Long-term outcomes
- 格式:pdf
- 大小:487.93 KB
- 文档页数:9
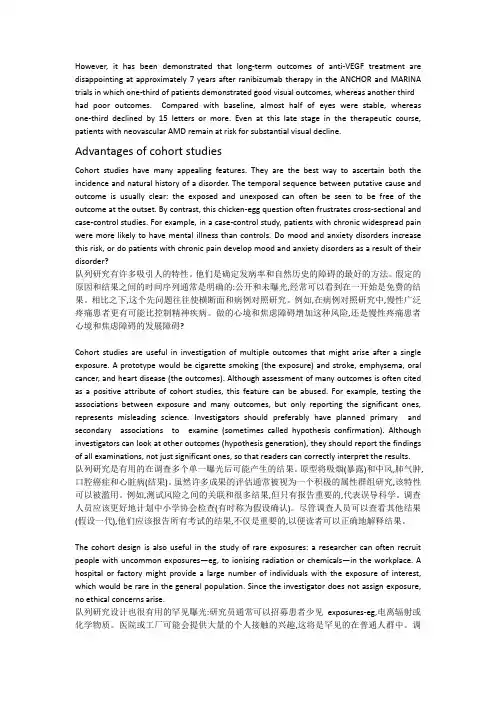
ORIGINAL ARTICLELong-term outcomes of the Ajust®Adjustable Single-Incision Sling for the treatment of stress urinary incontinenceGert Naumann&Thomas Hagemeier&Stefan Zachmann&Aktham Al-Ani&Stefan Albrich&Christine Skala&Rosa Laterza&Misti Linaberry&Heinz KoelblReceived:12February2012/Accepted:20May2012#The International Urogynecological Association2012AbstractIntroduction and hypothesis The aim of this study was to evaluate the effectiveness and overall safety of the Ajust®Adjustable Single-Incision Sling in the treatment of female stress urinary incontinence.Methods This was a prospective,multicenter study con-ducted in women diagnosed with stress urinary inconti-nence.The Ajust®Sling was implanted and patients were followed postoperatively for up to29months.Evaluations were performed to assess postoperative rate of continence, complications,and patient quality of life(QOL).Results From November2008through May2009,52 patients were enrolled and underwent a procedure to implant the Ajust®Sling.Overall,86.3%of the patients who successfully received the Ajust®Sling demonstrated total restoration or improvement of continence at the last study visit.QOL scores related to global bladder feeling and lifestyle improved.Only one patient reported the occurrence of mild pain which resolved without treatment or sequelae.Conclusions In long-term follow-up,the Ajust®Sling was safe and effective,restoring or improving continence in 86.3%of patients.Keywords Ajust®.Stress urinary incontinence.Adjustable sling.Single-incision sling.Long-term.Success rate AbbreviationsAjust®Sling Ajust®AdjustableSingle-Incision SlingBMI Body mass indexCST Cough stress testPGI-I Patient Global Impression of Improvement PPIUS Patient Perception of Intensityof Urgency ScalePVR Post-void residualQOL Quality of lifeSUI Stress urinary incontinenceTVT Tension-free vaginaltapeG.Naumann(*):S.Albrich:C.Skala:terza:H.KoelblDepartment of Obstetrics and Gynecology,University MedicalCenter,Johannes Gutenberg University Mainz,Langenbeckstrasse1,55131Mainz,Germanye-mail:gnaumann@uni-mainz.deS.Albriche-mail:albrich@uni-mainz.deC.Skalae-mail:skala@uni-mainz.deterzae-mail:rmslaterza@libero.itH.Koelble-mail:koelbl@frauen.klinik.uni-mainz.deT.HagemeierPelvic Floor Center SRH Hospital,Suhl,Germanye-mail:kuthagemeier@S.ZachmannDepartment of Obstetrics and Gynecology,Hospital Männedorf,Männedorf,Switzerlande-mail:s.zachmann@spitalmaennedorf.chA.Al-AniPelvic Floor Center,Hufeland Hospital,Bad Langensalza,GermanyM.LinaberryCorporate Clinical Affairs,C.R.Bard,Murray Hill,NJ,USAe-mail:misti.linaberry@Int Urogynecol JDOI10.1007/s00192-012-1843-7UUI Urgency urinary incontinenceV AS Visual analogue scaleIntroductionStress urinary incontinence(SUI)is estimated to affect up to 35%of women worldwide,leading to reduced quality of life(QOL)[1].Despite options for conservative treatment, surgery remains the primary treatment intervention.Several surgical procedures can create sufficient closure of the ure-thra;however,simplified surgical approaches have led to lower complication rates and fewer side effects with high rates of success.Traditional surgical therapies including the Burch colposuspension and autologous sling procedures have shown positive results.Yet,these methods are invasive and often require general anesthesia with hospital stay.The introduction of the retropubic tension-free vaginal tape(TVT)procedure in1996transformed treatment options,offering a minimally invasive,ambulatory proce-dure with long-term cure rates in women with SUI[2,3]. However,TVT has been associated with bladder perfora-tion,and on rare occasions,bowel and vascular injuries[4]. The transobturator approach was developed with the aims of reducing morbidity associated with blind retropubic needle placement[5].Clinical studies,both randomized and non-randomized,of the transobturator and retropubic approaches have shown transobturator slings to have similar efficacy in restoring continence as compared to the more traditional repairs[4,6–10].In2006,single-incision slings made from similarly con-structed light-weight mesh material as that of the TVT were introduced.These slings are inserted with suburethral place-ment for restoration of continence.The advantages of the single-incision slings include limiting the number of inci-sions,reducing the amount of material,eliminating blind trocar passage,and providing strong fixation on both pelvic walls.Short-term safety and efficacy have been reported; however,longer term data are limited.Some single-incision sling studies demonstrate results comparable to conventional midurethral slings,while others show lower cure rates.In a randomized study of one con-ventional sling and two single-incision slings,12-month follow-up data showed one single-incision sling to have slightly higher cure rate(MiniArc™;87%)than the con-ventional sling(TVT-O™;83%),while the other single-incision sling(TVT-Secur™)had a lower cure rate(67%) and higher percentage of failures(25%)[11].The24-month follow-up data were consistent with the12-month results, with the MiniArc™demonstrating a slightly higher cure rate(87%)than the TVT-O™(82%),while the TVT-Secur™had a lower cure rate(63%)and higher percentage of failures(25%)[12].The Ajust®Adjustable Single-Incision Sling(Ajust®Sling)represents a further advancement of the single-incision slings.Ajust®is the only post-insertion fully ad-justable,single-incision sling that anchors in the transobtu-rator muscle/membrane complex for tension-free support of the urethra.The aim of this study was to evaluate the use of the Ajust®Sling in women for the treatment of SUI.Patients were evaluated for the restoration of continence,complica-tions,and QOL with a focus on pain symptoms.Two-year follow-up data are reported.MethodsThis was a prospective,single-arm,observational,multicen-ter study conducted at four study centers in Germany(n03) and Switzerland(n01).Female patients with a body mass index(BMI)<35kg/m2,aged>18years,with a symptom-atic clinical and urodynamic diagnosis of primary SUI,and unsuccessful conservative treatment were enrolled.Study center Ethics Committees were informed of the study and all patients provided written informed consent for participation.Exclusion criteria were:accompanying vaginal prolapse; prior surgeries of mesh implants,Burch procedure,or anterior vaginal repair;mixed urinary incontinence where SUI-urgency urinary incontinence(UUI)or SUI<UUI;inconti-nence relapse;hypotonic urethra(maximum urethral closure pressure at rest of less than20cmH2O in urethral profilometry using an external fluid-filled catheter);and planned combina-tion surgeries for treatment of descensus.The primary objective and outcome endpoint measure was postoperative rate of continence as evaluated by a standardized cough stress test(CST)with a bladder volume of approximately300ml(confirmed by ultrasound).If the CST was positive and urine loss was observed with cough-ing,incontinence was defined using the Ingelman-Sundberg scale where grade I0leakage during strenuous activity, grade II0leakage during normal activity,and grade III0 urinary loss in the supine position[13].Secondary objectives and outcome endpoint measure-ments were complications and patient plications were assessed intra-,peri-,and postoperatively and included evaluation of bleeding>200ml,bladder lesions,erosions, perforations,penetrations,protrusions,hematomas,and bladder outlet obstructions.Terminology and classification of complications related to the insertion of prostheses and grafts in female pelvic floor surgery were consistent with those outlined by the International Continence Society and the International Urogynecological Association[14].Patient QOL assessments were performed for pain and bladder symptoms with a focus on SUI and lifestyle impactInt Urogynecol Jusing a visual analogue scale(V AS).The V AS used a10-cm measurement instrument to evaluate SUI symptoms.A score of0would indicate that the patient had no SUI symptoms and there was no impact on lifestyle,while a score of10 would indicate that the SUI was severe and adversely im-pacted the patient’s lifestyle to a significant degree.Urgency was evaluated using the Patient Perception of Intensity of Urgency Scale(PPIUS)which scored the intensity of urgen-cy at each void with a5-point scale(see Table1)[15]. Patients also completed the Patient Global Impression of Improvement(PGI-I),a validated,seven-item questionnaire used to assess improvement with therapy(very much better, much better,a little better,no change,a little worse,much worse,and very worse)[16].Questionnaires were complet-ed by patients prior to clinical examination.Additionally,data were collected on postoperative urine retention at the time of urinary void(post-void residual urine,PVR).The Ajust®Sling procedure was performed per the man-ufacturer’s instructions as provided in the Instructions for Use.Procedures were initiated with a1-cm midurethral vaginal incision and preparation of bilateral paraurethral tunnels to the posterior margin of the inferior pubic ramus. Surgeons used a curved introducer,loaded with self-fixating anchors,to pivot around the ischiopubic ramus and insert the anchor through the obturator internus muscle and obtu-rator membrane.The second,adjustable anchor was inserted,on the contralateral side,using the same technique. Following the insertion of both anchors,surgeons adjusted the sling for proper tensioning.In contrast to established retropubic and transobturator tapes(TOT),single-incision slings should be positioned in direct contact with the urethra without tension or narrowing.Postoperative care was not defined in the clinical study protocol and was to be per-formed per the institutions’standard of care.This included procedures for administration of antibiotics and removal of urinary catheters(typically performed at day1post procedure).Procedures were performed by trained urogynecologists who were experienced in pelvic floor surgery and single-incision sling insertion procedures.All investigators re-ceived product-specific training on the Ajust®Sling prior to their initial insertion procedure.Training included hands-on practice with pelvic models and instruction with a cadav-er implantation video.Additionally,a consulting physician/product expert attended and assisted in the initial cases for each investigator.Length of hospitalization was not defined in the study protocol but was influenced by country-specific reimburse-ment schedules,particularly in Germany where reimburse-ment was based on postoperative hospitalization of2nights.There were no formal a priori hypotheses defined for the study.Descriptive statistics[e.g.,sample size(n),mean, median,standard deviation,and range]were calculated for quantitative data.Proportions or frequency tables(n and percentage)were used to summarize qualitative data.Anal-yses of the postoperative rate of continence endpoint were conducted on two populations:(1)all patients who received the Ajust®Sling and(2)all patients who met protocol eligibility criteria.All other assessments were performed using the population including all patients who received the Ajust®Sling.Fifty-two women with SUI underwent a surgical proce-dure to receive the Ajust®Sling and were evaluated post-operatively at1day,6–8weeks,3months,6months, 12months,and at final follow-up performed in March 2011representing20–29months of total follow-up.Study follow-up procedures included vaginal examination,CST, QOL assessments,and urodynamic testing(PVR measured by ultrasound).ResultsDisposition,demographics,and procedural detailsFrom November2008through May2009,52patients with SUI were enrolled in this study and underwent a surgical procedure to receive the Ajust®Sling.Patients were fol-lowed for up to29months of postsurgical follow-up.The mean length of follow-up was25.2±2.24months(range20–29months).Forty-five(86.5%)patients completed the last scheduled follow-up visit in March2011.Demographic and baseline characteristics are shown in Table2.Patient dispo-sition and follow-up are shown in Fig.1.Seven patients who received the Ajust®Sling did not meet the protocol eligibility criteria including one patient who underwent a prior Burch procedure and six patients who had mixed stress or urgency incontinence.It was felt that since the Burch suspension was a retropubic openTable1Patient Perception of Intensity of Urgency Scale(PPIUS)0No urgency I felt no need to empty my bladder but did so for other reasons1Mild urgency I could postpone voiding as long as necessary without fear of wetting myself2Moderate urgency I could postpone voiding for a short while without fear of wetting myself3Severe urgency I could not postpone voiding but had to rush to the toilet in order not to wet myself 4Urgency incontinence I leaked before arriving at the toiletInt Urogynecol Jprocedure,the previous surgery would not have influenced the obturator muscle or membrane.All seven patients were included in the analyses to add to the generalizability of the study results.However,the analysis of postoperative rate of continence was performed with and without these seven patients.Sling implantation was performed under local,general, and spinal anesthesia in27(51.9%),24(46.2%),and1 (1.9%)patients,respectively.In all but one case,the place-ment procedure took less than30min.Of the52placement procedures,51(98.1%)were initially successful.The un-successful insertion attempt was determined to be related to improper placement of the sling,resulting in damage to the anchor during removal and repositioning attempts.Due to the anchor barb damage,the Ajust®Sling was not inserted and a conventional TOT was placed.The mean length of hospital stay was2.2±0.66days(range1–5days).Country-specific reimbursement schedules may have influenced the length of hospital stay.Postoperative rate of continenceThe postoperative rate of continence was calculated using two patient populations:(1)all patients who received the Ajust®Sling(including the seven patients who failed to meet protocol exclusion criteria)and(2)all patients who met protocol eligibility criteria.All patients who received the Ajust®Sling(n051)At the last study visit conducted in March2011,44(86.3%) of the51patients who received the Ajust®Sling demon-strated total restoration(n042;82.4%)or improvement of continence(n02;3.9%)(Table3).One patient(2.0%) demonstrated no SUI improvement over baseline.Six patients(11.8%)were discontinued from study follow-up early for the following reasons:two patients had indwelling catheters placed for reasons unrelated to the device or pro-cedure(ischemic stroke and Alzheimer’s disease),one pa-tient had the Ajust®Sling removed(due to dislocation of the sling at postoperative day14),two patients received addi-tional procedures(one patient received a bulking injection and the other underwent placement of a conventional TOT, both due to recurrence of incontinence),and one patient was lost to follow-up after the12-month visit though her conti-nence was reported as fully restored at the12-month visit. All eligible patients(n044)When the seven patients who failed to meet protocol eligibility were excluded from the analysis,the results showed that88.6% (n039)of the44eligible patients demonstrated total restoration (n037;84.1%)or improvement of continence(n02;4.5%) (see Fig.1).One patient(2.3%)demonstrated no SUI improve-ment over baseline.The remaining four patients discontinued prior to the March2011visit,as described above.Table2Demographics and baseline characteristics of enrolledpatients(n052)Age(years)[mean±SD(range)]62.8±10.5(39-88)n(%)PVR<50ml52(100)>50ml0History of previous procedure2(3.8)SUI grade I0II44(84.6)III8(15.4)Urgency No urgency46(88.5)Mild urgency0Moderate urgency2(3.8)Severe urgency3(5.8)Urgency incontinence1(1.9)Fig.1Disposition and follow-up of enrolled patients(n05)Int Urogynecol JPatients meeting exclusion criteriaOf the seven patients who met protocol-defined exclusion criteria,two were discontinued early[due to placement of indwelling catheter(Alzheimer’s disease)and loss to follow-up as described above]and five demonstrated full restoration of continence.ComplicationsNo complications of bleeding>200ml,bladder lesions, erosions,perforations,penetrations,protrusions,hemato-mas,or bladder outlet obstructions were reported at any time during the study.Although the event was not predefined as a complication, there was one case of recurrent urinary tract infection reported by one patient at the March2011visit,approxi-mately26months after the Ajust®Sling was placed.The events were treated with antibiotics.The patient did not report experiencing incontinence.PainOther than ibuprofen,which was given postoperatively,no other pain medications were administered to any patient at any time point during the study.One patient reported mild pain associated with the surgical procedure at1day post surgery.No further intervention was required for this event, which resolved on its own.No other patients reported pain after1day post surgery.Quality of lifeVisual analogue scaleMean preoperative V AS scores(baseline)were7.46±1.90cm (range4-10cm).At the March2011visit,mean V AS scores were decreased to1.09±1.19cm(range0-5cm),representing a mean change from baseline of−6.22±2.37cm.All patients’postoperative V AS scores improved(decreased)over their preoperative V AS scores,including patients who were en-rolled with mixed incontinence.Patient Global Impression of Improvement scoresPGI-I questionnaire data were collected and reported at the 6-month and March2011study visits(Fig.2).At month6, 86.3%of the patients reported that their continence was “very much better”(n039)or“much better”(n05)as com-pared to their condition prior to the Ajust®Sling placement procedure.One patient,who reported experiencing urinary leakage during normal activity between the3-and6-month visits,reported the6-month postoperative condition to be“a little worse.”Two patients reported“no change.”All other patients reported improvement.Of the45patients who completed the March2011study visit,82.4%of patients reported that their continence was“very much better”(n0 34)or“much better”(n08)as compared to their condition prior to the Ajust®Sling placement procedure.Two patients reported their condition to be“a little better”and one patient reported“no change.”UrgencyData available from baseline through last available observa-tion showed that45(88.2%)of the51patients who re-ceived an Ajust®Sling reported PPIUS scores of0or1, indicating the majority of patients felt no urgency or were able to postpone voiding as long as necessary without fear of wetting at each void(see Table4).This included three of the six patients who enrolled with existing urgency,though all were receiving anticholinergic medications.Of the six patients who did not report their last PPIUS score as a0or1,one patient had no available PPIUS scores after having her sling removed after the2-week study visit; however,the investigator reported that the patient had noTable3Continence by study visit(all patients who received the Ajust®Sling)n0511day post surgery6-8weeks postsurgery 3months postsurgery6months postsurgery12months postsurgeryMarch2011an(%)[95%CI]Continence fully restored49(96.1)[86.5–99.5]49(96.1)[86.5–99.5]49(96.1)[86.5–99.5]45(88.2)[76.1–95.6]43(84.3)[71.4–93.0]42(82.4)[69.1–91.6]Improved2(3.9)003(5.9)2(3.9)2(3.9) No improvement01(2.0)1(2.0)2(3.9)1(2.0)1(2.0) Discontinued study follow-up01(2.0)1(2.0)1(2.0)5(9.8)6(11.8)CI confidence intervala20-29months post surgeryInt Urogynecol Jurgency at the time of this procedure.Three patients noted improvement in urgency scores over baseline (baseline PPIUS scores of 3or 4were reduced to 2;all were receiving anticholinergic medications)and two patients reported se-vere urgency (discussed below).Based on clinical assessment,PPIUS scores of 2or greater were considered abnormal and represented cases of de novo (new onset)urgency.Two patients experienced moderate urgency (PPIUS score of 2)at a single follow-up time point and both cases improved to mild by the end of study participation without administration of any bladder control medications.Two other patients reported severe urgency.Both cases were treated with anticholinergic med-ications and treatment was ongoing at the end of study participation.Post-void residual volumeAt the 3-month post-procedure time point,all patients had PVRs of <50ml with the majority of patients (90.2%;46/51)having PVRs of <50ml at 1day post surgery (Table 5).DiscussionThe introduction of minimally invasive midurethral slings has changed the decision process for the surgical treatment of SUI in women.Several types of slings and placement procedures are available,including the relatively new ap-proach using single-incision slings aimed at reducing the invasiveness of more traditional methods.Adjustable single-incision slings with fixation in the transobturator space,such as the Ajust®Sling,represent the most recent advancement in the treatment of SUI and allow for post-insertion adjust-ment of the sling tension.There are few long-term data available,with most studies reporting cure rates at 6and 12months post procedure [17–20].Short-term data have shown the Ajust®Sling system to be effective in restoring continence with few complicationsand considerable improvements in reported patient QOL outcomes [17–20].However,there are very limited data available beyond 12months of follow-up.The final data of this prospective,multicenter study in-clude the longest follow-up period to date (mean 25.2±2.24months;range 20-29months).With 86.3%of the patients in this study achieving full restoration (n 042;82.4%)or improvement of continence (n 02;3.9%),these observed objective cure rates appear to be consistent with early results described in other studies of the Ajust®Sling system which have reported objective cure rates of 89.7%after 3months of follow-up [19],91.4%after 6months of follow-up [17],and 82–86%at 12months of follow-up [18,20].Together,the results from these studies demonstrate that the success rates observed with the Ajust®Sling are consis-tent and durable over prolonged follow-up.Additionally,the data from this study appear to be similar with the 24-month objective cure data reported for other single-incision slings (MiniArc ™)including Kennelly et al.[21]who reported 85.1%of patients with a negative CST and Resende et al.who reported an 87%cure with an additional 7%improvement [12].In a systematic review of the efficacy of three mini-slings (TVT-Secur ™,MiniArc ™,and Ajust ™),the overall7610642006716420102030405060708090100Very much better Much better better No changeA little A little worse Much worse Very muchworse% P a t i e n t sMonth 6March 2011Fig.2Patient GlobalImpression of Improvement scores from the March 2011study visitTable 4Patient Perception of Intensity of Urgency Scale (n 051)PPIUS grade Severity of urgency Preoperative scores Postoperative scores a 0None 45(88.2%)35(68.6%)1Mild 010(19.6%)2Moderate 2(3.9%)3(5.9%)3Severe3(5.9%)2(3.9%)4Incontinence1(2.0%)NA b1(2.0%)a Postoperative score 0last available postoperative observationbOne patient did not have a postoperative score,but the investigator reported no urgency at the time of Ajust®Sling removalInt Urogynecol Jobjective cure rate of the26studies included in the review was found to be81%(2,060/2,532)which is consistent with the82.4%cure rate seen in this study[22].Overall objec-tive cure rates with TVT-Secur™were75.6%.Another review and meta-analysis of nine randomized controlled trials comparing single-incision mini-slings(TVT-Secur™, MiniArc™,and Ophira™)and standard midurethral slings published through January2011showed significantly lower objective cure rates in patients receiving the single-incision mini-slings[23].The reviewers commented that these results may be attributed to the relatively short trajectory and less substantial fixation of the single-incision mini-slings as compared to the standard midurethral slings,result-ing in reduced anchoring and support,particularly with the TVT-Secur™.The Ajust®Sling is unique and allows for bidirectional adjustability(loosening and tightening)with strong,permanent anchoring in the obturator membrane.The single-incision sling utilizing the transobturator placement approach was designed to simplify previous tech-niques and minimize complication rates associated with blind needle passage.In this study,there were no complica-tions observed,including no reports of bleeding(>200ml), bladder lesions,erosions,perforations,penetrations,protru-sions,hematomas,or bladder outlet obstructions.Bladder injury has been reported in other studies to range between 0and1%of women during the placement of transobturator slings[22,24–27].Other studies of the Ajust®Sling system have also reported similar findings with most reporting no major complications.Rare accounts of vaginal bleeding and erosion have been reported[17–20].A few technical complications were experienced in this study.In one case,an unsuccessful insertion attempt was determined to be related to the improper placement of the Ajust®Sling,resulting in anchor barb damage.Due to this damage,the Ajust®Sling was not placed in the patient.A second patient received the sling but later had it removed due to improper placement and dislocation to the bladder neck.Other studies have reported minimal technical diffi-culty with the fixation of the anchors and reported that all procedures were successfully completed with most reinsert-ing a new Ajust®Sling[17,18].V oiding dysfunction has been reported following other transobturator sling procedures(4–11%)[25,28].However, the assessment criteria vary greatly.In this study,PVRs of greater than50ml were reported in five patients at1day post surgery and all PVRs were less than50ml by3months post procedure.No sling release procedures were performed for voiding dysfunction.Meschia et al.reported one case of urinary retention that required resection of the tape after9 days post Ajust®Sling placement,Mostafa et al.reported 4.3and1.4%of patients requiring catheterization or clean intermittent self-catheterization,respectively,following sur-gical placement of the Ajust®system,and Abdel-Fattah et al.noted unsatisfactory voiding in8.9%of patients,all consistent with the findings reported for other transobturator slings[17–19].Data available from baseline through last available ob-servation showed that the majority of patients(88.2%)felt no urgency or were able to postpone voiding as long as necessary without fear of wetting at each void.Very few patients developed de novo urgency.Postoperative de novo urgency seen in this study was similar to that seen in other patients following transobturator midurethral sling place-ment(7.8%in this study and6%for other transobturator approaches)[25]and was also within the range of de novo urgency reported in other Ajust®Sling studies(approxi-mately5–14.5%)[17,19,20].It is important to note that two of the patients who were reported as having de novo urgency actually reported PPIUS scores of2(moderate urgency with the ability to postpone voiding for a short time)at a single follow-up time point and both cases im-proved to mild(PPIUS score of1:ability to postpone void-ing as long as necessary)by the end of study participation. The remaining two cases appeared to be representative of true de novo urgency cases,as both patients reported severe urgency which was ongoing at the end of study participation and required anticholinergic medications.Additionally,a few patients with mixed stress and urgen-cy incontinence(where UUI≥SUI)were enrolled in this study and were included in the analysis for generalizability of the data.Results showed that of the six patients whoTable5Summary of study results from the51women who received the Ajust®SlingComplications,n(%)1aContinence improved or fullyrestored,n(%)44(86.3%)Fully restored42(82.4%) Improved over baseline2(3.9%)Pain,n(%)only1day postoperative1(2.0%)QOL V AS scores b(mean changefrom baseline,SD)−6.22±2.37PGI-I scores demonstrating improvement c44(86.3%)De novo urgency4(7.8%) Moderate,improved to mild2(3.9%)Severe,ongoing2(3.9%)PVR51(100%)WNL by3months post procedureQOL quality of life,VAS visual analogue scale,SD standard deviation, PVR post-void residual,WNL within normal limitsa Event of recurrent urinary tract infection listed as a complication related to the device was unclear given the timing of the event (26months post procedure)b n045patients who completed the V AS at the March2011study visitc Improvement0responses at the March2011visit of very much better (n034),much better(n08),and a little better(n02)Int Urogynecol J。