淋巴管肌瘤病的肺部CT表现
- 格式:ppt
- 大小:8.19 MB
- 文档页数:34

作者单位:100730中国医学科学院中国协和医科大学北京协和医院放射科胸部放射学肺淋巴管肌瘤病的临床表现及HRCT特点周 璐,张竹花,金征宇【摘要】 目的 探讨肺淋巴管肌瘤病(P LAM)的临床特征及高分辨率CT(HRCT)表现,旨在提高对该病的认识。
资料与方法 回顾性分析9例经病理证实并行HRCT检查的P LAM患者资料,分析其临床表现、肺功能结果、X线胸片及HRCT特点。
结果 9例均以进行性呼吸困难为主要临床表现,1例伴有反复自发性气胸,2例伴乳糜胸。
肺功能检查表现为以阻塞性通气功能障碍为主的混合性通气功能障碍和弥散功能降低;X线胸片8例呈弥漫性网状阴影,1例可见蜂窝状囊腔;HRCT扫描均见均匀散在性分布的直径2.0~20mm的薄壁囊腔,壁厚1.5~2.0 mm,病变早期囊腔之间可见正常肺组织。
结论 P LAM主要临床特征是进行性呼吸困难,常可伴有咯血、气胸、乳糜胸,疑诊P LAM时应及时行HRCT及肺功能检查,必要时需行肺活检,以明确病理诊断。
HRCT对该病的早期诊断、鉴别诊断具有重要价值。
【关键词】 肺淋巴管肌瘤病 高分辨率CTThe C li n i c and HRCT Fea tures of Pul m onary L ym phang i o m yoma tosisZHOU Lu,Z HANG Zhuhua,J I N ZhengyuDepart m ent of Radi ol ogy,Peking Uni on Medical College Hos p ital,Chinese Acade myof Medical Science,Beijing100730,P.R.China【Abstract】 O bjecti ve To discuss clinic and high res oluti on computed t omograghy(HRCT)features in pul m onary ly m2 phangi omyomat osis(P LAM)and t o make a further understanding of this disease.M a ter i a ls and M ethods 9cases of P LAM with pathol ogically p r oved were revie wed retr os pectively.Clinic manifestati ons,pul m onary functi on results,chest X ray and HRCT findings were analyzed.Results The main clinic manifestati ons included p r ogressive dys pnea(n=9), repeated pneu mothorax(n=1),and chyl op leura(n=2).Pul m onary functi on showed m ixed ventilati on disturbance with obstructive ventilati on disturbance mainly.I n8patients,chest X2ray showed reticular opacities and honeycombing opacities in1patient.HRCT de monstrated thin2walled cysts2-20mm in diameter and1.5-2.0mm in wall thickness in all pa2 tients,scattering at random in all parts of the lung.I n the early stage of the disease,lung tissue bet w een cysts appeared nor mal.Conclusi on The main clinic manifestati ons of P LAM are p r ogressive dys pnea with repeated pneu mothorax,chy2 l op leura and he mop tysis.HRCT is a valuable modality in the early diagnosis of P LAM.【Key words】 Pul m onary ly mphangi omyomat osis H igh res oluti on computed t omograghy 肺淋巴管肌瘤病(pul m onary ly mphangi omyoma2 t osis,P LAM)是一种罕见、原因不明的错构瘤样病变,以支气管、细支气管、肺泡间隔和肺血管、淋巴管周围的不典型平滑肌细胞进行性浸润为主要病理特征。
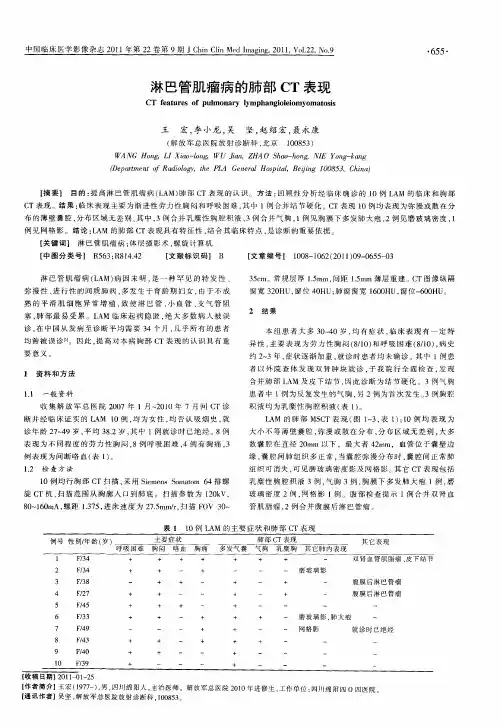
淋巴管肌瘤病的影像表现陈孝柏侯睿张建梅温廷国石峰目的探讨淋巴管肌瘤病(LAM)的影像学诊断价值。
方法回顾性分析15例经临床和病理证实的LAM胸部X线平片、HRCT,腹部CT和直接淋巴管造影(DLG)及DLG后胸腹部CT扫描等影像资料。
结果15例中,X线胸片上未见异常1例,双肺纹理增多3例,弥漫性小蜂窝状影或网格状影11例,气胸2例,胸腔积液14例。
胸部常规CT和HRCT扫描显示15例均具有典型LAM表现,均可见两肺散在囊状影或广泛密布的囊状影。
按Avi1a等肺部疾病程度分级标准:Ⅰ级3例;Ⅱ级5例;Ⅲ级7例。
腹部CT显示14例在腹膜后、盆腔可见囊性淋巴管瘤9例,淋巴管肌瘤13例,二者共同存在7例,并发肝脏脂肪瘤和血管平滑肌脂肪瘤、肾脏小错构瘤及子宫肌瘤各1例。
DLG检查,除1例淋巴管梗阻部位在腰3水平外,其余14例均可见胸导管不同程度的狭窄、梗阻及颈干和(或)锁骨下干和(或)支气管纵隔干淋巴管反流。
DLG术后CT,除3例未显示胸导管出口梗阻外,其余12例显示胸导管出口梗阻情况与DLG基本一致。
结论HRCT对肺淋巴管肌瘤(PLAM)的诊断具有特征性价值,CT可发现腹部LAM,DLG和DLG后MSCT对因LAM引起的胸导管或淋巴管干梗阻部位的显示具有价值,可为手术治疗提供一定的帮助。
淋巴管肌瘤病;体层摄影术,X线计算机;淋巴造影术Imaging diagnosis of the lymphangioleiomyomatosis CHEN Xiao-bai* HOU RuiZHANG Jian-meiWEN Ting-guo SHI Feng Department of Radiology, Beijing Shijitan Hospital , Beijing 100038, China Objective To investigate the value of imaging diagnosis of the lymphangioleiomyomatosis( LAM ). Methods Fifteen patients with LAM confirmed by pathological assessment were analyzed retrospectively for radiologic findings. They had chest radiograph, chest highresolution CT (HRCT),abdominal CT, direct lymphangiography(DLG), chest CT and abdominal CT after DLG. Results Chest radiograph findings included normal (1), increasing of lung markings (3),disseminated honeycomb or reticular pattern ( 11 ), pneumothorax ( 2 ), and pleural effusion ( 14 ). Chest conventional CT and HRCT showed typical imaging manifestation of PLAM in all cases, including sporadic or disseminated cysts in bilateral lungs. According to the grading standard of pulmonary disease made by Avila et at, there were 3 cases in grade Ⅰ , 5 cases in grade Ⅱ and 7 cases in grade Ⅲ . Fourteen of 15 patients with LAM had positive abdominal CT findings in retroperitoneum and pelvic cavity. Common abdominal CT findings included cystic lymphangioma in 9 of 14 patients, lymphangiomyoma in 13 and both coexisting in 7.One of the 14 patients also had hepatic lipoma and angiomyolipomas. One patient had renal angiomyolipomas; and one patient had hysteromyoma. All 15 cases underwent DLG, 1 cases had lymphatic obstruction in the lumbar 3 level, the remaining 14 cases had varying degrees of thoracic duct stenosis, or obstruction. Neck trunk, subclavian trunk and bronchial trunk showed lymphatic reflux. On post-DLG CT,thoracic duet outlet obstruction was not demonstrated in 3 cases, the remaining 12 cases showed thoracic outlet obstruction, consistent with the DLG findings. Conclusion HRCT is a useful diagnostic method showing characteristic findings of PLAM. MSCT can help to detect abdominal LAM. DLG and MSCT after DLG have value in displaying obstruction site of thoracic duct or lymphatic trunks and provide guidance for operative treatment. Lymphangiomyomatosis; Tomography,X-ray computed ; Lymphography 10. 3760/cma. j. issn. 1005-1201. 2011. 09. 009 作者单位:100038 北京世纪坛医院放射中心(陈孝柏、侯睿、张建梅,温廷国).病理科(石峰)万方数据842万方数据843万方数据万方数据@@[1 ] Avila NA, Chen CC, Chu SC, et al. Pulmonary [ymphangioleiomyomatosis: conrelation of ventilation-perfusion scintigraphy, chest radiogrsphy, and CT with pulmonary function tests. Radiology, 2000,214: 441-446.@@[2] Müller NL, Chiles C, Kullnig P. Pulmonary lymphangiomyomatosis: correlation of CT with radiographic and functional findings. Radiology, 1990,175:335-339.@@[3] Aberle DR, Hansell DM, Brown K, et al. Lymphangiomyomatosis: CT, chest radiographic, and functional correlations. Radiology, 1990,176:381-387.@@[4] Avila NA, Dwyer AJ, Rabel A, et al. Sporadic lymphangiomyomatosis and tuberous sclerosis complex with lymphangiomyomatosis : comparison of CT features. Radiology, 2007,242:277-285.@@[5]刘亦庸,张连郁,张熙曾,等.一种罕见疾病胸内淋巴管肌瘤 病一例.中国肿瘤临床,1986,13:116-118.@@[6]从振杰,刘旭林,周承涛,等.淋巴管肌瘤病的CT诊断(附二 例报告及文献复习).中华放射学杂志,2004,38:755 -758.@@[7] Taylor JR, Ryu J, Colby TV, et al. Lymphangiomyomatosis: clinical course in patients. N Engl J Med,1990,323:1254-1260. @@[8] Kitaichi M, Nishimura K, Itoh H, et al. Pulmonary lymphangioleiomyomatosis: a report of 46 patients including a clinicopathologic study of prognsstic factors. Am J Respir Crit Care Med, 1995,151:527-533. @@[9] Matsui K, Beasley MB, Nelson WK, et al. Prognostic significance of pulmonary lymphangioleiomyomatosis histologic score. Am J Surg Patho1,2001 ,25:479-484.@@[10] Avila NA, Kelly JA, Dwyer AJ, et al. Lymphangioleiomyomatosis : correlation of qualitative and quantitative thin-section CT with pulmonary function tests and assessment of dependence on pleurodesis. Radiology, 2002,223 : 189-197.@@[ 11 ] Avila NA, Kelly JA, Chu SC, et al. Lymphangioleiomyomatosis: abdomino pelvic CT and US findings. Radiology, 2000, 216: 147-153.@@[12] Casper KA, Donnelly LF, Chen B, et al. Tuberous sclerosis complex : renal imaging findings. Radiology ,2002,225:451-456.@@[ 13] Abbott GF, Rosado-de-Christenson ML, Frazier AA,et al. From the archives of the AFIP: lymphangioleiomyomatosis: radiologic pathologic correlation. Radiographics,2005,25: 803-828.@@[ 14] Avila NA, Bechtle J, Dwyer AJ, et al. Lymphangioleiomyomatosis : CT of diurnal variation of ]ymphangioleiomyomas. Radiology, 2001, 221:415-421.@@[15] Pallisa E, Sanz P, Roman A, et al. Lymphangioleiomyomatosis: pulmonary and abdominal findings with pathologic correlationL Radiographics, 2002,22 : 185-198.@@[16] Guermazi A, Brice U, Hennequin C, et al. Lymphography: an old technique retains its usefulness. Radiographics, 2003,23: 1541-1558.2011-02-15万方数据。
肺淋巴管肌瘤病的胸部影像学表现张莉;欧陕兴;彭光明;郭元星;齐燕;李小荣;刘海凌;罗道首【摘要】目的探讨肺淋巴管肌瘤病(PLAM)的影像学表现.方法报告3例PLAM病例,结合文献资料对该病病因、临床特点及影像学表现进行讨论.结果 3例患者均为育龄期女性,首发症状均为活动后呼吸困难,其中1例合并气胸,1例合并气胸及乳糜胸,1例合并肺外淋巴管肌瘤.结合文献资料,本病常发于育龄期女性,临床表现依次为呼吸困难、咯血、气胸、乳糜胸等.本病X线片常呈非特异改变,CT较具特异性,主要表现为多发均匀分布囊状影,伴有间隔线,呈网格状改变,同时出现液气胸和淋巴结肿大,肺外也可有多发相关改变.肺功能测定常伴有阻塞性通气功能障碍.结论 CT检查对PLAM具有诊断价值.对育龄期妇女发生的渐进性呼吸困难、咯血、自发性气胸应及时进行胸部CT检查,并应常规进行腹部和盆腔影像学检查以了解患者是否合并肺外淋巴管平滑肌瘤.【期刊名称】《临床肺科杂志》【年(卷),期】2010(015)012【总页数】3页(P1704-1706)【关键词】肺淋巴管肌瘤病;CT;影像学诊断【作者】张莉;欧陕兴;彭光明;郭元星;齐燕;李小荣;刘海凌;罗道首【作者单位】510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科;510010,广东,广州,广州军区广州总医院放射科【正文语种】中文【中图分类】R73淋巴管肌瘤病(Lymphangioleiomyomatosis,LAM)是一种主要累及肺、纵隔及腹部淋巴结的罕见综合征。
本病的CT表现具有特征性改变,尤其是胸部影像学改变较特异。
肺淋巴管肌瘤病的影像学诊断目的:分析肺淋巴管肌瘤病的影像学表现的特点,讨论其诊断和鉴别诊断。
方法:对4 例经病理证实的肺淋巴管肌瘤病影像学资料进行回顾性分析。
所有病例均行X线胸片、胸部常规CT 及HRCT 扫描。
结果:X线缺乏特异性,常规胸部CT见两肺密度减低影及少许囊状影,相应水平上HRCT清晰显示全肺囊状影,无分布差异。
结论:常规CT可显示肺淋巴管肌瘤病部分肺部改变,而HRCT能更全面显示病变细微结构,对该病的早期诊断、鉴别诊断具有重要价值,同时对病变的进展及患者预后评估具有重要的参考价值。
标签:肺淋巴管肌瘤病;影像诊断肺淋巴管肌瘤病(PLAM)是一种发生于年轻女性的罕见疾病, 1937年由V on Stossel 首先报道,1966年由Cornog和Enterline正式命名。
病因不明,大多数学者认为与雌激素有关,常易误诊为慢性支气管炎、肺气肿而延误治疗。
本文通过对4 例经病理证实的PLAM的X线、CT及HRCT影像表现进行分析,讨论其诊断及鉴别诊断。
1 资料与方法收集4例经纤维支气管镜肺活检病理证实的PLAM患者,均为女性,年龄24~45岁,4例患者均行X线胸片、肺常规CT和HRCT检查。
临床表现有活动后胸闷、气促者2例,反复发作气胸1例,乳糜胸腔积液1例。
4例肺功能检查均表现为严重阻塞性通气功能障碍。
2 结果X线胸片显示1例表现气胸,双肺被压缩约40%,该患者为24岁女性,病理取小块肺组织约 4.0 cm×1.0 cm×0.2 cm,切面未见特殊,酶标示:ER(-),PR 70%(+),D2-40(+),HMB-45(20%+),SMA(+++),ki-67(-),DES(+),CK7肺泡上皮(+),PCNA(80%+),MSA(+),SPA肺泡上皮(+),CD34血管(+),A103(-);另外1例表现为肺纹理粗乱并双侧胸腔积液,经穿刺抽出液体,化验为真性乳糜液;其余2例显示肺纹理增多。
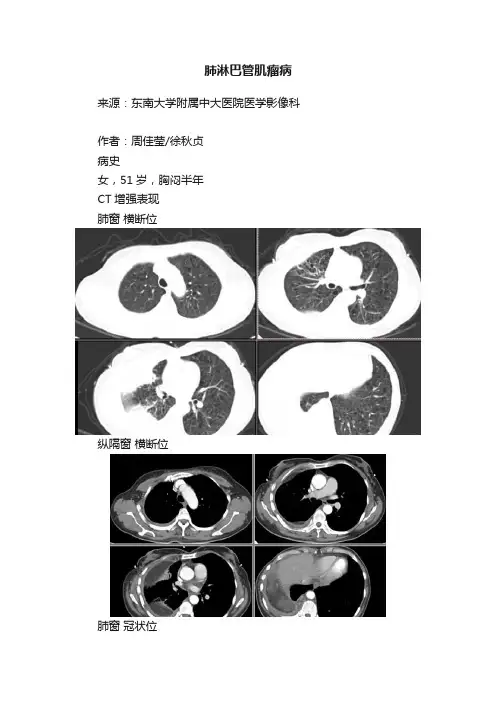
肺淋巴管肌瘤病来源:东南大学附属中大医院医学影像科作者:周佳莹/徐秋贞病史女,51岁,胸闷半年CT增强表现肺窗横断位纵隔窗横断位肺窗冠状位纵隔窗冠状位诊断结果示:肺淋巴管肌瘤病,右侧胸腔乳糜胸肺淋巴管肌瘤病:4、淋巴细胞间质性肺炎(LIP)最常见与Sjogren综合征(干燥综合征)相关,也可与AIDS、原发胆汁性肝硬化、淋巴结增生症及自身免疫性甲状腺疾病。
病理显示淋巴细胞及浆细胞弥散性间质性增殖,淋巴管周围间质包括支气管血管周围间质、小叶间隔及胸膜均受累。
HRCT显示磨玻璃样密度,边界不清的小叶中心结节,基底部的薄壁囊泡,囊泡一般小于3cm,数量少于淋巴管肌腺症及LCH。
HRCT 还可显示支气管血管周围间质、小叶间隔增厚,胸膜下结节,淋巴结肿大并融合。
图1示:干燥综合征伴LIP患者,HRCT示大小不等薄壁囊泡,部分位于胸膜下(小于3cm)。
图2示:LIP患者,HRCT示支气管血管旁间质、小叶间隔增厚,胸膜下结节及融合;此患者囊泡较小(箭头)5、Birt-Hogg-Dubé́综合征常染色体显性遗传疾病;常见30-50岁;皮肤,分布在面部、颈部、上部躯干的纤维毛囊瘤或丘疹, ;肾脏肿瘤(囊肿、良性、恶性);结肠息肉;视网膜疾病;大泡性肺气肿;小的薄壁囊泡,边缘为正常肺组织,囊泡以分布于基底部、胸膜下为特征,面积小于30%肺体积,囊泡内可有小分隔;75% 患者中出现气胸。
参考文献:[1] Danielle M. S, Cristopher A. M,Matthew D. G,Francis X. M. Diffuse Cystic Lung Disease at High-Resolution CT. AJR 2011; 196:1305–1311.[2] Sanghoon Park, Eun Joo Lee.Diagnosis and treatment of cystic lung disease.Korean J Intern Med 2017;32:229-238.[3] Nilo A. A,Andrew J. ,Antoinette Rabel,Joel Moss.Sporadic Lymphangioleio- myomatosis and Tuberous Sclerosis Complex with Lymphangioleiomyomatosis: Comparison of CT Features. Radiology 2007;242: 277-285.[4]徐文帅,徐凯峰.淋巴管肌瘤病诊疗进展. Int J Respir,April 2016;36:620-623.。
肺淋巴管平滑肌瘤病诊断标准
肺淋巴管平滑肌瘤病(LAM)是一种罕见的肺部疾病,主要影响女性,且常伴随肾脏淋巴管平滑肌瘤病出现。
目前尚无特效治疗方法,但有临床实践指导LAM
的管理和治疗。
那么,如何确诊肺淋巴管平滑肌瘤病呢?
1、临床表现
肺淋巴管平滑肌瘤病的症状包括呼吸困难、咳嗽、胸痛等。
由于这些症状与其
他许多呼吸系统疾病相似,LAM的诊断通常需要进一步的检查来确认。
2、影像检查
肺部CT扫描可以显示肺部的异常情况,如囊肿、肺泡扩张、肺实变等。
在LAM患者中,肺囊肿是最常见的表现形式。
3、肺功能测试
LAM病变常会引起肺功能下降,因此肺功能测试也是诊断LAM的重要手段。
这些测试包括肺活量测试、气流限制测试等。
4、生物标记物
除了影像检查和肺功能测试,分析血液、尿液和呼出气等生物标本,可以有助
于LAM的诊断。
例如,血液中的VEGF-D浓度在LAM患者中通常较高。
5、切片检查
最终确诊肺淋巴管平滑肌瘤病的方法是通过活检或手术获取肺部组织进行显微
镜下的观察。
在LAM患者中,通常能看到在肺泡和囊肿中的典型肌肉母细胞增生。
由于这种检查涉及到手术或穿刺等操作,对患者的谨慎和保护相当重要。
总的来说,使用多种手段综合分析可以更准确和快速地诊断出肺淋巴管平滑肌瘤病。
对LAM患者及时诊断会有助于选择适合的治疗方法,有助于改善生活质量和预后。
肺淋巴管肌瘤病诊断标准
肺淋巴管肌瘤病是一种罕见的肺部疾病,其诊断标准主要包括以下几个方面:
1.临床表现:肺淋巴管肌瘤病患者在幼年或年轻时发病,主要表现为呼吸困难、气促、咳嗽等症状。
随着病情的发展,患者可能会出现胸痛、咯血、体重减轻等症状。
2.X线胸片或CT扫描:X线胸片或CT扫描是诊断肺淋巴管肌瘤病的重要手段。
其典型表现为两肺弥漫性囊性病变,呈蜂窝状或网格状改变。
这些病变以中、下肺叶近肺门部密度较高,总的病变范围不超过全肺的1/3。
3.肺功能检查:肺功能检查可显示限制性或混合性通气功能障碍,表现为肺活量减低,肺顺应性降低,残气量降低,功能残气量增高。
随着病情的发展,患者可能会出现弥散障碍和低氧血症。
4.病理学检查:经支气管镜或胸腔镜取病变组织进行病理检查,可发现特征性的平滑肌细胞增生和胶原沉积,即可诊断为肺淋巴管肌瘤病。
5.其他辅助检查:如血气分析、肺活检等,也可有助于诊断。
综合以上几个方面的表现,即可对肺淋巴管肌瘤病进行诊断。
需要注意的是,该病是一种罕见病,诊断可能需要多家医院会诊,并结合临床病史、影像学和病理学检查结果进行综合判断。
肺淋巴管腺肌瘤病的高分辨率CT诊断
卢跃忠;葛宇曦
【期刊名称】《医学影像学杂志》
【年(卷),期】2015(025)010
【摘要】目的探讨12例肺淋巴管腺肌瘤病的HRCT表现,并随访其中5例CT表现,以提高对该病的诊断及认识.方法回顾性分析12例经病理证实的肺淋巴管腺肌瘤病患者的HRCT资料,观察并总结其囊变特征;并随访其中5例患者的CT表现及发展预后.结果 12例病例HRCT均表现为两肺弥漫分布大小不等薄壁囊状影,直径约1~84mm,壁厚2mm以下;9例小叶间隔增厚,3例磨玻璃结节影,3例发现气胸,4例发现胸腔积液;5例CT随访患者均发现的肺实质改变进行性增加.结论HRCT对肺淋巴管腺肌瘤病的诊断及鉴别诊断具有重要价值.
【总页数】5页(P1772-1776)
【作者】卢跃忠;葛宇曦
【作者单位】浙江省湖州市长兴县人民医院放射科浙江湖州 313100;江南大学附属医院影像科江苏无锡214062
【正文语种】中文
【中图分类】R734.2;R814.42
【相关文献】
1.肺癌性淋巴管炎的高分辨率CT诊断价值 [J], 韦红星;梁晟伟
2.肺淋巴管肌瘤病的高分辨率CT诊断 [J], 高军
3.肺淋巴管肌瘤病的高分辨率CT诊断 [J], 冯骏;邱君澜;周科峰;张雪斌;程乐
4.高分辨率CT诊断肺淋巴管肌瘤病八例分析 [J], 李丰才;李至
5.肺淋巴管肌瘤病的高分辨率CT诊断价值 [J], 张定;周子和;刘国庆;韩波;周楠凯因版权原因,仅展示原文概要,查看原文内容请购买。
肺淋巴管平滑肌瘤病高分辨率CT分析
董莱;李慧;王晗琦;管鑫;陈克敏
【期刊名称】《中国医学计算机成像杂志》
【年(卷),期】2024(30)1
【摘要】目的:分析并总结肺淋巴管平滑肌瘤病(PLAM)的高分辨率CT(HRCT)影像特征,探讨胸部HRCT对该病的诊断价值。
方法:回顾性分析50例于上海市黄浦区香山中医医院LAM中医特色专科门诊就诊的PLAM患者的HRCT资料,总结其典型的CT表现,包括弥漫囊样影及不同表现的肺间质病变等。
结果:50例确诊的PLAM患者HRCT影像显示双肺弥漫性囊状影及肺间质病变的不同表现,部分病例出现胸腔积液、气胸病史、肺部感染及支气管扩张征象。
结论:胸部HRCT检查所提供的影像学表现在PLAM干预中具有显著价值,可为疾病的后续诊治提供有效依据,提高疾病诊断准确性。
【总页数】6页(P33-38)
【作者】董莱;李慧;王晗琦;管鑫;陈克敏
【作者单位】上海市黄浦区香山中医医院放射科;上海交通大学医学院附属瑞金医院放射科;上海市黄浦区香山中医医院治未病科
【正文语种】中文
【中图分类】R445.3
【相关文献】
1.2例肺淋巴管平滑肌瘤病的X线与CT表现
2.肺淋巴管平滑肌瘤病高分辨率CT 影像学分析
3.肺淋巴管平滑肌瘤病合并胸部结节病的CT表现
4.高分辨率CT诊断肺淋巴管肌瘤病八例分析
因版权原因,仅展示原文概要,查看原文内容请购买。