Some orthogonal very-well-poised $_8varphi_7$-functions that generalize Askey-Wilson polyno
- 格式:pdf
- 大小:293.22 KB
- 文档页数:31

Anti-thyroperoxidase antibodies from patients with Hashimoto'sencephalopathy bind to cerebellar astrocytesStéphanie Blanchin a,⁎,Christine Coffin b ,Fausto Viader c ,Jean Ruf d ,Pierre Carayon d ,Francette Potier a ,Estelle Portier a ,Elisabeth Comby a ,Stéphane Allouche e ,Yann Ollivier f ,Yves Reznik b ,Jean Jacques Ballet aaLaboratoire d ’Immunologie et d ’Immunopathologie,UPRES-EA 2128,CHU Clémenceau,14033Caen cedex,FrancebService d ’Endocrinologie et Maladies Métaboliques,CHU Côte de Nacre,14033Caen cedex,FrancecService de Neurologie,CHU Côte de Nacre,14033Caen cedex,FrancedINSERM U555,Facultéde médecine Timone,Universitéde la Méditerranée,13385,Marseille cedex 5,FranceeLaboratoire de Biochimie,CHU Côte de Nacre,14033Caen cedex,France fService de Médecine Interne,CHU Côte de Nacre,14033Caen cedex,FranceReceived 28June 2007;received in revised form 31July 2007;accepted 6August 2007AbstractA cohort of 10Hashimoto's encephalopathy (HE)patients,33patients with unrelated neurological symptoms,12Hashimoto's thyroiditis patients and 4healthy adult donors was studied to explore the neurological targets of anti-thyroperoxidase (TPO)autoantibodies (aAb)in HE.High levels of anti-TPO aAb were only detected in HE group's cerebrospinal fluids.In immunofluorescence assays on monkey brain cerebellum sections,both HE patients'sera and anti-TPO monoclonal antibodies (mAb)were able to bind cerebellar cells expressing glial fibrillary acid protein.Normal human astrocytes from primary cultures also reacted with anti-TPO mAb.Specific astrocyte binding of anti-TPO aAb suggests a role of these aAb in the HE pathogenesis.©2007Elsevier B.V .All rights reserved.Keywords:Anti-thyroperoxidase antibodies;Astrocytes;Cerebrospinal fluid;Hashimoto's encephalopathy;Hashimoto's thyroiditis1.IntroductionHashimoto's encephalopathy (HE)is a rare,often misdiag-nosed and poorly understood corticosteroid-responsive neuro-logical syndrome occurring in patients with autoimmune thyroid disease (AITD).Since the first description in 1966by Brain et al.(Brain et al.,1966),case reports described heterogeneous clinical manifestations such as psychiatric impairments and neurological disturbances (Kothbauer-Margreiter et al.,1996).The diagnosis was established on the basis of unspecific central nervous dys-function with the presence of serum anti-thyroid autoantibodies (aAb),regardless of the thyroid disorder (Fatourechi,2005).An autoimmune pathogenic link was suggested between HE and AITD based on HE features such as (i)presence of serum anti-thyroid aAb indicating active thyroiditis (Brain et al.,1966),(ii)cerebrospinal fluid (CSF)biochemistry suggesting inflammatory process (Ferracci et al.,2003),(iii)association with other autoimmune diseases such as systemic lupus erythematosus and rheumatoid arthritis (Mulhern et al.,1966),(iv)sex ratio and age distribution similar to AITD (Chaudhuri and Behan,2003;Sawka et al.,2002),(v)the improvement of symptoms after corticoste-roid therapy (Chong et al.,2003),and (vi)presence of serum aAb against neuronal alpha-enolase (Fujii et al.,2005;Ochi et al.,2002;Yoneda et al.,2007)and an unidentified 36kDa autoantigen (Oide et al.,2004).HE is also characterized by an increase in the CSF anti-thyroid,especially anti-thyroperoxidase (TPO)aAb levels (Ferracci et al.,2003)which was proposed as a valuable marker of diagnosis (Ferracci et al.,2004).The main thyroid autoantigens,TPO and thyroglobulin (Tg),are the enzyme-substrate pair involved in thyroid hormone production (Ruf and Carayon,2006).TPO is a 933-amino-acidJournal of Neuroimmunology 192(2007)13–20/locate/jneuroim⁎Corresponding author.Tel.:+33231272551;fax:+33231272550.E-mail address:blanchin-s@chu-caen.fr (S.Blanchin).0165-5728/$-see front matter ©2007Elsevier B.V .All rights reserved.doi:10.1016/j.jneuroim.2007.08.012long,type I integral membrane protein,which carries out the iodination and the intramolecular coupling of tyrosine residues of Tg to form thyroid hormones.Human(Chazenbalk et al., 1993)and murine(Ruf et al.,1989)monoclonal antibodies (mAb)have been used for characterization of the TPO immuno-dominant region(IDR).The aim of the present study was to assess the reactivity of anti-TPO aAb from HE patients with central nervous system (CNS)tissues.In immunofluorescence assays,both HE patient serum anti-TPO aAb and murine anti-TPO mAb were bound to astrocytic cells.2.Materials and methods2.1.HE patients and control subjectsSera and CSF from10HE patients admitted between January 1999and April2006to the neurological ward of Caen University Hospital were collected and kept at−80°C until used.Diagnosis was based on the neurological clinical manifestations and the presence of anti-Tg and-TPO aAb in the serum and CSF in the absence of other central neurological conditions.Serum and CSF samples were also obtained from a panel of33control patients who were referred to the emergency ward with meningitis(15), intractable headache(8),peripheral neuropathy(4),multiple sclerosis(6).They were free of AITD except two who were diagnosed with an Hashimoto's thyroiditis(HT)(serum anti-TPO aAb:80and100IU/mL,normal values:b25IU/mL).Sera from 12patients with a documented HTand serum anti-TPO aAb levels ranging from90to N200IU/mL were obtained from experienced endocrinologists.Normal sera were generous gifts from4healthy adult volunteers without AITD or CNS disease.Sera from HE patients and healthy control donors were tested for the presence of anti-nuclear aAb as described(Comby et al.,2006)and of anti-onconeuronal aAb(anti-Ri,-Hu,-Yo,-CV2,-amphiphysin,-Ma2 assays,Euroimmun GmbH,Gross Grönau,Germany,and Ravo Diagnostika GmbH,Freiburg,Germany)according to the manufacturers'instructions.The procedures used in this study were approved by the local institutional review committee,and informed consent was ob-tained from all donors.2.2.ELISA for the detection of serum and CSF anti-thyroid aAbWells of microtiter plates(Dynatech Laboratories Inc., Chantilly,V A)were coated with phosphate-buffered saline (PBS),pH7.4,containing300ng human TPO(Biodesign Inter-national,Saco,ME)or1000ng human Tg(Valbiotech,Paris, France).After being incubated overnight at4°C,the wells were saturated with1%bovine serum albumin(BSA;Laboratoires Eurobio,Courtaboeuf,France)in PBS.They were then incubated with1/800serum dilution for anti-TPO aAb,1/400serum dilution for anti-Tg aAb or1/5dilution for CSF samples in PBS,1%BSA with0.05%Tween20for1h30min at37°C.A calibration curve was drawn up using World Health Organization standards (NIBSC Codes:66/387and65/93for anti-TPO and-Tg aAb,respectively)and the BP114as substandard plasma(The Binding Site,Saint Egreve,France).After a washing step,the anti-Tg and -TPO aAb levels were both determined using alkaline phospha-tase-coupled goat antibodies to human IgG(P.A.R.I.S,Com-piègne,France)and p-nitrophenyl phosphate(Interchim, Montluçon,France)as substrate.Optical density(OD)was read at405nm using a Bio-Tek Elx808microplate reader(Bio-Tek Instruments Inc,Winooski,VT).Results were expressed as means of duplicate measurements in IU/mL in the case of sera and OD [ΔOD405nm=(OD405nm of coated wells)minus(OD405nm of uncoated wells)]in that of CSF.For18sera from healthy adult volunteers,threshold values for both anti-TPO and-Tg aAb was 25IU/ml,determined as mean values plus3SD from the mean.2.3.Depletion of HE patients’sera in anti-TPO aAbAnti-TPO aAb in sera of HE patients were depleted by performing affinity chromatography(Ruf et al.,1992).Briefly, 10mg of purified human TPO was coupled to25mL Affi-Gel15 (Bio-Rad,Marnes la Coquette,France).After extensive PBS washing,patients’sera were incubated overnight with the coupled gel at4°C under shaking.Unbound material was then checked by ELISA to ensure that it contained no anti-thyroid aAb.2.4.Primary normal human astrocyte cell culturesNormal primary human astrocytes derived from the whole brain of one donor,18weeks old fetus,(Cambrex Bio Science, Verviers,Belgium)were grown on coverslips in Astrocyte Basal Medium supplemented with the Astrocyte Growth Medium SingleQuots(Cambrex Bio Science).2.5.Immunofluorescence assaysStaining was performed on cerebrum,cerebellum and thy-roid tissue sections from Macaccus rhesus monkeys(The Binding Site)and normal human astrocyte coverslips.Human astrocytes were fixed and permeabilized in100%acetone.After BSA saturation,tissues and astrocytes were incubated for1h with HE patients’sera(1/15dilution),HE patients’sera devoid of anti-TPO aAb(1/15dilution),HT patients’sera and normal sera(1/15dilution),4murine anti-TPO mAb directed towards TPO IDR:mAb47,60,15and9(Ruf et al.,1989)and1murine anti-Tg mAb:mAbJ7C9.3(Ruf et al.,1983)(1/300dilution) and with anti-glial fibrillary acid protein(GFAP)mAb(1/1000 dilution;Sigma-Aldrich,Saint Quentin Fallavier,France)in PBS,3%BSA.Dilutions of sera and antibodies yielding optimal signal/background fluorescence were experimentally determined by serial tests.Staining patterns were revealed with rhodamine or FITC coupled goat antibodies against mouse IgG (Jackson ImmunoResearch Laboratories,West Grove,PA)or FITC coupled goat antibodies against human IgG(Euroimmun GmbH)for1h.Sections were then mounted with Vectashield-DAPI(Vector Laboratories,Peterborough,UK)and viewed using an Axioskop2Plus fluorescence microscope(Carl Zeiss Vision GmbH,Munchen,Germany)with a40×oil immersion lens.Pictures were acquired with an AxioCam HRC digital14S.Blanchin et al./Journal of Neuroimmunology192(2007)13–20camera equipped with an AxioVision 3.2software program.The Photoshop software program (version 6;Adobe System Inc.,San Jose,CA)was used to superimpose the pictures for colocalization viewing.2.6.SDS-PAGE and western blot analysisTwo μg of purified human TPO were incubated in Laemmli sample buffer and loaded onto 7.5%acrylamide gels.Proteins were either stained with Coomassie brilliant blue or electro-transferred onto a nitrocellulose sheet (Amersham Biosciences,Buckinghamshire,UK)for western blotting.After BSA satura-tion,the blotted membranes were incubated overnight at 4°C with HE patients'sera (1/100dilution)or mAb47(1/300dilu-tion)in PBS,0.05%Tween 20.Membranes were then incubated with alkaline phosphatase-labeled goat antibodies against human IgG or rabbit antibodies against mouse IgG (Rockland Immunochemicals for research,Gilbertsville,PA)for 2h.Finally,a revelation step was performed using 5-bromo-4-chloro-3-indolyl phosphate/nitro blue tetrazolium as the appro-priate substrate (Sigma-Aldrich).2.7.Statistical analysisResults are expressed as means ±1SD.Significance was determined using unpaired t -tests or one-way ANOVA with Dunnett's post test.Linear correlations were evaluated using R values.Significance levels were set at p b 0.01.3.Results3.1.Clinical and biological characteristics of HE patients The HE cohort consists of 1man and 9women.Their ages ranged from 25to 85(mean:53years)at the onset of the disease.The autoimmune thyroid disorders were HT for 8patients and Graves'disease (GD)with anti-TPO aAb for 2patients.Clinical data are presented in Table 1according to major criteria from Chaudhuri and Behan (2003)and Ferracci et al.(2004).The clinical manifestations included impaired consciousness,tremor,cephalalgia,coma,seizure,paraparesis,hemiparesis,confusion,ataxia,memory loss,myoclonus,apraxia and aphasia.Neither dementia nor behavioural disturbance was observed.In 4patients,non-migraine-type cephalalgia was initially recorded as a prominent symptom,and resolved within 2months in one while persisting for over 6months in the three others.Abnormal electroencephalography (EEG)tracing changes were observed in 3/10patients with diffuse intermittent runs of synchronous sharp waves.Brain magnetic resonance imaging (MRI)was performed in 7/10patients with normal imaging in all subjects except one with unspecific hyperintense spots in the white matter.One day to 4months after initial manifestations,9/10patients underwent a corticosteroid trial (prednisone equivalent:1mg/kg/day)during a minimum period of 6months.One patient (no.2)remained in spontaneous remission for at least 2years and did not receive corticosteroid therapy.Two months after initiation of therapy,symptoms were present in 5/9treated patients and absent in 4/9.Table 1Clinical features of HE patients Patient no.12345678910Sex F F F F F F F F F M Age51413545858457552553Thyroid disorderHT HT HT HT HT HT GD HT GD HT SymptomsImpaired consciousness +−−++++−++Tremor ++++++++++Cephalalgia−−++−−−++−Migraine-type headache −−−−−−−−−−Coma −−−−−−−−+−Seizure −−+−−−−−+−Paraparesis −−+−−−−−−−Hemiparesis +−+−−−−−−−Confusion −−−++++−++Ataxia+++−−−−++−Memory loss +−−−−−−+−+Myoclonus −−−+−−−−++Apraxia −+−−−−−−−−Aphasia−+−−−−−+++Focal neurological deficit −−−−−−−−−−EEG Normal Diffuse abn Normal Normal Normal Normal Normal Normal Diffuse abn Diffuse abn MRINA Normal Normal Hypersignal NA Normal Normal Normal NA Normal Corticosteroid therapy +−++++++++Evolution at 6monthsCR CR CD CR Death CD CD CR CD CR Persisting symptoms at 6months/12months−/−−/−+/−+/−+/NA−/NA+/NA+/−+/+−/−F:female,M:male,HT:Hashimoto's thyroiditis,GD:Graves ’disease,+:presence,−:absence,abn:abnormalities,NA:not available,CR:complete remission,CD:corticodependence.15S.Blanchin et al./Journal of Neuroimmunology 192(2007)13–20At6months,steroid therapy was discontinued in8/9patients. From6months to12months,corticodependence was observed in 4/9patients(no.3,6,7,9).All9steroid-treated patients were clinically improved.At12months,1(no.9)was symptomatic under therapy,5(no.1,3,4,8,10)were asymptomatic after cessation of therapy and2(no.6,7)were under therapy with a follow-up limited to7months.One patient(no.5)had died of an unrelated condition.From12months,therapy was continued in only1/10patient(no.9).All10HE patients exhibited high levels (N50IU/mL)of anti-TPO or-Tg aAb in their sera,or both (Table2).Nine HE patients were evaluated for CSF protein concentration and IgG index which were within normal or near normal ranges(Table2).No serum antibodies against nuclear and onconeuronal antigens were found in HE patients nor healthy donors(data not shown).3.2.High frequency of anti-TPO aAb in CSF from HE patientsThirty three CSF control samples corresponding to diverse CNS diseases with or without HT(2patients)status were quantified for their respective anti-TPO and-Tg aAb level.All these CSF exhibited lowest levels of anti-TPO and-Tg aAb which were used to determine threshold values.These values expressed inΔOD405nm(meanΔOD405nm+2SD),were set at0.228for anti-TPO aAb and0.115for anti-Tg aAb.High levels of anti-TPO (ΔOD N0.228)and-Tg(ΔOD N0.115)aAb were detected in all the HE patients'CSF(p b0.01;Fig.1).No correlation was found between serum and CSF levels of anti-TPO and-Tg aAb or between the respective anti-Tg and-TPO aAb levels.3.3.Serum anti-TPO autoantibody titer follow-up after initiation of corticosteroid therapyIn6HE patients(no.1,2,3,4,9,10),serum anti-TPO aAb levels were evaluated2and12months after initiation of corticosteroid therapy(Fig.2).Four out of6exhibited decreased anti-TPO aAb levels after2months(p b0.01),and in3,antibody titers fell below the threshold anti-TPO aAb value (b25IU/mL)after12months.Interestingly,no alteration of anti-TPO aAb(N200IU/mL)was noted in one HE patient(no.9)after a5-year therapy(data not shown).3.4.Anti-TPO aAb and mAb recognize the same TPO isoformsTo determine the specificity of anti-TPO aAb from HE patients’sera,a western blotting assay was performed on affinity-purified human TPO.TPO at100kDa was detected by performing Coomassie brilliant blue staining(Fig.3,A2).In western blotting assays,anti-TPO mAb47,reacted with the2 main isoforms forming the characteristic TPO doublet around 100kDa(Fig.3,B2).Both TPO isoforms were recognized by sera from the10HE patients as shown in Fig.3,C2which depicts the typical reactivity of the HE patient's no.9serum.3.5.Anti-TPO aAb bind to primate cerebellar tissuesTo investigate more closely the role of anti-TPO aAb in CNS abnormalities,indirect immunofluorescence assays with10HE patients,12HT patients and4healthy donors’sera were performed on CNS and thyroid tissues from M.rhesus.Fig.4A depicts the typical reactivity of one of HE patients'sera(no.9), the same serum depleted from anti-TPO aAb,one HT patient serum(anti-TPO aAb N200IU/mL)and normal serum on cerebellum and thyroid tissues.The anti-TPO aAb reactivity of all sera were first evaluated by specific staining of the thyroidTable2Biological features of HE patientsPatient no.12345678910CSF proteins(NR:0.15–0.45g/L)NA0.420.360.28NA0.35NA0.56NA0.69 IgG index(NR b0.7)NA0.58NA0.580.45NA NA0.47NA0.66 Serum anti-Tg aAb(NR b25IU/mL)17844N300225N30065150N30020041 Serum anti-TPO aAb(NR b25IU/mL)25150N20060N200N20080N200N200170 CSF anti-Tg aAb(ΔOD405nm b0.115)NA0.20 1.500.50 1.500.250.31 2.25 1.470.14 CSF anti-TPO aAb(ΔOD405nm b0.228)NA 3.49 2.320.280.78 2.670.75 4.03 3.91 1.89CSF:cerebrospinal fluid,NA:not available,NR:normal range,aAb:autoantibodies,Tg:thyroglobulin,TPO:thyroperoxidase,ΔOD405nm:optical densities at 405nm.Fig.1.Anti-TPO and-Tg aAb in CSF from HE patients.CSF from9HE patientswas analysed by ELISA to determine the anti-TPO(A,white bars)and-Tg(B,blackbars)aAb levels.Results were expressed as the meanΔOD405nm value±1SD(error bars).Dotted lines give threshold values for anti-TPO and-Tg aAb.16S.Blanchin et al./Journal of Neuroimmunology192(2007)13–20cell membrane (Fig.4,A6).The 10sera from HE patients (Fig.4,A1)but not the 12from HT patients (Fig.4,A3)or the 4from healthy subjects (Fig.4,A4)bound to structures in primate cerebellar tissues.After the depletion procedure which removed more than 90%of anti-TPO aAb but not anti-Tg aAb (Fig.4D and data not shown),the serum did not bind significantly to either thyroid cells or cerebellar cells (Fig.4,A2and A7).As the HE patients'sera contained anti-TPO and -Tg aAb,immuno-fluorescence assays were also performed with mAb directed against human TPO or Tg (Fig.4,B and C)to confirm the specificity of cerebellar staining.Four mAb characteristic of the TPO IDR (mAb47,60,15,9)and one directed toward human Tg (J7C9.3)were selected.The 4anti-TPO mAb all showed a similar reactivity pattern as seen with HE patients'sera on primate cerebellar cells (Fig.4B).Stained cells were mostly located in the subcortical cerebellar white matter,near the granular cell layer.No staining of cerebellar neuronal cells,including granular and Purkinje cells,was observed.The anti-Tg mAbJ7C9.3did not bind to cerebellar tissues (Fig.4,C1).None of the above sera and mAb bound to primate cerebrum tissues (data not shown).These results further suggest that the sole anti-TPO aAb electively recognize primate cerebellum structures.3.6.Reactivity of anti-TPO antibodies to GF AP-expressing astrocytic cellsTo identify further the cerebellar cell type(s)reacting with anti-TPO aAb,a double immunofluorescence assay with HE patients'sera and anti-GFAP mAb was performed on cerebellar tissues (Fig.5).Anti-TPO aAb from 2HE patients'sera (no.2and no.3)bound to GFAP-positive astrocytic cells.Similarly,the anti-TPO mAb47stained strongly at the membrane (Fig.5,D)of normal human astrocyte primary cell cultures expressing GFAP (Fig.5,E).These data therefore indicate that anti-TPO aAb from HE patients and anti-TPO mAb both bind to astrocytes.4.DiscussionPresent data suggest that anti-TPO and/or -Tg aAb are present in the CSF of HE patients and that their serum anti-TPO aAb bind cells of astrocyte lineage.A sensitive ELISA was performed to detect CSF anti-thyroid aAb in two groups,i.e.9HE patients and 33control adults with other neurological conditions.In accordance with the HE cases already reported in the literature (Chong et al.,2003),2GD patients with subclinical or overt hyperthyroidism were included.In the HE patients,anti-TPO and/or anti-Tg aAb were detected at variable levels in sera and significant levels in CSF,consistent with previous reports (Castillo et al.,2006;Ferracci et al.,2003).Their absence in the 33control patients including 2patients with HT suggests that this finding was restricted to HE and thus may provide a clue for early HE S inflammation was not documented since normal or near normal range CSF protein concentrations and IgG indices,and normal or unspecific brain MRI and EEG patterns were found.There is no evidence to conclude between either local antibody synthesis or blood brain barrier passage which is suggested in patients no.4and no.7with lowest serum and CSF aAb levels.Anti-TPO aAb in the CNS of HE patients might contribute to CNS pathology by interacting with CNS tissues,although not excluding a role for some other pathogenic antibodies.A role of aAb is further suggested by the marked clinicalimprovementFig.2.Time course study of serum anti-TPO aAb level in HE patients.Serum anti-TPO aAb levels (IU/ml)were sequentially determined in 6HE patients (no.1,2,3,4,9and 10)for 2to 12months after the onset of corticosteroid therapy.Results were expressed as mean values of triplicated experiments.Standard deviations from all means were lower than 10%of the mean.Threshold value for normal sera (25IU/mL)as described in the Materials and methodssection.Fig.3.Reactivity of anti-TPO aAb from HE patients and anti-TPO mAb with purified human TPO.Purified human TPO samples were run on SDS-PAGE gel and proteins were either directly stained with Coomassie brillant blue (A,2)or electrotransferred onto a nitrocellulose membrane and revealed in western blotting experiments using either anti-TPO mAb47(B,2)or HE patient's no.9serum (C,2).The molecular weights of the standards (column 1)are indicated in kDa on the left.Data shown are of a representative experiment.17S.Blanchin et al./Journal of Neuroimmunology 192(2007)13–20seen in 9HE patients following corticosteroid therapy which paralleled in 4/6the decrease in anti-TPO aAb level.A pathogenic role for anti-TPO aAb was also previously suspected in other conditions such as decreased intelligence quotient scores in children from mothers with high levels anti-TPO aAb and normal thyroid function during pregnancy (Pop et al.,1995)and the predisposition to depression found directly correlated with anti-TPO aAb levels (Pop et al.,1998).The complement-mediated thyrocyte cytotoxicity of anti-TPO aAb from AITD patients was found inhibited by human TPO and absent in patients with other autoimmune diseases such as lupus erythematosus and glomerulonephritis (Wa deleux et al.,1989).Antibody-dependent cell cytotoxicity against thyrocytes was dependent on anti-TPO and not anti-Tg aAb (R odien et al.,1996).A human chimeric anti-TPO Fab-dependent cell cyto-toxicity on human thyroid cells was exerted by peripheral blood mononuclear cells (Guo et al.,1997).Due to limited CSF concentrations of anti-TPO aAb,serum anti-TPO aAb and a panel of murine anti-TPO mAb cross-reacting with HT and GD patients'sera (Ruf et al.,1989),were preferentially used for investigating further their interactions with neurological cells.Indirect immunofluorescenceexperimentsFig.4.Reactivity of anti-TPO aAb from HE patients'sera and anti-TPO mAb to primate cerebellum and thyroid tissues.Immunofluorescent stainings of human sera (A),anti-TPO mAb (B)and anti-Tg mAb (C)were performed on monkey cerebellum (A1–A5,B1–B5,C1–C2)and thyroid (A6–A10,B6–B10,C3–C4)tissues (original magnification ×400).Used antibodies are the following:one typical HE patient serum (no.9;A1,A6),the depleted HE patient no.9serum (A2,A7),one HT patient serum (A3,A8),one healthy individual serum (A4,A9),anti-TPO mAb47(B1,B6),60(B2,B7),15(B3,B8),9(B4,B9)and anti-Tg mAbJ7C9.3(C1,C4).Nucleus DAPI staining is shown in blue.Slides A-5/10,B-5/10and C-2/4exhibit non-specific binding for each tissue when no first antibody was added.Panel D depicts the results of a representative experiment where the HE patient no.9serum were depleted from anti-TPO aAb.Results are expressed as the binding rate to coated human TPO±1SD (error bars).18S.Blanchin et al./Journal of Neuroimmunology 192(2007)13–20exhibited specific staining of cerebellar cells from M.rhesus monkeys while none using HT patients'and healthy donors'sera.The reactivity of HE aAb with TPO epitopes was ascertained by the similar binding pattern of 4anti-TPO mAb on the same cells and confirmed in western blotting experiments showing that HE patients'sera and mAb47,an anti-TPO IDR mAb bound the same TPO isoforms forming a doublet around 100kDa (Ruf and Carayon,2006).Anti-TPO aAb depletion from HE patients'sera confirmed that the anti-TPO aAb bound solely to CNS structures.Furthermore,no cerebellar binding was detected with anti-Tg mAbJ7C9.3,which do not cross-react with anti-TPO aAb (Ruf et al.,1992).Serum aAb from HT patients did not bind cerebellar tissue consistent with differences in anti-TPO aAb repertoire between HT and HE patients.Localization of the stained cells in the subcortical cerebellar white matter and their typical star-shaped morphology were consistent with their astrocytic lineage.In double immunostaining experiments,binding of anti-TPO aAb from HE patients was colocalized with GFAP,an astrocytic marker.This was further supported by binding of the anti-TPO mAb47to normal human astrocytes in primary cultures.In-terestingly,a strong relationship between HTand cerebellar ataxia was reported (Selim and Drachman,2001).Moreover,mild astrocytic gliosis and microglial activation were previously mentioned in reports based on brain biopsies from HE patients (Castillo et al.,2006;Nolte et al.,2000).An involvement of astrocytes was noted in other CNS dysfunctions such as epilepsy and Alzheimer's disease (Blasko et al.,2004;Schipper,1996).Cephalalgia observed in several of the present HE patients may reveal astrocyte-related spreading depression (Chuquet et al.,2007).That aAb trigger neuropathic mechanisms has been previ-ously documented for anti-glutamic acid decarboxylase aAb and anti-calcium channel aAb in patients with the Stiff-personsyndrome (Dalakas et al.,2000)and the Lambert –Eaton myasthenic syndrome,respectively (Rosenfeld et al.,1993).In the present study,presence of serum and CSF anti-TPO aAb,binding of anti-TPO aAb on astrocytic cells,and improvement of the clinical symptoms after reducing the level of serum anti-TPO aAb partially meet the criteria for demonstrating patho-genicity of aAb (Sutton and Winer,2002).Although not excluding the role of other neuropathogenic antibody(ies)in HE,present data prompt identification of the astrocytic anti-genic target(s)of HE anti-TPO aAb.Experimental animal studies are needed to investigate whether passive anti-TPO aAb transfer reproduces the main features of the disease and im-munization with the putative antigen(s)leads to an animal model of the disease providing clues how neurological func-tions are impaired.AcknowledgmentsThis research was supported by a grant from the french ministère de la santéet de la protection sociale,programme hos-pitalier G42006:“Lymphocytes B et ses effecteurs normaux et pathologiques ”.We thank Dr.Benoit Dupuy and Dr.Nizam Kassis,hôpital Louis Pasteur Cherbourg,for providing sera and CSF from HE patient.The authors are also grateful to Pr.Françoise Chapon,laboratoire de neuropathologie CHU Caen,for helpful advices.ReferencesBlasko,I.,Stampfer-Kountchev,M.,Robatscher,P.,Veerhuis,R.,Eikelenboom,P.,Grubeck-Loebenstein,B.,2004.How chronic inflammation can affect the brain and support the development of Alzheimer's disease in old age:the role of microglia and astrocytes.Aging Cell 3,169–176.Brain,L.,Jellinek,E.H.,Ball,K.,1966.Hashimoto's disease and ncet 2,512–514.Fig.5.Immunoreactivity of anti-TPO aAb and mAb47to GFAP-specific astrocytic cells.Immunofluorescent staining patterns were obtained on monkey cerebellum (A –C)with sera from HE patients no.2and no.3(A –B,in green)and anti-GFAP mAb (A –B,in red)and on normal human astrocyte primary cultures (D –F)with anti-TPO mAb47(D,in red)and anti-GFAP mAb (E,in red).Nuclei are shown in blue.Non-specific binding are shown in slides C and F.(Original magnification ×400).19S.Blanchin et al./Journal of Neuroimmunology 192(2007)13–20。
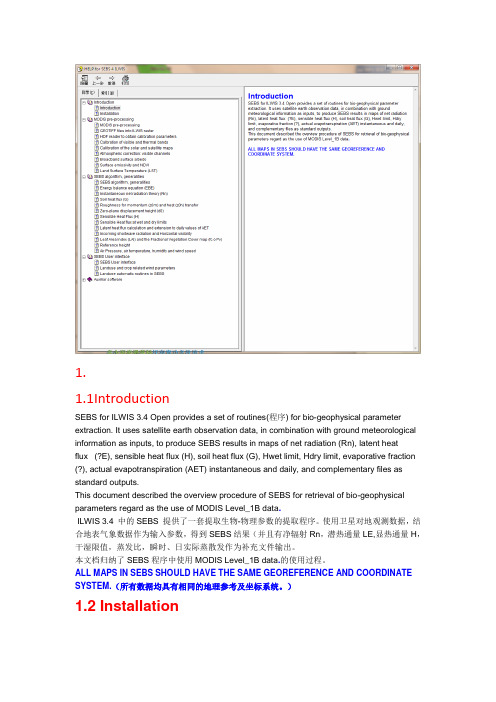
1.1.1IntroductionSEBS for ILWIS 3.4 Open provides a set of routines(程序) for bio-geophysical parameter extraction. It uses satellite earth observation data, in combination with ground meteorological information as inputs, to produce SEBS results in maps of net radiation (Rn), latent heatflux (?E), sensible heat flux (H), soil heat flux (G), Hwet limit, Hdry limit, evaporative fraction (?), actual evapotranspiration (AET) instantaneous and daily, and complementary files as standard outputs.This document described the overview procedure of SEBS for retrieval of bio-geophysical parameters regard as the use of MODIS Level_1B data.ILWIS 3.4 中的SEBS 提供了一套提取生物-物理参数的提取程序。
使用卫星对地观测数据,结合地表气象数据作为输入参数,得到SEBS结果(并且有净辐射Rn,潜热通量LE,显热通量H,干湿限值,蒸发比,瞬时、日实际蒸散发作为补充文件输出。
本文档归纳了SEBS程序中使用MODIS Level_1B data.的使用过程。
ALL MAPS IN SEBS SHOULD HAVE THE SAME GEOREFERENCE AND COORDINATE SYSTEM.(所有数据均具有相同的地理参考及坐标系统。

A role of SMAD4in iron metabolism through the positive regulation of hepcidin expressionRui-Hong Wang,1,5Cuiling Li,1,5Xiaoling Xu,1Yin Zheng,1Cuiying Xiao,1Patricia Zerfas,2Sharon Cooperman,3 Michael Eckhaus,2Tracey Rouault,3Lopa Mishra,4and Chu-Xia Deng1,*1Genetics of Development and Disease Branch,10/9N105,National Institute of Diabetes and Digestive and Kidney Diseases2Division of Veterinary Resources,Office of Research Services3Cell Biology and Metabolism Branch,National Institute of Child Health and Human DevelopmentNational Institutes of Health,Bethesda,Maryland208924Laboratory of Developmental Biology,Department of Medicine and Surgery,Georgetown University,Washington,DC200075These authors have contributed equally to this work.*Correspondence:chuxiad@SummaryHereditary hemochromatosis,characterized by iron overload in multiple organs,is one of the most common genetic disor-ders among Caucasians.Hepcidin,which is synthesized in the liver,plays important roles in iron overload syndromes.Here, we show that a Cre-loxP-mediated liver-specific disruption of SMAD4results in markedly decreased hepcidin expression and accumulation of iron in many organs,which is most pronounced in liver,kidney,and pancreas.Transcript levels of genes involved in intestinal iron absorption,including Dcytb,DMT1,and ferroportin,are significantly elevated in the absence of hepcidin.We demonstrate that ectopic overexpression of SMAD4activates the hepcidin promoter and is associated with epigenetic modification of histone H3to a transcriptionally active form.Moreover,transcriptional activation of hepcidin is abrogated in SMAD4-deficient hepatocytes in response to iron overload,TGF-b,BMP,or IL-6.Our study uncovers a novel role of TGF-b/SMAD4in regulating hepcidin expression and thus intestinal iron transport and iron homeostasis.IntroductionIron is a key component of oxygen-transporting storage mole-cules,such as hemoglobin and myoglobin.Iron deficiency re-sults in anemia,while iron overload leads to tissue damage andfibrosis.Iron overload in multiple organs/tissues is charac-teristic of hereditary hemochromatosis,one of the most com-mon genetic disorders among Caucasians.The majority of pa-tients with hereditary hemochromatosis are homozygous for a unique missense mutation(C282Y)that alters a major histo-compatibility complex class I-like protein(HFE).Recent investi-gations have also revealed a number of forms of nonHFE hered-itary hemochromatosis that are caused by mutations of several other genes,including ferroportin1(FPN1)(Montosi et al.,2001; Njajou et al.,2001),transferrin receptor2(TFR2)(Camaschella et al.,2000),hemojuvelin(HFE2)(Papanikolaou et al.,2004), and hepcidin(HAMP)(Roetto et al.,2003).Recent studies indicated that hepcidin(hepcidin-1in mouse) plays an essential role in regulating iron absorption(Kaplan, 2002;Leong and Lonnerdal,2004).Hepcidin was independently isolated as a circulating antimicrobial peptide from human urine (Park et al.,2001)and serum(Krause et al.,2000).A lack of hep-cidin expression has been associated with iron overload while overexpression of hepcidin results in iron-deficiency anemia in mice(Nicolas et al.,2001,2002).Furthermore,homozygous mu-tations of hepcidin in humans have been found to cause severe juvenile hemochromatosis(Roetto et al.,2003).Prohepcidin is produced predominantly by liver,although a number of other or-gans,such as lung and heart,also express it at much lower lev-els(Leong and Lonnerdal,2004).Once cleaved,the mature form,a25aa peptide,is secreted into the circulation.Hepcidin in plasma negatively regulates iron absorption in duodenal crypt cells and/or villous enterocytes and inhibits iron release from macrophages(Leong and Lonnerdal,2004).In HFE hemochro-matosis,production of hepcidin appears to be abnormally low (Bridle et al.,2003;Gehrke et al.,2003),suggesting that HFE positively regulates hepcidin expression.Additional factors/ conditions,including IL-6,c/EBP a,iron,hypoxia,and inflamma-tion,also regulate hepcidin expression(Courselaud et al.,2002; Nemeth et al.,2004a).Members of the transforming growth factor b(TGF-b)super-family play numerous important functions in diverse develop-mental processes by regulating proliferation,differentiation, and apoptosis(reviewed in Derynck et al.,2001;Pollard,2001; Wakefield et al.,2001).After activating their transmembrane re-ceptors,TGF-b signaling is transduced into the nucleus by SMADs,a family of at least eight members,of which SMAD4 serves as a central mediator(reviewed in Heldin et al.,1997; Massague,1998).SMAD4is a well-known tumor suppressor gene,and SMAD4mutations are frequently detected in pancre-atic cancer,colon cancer,and gastric polyposis and adenocar-cinomas(Friedl et al.,1999;Hahn et al.,1996;Howe et al.,1998; Maesawa et al.,1997;Nagatake et al.,1996;Schutte et al., 1996).Loss of SMAD4results in lethality at embryonic(E)days 6–7due to impaired extraembryonic membrane formation and decreased epiblast proliferation(Sirard et al.,1998;Weinstein et al.,1998).Due to the potential functions of SMAD4at postna-tal stages of mammalian development,we have been using the Cre-loxP system to overcome the early lethality and have stud-ied its functions in brain(Zhou et al.,2003)and mammary glandA R T I C L Edevelopment and neoplasia(Li et al.,2003).In an attempt to as-sess the role of SMAD4in liver development and maintenance, using hepatocyte-specific promoter-driven Cre,we unexpect-edly found that the absence of SMAD4in mouse liver results in iron overload in multiple organs and premature death.We demonstrate that loss of hepatic SMAD4is associated with dra-matically decreased expression of hepcidin in liver and in-creased duodenal expression of genes involved in intestinal iron absorption,including Dcytb(an apical iron reductase), DMT1(an apical iron transporter),and ferroportin(a basolateral iron exporter).Furthermore,SMAD4deficiency also completely blocked hepcidin induction by IL-6treatment and iron overload. ResultsSMAD4does not play an indispensable function during postnatal liver developmentTo obtain liver-specific knockout of Smad4,we generated mu-tant mice carrying a Smad4conditional allele(Yang et al., 2002)and an albumin-Cre transgene(Yakar et al.,1999) (Smad4Co/Co;Alb-Cre).The albumin promoter is active specifi-cally in liver at low levels at E19and gradually reaches adult lev-els at1–2weeks postnatally(Yakar et al.,1999).Using the Rosa-26reporter mouse(Soriano,1999),we detected Cre-mediated recombination in about40%of hepatic cells at postnatal day 15(P15)(Figure1A),which increased to about90%of cells at P37(Figure1B).PCR analysis on DNA isolated from multiple or-gans,including liver,pancreas,spleen,lung,heart,kidney,and testis,revealed recombination only in liver(Figure1C).Consis-tently,Northern blot analysis revealed about90%reduction of Smad4mRNA isolated from Smad4Co/Co;Alb-Cre liver com-pared with that of control liver(Figure1D).These observations indicated that albumin-Cre efficiently disrupts Smad4expres-sion in the majority of liver cells.Next,we analyzed Smad4Co/Co;Alb-Cre mice for a possible impact on liver development.Histopathologic analysis revealed no obvious defects in mutant liver before8months of age(data not shown).This observation indicates that the absence of SMAD4does not play a major role in liver development.After 8months,some livers showedfibrosis and accumulation of neu-trophils(Figure1F)and macrophages(Figure1H),which were not observed in wild-type control livers(Figures1E and1G). These histologic lesions might be associated with compromised liver function as evidenced by elevations of SGOT(serum gluta-mic oxaloacetic transaminase),SGPT(serum glutamate pyru-vate transaminase),and bilirubin in older mutant mice(Table S1in the Supplemental Data available with this article online). Liver-specific knockout of Smad4results in iron overloadin multiple organs/tissuesHowever,Smad4Co/Co;Alb-Cre mice gradually lost weight with over half of them becoming sick in appearance(rough-looking fur,skinny,loss of muscle mass,and slower movement)at10 months of age.Some of them(5/18)died at this stage of devel-opment.To investigate the possible causes for the wasting of these animals,we performed autopsies on these sick animals and found that they all developed a dark-red pancreas and brownish pigment deposition in multiple organs,including the liver and the proximal tubular epithelium of the kidney(data not shown).After extensive analysis,we detected a significant overload of iron in samples from mutant mice.Prussian blue staining showed that beginning from the age of2months,iron accumu-lated in all the organs with pigmentation,such as liver(Figures 2A and2B),pancreas(Figures2C and2D),and proximal tubule of the kidney(Figures2E and2F).In contrast,mutant bone mar-row and spleen demonstrated reduced staining(Figures2G and 2H,and data not shown),primarily due to the lower iron levels of macrophages in the mutant mice.Quantitative measurement of iron concentrations confirmed alteration of iron levels in these organs(Table1).Increased serum transferrin saturation levels (about2-fold,i.e.,78%in mutants vs42%in controls)were found in all4month-old mutant mice examined(n=3).Hepatic iron overload associated with macrophage iron depletion is characteristic of mouse models for human hemochromatosis (Fleming et al.,2002;Nicolas et al.,2001;Santos et al.,1996; Zhou et al.,1998).Because Alb-Cre expresses specifically in liver(Figure1C) (Yakar et al.,1999),the liver should theoretically be the only af-fected organ.Thus,it was initially surprising that a liver-specific knockout of SMAD4resulted in iron overload in multiple organs/ tissues.An important feature of liver is that it functions as a se-cretory organ and is crucial for producing a majority of circulat-ing plasma proteins,which function in many other organs.We therefore hypothesized that the targeted disruption of Smad4 in the liver must affect normal production of some of these mol-ecules that are responsible for increased iron absorption,lead-ing to a condition mimicking human hemochromatosis. Dramatically reduced expression of hepcidin in the liverof Smad4Co/Co;Alb-Cre miceTo test this hypothesis,we used liver RNA and performed a can-didate approach to study expression of a number of genes that are involved in iron metabolism,including Hfe,hepcidin,Trf-1, Trf-2and Fpn.Our RT-PCR(Figure S1),and real-time PCR (Figure3A)analyses revealed that hepcidin levels decreased about100-fold in the liver of Smad4Co/Co;Alb-Cre mice at2 to6months of age,while expression of other genes was not sig-nificantly altered(Figure S1).Hepcidin represses intestinal iron absorption and enhances macrophage iron sequestration(Ganz,2005;Viatte et al., 2005).The dramatic decrease in hepcidin in liver tissues from Smad4Co/Co;Alb-Cre mice led us to evaluate potential down-stream targets of hepcidin,including DMT1,FPN1and DCYTB1 (Frazer et al.,2002;Millard et al.,2004;Nemeth et al.,2004b; Viatte et al.,2005;Yeh et al.,2004).Our real-time PCR analysis revealed that Dmt1and Dcytb1were each elevated about 3-fold,while Fpn1was increased about2-fold in duodenum, though there were no changes in liver expression of these tran-scripts(Figure3B).Increased protein levels in mutant duode-num compared with control were detected by immunohisto-chemical staining using antibodies against DCYTB1(Figures 3C and3D),DMT1(Figures3E and3F),and FPN(Figures3G and3H).TGF-b and BMP positively regulate hepcidin expression through SMAD4Our data thus far suggested that TGF-b/SMAD4signals posi-tively regulate hepcidin expression.To test this,we treated wild-type and SMAD4null(2/2)hepatocyte cell lines with either TGF-b1or BMP-4.While hepcidin was induced up to4-to8-foldA R T I C L Ewith TGF-b 1or BMP-4in wild-type cells,SMAD42/2cells had no response (Figures 4A and 4B).This observation indicates that TGF-b 1and BMP-4require SMAD4for induction of hepci-din expression.To determine whether the induction by TGF-b 1and BMP-4in hepcidin expression is direct or indirect,we in-cluded cycloheximide in the experiment to inhibit new protein synthesis.Because SMAD4is not stable with a half-life of about 8hr,we followed hepcidin expression and SMAD4levels up to 8hr after the treatment.Our data indicated that both the TGF-b 1and BMP-4treatment increased hepcidin transcripts during the first 6hr,reaching 9-and 6-fold,respectively,and hepcidinexpression levels declined at 8hr after the treatment (Figure 4C).These observations suggest that both TGF-b 1and BMP-4in-crease hepcidin expression by directly activating SMAD4pro-tein,which is consistent with the direct activation of SMAD4by TGF-b signaling demonstrated previously (reviewed by Hel-din et al.,1997;Massague,1998;ten Dijke and Hill,2004).To confirm that the lack of response to TGF-b and BMP ob-served in SMAD4null cells is indeed due to the absence of SMAD4,we transfected a Smad4expression plasmid into SMAD4null cells and determined endogenous hepcidin expres-sion.Our data indicated that hepcidin transcription levelswereFigure 1.Abnormality of Smad4Co/Co ;Alb-Cre mice A and B)Expression pattern of Alb-Cre in P15(A )and P37(B )mice as assayed by a Rosa-26reporter.Liver sections are stained with b -gal.C)Alb-Cre promotes recombination of Smad4con-ditional alleles in a liver-specific fashion.D)Northern blot to show the reduction of both 4kb and 8kb Smad4transcripts in Smad4Co/Co ;Alb-Cre liver.E–H)Neutrophil invasion (F )and accumulation of macrophages (H )were observed in the liver of 8-month-old Smad4Co/Co ;Alb-Cre mice but not in wild-type liver (E and G ).SMAD4and hereditary hemochromatosisinduced up to 5-fold when 0.1-1m g of Smad4expression plas-mid was transfected (Figure 4D).SMAD4positively regulates hepcidin promoter activityTo study the underlying mechanism by which TGF-b and BMP-4positively regulate hepcidin expression via SMAD4,we per-formed luciferase reporter assays using a luciferase reporter construct with a fragment of the mouse hepcidin promoter (Courselaud et al.,2002).Wild-type hepatocytes transfected with the luciferase reporter construct had a 2-fold increase in lu-ciferase activity relative to hepatocytes transfected with vector (pGL3B)only.Treatment with BMP4led to a 3-fold increase in luciferase activity in the reporter construct transfected cells rel-ative to the untreated cells (Figure 4E).A 6-fold increase in lucif-erase activity was observed when the comparison was made between the reporter construct transfected cells and the vector transfected cells (vector only or vector +BMP-4treatment,Figure 4E).The increased luciferase activity was likely SMAD4dependent,as no such increase was observed in SMAD42/2hepatocytes upon BMP-4treatment (Figure 4E).To confirm this,we reconstituted SMAD4in the SMAD42/2cells by trans-fecting a Smad4expression construct.SMAD42/2hepatocytes that were cotransfected with the hepcidin promoter-containing luciferase reporter construct and the SMAD4expression con-struct showed increasing luciferase activity with increasing amounts of transfected SMAD4expression construct in a dosage-dependent manner (Figure 4F).We also cotransfected the hepcidin promoter-containing luciferase reporterconstructFigure 2.Iron accumulation in multiple organs of 4-month-old Smad4Co/Co ;Alb-Cre micePrussian blue staining shows iron accumulation in mutant liver (B ),pancreas (D ),kidney (F ),but not in bone marrow (H ).Iron accumulation did not occur in organs of control littermate mice (A ,C ,E ,and G ).A R T I C L Eand the Smad4expression construct into HEPA1-6cells,a cell line that was derived from a SMAD4wild-type hepatocyte carcinoma(Monga et al.,2002),and found similar SMAD4-dependent increases in luciferase activity(Figure4F).We con-clude that SMAD4is required to transduce signaling of both BMP and TGF-b subfamilies on the hepcidin promoter. Histone modification plays an important role in controlling gene expression(He and Lehming,2003).For example,the acetylation(Ac)of histone H3at lysine9and methylation(Me) at lysine4is associated with transcriptional activation.To eval-uate whether SMAD4has an effect on histone H3modification, we performed chromatin immunoprecipitation(ChIP)assay us-ing SMAD4null cells that had been transfected with either the Smad4construct or empty vector.Antibodies specific for Me-K4and Ac-K9modified H3precipitated the hepcidin promoter sequences from extracts of Smad4transfected cells and precip-itated much weaker bands from extracts of empty vector trans-fected cells(Figure4G).The antibody against Me-K4precipi-tated significantly more DNA from the hepcidin promoter than the antibody against Ac-K9,suggesting that SMAD4has a stron-ger effect on the K4modification of histone H3.To determine whether treatment with TGF-b or BMP has a similar effect on his-tone H3K4methylation,we performed the ChIP assay in Smad4 wild-type cells before and after treatment with TGF-b or BMP. We detected significantly stronger H3K4methylation of the hep-cidin promoter after treatment of either TGF-b or BMP than in un-treated cells(Figure4H).These data imply that expression of TGF-b/SMAD4signaling leads to modification of histone H3 in the hepcidin promoter,consistent with the increased expres-sion of endogenous hepcidin(Figure4D),and increased pro-moter reporter activity(Figure4F)in SMAD4transfected cells. Failure of hepcidin induction in SMAD4deficient liverafter administration of IL-6or iron-dextranMuch is known about the downstream effects of hepcidin on iron homeostasis,but less is known about upstream effectors. IL-6stimulates hepcidin transcription in cultured primary hepa-tocytes(Nemeth et al.,2003).It was further demonstrated that the activation of hepcidin transcription by IL-6does not require HFE or TFR-2(Lee et al.,2004).To determine if IL-6-dependent induction of hepcidin requires SMAD4,we treated SMAD4mu-tant and control mice with IL-6.Our data indicated that hepcidin levels increased to2.3-and1.9-fold at4and9hr after IL-6ad-ministration in wild-type animals(Figure5A).This level of hepci-din induction is comparable to that found in the primary hepato-cytes(Nemeth et al.,2003).In contrast,hepcidin expression in Smad4Co/Co;Alb-Cre mice maintained very low,from0.0243 (PBS treated)to0.03(4h after IL-6treatment)and0.025(9h after IL-6treatment),in relation to hepcidin expression in PBS treated control mice,which was set at1(Figure5A).This observation suggests that the absence of SMAD4not only interfere with baseline hepcidin expression but also blocked the induction of hepcidin by IL-6.Known as a common mediator for TGF-b superfamily(Heldin et al.,1997;Massague,1998;ten Dijke and Hill,2004),SMAD4is unlikely to be a part of the IL-6pathway.Based on the data pre-sented earlier suggesting that expression of Smad4or treatment with its ligands results in an epigenetic modification of histone H3to a transcriptionally active form,we suspected that rather than mediating IL-6signaling,Smad4might be required to open the chromatin of the hepcidin promoter.To determine whether IL-6signaling pathways are intact in Smad4Co/Co;Alb-Cre mice,we examined transcription of several acute phase genes known to be induced by IL-6including CRP,SAA and Al-bumin.Our data indicated that Smad4Co/Co;Alb-Cre mice main-tained an intact response to the IL-6treatment,although the re-sponsiveness seemed to be stronger than in the wild-type controls,especially for CRP and SAA-1(Figures5B–5D).While these observations revealed a complex relationship between SMAD4and IL-6,they suggest that failure of IL-6to induce hep-cidin in Smad4Co/Co;Alb-Cre mice is not due to a nonspecific block of IL-6signaling by SMAD4deficiency.Hepcidin expression is also induced by iron overload(Pigeon et al.,2001).Because hepcidin inhibits iron absorption,the in-duction of hepcidin may represent a feedback mechanism,i.e, when iron levels are high,hepcidin expression increase,and the increased hepcidin,in turn,inhibits expression of iron trans-porters in the intestine to decrease iron absorption.To deter-mine whether SMAD4plays a role in this process,we treated SMAD4mutant and control mice with iron-dextran to induce iron overload.Our data indicated that iron overload increased hepcidin expression in control mice by about2.8-fold3days af-ter the treatment.In contrast,hepcidin expression remained low and was nonresponsive to iron treatment in mutant mice(0.03in PBS-treated and0.022in iron-treated mice,Figure5E).Be-cause Smad4Co/Co;Alb-Cre mice are already iron overloaded,a potential caveat is that injection of iron-dextran might not result in further iron overload and that the failure of Smad4Co/Co;Alb-Cre mice to increase hepcidin expression in response to treat-ment with iron dextran might be due to the lack of change in iron level.To investigate this,we stained liver sections with Prus-sian blue and found that iron-dextran treatment significantly in-creased iron levels in both control and mutant livers(Figures5F–5I).Altogether,these observations indicate that this feedback pathway to induce hepcidin by increased levels of iron cannot operate when SMAD4is absent.DiscussionIn this study,we investigated the role of the TGF-b/BMP signal-ing pathway in liver development and maintenance by using Alb-Cre to abate SMAD4expression in the liver specifically.Table1.Iron concentrations(m M/g6SD)in Smad4Co/Co;Alb-Cre mutant and control miceSamples Liver Pancreas Kidney SpleenControl(2M) 4.7361.60 3.2861.63 2.4861.015.5160.51 Mutant(2M)42.9963.635.6166.2921.16611.5 4.6261.56Control(4M)8.0861.12 5.9962.94 4.5362.7226.3865.35 Mutant(4M)45.5162.945.7865.830.88610.926.42614.0 Control(6M) 4.4561.7 3.3160.60 4.47561.517.2467.8Mutant(6M)41.7663.544.6464.822.3665.911.8663.3SMAD4and hereditary hemochromatosisUnexpectedly,the liver-specific knockout of SMAD4does not have a major impact on liver development;instead,it results in a dramatic accumulation of iron in the liver of Smad4Co/Co ;Alb-Cre mice.In addition,several other organs that have intact SMAD4,including pancreas,kidney,eye and brain,also exhibit accumulation of iron starting from 2months of age.Thus,our work not only creates a new animal model for hemochromato-sis,but also clearly indicates that the liver is a physiological cen-ter for regulation of iron homeostasis.The molecular basis for such a phenotype is that liver-specific knockout of SMAD4inSmad4Co/Co ;Alb-Cre mice results in diminished expression of hepcidin,which is made specifically in liver and regulates iron absorption in the duodenum.The absence of hepcidin results in significantly increased expression of iron transporters (FPN1and DMT1)and ferric reductase (DCYTB1)in small intestine,and enhanced iron absorption,leading to iron overload.While iron overload was observed in Smad4mutant mice of all ages,liver-specific knockout of Smad4also caused severe damage of pancreas in older mutant mice.This phenotype may not be explained by the down regulation of hepcidinasFigure 3.Absence of hepatic SMAD4results in al-tered expression of hepcidin and several iron trans-portersA )Real-time RT-PCR shows dramatically decreased hepcidin expression in livers of 2-,4-,and 6-month-old SMAD4mutant mice compared with normal con-trols.Hepcidin levels in control mice were arbitrarily assigned a value of 1.B )Expression of Dcytb1,Dmt1,and Fpn in intestine (duodenum)and liver in 2-month-old Smad4Co/Co;Alb-Cre mice was detected by real-time RT-PCR.Expression levels for each gene in controls were arbitrarily assigned a value of 1.C–H )Immunohistochemical staining of DCYTB1(C and D ),DMT1(E and F ),and FPN (G and H )in duode-num of control (C ,E ,and G )and mutant (D ,F ,and H )mice reveals dramatically increased expression of DCYTB1and DMT1,and slightly increased expres-sion of FPN.Values are expressed as mean 6SD.A R T I C L Eno such abnormality was reported in mice carrying targeted dis-ruption of hepcidin (Nicolas et al.,2001).Liver produces multiple factors that may be essential for maintenance of pancreatic ac-inar cells and the production of some of these factors may be im-paired in Smad4mutant mice.To investigate whether levels of factors potentially important for the maintenance of pancreatic acinar cells are altered in Smad4mutant mice,we have per-formed microarray analysis on the liver of Smad4Co/Co ;Alb-Cre and control mice at 2and 4months of age.This study revealed alterations in the expression of many genes other than hepcidin,including several members of the cytochrome p450family,Igfbp1,Cdkn1a,and Sparc (Table S2).Thus,in addition to iron overload resulting from decreased hepcidin expression,changes in the expression of other genes may contribute to the pathology of Smad4mutant mice.This possibility remains to be tested in future study.Importantly,our study reveals a novel role for TGF-b /BMP sig-naling in induction of hepcidin expression and shows that SMAD4is required for this activity.Although iron has been con-sidered as a vital metal for the proliferation of all cells inside the body for long time,our experimental data connect iron absorp-tion with growth factor signals.Our data indicated thattheFigure 4.Induction of hepcidin expression by TGF-b signaling requires SMAD4A andB )TGF-b 1(A)and BMP-4(B)positively regu-late endogenous hepcidin expression through SMAD4in wild-type SMAD4(+/+),but not in SMAD4null (2/2)hepatic cell lines.C )TGF-b /BMP4directly induces hepcidin expres-sion.Cells were treated with 10m g/ml cycloheximide for 30min before TGF-b 1or BMP-4was added.Data were normalized with cells treated with cyclohexi-mate only.Lower panel shows Smad4(S4)and b -ac-tin (b -a)levels at the multiple time points up to 8hr af-ter cycloheximate treatment.D )Reconstitution of SMAD4in SMAD4null cells in-creased endogenous hepcidin expression.Insert is a Western blot analysis showing SMAD4levels prior to,24hr after,and 48hr after Smad4(1m g)transfec-tion.E )Hepcidin promoter activity,as reflected by lucifer-ase assay,is elevated by BMP-4treatment in wild-type cells but not in the Smad42/2cells.3B is a basal vector without hepcidin promoter,which is a frag-ment containing 2783to +49.F )Hepcidin promoter activation is SMAD4dosage dependent in both HEPA1-6and the MT cells.G and H )ChIP analysis showing histone H3acetyla-tion (Ac)at K9and methylation (Me)at K4on the hep-cidin promoter.The primers for ChIP assay cover 2933/2324fragment of Hepcidin promoter.Values are expressed as mean 6SD.All assays in (C )–(F )were performed 48hr after plasmid trans-fection.SMAD4and hereditary hemochromatosisincreased expression of hepcidin under TGF-b and BMP treat-ment or SMAD4overexpression was correlated with increased H3K4methylation,which is associated with transcriptional acti-vation (He and Lehming,2003).Therefore,it is possible that TGF-b /SMAD4signaling is needed for maintaining hepcidin ex-pression by keeping the hepcidin promoter in an active form.Notably,it was shown previously that expression of a domi-nant-negative mutant TGF-b type II receptor in liver of trans-genic mice did not cause obvious abnormalities in several or-gans examined,including liver,spleen,kidneys,intestine,lung and heart (Kanzler et al.,2001).It also did not cause any de-crease in the life span of transgenic mice.We have also exam-ined the liver of Smad32/2mice (Yang et al.,1999),and found they do not have any increased iron accumulation compared with the control liver (data not shown).These observations sug-gest that the absence of a single member of the TGF-b subfam-ily,or loss of a single intracellular mediator for signaling of a sub-family is not sufficient enough to cause iron accumulation.It is possible that BMP signals can maintain normal expression of hepcidin in the absence of TGF-b subfamily signals.Conversely,we also predict that loss of BMP subfamily signaling alone should not have an obvious effect on iron absorption due to the existence of the TGF-b subfamily and/or other subfamilies.Because SMAD4serves as a common mediator for the TGF-b super family (reviewed in (Heldin et al.,1997;Massague,1998;ten Dijke and Hill,2004)),the absence of SMAD4is predicted to block all the family members that either use SMAD2/SMAD3(for TGF-b and activin subfamilies),or use SMAD1/SMAD5/SMAD8(for BMP subfamily)for signaling,and could therefore lead to a profound effect on iron accumulation that might not occur if only one of the other family members were lost.In addition to TGF-b signaling,hepcidin expression is also sub-jected to regulation by a number of factors/conditions,including HFE,c/EBP a ,iron,hypoxia,IL-6,and inflammation.The OMIM database divides hemochromatosis into four classes:type1(HFE mutation related)(Bridle et al.,2003;Gehrke et al.,2003),two juvenile types:type2A (Hemojuvelin related)(Papanikolaou et al.,2004),and type2B (hepcidin related)(Roetto et al.,2003),and type3(TFR2related)(Kawabata et al.,2005)alldisplayFigure 5.Absence of SMAD4blocked induction of hepcidin by IL-6injection and iron overload A )Hepcidin levels in control and Smad4Co/Co ;Alb-Cre mice prior to and after IL-6injection.B–D )Expression of IL-6downstream genes.E )Hepcidin levels in control and Smad4Co/Co ;Alb-Cre mice prior to and after iron-dextran injection.F –I ),Prussian blue staining of control (F andG )and mutant (H andI )liver.Of note,the administration of iron-dextran further increased iron levels in mutant liver (I )compared with untreated mutant mice (H ).Values are expressed as mean 6SD.All animals were 2months of age,and at least three animals were used for each time point.A R T I C L E。
Atmos.Chem.Phys.,9,3357–3369,2009 /9/3357/2009/©Author(s)2009.This work is distributed under the Creative Commons Attribution3.0License.Atmospheric Chemistry and PhysicsHydration increases the lifetime of HSO5and enhances its ability to act as a nucleation precursor–a computational studyT.Kurt´e n1,T.Berndt2,and F.Stratmann21Department of Physics,P.O.Box64,00014University of Helsinki,Helsinki,Finland2Leibniz-Institut f¨u r Troposph¨a renforschung e.V.,Permoserstr.15,04318Leipzig,GermanyReceived:27November2008–Published in Atmos.Chem.Phys.Discuss.:28January2009Revised:4May2009–Accepted:18May2009–Published:25May2009Abstract.Recent experimentalfindings indicate that HSO5radicals may play a key role in the nucleation of atmosphericSO2oxidation products.HSO5radicals are metastableintermediates formed in the SO2oxidation process,andtheir stability and lifetime are,at present,highly uncer-tain.Previous high-level computational studies have pre-dicted rather low stabilities for HSO5with respect to disso-ciation into SO3+HO2,and have predicted the net reactionHSO3+OH→SO3+HO2to be slightly exothermal.However,these studies have not accounted for hydration of HSO5orits precursor HSO3.In this study,we have estimated the ef-fect of hydration on the stability and lifetime of HSO5us-ing the advanced quantum chemical methods CCSD(T)andG3B3.We have computed formation energies and free ener-gies for mono-and dihydrates of OH,HSO3,HSO5,SO3and HO2,and also reanalyzed the individual steps of theHSO3+O2→HSO5→SO3+HO2reaction at a higher level oftheory than previously published.Our results indicate thathydration is likely to significantly prolong the lifetime of theHSO5intermediate in atmospheric conditions,thus increas-ing the probability of reactions that form products with morethan one sulfur atom.Kinetic modeling indicates that theseresults may help explain the experimental observations that amixture of sulfur-containing products formed from SO2oxi-dation by OH radicals nucleates much more effectively thansulfuric acid taken from a liquidreservoir.Correspondence to:T.Kurt´e n (theo.kurten@helsinki.fi)1IntroductionThe formation of atmospheric aerosol particles by nucleation from gas-phase molecules has recently received growing ex-perimental and theoretical interest due to the climate and health–related effects offine particles(see e.g.Kulmala, 2003;Kulmala et al.,2004).Despite a large number of ex-perimental and modeling studies,little is known about the de-tailed molecular–scale processes behind the particle forma-tion events observed in the atmosphere.Based on observed correlations between particle formation rates and trace gas concentrations(see e.g.Weber et al.,1995;Kulmala et al., 2006;Riipinen et al.,2007),and also on thermodynamic classical nucleation theory calculations,nucleation in the lower troposphere has been thought to involve mainly water and sulfuric acid,with possible contributions from ions,am-monia or various organic molecules.A comparison offield measurements with laboratory experiments on sulfuric acid –ammonia–water mixtures reveals some curious discrep-ancies.For example,the nucleation rate typically depends on the7th or8th power of the sulfuric acid concentration in the laboratory experiments(Ball et al.,1999),but only on the1st or2nd power in thefield experiments(Weber et al., 1995;Kulmala et al.,2006;Riipinen et al.,2007).This in-dicates that the critical cluster(the smallest cluster for which growth is thermodynamically more favorable than decay)in field conditions contains only1–2sulfuric acid molecules, as opposed to7–8in laboratory conditions.Also,sulfu-ric acid concentrations in the atmosphere during nucleation events are typically around106–107molecules cm−3,while the threshold concentration for nucleation in laboratory ex-periments is around1010molecules cm−3.Recently,Berndt et al.(2005,2006,2007)compared the nucleation rates of sulfuric acid formed from SO2oxidation by OH radicals to that of sulfuric acid taken from a liquidPublished by Copernicus Publications on behalf of the European Geosciences Union.reservoir.They found that the threshold H2SO4concentra-tion for particle formation was107molecules cm−3if H2SO4 was produced in situ via the reaction of OH radicals with SO2 in the presence of water vapor,and1010molecules cm−3if the H2SO4was taken from a liquid reservoir or produced in situ via the reaction of SO3with water vapor.Other exper-imentalfindings confirm a H2SO4threshold concentration of about107–108molecules cm−3(Burkholder et al.,2007; Young et al.,2008;Benson et al.,2008)when produced in situ from SO2.It should be noted that the differences regard-ing the stated threshold H2SO4concentrations reported from various studies are probably caused by the different experi-mental conditions used.Sulfuric acid production from SO2oxidation proceeds via a series of radical reactions.First,SO2reacts with an OH radical,which is normally produced from water vapor via reaction with electronically excited atomic oxygen O(1D), which in turn is formed from ozone photolysis.(Alterna-tively,the OH radical can be formed from ozonolysis of an alkene in a dark reaction.)SO2+OH+M→HSO3+M(R1)Where M denotes a collision partner(typically N2or O2). The HSO3radical then rapidly reacts with molecular oxy-gen to yield either SO3and HO2or an intermediate complex HSO5:HSO3+O2→SO3+HO2(R2a) HSO3+O2+M→HSO5+M(R2b) SO3reacts with water(catalyzed by another water molecule) to yield sulfuric acid:SO3+2H2O→H2SO4+H2O(R3)The HSO5radical may also decompose to SO3and HO2,or it may react with other compounds.For example,self-reaction would form peroxodisulfuric acid,H2S2O8:HSO5→SO3+HO2(R4) HSO5+HSO5→H2S2O8+O2(R5) If Reaction(4)is very rapid,Reactions(2a)and(2b)can not necessarily be distinguished from each other.At present,it is not known if the direct Reaction(2a)is possible,or if the reaction always proceeds via a transient HSO5intermediate. Various authors(Davis et al.,1979;Wayne,2000)have sug-gested that HSO5in atmospheric conditions is likely to be hydrated,but to our knowledge no experimental or computa-tional evidence of this has been presented prior to this study. The HSO3+O2reaction has been investigated by several groups.In a computational study,Majumdar et al.(2000) proposed that the reaction proceeds via three steps:HSO3+O2+M→HSO5(R)+M(R2c)HSO5(R)→HSO5(TS)(R2d) HSO5(TS)→HSO5(P)(R2e) HSO5(P)→SO3+HO2(R2f) Where HSO5(R)is a reactant complex corresponding to HSO3•O2(HOSO2•O2),HSO5(P)is a product complex cor-responding to SO3•HO2,and HSO5(TS)is a transition state connecting the two,where the H-atom is shared by the S-O-O and S-O groups.It should be noted that R2d and R2e do not correspond to real,individual chemical reactions,but to elementary steps of the same reaction.Very recently,Berndt et al.(2008)and Laaksonen et al.(2008)have discussed the implications of the experimen-tal results in terms of these mechanisms,and concluded that a nucleation mechanism involving HSO5or its reaction prod-ucts is likely to explain nucleation starting from OH+SO2 observed in atmosphere as well as in the laboratory.Salo-nen et al.(2009)have investigated the stability of clusters of sulfuric acid together with various intermediate and alterna-tive products of the SO2oxidation chain,and concluded that while HSO5itself is unlikely to nucleate very effectively,a mixture of sulfuric acid and HSO5reaction products contain-ing more than one sulfur atom(such as peroxodisulfuric acid) are likely to nucleate more effectively than sulfuric acid on its own.A crucial uncertainty in the proposed nucleation mecha-nism is the lifetime of HSO5especially with respect to dis-sociation via path(4)and(2f).Based on computational and experimental studies(Stockwell and Calvert,1983;Li and McKee,1997),the dissociation of HSO5into SO3and HO2 could be very rapid.Thus,the fraction of HSO5molecules that live long enough to collide with other sulfur-containing molecules would be small,and any nucleation mechanism starting from HSO5would be inefficient.However,previous computational studies have neglected the effect of water va-por,which is always present in both laboratory andfield stud-ies in concentrations far exceeding those of all sulfur–con-taining molecules combined.In principle,hydration could increase the steady-state concentration of HSO5,and thus the probability of bimolecular reactions involving HSO5,by four different mechanisms:–Thermodynamic stabilization of HSO5with respect to the products SO3and HO2.–Thermodynamic stabilization of HSO5(R)with respect to HSO5(P).–Kinetic stabilization of HSO5(R)with respect to HSO5(P),i.e.the barrier for Reaction(2d)+(2e)above could be increased by hydration.–Increasing the fraction of HSO3+O2collisions that lead to HSO5formation as opposed to direct SO3+HO2for-mation(if the latter is at all possible).E.g.if HSO3wereAtmos.Chem.Phys.,9,3357–3369,/9/3357/2009/hydrated in Reactions(2a/2b),there would be more vi-brational degrees of freedom to accommodate the ex-cess energy liberated in the reaction,and thus a greater degree of energy accommodation,and a higher prob-ability for the transiently formed reaction complex to stay together.Mechanism number3is not very likely,as water typically tends to catalyze proton transfer reactions rather than hin-dering them.In this study,we have assessed the effect of mechanisms1and2above using advanced quantum chemi-cal methods,and found them both to be significant.2Computational detailsWe have computed free energies of formation for SO2,OH, HSO3,O2,HSO5,SO3and HO2molecules and most of their mono-and dihydrates.(The hydrates of O2were not stud-ied,as they are likely to be extremely weakly bound due to the nonpolarity of the O2molecule.Also,only the monohy-drate of SO2was considered,as experimental evidence(Der-mota et al.,2005)indicates that SO2in water clusters only interacts with one water molecule).Free energies have been computed using the G3B3combination method(Baboul et al.,1999)which involves B3LYP/6-31G(d)geometry opti-mizations and frequency calculations(using a scaling factor of0.96)together with a series of higher-level(MP2(full), MP4and QCSID(T))single-point energy calculations and empirical corrections.Assuming certain additivity rules,the G3B3energy is a reasonable estimate of the QCISD(T)(full) energy with a large triple-zeta basis set.For a sample set of299data points(Baboul et al.,1999),the mean absolute deviation of the energies predicted by the G3B3method is 0.99kcal/mol.Some calculations have also been performed with the G2combination method(Curtiss et al.,1991),which is similar to G3B3except that frequencies are computed at the HF/6-31G(d)level and geometries at the MP2/6-31G(d) level.Unfortunately,most of the G2calculations on hydrated HSO5failed as the MP2geometry optimizations did not con-verge.This may be related to thefinding by Majumdar et al.(2000)that the MP2method does not always yield reli-able results(especially structures or vibrational frequencies) for all configurations of the HSO5system.To assess the re-liability of the G3B3values(and also to compute more re-liable estimates for the reaction energetics than published in earlier studies),we further optimized the structures of the free molecules,monohydrates and selected dihydrates at the UB3LYP/6-311++G(3df,3pd)level(Becke,1993;Lee et al., 1988)and performed UCCSD(T)/6-311++G(3df,3pd)and UCCSD(T)/aug-cc-pV(T+d)Z(Knowles et al.,1993;Deegan and Knowles,1994)single-point energy calculations at these geometries.(The aug-cc-pV(T+d)Z basis set is identical to the standard aug-cc-pVTZ basis set forfirst-and second-row atoms,and contains an extra d–orbital for third-row atoms, as this has been shown to yield more accurate atomization energies,see Dunning et al.,2001).Due to the extreme computational cost and prohibitive scaling of the UCCSD(T) method,we were unable to treat the HSO5dihydrate clusters at this level.To maintain consistency with G3B3thermochemical pa-rameters,a scaling factor of0.967was used in calculat-ing the thermal entropy and enthalpy contributions at the UB3LYP/6-311++G(3df,3pd)level.This was based on data for the6-311+G(3df,2p)basis set from the Computational Chemistry Comparison and Benchmark Database(http:// /default.htm).This scaling factor was based on3448individual vibrational frequencies from308differ-ent molecules.A slightly larger scaling factor of0.970was given for the basis set6-311+G(3df,2pd),which is closer in size to the basis used in this work.However,as this value was not based on direct calculations,but on comparisons with B3LYP/cc-pVTZ calculations,we chose the former value as somewhat more reliable.This is partly supported by a re-cent study by Anderson and Uvdal(2005),in which a scaling factor of0.9679was recommended for B3LYP calculations with all Pople basis sets larger than6-311++G(d,p).In any case,the difference between results obtained with the three scaling factors(0.967,0.9679and0.970)are minimal.All thermochemical parameters presented here have been com-puted using the rigid rotor and(scaled)harmonic oscillator approximations.SO2•H2O,OH•(H2O)n,HSO3•H2O,SO3•(H2O)n and HO2•(H2O)n(with n=1,2,...)clusters have been compu-tationally studied previously(Li and McKee,1997;Du et al.,2006;Aaltonen and Fransisco,2003;Fliegl et al.,2006; Larson et al.,2000;Alongi et al.,2006),and initial geome-tries for these systems were taken from the published liter-ature.To our knowledge,there are no previous studies on HSO3•(H2O)2or HSO5•(H2O)1...2clusters.For these sys-tems,initial guesses were generated using the Spartan pro-gram(Wavefunction Inc,2002),and pre-optimized at the B3LYP/6-31G(d)level(and for some clusters also at the PBE/6-31+G(2d,p)level with densityfitting).For the HSO5 mono-and dihydrates,several of the initial guess geometries failed to converge at the B3LYP and PBE levels,and only a few structures couldfinally be used for the higher-level calculations.UCCSD(T)calculations were performed using the Molpro2006.1program(Werner et al.,2006),some RI-MP2test calculations(Weigend and H¨a ser,1997;Weigend et al.,1998)were performed on Turbomole5.10(Alrichs et al.,1989),and all other calculations were carried out using the Gaussian03program suite(Frisch et al.,2004).The de-fault energy and geometry convergence criteria for each pro-gram were used in all calculations.It should be noted that for the HSO5(TS)and HO2systems,both of which belong to the point group Cs,using the default symmetry settings of the Molpro program causes severe errors in the computed reaction energies,as the calculation then corresponds to an excited electronic state(with symmetry2A ).To compute the energy for the ground state(with symmetry2A ),the/9/3357/2009/Atmos.Chem.Phys.,9,3357–3369,2009Table1.Electronic energy change( E elec),enthalphy change( H)and Gibbs free energy change( G)for the reaction HSO3+O2→SO3+HO2,computed at various levels of theory.All values in kcal/mol.Enthalpies and Gibbs free energies correspond to298K and1atm reference pressure.A scaling factor of0.967has been used in the UB3LYP/6-311++G(3df,3pd)frequency calculations.E elec H GMP2/6-31G(d,p)a8.649.029.52B3LYP/6-31G(d,p)a9.299.9410.58MP2/TZ2P(f,d)++a 3.05 3.48 3.89B3LYP/TZ2P(f,d)++a 4.52 4.82 5.39MP2/cc-pVTZ a 2.35 2.77 3.26MP2/cc-pVQZ a0.58−−MP2/cc-pV5Z a−1.29−−B3LYP/cc-pVQZ a 3.80−−B3LYP/cc-pV5Z a 2.17−−MP4(SDTQ)/6-31G(d,p)//HF/3-21G(d)b11.912.312.8Thermochemical prediction c−8±2−Thermochemical prediction d−0.9−CCSD(T),MP2-F12e−2.3±0.7G2f,g−3.98−3.74−3.16G3B3g−2.68−2.44−1.76UCCSD/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)g−1.33−1.04−0.46UCCSD/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)g−0.74−0.460.13UCCSD(T)/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)g−1.24−0.95−0.37UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)g−0.61−0.320.26a Majumdar et al.(2000);b Nagase et al.(1988);a further extrapolation of the correlation energy beyond MP4gave H=10.6kcal/mol;c Based on data by Benson,1978;d Based on data by Atkinson et al.(1997);given by Li and McKee(1997);e Klopper et al.(2008);advanced multistep calculations involving MP2-F12/aug-cc-pwCV5Z and UCCSD(T)/cc-pV(T+d)Z calculations,together with anharmonic,hindered rotor and relativistic corrections.f Li and McKee(1997);g This studysymmetry of the ground-state wavefunction must either be explicitly specified(using the wf and occ keywords),or the calculation must be performed without using symmetry(key-word nosym).A similar phenomenon occurs for the OH rad-ical.The Cartesian co-ordinates,energetics and vibrational temperatures of all studied structures are given in the supporting information(/ 9/3357/2009/acp-9-3357-2009-supplement.pdf).3Results and discussion3.1HSO3+O2reaction energeticsPrevious studies have found the net reaction HSO3+O2→SO3+HO2(Reaction2a)to be either exother-mic(Li and McKee,1997;Klopper et al.,2008),weakly endothermic(Majumdar et al.,2000)or strongly en-dothermic(Benson,1978;Nagase et al.,1988).Ex-perimentally,the reaction is known to be the exclusive fate of HSO3in the atmosphere with a rate constant of 4.3×10−13cm3molecule−1s−1at293K(Gleason et al., 1987;Gleason and Howard,1988).The experimental results thus indicate that the studies predicting a strong endother-micity are likely to be in error.The reaction energetics predicted for this reaction at various levels of theory are given in Table1.(Note that several more basis sets were used in the study by Majumdar et al.,2000;the rest of their values lie between those presented here.)It can be seen from Table1that while B3LYP and MP2calculations predict the reaction to be strongly en-dothermic unless very large basis sets are used,the moreAtmos.Chem.Phys.,9,3357–3369,/9/3357/2009/Table2.Electronic energy change( E elec),enthalphy change( H)and Gibbs free energy change( G)for the four individual steps of the overall reaction HSO3+O2→SO3+HO2,computed at various levels of theory.A scaling factor of0.967has been used in the UB3LYP/6-311++G(3df,3pd)frequency calculations.All values in kcal/mol.Enthalpies and Gibbs free energies correspond to298K and1atm reference pressure.HSO5(R),HSO5(TS)and HSO5(P)correspond to the reactant,transition state and product complexes,respectively.(See the text and Fig.1for details.)reaction,method E elec H GHSO3+O2→HSO5(R)B3LYP/6-31G(d,p)a−8.09−6.26 5.06MP2/6-31G(d,p)a−3.67−2.299.20B3LYP/TZ2P++a−6.08−4.40 6.84MP2/TZ2P++a−6.28−4.447.06MP3/6-31G(d,p)//HF/3-21G(d)b−1.2 3.214.4Thermochemical prediction c−−16−G2e−20.13−18.56−6.89G3B3e−14.76−13.42−2.67UCCSD/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e−16.31−14.63−3.28UCCSD/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e−17.60−15.92−4.57UCCSD(T)/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e−16.01−14.32−2.98UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e−17.33−15.65−4.30HSO5(R)→HSO5(TS)B3LYP/6-31G(d,p)a 3.75 1.50 2.53MP2/6-31G(d,p)a 2.100.46 1.27B3LYP/TZ2P++a 4.20 1.60 2.65MP2/TZ2P++a 1.870.29 1.03G2e 6.49 4.06 4.79G3B3e 6.65 1.94 3.43UCCSD/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e10.467.898.80UCCSD/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e10.728.169.07UCCSD(T)/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e 6.49 3.92 4.83UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e 6.73 4.16 5.07a Majumdar et al.(2000);b Nagase et al.(1997);c Based on data by Benson(1978);d Solimannejad et al.(2004);e This studyadvanced methods including high-level correlation(G2, G3B3,UCCSD(T))predict the reaction energy and enthalpy to be slightly below,though quite close to,zero.The re-action free energies predicted by the more advanced meth-ods lie on both sides of zero,and are all quite small.The large differences between MP2or DFT energies on one hand and G2,G3B3or coupled-cluster energies on the other indi-cates that high-level electron correlation plays a central role in the energetic of the reaction,as noted by Majumdar et al.(2000).The difference between the G3B3,UCCSD and UCCSD(T)energies(as well as the UCCD and UCCSD(T) energies using two different basis sets)are of the same size as the predicted endo-or exothermicity,indicating that a quan-titatively reliable prediction of the sign of the energy change of the reaction likely requires even more advanced methods than those used here.In a very recent state-of-the-art com-putational study,Klopper et al.(2008)recalculated the heat of formation of HSO3using a combination of very high-level methods,and applied this data to estimate the enthalpy of Reaction(2a),finding it to be weakly exothermic.Our/9/3357/2009/Atmos.Chem.Phys.,9,3357–3369,2009Table2.Continued.reaction,method E elec H GHSO5(TS)→HSO5(P)B3LYP/6-31G(d,p)a−2.050.56−0.64MP2/6-31G(d,p)a−2.28−0.37−2.11B3LYP/TZ2P++a−3.84−1.05−2.34G2e−2.69−0.09−3.50G3B3e−4.82−2.08−3.34UCCSD/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e−5.70−2.98−4.33UCCSD/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e−4.90−2.18−3.53UCCSD(T)/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e−3.84−1.13−2.48UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e−3.04−0.33−1.68HSO5(P)→SO3+HO2B3LYP/6-31G(d,p)a15.6714.14 3.63MP2/6-31G(d,p)a12.519.39 1.16B3LYP/TZ2P++a10.939.36−1.05B3LYP/6-311++G(2df,2p)d11.20−−MP2/6-311++G(2df,2p)d12.19−−G3d11.5111.54 2.08G3MP2d10.2510.28 4.58G2e12.3510.85 2.44G3B3e12.6811.130.82UCCSD/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e10.228.67−1.65UCCSD/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e11.039.49−0.83UCCSD(T)/6-311++G(3df,3pd)//UB3LYP/6-311++G(3df,3pd)e12.1210.580.25UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)e13.0411.50 1.17a Majumdar et al.(2000);b Nagase et al.(1997);c Based on data by Benson(1978);d Solimannejad et al.(2004);e This studybest results are in fairly good agreement with their enthalpy value of−2.3±0.7kcal/paring the free energy and enthalpy values,we can conclude that also the free energy change of the reaction is very likely to be slightly below zero. To our knowledge,only Majumdar et al.(2000)have pre-viously addressed the detailed energetics of all the elemen-tary reaction steps2c–2f.The study by Nagase et al.(1988) contains data for Reaction(2c),while that of Solimannejad et al.(2004)contains data for Reaction(2f).The energet-ics of these individual steps are reported in Table2.The structure of the molecules HSO3,HSO5(R),HSO5(TS)and HSO5(P)are shown in Fig.1.The structures are drawn using the MOLEKEL4.3visualization package(Portmann,2002).As for the net Reaction(2a),there are considerable differ-ences between the different pared to the more advanced G2,G3,G3B3and coupled-cluster methods,MP2 and B3LYP significantly underestimate the binding energy of HSO5(R)and the barrier height for the HSO5(R)→HSO5(P) conversion.However,the energetics for Reaction(2f)pre-dicted by the different methods are relatively similar. Regardless of the method used,the HSO5(TS)tran-sition state is predicted to be lower in electronic energy and enthalpy than the reactants HSO3+O2.On the other hand,all methods except G2predict the tran-sition state to lie higher in free energy than the free reactant molecules.The highest-level(UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)) G valueAtmos.Chem.Phys.,9,3357–3369,/9/3357/2009/Table3.Electronic energy change( E elec),enthalphy change( H)and Gibb’s free energy change( G)for hydration reactions of various molecules:X+n(H2O)→X•(H2O)n.A scaling factor of0.967has been used in the UB3LYP/6-311++G(3df,3pd)frequency calculations. All values in kcal/mol.Enthalpies and Gibbs free energies correspond to298K and1atm reference pressure.HSO5(R),HSO5(TS)and HSO5(P)correspond to the reactant,transition state and product complexes,respectively.(See the text and Fig.1for details.)When multiple literature values exist for some parameter,only the highest-level ones are given.cluster,method E elec H GSO2•H2O,G2a−3.46−3.51 3.62SO2•H2O,G3B3h−4.55−3.06 4.44SO2•H2O,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−4.51−3.19 3.23OH•H2O,RCCSD(T)/aug-cc-pVTZ b−5.88−−OH•H2O,G3B3h−5.59−4.13 2.14OH•H2O,UCCSD(T)/aug-cc-pVTZ//UB3LYP/6-311++G(3df,3pd)h−5.88−4.52 1.70OH•(H2O)2,mTTM potential b−14.86−−OH•(H2O)2,G3B3h−14.37−10.62 6.28HSO3•H2O,UB3LYP/6-311++G(3df,3pd)c−10.90−−HSO3•H2O,G3B3h−12.29−10.51−1.06HSO3•H2O,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−12.56−10.94−1.93HSO3•(H2O)2,G3B3h−24.10−20.76−2.30HSO3•(H2O)2,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−24.45−21.36−3.00HSO5(R)•H2O,G3B3h−17.28−15.28−4.88HSO5(R)•H2O,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−14.35−12.91−3.78HSO5(R)•(H2O)2,G3B3h−29.09−26.11−6.07a Li and McKee(1997);b Du et al.(2006);c Aaltonen and Fransisco(2003);d Fliegl et al.(2006);advanced multistep calculations involving RI-MP2-R12/def2-QZVPP and CCSD(T)/aug-cc-pV(Q+d)Z energies together with B3LYP/cc-pVTZ frequencies.e Larsen et al.(2000);f Kanno et al.(2006);g Alongi et al.(2006);h This workfor the HSO3+O2→→HSO5(TS)free energy change is +0.77kcal/mol,indicating that,as for the net Reaction(2a), the value is likely to be close to zero,and even more advanced methods would be needed to reliably determine the sign of the free energy difference.Nevertheless,it is clear from the higher-level data that net barrier for the HSO3+O2→→HSO5(P)process is unlikely to be larger than a few kcal/mol,which supports the experimental observations(Gleason et al.,1987;Gleason and Howard, 1988)that the reaction should be reasonably fast at ambient temperatures.3.2Effect of hydrationTable3shows the formation energetics of X•H2O and X•(H2O)2clusters computed at various levels of theory, with X=SO2,OH,HSO3,HSO5(R),HSO5(P),SO3and HO2.For simplicity,only G3B3and UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)results aregiven Fig.1.Minimum–energy structures(at the G3B3level)of (a)HSO3,(b)HSO5(R),(c)HSO5(TS)and(d)HSO5(P).Dashed lines correspond to hydrogen bonds.Color coding:yellow=sulfur, red=oxygen,white=hydrogen.from this work,see the supporting information for lower-level coupled-cluster values.The minimum-energy struc-tures of the hydrated clusters are shown in Fig.2.(The struc-tures correspond to the B3LYP/6-31G(d)geometries used in the G3B3calculations,since these are available for all struc-tures.Qualitatively,these were in most cases–see below for/9/3357/2009/Atmos.Chem.Phys.,9,3357–3369,2009Table3.Continued.cluster,method E elec H GHSO5(P)•H2O,G3B3h−11.69−10.03−0.29HSO5(P)•H2O,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−11.12−9.72−0.37HSO5(P)•(H2O)2,G3B3h−27.71−24.60−3.48SO3•H2O,RI-MP2-R12,CCSD(T)d−9.8±0.2−8.3±1.0−SO3•H2O,G3B3h−10.32−8.51−0.38SO3•H2O,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−9.76−8.12−0.59SO3•(H2O)2,B3LYP/6-311++G(d,p)e−21.86−−SO3•(H2O)2,MP2/6-311++G(d,p)e−21.87−−SO3•(H2O)2,G3B3h−22.26−18.42−0.03SO3•(H2O)2,UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)h−22.31−18.78−1.07HO2•H2O,experimental f−7.4±1HO2•H2O,G3g−9.14−7.42−0.53HO2•H2O,G3B3h−8.88−6.77 2.33HO2•H2O,UCCSD(T)/aug-cc-pVTZ//UB3LYP/6-311++G(3df,3pd)h−9.48−7.680.44HO2•(H2O)2,G3g−20.64−16.98−0.47HO2•(H2O)2,G3B3h−20.33−16.44 2.33HO2•(H2O)2,UCCSD(T)/aug-cc-pVTZ//UB3LYP/6-311++G(3df,3pd)h−21.12−17.590.62a Li and McKee(1997);b Du et al.(2006);c Aaltonen and Fransisco(2003);d Fliegl et al.(2006);advanced multistep calculations involving RI-MP2-R12/def2-QZVPP and CCSD(T)/aug-cc-pV(Q+d)Z energies together with B3LYP/cc-pVTZ frequencies.e Larsen et al.(2000);f Kanno et al.(2006);g Alongi et al.(2006);h This workthe single major exception–very similar to the UB3LYP/6-311++G(3df,3pd)geometries computed for some of the clus-ters.See the supporting information for all computed Carte-sian co-ordinates.)For the molecules for which previous data on hydrates are available(SO2,OH,HSO3,SO3and HO2),our re-sults are in fairly good agreement with previous studies. It should especially be noted that the binding energy pre-dicted for the OH•H2O complex using the UCCSD(T)/aug-cc-pVTZ single-point energy computed at the UB3LYP/6-311++G(3df,3pd)geometry is within0.005kcal/mol of that computed by Du et al.(2006)using a full RCCSD(T)/aug-cc-pVTZ geometry optimization.This indicates that the errors induced by the DFT geometry optimization for our hydrated radical complexes are likely to be relatively mi-nor,at least if the basis set is large enough.Similarly,it should be noted that our hydration enthalpies for HO2are all within the error margins of the experimental result by Kanno et al.(2006),and that our best value for the SO3•H2O binding energy is within the estimated error margins of that computed by Fliegl et al.(2006)using a combination of very advanced methods.The G3B3and UCCSD(T)/aug-cc-pV(T+d)Z//UB3LYP/6-311++G(3df,3pd)values are also in reasonable agreement with each other,except for the HSO5(R)•H2O cluster,for which the coupled-cluster bind-ing energy is almost3kcal/mol less than the G3B3bind-ing energy.(The difference in free energies is only about 1.2kcal/mol.)The reason for this difference may be the fact that,as pointed out by Majumdar et al.(2000),the geometries predicted at the B3LYP level using double-and triple-zeta basis sets(6-31G(d,p)and TZ2P++in their case)differ quite significantly from each other with regard to the SOH...OOS distance.With the smaller basis sets,the distance is pre-dicted to be rather short(1.71and1.75˚A for the6-31G(d,p) and6-31G(d)basis sets,respectively),corresponding to an intramolecular hydrogen bond,whereas calculations witha large basis set predict the distance to be much larger(2.74for both the TZ2P++and6-311++G(3df,3pd)basis sets).Presumably,the B3LYP calculations with larger ba-sis sets correspond at least somewhat better to the high-level wavefunction-based methods employed in the G3B3and CCSD(T)energy calculations,as indicated by the excellentAtmos.Chem.Phys.,9,3357–3369,/9/3357/2009/。

Possible Escape of a Recombinant Isolate of Potato virus Yby Serological Indexing and Methods of its DetectionR. P. Singh, Agriculture and Agri-food Canada, Potato Research Centre, P.O. Box 20280, Fredericton, NB, E3B 4Z7, Canada; D. L. McLaren, AAFC, Brandon Research Centre, P.O. Box 1000A, R.R. 3, Brandon, MB R7A 5Y3, Can-ada; X. Nie, Agriculture and Agri-food Canada, Potato Research Centre, P.O. Box 20280, Fredericton, NB, E3B 4Z7, Canada; and M. Singh, Agricultural Certification Services, 1030 Lincoln Road, Fredericton, NB, E3B 8B7, CanadaPotato virus Y (PVY) is the type-species of genus Potyvirus, a positive strand mo-nopartite RNA virus that infects many important food and vegetable crops worldwide including pepper, potato, to-bacco, and tomato (28). Several strain groups of PVY are recognized on the basis of symptoms in naturally infected potatoes (Solanum tuberosum) and tobacco (Nico-tiana tabacum) (7,15). The common strain (PVY O) induces mild to severe mosaic and leaf drop streaks in potato, and systemic mottle in tobacco. The tobacco veinal ne-crosis group (PVY N) induces very mild mottling in most potato cultivars with oc-casional leaf necrosis in some (3,15) and induces severe systemic necrosis of leaf veins and petioles in tobacco (7). The PVY NTN subgroup strains of PVY N causing potato tuber necrotic ringspot disease in-duce chlorotic mottle to mosaic symptoms in potato plants and superficial to deeply sunken necrotic rings in tubers, and the veinal necrosis symptoms in tobacco (17).Some partially characterized strains, includ-ing recombinants of PVY N and PVY O(2,4,15,20), the PVY C strains which inducestipple streak symptoms in potato cultivarbearing the Nc gene, and the PVY Z strainswhich overcome the resistance genes againstboth PVY O and PVY C (12,15), also exist.PVY O and the PVY N strains that infectpotato and tobacco have been known forseven decades (39). However, the generalgroup of PVY N, including PVY NTN (15,17)(referred to here as PVY N/NTN), and otherpossible recombinants of PVY O and PVY Nincluding PVY Z (2,12), isolate Wilga (4),and the isolates L-56 and L-136 (20,21)(the latter designated as PVY N:O [25]) havebeen recently recognized. In addition to theincreasing number of strains, the PVY N/NTNgroup has been assigned to European (Eu)PVY N/NTN and North American (NA)PVY N/NTN geographical subgroups (24).The diagnosis of PVY N/NTN strains hasbecome complex due to the incidence ofmixed infections (27,41,42) and increasingnumbers of strains and substrains (24).Bioassay and serological and molecularassays may be required to provide conclu-sive identification of strains (36). Thecomplex assay requirement precludeslarge-scale testing of seed tubers to preventunwanted strains in planting material.PVY strains have the potential to sig-nificantly reduce potato yield and quality,and therefore, PVY-free potato seed isrequired by potato certification programsin many countries (38). Although carefulsanitary measures reduce the infection andspread of PVY O, a minimal number ofPVY O-infected tubers in a seed lot can betolerated. In contrast, it is a common prac-tice in North America to limit the importa-tion or introduction of seed potatoes fromareas where even a low percentage of pota-toes may be infected with PVY N (1,31,33).Consequently, the North American PlantProtection Organization (NAPPO) ap-proved a set of recommendations for PVY Nrisk management, which included a panelof three monoclonal antibodies (MAbs)with differing specificity (see the NAPPOwebsite) to screen seed potatoes for PVY N.Accurate and speedy diagnosis of PVYand its strains is an important considerationin the effective management of the potatoseed crop. Diagnosis based on bioassay isgenerally reliable but time-consuming(29,36). Enzyme-linked immunosorbentassay (ELISA) is rapid but relies on strain-specific antibodies, with separate tests fordifferent antibodies, and the need forsprouted rather than dormant tubers(11,37). However, false positive results canoccur with ELISA, especially for thePVY N:O isolates, which may share PVY O-like coat protein but cause PVY N-likesymptoms in tobacco (20,21).Reverse transcription-polymerase chainreaction (RT-PCR) is a powerful tool forpotato virus diagnosis (22,23,32,41). TheP1 gene of the PVY genome has been pro-posed as the most variable region amongthe potyviruses (8), including the variousstrains of PVY (18). For example, by tar-geting the P1 gene, a 3-primer system candifferentiate between the Eu-typePVY N/NTN and NA-PVY N/NTN (36,43).Similarly, Eu-type, and NA-type PVY N/NTNcan be distinguished from all other PVY Nand PVY NTN isolates in a competitive RT-PCR based on sequence variation in the P1gene (24,25). However, a multiplex RT-PCR protocol, which would facilitate si-multaneous detection and differentiation ofboth PVY O and PVY N, including the re-combinant (PVY N:O) strains, may be ofpractical use for large-scale tests to man-age PVY N in seed certification programs.In this study, the distribution of thePVY N:O-like isolates and their possiblesources of introduction in Manitoba andABSTRACTSingh, R. P., McLaren, D. L., Nie, X., and Singh, M. 2003. Possible escape of a recombinantisolate of Potato virus Y by serological indexing and methods of its detection. Plant Dis.87:679-685.Surveys of commercial and seed potato fields for virus diseases (1998 to 2002) in Manitobaestablished that Potato virus Y (PVY) is of concern in seed potato production. To determine theprevalence of PVY strains, PVY-infected tubers identified by reverse transcription-polymerasechain reaction (RT-PCR) from surveys (2000 to 2001) were grown for symptom expression andstrain characterization by strain-specific RT-PCR, bioassays, and serological assays. Of thesamples collected (2000 to 2001) and tested by RT-PCR, 4.0% contained PVY. Further analysisof the PVY-positive samples by a duplex RT-PCR facilitating the simultaneous detection ofcommon (PVY O) and tobacco veinal necrosis strains (PVY N/NTN) indicated that 37.5% containedPVY O and 63.5% contained PVY N-type isolates. Analysis of the PVY N-type samples using threemonoclonal antibodies (MAbs) showed that all reacted with only the PVY O MAbs and not withthe PVY N-specific MAb. Partial nucleotide sequences of both ends of PVY-RNA showed thatthe PVY N-type isolates resembled those reported in 1996 from Manitoba. These isolates aredesignated as PVY N:O. In view of the increased incidence of PVY N:O in one production area,seed tubers imported from other provinces of Canada and the neighboring United States wereanalyzed for PVY N:O. The PVY N:O was detected in imported seeds from Minnesota, Montana,and North Dakota.Corresponding author: R. P. SinghE-mail: singhr@agr.gc.caAccepted for publication 22 January 2003.Publication no. D-2003-0331-02RThis article is in the public domain and not copy-rightable. It may be freely reprinted with custom-ary crediting of the source. The American Phyto-pathological Society, 2003.Plant Disease / June 2003 679679their detection using a duplex RT-PCR, which simultaneously differentiates be-tween the PVY O group and the PVY N/NTN group, is described.MATERIALS AND METHODSPotato samples and symptom expres-sion. In Manitoba, 6,201 tubers from 34 fields (2000) and 2,383 tubers from 12 fields (2001) were collected randomly and examined for tuber necrosis symptoms. Both seed and processing potato fields were sampled. In 2001, 228 leaf samples biased in favor of mosaic symptoms were also collected from 20 fields. The leaf and tuber samples were first tested for PVY by a duplex RT-PCR devised for the simulta-neous detection of Potato leafroll virus (PLRV) and PVY (34), and the samples identified as infected by PVY were used for determination of PVY strains.One seed piece from each PVY-infected tuber was planted in a 15-cm plastic pot containing a soil mix. Plants were grown in a greenhouse with 12 h light (90 µm-2 s-1) at 15 to 18°C to optimize virus symptoms (29). Symptoms were recorded every month for 3 months. Progeny tubers were examined for tuber necrosis symptoms. Search for PVY N:O in potato regions. To determine sources of PVY N:O introduc-tion into Manitoba, where potato seed is imported from a number of Canadian prov-inces (Alberta, British Columbia, Sas-katchewan) and the neighboring United States (Minnesota, Montana, North Da-kota), tubers and leaves were tested. Seed tubers were collected prior to planting in late April and early May of 2002, and leaves were collected in the first 2 weeks of J uly 2002. Except for Montana, two seed lots from each imported and five do-mestic seed sources were selected. One seed lot was selected from Montana. A random sample of 180 to 210 seed tubers per seed lot were tested. A field survey during the first 2 weeks of J uly (to avoid current season spread of PVY in fields planted with the imported seed sources) was conducted prior to the onset of aphid flights in Manitoba. Two thousand plants were observed in 10 randomly selected areas in each field, and leaves from plants showing mosaic symptoms were collected. Both seed tubers and leaves were tested, first by duplex RT-PCR described in this study, then by ELISA and bioassay for the strain identification as described below. Serological assays. Triple antibody sandwich-ELISA was conducted to verify PVY infection and to identify strains, using three PVY MAbs recommended by NAPPO. The MAb 4C3 detects both PVY O and PVY N (9), MAb2 is specific for PVY O (19), and MAb 1F5 (9) is specific for PVY N. Leaf sap (300 µl) from healthy plants or plants with mosaic or veinal ne-crosis symptoms was mixed with 300 µl of extraction buffer (20 mM phosphate buffer, pH 7.4, 0.15 M NaCl, 0.05% Tween 20, 2% polyvinyl pyrrolidone [PVP-40], 0.3%skim milk powder) and incubated at roomtemperature for 3 h. The leaf extract (100µl) was loaded in duplicate wells coatedwith a polyclonal PVY antibody (Phytodi-agnostics Inc., Vancouver, Canada) at1:5,000 dilution. The loaded plates wereincubated at 4°C overnight, and washedthree times with double-distilled (dd) H2O.Specific monoclonal antibodies were addedat 1:4,000, 1:2,500, and 1:5,000 dilutionsfor 4C3, 1F5, and MAb2 (PhytodiagnosticsInc., Vancouver, Canada), respectively, andincubated at 37°C for 2.5 h. Plates werewashed three times with ddH2O, and alka-line phosphatase conjugated antibodies(Jackson ImmunoResearch Laboratories,Inc., West Grove, PA) were added at1:3,000 dilution and incubated at 37°C for2.5 h. After washing three times withddH2O, 0.5% p-nitrophenyl phosphate wasadded to the wells and incubated at roomtemperature for 1 h. The resultant absorb-ance at 405 nm was measured. The thresh-old for a positive reading was 0.100 if thehealthy control absorbance was 0.030 orless. If the healthy control average wasgreater than 0.030, then the mean of thehealthy controls was multiplied by fourand used as the positive threshold. ThePVY O-139 tobacco culture (30) was usedas the positive control for PVY O, while thePVY N N-Jg tobacco culture (24) was usedas the positive control for PVY N.Bioassay.Nicotiana tabacum cv. Sam-sun and Solanum brachycarpum were usedto determine the pathotype of PVY (29).Seedlings (three-leaf stage) of N. tabacumand S. brachycarpum grown in 15-cm plas-tic pots containing a soil mix were me-chanically inoculated with PVY extracts.Briefly, leaves of PVY-infected potatoplants were ground with a mortar and pes-tle in the extraction buffer (0.01 M sodiumphosphate, pH 7.5, containing 0.4% so-dium sulfite) (1:10, wt/vol) and mechani-cally inoculated to N. tabacum and S.brachycarpum for symptom expression(29). The inoculated plants were kept inthe same conditions as described above.Symptoms were recorded weekly for 5weeks.Compositing of tuber, sprout, and leafsamples. To increase the efficiency for alarge-scale survey of PVY N:O-like isolatesin a potato crop by a duplex RT-PCR (seebelow), the PVY N:O-infected field growntubers were used for the production ofcomposite samples that included infected(I) and healthy (H) materials. Infected andhealthy tubers, sprouts, and leaves of threecultivars (Chieftain, Norland, and YukonGold) from the same seed lot were used toprepare the composites of tissues (data notshown), saps (A), and nucleic acid extracts(B). Buffered saps (see “Nucleic acid ex-traction”) from healthy and infectedsprouts or healthy and infected tubers werecombined in I:H ratios of 1:10, 1:20, 1:30,1:40, 1:50, 1:70, and 1:100 and used fornucleic acid extraction. The ratios were1:50, 1:100, 1:200, 1:400, 1:600, 1:800,and 1:1,000 for leaf samples. The nucleicacid extracts of individual healthy andinfected sample were combined to provideI:H ratios of 1:10, 1:50, 1:100, 1:200,1:400, 1:800, and 1:1,200 for tubers; 1:10,1:50, 1:100, 1:200, 1:400, 1:800, 1:1,200,and 1:1,500 for sprouts; and 1:100, 1:500,1:1,500, 1:2,000, 1:2,500, and 1:3,000 forleaf extracts. Tests with composited sam-ples were repeated by two people and re-peated five times by each person. In eachtest, tubers, sprouts, and leaves from threecultivars were used. Each test had threereplicate samples at each I:H ratio.Nucleic acid extraction. Nucleic acidswere extracted from leaves, tubers, andsprouts using sodium sulfite (35). For eachsample, 300 µl of extraction buffer (0.1 MTris-HCl, pH 7.4, 2.5 mM MgCl2, 0.65%Na2SO3, and 6 U of DNase I) was com-bined with 5 drops (150 to 200 µl) of sap,obtained by a Tuber Slicer (Electrowerk,Behcke and Co., Hannover, Germany).Incubation at 37°C for 10 min was fol-lowed by extraction with an equal volumeof phenol:chloroform:isoamyl alcohol(25:24:1, vol/vol/vol) and precipitation ofRNA from the aqueous phase with 1 vol ofisopropanol in the presence of 0.1 vol of 3M sodium acetate (–20°C, overnight). Theprecipitate was collected by centrifugation(12,000 ×g, 15 min, 4°C), washed with70% ethanol, dried under a vacuum, anddissolved in 1,000 µl of sterile water forleaf and sprouts and 100 µl for tuber sam-ples.RT-PCR. RNA extract (2.5 µl, 400 ng)plus 2.5 µl of water was incubated at 65°Cfor 8 min and chilled on ice for 3 min todenature the RNA. The RT mixture wasadded to provide a final concentration of20 ng/µl of reverse primer (see below)(24,25): 50 mM Tris-HCl, pH 8.3, 75 mMKCl, 10 mM DTT, 2.5 mM MgCl2, 1.5mM of each dNTPs, 20 U RNasin(Promega Corp., Madison, WI), and 200 UMoloney murine leukemia virus-reversetranscriptase (Gibco BRL). Samples wereincubated 1 h at 42°C for RT and subse-quently incubated at 95°C for 3 min toterminate the reaction.The initial determination of PVY wascarried out by a duplex method developedfor PLRV and PVY (34), and the secondduplex RT-PCR derived from a multiplexcompetitive RT-PCR (25) was used forPVY strains. It was performed using 2.0 µlaliquots of the cDNA mixture in 25 µlcontaining 10 mM Tris-HCl, pH 8.3, 50mM KCl, 1.5 mM MgCl2, 100 µM each ofdATP, dCTP, dGTP, and dTTP (Promega),0.1 µg each of the primers (reverse, 5 -CATTTGTGCCCAATTGCC-3 [A]; andforward, 5 -GACAGTTGGACTTTTGCA-ACG-3 [S7] for an amplified product of281 bp of PVY O, 5 -GGTGAAGCTAAT-CATGTCAAC-3 [S6] for an amplifiedproduct of 443 bp of PVY N/NTN [25]), and680 Plant Disease / Vol. 87 No. 6 680Plant Disease / June 2003 681 6810.625 U of DNA polymerase (PE Applied Biosystems, Foster City, CA). Samples were amplified for 30 cycles using a Peltier Thermal Cycler (M JResearch, Watertown, MA). Annealing temperature was 62°C for the first 5 cycles, 60°C for the next 5 cycles, 58°C for the following 10 cycles, and 55°C for the last 10 cycles. Each cycle consisted of denaturation (92°C, 30 s), primer annealing (30 s) and primer extension at 72°C (90 s), and a final extension of 10 min at 72°C. Amplified products (8 µl) were separated by electro-phoresis in a 1.5% agarose gel containing ethidium bromide at 0.5 µg/ml and photo-graphed under UV illumination with an imaging system (Alpha Innotech IS1000, San Leandro, CA).Two cDNA clones derived from 5 and 3 ends of four isolates (Mb-20, Mb-23, Mb-112, and Mb-119) from Manitoba causing tobacco veinal necrosis or mosaic symptoms were sequenced in each direc-tion as previously described (20,24) to verify the genotype of the isolates (data not shown).RESULTS Relative proportions of PVY strains. During 2000 and 2001, leaves and dormant tubers were analyzed for the presence of PVY . Combined samples (8,812) of com-mercial and seed fields were tested by a duplex RT-PCR for PVY and PLRV (34), and 361 samples (4.0%) were positive for PVY (Table 1, Processing and Seed com-bined). In seed fields, PVY incidence was 2.3%, and in processing fields, the inci-dence was 7.7% (Table 1). Of the total 289 (Processing and Seed combined, 2000) RT-PCR positive tubers in 2000, 236 germi-nated, and the daughter plants were used for the determination of PVY strains. Onthe basis of symptoms expressed in the tobacco bioassay, an equal number (50.0%, 75 each) of tobacco plants had mild mosaic or veinal necrosis symptoms when the plants were inoculated with the samples from processing fields of year 2000 (Table 2). This indicates an equal proportion of PVY O and PVY N -like infection in the samples collected from processing fields in that year. However, when samples col-lected from seed lots of year 2000 were tested, 36.0% (31/86) contained PVY O and 64.0% (55/86) had PVY N -like infection (Table 2). In 2001, about one-third (6/16 and 1/3 for processing and seed samples, respectively) of the PVY-positive leaves collected from processing and seed lots contained PVY O , whereas two-thirds (10/16 and 2/3 for processing and seed samples, respectively) had PVY N -like in-fection. In the tuber samples, the propor-tion of PVY N -like infection increased dra-matically, reaching over 94.1% (16/17) in the PVY-positive tubers collected from seed potatoes and 100% (36/36) in the processing tubers (Table 2). There was complete agreement in the tobacco bioas-say and the RT-PCR results of these sam-ples (Table 2).A duplex RT -PCR for simultaneous detection of PVY O and PVY N group of strains in potato tubers and leaves. The proportion of PVY N -like infection in to-bacco was unexpectedly high in the popu-lation of PVY (Table 2) originating from potato samples, and this necessitated a large-scale routine testing of potato seed lots. To facilitate the simultaneous detec-tion of PVY O and PVY N -like strains in a routine indexing of potato samples, a modification of the tetraplex-competitiveRT-PCR (25) was carried out. The tetra-plex-competitive RT-PCR (25) showed that the PVY N/NTN from Manitoba was ampli-fied by primers specific to Eu-type PVY N/NTN (Fig. 1A, lanes 5 to 7) but not by the NA-type PVY NTN (Fig. 1A, lane 14). Since only two strains were regularly encountered in Manitoba tuber samples, a duplex-competitive RT-PCR derived from the tetraplex PCR, using primer S6 for amplification of PVY N/NTN and S7 for PVY O (25), was adopted. S6 and S7, when paired with the A, resulted in a fragment of 443 bp for PVY N -like strains and a frag-ment of 281 bp for PVY O (Fig. 1B). Analysis of tobacco plants with mosaic symptoms using duplex RT-PCR con-firmed that they contained only PVY O -specific PCR fragments (Fig. 1B, lanes 8, 12, 15, and 17), while those with the veinal necrotic symptoms contained PVY N/NTN -specific fragments (Fig. 1B, lanes 1 and 4). Differentiation of the PVY O and PVY N/NTN strains on the original potato tuber and leaves was also confirmed by duplex RT-PCR (data not shown). In addition, the duplex-RT-PCR of tobacco leaves showedthe existence of several doubly infected (PVY O + PVY N/NTN ) plants (Fig. 1B, lanes 2, 3, 5 to 7, 9 to 11, 13, 14, 16, and 18 to 20), and the virus titer based on band in-tensity of each strain in the doubly infected plants was variable without favoring a particular strain. Nature of PVY N -like isolates. S. brachycarpum is an indicator plant inwhich both PVY N and PVY O strains can be differentiated by the lethal necrosis or themosaic symptom they produce (29). When S. brachycarpum was inoculated with to-bacco sap from plants used in the RT-PCRstudies with mosaic or veinal necrosissymptoms (five samples of each), none ofthem developed lethal necrotic symptoms typical of PVY N . Although both resulted in mosaic symptoms similar to PVY O in S.brachycarpum plants, there was an in-creased crinkling of the leaves inoculatedwith the tobacco plants with necrotic symptoms compared to those with mosaic symptoms. When ELISA was carried out with vari-ous antibodies using tobacco leaves, theMAb 4C3 detected all samples from symp-Table 2. Incidence of Potato virus Y (PVY) strains in potato in Manitoba as determined by bioassay in tobacco and reverse transcription-polymerase chain reaction (RT-PCR)Processing SeedYear No. tested PVY Oa PVY Na No. tested PVY O PVY NBioassay2000 (tubers) 150 75 (50.0%) 75 (50.0%) 86 31 (36.0%) 55 (64.0%) 2001 (leaves) 16 6 (37.5%) 10 (62.5%) 3 1 (33.0%) 2 (67.0%) 2001 (tubers) 36 0 (0.0%) 36 (100.0%)17 1 (5.9%) 16 (94.1%) RT-PCR b2000 (tubers) 150 75 (50.0%) 75 (50.0%) 86 31 (36.0%) 55 (64.0%) 2001 (leaves) 16 6 (37.5%) 10 (62.5%) 3 1 (33.0%) 2 (67.0%) 2001 (tubers) 36 0 (0.0%) 36 (100.0%)17 1 (5.9%) 16 (94.1%)a PVY O is the common strain of PVY; and PVY N is the tobacco veinal necrotic strain of PVY .b PVY strain specific competitive RT-PCR described in this study.Table 1. Incidence of Potato virus Y (PVY) in potato in years 2000 and 2001 in ManitobaProcessing a Seed aYear No. tested PVY No. tested PVY 2000 (tubers) 2,277 175 (7.7%) 3,924 114 (2.9%)2001 (leaves) 67 16 (24.0%) 161 3 (1.9%)2001 (tubers) 598 36 (6.0%) 1,785 17 (1.0%) Total 2,942 227 (7.7%) 5,870 134 (2.3%) a Samples were tested by a duplex reverse transcription-polymerase chain reaction for PVY and Potato leafroll virus (PLRV) (34).682 Plant Disease / Vol. 87 No. 6 682tomatic leaves in which A 405 was signifi-cantly higher than that of healthy controls as PVY-positive (Table 3). When MAb2, the antibody specific to PVY O , was used, a high reading of A 405 was recorded for sam-ples with symptoms, regardless of the symptom type (Table 3). None of the sam-ples reacted with the PVY N -specific MAb 1F5.To ascertain if differences at the molecu-lar level existed in PVY N -like isolates, partial nucleotide sequence of the 3 and 5 ends of mosaic isolates (Mb-20 and Mb-23) and tobacco veinal necrotic symptom causing isolates (Mb-112 and Mb-119) was determined (data not shown). The se-quences of isolates (Mb-20 and Mb-23) exhibiting mosaic symptoms were identical to that of PVY O (30) in both ends of the genome. However, sequences of the iso-lates (Mb-112 and Mb-119) causing to-bacco veinal necrotic symptoms were simi-lar to that of PVY O in the 3 end, but different in the 5 end. In fact, they were similar to Eu-PVY N/NTN sequences such as PVY N -605 (GenBank accession number: X97895) in the 5 end (data not shown). The isolates appeared to possess similar genomic properties to the ones reported earlier from the same area (21) (data not shown).Absence of tuber necrosis symptoms. None of the PVY-infected samples col-lected from six potato cultivars (Chieftain, Norland, Russet Burbank, Russet Norko-tah, Shepody, and Yukon Gold) had rings-pot necrosis symptoms in the original field-grown tubers, or in the progenies grown in the greenhouse from the infected tubers (data not shown). Thus, these iso-lates that possess the coat protein region of PVY O causing veinal necrotic symptoms in tobacco similar to PVY N , and that lack the ability to cause potato tuber ringspot ne-crosis symptoms, are different from PVY NTN . Because of the unique genomic and pathological characteristics, and to differentiate these isolates from typical PVY N/NTN , they have been referred to as PVY N:O group of isolates.Sensitivity of PVY N:O detection in composite samples. In the composite tuber sap samples, detection of PVY N:O was unaffected by I:H ratios up to 1:100 in the two cultivars (Norland and Yukon Gold) (data not shown) but it was limited to 1:50 in cv. Chieftain (Fig. 2A, lane 5). In the composites of sprout sap up to 1:100 (the highest tested) (Fig. 2A, lane 14) and in the potato leaf sap up to 1:1,000 (Fig. 2A, lane 21), PVY N:O bands were observed. When extracted RNA from individual samples was used to prepare composites, the sensi-tivity of detection was extended to 1:1,200 to 1:1,500 in tubers and sprouts (Fig. 2B, lanes 1 to 7, 8 to 15) and over 1:2,000 in leaves (Fig. 2B, lanes 16 to 21). The am-plified bands were more intense in the composites of sprouts in contrast to the composites of tuber sap or tuber RNA (Fig. 2A and B). RNA extracts prepared from leaves appeared to be concentrated and sometimes needed further dilution to re-duce nonspecific amplifications.Search for PVY N:O strains in other po-tato growing areas. Most of the PVY N:O -infected plants developed mosaic symp-toms under greenhouse conditions similar to the field symptoms of PVY O -infected plants. Therefore, it appeared feasible to select potato plants on the basis of leaf symptoms during the growing season and determine the distribution of strains. In 2001, leaf sap from 1,625 leaves with mo-saic symptoms from fields in New Bruns-wick and Prince Edward Island, inoculated to tobacco, failed to develop veinal ne-crotic symptoms. At the same time, 19 leaf samples with mosaic symptoms from a field known to have PVY N:O infection inTable 3. Differentiation of Potato virus Y (PVY) strains in potato by a three antibody panel in enzyme-linked immunosorbent assay NAPPO a -recommended monoclonal antibodies average A 405 ± SD Year Symptoms in tobaccoNo. tested 4C3b (PVY) MAb2c (PVY O ) 1F5d (PVY N ) 2000 Mosaic 105 2.46 ± 0.50 2.83 ± 0.50 0.03 ± 0.02 2000 Necrosis 130 1.72 ± 0.71 2.74 ± 0.56 0.02 ± 0.04 2000 Healthy 50 0.05 ± 0.02 0.09 ± 0.05 0.02 ± 0.02 2001 Mosaic 10 1.48 ± 0.78 2.86 ± 0.13 0.03 ± 0.03 2001 Necrosis 54 1.90 ± 0.48 2.85 ± 0.08 0.03 ± 0.01 2001Healthy100.02 ± 0.010.01 ± 0.010.01 ± 0.01a North American Plant Protection Organization.b Monoclonal antibody 4C3 detects both the common (PVY O ) and the tobacco veinal necrotic (PVY N ) strains. c Monoclonal antibody MAb2 detects PVY O strain.d Monoclonal antibody 1F5 detects PVY Nstrain.Fig. 1. A, Nucleic acid extracts from dormant tubers infected with common strain of Potato virus Y (PVY O ), recombinant isolate of PVY (PVY N:O ), or doubly infected with PVY O + PVY N:O were ana-lyzed by a multiplex (tetraplex) reverse transcription-polymerase chain reaction (RT-PCR) for their strain groups. PVY O , lanes 1 to 3, 13; PVY N:O , lanes 5 to 7; PVY O + PVY N:O , lanes 8 to 12; North American (NA)-PVY NTN , lane 14; European (Eu)-PVY N/NTN , lane 15; negative control, lane 4; and DNA molecular markers, lanes M. B, Nucleic acid extracts from potato tubers infected by PVY O , PVY N:O , or PVY O + PVY N:O analyzed by a duplex RT-PCR. Top bands indicate PVY N/NTN (all PVY N -like isolates, including PVY N:O ), bottom bands are PVY O , and presence of two bands indicates double-infection by both strains. Lanes at both ends of gel are DNA size markers.。

Arsenic removal in synthetic ground water using ironelectrolysisLei Li a ,b ,Jun Li a ,Chen Shao a ,Kejia Zhang a ,c ,⇑,Shuili Yu a ,⇑,Naiyun Gao a ,Yang Deng d ,Daqiang Yin eaState Key Laboratory of Pollution Control and Resources Reuse,College of Environmental Science and Engineering,Tongji University,Shanghai 200092,China bDepartment of Civil and Environmental Engineering,University of California,Berkeley,Berkeley,CA 94720,USA cDepartment of Civil Engineering,Zhejiang University (Zijin gang Campus),Hangzhou 310058,China dDepartment of Earth and Environmental Studies,Montclair State University,Mallory Hall 252,1Normal Ave,Montclair,NJ 07043,USA eKey Laboratory of Yangtze River Water Environment,Ministry of Education,College of Environmental Science and Engineering,Tongji University,Shanghai 200092,Chinaa r t i c l e i n f o Article history:Received 23June 2013Received in revised form 6November 2013Accepted 7November 2013Available online 15November 2013Keywords:Iron scrapElectrocoagulation Arsenic removalSustainable water treatment Groundwatera b s t r a c tElectrocoagulation (EC)using electrodes made from iron scrap is a novel and promising strategy for arsenic (As)contaminated ground water remediation.In synthetic groundwater,amorphous hydrous fer-ric oxide (HFO)precipitates formed by the rapid dissolution of a sacrificial iron scrap anode adsorbed As very effectively.A competitive adsorption model developed in this study with parameters fitted for As and other coexisting anions (phosphate and silicate)was in good agreement with the observed results.It is indicated that the maximum adsorption capacity of HFO generated in the EC system was $0.70mol/mol.Reducing the As concentration in water from 500l g/L As(V)and As(III)to below 50l g/L (local drinking water standard in Bangladesh)required $8mg/L and $32mg/L iron respectively (pH =7.1±0.1,charge dosage rate =3coulomb/L/min).It was found that coexisting cations (Ca 2+and Mg 2+)neutralized the HFO surface charge,promoted aggregation and resulted in greater As removal.The presence of humic acid exhibited a negligible effect on As removal and HFO precipitate settling.Jar tests showed that the turbidity of the solution could be reduced to <1NTU with the addition of 2mg/L Al 3+.Ó2013Elsevier B.V.All rights reserved.1.IntroductionTens of millions of people worldwide are exposed to toxic con-centrations of naturally occurred arsenic (As)in groundwater drinking supplies [1,2].In Bangladesh,an estimated one third of tube wells deliver groundwater with As concentrations higher than Bangladesh’s standard of 50l g/L [3],and As accounts for one fifth of adult deaths [4].The United States Environmental Protection Agency (EPA),the World Health Organization (WHO)and some developing countries such as China have decreased the maximum contaminant level of arsenic in drinking water from 50to 10l g/L [5–7].Among the several proven technical approaches [8–10]for removing arsenic from municipal water supplies,iron-based strategy (i.e.chemical coagulation (CC)by Fe(III))is widely ac-cepted because of its high capacity for arsenate (As(V))adsorption and low cost [11,12].However,arsenite (As(III)),which is much more mobile and toxic than As(V)and accounts for up to 67–99%of the total As in groundwater [13],has orders of magnitude less affinity with Fe(III)precipitate than As(V)and other coexisting competitors such as Phosphate (P)[12,14].Therefore,As(III)is usually pre-oxidized to As(V)using an oxidant (e.g.ferrate ,chlorine,UV radiation,permanganate)to improve the removal effi-ciency [9,15].Much of recent research has focused on Fenton and Fenton-like reagents such as Fe(II)/H 2O 2,ZVI/O 2,and Fe(II)/O 2[14,16–18],since the intermediate production could oxidize As(III)to As(V),which could be easily absorbed by amorphous hydrous ferric oxide (HFO)precipitates formed afterwards.As a result,less iron is required as compared to direct adsorption [14].Electrocoagulation (EC),based on the generation of Fe(II)through the rapid dissolution of a sacrificial Fe(0)anode,is a prom-ising As removal strategy for drinking water as,(1)it is efficient,low cost and easy to maintain and operate with locally available materials [19,20],(2)EC introduces Fe(II)/Fe(III)[21]without intro-ducing undesirable anions into the solution,(3)the release of H 2(g)from the cathode [22]neutralizes the consumption of hydrox-ide by the Fe(III)hydrolysis and therefore likely to buffer the system better than CC,and (4)the gradual release of Fe(II)/Fe(III)in EC may produce intermediate oxidants that enhance the efficiency of As(III)oxidation as compared to CC [14,23].In addition,using electrodes made of iron scrap,an abundant byprod-uct from iron planing machines,would further reduce the material cost of EC compared with using iron plates.1383-5866/$-see front matter Ó2013Elsevier B.V.All rights reserved./10.1016/j.seppur.2013.11.012⇑Corresponding authors.Addresses:State Key Laboratory of Pollution Control and Resources Reuse,College of Environmental Science and Engineering,Tongji University,Shanghai 200092,China,Department of Civil Engineering,Zhejiang University (Zijin gang Campus),Hangzhou 310058,China (K.Zhang,S.Yu).E-mail addresses:zkj1025@ (K.Zhang),ysl@ (S.Yu).Previous EC researchers have mostly focused on the effect of design and operation parameters(current density(current per elec-trode area,amps/cm2),electrode distance and conductivity,pH)or water matrix(different initial As,P and Si concentrations)on As removal,and proposed some qualitative conclusions[11,12,19, 22,24],which were mainly applicable only under the particular con-ditions in which the data were taken.In addition,the effect of typical co-existing substances such as Ca2+,Mg2+and natural organic matter (NOM)on HFO precipitate formation and As removal in EC systems has not been previously reported,despite the fact that these substances exhibited great effects on HFO particle size and As re-moval efficiency in other similar As removal methods[15,25–27]. Moreover,the separation of HFO precipitates from EC system,one of the most significant steps for drinking water treatment,has rarely been explored in the literature.This paper reports the successful application of iron scrap electrolysis on arsenic remediation,discusses the redox reactions in the EC system,quantifies the effects of P and Si on As(V)and As(III)adsorption based on a competitive adsorption model and X-ray diffraction patterns,evaluates the effect of other co-existing substances(Ca2+,Mg2+and humic acid)in groundwater on As oxi-dation and adsorption,andfinally optimizes Al3+concentration and other parameters for better HFO sludge separation.2.Experimental procedures2.1.Chemicals and experimental set upAll chemicals were reagent grade or higher.Experiments were conducted in synthetic Bangladesh ground water(SBGW)contain-ing8.2mM NaHCO3, 2.5mM CaCl2, 1.6mM MgCl2,500l g/L As(III)/(V),3mg/L P and30mg/L Si according to British Geological Survey(BGS)[28]and previous study[14]for better comparison unless otherwise noted.Batches of SBGW were prepared by adding NaHCO3,MgCl2,Na2HPO4,and Na2SiO3as solids to ultrapure 18M X water in sequence under vigorous stirring.The pH was then reduced to$8by bubbling CO2(g).CaCl2stock solution(5%w/v) was added subsequently[14].As(III)or As(V)was added before adjusting pH to7.0by bubbling CO2(g).All batches were aged at least1h after all components had been added and then sampled to verify the initial concentrations of P,Si,As(III),and As(tot)[23].All experiments were conducted in a1-L glass beaker.The spring-shaped iron scrap(origin steel type:41CrAlMo74)were twist together to form solid electrodes before submerged in the SBGW and connected with the power supply by copper wires.Prior to experiments,electrodes were chemically cleaned with1%HCl and rinsed by ultrapure water3times to remove the iron oxides and any passivefilm that may have formed.Samples taken from the reactor under various electrolysis duration were mixed for 2h allowing complete Fe(II)oxidation and maximum As adsorption.Then,unfiltered samples were taken to determine total (dissolved and adsorbed)As(As(tot)).A second set of samples was filtered through0.45-l m nylonfilters to determine dissolved/ aqueous As,P and Si.2.2.Chemical analysisAs(III)and As(tot)concentrations were determined using a hy-dride generation atomicfluorescence spectrometer(AFS-230E).To selectively detect As(III),procedures were adopted from Roberts et al.[14].P,Si and Fe(III)were determined with ICP-OES or ICP-MS for low concentrations.All the detection procedures were done right after the experiment and the relative standard deviations (RSD)for all the determinations were<10%(normally<4%).A ferrozine method was used to determine the concentrations of dissolved and total Fe(II)[29].The suspension under various electrolysis duration in EC system were subjected to particle size detection at a90degree scattering angle using Dynamic Light Scat-tering,as well as zeta potential detection using Laser Doppler Microelectrophoresis(Zetasizer Nano ZS90,Malvern)within 10min after sampling.The deviations between repeated experi-ments were<10%if error bars are not shown.2.3.X-ray diffractionPowder diffraction data were collected at beamline11-ID-B of the Advanced Photon Source located at Argonne National Labora-tory(Argonne,IL).Air-dried samples were packed into3mm diameter polyimide tubes and diffraction data were obtained with 58keV(0.2128Å)X-rays.Radiation scattered from the sample was collected on an amorphous silicon MAR-345image plate detector and processed using the Fit2-D program[30].Diffraction data from a CeO2standard were used to calibrate the sample-to-detector distance and tilt angle of the detector.Diffraction data were also collected for2-line ferrihydrite prepared following the Schwert-mann and Cornell recipe[31].2.4.Jar test procedureAl2(SO4)3was newly made and added to the post-electrolysis solution prior to coagulation/flocculation in a1L jar tester run at 200RPM for2min,90RPM for6min and30RPM for9min.The supernatant was then sampled after different settling times for As and turbidity tests.3.Results and discussion3.1.Role of the electrodesWhich redox reactions(e.g.the mechanism of Fe(0)dissolution and As(III)oxidation)occur on the electrodes in the EC system has been debated[21,32].Reactions that could potentially be occurring on the electrodes are discussed in this section.As electrodes were exposed to the water and oxygen,Fe(0) would be sacrificed through electrolysis(Eqs.(1),(2))and natural corrosion(Eq.(3)).Fig.SI1shows that Fe(II)(total bivalent Fe)gen-erated in the system accounted for over90%of the total Fe (Fe(II)+Fe(III))while the solution was sealed and purged with N2 during the electrolysis(DO was kept below1mg/L),implying that Fe(II)instead of Fe(III)was generated through the sacrifice of the anode.This conclusion is consistent with previous research with a similar ground water recipe in an EC system[21].In addition, Fig.SI2shows that the total iron concentration matched well(error <15%)with the value calculated using Faraday’s law(Eq.(4),where m is mass(g)of iron oxidized at a specific current,I is current(A),t is the time(s),M is the molecular weight of iron,Z is the number of electrons involved,and F is the Faraday constant(96,485.3cou-lomb/mole))under both high and low charge dosage rates(24 and3coulomb/L/min,the corresponding currents and voltages were0.4A,$24V and0.05A,$3V).Thisfinding is consistent with the report from Lakshmanan et al.[21].When the electrode was submerged in the SBGW without current,$1.1mg/L iron was de-tected after30min exposure,indicating that natural corrosion of the electrode contributed negligibly to HFO generation.FeÀ2e!FeðIIÞð1ÞFeÀ3e!FeðIIIÞð2ÞFeþO2!FeðIIÞ=FeðIIIÞð3Þm¼IÂtÂMZÂFð4Þ226L.Li et al./Separation and Purification Technology122(2014)225–230It should be kept in mind that the redox reaction on the electrodes strongly depends on the water matrix.For instance,increasing P concentration to0.01M in SBGW decreased the iron concentration to less than half of that in the control test.Similarly,the detected iron concentration after the electrolysis was<10%of the calculated value through Faraday’s law when the test water merely contained NaNO3(0.1M)rather than all the chemicals used in other tests.This probably indicated some other electron donors(such as OHÀ) outcompeted Fe(0)to be oxidized on the anode during electrolysis.3.2.Adsorption properties of HFO precipitatesThe X-ray diffraction pattern of the iron precipitate obtained in SBGW under the current dosage rate of3coulomb/L/min(i.e. SBGW-3C/L/min)is presented in Fig.1.It exhibits two peaks simi-lar to the characteristic peaks of2-line ferrihydrite(2L-Fh)at d space approximately0.148and0.255nm.The peaks in this study were broader and the primary peak was shifted to0.270nm com-pared to0.255nm for2L-Fh,which was in good agreement with Voegelin et al.[33]and Carlson and Schwertmann[34],who claimed the high concentration of Si reduced the crystallinity and resulted in the peak drifting.For a much higher charge dosage rate(24coulomb/L/min)(i.e. SBGW-24C/L/min in Fig.1)in the EC process and higher Fe(II)con-centration in the CC processes(i.e.SGBG-CC(Fe(II)in Fig.1),X-ray diffraction exhibited a similar pattern,aligned with our wet chem-istry analysis that the adsorption capacity of As(V)and P under various charge dosage rates were quite similar(data not shown). This conclusion is consistent with an EXAFS study by van Genuch-ten et al.[35],which showed that both Fe and As K-edge spectra were similar between samples across a wide range of charge dos-age rates(0.06–18C/L/min).Besides the dosage rate,HFO adsorption properties might de-pend on water matrix.In Fig.1,different peak patterns were ob-served for SBGW without Si.The peak at0.270nm was replaced by two peaks at$0.252and$0.323nm,and a new distinct peak at0.197nm appeared.The altered and sharper peaks indicated that the HFO was more lepidocrocite(Lp)-like,was more crystal-line[26]and might has less adsorption capacity.Recent reports indicated that dissolved Si at Si/Fe molar ratios>0.5would result in the formation of amorphous short-range-ordered hydrous Fe(III)-precipitates[33].Given that Si concentrations of 19.2±4.7mg/L have been detected in water from Bangladesh ground water wells[28],both SBGW and real ground water in Bangladesh probably belong to the same category of silicate-rich hydrous ferric oxide(Si-HFO).Based on the results presented in this section,HFO in the EC system might be considered to be a uniform adsorbent regardless of the charge dosage rate and water matrix as long as the Si concentration is in similar level.3.3.Adsorption modelingAccording to the previous section,it is valid to treat the HFO as a uniform adsorbent under the various conditions in this study, and necessary to develop an adsorption model to quantitatively evaluate the effect of the anions that compete with As for adsorption.As assumed in Eq.(5),the number of adsorption sites (…Fe A OH)of HFO(…Fe A OH)should be proportional with Fe(III) concentration and the adsorption site concentration q(site/Fe(III)). The competitive adsorption of the anions is described as a set of fast and reversible equilibrium reactions with the sorption sites as shown in Eq.(6).B FeÀOH¼FeðIIIÞÂqð5ÞXþB FeÀOH B FeÀX K Xð6Þwhere X represents As(V),As(III),P or Si and K x represents the corresponding adsorption constant.The modeled adsorption con-stants of As(V),As(III),P and Si to Fe(III)precipitate and the adsorp-tion site concentration(q)in SBGW in the EC system are summarized in Table1according to the data from Figs.2and3 and Table SI1(refer SI for detail modeling procedure).As shown, the adsorption site concentration for HFO produced by EC was 0.70mol/mol iron,quite similar to the adsorption concentration for HFO produced by CC(0.71mol/mol iron)[14],considering the experimental andfitting errors.In addition,adsorption capacity of precipitate derived from Fe(II)is considerably higher than that of precipitate coming directly from Fe(III)(0.44mol/mol iron)[14]. However,diffractgram patterns did not show a crystallinity differ-ence(Fig.1).The difference in adsorption capacity likely ascribed to quick cross-linkage of the small Fe(III)polymeric units to form larger aggregates in which a considerable portion of the adsorption sites were no longer accessible[14],while in the case of Fe(II)or EC, Fe(III)precipitate was gradually formed from the Fe(II)oxidation, giving time for As,P and Si to migrate to the adsorption sites before they aggregated.As(V)removal in SBGW as a function of iron concentration in the EC system is shown in Fig.2.Approximately8mg/L of iron was required to reduce As(V)concentration from500to50l g/L (local standard of Bangladesh).P removal followed the same trend as As,while Si was hardly removed since its adsorption constant is orders of magnitude less than those of As(V)and P(Table1).The experimental and modeled data matched verywell.Table1Fitted adsorption constants and sorption site concentrations in EC and CC systems.EC a Fe(II)b Fe(III)bLog(K As(V)) 5.42±0.07 5.72±0.23 5.97±0.12Log(K As(III)) 4.10±0.04 3.67±0.11 4.47±0.07Log(K Si) 3.04±0.01 2.77±0.08 3.36±0.11Log(K P) 6.48±0.06 5.87±0.15 6.07±0.04[…Fe]/[Fe0]0.70±0.030.71±0.050.44±0.02a Data were subdivided into2independent sets each by taking every second datapoint through the successive data points shown in Figs.2and3,Fig.4(a)andTable SI1.Similar optimized values were obtained,indicating the model were wellconstrained.b Data adopted from Roberts et al.[14].L.Li et al./Separation and Purification Technology122(2014)225–2302273.4.As(III)oxidationOne of the recognized advantages of the EC process for As(III) removal is the As(III)oxidation during the simultaneous oxidation of Fe(II)by DO[24].As(III)oxidation and adsorption as well as the removal of other co-existing anions in the EC system were investi-gated in detail in this study,allowing for a deeper understanding of how these ions behave during EC.To examine the intermediate oxidant generated in EC system, 2-propanol in excess(14mM)on As(III)oxidation was found negligible in this study,which is consistent with the As(III)oxidant being an Fe(IV)species generated as an intermediate during the oxidation of Fe(II)in SBGW[36].As a result,Fe(IV)was supposed as the plausible intermediate product of oxidizing Fe(II)with DO as briefly expressed in Eq.(7).Then,Fe(IV)would be consumed by Fe(II)and As(III)according to Eqs.(8)and(9).K1and K2are the reaction rates of Fe(IV)with Fe(II)and As(III),respectively. Therefore,the amount of Fe(IV)consumed by As(III)(Fe(IV)As(III)) can be expressed by Eqs.(10)and(11).Accordingly,the mole ratio of As(III)to Fe(II)(R As(III)/Fe(II))was the controlling factor for As(III) oxidation efficiency[23].Fortunately,Fe(II)is generated gradually during EC as opposed to the one step Fe(II)dosage in CC.Gradual release of Fe(II)would result in a high R As(III)/Fe(II)value and there-fore enhance As(III)oxidation.As a result,the amount of iron required to reduce As(III)from500to50l g/L in the EC system (pH7.1±0.1,charge dosage rate3coulomb/L/min)was$32mg/ L,considerably below that in a Fe(II)CC system($50mg/L)under the same ions background[14].This improvement greatly reduces the iron scrap dosage and the cost of iron sludge disposal,as well as DO consumption caused by Fe(II)oxidation would therefore guarantee the oxidizing condition in the system.Simultaneous with As(III)oxidation,total As(V)concentration greatly increased in the initial stage and leveled off to$335l g/L as illustrated in Fig.3.The corresponding aqueous As(V)increased with the same trend when iron dosage was below$3mg/L,indi-cating minimum As(V)was adsorbed at this stage.It might be due to the presence of a much greater amount of P.Afterwards, aqueous As(V)concentration decreased and leveled off to0due to the complete removal of P.3FeðIIÞþO2!...!FeðIVÞð7ÞFeðIVÞþFeðIIÞ!2FeðIIIÞK1ð8ÞFeðIVÞþAsðIIIÞ!AsðVÞþFeðIIIÞK2ð9ÞFeðIVÞAsðIIIÞ¼K2½AsðIIIÞ =ðK2½AsðIIIÞ þK1½FeðIIÞ Þð10ÞFeðIVÞAsðIIIÞ¼1=ðK1½FeðIIÞ =K2½As½III þ1Þð11Þ3.5.Effects of Ca2+and Mg2+In SBGW,Ca2+/Mg2+were observed to have great impacts on precipitate formation and As removal(Fig.4).Without Ca2+/Mg2+228L.Li et al./Separation and Purification Technology122(2014)225–230(using equivalent NaCl to keep the same iron strength of the solu-tion),no higher than13%,15%and19%of iron,As and P respec-tively werefilterable by a0.45l m membrane when the iron concentration were below17mg/L(Fig.4(b)).With the present of Ca2+/Mg2+(Fig.4(a)),on other hand,nearly100%of iron wasfil-terable,leading to much greater removal rate of P and As.This may be mainly ascribed to the neutralization of surface charge of HFO by Ca2+/Mg2+,which facilitates its aggregation.As shown in Table2, the adding of Ca2+/Mg2+greatly increased the zeta potential of HFO from$À30mV to$À10mV,and enhanced HFO aggregation with the particle size increased from15.3,48.2and123.5to884.4,905.6 and963.6nm accordingly,which is consistent with previous re-port[25].Of note,the portion offilterable iron dramatically in-creased when the iron concentration was over18mg/L,which probably due to the increasing of HFO particles size caused by a higher particles density.In addition,the Ca2+/Mg2+in HFO precip-itate(filterable Ca2+/Mg2+)accounted for$10%of the total amount of Ca2+/Mg2+,indicating that$0.40mM Ca2+/Mg2+might be suffi-cient for HFO surface charge neutralization.Fortunately,most of the ground water found in Bangladesh contains sufficient levels of these cations[3].3.6.Effect of natural organic matter(NOM)NOM,another common compound in shallow ground water or contaminated deep ground water,has been reported to interfere with As removal by competing for adsorption sites[27,37],increas-ing time required to reach equilibrium[27],reducing the settling ability of the precipitate[15],and potentially interfering with As(III)oxidation by interacting with reactive oxygen species.As previously reported research of NOM effects on As removal were conducted under various conditions and with different water matrices,which may be different from As removal under SBGW background in the EC system,this research also investigated the effects of NOM.Humic acid(HA)was added as the surrogate to the water matrix to evaluate the overall effect of NOM on As(III) oxidation and adsorption(Fig.SI3).For HA concentrations of0,5 and15mg/L the remaining respective As(III)concentrations were 150,137and125l g/L total As(III),47,45,and45l g/L.In addition,the remaining HA was under10%of the initial concentration, implying different removal pathways for HA and As in this system. Moreover,the turbidity of HFO and its settling properties were not significantly affected by the addition of HA.The lack of an effect of HAfinding in this research is inconsistent with previous reports [15,37].This is probably due to the co-existing Ca2+/Mg2+in ground water neutralizing the surface charge of the Fe(III)-HA complex [25]and therefore minimizing the effect of HA on HFO properties and As removal.Further study is warranted to make discussion in detail.4.Jar testsAlthough the Fe(II)has been shown to have higher adsorption capacity than Fe(III)(Table2),the precipitate attained from Fe(II) was harder to settle than that attained from Fe(III)according to our tests and the literature[14].Jar tests were therefore conducted to optimize operation parameters to enhance HFO settling and sludge separation.Subsequent to electrolysis,the solution was mixed for60min to ensure the complete oxidation of Fe(II)(final Fe(II)/Fe(III)ratio was<3%).Of note,to simulatefield conditions, pH was not controlled,and increased to$7.7during the mixing. Results in Fig.5showed that the turbidity would decrease from $140to54NTU after30min of settling without coagulant,while the turbidity removal was greatly enhanced with the addition of Al3+at concentrations of1,2,3,5,and8mg/L.The corresponding terminal turbidies were 1.2,0.67,0.91, 1.2and 1.5NTU after 120min of settling.In other words,2mg/L Al3+was sufficient to reduce turbidity to below1NTU after the clarification process, implying no need for furtherfiltration.In addition,the correspond-ing remaining arsenic concentrations of the supernatants for the sets were54.2,49.9,52.1,61.3and54.7l g/L,which were in agree-ment with the directlyfiltrated sample(49.2l g/L),indicating that enhanced aggregation or coagulation by Al3+has no obvious effect on the adsorption capacity of HFO.In agreement with the wet chemical analysis,there were no obvious differences between the X-ray diffraction patterns(Fig.1)of the HFO before and after coagulation.5.Conclusions and implicationsIn this study,many of the uninvestigated engineering and scientific aspects of As(III)removal by EC were comprehensively studied.Our results indicate that As(III)removal efficiency was considerably higher than with the widely used CC process and other iron based processes.Iron scrap,an abundant byproduct from iron planing machines,exhibited the same capacity as iron plates for As removal during electrolysis,further reducing the material cost of EC.Settle-ability of HFO precipitates can be greatly enhanced by the addition of2mg/L Al3+,which reduced the turbid-ity of the supernatant to<1NTU(drinking water standard for many countries or regions)after120min settling.These conclusions offer new scientific and engineering insights for practitioners and other researchers seeking better and more efficient treatment of As-contaminated ground water.Table2Effect of Ca2+/Mg2+on the HFO particle size and zeta potential(initial concentrations:500l g/L As(III),3.0mg/L P,and30mg/L Si with and without Ca2+/Mg2+).Iron concentration(mg/L)Without Ca2+/Mg2+Iron concentration(mg/L)With Ca2+/Mg2+Zeta potential(mV)Average particle size(nm)Zeta potential(mV)Average particle size(nm)5.2À28.815.3 4.8À8.988410.1À26.048.29.6À9.390618.2À28.4123.519.3À11.6964L.Li et al./Separation and Purification Technology122(2014)225–230229AcknowledgmentsWe gratefully acknowledge support for this work by The Richard C.Blum Center for Developing Economies,USEPA P3Phase II award,support from China Postdoctoral Science Foundation (2013M531215),State Key Laboratory of Pollution Control and Resource Reuse Foundation(PCRRY12002),and China National Major Science and Technology Project of China(No. 2012ZX07403-001).We also thank Mr.John Erickson from UC Berkeley for editing the English and anonymous reviewers and editors for their efforts on this paper.Appendix A.Supplementary materialSupplementary data associated with this article can be found,in the online version,at /10.1016/ j.seppur.2013.11.012.References[1]M.Karim,Arsenic in groundwater and health problems in Bangladesh,WaterRes.34(2000)304–310.[2]N.Singh,D.Kumar,A.P.Sahu,Arsenic in the environment:effects on humanhealth and possible prevention,J.Environ.Biol.28(2007)359–365.[3]D.G.Kinniburgh,P.L.Smedley,Arsenic contamination of ground water inBangadesh.Final Report Summary,British Geological Survey,Bangladesh Department for Public Health,Engineering,2001.[4]M.Argos,T.Kalra,P.J.Rathouz,Y.Chen,B.Pierce,F.Parvez,T.Islam,A.Ahmed,M.Rakibuz-Zaman,R.Hasan,G.Sarwar,V.Slavkovich,A.van Geen,J.Graziano,H.Ahsan,Arsenic exposure from drinking water,and all-cause and chronic-disease mortalities in Bangladesh(HEALS):a prospective cohort study,Lancet 376(2010)252–258.[5]Who,Guidelines for drinking-water quality,second ed.,vol. 1.Recommendations,WHO{a},Geneva,Switzerland,1993.[6]USEPA,Arsenic treatment technologies for soil,waste and water,Tech.ReportNo.EPA-542-R-02-004,2002.[7]CMOH,China Ministry of Health(CMOH),Standards for Drinking WaterQuality-GB5749-2006,2006(in Chinese).[8]K.Ng,Z.Ujang,P.Le-Clech,Arsenic removal technologies for drinking watertreatment,Rev.Environ.Sci.Biotechnol.3(2004)43–53.[9]M.Bissen,F.H.Frimmel,Arsenic–a review.Part II:Oxidation of arsenic and itsremoval in water treatment,Acta Hydrochim.Hydrobiol.31(2003)97–107.[10]M.Bissen,F.H.Frimmel,Arsenic–a review.–Part1:Occurrence,toxicity,speciation,mobility,Acta Hydrochim.Hydrobiol.31(2003)9–18.[11]X.G.Meng,G.P.Korfiatis,S.B.Bang,K.W.Bang,Combined effects of anions onarsenic removal by iron hydroxides,Toxicol.Lett.133(2002)103–111. [12]X.G.Meng,S.Bang,G.P.Korfiatis,Effects of silicate,sulfate,and carbonate onarsenic removal by ferric chloride,Water Res.34(2000)1255–1261.[13]A.B.Mukherjee,P.Bhattacharya,Arsenic in groundwater in the Bengal DeltaPlain:slow poisoning in Bangladesh,Environ.Rev.9(2001)189–220.[14]L.C.Roberts,S.J.Hug,T.Ruettimann,M.Billah, A.W.Khan,M.T.Rahman,Arsenic removal with iron(II)and iron(III)waters with high silicate and phosphate concentrations,Environ.Sci.Technol.38(2004)307–315.[15]X.H.Guan,H.R.Dong,J.Ma,L.Jiang,Removal of arsenic from water:effects ofcompeting anions on As(III)removal in KMnO4–Fe(II)process,Water Res.43 (2009)3891–3899.[16]S.-Y.Pang,J.Jiang,J.Ma,Oxidation of sulfoxides and Arsenic(III)in corrosion ofnanoscale zero valent iron by oxygen:evidence against ferryl ions(Fe(IV))asactive intermediates in Fenton reaction,Environ.Sci.Technol.45(2010)307–312.[17]A.K.Leuz,S.J.Hug, B.Wehrli, C.A.Johnson,Iron-mediated oxidation ofantimony(III)by oxygen and hydrogen peroxide compared to arsenic(III) oxidation,Environ.Sci.Technol.40(2006)2565–2571.[18]I.A.Katsoyiannis,T.Ruettimann,S.J.Hug,PH dependence of Fenton reagentgeneration and As(III)oxidation and removal by corrosion of zero valent iron in aerated water,Environ.Sci.Technol.42(2008)7424–7430.[19]P.K.Holt,G.W.Barton,C.A.Mitchell,The future for electrocoagulation as alocalised water treatment technology,Chemosphere59(2005)355–367. [20]P.R.Kumar,S.Chaudhari,K.C.Khilar,S.P.Mahajan,Removal of arsenic fromwater by electrocoagulation,Chemosphere55(2004)1245–1252.[21]kshmanan,D.A.Clifford,G.Samanta,Ferrous and ferric ion generationduring iron electrocoagulation,Environ.Sci.Technol.43(2009)3853–3859.[22]X.Zhao,B.F.Zhang,H.J.Liu,J.H.Qu,Removal of arsenite by simultaneouselectro-oxidation and electro-coagulation process,J.Hazard.Mater.184 (2010)472–476.[23]L.Li,C.M.van Genuchten,S.E.A.Addy,J.Yao,N.Gao,A.J.Gadgil,ModelingAs(III)oxidation and removal with iron electrocoagulation in groundwater, Environ.Sci.Technol.46(2012)12038–12045.[24]W.Wan,T.J.Pepping,T.Banerji,S.Chaudhari,D.E.Giammar,Effects of waterchemistry on arsenic removal from drinking water by electrocoagulation, Water Res.45(2011)384–392.[25]X.H.Guan,J.Ma,H.R.Dong,L.Jiang,Removal of arsenic from water:effect ofcalcium ions on As(III)removal in the KMnO4–Fe(II)process,Water Res.43 (2009)5119–5128.[26]R.Kaegi,A.Voegelin,D.Folini,S.J.Hug,Effect of phosphate,silicate,and Ca onthe morphology,structure and elemental composition of Fe(III)-precipitates formed in aerated Fe(II)and As(III)containing water,Geochim.Cosmochim.Acta74(2010)5798–5816.[27]A.D.Redman,D.L.Macalady,D.Ahmann,Natural organic matter affects arsenicspeciation and sorption onto hematite,Environ.Sci.Technol.36(2002)2889–2896.[28]D.G.Kinniburgh,P.L.Smedley,Arsenic contamination of ground water inBangadesh.Final Report Summary,British Geological Survey,Bangladesh Department for Public Health Engineering,2001.[29]B.M.Voelker, B.Sulzberger,Effects of fulvic acid on Fe(II)oxidation byhydrogen peroxide,Environ.Sci.Technol.30(1996)1106–1114.[30]A.P.Hammersley,S.O.Svensson,M.Hanfland,A.N.Fitch,D.Hausermann,Two-dimensional detector software:from real detector to idealised image or two-theta scan,High Pressure Res.14(1996)235–248.[31]U.Schwertmann,R.M.Cornell,Iron oxides in the laboratory preparation andcharacterization,1991.[32]kshmanan, D.A.Clifford,G.Samanta,Comparative study of arsenicremoval by iron using electrocoagulation and chemical coagulation,Water Res.(Oxford)44(2010)5641–5652.[33]A.Voegelin,R.Kaegi,J.Frommer,D.Vantelon,S.J.Hug,Effect of phosphate,silicate,and Ca on Fe(III)-precipitates formed in aerated Fe(II)-and As(III)-containing water studied by X-ray absorption spectroscopy,Geochim.Cosmochim.Acta74(2010)164–186.[34]L.Carlson,U.Schwertmann,Natural ferrihydrites in surface deposits fromFinland and their association with silica,Geochim.Cosmochim.Acta45(1981) 421–429.[35]C.M.van Genuchten,S.E.A.Addy,J.Pena,A.J.Gadgil,Removing arsenic fromsynthetic groundwater with iron electrocoagulation:an Fe and As K-Edge EXAFS study,Environ.Sci.Technol.46(2012)986–994.[36]S.J.Hug,O.Leupin,Iron-catalyzed oxidation of arsenic(III)by oxygen and byhydrogen peroxide:pH-dependent formation of oxidants in the Fenton reaction,Environ.Sci.Technol.37(2003)2734–2742.[37]V.Pallier,G.Feuillade-Cathalifaud,B.Serpaud,Influence of organic matter onarsenic removal by continuousflow electrocoagulation treatment of weakly mineralized waters,Chemosphere83(2011)21–28.230L.Li et al./Separation and Purification Technology122(2014)225–230。
Serum parameters of Adriatic sturgeon Acipenser naccarii(Pisces: Acipenseriformes):effects of temperature and stressE.Cataldi a,*,P.Di Marco a,A.Mandich b,S.Cataudella aa Dipartimento di Biologia,Uni6ersita`‘Tor Vergata’,Via della Ricerca Scientifica,00133Rome,Italyb Istituto di Anatomia Comparata,Uni6ersita`di Geno6a,Via Benedetto XV5,16132Geno6a,ItalyReceived24March1998;received in revised form17September1998;accepted18September1998AbstractData on the concentrations of some blood constituents of captive Adriatic sturgeon,Acipenser naccarii,a primitive bonyfish, are reported.Serum osmolality,Na+,K+,Cl−,Ca2+,cortisol,glucose and total protein concentrations were measured.The effects of anaesthesia,temperature,crowding and prolonged handling stress were tested on a group of124-year-old sturgeons sampled repeatedly.The anaesthetic dose of MS222(140mg l−1)induced significant osmolality elevation in the sturgeon.After exposure to colder temperature(17versus25°C),cortisol and Cl−concentrations significantly decreased.The cultured sturgeon did not seem susceptible to crowding and prolonged handling stress,since neither the serum cortisol and glucose levels nor the other blood parameters were affected by these stressors.Results are compared with the few available data on other chondrostean fish and with those on teleosts.©1998Elsevier Science Inc.All rights reserved.Keywords:Acipenser naccarii;Blood chemistry;Cortisol;Osmolality;Serum constituent;Stress;Sturgeon;Temperature1.IntroductionBlood parameters are increasingly used as indicators of the physiological or sublethal stress response infish to endogenous or exogenous changes.The possibility of evaluation depends on the availability of reference val-ues as close as possible to‘normal’values of the various blood components considered as reliable descriptors of healthyfish under natural conditions.Taking into account the long evolutionary history of bonyfishes and the many adaptations to different environments,no species can be used as a representa-tive model for allfish.This explains the rapidly expand-ing literature on the chemical properties offish blood. However,at present,few reports deal with the blood of primitivefish(e.g.the chondrosteans),as is evident from the extensive reviews of the subject offish blood [9].The Adriatic sturgeon,Acipenser naccarii,is a species endemic to the waters of North Italy and the countries bordering the eastern Adriatic.Little is known about the ecology and biology of this primitive bonyfish [3,11–14,16].It is generally considered a euryhaline species,because it is sometimes found in estuaries.Once abundant in all the riversflowing into the North Adri-atic Sea,its present distribution range has been greatly reduced by the impact of overfishing and habitat deteri-oration.Interest in this species was recently aroused by successful attempts at artificial reproduction[1],which suggest that Acipenser naccarii may be suitable forfish farming and restocking.Therefore it is important to provide reference values for an assessment of the status of this species in both natural and rearing conditions. In this initial study on the blood chemistry of captive Italian sturgeons,the concentrations of some compo-nents of the serum were measured and the variations resulting from temperature,anaesthesia,crowding and handling,which represent some conditions associated*Corresponding author.Fax:+3962026189;e-mail:*******************1095-6433/98/$-see front matter©1998Elsevier Science Inc.All rights reserved. PII S1095-6433(98)10134-4E.Cataldi et al./Comparati6e Biochemistry and Physiology,Part A121(1998)351–354 352with culture practices and sampling procedure,were recorded.2.Materials and methods2.1.Origin and maintenance offishAdriatic sturgeon juveniles,derived from artificial reproduction,were reared in the Laboratory of Experi-mental Ecology and Aquaculture of the University‘Tor Vergata’of Rome.Fish were maintained in square fiberglass tanks supplied with freshwater at25°C and at a density of8kg m−3.Sturgeon were fed on commer-cial dry pellets(Universal Mangimi).A group of124-year-oldfish,which had mean (9S.D.)weight and total length of2.391.2kg and 82.2913.4cm,respectively,were used and repeatedly sampled in different conditions,after allowing the spec-imens to recover for a minimum of15days[9].Fish were fasted for2days before sampling.2.2.Sampling conditionsIn thefirst trial,blood samples were rapidly collected by cardiac puncture from sturgeons serially netted and manually immobilized without anaesthesia.After15days,the recovered sturgeons were sampled after anaesthesia in140mg l−1buffered solution of tricaine methane sulphonate(MS222),which induced loss of body and opercular movements within4–8min after exposure.In the third trial,fish previously acclimated for1 month to17°C were sampled after anaesthesia as above.The sturgeons maintained at a low temperature (17°C)were then exposed to crowding stress by confi-nement to a tank for24h at a density of16kg m−3.In addition,the sturgeons were stressed by prolonged han-dling.Anaesthetizedfish were sampled as above.2.3.Variables examined and analytical methods Clotted blood was centrifuged at3000×g for10min and the analyses were performed immediately.Serum osmolality was determined by a cryoscopic method (One-ten Osmometer,Fiske).Na+,K+and Cl−con-centrations were measured using an electrolyte analyzer with ion-specific electrodes(SPOTCHEM SE-1510, Menarini).Glucose,calcium and total protein were determined using an autodry chemistry analyzer (SPOTCHEM SP-4410,Menarini).Cortisol concentration was measured using Coat-A-Co Cortisol(Kontron Analytical MDA312)and ra-dioimmunoassay software.The kits were supplied by Diagnostic Product Corporation.2.4.Data analysisRange values,means and standard deviations were determined for all the parameters examined.Differ-ences between groups as regards both serum compo-nent concentrations and Na:Cl ratio were analyzed by the Mann–Whitney U-test.Significance was accepted at P B0.01.The contribution of Na+and Cl−to total serum osmolality was obtained using the formula Osm NaCl= (Na++Cl−)×0.91[9].3.ResultsThe effects of anaesthesia,temperature,crowding and handling stress on mean value of the blood parameters are reported in Table1.In all the different sampling conditions tested,the individual plasma cortisol and glucose concentrations were found to be highly variable(as indicated by the range reported in Table1)and the increase in levels did not depend on the order in which thefish were taken from the tank.The values of these parameters,for example,in sturgeons maintained at25°C and serially sampled without anaesthesia were,progressively,45.5, 116.4,43.0,77.5,303.5,177.1,17.1,31.4,44.7,186.7, 142.3nmol l−1and1.7,1.8,2.3,1.9,3.9,3.8,1.1,1.6, 1.7,1.4,2.2mmol l−1,respectively.The values of the other parameters were more constant.The comparison between sturgeon maintained at 25°C sampled with and without anaesthesia showed that the anaesthetized sturgeon differed significantly only in its higher osmolality.The trend of Na+and Cl−concentrations was also towards higher levels,and in fact contributed to total osmolality about in the same percentage(Osm NaCl=237.0mOsm kg−1;83.4%) as non-anaesthetized sturgeon(Osm NaCl=230.6mOsm kg−1;88%).The Na:Cl ratios in anaesthetized and non-anaesthetized sturgeons,respectively1.22and1.24, were not significantly different.After acclimation to the temperature of17°C,the cortisol level and Cl−concentration decreased signifi-cantly.Na+and Cl−(Osm NaCl=220.8)contributed only79.6%to total serum osmolality,due to very low Cl−concentration.In fact,the Na:Cl ratio measured 1.46in this group.The other blood parameters were unaffected by low temperature acclimation. Crowding and prolonged handling did not seem to affect sturgeon blood chemistry.In fact,no significant increase in mean serum cortisol or glucose levels or in other components were detected.Nevertheless,the indi-vidual concentrations of all parameters resulted in a much broader range than the respective values mea-sured in unstressed sturgeon.E.Cataldi et al./Comparati6e Biochemistry and Physiology,Part A121(1998)351–354353 Table1Mean9S.D.and range(in parentheses)values of serum constituents of Adriatic sturgeon sampled at25°C with and without anaesthesia,and at 17°C with and without stressGroupAnaesthetized,Anaesthetized,Not anaethetized,Anaesthetized,not stressed,not stressed,not stressed,stressed,17°C(n=12)25°C(n=11)25°C(n=11)17°C(n=12)83.6945.52(62.2–153.9)32.0918.7b(13.2–81.4)Cortisol(nmol l−1)43.0943.8(2.7–172.1) 107.8988.0(17.1–303.5)2.390.9(1.3–4.0) 2.691.1(1.4–4.6)Glucose(mmol l−1) 2.190.9(1.1–3.9) 3.491.6(1.3–6.7)277.193.9(270.7–283.3)273.396.0a(266.0–286.2)279.596.8(269.6–291.0) 262.4.96.9(251.0–280.3)Osmolality(mOsm kg−1)143.595.2(136.0–154.0)144.193.7(137.0–148.0)Na+(mEq l−1)140.694.8(134.0–152.0)143.695.5(135.0–155.0)3.490.8(2.4–5.3) 3.290.5(2.7–4.5)K+(mEq l−1) 3.690.3(3.0–4.3) 3.190.3a(2.7–3.7)117.093.1(112.0–122.0)98.596.5b(88.0–107.0)Cl−(mEq l−1)112.993.5(107.0–120.0)104.393.7(98.0–111.0)2.390.3(1.7–2.8) 2.690.3(1.9–2.9) 2.490.3(1.8–2.9)2.390.1(2.1–2.6)Ca2+(mEq l−1)2.290.3(1.9–2.6) 2.390.3(1.9–2.8) 2.590.5(1.9–3.6) 2.590.6(1.9–3.6)T-protein(g dl−1)The four groups were compared using the Mann–Whitney U-test.a Significant difference,at P B0.01,between sturgeon sampled at25°C with and without anaesthesia.b Significant difference,at P B0.01,between sturgeon sampled at25°C and17°C and anaesthetized.4.DiscussionIn sturgeon[7],as well as in teleosts[9],the in-crease of serum cortisol level was considered a pri-mary indicator of stress response.The other para-meters were also liable to change in response to stress or environmental variations.The serum cortisol levels detected in sturgeon main-tained at17°C are consistent with the‘normal’values reported in Acipenser baeri,whereas the high levels found at25°C are consistent with those found under acute hypoxic stress in the same species[7]. Therefore the cortisol level detected at17°C might suggest a relatively‘unstressed’condition of captive Adriatic sturgeon at such temperatures,and all the parameters measured might also be considered as ‘normal’values.The glucose mean value is lower than resting levels detected in A.baeri[7].Total protein is in the range of values measured in the Russian stur-geon[15].However,osmolality and ion concentra-tions might be affected slightly by anaesthesia,as in sturgeons sampled at25°C.The effect of anaesthesia on salt and water balance was clearly demonstrated in teleosts[4].Nevertheless,the serum osmolality and ion concentrations measured in the low-temperature group are comparable to the values indicated for Acipenser transmontanus,a euryhaline sturgeon[10]. In A.naccarii Na+and Cl−contribute to over75% of total osmolality as in teleosts,whereas the Na:Cl ratio(1.46)may be considered exceptional,and is the same only in anguillids.In other teleosts it averages 1.1[9].To elucidate true resting levels of serum parameters of this primitive bonyfish,daily and seasonalfluctua-tions will have to be checked.Moreover,in eury-haline anadromous teleost species,and presumably in the Adriatic sturgeon,some parameters can be linked to physiological adjustments to migration.The higher cortisol value measured in sturgeon maintained at25°C may indicate that upper tempera-ture causes chronic stress,which also affects ion con-centration.The Adriatic sturgeon was successfully reared at constant high temperature conditions(239 2°C)which offered better growth performance if com-pared to sturgeon grown both at15–18°C and at fluctuating temperature regimes(10–30°C)[2].How-ever,in some teleosts,temperature preferences have been reported and they may depend on endogenous and environmental conditions[5,6].A.naccarii does not seem susceptible to crowding and handling stress.The mean values of cortisol,glu-cose and osmolality,in fact,were not altered;further-more,no apparent cumulative effects were observed. This could suggest the domesticated conditions of the hatchery-reared sturgeons,as it has been demon-strated in chinook salmon[8].However,the different individual susceptibility to stressors,as indicated by the broad range of values detected,may be an important consideration in the evaluation of certain situations. AcknowledgementsThis research was carried out within the‘Project for the Development of National Aquaculture,1993–1997’supported by a grant from Italian Ministry of Agriculture(L.201/91).E.Cataldi et al./Comparati6e Biochemistry and Physiology,Part A121(1998)351–354 354References[1]Arlati G,Bronzi P,Colombo L,Giovannini G.Induzione dellariproduzione dello storione italiano(Acipenser naccarii)allevato in cattivita`.Riv Ital Acquacolt1988;23:94–6.[2]Arlati G,Bronzi P.Sturgeon farming in Italy.In:GershanovichAD,Smith TIJ,editors.Proceedings of Second International Symposium on Sturgeons,6–11September1993,Moscow.Moscow:VNIRO,1995:321–32.[3]Cataldi E,Ciccotti E,Di Marco P,Di Santo O,Bronzi P,Cataudella S.Acclimation trials of juvenile Italian sturgeon to different salinities:morpho-physiological descriptors.J Fish Biol 1995;47:609–18.[4]Eddy FB.Effects of stress on osmotic and ionic regulation infish.In:Pickering AD,editor.Stress and Fish.New York: Academic Press,1981:209–245.[5]Elliot JM.Some aspects of thermal stress on freshwater teleosts.In:Pickering AD,editor.Stress and Fish.New York:Academic Press,1981:77–102.[6]Hazel JR.Thermal biology.In:Evans DH,editor.The Physiol-ogy of Fishes.London:CRC Press,1993:427–467.[7]Maxime V,Nonnotte G,Peyraud C,Williot P,Truchot JP.Circulatory and respiratory effects of an hypoxic stress in the Siberian sturgeon.Resp Physiol1995;100:203–12.[8]Mazur CF,Iwama GK.Effect of handling and stocking densityon hematocrit,plasma cortisol,and survival in wild and hatch-ery-reared chinnok salmon(Oncorhynchus tshawytscha).Aqua-culture1993;112:291–9.[9]McDonald DG,Milligan CL.Chemical properties of the blood.In:Hoar WS,Randall DJ,Farrell AP,editors.Fish Physiology, vol.XIIB.London:Academic Press,1992:56–133.[10]McEnroe A,Cech JJ.Osmoregulation in white sturgeon:lifehistory aspects.Am Fish Soc Symp1987;1:191–6.[11]Paccagnella B.Osservazioni sulla biologia degli storioni delBacino Padano.Arch Oceanogr Limnol1948;5:141–54. [12]Potts WT,Rudy PP.Aspects of osmotic and ionic regulation inthe sturgeon.J Exp Biol1972;56:703–15.[13]Rochard E,Castelnaud G,Lepage M.Sturgeons(Pisces:Acipenseridae):threats and prospects.J Fish Biol1991;37(Suppl.A):123–32.[14]Rossi R,Grandi G,Trisolini R,Franzoi P,Carrieri A,DezfuliBS,Vecchietti E.Osservazioni sulla biologia e la pesca dello storione cobice Acipenser naccarii Bonaparte nella parte termi-nale delfiume Po`.Atti Soc Ital Sci Nat Museo Civico Storia Nat Milano1992;132:121–42.[15]Skelukhin GK,Metallov GF,Geraskin PP.Effect of tempera-ture and salinity of Caspian sea water on juvenile Russian sturgeon,Acipenser guldenstadti.Voprosy Iktiologii1990;30: 296–304.[16]Tortonese E.Acipenser naccarii Bonaparte,1836.In:Holcik J,editor.The Freshwater Fishes of Europe.General Introduction to Fishes.Acipenseriformes,vol.I,part II.Wiesbaden:AULA-Verlag,1989:285–93.。
© World Health OrganizationWHO Technical Report Series, No. 937, 2006Annex 8Proposal to waive in vivo bioequivalence requirements for WHO Model List of Essential Medicines immediate-release, solid oral dosage forms Introduction1. Background2. WHO revisions to the criteria for Biopharmaceutics Classifi cation Systemclassifi cation3. WHO extensions to the scope of application of the biowaiver4. WHO additional criteria for application of the biowaiver procedure5. Explanation of the tables6. Biowaiver testing procedure according to WHOIntroductionThis proposal is closely linked to the Multisource (generic) pharmaceutical products: guidelines on registration requirements to establish interchange-ability (WHO Technical Report Series, No. 937, Annex 7). It aims to give national authorities suffi cient background information on the various orally administered active pharmaceutical ingredients (APIs) on the WHO Model List of Essential Medicines (EML), also taking into account local usage of the API, to enable them to make an informed decision as to whether generic formulations should be subjected to in vivo bioequivalence (B E) studies or whether a biowaiver can be granted. In light of scientifi c work and dis-cussion in the last decade, some of the criteria used to evaluate the API in terms of potential for a biowaiver have been revised to allow a broadened scope of application. The result is that many APIs on the EML can now be considered for the biowaiver procedure, subject to the usage and risks in the national setting.1. Background1.1Initiatives to allow biowaivers based on the BiopharmaceuticsClassifi cation SystemIn 1995 the American Department of Health and Human Services, US Food and Drug Administration (HHS-FDA) instigated the B iopharmaceutics391Classifi cation System (BCS), with the aim of granting so-called biowaiv-ers for scale-up and post-approval changes (SUPAC) (/cder/ guidance/cmc5.pdf). A biowaiver means that in vivo bioavailability and/or bioequivalence studies may be waived (i.e. not considered necessary for product approval). Instead of conducting expensive and time-consuming in vivo studies, a dissolution test could be adopted as the surrogate basis for the decision as to whether two pharmaceutical products are equivalent. At that time the biowaiver was only considered for SUPAC to pharmaceutical products.More recently, the application of the biowaiver concept has been extended to approval of certain orally administered generic products (/ cder/guidance/3618fnl.htm).Within the context of the documents cited above, only APIs with high solu-bility and high permeability and which are formulated in solid, immediate-release (IR) oral formulations can be approved on the basis of the biowaiver procedure. A major advantage of the biowaiver procedure is the simplifi ca-tion of the product approval process and the reduction of the time required, thus reducing the cost of bringing new products to market.1.2What is the Biopharmaceutics Classifi cation System?The Biopharmaceutics Classifi cation System (BCS) was proposed in 1995 by Amidon et al.1 It is a scientifi c framework which divides APIs into four groups, according to their solubility and permeability properties.1.3 Classifi cation of active pharmaceutical ingredients accordingto the Biopharmaceutics Classifi cation SystemAccording to the HHS-FDA defi nitions in the documents cited above, the four possible categories for an API according to the BCS are:•BCS class I: “high” solubility – “high” permeability•BCS class II: “low” solubility – “high” permeability•BCS class III: “high” solubility – “low” permeability•BCS class IV: “low” solubility – “low” permeability.Depending on the classifi cation, the oral availability of the API may be expected to range from being heavily dependent on the formulation and manufacturing method (e.g. Class II APIs: poorly soluble yet highly perme-able) to being mostly dependent on the API permeability properties (e.g.Class III APIs: highly soluble yet poorly permeable).1Amidon GL, Lennemas H, Shah VP, Crison JR. A theoretical basis for a biopharmaceutic drug classifi cation: the correlation of in vitro drug product dissolution and in vivo bioavailability. Phar-maceutics Research, 1995, 12:413–420.3921.4How is high or low solubility currently defi ned by the Departmentof Health and Human Services, US Food and Drug Administration?The aqueous solubility of a drug substance is considered as high according to the HHS-FDA BCS criteria when:• the ratio of the highest orally administered dose (in mg) to the solubility (mg/ml) is 250 ml or lower.—This criterion is met over the pH range 1–7.5 at 37 °C.According to HHS-FDA guidances, the determination of the equilibrium solubility should be carried out with the shake-fl ask method (other methods such as acid or base titration are permitted when their ability to predict the equilibrium solubility is justifi ed). The experiments should be carried out at a temperature of 37 ± 1°C. Further, a suffi cient number of pH conditions should be chosen to cover the pH range of 1–7.5 and each determination should be carried out at least in triplicate. The buffer solutions given in the United States Pharmacopeia (USP) are appropriate for the tests, but other buffers are also allowed for these experiments. The pH value of each buffer solution should be checked before and after each experiment. Degradation of the API due to pH or buffer composition should be reported together with other stability data.The reason for the 250-ml cut-off criterion for the dose:solubility ratio is that in pharmacokinetic bioequivalence studies, the API formulation is to be ingested with a large glass of water (8 ounces corresponds to about 250 ml). If the highest orally administered dose can be completely dissolved in this amount of water, independent of the physiological pH value (hence the determination over the pH range 1–7.5), solubility problems are not expected to hinder the uptake of the API in the small intestine.The other important parameter for the BCS is the intestinal permeability of the API.1.5How is high or low permeability currently defi ned by the Departmentof Health and Human Services, US Food and Drug Administration?According to HHS-FDA a drug is considered highly permeable, when 90 % or more of the orally administered dose is absorbed in the small intestine.Permeability can be assessed by pharmacokinetic studies (for example, mass balance studies), or intestinal permeability methods, e.g. intestinal perfusion in humans, animal models, Caco 2 cell lines or other suitable, validated cell lines. In vivo or in situ animal models or in vitro models (cell lines) are only considered appropriate by HHS-FDA for passively trans-ported drugs. It should be noted that all of these measurements assess the fraction absorbed (as opposed to the bioavailability, which can be reduced substantially by fi rst-pass metabolism).393HHS-FDA suggests use of two different methods for determining the per-meability classifi cation if results with one method are inconclusive.1.6Which pharmaceutical formulations can currently be consideredfor a biowaiver according to the Department of Health andHuman Services, US Food and Drug Administration?To be considered bioequivalent according to the HHS-FDA biowaiver pro-cedure, a pharmaceutical product:• should contain a Class I API;• should be rapidly dissolving, meaning it should release at least 85% of its content in 30 minutes in three different media (pH 1.2, pH 4.5 and pH6.8, composition see “Multisource document”)1 in a paddle (50 rpm) orbasket (100 rpm) apparatus at 37 °C and a volume of 900 ml;• should not contain excipients which could infl uence the absorption of the API;• should not contain an API with a narrow therapeutic index; and• should not be designed to be absorbed from the oral cavity.The reasoning for the above-mentioned dissolution restrictions is that whena highly soluble, highly permeable API dissolves rapidly, it behaves like asolution in the gastrointestinal tract. If this is the case, the pharmaceutical composition of the product is insignifi cant, provided that excipients which infl uence the uptake across the gut wall are excluded from the formulation.The API is not prone to precipitation after its dissolution due to its good solu-bility under all pH conditions likely to be found in the upper gastrointestinal tract. The high permeability ensures the complete uptake (> 90%) of the API during its passage through the small intestine. The rapid dissolution of the product guarantees that the API is available long enough for the uptake in the small intestine (the passage time in the small intestine is approximately four hours) and negates any slight differences between the formulations.Pharmaceutical products containing an API with a narrow therapeutic index should always be tested with in vivo methods, because the risk to the patient resulting from a possible incorrect bioequivalence decision using the bio-waiver procedure is considered too high with these kinds of APIs.As the BCS is only applicable to APIs which are absorbed from the small intestine; drugs absorbed from other sites (e.g. from the oral cavity) are not eligible for a biowaiver.It is clear that the HHS-FDA requirements for the classifi cation of APIs and eligibility criteria for the biowaiver are very strict. During the last decade,1Multisource (generic) pharmaceutical products: guidelines on registration requirements to establish interchangeability (WHO Technical Report Series, No. 937, Annex 7).394several publications and continuing scientifi c discussions have suggested that the original HHS-FDA criteria for application of the biowaiver pro-cedure could be relaxed without substantially increasing the risk to public health or to the individual patient. On the basis of these publications and dialogue, WHO has proposed revised BCS criteria and additional consid-erations for the eligibility of a pharmaceutical product for the biowaiver procedure in the “Multisource document”.12.WHO revisions to the criteria for BCS classifi cationWHO revisions to the BCS criteria are as follows:•WHO high-solubility defi nitionWhen an API shows a dose:solubility ratio of 250 ml or lower at 37 °C over a pH range of 1.2–6.8, it can be classifi ed as “highly soluble”. The decrease in pH from 7.5 in the FDA guidances to 6.8 refl ects the need to dissolve the drug before it reaches the mid-jejunum to ensure absorption from the gastrointestinal tract.• Furthermore, the dose that is to be used for the calculation is the highestdose indicated in the Model List of Essential Medicines (EML). In some countries, products may be available at doses exceeding the highest dose on the EML. In such cases, the classifi cation given in the tables at the end of this Annex may no longer be appropriate and the dose:solubil-ity ratio and the permeability will have to be reassessed at the product dose.•WHO permeability defi nitionWhen an API is absorbed to an extent of 85% or more, it is considered to be “highly permeable”. The permeability criterion was relaxed from 90% in the FDA guidance to 85% in the WHO “Multisource document”.Some examples of APIs now included in BCS Class I that were previ-ously considered to be in Class III are paracetamol, acetylsalicylic acid, allopurinol, lamivudine and promethazine.Application of these revised criteria has changed the classifi cation of some APIs in the list. Thus, the classifi cations in the tables attached to this docu-ment supersede those in previous publications. As new APIs appear on the EML, it will be necessary to classify them according to the revised BCS;so it is therefore anticipated that the tables will be revised regularly. In addition, some APIs have not yet been suffi ciently characterized to assign them a BCS classifi cation. As the tables evolve, it is anticipated that more concrete information will be generated for these APIs as well.1Multisource (generic) pharmaceutical products: guidelines on registration requirements to establish interchangeability (WHO Technical Report Series, No. 937, Annex 7).395the basket apparatus (applies to pharmaceutical products containingClass III APIs);—rapidly dissolving (release of > 85% of the labelled amount of drug in 30 minutes) in standard media at pH 1.2, 4.5 and 6.8, at a rota-tional speed of 75 rpm in the paddle apparatus or 100 rpm in the bas-ket apparatus (applies to pharmaceutical products containing Class IAPIs and/or Class II APIs which are weak acids and meet the 250 mldose:solubility requirement at pH 6.8).(4)Considerations relating to excipientsThe national authority should be aware that some excipients can infl uencemotility and/or permeability in the gastrointestinal tract. Therefore, the ex-cipients used in the multisource product formulation should be scrutinized.In this regard, the national authority can draw on the experience relat-ing to formulations which have been approved on the basis of humanbioequivalence studies in their own or in other jurisdictions.If the multisource product under consideration contains excipients thathave been used before in similar amounts in other formulations of thesame API, it can be reasonably concluded that these excipients will haveno unexpected consequences for the bioavailability of the product. If,however, the formulation contains different excipients, or amounts ofthe same excipients that are very different from usual, the national au-thority may choose to declare the biowaiver procedure inapplicable.A list of usual and acceptable excipients can be found at the following website: /cder/iig/iigfaqWEB.htm; formulations of some productscan be found on the web sites of some national drug regulatory authorities.5.Explanation of the tablesThe decision of a national authority to allow a biowaiver based on the BCS should take into consideration the solubility and permeability char-acteristics as well as the therapeutic use and therapeutic index of the API, its pharmacokinetic properties, the similarity of the dissolution profi les of the multisource and the comparator products in standard buffers with a pH of 1.2, pH 4.5 and pH 6.8 at 37 °C. Data related to the excipients compo-sition in the multisource product are also required. A systematic approach to the biowaiver decision has been established by the International Pharma-ceutical Federation (FIP) and published in the Journal of Pharmaceutical Sciences (/cgi-bin/jhome/68503813).The relevant documents can also be downloaded from the FIP web site at: http://www.fi/. These monographs provide detailed information which should be taken into account whenever available in the biowaiver consideration.3985.1Which active pharmaceutical ingredients are included in thetables?The substances listed in the 14th WHO Model List of Essential Medicines (EML) of March 2005 have been evaluated and classifi ed according to the revised criteria given above.5.2Where do the data come from?The solubility and permeability values were found in the publicly available literature, such as Martindale’s, the Merck Index and scientifi c journals.Please note that the doses used for the calculation of the dose:solubility ratio are those stated in the EML.The indications given in the tables are reproduced directly from the EML. If the EML specifi es the dosage form (e.g. sublingual tablet) this is indicated under “comments”.5.3“Worst case” approach to the Biopharmaceutics Classifi cationSystemThe drugs listed in the EML were classifi ed according to the criteria explained above. Where no clear classifi cation could be made, the “worst case” was as-sumed. For example if a substance is highly soluble, but absolute bioavailability data were not available, the test conditions for BCS Class III substances have been proposed. The same procedure was adopted for fi xed combinations, for example amoxicillin and clavulanic acid, the testing procedure was always fi xed according to the “worst” BCS classifi cation, in this example clavulanic acid (BCS Class III/1), because amoxicillin is a BCS Class I drug. This com-bination would therefore be tested according to BCS Class III requirements.The results of the revised classifi cation can be found in Tables 1–3.5.4Why are there three Tables?Table 1 lists all APIs on the EML that are administered orally, with the excep-tion of the APIs listed as complementary. Table 2 summarizes the APIs listed as complementary in the EML and Table 3 lists the APIs for which no classifi cation had previously been assigned, or that had been introduced with the 14th EML (March 2005), together with a more detailed explanation of their classifi cation.5.5 Risk assessmentTo minimize the risks of an incorrect biowaiver decision in terms of public health and risks to individual patients, the therapeutic indications of the API, known pharmacokinetic variations, food effects, etc. should be evalu-ated based on local clinical experience, taking into account the indications399for which the API is prescribed in that country as well as specifi c pharmaco-kinetic population variations (for example CYP polymorphisms). Known potential risks are listed under “potential risks” in the tables. The absence of an entry under “potential risks” should not, however, be misconstrued as meaning that there are no risks associated with the use of the medicine. 6.Biowaiver testing procedure according to WHODepending on the BCS classifi cation of the API, based on solubility and permeability characteristics listed in the accompanying tables, the testing procedure is defi ned in section 9.2.1 of the “Multisource document”1:6.1For pharmaceutical products containing BiopharmaceuticsClassifi cation System Class I (highly soluble, highlypermeable) APIsFor rapidly dissolving (as defi ned above) pharmaceutical products contain-ing BCS Class I APIs, more than 85% dissolution of the labelled amount is required within 30 minutes in standard media at pH 1.2, 4.5 and 6.8 using the paddle apparatus at 75 rpm or the basket apparatus at 100 rpm. The dis-solution profi les of the comparator and the multisource products should be compared by an f> 50 or an equivalent statistical criterion.2If within 15 minutes more than 85% of the API are released from the compar-ator and the multisource formulation under the above-mentioned conditions the products will be considered very rapidly dissolving. In this case the prod-ucts are deemed to be equivalent and a profi le comparison is not required.6.2For pharmaceutical products containing BiopharmaceuticsClassifi cation System Class III (highly soluble, lowpermeability) APIsA biowaiver can be considered only if both the multisource and the com-parator product are very rapidly dissolving. Eighty-fi ve per cent or more dissolution of the labelled amount of the API should be achieved within15 minutes in standard media at pH 1.2, 4.5 and 6.8 using the paddle ap-paratus at 75 rpm or the basket apparatus at 100 rpm.Generally, the risks of an inappropriate biowaiver decision should be more critically reviewed (e.g. site-specifi c absorption, induction/competition at the absorption site, excipient composition and therapeutic risks) for prod-ucts containing BCS Class III APIs than for BCS Class I drugs.1Multisource (generic) pharmaceutical products: guidelines on registration requirements to establish interchangeability (WHO Technical Report Series, No. 937, Annex 7).4006.3For pharmaceutical products containing APIs with highsolubility at pH 6.8 but not at pH 1.2 or 4.5 and with highpermeability (by defi nition, BCS Class II compoundswith weak acidic properties)These are eligible for a biowaiver provided that the multisource product:• is rapidly dissolving, i.e. 85% or more dissolution of the labelled amount of the API should be achieved within 30 minutes in standard media at pH 6.8 using the paddle apparatus at 75 rpm or the basket apparatus at 100 rpm; and• the multisource product exhibits similar dissolution profiles, as deter-mined with the f2 value or equivalent statistical evaluation, to those ofthe comparator product in buffers at all three pH values (pH 1.2, 4.5 and6.8).For multisource products containing BCS Class II APIs with dose:solubility ratios of 250 ml or less, at pH 6.8, the excipients should also be critically evaluated in terms of type and amounts of surfactants in the formulation.Further details of eligibility for the biowaiver and appropriate test proce-dures can be found in sections 5 and 9 of the “Multisource document”.11Multisource (generic) pharmaceutical products: guidelines on registration requirements to establish interchangeability (WHO Technical Report Series, No. 937, Annex 7).401405c h l o r p h e n a -m i n e h yd r o ge n m a l e a t e 4 m g h i g hB A 25-59%, fi r s t p a s s 3/19.2.1.2C Y P 2D 6 p o l y -m o r p h i s m a n t i a l l e r g i ce x t e n t of fi r s t -p a s s m e t a b o l i s m u n c e r t a i nc h l o r p r o m a z i n e h yd r o c h l o r i de 100 m gh i g hl o w39.2.1.2 p s y c h o t h e r a p e u -t i c m e d i c i n e c i p r o fl o x a c i nh y d r o c h l o r i d e 250 m g h i g hB A 70–82%, p o s s i b l e fi r s t p a s s , h i g h i nC a c o -2 c e l l s3/19.2.1.2 a n t i b a c t e r i a le x t e n t of fi r s t - p a s s m e t a b o l i s m u n c e r t a i nc l o f a z i m i n e100 m gi n s u f fi c i e n t l i t e r a t u r e l o w 4/3N o t e l i g i b l e f o r b i o w a i v e r a t p r e s e n t a n t i l e p r o s y m e d i c i n ec l o m i f e n e c i t r a t e50 m g h i g h i n s u f fi c i e n t l i t e r a t u r e 3/19.2.1.2o v u l a t i o n i n d u c e rc l o m i p r a m i n e h yd r o c h l o r i de 25 m g h i g h66% e x c r e t e d i n t h e u r i n e , t h e r e m a i n d e r b e i n g e l i m i -n a t e d i n t h e f a e c e s 3/19.2.1.2p s y c h o t h e r a p e u -t i c m e d i c i n el a c k o f a b s o l u t e b i o a v a i l a b i l i t y d a t ac l o x a c i l l i n (a s s od i u m s a l t )1000 m g h i g hl o w 39.2.1.2a n t i b a c t e r i a lc ode i n e p h o s p h a t e 30 m g h i g h l o w39.2.1.2r i s k o f a b u s eo p i o i d a n a l g e s i c ,d i a r r h oe a i n a d u l t sd a p s o n e100 m gl o w (w e a k b a s e ) h i g h 2N o t e l i g i b l e f o r b i o w a i v e rG 6P D d e fi -c i e n c ya n t i l e p r o s y m e d i c i n ed i a ze p a m 5 m g h i g hh i g h19.2.1.1p s y c h o t h e r a p e u -t i c m e d i c i n e s c o r e d t a b l e tB A , B i o a v a i l a b i l i t y ; G 6P D , g l u c o s e -6-p h o s p h a t e d e h y d r o g e n a s e .409g l y c e r y l t r i n i t r a t e 500 μgh i g hs u b l i n g u a l a p p l i c a t i o n ,p e r m e a b i l -i t y i n t h e o r a l c a v i t y m o r e i m p o r t a n t t h a n G I p e r m e a b i l i t y3/1N A hl o c a l a b s o r p t i o n a n t i a n g i n a l m e d i c i n e s u b l i n g u a l a p p l i c a t i o ng r i s e o f u l v i n 250 m gl o w (n e u t r a l ) h i g h2N o t e l i g i b l e f o r b i o w a i v e r a n t i f u n g a lh a l o p e r i d o l2 m gb o r d e r l i n e < 0.01 m g /m l 2l o w 4/3N o t e l i g i b l e f o r b i o w a i v e rp s y c h o t h e r a p e u -t i c m e d i c i n eh y d r a l a z i n e h y d r o c h l o r i d e50 m g h i g hl o w 39.2.1.2a n t i h y p e r t e n s i v e m e d i c i n eh y d r o c h l o r o -t h i a z i d e 25 m g h i g h l o w 39.2.1.2a n t i h y p e r t e n s i v e m e d i c i n e , d i u r e t i c a n d u s e d i n h e a r t f a i l u r es c o r e d t a b l e ti b u p r o f e n 400 m gl o w , w e a k a c i d (p K a 4.4,5.2)h i g h 29.2.1.3N S A I D , a n t i m i -g r a i n e m e d i c i n ei n d i n a v i r s u l f a t e 400 m g l o w l o w (?)4/2N o t e l i g i b l e f o r b i o w a i v e r C Y P 450 3A 4, f o o d e f f e c t (–)a n t i r e t r o v i r a lu n k n o w n w h e t h e r p o o r B A i s d u e t o p o o r s o l u b i l i t y o r p o o r s o l u b i l i t y a n d p o o r p e r m e a b i l i t yD :S , D o s e :s o l u b i l i t y r a t i o ; B A , b i o a v a i l a b i l i t y .426T a b l e 3C o m p o u n d s i n t r o d u c e d t o t h e W H O M o d e l L i s t o f E s s e n t i a l M e d i c i n e s s i n c e M a r c h 2005 f o r w h i c h n o c e r t a i n c l a s s i fi c a t i o n h a d b e e n p r e v i o u s l y r e p o r t e d (t h e s e c o m p o u n d s a l s o a p p e a r i n T a b l e 1 a n d T a b l e 2)M e d i c i n e aH i g h e s t o r a l s t r e n g t h a c c o r d i n g t o W H O E s s e n t i a l M e d i c i n e s L i s t a S o l u b i l i t y bP e r m e a b i l i t y c B C S c l a s s dD i s s o l u t i o n t e s t (f o r b i o w a i v e r )e P o t e n t i a l r i s k s fI n d i c a t i o n (s )a c c o r d i n g t o W H O E s s e n t i a l M e d i c i n e s L i s t (E M L )aC o m m e n t s a n d s p e c i a l d o s a g e f o r m i n d i c a t i o n s aa m l o d i p i n e 5 m gs l i g h t l y s o l u b l e (1),D :S 5 m lB A a b s60–65%,e x c r e t i o n o f d r u g m e t a b o -l i t e s i n u r i n e 90–95% (2)19.2.1.1a n t i h y p e r t e n s i v e m e d i c i n eB A a b s < 85% a s c r i b e d t o fi r s t -p a s s m e t a b o l i s ma m o d i a q u i n e(b a s e )200 m g45 m g /m l 2,D :S 4.4 m lB A > 75% (3)3/19.2.1.2C Y P 2C 8p o l y m o r p h i s m ,i n c r e a s e d r i s k f o r a g r a n u l o c y -t o s i s a n d h e p a -t o t o x i c i t y (4)a n t i m a l a r i a la m o x i c i l l i n + c l a v u l a n i c a c i d 500 m g + 125 m gf r e e l y s o l u b l e i n w a t e r (1),D :S 1.25 m la b s o r p t i o n > 73% (5)1 + 3/19.2.1.2a n t ib ac t e r i a lt e s t s b a s e d o n c l a v u l a n i c a c i d c l a s s i fi c a t i o na r t e s u n a t e 50 m gv e r ys l i g h t l y s o l u b l e (6),D :S 500 m l ;(w e a k a c i d ,p K a ~ 6.4)B A a b s 82% (1),B A a b s 88% (7),B A a b s 61% (8)4/2N o t e l i g i b l e f o r b i o w a i v e ra n t i m a l a r i a lp e r m e a b i l i t y d e p e n d s o n s e v e r i t y o f d i s e a s eD :S , D o s e : s o l u b i l i t y ; B A , B i o a v a i l a b i l i t y .427a z i t h r o m y c i n 500 m gp r a c t i c a l l y i n s o l u b l e i n w a t e r (1)< 0.01m g /m l , D :S 50 000 m lB A a b s 16% (9);B A 37%(10, 11); 4/2N o t e l i g i b l e f o r b i o w a i v e ra n t ib ac t e r i a l u n k n o w n w h e t h e r p o o r B A i sd ue t o p o o r s o l u b i l i t y o r p o o r s o l u b i l i t y a n d p o o r p e r m e a b i l i t yc a l c i u m f o l i n a t e 15 m gs p a r i n g l y s o l u b l e i n w a t e r (P h . E u r . 5.2); v e r y s o l u b l e (U S P 28); D :S 15 m l a n d 0.015 m l , r e s p e c -t i v e l yB A a b s 92% 25 m g (12, 13);B A a b s 73.4%(15 m g ) (14);f u l l y a b s o r b e d ;A UC a n d t 1/2s i m i l a r a f t e r i.v . & p .o (15)19.2.1.1 a n t i c y t o t o x i c m e d i c i n el e v o d o p a (l ) + c a r b i d o p a (c )(l ) 250 m g + (c ) 25 m g(l ) h i g h +(c ) s o l u b l e 1 i n 500 o f w a t e r , f r e e l y s o l u b l e i n 3 M H C l (1)(l ) h i g h +(c ) B A 58% (16); B A a b s88% (d o g s ) (17)(l ) 1 +(c ) 3/19.2.1.2n a r r o w t h e r a p e u t i c i n d e xa n t i p a r k i n s o n m e d i c i n et e s t s b a s e d o n c a r b i d o p a c l a s s i fi c a t i o nc e fi x i m e 400 m gs l i g h t l ys o l u b l e (2),D :S 400 m l22–54% (2)4N o t e l i g i b l e f o r b i o w a i v e ra n t ib ac t e r i a lD :S , D o s e : s o l u b i l i t y ; B A : B i o a v a i l a b i l i t y ; P h .E u r ., E u r o p e a n P h a r m a c o p o e i a ; U S P , U n i t e d S t a t e s P h a r m a c o p o e i a ; A U C , a r e a u n d e r t h e c u r v e ; i.v ., i n t r a v e n o u s .。
Some heightened sensitivityAndrew E Hudson1* and Alex Proekt21Department of Anesthesiology and Perioperative Medicine, David Geffen School of Medicine, University of California, Los Angeles, 757 Westwood Plaza Suite 3325, Los Angeles, CA 900952Department of Anesthesiology, Weill Cornell Medical College, 535 E 68th St, New York, NY 10065*Correspondingauthor,Email:*******************.eduWith the progressive aging of the population, anaesthetists are increasingly facedwith geriatric patients. As our patient population greys, there have been regular calls to limit anaesthetic exposure in older patients out of fear of overdose. The currentconcern over postoperative cognitive dysfunction weighs heavily on some patient’s minds, while anaesthetist ponder the significance of the “triple low” as a predictor of morbidity and mortality.1 2 Anecdotally, elderly patients take a variable, but prolonged, amount of time to recover from anaesthesia relative to younger patients. The open question remains, how and why is the older brain different in its response to anaesthetics?One possibility is that the older brain is simply more sensitive to anaesthetics; lower doses are required to achieve the same effect. The minimum alveolar concentration (MAC) of volatile anaesthetic required to inhibit movement in response to a surgical stimulus3 decreases with age.4 Yet, a series of elegant experiments in ruminants, which have separable cerebral and vertebral circulations, demonstrated that MAC correlates with levels of anaesthetic in the spinal cord rather than with cortical processing,5 so it is unclear whether the change in anaesthetic sensitivity responsible for the age-related decline in MAC includes a cortical effect. Elderly patients are also more sensitive to propofol for induction.6 Older rats required higher brain concentrations of propofol to induce 1s suppressions on EEG.7In this issue of the British Journal of Anaesthesia, Chemali and colleagues report on the results of a series of experiments measuring the effect of aging on anaesthetic sensitivity in the line of Fischer 344 rats maintained by the US National Institute on Aging. Paralleling previous work on age-adjusted MAC, the authors found that young adults were significantly less sensitive to isoflurane than older animals (recovering the righting reflex at lower steady-state concentrations of anaesthetic). Moreover, older rats took a longer and more variable time to recover from both isoflurane and from a single bolus dose of propofol. Because aging can affect a number of physiologic parameters, including cardiac output, functional residual capacity, and body composition, it is unclear whether the prolonged recovery is due to some combination of a change in clearance, distribution and/or a change in the central response to the anaesthetic. Finally, the authors demonstrate that methylphenidate, a centrally acting catecholamine reuptake inhibitor, can speed the recovery of older rats to be faster than young rats not exposed to methylphenidate.The major advance of Chemali and colleagues is the application of a measure of cortical burst suppression derived from the electroencephalogram (EEG), which demonstrates that the change in anaesthetic sensitivity is present in brain.8 To avoid a confound from the declining voltage amplitude in the EEG signal with aging, the authors developed a sophisticated measure to detect burst suppression rather than the routine voltage threshold of 10 microvolts. This was used to build a time-varying estimate of the probability that the animal was in burst suppression. By developing a continuous, quantitative measure of cortical suppression, the authors are able to show that, at a steady state of isoflurane, aged rat cortex is more sensitive to isoflurane. This demonstrates that the behavioural sensitivity change is apharmacodynamic rather than just a pharmacokinetic effect. Finally, the cortical recovery timeframe from propofol parallels the behavioural results, suggesting that the prolonged effect of propofol is due to increased cortical sensitivity.It is currently unclear what mechanism might underlie a change in global sensitivity to anaesthetics. Both propofol and isoflurane have some GABA-ergic effects, but it is unclear from the current work whether this effect is mediated by some effect on GABA receptors or via another system. On the one hand, mice expressing an isoflurane-resistant knock-in alpha1 GABAA receptor subunit did not change either MAC or the suppression of neuronal responses to noxious stimulation.9 Yet sensitivity to other GABA-ergic sedatives, including methohexital10 and midazolam,11 also increases with aging. Perhaps aging-related changes in GABAA receptor subunit expression or other, compensatory modifications that occur with aging could explain the increased sensitivity to anaesthetics in older animals.12 13 Alternatively, there could be some downstream effect of aging that explains a generic increase in sensitivity to sedative medications.But as Chemali and colleagues demonstrate, the anaesthetic state depends upon a balance of cortical suppression and the various arousal systems of the brain. The same group has previously demonstrated that the “reanimation” observed with systemically administered methylphenidate parallels the effect of stimulating the dopaminergic ventral tegmental area. Perhaps the tone of the dopaminergic system sets the anaesthetic sensitivity of the brain and declining dopaminergic tone with aging causes increased anaesthetic sensitivity – this would certainly be a parsimonious explanation with obvious appeal.This minimal model of anaesthetic sensitivity makes several predictions that can be tested against the data presented in Chemali’s report. Begin by assuming that aging shifts the sensitivity curve to the left and methylphenidate moves it back to the right (Figure 1A). If we look at the mean recovery times, this simple model does surprisingly well. Yet one very salient feature in Chemali’s recovery time data presented in their Figure 1 is that the spread of the recovery times decreases as the recovery times shorten; an alternative way of saying this is that the variance of the distribution decreases as the mean decreases.Can we capture this spread in the recovery times with this minimal model of sensitivity changes? If recovery from anaesthesia were simply a probabilistic sigmoidal function of effect site anaesthetic concentration, one would not expect any difference in the width of the distribution of times to recovery with a change in sensitivity. Yet the simple addition of first order kinetics to effect site concentration, Figure 1B, leads to a much slower transition through the steep portion of the dose-response curve for the more sensitive population, which will produce a wider distribution of times as the average recovery time increases, Figure 1C. Our toy model is doing surprisingly well.One observation from the authors’ data in their Figure 1, however, stands in starkcontrast to our model prediction. For all groups except the older rats given methylphenidate, the amount of variance in the time to recovery changes in parallelwith the mean time to recovery. The recovery times in aged rats given methylphenidate are less variable than in aged rats given only propofol, but substantially more variable than in younger rats given only propofol, who take longer to wake. Yet our simple model that combines a sensitivity change with pharmacokinetics would predict the variance in older rats given methylphenidate to fall between the young rats given propofol only and the young rats given propofol and methylphenidate The failure of this prediction suggests that age-related shifting the dose-response curve of general anaesthetics that is opposed by methylphenidate within a single pathway is insufficient.Indeed, even Chemali and colleagues’ careful characterization of anaesthetic sensitivity is incomplete. Kelz and colleagues have definitively demonstrated that recovery from anaesthesia is not simply due to washout of anaesthetic agent, as the sensitivity curve for induction and recovery are shifted versions of each other, with induction taking the role of the blue curve and recovery taking the role of the black curve in Figure 1D.14 Kelz termed this tendency for the awake brain to remain awake and the anaesthetized brain to remain anaesthetized “neural inertia”. Given that Chemali and colleagues only examined the recovery arm in their experiments, it remains an open question as to whether aging shifts the induction curve in parallel to the recovery curve, or whether the degree of neural inertia in the aged brain changes.The presence of neural inertia is a form of state path-dependence, known generically as hysteresis. A simple two-state model that can capture anaesthetic hysteresis incorporates two different energy wells, one well for the “awake” state and one for the “anaesthetised” state, separated by an energy barrier. The probability of crossing the barrier, one measure of anaesthetic sensitivity, is a function of the depth of the well and the kinetic energy of the particle (Figure 1D). Because the two wells can each change depth at different anaesthetic concentrations, the probability of crossing the wall in one direction need not be the same as the probability of moving in the opposite direction. The presence of neural inertia dictates that at least this minimum model is necessary to capture the brain’s sensitivity to anaesthetics. Moreover, this offers more parameters that could affect anaesthetic sensitivity to explain the interaction of methylphenidate with aging; perhaps methylphenidate selectively affects the kinetic energy of the particle without changing the depth of the energy wells.Developing a better predictive model of what governs behavioural state changes in the brain will require much more quantitative data. The technique employed by Chemali gives us more useful data points, by adding a measure of cortical suppression to overt behavioural measures. This technique can be exploited for characterizing both induction and recovery and seems to parallel the behavioural changes seen in time to recovery.Yet it is worth noting that there is a long way between burst-suppression and wakefulness. We have previously reported that there are some characteristic features in brain activity that occur during recovery from anaesthesia, and transitions between these different states reveals a required sequence of states that appear prior to recovery15 Are other EEG activity patterns that occur at intermediate anaesthetic doses also affected by aging in the same way as burst-suppression, with a shift to the left in the curve, or is there a change in the architecture of the network of brain activity states? Perhaps certain rhythms are more stable in old brains, and others simply do not occur. At present we have no sense of how aging impacts the functional effects of anaesthetics on brain activity patterns.Understanding how the dopaminergic and other arousal systems interact with general anaesthesia will help inform our understanding about rational interventions to facilitate recovery from anaesthetics in aging patients. Given that much of the concern over anaesthesia in the geriatric population could be characterized as recovery gone awry, developing and characterizing an adequate model of recovery that captures the effect of aging is of compelling importance.References1. Sessler Daniel I. MD, Sigl Jeffrey C. PD, Kelley Scott D. MD, et al. Hospital Stayand Mortality Are Increased in Patients Having a ‘Triple Low’ of Low BloodPressure, Low Bispectral Index, and Low Minimum Alveolar Concentration of Volatile Anesthesia. J Am Soc Anesthesiol 2012;116:1195–2032. Kertai MD, White WD, Gan TJ. Cumulative Duration of ‘Triple Low’ State ofLow Blood Pressure, Low Bispectral Index, and Low Minimum AlveolarConcentration of Volatile Anesthesia Is Not Associated with IncreasedMortality. J Am Soc Anesthesiol 2014;121:18–28.3. Eger E, Saidman L, Brandstater B. Minimum Alveolar AnestheticConcentration: A Standard of Anesthetic Potency. Anesthesiology1965;26:756–63.4. Eger EI. Age, Minimum Alveolar Anesthetic Concentration, and MinimumAlveolar Anesthetic Concentration-Awake. Anesth Analg 2001;93:947–53.5. Antognini J, Schwartz K. Exaggerated anesthetic requirements in thepreferentially anesthetized brain. Anesthesiology 1993;79:1244–9.6. Dundee JW, Robinson FP, McCollum JS, Patterson CC. Sensitivity to propofol inthe elderly. Anaesthesia 1986;41:482–5.7. Larsson JE, Wahlström G. The influence of age and administration rate on thebrain sensitivity to propofol in rats. Acta Anaesthesiol Scand 1998;42:987–94.8. Pilge S, Jordan D, Kreuzer M, Kochs EF, Schneider G. Burst suppression-MACand burst suppression-CP50 as measures of cerebral effects of anaesthetics.Br J Anaesth 2014;112 :1067–74.9. Kim J, Atherley R, Werner DF, Homanics GE, Carstens E, Antognini JF.Isoflurane depression of spinal nociceptive processing and minimum alveolar anesthetic concentration are not attenuated in mice expressing isofluraneresistant gamma-aminobutyric acid type-A receptors. Neurosci Lett2007;420:209–12.10. Sear JW, Prys-Roberts C, Phillips KC. Age influences the minimum infusion rate(ED50) for continuous infusions of Althesin and methohexitone. Eur JAnaesthesiol 1984;1:319–25.11. Jacobs JR, Reves JG, Marty J, White WD, Bai SA, Smith LR. Aging IncreasesPharmacodynamic Sensitivity to the Hypnotic Effects of Midazolam. AnesthAnalg 1995;80:143–812. Caspary DM, Hughes LF, Ling LL. Age-related GABAA receptor changes in ratauditory cortex. Neurobiol Aging 2013;34:1486–9613. Rissman RA, De Blas AL, Armstrong DM. GABA(A) receptors in aging andAlzheimer’s disease. J Neurochem 2007;103:1285–92.14. Friedman EB, Sun Y, Moore JT, et al. A conserved behavioral state barrierimpedes transitions between anesthetic-induced unconsciousness andwakefulness: evidence for neural inertia. PLoS One 2010;5:e1190315. Hudson AE, Calderon DP, Pfaff DW, Proekt A. Recovery of consciousness ismediated by a network of discrete metastable activity states. Proc Natl Acad Sci 2014;111 :9283–8.Figure LegendFigure 1.Panel A. Curves reflecting different anaesthetic sensitivities, where the EC50 for two populations differs by a factor of 100. The population depicted by the blue curve is less sensitive to anaesthesia, and hence remains awake at anaesthetic concentrations that render the black population unconscious. In Chemali’s experiment, the black curve corresponds to older rats and the blue curve corresponds to younger rats. Panel B. First order drug kinetics yield an exponential decline in effect site concentration over time. Panel C. A sensitivity shift with first order drug kinetics predicts longer time to emergence with broader distribution of emergence times. We simulated 10000 animals emerging from anaesthesia with both sensitivity relationships in (A) with the effect site concentration from (B). The distribution of times to waking for the young, less sensitive population (blue) was shorter and narrower than the distribution of times for the aged, more sensitive, population (black). Panel D. Emergence is not the reverse of induction. During induction the organism is less sensitive to anaesthetics than during emergence. A simple model to explain hysteresis is that the brain tends to stay in its current state, as though it is trapped in a potential energy well. The probability of switching states is a function of the height of the barrier above the bottom of the well. The arrows show induction (black) and recovery (blue) from anaesthesia that correspond to the transition from one energy well to the other. Note that these transitions do not occur at the same anaesthetic concentration. This minimal model is consistent with the results of Friedman et al.14。
Re v iewProcalcitonin as a marker of sepsisE.D.Carrol a,*,A.P.J.Thomson a ,C.A.Hart baInstitute of Child Health,Royal Li v erpool Children’s Hospital NHS Trust,Alder Hey,Eaton Road,Li v erpool L122AP,UK bDepartment of Medical Microbiology,Uni v ersity of Li v erpool,8th Floor Duncan Building,Daulby Street,Li v erpool L693GA,UKAbstractPrompt diagnosis and treatment with appropriate antimicrobial chemotherapy is of paramount importance to reduce morbidity and mortality associated with sepsis.Inflammatory markers currently in use,such as C-reacti v e protein (CRP)do not reliably differentiate between the systemic inflammatory response and sepsis.Procalcitonin (PCT),a precursor of calcitonin,is a 116amino acid protein that has been proposed as a marker of disease se v erity in conditions such as septicaemia,meningitis,pneumonia,urinary tract infection (UTI)and fungal and parasitic infection.In particular,serial measurements are useful in order to monitor response to therapy.Together with good clinical judgement and judicious use of antimicrobial agents,PCT should ser v e as a v aluable adjunct in the diagnosis and management of sepsis.#2002Elsevier Science B.V.and International Society of Chemotherapy.All rights reserved.Keywords:Procalcitonin;C-reacti v e protein;Sepsis;Bacterial;Viral1.IntroductionThe term sepsis is used to define the systemic inflammatory response to an infectious agent:bacterial,v iral,fungal or parasitic.Sepsis is a significant cause of morbidity and mortality,particularly in the immuno-compromised,elderly and critically ill.It is the leading cause of death on intensi v e care units.In an attempt to clarify and standardise the terminology used in sepsis,some definitions ha v e been agreed to assist researchers and clinicians dealing with sepsis and its sequelae [1].Septic shock is a less precise term,as it may be di v ided into early septic shock (responds to intra v enous fluids and/or pharmacological inter v entions),or refractory septic shock (lasting for more than 1h despite intra v e-nous fluids and pharmacological inter v ention,and requiring inotropic support).Variable terminology is used in this re v iew because of the terms used in the cited references.Howe v er,the terminology used is defined in Table 1and has been adapted for use in paediatrics [2].The rapid detection of sepsis in an ill patient is of paramount importance in order to institute the promptadministration of appropriate antimicrobial chemother-apy.Various markers of inflammation such as IL-1b ,TNF-a ,IL-6and IL-8ha v e all been studied.These cytokines are well recognised to correlate with disease se v erity in sepsis [3Á5].Howe v er,they are neither sensiti v e nor specific enough,are time consuming and expensi v e to perform.1.1.Physicochemical propertiesProcalcitonin (PCT)is a precursor of calcitonin,and is a 116amino acid protein with a molecular mass of 13kDa.It undergoes successi v e clea v ages in the neuroen-docrine cells of the thyroid,lung and pancreas to form three distinct molecules;calcitonin (32amino acids),katacalcin (21amino acids)and an N-terminal fragment called aminoprocalcitonin (57amino acids)(Fig.1).The first description of ele v ated serum PCT concentrations in sepsis was by Assicot in 1993[6].This article describes high concentrations of a substance with calcitonin-like immunoreacti v ity in patients with v arious bacterial and v iral infections.Serum PCT le v els decreased rapidly during antibiotic therapy.Concentrations of mature calcitonin were normal in all subjects irrespecti v e of the PCT concentration.*Corresponding author.Tel.:'44-151-228-4811;fax:'44-151-228-2024.E-mail address:edcarrol@li v (E.D.Carrol).International Journal of Antimicrobial Agents 20(2002)1Á90924-8579/02/$-see front matter #2002Elsevier Science B.V.and International Society of Chemotherapy.All rights reserved.PII:S 0924-8579(02)00047-X1.2.PhysiologyBacterial lipopolysaccharide (LPS)has been shown to be a potent inducer of PCT release into the systemic circulation.This release is not associated with an increase in calcitonin.PCT le v els increase from 3to 4h,peak at about 6h and then plateau for up to 24h [7,8].It is degraded by specific protease and has a half-life of between 25and 30h [9].In contrast,C-reacti v e protein (CRP)le v els rise between 12and 18h after bacterial challenge.In healthy indi v iduals circulating le v els of PCT are v ery low,usually below 0.1ng/ml.In v iral infections and inflammatory states,PCT concentrations are slightly ele v ated up to 1.5ng/ml,but in bacterial infection le v els may exceed 1000ng/ml [6,8,10].This 3Á5log-fold increase makes it an ideal marker of bacterial sepsis.1.3.ProductionThe exact sites of PCT production are unknown but it is thought that the li v er is a major site.The e v idence for this comes from a study that showed that hepatocytes produced large quantities of PCT following stimulation with TNF-a and IL-6[11].Another study has demon-strated expression of PCT in peripheral blood mono-nuclear cells (PBMCs)following stimulation with LPS.This expression appears to be modulated by LPS and the pro-inflammatory cytokines TNF-a ,IL-1b ,IL-2and IL-6[12].The finding of high PCT le v els in patients who ha v e undergone thyroidectomy makes thyroid origin unlikely [6].1.4.Biological functionThe precise physiological role of PCT is unclear.One study has shown that increased concentrations exacer-bate mortality in an animal model,whereas neutralisa-tion with polyclonal antibody increases sur v i v al [13].It suggests that PCT acts as a mediator that sustains and augments the inflammatory response in a manner similar to IL-6and IL-8,and that it is integral to the host response and to the ultimate outcome of sepsis.The authors raise the possibility that PCT might be a potential target for therapeutic blockade.It would be unlikely phylogenetically that a substance be released in sepsis by a host in response to an in v ading organism that caused it to succumb to the organism.A reasonable hypothesis is that PCT may function in a similar manner to TNF-a ha v ing a beneficial effect in small quantities but detrimental effects in excessi v e quantities.1.5.MeasurementThe assay most widely used is commercially a v ailable (Brahms Diagnostica,Berlin,Germany)and utilises a sandwich immunoluminometric method.Two antigen specific monoclonal antibodies are used,one of which binds the C-terminal region (katacalcin)and the other,which is fluorescent labelled with acridinium ester,binds calcitonin.The inner surface of the tube is pre-coated with katacalcin antibody,which binds to PCT in the patient sample,and this in turn binds to the luminescent labelled antibody creating a ‘sandwich complex’.TheFig.1.Schematic diagram of the PCT molecule.Table 1DefinitionsSystemic inflammatory response syndrome (SIRS):The systemic inflammatory response to a v ariety of clinical insults.The response is manifested by two or more of the following conditions Temperature 388C or B 368C Heart rate 90beats per minRespiratory rate 20breaths per min or PaCO 232mmHg (B 4.3kPa)WBC 12000cells per mm 3,B 4000cells per mm 3,or 10%immature (band)formsSepsis:The systemic response to infection (i.e.SIRS with an infection).This systemic response is manifested by two or more of the following conditions as a result of infection Temperature 388C or B 368C Heart rate 90beats per minRespiratory rate 20breaths per min or PaCO 232mmHg (B 4.3kPa)WBC 12000cells per mm 3,B 4000cells per mm 3,or 10%immature (band)formsSeptic shock:Sepsis associated with hypotension (blood pressure below 5thpercentile for age)despite adequate fluid resuscitation,in addition to peripheral hypoperfusion which may include lactic acidosis,oliguria or an acute alteration in mental status.E.D.Carrol et al./International Journal of Antimicrobial Agents 20(2002)1Á92intensity of the signal is measured using a luminometer. This is directly proportional to the concentration of PCT and results are calculated from a standard cur v e. The detection limit is0.1ng/ml.The assay requires20m l of plasma and can be performed within2h.A semiquantitati v e immunochromatographic bedside test is also a v ailable from the same company[14].In this assay,200m l of EDTA plasma is added to the test strip. PCT in the sample binds to mouse anti-katacalcin antibody complexed to colloidial gold.This complex mo v es by capillary action through the test strip and the sandwich complex can be seen as a reddish band.The colour intensity is proportional to the PCT concentra-tion.There are four bands;B0.5ng/ml,0.5Á2ng/ml, 2Á10ng/ml,and 10ng/ml.This stratification(de-pending on which study is used as a reference criterion) would be translated to negati v e(B0.5);consistent with no infection or v iral infection,positi v e(0.5Á2)and positi v e(2Á10);both consistent with bacterial or v iral infection,and positi v e( 10);consistent with bacterial infection.2.Procalcitonin in bacterial infection2.1.Bacteraemia and septicaemiaIn a study of300patients hospitalised with fe v er,PCT was shown to be of better predicti v e v alue for microbial infection than some clinical v ariables used in the definition of SIRS(temperature,tachycardia,tachyp-noea and abnormal white blood count).The neutrophil elastase-a1-antitrypsin le v el was also predicti v e for microbial infection and better than PCT in predicting mortality[15].Another large study of337adult patients demonstrated that patients with microbiologically and clinically documented infection had significantly higher PCT le v els than patients fulfilling only the SIRS criteria without signs of infection[16].In HIV-infected patients,PCT was not ele v ated in patients with e v ol v ing secondary infections such as Pneumocystis carinii pneumonia,cerebral toxoplasmo-sis,v iral infections,fungal infections,malignancies and mycobacterial infections,but was ele v ated in patients with septicaemia[17].PCT has been shown to be ele v ated in melioidosis with the highest v alues in those with septicaemia,and increased mortality in those with le v els 100ng/ml[18].Le v els of PCT 5ng/ml ha v e always been associated with se v ere infection,usually with bacteraemia[16,19].2.2.Bacterial meningitisIn a study of59children with meningitis,plasma PCT le v els were significantly higher in those with bacterial meningitis compared with those with v iral meningitis.CSF cell count and protein and serum CRP did not adequately differentiate between the two[20].A cut-off PCT v alue of5ng/ml distinguished a bacterial aetiology in17/18patients whereas CRP was B50ng/ml in2/18 patients with bacterial meningitis.The reason for this may be that CRP le v els can initially be normal or low in bacterial infection if the duration of illness is short.In a study of30adults with meningitis,admission PCT,CRP,white blood cell(WBC)count,CSF white cell count(WCC)protein and lactate were significantly higher in patients with bacterial meningitis than those with v iral meningitis.PCT had the highest specificity for bacterial infection(100%),but a sensiti v ity of only69%. PCT le v els,which were persistently ele v ated or increas-ing after2days,were associated with a poor prognosis [21].In another study of106adults with meningitis, although these parameters were significantly different between bacterial and v iral meningitis,there was a wide degree of o v erlap between the v alues for CRP and CSF parameters,but not for PCT.Serum PCT le v els 0.2 ng/ml had a sensiti v ity and specificity of up to100%in the diagnosis of bacterial meningitis.They concluded that serum PCT is the best marker for differentiating between bacterial and v iral meningitis in adults[22]. Bacterial sepsis is a major cause of mortality and morbidity in infants and children.In this group of patients,signs of sepsis are often v ery non-specific and easily missed by the inexperienced clinician.A study of 116children and neonates with and without sepsis were studied;PCT was a better diagnostic marker of sepsis than CRP and serum amyloid in critically ill children, whereas in critically ill neonates they were similar.A PCT concentration greater than8.1ng/ml identified all children with bacterial sepsis[23].munity-acquired pneumoniaPCT,CRP and IL-6were measured in a study of126 children hospitalised with community-acquired pneu-monia.Children with bacterial pneumonia had signifi-cantly higher PCT and CRP le v els than those with a sole v iral aetiology,but there was a significant degree of o v erlap.The study concluded that the measurement of PCT,CRP and IL-6were of little v alue in differentiating between bacterial and v iral pneumonia in children[24].A more recent study of72children found that a PCT cut off v alue of1ng/ml was more sensiti v e and specific and had greater positi v e and negati v e predicti v e v alues than CRP,IL-6and WBC in differentiating bacterial and v iral causes of community acquired pneumonia[25].2.4.Urinary tract infectionUrinary tract infection(UTI)is a common problem in children and accurate diagnosis is particularly important in such patients in order to pre v ent parenchymalE.D.Carrol et al./International Journal of Antimicrobial Agents20(2002)1Á93scarring which may cause hypertension or chronic renal failure in adult life.PCT has been shown to correlate with the se v erity of renal scars in children[26].A recent study looked at54children with pro v en UTI,63%of whom had renal in v ol v ement and37%had infection confined to the lower tract[27].There was no difference between WBC between the groups.A positi v e PCT v alue(measured using a semiquantitati v e assay)pre-dicted renal in v ol v ement in87Á92%of children com-pared with44Á83%using CRP.The study concluded that the new semiquantitati v e bedside PCT test may be useful in the management of febrile children with pro v en UTI in the emergency room.2.5.Febrile neutropeniaIn patients with febrile neutropenia,Gram-negati v e bacteraemia was accompanied by higher v alues of PCT than Gram-positi v e bacteraemia[28],but subsequent studies ha v e failed to show this difference[29].Howe v er, all the studies appear to be in agreement that in febrile neutropenia,a cut-off v alue of0.5ng/ml for PCT gi v es the best sensiti v ity,specificity and predicti v e v alues for the early diagnosis of bacterial infection[28Á30].A study of115patients with febrile neutropenia demonstrated a significantly higher PCT le v el in those with bacteraemia compared with those with localised bacterial infections.PCT was also significantly higher in patients with se v ere sepsis compared with those with localised infection.PCT le v els decreased after resolution of the infection,but increased when infections worsened [31].PCT v alues of0.5Á1.0ng/ml appeared to suggest localised infection,v alues 1.0ng/ml suggested prob-able bacteraemia and v alues 2.0ng/ml a septic response.They concluded that PCT might be a useful diagnostic tool in the early detection of systemic infection in febrile neutropenia.3.Procalcitonin and viral infectionsPCT increases in bacterial infections but remains low in v iral infections,although cytokine and CRP v alues may be ele v ated in certain v iral infections.PCT was measured in360infants and children hospitalised for bacterial and v iral infection,and compared with IL-6, CRP and interferon-alpha.PCT of]1ng/ml had better specificity,sensiti v ity predicti v e v alue than CRP,inter-feron-alpha and IL-6in distinguishing between v iral and bacterial infection.If a cut-off v alue of1ng/ml is used, PCT differentiates between se v ere and mild bacterial infection[32].This study also found that CRP 20mg/l had a sensiti v ity close to that of PCT(83%),but with much lower specificity(71v s.93%).A total of27%of children with v iral infections had a CRP 20mg/ml, therefore,using CRP alone as a marker of bacterial sepsis would ha v e resulted in o v ertreatment with anti-biotics.Interferon-alpha appeared to be v ery specific for v iral infection,but with low sensiti v ity.It was present in 77%of patients with v iral infection and8.6%with bacterial.Interferon-alpha has been shown to be detect-able in the early stages of respiratory infection in79%of patients with v iral infection and6%of those with bacterial infection.The production of interferon-alpha appears to be independent of age,with detectable le v els being found in infants and children with acute v iral illness[33].Unfortunately,the test takes48h,thereby limiting its use in the emergency setting of distinguishing between v iral and bacterial aetiologies to guide rational antibiotic prescribing.A case report describes a neonate with disseminated herpes simplex infection who presented with septic shock.A low PCT le v el(1.6ng/ml)inconsistent with bacteraemia raised the suspicion of an alternati v e aetiology and strengthened the case for anti v iral therapy [34].4.Procalcitonin in the neonatal periodEarly recognition of sepsis and prompt initiation of appropriate antibiotic therapy is essential for the successful treatment of bacterial infections in the neonatal period.Symptoms and signs of sepsis in the neonatal period can be v ery non-specific and,therefore, easily missed.The incidence of sepsis in neonatal intensi v e care units(NICU)is high because the patients managed there are often v ery immature,and conse-quently,immunocompromised.Another confounding factor is the potential transplacental transfer of anti-biotics administered to mothers during the pre-and intrapartum period which might increase the likelihood of culture-negati v e sepsis[35,36].It is in this group of patients that the a v ailability of a test that rapidly and reliably identified the presence of sepsis would be immensely v aluable.Such a test would radically alter neonatal prescribing practices and limit the unnecessary administration of antibiotics to uninfected infants.In the neonatal period,PCT v alues rise soon after birth,peak at21Á24h,then fall again.Gestational diabetes appears to significantly increase PCT v alues. The reason for these changes is at present unclear. Prematurity does not appear to ha v e any effect on the PCT response.WBC is of limited diagnostic v alue in neonatal sepsis[37],and CRP le v els when used alone may miss a significant number of patients in the early phase of coagulase-negati v e staphylococcal infection [38].In early onset sepsis,PCT yielded a sensiti v ity of 92.6%and a specificity of97.5%.PCT appears to be a highly specific and sensiti v e marker of early-onset neonatal sepsis pro v ided that PCT determinations areE.D.Carrol et al./International Journal of Antimicrobial Agents20(2002)1Á9 4repeated within the next24h.In late-onset sepsis(3Á30 days),PCT ga v e a sensiti v ity and specificity of100%in identifying bacterial sepsis[39].High PCT le v els ha v e been demonstrated in neonates with pro v en or clinically diagnosed bacterial infection, with a decrease corresponding to a response to appro-priate antibiotic therapy.CRP,although it had a high specificity for neonatal infection,was often normal early in the course of sepsis[40,41].Howe v er,a more recent study of197new-born infants demonstrated that a combination of IL-8and CRP was a more useful marker than PCT for the diagnosis of bacterial infection [42].The excessi v e use of antibiotics in the NICU can be justified by the fact that these are often critically ill premature neonates at the limits of v iability.Howe v er, this practice might promote the emergence of multi-resistant organisms,which in turn will significantly increase neonatal morbidity and mortality[35,36].This is a compelling reason for the introduction of impro v ed diagnostic tests that might identify early neonates with sepsis,thus tailoring antibiotic therapy to those who need it.5.Procalcitonin and intensive care units5.1.Septic shockIn a study comparing nitrite/nitrate(metabolites of nitric oxide),soluble TNF receptors IL-6and PCT in patients with septic shock,cardiogenic shock and bacterial pneumonia,measurements of nitrite/nitrate and PCT appeared to be the most reliable markers of septic shock[43].One study compared PCT and CRP and found that PCT had a lower sensiti v ity,specificity and area under the cur v e(AUC)than CRP as a marker of infection. Combining PCT and CRP increased the specificity for infection to82.3%.In infected patients,PCT was higher in non-sur v i v ors.Infected patients with bacteraemia had higher PCT concentrations than those without,but similar CRP concentrations.PCT le v els were particu-larly high in those with septic shock[44].Admission PCT was significantly higher in children with septic shock compared with those with localised bacterial infection,v iral infection and non-infected controls.Cut off concentrations for optimum prediction of septic shock were 2ng/ml for PCT and 50mg/l for CRP.A PCT le v el of 2ng/ml identified all patients with bacterial meningitis or septic shock[10]. PCT is a more sensiti v e marker of sepsis than CRP,IL-6 and lactate in medical ICU patients.High concentra-tions of PCT were associated with a poor prognosis[45].5.2.TraumaMechanical trauma causes ele v ated PCT le v els de-pending on the se v erity of the injury.Le v els peak on day 1Á3and fall thereafter.PCT is a sensiti v e marker of sepsis and se v ere multiple organ dysfunction syndrome (MODS)in injured patients.Routine PCT analysis appears to be useful in the early recognition of post-traumatic complications[46].A secondary rise in PCT appears to indicate superadded bacterial sepsis[47].5.3.SurgeryInflammatory markers usually remain ele v ated for up to2weeks post-surgery,whereas with PCT there is only a modest but transient rise.PCT le v els peak at24Á48h, and rarely exceed5ng/ml[48].PCT increases were greatest in abdominal surgery,with only moderate increases in aseptic surgery[49].5.4.Acute pancreatitisPCT is useful in differentiating sterile from infected pancreatitis;a cut-off le v el of1.8ng/ml o v er2days ga v e a sensiti v ity of94%and a specificity of91%[50].These findings were confirmed in a subsequent study[51].At admission to hospital,PCT but not CRP,soluble E-selectin or soluble IL-2receptor were higher in patients with acute pancreatitis than in patients with mild pancreatitis[52].A rapid semiquantitati v e PCT test was more accurate in predicting se v ere acute pancreatitis than CRP,APACHE II score and Ranson score[53].6.Procalcitonin and inflammationIt has been suggested that PCT is an acute phase protein,because it increases sharply after inflammation; it is thought to be produced by the li v er and can be induced by IL-6or TNF-a[11].There are currently no e v idence-based data to justify using CRP as a basis for management decisions regard-ing the institution,continuation or withholding of antibiotics,or for differentiating between bacterial and v iral aetiologies[54].PCT is not ele v ated in inflamma-tory disease states such as autoimmune disease(e.g. systemic antineutrophil cytoplasmic antibody-associated v asculitis)or inflammatory bowel disease,in contrast to acute phase proteins such as CRP,IL-6or neopterin [55,56].In these conditions,PCT rises usually indicate bacterial superinfection as opposed to flare-ups alone, whereas CRP and ESR rises may occur with either[55]. PCT correlates positi v ely with markers of inflamma-tion such as CRP and fibrinogen in haemodialysis patients[57].In acute coronary syndromes,admission CRP,serum amyloid A protein,fibrinogen and IL-6E.D.Carrol et al./International Journal of Antimicrobial Agents20(2002)1Á95were all ele v ated and increased further at48h,whereas PCT and neopterin remained unchanged[58].In a study of40patients with systemic inflammation and MODS,PCT was shown to be induced to v ery high serum concentrations during ad v anced stages of MODS and se v ere systemic inflammation,whereas CRP was often already in the upper concentration range e v en in patients with low se v erity scores.PCT declined more rapidly to normal during reco v ery than did CRP. Higher sepsis-related organ failure assessment(SOFA) scores were associated with significantly higher PCT plasma concentrations,whereas CRP was ele v ated irrespecti v e of the scores obser v ed[59].7.Procalcitonin and fungal and parasitic infectionsIn the post-transplant period where the risk of bacterial and fungal infection is increased because of immunosuppressi v e therapy,PCT appears to be reliable in differentiating bacterial or fungal as opposed to v iral infection or rejection after heart transplantation[60Á62].There was only a moderate rise in PCT in two14 year-old girls with disseminated aspergillosis after bone marrow transplant,whereas the CRP rise was significant [63].Falciparum malaria is a potentially fatal illness,and it is imperati v e that patients with a high risk of complica-tions and mortality are identified early,so that intensi v e therapies may be targeted at them.PCT has been shown to be a better marker of disease se v erity and response to treatment than IL-6,and is of good prognostic v alue [64Á66].Lowest concentrations of PCT ha v e been seen in semi-immune patients with uncomplicated malaria, and highest in those with se v ere complicated disease. PCT concentrations decreased on day2of illness in sur v i v ors,but not in non-sur v i v ors.There was a high correlation between le v el of parasitaemia and PCT,but not neopterin,lactate dehydrogenase and creatinine[67].8.Procalcitonin and hypocalcaemiaHypocalcaemia is a common finding in septic pa-tients,and PCT has been shown to be ele v ated in sepsis without increasing calcitonin[6].Se v eral mechanisms for the occurrence of hypocalcaemia in septic shock ha v e been postulated,but there is little e v idence to support any of them.Hypocalcaemia is a common finding in staphylococcal toxic shock syndrome,with significantly lower ionised and total calcium,but significantly ele v ated immunoreacti v e calcitonin[68]. This paper was published10years before the first description of PCT in sepsis by Assicot,and it may be that the molecule being measured was PCT.Hypocalcaemia is common in septic ICU patients,but not in those who undergo major surgery.It is not caused by increased urinary excretion of calcium or by attenu-ated bone resorption,but appears to be related to the septic response.In most septic patients and patients who underwent major surgery increased parathyroid hor-mone(PTH)concentrations were found.This suggests that calcium homeosatsis may be upset in critical illness [69].Total and ionised calcium ha v e also been shown to be ele v ated in70%of critically children with meningococ-cal sepsis,with lower calcium concentrations in the sickest children.In this study,60%of children with ionised hypocalcaemia had ele v ated PTH[70].A sig-nificant negati v e correlation has been shown between PCT and admission total calcium in children with meningococcal disease[71].It is unclear if and how the inflammatory response induces hypocalcaemia,or whether specific cytokines or other mediators are responsible for the hypocalcaemia. There is currently no e v idence that PCT has a role to play,but further studies are required to conclusi v ely exclude this.9.ConclusionCurrently used markers of SIRS such as CRP,IL-8 and TNF-a,which are ele v ated in sepsis,are also raised during most other causes of inflammation.PCT appears to be a v aluable marker,which is able rapidly and reliably to differentiate sepsis from SIRS.The preceding text highlights some limitations of PCT as a marker of bacterial sepsis:the cut-off v alues appear to be quite v ariable0.2[22]to5ng/ml[20].Some of the studies cited conclude that PCT was less useful than CRP[42,44,63],or of little v alue[24].These negati v e results,in addition to likely publication bias,indicate that the case for PCT is not yet conclusi v ely pro v en.The key point to be addressed when considering the use of any new medical technology is‘Does it impro v e any accepted outcome measures such as mortality,length of hospital stay,or treatment costs?’This question does not yet appear to ha v e been answered for PCT. Although the precise function of PCT is still un-known,in e v olutionary terms,a protein that is synthe-sised during inflammation must ha v e a physiological role.Hypotheses include a role in calcium metabolism, the cytokine network and modulation of NO synthesis and a‘non-steroidal analgesic effect’[72].Further work is needed to understand exactly where this protein is produced and how it is regulated.PCT may ha v e a role to play in the management of infectious diseases such as bacteraemia,septicaemia, meningitis,pneumonia,UTI,the neonatal period,and in fungal and parasitic infection.It appears to be aE.D.Carrol et al./International Journal of Antimicrobial Agents20(2002)1Á9 6。