英文健康体检表 CERTIFICATE OF HEALTH最新文档
- 格式:doc
- 大小:757.00 KB
- 文档页数:19

英语体检报告范本Physical Examination ReportName: [Insert Name]Date of Birth: [Insert Date of Birth]Gender: [Insert Gender]Nationality: [Insert Nationality]Date of Examination: [Insert Date of Examination]1. Vital Signs:- Blood Pressure (BP): [Insert BP]- Heart Rate (HR): [Insert HR]- Respiratory Rate (RR): [Insert RR]- Body Temperature (BT): [Insert BT]2. General Appearance:The patient appears to be in good health and maintains normal body posture. No signs of distress or discomfort are observed.3. Head and Neck:- Head: The patient's head is normocephalic without any visible abnormalities.- Eyes: The patient's eyes show normal conjunctiva and sclera, and the pupils are equal in size and responsive to light.- Ears: The external ears are symmetrical and without any signs of inflammation or discharge.- Nose: The nose is symmetrical, and there is no nasal discharge or deformity.- Throat: No redness, swelling, or tonsillar enlargement is observed in the throat.4. Respiratory System:- Lung Sounds: Clear breath sounds are auscultated bilaterally on inhalation and exhalation.- Respiratory Effort: Breathing is regular, and the patient shows no signs of difficulty or increased effort.- Cough: No productive or non-productive cough is reported by the patient.5. Cardiovascular System:- Heart Sounds: S1 and S2 heart sounds are normal and regular without any extra sounds or murmurs.- Peripheral Pulses: Radial and pedal pulses are strong and palpable bilaterally.- Edema: No edema is observed in the extremities.6. Gastrointestinal System:- Abdomen: The abdomen is soft and non-tender upon palpation. No organomegaly or masses are detected.- Bowel Movements: The patient reports having regular bowel movements without any difficulty or abnormality.7. Genitourinary System:- Urinary Function: The patient reports normal urinary frequency and without any pain or discomfort during urination.- Genitalia: No abnormalities or signs of inflammation are observed.8. Musculoskeletal System:- Range of Motion: The patient demonstrates full range of motion in all major joints without pain or limitations.- Muscle Strength: Equal and symmetric muscle strength is observed in major muscle groups.9. Neurological System:- Mental Status: The patient appears alert and oriented to time, place, and person.- Cranial Nerves: All cranial nerves are intact and functioning properly.- Reflexes: Deep tendon reflexes are normal and symmetric in all extremities.10. Skin:- Skin Integrity: The skin is intact with no evidence of lesions, rashes, or discoloration.- Hygiene: The patient maintains good personal hygiene.Conclusion:Based on the physical examination, the patient's overall health appears to be in excellent condition. No significant abnormalities or concerns are noted. These findings are based solely on the physical examination conducted on the specified date and should be interpreted in conjunction with the patient's medical history. Additional diagnostic tests may be required for a comprehensive evaluation if deemed necessary.Note: This is a sample physical examination report and should not be used as an official medical document. Personal information and results should be modified to reflect individual cases.。

The Vitality of Physical Examination Forms: A Journey through Health and WellnessIn the fast-paced world of modern medicine, thephysical examination form stands as a silent sentinel, a comprehensive record of one's health status. This document, often overlooked in the hustle and bustle of daily life, holds the key to understanding our physical well-being, mapping out our health history, and guiding future healthcare decisions.The physical examination form is a comprehensive document, containing a wide array of information. At its core, it documents basic personal details such as name, age, gender, and contact information. Beyond these basics, it delves into a detailed medical history, capturing surgeries, chronic conditions, allergies, and immunizations. It also serves as a timeline, recording vital signs like temperature, pulse, blood pressure, and respiratory rate, painting a picture of one's physiological landscape.The form is not just a static record, however; it's a dynamic tool that evolves with the individual. As health status changes, so do the entries on the form. It becomes achronicle of health journeys, documenting weight loss or gain, changes in vision or hearing, and new medical diagnoses. In this way, the form serves as a continuous reminder of the importance of self-care and regular check-ups.The importance of the physical examination form extends beyond the individual. It's a communication tool between patients and healthcare providers, ensuring that critical information is accurately transmitted. Doctors rely on these forms to gain a quick understanding of theirpatients' health backgrounds, allowing them to make informed decisions about treatment plans and medications. Moreover, the form serves as a link to the larger healthcare system. It's often shared among multiple providers, ensuring continuity of care even when patients transition between different facilities or specialists. In this way, the form helps to build a comprehensive health profile that can be accessed and referenced by multiple parties.In conclusion, the physical examination form is a vital component of our healthcare system. It's a dynamic documentthat evolves with us, capturing our health journeys and serving as a guide for future care. It's a communicationtool that bridges the gap between patients and providers, ensuring that critical information is shared and understood. And it's a link to the larger healthcare system, connecting us to the resources and providers we need to maintain our well-being. As we navigate the complexities of modern healthcare, let us remember the importance of the physical examination form and the role it plays in our journey towards health and wellness.**体检表的重要性:健康与福祉的旅程**在现代医学的快节奏世界中,体检表如同一位沉默的守护者,记录着个人的健康状况。

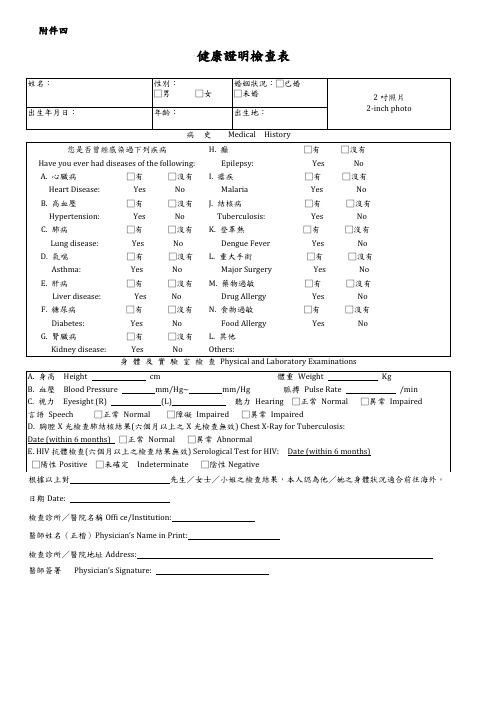
健康診断書CERTIFICATE OF HEALTH (to be completed by the examining physician)日本語又は英語により明瞭に記載すること。
Please fill out (PRINT/TYPE) in Japanese or English.氏名□男Male 生年月日年齢Name: , □女Female Date of Birth:Age: Family name, First name Middle name1.身体検査Physical Examination(1) 身長体重Height cm Weight kg(2) 血圧血液型脈拍□整regular Blood pressure mm/Hg~mm/Hg Pulse□不整irregular(3) 視力Eyesight: (R) (L)(R) (L)色覚異常の有無□正常normal 裸眼Without glasses矯正With glasses or contact lenses Color blindness □異常impaired(4) 聴力□正常normal 言語□正常normalHearing: □低下impaired Speech: □異常impaired2.申請者の胸部について,聴診とX線検査の結果を記入してください。
X線検査の日付も記入すること(6ヶ月以上前の検査は無効。) Please describe the results of physical and X-ray examinations of the applicant's chest x-rays (X-rays taken more than 6 months priorto this certification are NOT valid).肺□正常normal 心臓□正常normalLungs:□異常impaired Cardiomegaly: □異常impaired↓←Date 異常がある場合Film No. 心電図Electrocardiograph :□正常normal□異常impaired Describe the condition of applicant's lungs.3.現在治療中の病気□Yes (Conditions/particulars: ) Under medical treatment at present □No4.既往症Past history : Please indicate with +or -and fill in the date of recoveryTuberculosis......□( . . ) Malaria.......□( . . ) Other communicable disease......□( . . )Epilepsy......□( . . ) Kidney disease.....□( . . ) Heart disease......□( . . )Diabetes......□( . . ) Drug allergy......□( . . ) Psychosis.....□( . . )Functional disorder in extremities......□( . . )5.検査Laboratory tests検尿Urinalysis: glucose ( ), protein ( ), occult blood ( )赤沈ESR:mm/Hr, WBC count:/cmm 貧血□anemiaHemoglobin:gm/dl, GPT:6.志願者の既往歴,診察・検査の結果から判断して,現在の健康の状況は充分に留学に耐えうるものと思われますか?Yes又はNoにチェックをしてください。

健康診断書CERTIFICATE OF HEALTHPlease fill out (PRINT/TYPE) in Japanese or English.氏名生年月日□男Male Name: , Date of Birth: //□女Female Family name First name , Middle nameApplicant健康診断の前に下記の質問に答えてください。
Please answer the questions below before submitting to a physician for your physical examination.1. 過去5年間に以下の病気あるいは大きな病気にかかったことがあれば記入してください。
Please check the list of diseases below and/or specify if you have had in the past five years.□ぜんそくAsthma □結核Tuberculosis □マラリアMalaria □てんかん Epilepsy □糖尿病 Diabetes □心臓病Heart Disease □腎臓病 Kidney Disease □肝臓病 Liver Disease □精神疾患 Psychosis□その他Other()2.薬、食べ物、動物、その他でアレルギーがありますか。
はいいいえDo you have any allergies to drugs ,foods, animals and other? Yes /No具体的に記入してください。
Please specify.( )3.現在、何かの病気で薬を常用していますか。
はいいいえAre you taking medication now? Yes / No 病名Disease 服用薬 medication( ) ()Physician1. 身体検査Physical Examination身長体重血液型 RH +Height cm Weight kg Blood Type - A B O AB血圧Blood Pressure mm/Hg ~mm/Hg視力Eyesight (R) (L) (R) (L) 色覚異常の有無□正常normal 裸眼without glasses 矯正 with glasses or contact lenses color blindness □異常 impaired聴力□正常 normalHearing □低下 impaired2. 申請者の胸部について、聴診とX線検査の結果を記入してください。

英语介绍体检表,作文结尾英文回答:A physical exam, also known as a checkup, is a medical examination performed by a healthcare professional to assess a person's overall health and well-being. It typically involves a series of tests and measurements, including:Medical history: The healthcare professional will ask about the patient's past and present medical history, including any illnesses, surgeries, or medications.Physical examination: The healthcare professional will examine the patient's head, neck, chest, abdomen, and extremities, looking for any signs of illness or injury.Vital signs: The healthcare professional will measure the patient's blood pressure, heart rate, temperature, and respiratory rate.Laboratory tests: The healthcare professional may order laboratory tests, such as blood tests or urine tests, to check for any underlying medical conditions.Imaging tests: The healthcare professional may order imaging tests, such as X-rays or CT scans, to visualize the patient's internal organs and structures.Physical exams are typically performed on a regular basis, such as once a year, to screen for any health problems and to monitor overall health. They can also be performed more frequently if a person is experiencing symptoms of an illness or injury.There are many benefits to getting regular physical exams. These benefits include:Early detection of health problems: Physical exams can help to detect health problems early on, when they are most treatable. This can help to prevent serious health problems or even death.Monitoring of chronic conditions: If a person has a chronic condition, such as diabetes or heart disease, regular physical exams can help to monitor the condition and make sure that it is being managed properly.Health education: Physical exams can be a good opportunity to learn about your health and how to improve it. The healthcare professional can provide you with information on healthy eating, exercise, and otherlifestyle factors.Overall, physical exams are an important part of maintaining good health. By getting regular physical exams, you can help to detect health problems early on, monitor chronic conditions, and learn about your health and how to improve it.中文回答:体检,也称为健康检查,是由医疗专业人员进行的一项医学检查,用于评估个人的整体健康状况和健康状况。

体检报告英模板IntroductionHealth is an important aspect of living. Regular health check-ups can help identify any potential health problems earlier and prevent them from turning into more serious conditions later on. In this document, we provide a template for a health check-up report in English.Patient Information•Name:•Age:•Gender:•Date of birth:•Blood type:•Date of check-up:Medical History•Allergies:•Chronic diseases:•Past surgeries:•Regular medications:Vital Signs•Blood pressure:•Heart rate:•Respiratory rate:•Temperature:Laboratory ResultsBlood Tests•White blood cells (WBC):•Red blood cells (RBC):•Hemoglobin (HGB):•Hematocrit (HCT):•Platelets (PLT):•Glucose:•Total cholesterol:•LDL cholesterol:•HDL cholesterol:•Triglycerides:Urine Tests•Color:•Appearance:•pH:•Protein:•Glucose:•Ketones:•Bilirubin:•Urobilinogen:Stool Tests•Color:•Consistency:•Occult blood:•Ova and parasites:Imaging Tests•X-ray:•Ultrasound:•CT scan:•MRI:RecommendationsBased on the results of the health check-up, the following recommendations are made:•Maintain a healthy diet and exercise regularly to lower total cholesterol and LDL cholesterol levels.•Regularly monitor blood pressure and schedule follow-up appointments if it remains high.•Reduce stress levels by practicing relaxation techniques, such as meditation or yoga.•Get regular cancer screenings based on age and family history.ConclusionOverall, the health check-up showed no serious health problems. Recommendations have been made to address any minor issues. The patient is advised to maintain regular check-ups and follow up on any recommendations provided.。
英语作文健康证明模板英文回答:Health Certificate Template。
Personal Information。
Name:Date of Birth:Gender:Occupation:Address:Contact Number:Medical History。
Current Medications: List all medications you are currently taking, including prescription and over-the-counter drugs.Allergies: List any allergies you have, including food, medication, or environmental allergies.Immunization Status: List all immunizations you have received, including dates and types.Past Medical Conditions: Describe any significant medical conditions you have had in the past, including treatments received and outcomes.Family Medical History: Describe any significant medical conditions that run in your family, including those that are hereditary.Physical Examination。
General Appearance: Describe the patient's overallappearance, including weight, height, and body mass index (BMI).Vital Signs: Include blood pressure, pulse,respiration rate, and temperature.Head, Neck, and Thyroid: Describe any abnormalities in the head, neck, or thyroid area.Cardiovascular System: Auscultate the heart and lungs for any murmurs, rales, or wheezes.Respiratory System: Note any abnormalities in the respiratory system, such as shortness of breath or coughing.Gastrointestinal System: Palpate the abdomen for any tenderness, masses, or hernias.Genitourinary System: Examine the external genitalia and perform a prostate exam if indicated.Musculoskeletal System: Assess the patient's range ofmotion and joint function.Neurological System: Test the patient's reflexes, coordination, and sensation.Psychiatric Examination: Evaluate the patient's mental health, including mood, affect, and thought processes.Laboratory Tests。

the health examination report date:篇二:检验报告常用英文汇总【简要介绍】除了上次介绍的血常规检查以外,血生化也是一项很常见的化验检查项目。
cmp是相对于bmp(basic metabolic panel)而言的。
bmp俗称“小生化”,或“基本生化”。
bmp包括8项“核心”生化检查。
cmp则在bmp所检查的8项核心内容的基础上,又添加了6项检查,共14项,因此称为“生化全项”。
另外,在一些国家和地区,除了cmp中的14项检查外,更进一步添加另外6项内容,合称“血生化20项”,英文简写为sma-20,或smac-20,或chem 20等。
【检查项目】本文主要介绍生化20项中除了血胆固醇外的19项内容,并另外加上一项“血镁”。
有关血胆固醇的信息将在以后的“血脂”检查中进一步讨论。
主要项目有:1。
bmp。
包括5项基本电解质:钠(sodium,,na),钾( potassium,k),氯(chloride,,cl),碳酸氢离子(bicarbonate,hco3),以及钙(calcium ca)。
2项肾功能检查:肌酐(creatinine),及尿素氮(blood urea nitrogen,bun)。
再加1项血糖(glucose)。
2。
cmp中另外6项。
包括2项蛋白指标:总蛋白(total protein,tp)及白蛋白(albumin)。
和4项肝功能检查:碱性磷酸酶(alkaline phosphatase,alp),谷丙转氨酶(alanine aminotransferase,alt/sgpt),谷草转氨酶(aspartate amino transferase,alt/sgot),和胆红素(bilirubin)。
3。
sma-20(或chem 20)中多出来的6项。
包括3项肝功能检查:直接胆红素(directbilirubin),谷酰转肽酶(gamma-glutamyl transpeptidase,ggt),乳酸脱氢酶(lactate dehydrogenase,ldh)。


新版健康证明英文翻译模板IntroductionContentThe translation should include the following information:- Name of the individual- Identification number or passport number- Date of birth- Gender- Nationality- Issuing authority of the health certificate- Date of issue- Validity period of the health certificate- Description of the health condition, stating that the individual is in good health and free from any infectious diseases- Stamp or seal of the issuing authoritySample Translation TemplateNew Version Health Certificate (English Translation)Name: [Full Name]ID/Passport Number: [Identification or Passport Number]Date of Birth: [Date of Birth]Gender: [Gender]Nationality: [Nationality]This is to certify that [Full Name], holder of ID/Passport number [Identification or Passport Number], born on [Date of Birth], is in good health and free from any infectious diseases. The health certificate is issued by [Issuing Authority] on [Date of Issue] and is valid until [Validity Period].Issue Date: [Date of Issue]Valid until: [Validity Period]Issuing Authority: [Issuing Authority]Stamp/Seal: [Stamp/Seal]Please note that this translation is provided for reference purposes only and should be verified by the relevant authorities.Please remember to verify the accuracy of the translation with the relevant authorities before using it for any official purposes.以上是关于"新版健康证明英文翻译模板"的文档,该模板可以用于将"新版健康证明"翻译成英文。

3HEAL TH CERTIFICA TE健康診断書Full Name: Date of Birth:(氏名)(生年月日)Y ear / Month / DayPlease answer the questions below by checking the appropriate box, before submitting to a physician for your physical examination.(健康診断を医師に申込む前に下記の設問に関しいずれかをチェックしてください。
)1.What diseases, disorders or injuries have you had in the past five years? (過去5年間にかかった病気あるいは怪我の名を書いてください。
)2.Do you have any allergies to foods, plants or animals? Y es / No(食物、動植物にアレルギーはありますか。
)3.Have you ever had an adverse reaction to medication? Y es / No(薬に対してアレルギーはありますか。
)4.Are you taking medication now? (現在、何か薬を飲んでいますか。
) Y es / NoTo the physician (医師の方へ):Please review the applicant’s medical history and complete the information below, giving details concerning any positive indications. If there are any abnormalities in the following systems, circle the appropriate answer and explain in detail. (患者の病・傷害歴をお読みになってから診断、ご記入ください。

健康证明英文模板HEALTH CERTIFICATECertificate No.: [编号]Name of the Certificate Holder: [持有人姓名]Date of Birth: [出生日期]Gender: [性别]Issuing Date: [签发日期]Validity Period: [有效期]I, the undersigned medical practitioner, certify that I have examined [持有人姓名], and based on my examination, I confirm that:1. The certificate holder is free from any communicable diseases.2. The certificate holder is physically and mentally fit.3. No symptoms or signs of COVID-19 have been observed in the certificate holder.This certificate is issued for the purpose of [健康证明用途,例如:travel, employment, education等]. It is valid for [有效期] from the date of issuance.Medical Practitioner: [医生签名]Name: [医生姓名]Qualification: [医生资质]Clinic/Hospital Name: [诊所/医院名称]Contact Number: [联系电话]Stamp/Seal of the Clinic/Hospital: [诊所/医院盖章]请注意,如果您需要使用这种健康证明,您可能需要找一个合格的医生进行检查,并由医生填写和签署该证明。

醫院標誌Hospital’s Logo健康檢查證明應檢查項目表(乙表)(國名、醫院名稱、地址、電話、傳真機)ITEMS REQUIRED FOR HEAL TH CER TIFICA TE (Type B)(National Name, Hospital’s Name, Address, Tel, FAX)檢查日期 ____/____/____(年) (月) (日)____/____/____(M) (D) (Y)Date of Examination一、本表供外籍人士等申請在台灣定居或居留時使用。
This form is for residence application.二、兒童6歲以下免辦理健康檢查,但須檢具預防接種證明備查(年滿1歲以上者,至少接種1劑麻疹、德國麻疹疫苗)。
A child under 6 years old is not necessary to have laboratory examination, but the certificate of vaccination is necessary. Child age one and above should get at least one dose of measles and rubella vaccines.三、妊娠孕婦及兒童12歲以下免接受「胸部X光檢查」。
Pregnant women and children under 12 years of age areexempted from chest X-ray examination.四、兒童15歲以下免接受「HIV抗體檢查」及「梅毒血清檢查」。
A child under 15 years old is not necessary to haveSerological Test for HIV or Syphilis.五、居住於北美洲、歐洲、紐西蘭、澳洲、日本、南韓、香港、澳門及新加坡等地區或國家之申請者,得免驗腸內寄生蟲糞便檢查。
英文健康体检表CERTIFICATE OF HEALTH最新文档(可以直接使用,可编辑最新文档,欢迎下载)健康診断書CERTIFICATE OF HEALTHPlease fill out (PRINT/TYPE) in Japanese or English.氏名生年月日□男MaleName: , Date of Birth: //□女FemaleFamily nameFirst name,Middle nameApplicant健康診断の前に下記の質問に答えてください。
Please answer the questions below before submitting to a physician for your physical examination.1. 過去5年間に以下の病気あるいは大きな病気にかかったことがあれば記入してください。
Please check the list of diseases belowand/or specify if you have had in the past five years.□ぜんそくAsthma □結核Tuberculosis □マラリアMalaria □てんかん Epilepsy □糖尿病 Diabetes □心臓病Heart Disease □腎臓病 Kidney Disease □肝臓病 Liver Disease□精神疾患 Psychosis□その他Other()2.薬、食べ物、動物、その他でアレルギーがありますか。
はいいいえDo you have any allergies to drugs ,foods, animals and other? Yes /No具体的に記入してください。
Please specify.( )3.現在、何かの病気で薬を常用していますか。
はいいいえAre you taking medication now? Yes / No 病名Disease 服用薬medication( ) ()Physician1. 身体検査Physical Examination身長体重血液型 RH +Height cm Weight kg Blood Type - AB O AB血圧Blood Pressure mm/Hg ~mm/Hg視力Eyesight (R) (L) (R) (L) 色覚異常の有無□正常normal裸眼without glasses 矯正 with glasses or contact lenses color blindness □異常 impaired聴力□正常 normalHearing □低下 impaired2. 申請者の胸部について、聴診とX線検査の結果を記入してください。
X線検査の日付も記入すること(6ヶ月以上前の検査は無効)Please describe the results of physical and X-ray examinations of applicant’s chest (X-ray taken more than 6 months prior to the certification is NOT valid).肺□正常normal 心臓□正常normalLung □異常 impaired Heart□異常 impaired↓Date 心電図Film No Electrocardiograph:□正常normalDescribe the condition of applicant’slung. □異常 impaired3.検査Laboratory tests検尿Urinalysis糖Glucose(), 蛋白Protein(), 潜血Occult blood()血液検査Blood test赤血球数 WBC count:×104 /μl, 白血球数WBC count: /μl4.Please describe your impression.5.志願者の既往歴,診察・検査の結果から判断して,現在の健康状況は十分に留学に耐えうるものと思われますか?In view of the applicant’s history and the above findings, do you think his/her health status is adequate to pursue study in Japan? はいいいえYES / NO日付署名Date: Signature医師氏名Physician’s name in print:検査施設名Office/Institution所在地Address工人健康体检表健康体检表高血压患者健康管理服务规范一、服务对象辖区内35岁及以上原发性高血压患者。
二、服务内容(一)筛查1.对辖区内35岁及以上常住居民,每年在其第一次到乡镇卫生院、村卫生室、社区卫生服务中心(站)就诊时为其测量血压。
2.对第一次发现收缩压≥140mmHg和(或)舒张压≥90mmHg的居民在去除可能引起血压升高的因素后预约其复查,非同日3次血压高于正常,可初步诊断为高血压。
如有必要,建议转诊到上级医院确诊,2周内随访转诊结果,对已确诊的原发性高血压患者纳入高血压患者健康管理。
对可疑继发性高血压患者,及时转诊。
3.建议高危人群每半年至少测量1次血压,并接受医务人员的生活方式指导。
(二)随访评估对原发性高血压患者,每年要提供至少4次面对面的随访。
(1)测量血压并评估是否存在危急情况,如出现收缩压≥180mmHg和(或)舒张压≥110mmHg;意识改变、剧烈头痛或头晕、恶心呕吐、视力模糊、眼痛、心悸、胸闷、喘憋不能平卧及处于妊娠期或哺乳期同时血压高于正常等危急情况之一,或存在不能处理的其他疾病时,须在处理后紧急转诊。
对于紧急转诊者,乡镇卫生院、村卫生室、社区卫生服务中心(站)应在2周内主动随访转诊情况。
(2)若不需紧急转诊,询问上次随访到此次随访期间的症状。
(3)测量体重、心率,计算体质指数(BMI)。
(4)询问患者疾病情况和生活方式,包括心脑血管疾病、糖尿病、吸烟、饮酒、运动、摄盐情况等。
(5)了解患者服药情况。
(三)分类干预(1)对血压控制满意(收缩压<140且舒张压<90mmHg)、无药物不良反应、无新发并发症或原有并发症无加重的患者,预约进行下一次随访时间。
(2)对第一次出现血压控制不满意,即收缩压≥140 mmHg和(或)舒张压≥90mmHg,或出现药物不良反应的患者,结合其服药依从性,必要时增加现用药物剂量、更换或增加不同类的降压药物,2周内随访。
(3)对连续两次出现血压控制不满意或药物不良反应难以控制以及出现新的并发症或原有并发症加重的患者,建议其转诊到上级医院,2周内主动随访转诊情况。
(4)对所有的患者进行有针对性的健康教育,与患者一起制定生活方式改进目标并在下一次随访时评估进展。
告诉患者出现哪些异常时应立即就诊。
(四)健康体检对原发性高血压患者,每年进行1次较全面的健康检查,可与随访相结合。
内容包括体温、脉搏、呼吸、血压、身高、体重、腰围、皮肤、浅表淋巴结、心脏、肺部、腹部等常规体格检查,并对口腔、视力、听力和运动功能等进行粗测判断。
具体内容参照《城乡居民健康健康档案管理服务规范》健康体检表。
四、服务要求(一)高血压患者的健康管理由医生负责,应与门诊服务相结合,对未能按照管理要求接受随访的患者,乡镇卫生院、村卫生室、社区卫生服务中心(站)医务人员应主动与患者联系,保证管理的连续性。
(二)随访包括预约患者到门诊就诊、追踪和家庭访视等方式。
(三)乡镇卫生院、村卫生室、社区卫生服务中心(站)可通过本地区社区卫生诊断和门诊服务等途径筛查和发现高血压患者。
有条件的地区,对人员进行规范培训后,可参考《中国高血压防治指南》对高血压患者进行健康管理。
(四)发挥中医药在改善临床症状、提高生活质量、防治并发症中的特色和作用,积极应用中医药方法开展高血压患者健康管理服务。
(五)加强宣传,告知服务内容,使更多的患者和居民愿意接受服务。
(六)每次提供服务后及时将相关信息记入患者的健康档案。
填表说明1.本表为高血压患者在接受随访服务时由医生填写。
每年的健康体检后填写城乡居民健康档案管理服务规范的健康体检表。
2.体征:体质指数=体重(kg)/身高的平方(m2),体重和体质指数斜线前填写目前情况,斜线后下填写下次随访时应调整到的目标。
如果是超重或是肥胖的高血压患者,要求每次随访时测量体重并指导患者控制体重;正常体重人群可每年测量一次体重及体质指数。
如有其他阳性体征,请填写在“其他”一栏。
3.生活方式指导:在询问患者生活方式时,同时对患者进行生活方式指导,与患者共同制定下次随访目标。
日吸烟量:斜线前填写目前吸烟量,不吸烟填“0”,吸烟者写出每天的吸烟量“××支”,斜线后填写吸烟者下次随访目标吸烟量“××支”。
日饮酒量:斜线前填写目前饮酒量,不饮酒填“0”,饮酒者写出每天的饮酒量相当于白酒“××两”,斜线后填写饮酒者下次随访目标饮酒量相当于白酒“××两”。
白酒1两相当于葡萄酒4两,黄酒半斤,啤酒1瓶,果酒4两。
运动:填写每周几次,每次多少分钟。
即“××次/周,××分钟/次”。
横线上填写目前情况,横线下填写下次随访时应达到的目标。
摄盐情况:斜线前填写目前摄盐的咸淡情况。
根据患者饮食的摄盐情况,按咸淡程度在列出的“轻、中、重”之一上划“√”分类,斜线后填写患者下次随访目标摄盐情况。
心理调整:根据医生印象选择对应的选项。
遵医行为:指患者是否遵照医生的指导去改善生活方式。
4.辅助检查:记录患者在上次随访到这次随访之间到各医疗机构进行的辅助检查结果。
5.服药依从性:“规律”为按医嘱服药,“间断”为未按医嘱服药,频次或数量不足,“不服药”即为医生开了处方,但患者未使用此药。
6.药物不良反应:如果患者服用的降压药物有明显的药物不良反应,具体描述哪种药物,何种不良反应。
7.此次随访分类:根据此次随访时的分类结果,由随访医生在4种分类结果中选择一项在“□”中填上相应的数字。
“控制满意”意为血压控制满意,无其他异常、“控制不满意”意为血压控制不满意,无其他异常、“不良反应”意为存在药物不良反应、“并发症”意为出现新的并发症或并发症出现异常。
如果患者同时并存几种情况,填写最严重的一种情况,同时结合上次随访情况确定患者下次随访时间,并告知患者。
8.用药情况:根据患者整体情况,为患者开具处方,并填写在表格中,写明用法、用量。