur. and they only apply in cases where the methods are found to be adequate for the specific purposes. However, due attention is also to be paid to the development of new methods that offer significant improvements in terms of sensitivity, precision, accuracy or discriminating power (selectivity).Methods included in monographs must be validated as described in the chapter on analytical validation and other relevant specific chapters of this guide. Validation reports are provided to the EDQM but are not published or otherwise provided to users.The test procedures included in a monograph should be verified in 2 or more laboratories and the laboratory reports on this verification should be provided to the EDQM to ensure future traceability.The instructions describing any method of analysis cover all factors that can influence the results and that are deemed essential to enable an experienced analyst working according to acknowledged laboratory practices, yet without necessarily having any prior knowledge of the investigation in question, to perform the analysis. Variations in the description of similar methods are to be avoided.If an analytical procedure is expected to be used generally or if it requires a lengthy description and is used more than once, it may be proposed for inclusion in the general chapters of the Ph. Eur., to be referred to in the individual monographs. The methods are prescribed on the scale conventionally applied in the Ph. Eur. except in cases where for reasons of availability of the material to be analysed, or because of its toxicity or its cost, work on a small scale would be advantageous.I.3.EQUIPMENTIf the equipment utilised for a method of analysis is not generally available in the States party to the European Pharmacopoeia Convention, it must be possible to have it constructed according to its description in the Ph. Eur.I.4.QUANTITIESIn prescribing the quantities, i.e. masses and volumes, of substances, reagents, and solvents to be taken for identifications, tests and assays, it is the practice of the Ph. Eur. to indicate the accuracy with which they are to be measured (see General Notices). It is therefore necessary to take this aspect into consideration when drafting pharmacopoeial texts.As guidance to minimise errors in the preparation of analytical solutions, Table 1, giving estimations of the relative uncertainty, is to be consulted.In order to avoid either the use of extremely low amounts or an unnecessarily large expenditure of solvents, a dilution series will often have to be prescribed for the preparation of dilute solutions used particularly for spectrophotometric measurement. In this context not all combinations of (usually 2 or 3) dilution steps will contribute equally to the random error of the dilution procedure. If critical for the purpose, the optimal dilution is prescribed in consideration of the relative errors (capacity tolerance divided by nominal volume) associated with the various sizes of volumetric pipettes and volumetric flasks commonly used for these operations (taking the usual formula: square root of the sum of the squares of individual relative errors, to estimate the relative dilution error).Tables giving the optimal number and nature of dilution steps needed to achieve a given dilution ratio, based upon given specifications for the capacity tolerances of volumetric glassware, are available in the literature. For guidance see Table 2 (it is to be noted that these factors do not include reading errors).Table 1 – Relative uncertainties in the preparation of analytical solutionsConcentration to be prepared Preparation of solution Percentage relative uncertainty Mass Volume Total10 g/1000 mL 10 g/1000 mL1 g/100 mL0.5 g/50 mL0.25 g/25 mL0.1 g/10 mL< 0.010.020.040.080.020.050.120.170.230.500.050.120.170.240.541g/1000 mL1 g/1000 mL0.5 g/500 mL0.25 g/25 mL100 mg/100 mL50 mg/50 mL10 mg/10 mL0.020.040.080.20.42.00.050.070.230.120.170.500.050.080.240.230.432.060.1 g/1000 mL 100 mg/1000 mL50 mg/500 mL25 mg/250 mL10 mg/100 mL5 mg/50 mL1 mg/10 mL0.20.40.82.04.020.00.050.070.080.120.170.500.210.410.802.04.020.00.01 g/1000 mL 10 mg/1000 mL5 mg/500 mL1 mg/100 mL2.04.020.00.050.070.122.04.020.0An uncertainty of 0.2 mg for the weighing procedure has been assumed for the calculations of the percentage relative uncertainties.Table 2 – Relative errors for dilution with analytical glassware (pipettes P/flasks F)Concentration ratio No. of steps Step 1 Step 2 Relative errorP F P F1/2 1 25 50 0.161/2.5 1 20 50 0.181/5 1 20 100 0.171/10 1 25 250 0.131/12.5 1 20 250 0.161/30 1 15 500 0.201/50 1 20 1000 0.151/100 1 25 250 25 250 0.181/125 2 20 250 25 250 0.201/160 2 25 1000 25 100 0.191/200 2 25 500 25 100 0.181/250 2 20 250 25 500 0.201/400 2 25 250 25 1000 0.181/500 2 20 500 25 500 0.201/1000 2 20 1000 25 500 0.20Adapted from R.B. Lam and T.L. Isenhour, Minimizing relative error in preparation of standard solutions by judicious choice of volumetric glassware, Analytical Chemistry, 1980, 53, 1158-1161.I.5.REAGENTSWhen the quality of a reagent substance in one or more respects is critical for its intended use, it must be carefully defined, when necessary by prescribing appropriate tests to demonstrate its suitability. Normally, analytical grade reagents are employed in which case it is sufficient to give the name of the reagent, the CAS number and its formula.Whenever possible, the reagent substances, reagent solutions, volumetric solutions and standard solutions for limit tests already described in the chapter 4.Reagents of the Ph. Eur. are to be employed. Simple solutions of reagent substances or solutions that are prepared for use on a single occasion are to be described in the monograph itself.The use of reagents that are acknowledged to be extremely toxic or otherwise hazardous (e.g. carcinogenic), is to be avoided, especially in circumstances where their dangerous properties are difficult to control, e.g. when handled as fine powders or in spray reagents. The use of those substances that are prohibited or restricted in one or more of the States party to the European Pharmacopoeia Convention is also to be avoided (e.g. mercury containing reagents, REACH regulation annex XIV).MERCIAL NAMESCommercial names are given systematically as footnotes in draft monographs for chromatography columns/plates and based on usefulness for the analysts in other cases (e.g. test kits, reagents that are available from a single supplier, etc.). Commercial names are not included in the text published in the Ph. Eur. but are transferred to the EDQM Knowledge Database after adoption of the monograph.I.7.REFERENCE STANDARDSThe policy and procedures regarding reference standards are described for information in general chapter 5.12.Reference standards. Procurement, establishment, storage and monitoring of reference standards are the responsibility of the EDQM. Many reference standards, notably impurity standards, are available only in limited quantities, and the amount prescribed for preparation of solutions must be kept to a minimum. Before publication of a monograph in Pharmeuropa, the required quantities of reference standards should be supplied to the EDQM, who will advise on the best strategy for optimising the use of substances that are available in limited quantities (for example, preparation of a spiked substance rather than supply of the single impurity). The aim of the EDQM is to present the reference standards for adoption at the same time as the monograph or, failing that, by the time of publication at the very latest.For IR identification, preference is given to chemical reference substances over reference spectra, except in special cases, for example where provision of a reference substance entails practical difficulties.II.MONOGRAPH ON A SUBSTANCE FOR PHARMACEUTICAL USE Monographs are based on the specifications for substances used in medicinal products approved in Member States. When a monograph is added to the work programme, enquiries are made by the EDQM to identify manufacturers of such substances and all data received is taken into account for preparation of the monograph. Interested parties should be invited to participate in the elaboration of the monograph before publication in Pharmeuropa, since the 3-month public period will often be too short for all interested parties to check the draft monograph.Prior to the preparation of any monograph, it is essential to gather as much information as possible on the substance in question.In particular it is necessary to ascertain:•whether the substance is of natural, synthetic or semi-synthetic origin;•whether the substance is a mixture or a single entity;•the method(s) of preparation in detail;•whether there are different crystalline forms, since the properties of the substance may vary in accordance with this parameter;•whether both an enantiomer as well as the racemate or other mixtures of enantiomers are available;•whether different hydrates are available;•whether different entities (acid, base, salt, etc) are available.The Ph. Eur. and other relevant documents on the state of work must be consulted to see if monographs on similar substances exist or are being elaborated. If this is the case, it is important to ensure that similar monographs follow the same approach unless there are good reasons to deviate, e.g. developments in analytical techniques.When a substance exists both in a water-free form and in the form of (a) hydrate(s) with different water contents, and if all these forms are used, they are normally treated as individual substances requiring separate monographs. The same rule applies for other solvates.Substances that are to be described in a monograph may be members of a group of very similar substances (family). This holds true especially for excipients such as macrogols. A master monograph (family monograph) is to be drafted clearly stating the attributes common to all members of the family and that can be used to identify single members of the family.All active substances and excipients described in the Ph. Eur. are subject to the provisions of the general monograph Substances for pharmaceutical use (2034).II.1.TITLEThe International Nonproprietary Name (INN) established by the World Health Organization should be used wherever it is available; it is supplemented as appropriate by the name of the anion or cation and by the degree of hydration. Anions and cations are indicated as “mono-, di-, tri-, etc.”, as appropriate.The following rules apply for the degree of hydration.•In the case of a well-defined hydrate, “mono-, di-, tri-, etc…hydrate” is added to the title whereas if the monograph covers more than one degree of hydration, the general term “hydrate” is used. In the latter case, a sentence is added to the DEFINTION section (see chapter II.2). For monographs published prior to the 9th edition of the Ph. Eur., retrospective introduction of the degree of hydration in titles would only be made after careful consideration.•As of the 9th edition of the Ph. Eur, monographs referring to “anhydrous” substances will no longer specify this in their title with the exception of a few monographs where the information has a recognised added value and/or is used in common scientific language(e.g. Ethanol, anhydrous).•For monographs covering substances that can be either water-free or with, a defined or variable, degree of hydration, no mention will be added to the title. This information will be supplemented in the DEFINITION section of the monographs (see part II.2.).Where a substance is used in approved medicinal products for veterinary use only in Member States, “for veterinary use” is included in the title.II.2.DEFINITIONThe chemical structure must be ascertained with the greatest possible care in order to establish the exact:•graphic formula;•empirical formula and relative molecular mass. The latter is calculated as follows: first, the relative atomic masses, or multiples thereof, are added together using all thefigures of the International Table of Relative Atomic Masses; the total is then roundedoff to 4 significant figures if the initial digit is 1, 2, 3, 4 or 5, or to 3 significant figures ifthe initial digit is 6, 7, 8 or 9; the last figure is increased by 1 when the part rejectedexceeds one half-unit. When the part rejected is equal to or less than one half-unit, thelast figure taken is not modified;•chemical name. This involves investigating in particular:o the possible existence of isomers so as to be able to specify which isomer is used or, otherwise, to state that the product is a mixture of isomers;o in the case of an optical isomer, it is insufficient to take into account only the direction of the optical rotation. The absolute configuration is given by the R/Ssystem at the asymmetrical centre(s) or any other appropriate system (e.g., forcarbohydrates and amino acids);o ascertaining the state of hydration so as to distinguish clearly between the well-defined hydrates (mono-, di-, tri-, etc… hydrate) and the products that containvariable quantities of water. In the latter case, the term “x-hydrate” is introduced inthe chemical name.If the substance contains a variable quantity of water, or refers to both water-free and hydrate form, a sentence is added to the DEFINITION section to explain the exact scope of the monograph.Some chemical substances, particularly those obtained from raw materials of natural origin and substances produced by fermentation may not be easily separated from certain related substances (for instance, quinine salts). These may be treated as:• a chemical product when obtained in a very pure state and when they can be assayed by a physico-chemical method;• a substance accompanied by a certain proportion of related substances, giving an exact definition of the main component only (e.g. neomycin);• a mixture of several components, sometimes difficult to define, where an overall description may suffice (e.g. nystatin).Where applicable, the origin of the substance must be specified (name and strain of the organism from which the substance is derived). Where applicable, the monograph indicates that the substance is semi-synthetic and derived from a fermentation product [to clarify application of the general monograph Substances for pharmaceutical use (2034)].binationsIn therapeutics, more or less well-defined chemical combinations (for instance, theophylline- ethylenediamine) or even mixtures are sometimes used. In such cases, it is necessary to specify precisely each component of the combination or mixture, with its chemical structure and the proportion in which it is present.II.2.2.ContentThe substance described by a monograph is never a wholly pure substance but contains a limited proportion of impurities. The content is therefore an important part of the definition. Assay limits are specified between which the content must fall.In setting these limits for the active substance content, account is taken of:•the method of preparation, which determines the degree of purity that may be reasonably required;•the reproducibility and accuracy of the analytical method;•current batch data of about 10 production batches at release;•the evaluation of batch stability data;• a sufficient number of experimental results obtained on several batches (at least 3), if possible, of different origins and ages.For a non-specific assay by titrimetry the limits are set according to the table provided in part III.3.7 i.e. usually 99.0-101.0 %. Some monographs still include an assay by UV-Vis spectrophotometry usually bearing wider limits.For a specific assay using a separation technique (for example, liquid or gas chromatography), the upper assay limit is normally 102.0 %; the lower assay limit will take any necessary account of the impurities present based on the available batch data and approved specifications. It may therefore be lower than 98.0 %.assay, or when it contains only a very low proportion of impurities interfering with the assay, the results of the assay can be used directly. It will then be stated that: “[the substance] contains not less than x per cent and not more than the equivalent of y per cent (at least 100.5 %, but often a little more) of [chemical definition of the pure product]”. The content of the substance is usually expressed with reference to the anhydrous or dried substance. According to the general monograph Substances for pharmaceutical use (2034) the content of residual solvent is taken into account for calculation of the assay content of the substance, therefore no reference in the DEFINITION section of the individual monograph is made.In cases where the water content is high (e.g. in the case of disodium phosphate dodecahydrate), limits of content may be expressed with reference to the hydrate form of the substance, taking into account the molecular mass of the hydrate form (only for well-defined hydrates) or with reference to the substance on the anhydrous/dried basis in combination with determination of water content/loss on drying.When the substance to be examined contains a relatively large proportion (a few %) of impurities, which are determined at the same time as the active ingredient, an appropriate wording is to be used (for instance, in the case of quinine salts: “x per cent of total alkaloid salts, expressed as quinine salts”).Exceptionally reference is made to only a part of the molecule or to an element (for example assay of magnesium oxide in light magnesium carbonate or assay of magnesium in magnesium stearate).In the case of antibiotics determined by microbiological assays, the active ingredient content is expressed in International Units, where these exist, and only a minimum value is given.See also under part II.6.II.3.CHARACTERSAs defined in the General Notices, statements under the heading CHARACTERS are not to be interpreted in a strict sense and are not regarded as analytical requirements. The principal items that may be referred to under this heading are the following.II.3.1.AppearanceThis description will normally embrace colour and physical form. The term “white” is not used without qualification since, if viewed against a standard white material, very few pharmaceutical materials will appear truly white. It is, of course, not intended that such a comparison be made but experience shows that certain users of the Ph. Eur. may insist on doing so as part of a purchasing contract. The term “white or almost white” is used instead. Where positive colours are to be described, this is done in terms of primary colours or combinations of primary colours.Colour: the following descriptive terms are used: black, orange, blue, pink, brown, red, colourless, violet, green, white/almost white, grey, yellowCompound terms may be used:English Frenchgreenish-blue bleu-vertbluish-green vert-bleuviolet-red rouge-violetreddish-violet violet-rougebrownish-red rouge-brunreddish-brown brun-rougeIt can be noted that in English, the dominant is placed second, whereas in French, it is placed first. Expressions such as lemon-yellow, buff, salmon-pink are to be avoided; standard dictionaries give equivalents for such terms as spectral colours with suitable qualifiers (for example, buff is described as “dull yellow”). The following adjectives are also used; light, slight, fluorescent, intense, pale, dull, deep, dark.It is to be noted that the allowed colours and colour combinations also apply to the description of the colour changes of indicators when used in acid/alkalinity tests or in titrimetric assay procedures.II.3.2.TasteThe taste is not to be taken into consideration.II.3.3.OdourIn general, no reference is made to odour. In particular no reference to odour is made for those materials that would constitute a hazard if inhaled. Mention of odour in other cases must be justified.II.3.4.SolubilityA method recommended for the estimation of solubility is given in general chapter5.11.Characters section in monographs. All solubilities are quoted in the general terms defined in the General Notices. Solvents quoted are normally confined to water, an alcohol and a lipophilic solvent (e.g. water, ethanol, heptane). Solubilities in chloroform and ether are not mentioned and the use of hexane is discouraged. In special cases the solubility of different samples of a material may vary rather considerably even though their composition is still within the limits set by the monograph. The solubilities in the solvents thereby affected are then given to cover more than one solubility class, e.g. “sparingly soluble to soluble in...”. The solubilities or miscibilities in other solvents with which the material is often combined in practice such as fatty oils, etc., may also be mentioned. In some cases it may be useful to specify solubility in alkalis or acids and, particularly in cases of materials that are very insoluble in the above-mentioned solvents, a special solvent may be indicated, e.g. dimethylformamide or dimethyl sulfoxide. It is not necessary to specify the solubility in every solvent that is used in performing the tests of the。
医药制造业面临的机遇和挑战分析一、我国医药制造行业发展概况1、医药产品市场规模保持持续增长医药制造业是关系民生的重要行业,也是我国国民经济的重要组成部分。
我国人口众多且结构趋于老龄化,药品消费需求刚性巨大。
近年来,受到两票制、集中带量采购等政策改革的影响,我国医药制造业的增速有所放缓,产业规模增长受到一定影响,但仍维持在较高水平。
根据FroStGSullivan统计,我国医药市场规模从2016年的 13,294亿元增长至2020年的14,480亿元,预计2025年将达到 22,873 亿元。
2、化学药市场份额最大按药品类型划分,我国药品可分为化学药、中药、生物药。
根据FroSt&SulIivan数据,2020年,我国化学药市场份额最大,占比49. 27%;中药市场份额占比26.69%;生物药市场份额占比24. 04%。
3、公立医院市场份额最大,终端药店市场份额逐步提升按终端客户类型划分,我国药品终端市场可划分为公立医院、零售药店(含实体药店和网上药店)、公立基层医疗机构(含社区卫生中心、乡镇卫生院)三大类。
米内网数据显示,近年来我国医药终端市场中,公立医院终端市场份额最大,占比65%左右;零售药店市场份额其次,占比25%左右,并逐步上升;公立基层医疗机构占比10%左右。
二、面临的机遇和挑战1、面临的机遇(1)国家政策对医药行业的整体扶持国家政策对医药行业的扶持给行业发展带来机遇。
医药制造行业为国家鼓励类行业,近年来国家出台一系列政策鼓励医药制造业的健康发展,为本行业的发展提供了良好的宏观市场环境,也迎来发展机遇。
(2)国家医保政策改革保障居民用药需求2018年5月国家医疗保障局正式挂牌成立,主要职能是药品和医疗服务价格管理、药品集中招标和医保支付,进一步完善了我国的医疗保障体系。
同时,医保改革的逐渐深入,部分惠及民生安全的药品通过谈判方式纳入医保、推进城乡居民医疗保险整合,提高医保财政补助、逐步扩大按病种付费的病种数量等多项医保政策的实施,有效保障了我国居民的用药需求,进一步促进了医药市场的健康发展,为行业发展提供机遇。
一贴膏药如何火爆十五年记者实地考察揭开郁鑫膏神秘面纱[本刊记者]初玮8月25日记者再次实地考察长春郁鑫医药有限公司。
这是第几次实地采访薛总,记者也记不清了。
但每一次来,却总能带给记者惊喜。
在郁鑫医药有限公司总部,薛总对记者说:“咱俩先聊点别的,我邀请了一个加盟商,你一会采访她,我跟你说,她可老厉害了。
”究竟怎么厉害呢?记者怀着一份好奇的心等待着,并和薛总聊起了郁鑫膏。
怎样让患者认可?———关键是要看疗效。
郁鑫医药的文章记者已经连续写了3年,每期都有新内容,每期都有新案例,就是想让读者看一看,郁鑫医药十五年来的不断变化创新。
但细心的读者会发现,不论案例怎么变化,郁鑫膏内在的品质却不曾改变,即:药效和主治病症不会变。
薛总说:“现在不论什么产品,关键得看疗效。
要是没有效果,说什么都是白费。
”郁鑫膏是纯天然中草药提纯精制而成,与市面上的膏药有着显著的区别。
贴上之后绝无灼热感、针刺感,疗效立竿见影,不是那种有病没病贴上之后都有灼热感、针刺感。
郁鑫膏适用以下病症:风湿性关节炎、类风湿性关节炎、颈椎病、肩周炎、腰间盘突出、坐骨神经痛、骨质增生、腰肌劳损、手脚麻木、跌打损伤、抽筋、痛风、脊柱炎、腱鞘炎、网球肘、跟骨刺、关节炎、滑膜炎、骨折骨伤、股骨头坏死。
除对以上风湿骨病作用外,还适用于以下病症:月经不调、小肠疝气、痔疮、疗疮、哮喘咳嗽、前列腺炎、乳腺炎、腮腺炎、胆囊炎、阑尾炎、鼻炎、肠炎、牙痛、胃痛、胸膜炎、牛皮癣、静脉曲张、蚊虫叮咬、脚鸡眼、肿瘤疼痛、三叉神经痛、淋巴腺炎及各种无名疼痛。
除此之外,对面目斑痘(俗称青春痘)也有很好的治愈作用。
怎样让意向投资者放心?———证件齐全,无后顾之忧。
很多加盟商都曾遇到过这样的事。
加盟某个项目,总部证件不全,相关部门经常上门检查,不仅影响客流量,有的甚至还要面对罚款的问题。
加盟郁鑫膏,就不会发生这样的问题。
因为人家的手续完备,证件齐全。
郁鑫医药参加国药会就能说明一切问题。
国家中医药管理局关于公布2015年全国基层名老中医药专家传承工作室建设项目专家名单的通知
【法规类别】中药管理
【发文字号】国中医药人教函[2015]174号
【发布部门】国家中医药管理局
【发布日期】2015.09.30
【实施日期】2015.09.30
【时效性】现行有效
【效力级别】XE0303
国家中医药管理局关于公布2015年全国基层名老中医药专家传承工作室建设项目专家名
单的通知
(国中医药人教函〔2015〕174号)
各省、自治区、直辖市中医药管理局:
根据《国家中医药管理局办公室关于印发2015年全国基层名老中医药专家传承工作室建设项目实施方案的通知》(国中医药办人教发〔2015〕25号)精神,我局组织开展了2015年全国基层名老中医药专家传承工作室建设项目。
在各省(区、市)遴选推荐的基础上,经我局审核,确定于增瑞等200人为2015年全国基层名老中医药专家传承工作室建设项目专家。
现予公布。
附件:2015年全国基层名老中医药专家传承工作室建设项目专家名单
国家中医药管理局
2015年9月30日
附件
2015年全国基层名老中医药专家传承工作室建设项目专家名单。
客观结构化临床考试(OSCE)题型资料(临床类)福建中医药大学教务处2015年3月目录第一站病史采集 (1)第二站体格检查 (15)第三站急救技能 (34)第四站内科技能 (41)第五站外科技能 (55)第六站病例分析 (65)第八站辅助检查 (68)附件:1.病例分析考核答题纸(临床类) (70)2.辅助检查考核答题纸(临床类) (72)第一站病史采集一、发热【样题】简要病史:男孩,9岁2个月。
发热2天,皮疹1天门诊就诊。
要求:你作为住院医师,请围绕以上简要病史,口述应如何询问该患者的现病史及相关病史的内容。
【答案及评分要点】1.现病史(70分)(1〕根据主诉及相关鉴别询问①发病诱因:有无受凉、上呼吸道感染(10分)。
②发热:程度,体温变化情况,有无畏寒或寒战(10分)。
③皮疹:部位、形状、颜色、发疹顺序,有无瘙痒,与体温的关系(10分)。
④伴随症状:有无咳嗽、流涕、咽痛,有无头痛、呕吐、腹泻(10分)。
(2)诊疗经过①是否曾到医院就诊,做过哪些检查:血常规(10分)。
②治疗情况:是否用过抗菌药物或退热药物治疗,疗效如何(10分)。
(3)一般情况发病以来精神、饮食、睡眠及小便情况(10分)。
2.其他相关病史(20分)①生长发育情况(7分)。
②有无药物过敏史,预防接种史(6分)。
③与该病有关的其他病史:既往有无类似情况。
有无传染病患者接触史(7分)。
3.问诊技巧(10分)①条理性强,能抓住重点(5分);②能围绕病情询问(5分)。
二、皮肤黏膜出血【样题】简要病史:男性,25岁,发现双下肢皮肤对称性紫癜5天门诊就诊。
要求:你作为住院医师,请围绕以上简要病史,口述应如何询问该患者的现病史及相关病史的内容。
【答案及评分要点】(一)现病史(70分)(1)根据主诉及相关鉴别询问①发病病因或诱因:如发病前有无感染(特别是上呼吸道感染),进食鱼、虾、蛋等异性蛋白食品及服用某些药物。
(10分)②皮肤紫癜情况:颜色、数量多少,有无痒感,是否高起皮肤。
全国医疗卫生服务体系规划纲要(2015—2020年)为贯彻落实《中共中央关于全面深化改革若干重大问题的决定》、《中共中央国务院关于深化医药卫生体制改革的意见》、《国务院关于促进健康服务业发展的若干意见》(国发〔2013〕40号)精神,促进我国医疗卫生资源进一步优化配置,提高服务可及性、能力和资源利用效率,指导各地科学、合理地制订实施区域卫生规划和医疗机构设置规划,制定本规划纲要。
第一章规划背景第一节现状经过长期发展,我国已经建立了由医院、基层医疗卫生机构、专业公共卫生机构等组成的覆盖城乡的医疗卫生服务体系.截至2013年底,我国有医疗卫生机构97.44万个,其中医院2。
47万个,基层医疗卫生机构91.54万个,专业公共卫生机构3.12万个;卫生人员979万名,其中卫生技术人员721万名;床位618万张.每千常住人口拥有医疗卫生机构床位4.55张、执业(助理)医师2。
06名、注册护士2.05名.2004-2013年,全国医疗卫生机构总诊疗人次由每年39。
91亿人次增加到73。
14亿人次,年均增长6。
96%,住院人数由每年6657万人增加到1.91亿人,年均增长12。
42%。
但是,医疗卫生资源总量不足、质量不高、结构与布局不合理、服务体系碎片化、部分公立医院单体规模不合理扩张等问题依然突出。
一是与经济社会发展和人民群众日益增长的服务需求相比,医疗卫生资源总量相对不足,质量有待提高。
每千人口执业(助理)医师数、护士数、床位数相对较低。
执业(助理)医师中,大学本科及以上学历者占比仅为45%;注册护士中,大学本科及以上学历者占比仅为10%.二是资源布局结构不合理,影响医疗卫生服务提供的公平与效率。
西部地区医疗卫生资源质量较低。
基层医疗卫生机构服务能力不足,利用效率不高.中西医发展不协调,中医药(含民族医药,下同)特色优势尚未得到充分发挥。
公共卫生服务体系发展相对滞后。
公立医疗机构所占比重过大,床位占比近90%。