Body position
- 格式:pdf
- 大小:108.03 KB
- 文档页数:7

html5元素的坐标HTML5元素的坐标通常指的是元素在页面中的位置,可以使用CSS的position属性来指定元素的位置。
常用的position值有:1. static(默认值):元素在文档流中正常的位置,不受其他定位属性的影响。
2. fixed:元素相对于浏览器窗口进行定位,始终保持在指定位置,不随页面滚动而移动。
3. relative:元素相对于其正常位置进行定位,可以通过top、right、bottom、left属性来指定距离。
4. absolute:元素相对于最近的非static定位的父元素进行定位,如果没有非static定位的父元素,则相对于body元素进行定位。
通过设置position属性,可以使用top、right、bottom、left属性来调整元素的位置。
这些属性可以接受具体的像素值,也可以使用百分比来表示相对于父元素的距离。
例如,下面的代码使用CSS来设置元素的位置:```<!DOCTYPE html><html><head><style>#myElement {position: absolute;top: 50px;left: 100px;}</style></head><body><div id="myElement">This is my element.</div></body></html>```上述代码中,id为“myElement”的元素被设置为绝对定位,距离其最近的非static定位的父元素的top距离为50px,左边距离为100px,因此该元素会在页面中距离左上角(0,0)的位置(100,50)处显示。

滑雪常见基本术语中英文对照有哪些想要更好地了解滑雪这一项运动就需要了解他的术语,今天店铺给大家分享一些滑雪常见术语,希望对大家有所帮助。
滑雪术语一:猫跳滑雪的基本身体姿势Stack: Basic Body alignment with thehips and shoulders stacked over the down hill foot.堆叠:臀部和肩部叠在山下脚上方的基本身体姿势Lead Change: When the body isstacked properly over the downhill foot the uphill knee naturallyadvances forward. The leading knee changes as the weight shiftsonto the new downhill ski引导变换:当身体正确叠在山下脚的上方时,山上腿的膝盖是自然前出的。
随着重心转移到新的山下板时,引导膝盖也发生了变化。
Transitions: The weight shifts fromdown hill ski to the new downhill ski using lead change with out upweighting and down weighting.转换:利用引导变换将重心从山下板转移到新的山下板上,没有重心的上下移动。
Knee Roll: As the weight shifts ontothe new ski the knees roll into the angle of the new turn.膝盖转动:随着重心移到新的雪板上,膝盖转动到下个回转的角度。
Knee Angle: The ski is put on edgewith knee angle not hip angle. This allows the knees to bend freelyup and down.膝盖角度:雪板要置于膝盖的角度而不是臀部的角度。
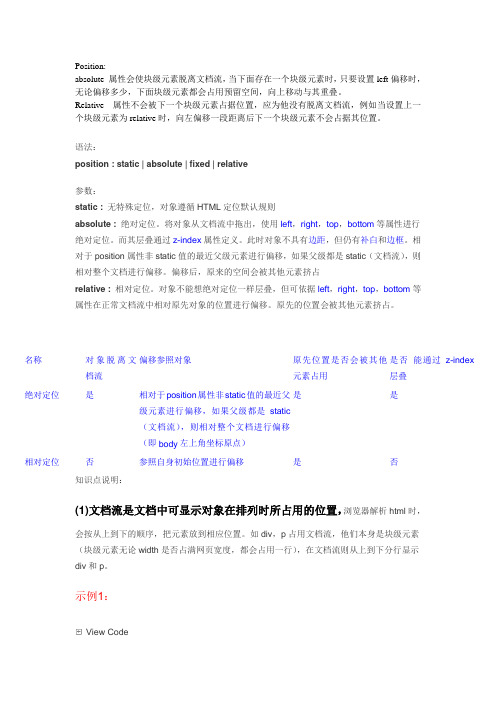
Position: absolute 属性会使块级元素脱离文档流,当下面存在一个块级元素时,只要设置left 偏移时,无论偏移多少,下面块级元素都会占用预留空间,向上移动与其重叠。
Relative 属性不会被下一个块级元素占据位置,应为他没有脱离文档流,例如当设置上一个块级元素为relative 时,向左偏移一段距离后下一个块级元素不会占据其位置。
语法: position : static | absolute | fixed | relative 参数: static : 无特殊定位,对象遵循HTML 定位默认规则 absolute : 绝对定位。
将对象从文档流中拖出,使用left ,right ,top ,bottom 等属性进行绝对定位。
而其层叠通过z-index 属性定义。
此时对象不具有边距,但仍有补白和边框。
相对于position 属性非static 值的最近父级元素进行偏移,如果父级都是static (文档流),则相对整个文档进行偏移。
偏移后,原来的空间会被其他元素挤占 relative : 相对定位。
对象不能想绝对定位一样层叠,但可依据left ,right ,top ,bottom 等属性在正常文档流中相对原先对象的位置进行偏移。
原先的位置会被其他元素挤占。
知识点说明:(1)文档流是文档中可显示对象在排列时所占用的位置,浏览器解析html 时,会按从上到下的顺序,把元素放到相应位置。
如div ,p 占用文档流,他们本身是块级元素(块级元素无论width 是否占满网页宽度,都会占用一行),在文档流则从上到下分行显示div 和p 。
示例1:View Code 名称对象脱离文档流 偏移参照对象 原先位置是否会被其他元素占用 是否 能通过z-index 层叠 绝对定位是 相对于position 属性非static 值的最近父级元素进行偏移,如果父级都是static (文档流),则相对整个文档进行偏移(即body 左上角坐标原点) 是 是 相对定位否 参照自身初始位置进行偏移 是 否<div style="width:300px;height:100px;border:1px solid red">我是div标签</div><p style="width:300px;height:100px;border:1px solid red">我是p标签</p>而如果想让div位置脱离文档流偏移,让解析时,把div脱离文档流,相对左上角原点向右偏移400px,把p放到文档流中,占用div本来的位置,则可以用绝对定位。
<html>:表示html文件的起始和终止,<html>标签在首行,</html>标签在最后一行,两个要一起使用,网页中其他内容都要放在这两个标签之间。
<head>:表示网页的头部标签,用来定义文件的头部信息,与<html>标签一样,也是<head></head>成对使用。
<body>:表示出文件主体区,<body></body>之间是网页的主题内容和其他用于控制文本显示方式的标签。
<title>:网页标题,用于定义浏览器窗口标题栏上的文本信息,可以是网页的标题名或创作信息等网页说明信息。
<hr>:用于显示水平线,使页面看起来更整齐明了。
<pre>:将内容以原始格式显示。
<address>:标注联络人姓名、电话、地址等信息。
<blockquote>:区段引用标签。
<!————>:注释标签,使用注释标签的目的是为网页代码中不同部分加上说明,方便日后的修改。
注释的内容是不会在浏览器上显示出来的,如<——要注释的内容——>。
<p>:文本段落,可以用align属性设置left、center、right 3种对齐方式。
<br/>:强制换行,没有结束标签,在网页中产生换行效果。
<center>:使文字或其他网页元素居中显示。
<marquee>:文本或图片移动显示,属性direction用来指示移动方向。
<dl>、<dt>、<dd>:<dl></dl>标签创建无序列表,<dt></dt>定义上层项目,<dd>、</dd>定义下层项目,<dt>、</dt>和<dd></dd>标签一定要放在<dl></dl>标签中才能使用。

Swimming is a fantastic sport that offers a fullbody workout and is enjoyed by people of all ages.It is not only a great way to stay fit but also a lifesaving skill.There are four main swimming strokes that are widely recognized and practiced:freestyle, breaststroke,backstroke,and butterfly.Each stroke has its own unique technique and is suited to different types of swimmers.Freestyle Front Crawl:The freestyle is the fastest swimming stroke and is often the first stroke taught to beginners.It involves a symmetrical arm movement where one arm enters the water and pulls while the other arm recovers above the water.The legs perform a flutter kick, similar to a dolphins tail.The head turns to the side to breathe,with the body remaining as horizontal as possible.This stroke is called freestyle because swimmers are free to choose their breathing pattern and the timing of their strokes.Breaststroke:The breaststroke is a more leisurely stroke that is characterized by its unique kick,which is similar to a frogs leg movement.The arms move in an outward,semicircular motion, then inward and forward,with the palms facing outward.The head is lifted out of the water during the arm recovery phase,allowing the swimmer to breathe.The body position in breaststroke is more upright compared to other strokes,and the kick is performed with the legs bent at the knees and then extended outwards and back together.Backstroke:Swimming on ones back,the backstroke is a relaxing and enjoyable stroke.The arms move in alternating,windmilllike motions,with the palms facing down and the recovery phase above the water.The legs perform a flutter kick,similar to the freestyle,but with the body in a supine position.Breathing is straightforward in backstroke as the swimmers face is always above water.Its essential to keep the head in a neutral position to avoid straining the neck.Butterfly:The butterfly stroke is the most physically demanding of the four strokes and is often reserved for more advanced swimmers.It involves a simultaneous,undulating arm movement that starts with the arms extended above the head and then pulling down and out in a wide arc.The legs perform a dolphin kick,with a slight bend at the knees, moving in a continuous,undulating motion.The head moves in a rhythm with the arm movements,lifting out of the water to breathe during the recovery phase.Each of these strokes requires practice to master,and they all contribute to building strength,endurance,and cardiovascular fitness.Whether youre swimming for fun,competition,or as part of a fitness routine,understanding and practicing these four strokes can greatly enhance your swimming experience.。

自由泳练习方法的英语Freestyle Swimming: Techniques and Practice MethodsFreestyle swimming, also known as the front crawl, is a popular and versatile stroke used in competitive swimming and recreational water activities. It is characterized by its continuous arm movements, alternating leg kicks, and streamlined body position. Here are some fundamental techniques and practice methods to improve your freestyle swimming skills.1. Body Position:Maintaining a horizontal body position is crucial forefficient freestyle swimming. Keep your head in line with your spine, looking slightly downward into the water to avoid lifting your head too high, which can disrupt your body alignment and slow you down.2. Arm Movement:The arm movement in freestyle consists of an alternating pattern. One arm enters the water ahead and extends fully while the other arm recovers and swings forward. The catch phase involves pulling the water from a high elbow position, followed by a push phase where the hand propels backward towards the thigh.3. Breathing Technique:Breathing in freestyle is typically done by turning your headto the side, allowing one ear to remain in the water. Inhale quickly as your mouth clears the water and then exhale slowly underwater. Practice bilateral breathing, alternating sides, to maintain balance and body rotation.4. Leg Kick:The leg kick in freestyle is a continuous flutter kick, with alternating up and down movements. Keep your legs close together and kick from the hips, not the knees. This kick helps maintain body position and propulsion without expending too much energy.5. Body Rotation:Rotating your body from the hips while swimming can enhance your stroke efficiency. It allows for a more powerful armpull and helps with breathing. Aim for a slight rotation, about 45 degrees, from the centerline of your body.6. Drills for Improvement:- Sculling Drills: Use your hands to create propulsion while floating on your back or stomach. This helps with hand positioning and feel for the water.- Kickboard Drills: Use a kickboard to focus solely on your leg kick, ensuring proper technique without the distraction of arm movements.- Pull Buoy Drills: Hold a pull buoy between your legs to isolate your upper body work, focusing on arm movements and body rotation.7. Endurance Training:Incorporate endurance sets into your training routine. Thesesets involve swimming a set distance or number of lapswithout stopping, which helps build stamina and muscle memory.8. Interval Training:Interval training involves alternating periods of high-intensity swimming with periods of rest or low-intensity swimming. This method is excellent for improving speed and cardiovascular fitness.9. Proper Equipment:Using the right equipment such as goggles, swim caps, and properly fitting swimwear can enhance your practice sessionsby reducing distractions and increasing comfort in the water.10. Consistent Practice:Regular practice is key to improving your freestyle swimming. Set goals for yourself and track your progress over time.11. Coaching and Feedback:Working with a coach or seeking feedback from experienced swimmers can provide valuable insights into your techniqueand areas for improvement.12. Visualization:Before entering the water, take a moment to visualize your stroke. This mental rehearsal can help reinforce proper technique and improve performance.By focusing on these techniques and incorporating them into your swimming practice, you can enhance your freestyle swimming skills and enjoy a more efficient and enjoyableexperience in the water. Remember, patience and consistent practice are essential for mastering any swimming stroke.。
一般检查generalexamination一, 性别sex男Male女Female二,年龄age三,生命体征:vital age体温body temperaturea,口测法oral measurementﻩb,肛测法archos measurementc,腋测法axil measurement呼吸respirations脉搏pulse血压blood pressure四,发育development体型(Habitus):无力型(asthenic type)、超力型(sthenictype)、正力型(orthosthenic type)五,营养state of nutrition:良好well、中等moderatelty.肥胖(Obesity)、消瘦slake六,意识consciousness: 嗜睡drowsiness、意识模糊clouding ofconsciousness昏睡hyponody、昏迷coma(浅,中,深度),谵妄acute confusionalstate七,语调tone 语态voice八,面容facial features急性病容faceof acuteill,慢性病容chronic disease face,贫血面容anemic face,甲亢面容hypert hyreosis feature,粘液性水肿面容myxedema face, 二尖瓣面容mitralfacies,满月脸面容moon face,肢端肥大症面容acromegaly facies,伤寒面容typhoidface,病危面容,Hippocrates face表情expression 正常normal,淡漠indifference烦躁不安dysphoria,痛苦suffering忧郁gloom九,体位positiona,自主体位active position b,被动体位passive position 极度意识衰竭和丧失culmination consciousness failureandlossc,强迫体位compulsiveposition强迫坐位(端坐呼吸)compulsivesitting position (orthopnea)十,姿势posture十一,步态gaitaa,蹒跚步态waddling gaitb,醉酒步态drinken man gaitc,共济失调步态ataxicgait d,慌张步态fe stinating gait e,跨閱步态steppage gaitf,剪刀步态scissorgait g,间歇性跛行intermittent gait十二,皮肤skin1,颜色skincolor a,苍白pallor 贫血anaemiab,发红redness发热fever c,发绀cyanosis 缺氧ﻩhypoxia d,黄染stainedyellow 肝病liverdisease e,色素沉着pigmentation 肝病li verdisease f,色素脱失coloringmaterialloss 白化症albinismus2,湿度moisture 干燥dry脱水dewat湿润moist休克shock 3,弹性elasticity4,皮疹skin eruptiona斑疹maculate b玫瑰疹roseola c 丘疹papules; d 斑丘疹maculopapulate ,e荨麻疹urticaria5,脱屑scales6赘生物vegetation 7,皮下出血subcutaneous hemorrhagea 瘀点petechiab瘀斑ecchymosis c 紫癜purpura d血肿hematome8,蜘蛛痣spiderangioma肝掌liver palms 9,水肿edema 10,皮下结节subcutaneous nodules 11,瘢痕scar12,毛发hair 13,淋巴lymph体检(胸腹部)[Physical examination(chestand belly)]1、肋骨和软组织[ribs andsoft tissure]·胸骨上切迹[suprasternalnotch]·浮肋[freeribs]·胸壁[chest wall]·扁平(桶状、佝偻、漏头、鸡)胸[flat (barrel,rachitic,funnel,pigeon)chest]·皮下气肿[subcutaneousemphysema]·捻发音[Crepitus]·软组织损伤[soft tissue injury]·肋骨畸形[abnormality of the ribs(rib deformity,costal anomaly)]·肋软骨畸形[costochondral deformity]·肋软骨增生[costal cartilage hyperplasia]·肋下切口[subcostal incision]·肋间隙宽(窄)[wide (narrow) intercostal space]乳房[breast]3、肺[lung]·呼吸缓慢(急促)[bradypnea (tachypnea)]·呼吸浅慢(深快)[hypopnea (hyperpnea)]·呼吸不规则[irregular respiration]·点头呼吸[noddingbreathing]·端坐呼吸[orthopnea]·三凹征[retractionsign ofthree fossae]·叹息样呼吸[sighing respiration]·浅快[shallow and rapid]·呼(吸)气性呼吸困难[expiratory(inspiratory) dyspnea]·呼吸道烧伤(塌陷)[burn (collapse) ofrespiratorytract(airway)]·呼吸道阻塞[respiratory tractobstruction]·呼吸均匀(呼吸加深或加快)[eupnea(exaggerated or accleratedrespiratory)]·呼吸停止[apnea]·呼吸费力[respirationis labored]·语音(触觉)震颤[vocal(tactile)fremitus]·语颤相等(减弱、增强)[vocal fremitusis equal(diminished,accentuated)]·间接(直接)叩诊[mediate (immediate) percussion]·浊(实、鼓、清、过清、金属)音[dullness(flatness, tympany, vesicular resonance, hyperresonance, bell)]·移动范围[rangeofmovement]·呼吸音消失(减弱,增强)[absence(diminution,exaggeration) ofbreath sound]·呼吸音粗(清)[sound ofbreath(SOB)isrough (clear)]·支气管(支气管肺泡,肺泡)音[bronchophony (bronchovesicular sound,vesicular sound)]·管状呼吸音[tubular breath sound]·捻发音[crepitant rales]·爆裂音[crackles]·干(湿)罗音[dry (moist)rales]·细(中等、粗)罗音[fine(medium, coarse) rales]·呼(吸)气未罗音[end-inspiratory(expiratory)rales]·胸膜摩擦音[pleuralfriction rub]·呼(吸)气延长[prolongedinspiratory (expiratory)]·高(低)调鼾音[sibilant(sonorous) rhonchi(sonorous rales)]·哨笛音[sibilant rales]·哮鸣音[wheezing]·小(中、大)水泡音[small(middle, big) bubbles]·支气管语音[bronchophony]·耳语音[whispered]·羊鸣音[egophony]·高(低)音调[high(low)-pitched]·两肺部(右背部)[over both lung fields (rightback)]·两(左)肺底[over theboth (left)lowerlung]·整个肺野[the whole lung field]·左(右)上(下)肺[theleft (right)upper (lower) lung]·肺尖(底)[apex (base) oflung]4、心脏[Heart]心房心室室间隔房间隔主动脉瓣肺动脉瓣二尖瓣三尖瓣·用手掌(指尖)触诊心尖搏动[palpate apical areawith palm numbness (fingertips)]·心前区隆起(凹陷)[precordial bulge (retraction)]·搏动弥漫(局限)[diffuse(local) pulsation]·负性搏动[inwardinpulse]·心尖搏动[apex beat (apicalimpulse)]·剑突下搏动[xiphoideusal pulsaton]·抬举性心尖搏动[heaving apex impulse]·心尖搏动最强点[point of maximalimpulse (PMI)]·锁骨中线[mid-calvicularline (MCL)]·肋间[intercostalspace(ICS)]·收缩(舒张)期震颤[systolic (diastolic) thrill]·心浊音界[theborderof cardiac dullnes]·心绝对(相对)浊音界扩大(缩小)[enlarged (diminished)absolute(relative) cardiac dullnes s]·叩诊心脏大小正常[heart sizeis normal on(to) percussion]·心脏向左(右)扩大[cardiacdilation (enlargement) to the left(right)]·第1(2、3、4)心音[S1(S2,S3,S4)]·第1心音增强(减弱,听不清)[first heartsound is exaggerate (decreased, muffled)]·生(病)理性杂音(分裂)[physiologic (pathological)murmur (splitting)]·生理性(固定、反常、逆)分裂[physiologic(fixed, paradoxical,reversed) splitting]·肺动脉瓣第2心音>(=,<)主动脉瓣第2心音[P2>(=,〈)A2]·大炮音[connonsound]·心音消失[heart sound is absent (disapeared)]·心音增强(减弱)[accentuated(diminished)cardiacsound]·心音响亮(遥远)[cardiac sound is loud (distant)]·收缩期(舒张期,连续性)杂音[systolic (diastolic, continuous)murmur]·收缩(舒张)前(中、晚)期杂音[pre-(mid—,post) systolic(diastolic)murmur]·全收缩期的[holosystolic(pansystolic)]·全舒张期的[holodiastolic (pandiastolic)]·低(高)音调[low (high)pitched]·递减(递增,递减—递增)性杂音[decrescendo (crescendo, decrescendo—crescendo)murmur]·呈喷射型[beejectionin type]·Ⅳ级喷射型收缩期杂音[gradeⅣ(I-Ⅳ/6)systolic ejectionmurmur]·吹风样杂音[murmurof puffing character]·低音调隆隆样[low-pitched rumbling quality]·柔和(粗糙)的[soft(harshor rough)]·吹风样(喷射性、隆隆样、沙沙声样、搔抓声样、机器声样、汽笛声样、倒水声样)杂音[blowing (ejection, rumbling, rustting,scratching, machinary, whistling, pouring)murmur]·功能性(器质性)杂音[functional (organic) murmur]·血管(静脉)杂音[vascular(venous)murmur]·枪击音[pistol shotsound]·静脉营营音[venous hum]·奔马律[galloprhythm]·胎心律[embryocardia]·心律齐(不齐)[regular (irregular) rhythm]·心律不齐[arrhythmia]·二(三)联律[bigeminy (trigeminy)]·早搏[premature (extrasystol)]·喀嗽音[click]·钟摆律[pendular rhythm]·二尖瓣开瓣音[mitralopening snap]·心包摩擦音[pericardial frictionsound]·听诊[on auscultation]·二尖瓣(主瓣,肺瓣,三尖瓣)听诊区[mitral (aortic,pulmonary,tricuspid)valve area]·心包叩击音[pericardial knock]·肿瘤扑落音[tumorplop]5、腹部[abdomen]·腹膨隆[abdominaldistention(prominence)]·腹平坦(凹陷)[abdominal flatness(retraction)]·蛙状(球状、舟状)腹[frog(bulbous, scaphoid) belly (abdomen)]·腹围增大[increased abdominal girth]·肠型[intestinal pattern]·胃(小肠)蠕动波[gastric (intestinal) peristalticwave]·静脉曲张[varicosity(dilated tortuousvein)]·疤痕[scar]·腹壁紧张(松驰)[guarding (abdominal muscular relaxation)]·腹壁切口(创伤)[incision(wound) of abdominal wall]·腹部分区[abdominal region]·左(右)上(下)腹[left(right) upper(lower)quadrant]·脐膨出[projection ofthe umbilicus]·腹式呼吸[abdominal(diaphragmatic)breathing]·腹壁松弛[lax abdominal wall]·肝肿大[hepatomegaly (enlargement of the liver)]·脾肿大[splenomegaly(enlargement of thespleen)]·右肋下5厘米[5cmbelowtheright costalmargin]·肿块(肝)质硬[firm mass(liver)]·莫菲氏征[murphy`ssigh]·肌卫现象[muscle guarding(tension)]·反跳痛[reboundtenderness]·压痛点[tenderness point]·剑突下压痛[tendernessbeneath the xiphoidprocess]·麦氏点压痛[McBurney`s point tenderness]·腹肌强直(板状腹,板样强直)[rigorofabdominal muscle(wooden belly, board—like rigidity)]·柔韧感[doughkneedingsensation]·波动感[fluctuation]·腹股沟疝[inguinalfemoralhernia]·腹壁反射[abdominalreflex]·腹水征[signof ascites]·膀胱肿大[bladder expansion]·膀胱区(脊肋角)压痛[tenderness of bladder region(costovertebral angle)]·肾(肝)区叩击病[percussion tenderness onkidney(liver) region]·移动性浊音[shiftingdullness]·鼓音[tympany(tampanitic resonance)]·肝(脾)浊音区[hepatic (splenic)dullness area]·肠鸣音正常(亢进、减弱、消失)[normal (hyperactive,diminished, absent) bowel sound]·气过水声[gurgling]·振水声[succusion(splashing)sound]2、常见症状·[Fever] 发热·[Pain]疼痛·[Edema] 水肿·[Mucocutaneoushemorrhage(bleeding)]皮肤粘膜出血·[Dyspnea(Difficulyin breathing;Respiratory difficulty;short of breath)] 呼吸困难·[Coughand expectoration(Sputum;Phlegm)]咳嗽和咯痰·[Hemoptysis] 咯血·[Cyanosis]紫绀·[Palpitation]心悸·[Chest discomfort] 胸闷·[Nausea(Retch;DryV omiting)and V omiting]恶心和呕吐·[Hematemesis(V omitingof blood)]呕血·[Hematochezia (Hemafecia)]便血·[Diarrhea] 腹泻·[Constipation (Obstipation)]便秘·[Vertigo (Giddiness;Dizziness)]眩晕·[Jaundice(Icterus)] 黄疸·[Convulsion]惊厥·[Disturbance of consciousness] 意识障碍·[Hematuria] 血尿·[Frequentmicturition,urgentmicturition and dysuria]尿频,尿急和尿痛·[Incontinenceof urine] 尿失禁·[Retention of urine]尿潴留(1)发热的表示方法·[Infective (Septic)fever] 感染性发热·[Non-infective(Aseptic)fever]非感染性发热·[Dehydration(Inanition)fever] 脱水热·[Drugfever]药物热·[Functional hypothermia]功能性低热·[Absorption fever]吸收热·[Centralfever] 中枢性发热·[Fever type] 热型▲[Continuous fever]稽留热▲[Remittentfever]驰张热▲[Intermittent fever]间歇热▲[Undulant fever] 波状热▲[Recurrentfever]回归热▲[Periodic fever]周期热▲[Irregularfever]不规则热▲[Ephemeralfever]短暂热▲[Doublepeaked fever]双峰热·[Feverof undetermined(unknown) origin,FUO]不明原因发热·[Rigor(shivering;chill;shakingchill;ague)] 寒战·[ChillySensation(Fell chilly;coldfits;coldness)]畏寒·[Ultra-hyperpyrexia]超高热·[Hyperthermia(A high fever;hyperpyrexia;ardentfever)]高热·[Moderate fever] 中度发热·[Hypothermia (Low—grade fever;slight fever;subfebrile temperature)] 低热·[Becomefeverish(Have a temperature)]发热·[Crisis]骤降·[Lysis]渐降·[Rheumatic fever]风湿热·[Cancerous fever] 癌性发热·[Fervescenceperiod]升热期·[Defervescence period]退热期·[Persistent febrile period] 持续发热期(2)疼痛的表示方法·[Backache(Backpain)] 背痛·[Lumbago] 腰痛·[Headache] 头痛▲[Vasomotor headache]血管舒缩性头痛▲[Migraine headache] 偏头痛·[Chest pain]胸痛·[Precardial pain] 心前区痛·[Retrosternal pain]胸骨后痛·[Abdominal pain(Stomachache)] 腹痛·[Acrodynia(pain in limbs)] 肢体痛·[Arthrodynia (Arthralgia)] 关节痛·[Dull pain]钝痛·[Sharp pain]锐痛·[Twingepain]刺痛·[Knife-likepain (Piercing pain)] 刀割(刺)样痛·[Achingpain]酸痛·[Burningpain] 烧灼痛·[Colicky (Griping;cramp)pain] 绞痛·[Colic] 绞痛·[Bursting pain]胀痛(撕裂痛)·[Hunger pain] 饥饿痛·[Ticpain] 抽搐痛·[Bearing—down pain]坠痛·[Shock—like pain] 电击样痛·[Jumping pain]反跳痛·[Tenderness pain] 触痛(压痛)·[Girdle—like pain]束带样痛·[Wandering pain]游走性痛·[Throbbing pain] 搏动性痛·[Radiating pain] 放射性痛·[Crampingpain] 痉挛性痛·[Boring pain]钻痛·[Intensepain]剧痛·[Dragging pain]牵引痛·[Labor pain]阵痛·[Cancerous pain]癌性疼痛·[Referred pain]牵涉痛·[Persistent pain(Unremittingpain)] 持续性痛·[Constantpain]经常性痛·[Intermittent pain]间歇性痛(3)水肿的表示方法·[Mucous edema (Myxedema)] 粘液性水肿·[Cardiac (Cardiogenic) edema]心源性水肿·[Nephrotic (renal)edema] 肾源性水肿·[Hepatic edema]肝源性水肿·[Alimentary (Nutritional)edema] 营养不良性水肿·[Angioneurotic edema] 血管神经性水肿·[Pitting] 凹陷性·[Nonpitting]非凹陷性·[Localized (Local) edema] 局限性水肿·[Generalized edema (Anasarca)]全身性水肿·[Hydrops]积水·[Cerebral(Brain)edema] 脑水肿·[Pulmonary edema(Hydropneumonia0] 肺水肿·[Hydrocephalus]脑积水·[Invisible (Recessive) edema]隐性水肿·[Frankedema]显性水肿·[Inflammatoryedema]炎性水肿·[Idiopathic edema] 特发性水肿·[Cyclical edema] 周期性水肿·[Ascites (Abdominal effusion;hydroperiotoneum)]腹水·[Pleural effusion(Hydrothorax)]胸水·[Pericardialeffusion(Hydropericardium)] 心包积液·[Bronchoedema] 支气管水肿·[Slight(Mild)]轻度·[Moderate] 中度·[Serious]重度·[Transudate] 漏出液·[Exudate] 渗出液(4)呼吸困难的表示方法·[Cardiacdyspnea] 心原性呼吸困难·[Inspiratory]吸气性·[Expiratory] 呼气性·[Mixed] 混合性·[Obstructive] 梗阻性·[Dyspnea at rest] 静息时呼吸困难·[Dyspneaon exertion] 活动时呼吸困难·[Dyspneaonlying down]躺下时呼吸困难·[Paroxysmal nocturnal dyspnea,PND]夜间阵发性呼吸困难·[Orthopnea] 端坐呼吸·[Asthma] 哮喘·[Cardiac asthma] 心源性哮喘·[Bronchial asthma]支气管性哮喘·[Hyperpnea]呼吸深快·[Periodicbreathing]周期性呼吸·[Tachypnea(Rapid orfast breathing;accelerated breathing;short ofbreath)]气促·[Bradypnea(Slowbreathing)] 呼吸缓慢·[Irregularbreathing] 不规则呼吸(5)皮肤粘膜出血的表示方法·[Bleeding spots intheskin]皮肤出血点·[Petechia] 瘀点·[Eccymosis]瘀斑·[Purpura] 紫癜·[Splinter hemorrhage] 片状出血·[Oozing of the blood (Errhysis)] 渗血·[Hemorrhinia (Nasalbleeding)]鼻衄·[Ecchymoma] 皮下血肿(6)咳嗽与咯痰的表示方法·[Drycough (Nonproductive cough;hacking cough)] 干咳·[Sharp cough] 剧咳·[Wetcough(Moistcough)] 湿咳·[Productive cough (Loose cough)] 排痰性咳·[Chronic cough] 慢性咳嗽·[Irritable cough] 刺激性咳嗽·[Paroxysmalcough] 发作性(阵发性)咳嗽·[Cough continually] 持续性咳嗽·[Spasmodic cough]痉挛性咳嗽·[Whooping cough]百日咳·[Wheezingcough]喘咳·[Short cough] 短咳·[Distressed cough]难咳·[Droplet]飞沫·[Frothy sputum] 泡沫样痰·[Bloodysputum]血痰·[Mucous(Mucoid) sputum] 粘液样痰·[Purulent sputum]脓痰·[Mucopurulentsputum]粘液脓性痰·[White (Yellow,green)sputum]白(黄,绿)痰·[Fetid(Foul) sputum] 恶臭痰·[Iron—rust (Rusty)sputum]铁锈色痰·[Chocolatecoloured sputum]巧克力色痰·[Thick sputum]浓痰·[Thinsputum]淡痰·[Viscous sputum] 粘痰·[Transparent sputum]透明痰·[Much (Largeamounts of)sputum]大量痰·[Moderate amounts of sputum]中等量痰·[Not much (Small amounts of) sputum]少量痰(7)内脏出血的表示方法·[Massivehematemesis]大量呕血·[Epistasis (Nosebleed;Nasal bleeding;Hemorrhinia;rhinorrhagia)]鼻衄·[Hematuria]血尿·[Initial hematuria] 初血尿·[Idiopathic hematuria] 特发性血尿·[Painless hematuria]无痛性血尿·[Terminal hematuria]终末性血尿·[Gross (Macroscopic) hematuria] 肉眼血尿·[Microscopic hematuria]镜下血尿·[Hematuria in the whole processofurination] 全程血尿·[Gingivalbleeding (Ulaemorrhagia;gum bleeding)]牙龈出血·[Hematochezia]便血·[Bloodystool] 血便·[Black stool(Melena)]黑便·[Tarry stool] 柏油样便·[Occult blood,OB] 隐血·[Hemathorax]血胸··[Hematocoelia]腹腔积血·[Hematoma]血肿·[Hemopericardium] 心包积血·[Cerebral hemorrhage]脑出血·[Subarachnoid hemorrhage(SAH)] 蛛网膜下腔出血·[Excessive(Heavy) menstrual flowwith passage ofclots]月经量多伴血块·[Mild (Moderate)menses] 月经量少(中等)(8)紫绀的表示方法·[Congenital cyanosis]先天性紫绀·[Enterogenous]肠源性·[Central]中枢性·[Peripheral]周围性·[Mixed]混合性·[Acrocyanosis] 指端紫绀(9)恶心与呕吐的表示方法·[Vomiturition(Retching)]干呕·[Feel nauseated] 恶心感·[Postprandialnausea] 饭后恶心·[Hiccup] 呃逆·[Sour regurgitation]返酸·[undigested food V omiting]吐不消化食物·[BiliousVomiting] 吐胆汁(10)腹泻与便秘的表示方法·[Moning diarrhea]晨泻·[Watery (Liquid)diarrhea] 水泻·[Mucous diarrhea] 粘液泻·[Fatty diarrhea]脂肪泻·[Chronic (Acute)] 慢性(急性)·[Milddiarrhea] 轻度腹泻·[Intractable(Uncontrolled)diarrhea]难治性腹泻·[Protracted diarrhea] 迁延性腹泻·[Bloody stool]血梗·[Frothy stool] 泡沫样便·[Formless(Formed)stool] 不成形(成形)便·[Loose (Hard)stool]稀(硬)便·[Rice—water stool]米泔样便·[Undigested stool]不消化便·[Dysenteric diarrhea] 痢疾样腹泻·[Inflammatorydiarrhea] 炎症性腹泻·[Osmotic] 渗透性·[Secretory]分泌性·[Malabsorption] 吸收不良性·[Lienteric]消化不良性·[Pancreatic diarrhea]胰性腹泻·[Tenesmus]里急后重·[Pass a stool (Have apassage;open orrelax the bowel)] 解大便·[Have a call ofnature] 便意·[Fecal incontinence(Copracrasia)] 大便失禁·[Functional constipation] 功能性便秘·[Organic constipation] 器质性便秘·[Habitualconstipation] 习惯性便秘·[Have atendency to be constipated] 便秘倾向(11)黄疸的表示方法·[Latent (occult)jaundice] 隐性黄疸·[Clinicalejaundic] 显性黄疸·[Nuclear icterus]核黄疸·[Physiologic icterus] 生理性黄疸·[Icterus simplex]传染性黄疸·[Toxemicicterus]中毒性黄疸·[Hemolytic ejaundic ] 溶血性黄疸·[Hepatocellular]肝细胞性·[Obstructive]阻塞性·[Congenital]先天性·[Familial] 家族性·[Cholestatic]胆汁淤积性·[Hematogenous]血源性·[Malignant] 恶性·[Painless]无痛性(12)意识障碍的表示方法·[Somnolence]嗜睡·[Confusion] 意识模糊·[Stupor]昏睡·[Coma]昏迷·[Delirium] 谵妄·[Syncope (swoon;faint)]晕厥·[Drowsiness] 倦睡(13)排尿的表示方法·[Anuria]无尿·[Nocturia] 夜尿·[Oliguria]少尿·[Polyuria]多尿·[Pass water (Make water; urinate; micturition)]排尿·[Frequentmicturition(Frequency of micturition;fruquent urinatio n;Pollakiuria)]尿频·[Urgent micturition (Urgencyof urinationor micturition)]尿急·[Urodynia (Pain on micturition; painful micturition; alginuresis;micturition pain)]尿痛·[Dysuria(Difficulty in micturition;disturbance of micturition)]排尿困难3.少见症状·[Weekness(Debility; asthenia;debilitating)]虚弱(无力)·[Fatigue (Tire;lassitude)] 疲乏·[Wasting(thin;underweight; emaciation; lean)] 消瘦·[Night sweating] 盗汗·[Sweat (Perspiration)]出汗·[Cold sweat] 冷汗·[Pruritus (Iching)]搔痒·[Asthma] 气喘·[Squeezing (Tightness;choking;pressing)sensationof the chest] 胸部紧缩(压榨)感·[Intermittent claudication]间歇性跛行·[Difficulty in swallowing(Dysphagia;difficultswallowing;acataposis)]吞咽困难·[Epigastric (Upper abdominal)discomfort]上腹部不适·[Anorexia(Sitophobia)] 厌食·[Poor appetite (Loss of appetite)]纳差·[Heart—burn(Pyrosis)]胃灼热·[Stomachache(Painin stomach)] 胃部痛·[Periumbilial pain] 脐周痛·[Belching (Eructation)]嗳气·[Sour regurgitation] 返酸·[Abdominaldistention(bloating)]腹胀·[Pass gas(Breakwink)] 肛门排气·[Small(Large)stool]大便少(多)·[Painover the liver]肝区痛·[Lumbago]腰痛·[Pica(Parorexia;allotriophagy)]异食癖·[Menoxenia (Irregular menstruation)]月经不调·[Jointpain(Arthralgia; arthrodynia)]关节痛·[Polydipsia (Excessive thirst)] 多饮(烦渴)·[Polyphagia(Excessive appetite; hyperorexia;bulimia)] 多食·[Cold(Heat) intolerance]怕冷(热)·[Dwarfism(Excessiveheight)]身材矮小(高大)·[Excessive sweating] 多汗·[Handstremble] 手抖·[Obesity(Fatty)]肥胖·[Agitation(Anxiety;nervous irritability)]焦虑(忧虑)·[Formication]蚁走感·[Tingling]麻刺感·[Hyperpathia]痛觉过敏·[Hypalgesia] 痛觉减退·[Insomnia(Poor sleepness;sleeplessness)]失眠·[Numbness]麻木·[Limitation of motion]活动受限·[Tetany]手足抽搐·[Dischargeofpus]流脓·[Blurred vision(Hazyvision;blurring ofvision; dimnessof vision)]视物模糊·[Burning (Dry) sensation] 烧灼(干燥)感·[Tearing (Dacryorrhea;Lacrimation)]流泪·[Doublevision (Diplopia)]复视·[Strabismus]斜视·[Hemianopia] 偏盲·[Foreign bodysensation]异物感·[Lose the sight(Loseof vision)]失明·[Diminution ofvision]视力减退·[Photophobia] 畏光·[Tinnitus]耳鸣·[Nasal obstruction(blockage)]鼻塞·[Dryness of thenose] 鼻干燥·[Rhinorrhea(Snivel;Nasal discharge)] 流鼻涕·[Sneezing]打喷嚏·[Snoring]打鼾·[Hyposmia(Reduction of thesenseof smell)] 嗅觉减退·[Anosmia (Completeloss of sense of smell)]嗅觉丧失·[Dysphonia]发音困难·[Hoarseness]声嘶·[Pain on swallowing]吞咽痛·[Saliva dribblies from the mouth]流涎·[Troaty voice]声音沙哑·[Stridor]喘鸣·[Redand swollen]红肿·[Apathy]情感淡漠医学专业英语·[Delusion]妄想11 / 11。
体操是一项古老而又优美的运动项目,它融合了力量、柔韧性、平衡和协调性。
体操运动员在比赛中所展现出来的各种动作和姿势都需要精湛的技巧和高超的身体控制能力。
而"hollow body position"(空心身体位置)就是体操运动中常用的一个术语,它在体操训练中具有非常重要的作用。
5.1 hollow body position的定义"hollow body position"是体操运动中常用的一个姿势,它要求身体平躺在地面上,同时腿部和上半身都要离开地面,形成一个弓形的弯曲,使得身体中间部分形成一个凹陷。
头部和肩部保持离地并保持稳定。
整个身体处于紧绷状态,腹部肌肉始终紧绷,臀部和腰部也要保持收紧,腿部和脚部要保持伸直。
在训练中,运动员需要将"hollow body position"保持一段时间,这样可以锻炼核心力量和腹部肌肉,并且提高身体的协调性和稳定性。
这个姿势也是许多体操动作的基础,只有掌握了"hollow body position",运动员才能更好地完成其他复杂的技术动作。
5.2 hollow body position的训练方法要想掌握"hollow body position",运动员需要进行一定的训练。
以下是一些常见的训练方法:1. 起始练习:初学者可以先从仰卧姿势开始,将双腿抬起,然后利用腹部力量将腰部离开地面,使得身体呈现一个略微弯曲的姿势。
同时保持双手伸直向上,头部和肩部离地。
2. 强化训练:随着对"hollow body position"的掌握程度提高,运动员可以逐渐加大训练难度。
可以利用哑铃、弹力带或者其他辅助器械来增加训练的挑战度,比如在双手持哑铃的情况下进行"hollow body position"练习,或者利用弹力带增加身体的平衡难度等。
分解动作作文英文回答:Introduction:Decomposing movement into its constituent parts involves analyzing the individual elements that contribute to the overall motion. By breaking down complex movements into smaller, more manageable units, it becomes possible to understand the underlying mechanics and neuromuscular control involved.Elements of Movement:The primary elements of movement include:Body position: The arrangement of the body's segments relative to each other.Center of mass: The point at which the body's mass isconcentrated.Range of motion: The extent to which a joint can move in various directions.Force: The application of effort against an object or surface.Velocity: The rate at which the body or body segments are moving.Acceleration: The rate at which the body's velocity is changing.Biomechanical Analysis:Biomechanical analysis is used to evaluate the mechanics of movement by examining factors such as:Joint angles: The angles at which the joints move during a specific motion.Muscle activity: The muscles involved in generating and controlling the movement.Ground reaction forces: The forces exerted by the body against the ground during movement.Kinematic Analysis:Kinematic analysis focuses on describing the movement of the body without considering the forces involved. It typically involves measuring:Displacement: The change in the position of the body or body segments.Velocity: The rate at which the body or body segments are moving.Acceleration: The rate at which the body's velocity is changing.Neuromuscular Control:Neuromuscular control refers to the role of the nervous system in regulating movement. The nervous system sends signals to muscles to initiate and coordinate movements. Factors involved in neuromuscular control include:Motor planning: The development of a plan for the desired movement.Motor commands: The signals sent from the brain to the muscles.Sensory feedback: Information received from the body's sensory receptors about the current state of the body andits environment.Conclusion:Decomposing movement into its constituent parts allows for a comprehensive understanding of the complex interplay between biomechanical, kinematic, and neuromuscular factors. By analyzing these individual elements, it becomes possibleto identify potential areas for improvement, optimize performance, and prevent or rehabilitate injuries.中文回答:导言:分解动作包括分析组成整体运动的各个元素。
American Journal of Gastroenterology ISSN0002-9270 C 2006by Am.Coll.of Gastroenterology doi:10.1111/j.1572-0241.2006.00827.x Published by Blackwell PublishingInfluence of Body Position and Stool Characteristicson Defecation in HumansSatish S.C.Rao,M.D.,Ph.D.,F.R.C.P.,Renae Kavlock,M.D.,and Sheila Rao,R.N.Division of Gastroenterology/Hepatology,Department of Internal Medicine,University of IowaCarver College of Medicine,Iowa City,IowaBACKGROUND:Whether defecation is influenced by body position or stool characteristics is unclear.AIM:We investigated effects of body position,presence of stool-like sensation,and stool form on defecation patterns and manometric profiles.METHODS:Rectal and anal pressures were assessed in25healthy volunteers during attempted defecation either in the lying or sitting positions and with balloon-filled or empty rectum.Subjects also expelleda water-filled(50cc)balloon or silicone-stool(FECOM)either lying or sitting and rated their stoolingsensation.RESULTS:When attempting to defecate in the lying position,a dyssynergic pattern was seen in36%of subjects with empty rectum and24%with distended rectum.When sitting,20%showed dyssynergiawith empty rectum and8%with distended rectum.More subjects(p<0.05)showed dyssynergia inlying position.When lying,60%could not expel balloon and44%FECOM.When sitting,fewer(p<0.05)failed to expel balloon(16%)or FECOM(4%).FECOM expulsion time was quicker(p<0.02).Stool-like sensation was more commonly(p<0.005)evoked by FECOM than balloon.CONCLUSIONS:In the lying position,one-third showed dyssynergia and one-half could not expel artificial stool.Whereas when sitting with distended rectum,most showed normal defecation pattern and ability toexpel stool.Thus,body position,sensation of stooling and stool characteristics may each influencedefecation.Defecation is best evaluated in the sitting position with artificial stool.(Am J Gastroenterol2006;101:2790–2796)INTRODUCTIONSymptoms such as excessive straining,hard stools,feeling of incomplete evacuation,and the use of manual maneuvers to assist defecation are reported by approximately20%of the population(1,2).These symptoms of difficult defecation are now recognized as important features of chronic con-stipation(1–5).However,symptoms alone do not provide sufficient discriminant value to either support a diagnosis of constipation or to provide pathophysiological information (3,6).Hence,physiological testing has been advocated to aid diagnosis and provide mechanistic insights(3,6).Tests of anorectal function,such as anorectal manometry or simu-lated defecation studies,reveal that many patients with consti-pation exhibit dyssynergic or obstructive defecation(6–10). However,in many centers,it is common practice to instruct patients to attempt defecation or undergo biofeedback train-ing for constipation in the lying position(11,13),but the act of defecation is usually accomplished in the sitting or squatting position.Moreover,when attempting to defecate in the left lateral position,it has been reported that some normal subjects may show an obstructive or incoordinated (dyssynergic)pattern of defecation(12,14).It has also been argued that this pattern may be a laboratory artifact(15). But,whether the body position is partly responsible for the dyssynergia observed in normal subjects and in patients with difficult defecation is not known.In addition to the evaluation of symptoms and rectal ex-amination,a test of simulated defecation(6,7,16–18)can be useful in the routine assessment of patients with defeca-tion disorders,as has been endorsed recently by the Amer-ican and European Societies of Neurogastroenterology and Motility(19).But,there is no uniform methodology of per-forming this test(7,12,15,17,18).In a survey of seven centers,only three routinely performed a test of simulated defecation and two of these centers asked patients to attempt defecation in the left lateral position(11).In a systematic re-view,several techniques of performing the balloon expulsion test were identified and the positive yield of balloon expul-sion test varied from23to67%,largely because of the testing conditions(7).Thus,an ideal method for performing the sim-ulated defection test remains to be defined,and whether the testing conditions influence the outcome of this test is not known.2790Body Position,Stool Form,and Defecation2791We tested the following hypotheses:(i)The left lateral posi-tion,although convenient for physiologic testing,is unnatural for defecation and results in higher frequency of abnormal findings such as dyssynergia when compared with the sitting position,even in normal subjects;and(ii)the FECOM is more stool-like and more likely to be expelled than a water-filled balloon.The aims of our study were twofold:(a)To examine the manometric pressure profiles of the anal sphincter and the rectum in healthy subjects during attempted defecation,both in the left lateral position and in the sitting position,and either with an empty rectum or after balloon distention of the rectum;and(b)To determine the subject’s ability to expel a water-filled balloon or a silicone-filled device(FECOM)in the lying and sitting positions.METHODSSubjectsT wenty-five healthy volunteers,m/f=10/15,mean age (range)=50yr(33–71),were recruited through a hospi-tal advertisement.All subjects were free of gastrointestinal symptoms and were not taking any medications except oral contraceptives.None of them had any previous abdominal or anorectal surgery or significant obstetric injury,such as third or fourth degree perineal tear.All of them reported a normal bowel habit and denied any symptoms of difficult defecation or rectal bleeding on a symptom questionnaire that inquired about stool frequency,straining effort,feeling of incomplete evacuation,use of digital maneuvers,painful defecation,hard stools,abdominal pain,and reflux symptoms.All subjects gave written informed consent and the study protocol was ap-proved by the Human Subjects Investigation review board. Study ProtocolIn order to test our objectives,each subject was asked to attempt defecation under four separate experimental condi-tions.Experiment1:Here,with the subject lying on a bed and in the left lateral position,a six-sensor solid-state manometry probe(Gaeltec,Isle of Skye,UK)with a4cm long balloon was placed in the rectum and taped to the perineum with a Tegaderm(3M,St.Paul,Minnesota).When correctly posi-tioned,the pressure sensors were located at1cm,1.5cm,2 cm,3cm,9cm(inside balloon),and14cm from the anal verge (14).The probe was connected to an amplifier/records(Gael-tec,T-MPR,Isle of Skye,UK).After a15-min rest period,the subject was asked to attempt defecation on two separate occa-sions,with a2-min rest period between each maneuver.Next, the subject was asked to sit on a commode and once again attempt defecation twice with a2-min rest period between each maneuver.Experiment2:With the subject lying on a bed in the left lateral position and with the manometry probe in situ(as described above),the balloon located in the rectum was dis-tended with volumes of50–100cc of air until the subject reported a desire to defecate.Subsequently,the subject was asked to attempt defecation on two separate occasions with a2-min rest between the maneuvers.Next,the balloon was deflated.After a15-min rest,the subject was asked to sit on a commode.Again,the rectal balloon was distended with50–100cc of air,as described above,and the subject was asked to attempt defecation twice.If the subject expelled the probe, the maneuver was not repeated.Thereafter,the probe was removed.Experiment3:After a30-min rest,with the subject lying on a bed,a5cm long latex balloon tied to a2mm plastic tube was placed in the rectum8cm from the anal verge.The balloon was distended with50cc water at37◦C.The subject was asked to expel this water-filled balloon in privacy lying on the bed,and the time taken to expel the balloon was noted by using a stop clock.The attendant returned after5min,and if the subject had failed to expel the balloon,it was removed. If expelled,the balloon was deflated and repositioned in the rectum.Next,the subject was asked to sit on a commode. The balloon was once again inflated with50cc water and the subject was asked to expel the balloon in privacy and the time taken was noted.Experiment4:After a15-min rest,a cylindrical,9cm long,silicone-filled(35cc)deformable device,FECOM,was placed in the rectum(20).Next,as described in Experiment 3,the subject was asked to expel the device,first when lying on the bed and next in the sitting position on a commode. Privacy was provided and the time taken to expel the device in each position was noted.Also,after placement of each stool-like device,the sub-jects were asked to describe their anorectal sensation for the following four symptoms on a visual100mm analog scale (rating of0–10):anorectal discomfort,did the device evoke a sensation of stooling,did the device evoke a desire to defe-cate,and did the device evoke urgency to defecate.Also,we inquired which of the two devices(device1or2)evoked a stool-like sensation when compared with their usual sensa-tion of stooling,and if used for testing their defecation,which device they would prefer.First,we performed experiments1or2in a random order. Next,we performed experiments3or4in a random order. In the latter two experiments,the subjects were blinded to the placement of either a50cc water-filled balloon or a FE-COM.Data AnalysisDuring each experiment,of the two attempts to defecate,the maneuver that most closely resembled a normal pattern of defecation(6,14)was used for performing the data analyses. For experiments1and2and during each attempt to defe-cate,we measured the maximum intrarectal pressure and at the same time,the minimum anal residual pressure and from these data a defecation index was calculated using previ-ously described criteria(6,14).The defecation index was defined as the ratio between the maximum intrarectal pres-sure and the minimum anal residual pressure(6,14).Also,we2792Rao et al.observed the pattern of defecation and classified it as normal or dyssynergic,as described previously(6).The percentage anal relaxation=100×(resting sphincter pressure–residual anal sphincter pressure)/resting sphincter pressure(14,19). For experiments3and4,we assessed the subject’s ability to expel the artificial stool(balloon or FECOM),either on the bed or on the commode,and the time taken for expulsion. StatisticsThe rectal and anal pressure changes during attempted defe-cation in the lying position or in the sitting position and with either an empty rectum or after distension of the rectum with a balloon were compared using the paired Student’s t-test.The proportion of subjects who exhibited a normal or dyssynergic pattern was compared using theχ2test.The number of sub-jects who could or could not expel a water-filled balloon or FECOM and the visual analog scores for a subject’s sensation of stooling were compared using the2-tailed Fisher’s exact test.The preference for each stool-like device was compared using an exact2-tailed test to answer the question whether the binomial proportion of the more frequent preference dif-fers from the null hypothesis that the proportions are equal. The proportions are expressed as percentages.Finally,we performed repeated generalized estimating equation(GEE) logistic regression analysis of the dependent variable,whether expulsion of balloon or FECOM occurred in a person who ex-hibited dyssynergia.In these analyses,the dyssynergia vari-able was defined as“dyssynergia present”if it was observed with any of the four conditions:empty rectal balloon sit-ting position,empty rectal balloon lying position,inflated rectal balloon sitting position,and inflated rectal balloon ly-ing position.Dyssynergia“presence”or“absence”was the only predictor variable in the GEE model.We specified an exchangeable structure for the working correlation matrix among repeated observations within subjects. RESULTSInfluence of Body Position on Manometric Pattern During DefecationWhen attempting to defecate with an empty rectum,9/25 (36%)subjects showed a dyssynergic pattern in the lying po-sition and5/25(20%)subjects in the sitting position.This dif-ference was significant(p<0.05).The dyssynergic pattern mostly consisted of an adequate pushing effort as demon-strated by a rise in the intrarectal pressure along with a para-doxical contraction or increase in anal sphincter pressure (Fig.1).When defecation was attempted after distending a balloon in the rectum,6/25(24%)subjects showed a dyssyn-ergic pattern in the lying position and2/25(8%)subjects in the sitting position,and this difference was not significant. Rectal and Anal Pressure Changes During Attempted Defecationa).When attempting to defecate with an empty rectum,theintrarectal pressure was higher(p<0.02)and theanal Figure1.Thisfigure shows the manometric pressure changes in the rectum and the anal canal during attempted defecation,in a sin-gle subject with an empty rectum.(A)This shows the occurrence of a dyssynergic pattern of defecation in the lying position with a paradoxical increase in anal sphincter pressure and a rise in the in-trarectal pressure.(B)When sitting on a commode,the same subject shows a more normal pattern of defecation comprising of a rise in intrarectal pressure synchronized with anal sphincter relaxation.residual pressure was lower(p<0.05)in the sitting po-sition on the commode when compared with the pres-sures in the lying position on the bed(Fig.2).Also, the defecation index was higher in the sitting position, mean(95%CI),sitting versus lying,1.8(0.3)versus1.43(0.2),p=0.05.The anal resting pressure was higher(p<0.02)in the sitting position when compared with the ly-ing down position and likewise the anal residual pressureBody Position,Stool Form,and Defecation 279320406080100120140160180P r e s s u r e (m m H g )Figure 2.The individual values for the intrarectal pressure and the anal residual sphincter pressure during attempted defecation in the lying and sitting positions,with an empty rectum.was also higher (p <0.05).However,the percentage anal relaxation was similar in both positions (lying vs sitting =35±11%vs 36±18%).b).After distension of the balloon in the rectum,the analresting pressure was higher in the sitting position when compared with the lying position (Fig.3),but the percent-age anal relaxation was similar in both positions (lying vs sitting,32±10vs 37±12%,p =N.S.).20406080100120140160180P r e s s u r e (m m H g )Figure 3.The individual values for the changes in the anal resting sphincter pressure and the anal residual sphincter pressure during attempted defecation in the lying and in the sitting positions,after balloon distension of the rectum.In fluence of Stool F orm and Stool Consistency on DefecationIn the lying position,15/25(60%)subjects could not expel a 50cc water-filled balloon,whereas in the sitting position,4/25(16%)subjects failed to expel the balloon (p <0.005).In the lying position,11/25(44%)subjects could not expel the FECOM,whereas in the sitting position,1/25(4%)subjects failed to expel the FECOM (p <0.005).In the sitting position,2794Rao et al.Table1.Expulsion Time,Preference(Stool-Like),and Subjective Responses on a Visual Analog Scale(0–10cm)for Each Artificial Stool Device in the Sitting PositionFECOM50cc Balloon(N=25)(N=25)p Value Expulsion time(s)48±3775±45p<0.02 Preferred stool device∗(%)19(76%)5(20%)p=0.006 Discomfort(0–10) 2.7±0.8 2.6±0.7N.S. Evoked sensation of7±1.2 5.6±1.3p<0.05 stooling(0–10)Desire to defecate(0–10)7.2±1.4 5.9±1.4p=0.05 Urgency(0–10) 4.6±1.3 3.9±1.2N.S.∗One person had no preference.Mean±95%CI,V AS scores:1=no and10=yes.the FECOM was expelled more quickly(p<0.02)than a50 cc water-filled balloon(mean[CI]48[37]vs75[45]s,p< 0.02)(Table1).The presence or absence of dyssynergia,irrespective of position,did not have a statistically significant effect on the probability of expulsion failure(p=0.0599).The predicted probability of expulsion failure(censoring)in the presence of dyssynergia was0.375(95%CI0.23–0.54)and in the absence of dyssynergia was0.196(95%CI0.09–0.35). Subjective Assessment of Stool-Like DeviceAmong the25subjects,19(76%)felt that the presence of FECOM in their rectum more closely mimicked their usual sensation for a desire to defecate.In contrast,5(20%)subjects felt that the balloon was more stool-like,and one subject had no preference(Table1).The FECOM was preferred by more (p=0.006)subjects than the balloon.When asked to score their desire to defecate with each stool-like device on a visual analog scale,the subjects rated the FECOM as more(p< 0.05)likely to evoke a desire to defecate. DISCUSSIONOur study showed that36%of normal healthy subjects ex-hibited a dyssynergic pattern when attempting to defecate with an empty rectum in the left lateral position.In contrast, 20%of subjects exhibited a similar pattern in the sitting po-sition.Thus,body position appeared to influence the pattern of defecation within a laboratory setting.When the experi-ments were repeated after the subjects were provided with a sensation of stooling through rectal balloon distension,24% of subjects showed a dyssynergic pattern in the lying position and8%in the sitting position.Thus,not only the body posi-tion but also a stool-like sensation influenced the pattern of defecation.The sitting position appears to be more conducive for defecation than the lying position.The manometric recordings during attempted defecation showed that the intrarectal pressure was lower in the left lat-eral position than in the sitting position.The anal resting and residual pressures were also lower in the left lateral position but higher in the sitting position,in part due to positional ef-fects on sphincter tone and the additional effect of the weight of intraabdominal viscera and that of the upper half of the body.Thesefindings confirm our hypothesis by demonstrat-ing that the dynamics for rectoanal coordination are less effi-cient in the lying position,and more subjects exhibit dyssyn-ergia in the lying position.Thus,our results indicate that both the body position and the sensation of stooling can in-fluence the pattern of defecation and the pressure changes in the anorectum.The aforementionedfindings were further corroborated by experiments with an artificial stool.In the left lateral posi-tion,60%of subjects could not expel a50cc water-filled balloon and40%of subjects could not expel a silicone-filled deformable device,FECOM.In contrast,only4(10%)sub-jects could not expel the balloon and only one subject the FECOM in the sitting position.Thus,the higher incidence of dyssynergia and the inability to expel“stool-like”devices in the left lateral position even in healthy controls,underscores the need to exercise caution when interpreting manometric tests that are usually performed in the left lateral position. Ourfindings contrast with those of Barnes et al.(21)who reported that all but one of their control subjects were able to expel balloons in the left lateral position.This discrepancy may in part be due to subject selection,as in the previous study,the subjects were not healthy normal controls,but pa-tients who had gastrointestinal evaluation for colon polyps, Crohn’s disease,or anal warts;also their age and gender dis-tribution was not stated.Although it is difficult to simulate normal stooling in the laboratory environment,if at all pos-sible,one should strive to test the ability to defecate more optimally in the laboratory.From our studies,it appears that ideally,a subject should be tested for attempted defecation in the sitting position,on a commode,and preferably after evoking a sensation of stooling.In addition,we found that76%of our subjects preferred a silicone-filled artificial stool,FECOM,to a water-filled bal-loon,suggesting that the form and consistency of a stool-like device may also influence defecation.The FECOM was also more likely to evoke a subject’s usual sensation of stooling than the balloon,confirming previous observations(20,22). These results suggest that the characteristics of stool,in par-ticular the sensation it evokes and its consistency,may also influence defecation,supporting our hypothesis.Also,ourfindings of a dyssynergic pattern of defecation in healthy controls further supports the notion that a sin-glefinding,such as an abnormal manometric pattern dur-ing attempted defecation,by itself,is insufficient to diagnose dyssynergia,as it has low specificity(6,7).Additional tests may be required,such as prolonged balloon expulsion time, or prolonged retention of markers on a colonic transit study, or prolonged difficulty with evacuating barium paste during defecography.These studies can provide corroborative evi-dence for anorectal dysfunction(6,7,17,18,23).The limitations of our study included our inability to mea-sure the axial expulsion forces during attempted defecation and the individual contributions of the abdominal muscles, pelvicfloor movement,and rectal forces(24).This informa-tion may have provided some additional understanding of the overall defecation dynamics.Also,whether the laboratoryBody Position,Stool Form,and Defecation2795conditions influenced the subject’s performance during one or more attempts to defecate cannot be excluded.Finally,the presence or absence of dyssynergia did not have a significant effect on the ability to predict a failure of expulsion of either FECOM or balloon.This may in part be due to the use of healthy controls and/or a type II error.In conclusion,our study shows that the body position,the sensation of stooling,and the consistency of stool may each influence the ability to defecate in healthy subjects.It is there-fore conceivable that these factors could play a significant role in the pathogenesis of symptoms in patients with diffi-cult defecation.All of these factors must be considered when evaluating patients with difficult defecation and in particular when interpreting the physiological tests of anorectal func-tion.Based on our observations,we recommend that a test of simulated defecation is best performed in the sitting position, and with an artificial stool,such as the FECOM,in order to minimize false positive results. ACKNOWLEDGMENTSThis research was supported in part by grant R01DK57100-03,National Institute of Health,and portions of this work were presented at Digestive Disease Week and published as an abstract:Gastroenterology1996;110:A741.The authors wish to thank Mrs.Heidi Vekemans for her excellent secretarial assistance and CK Brown for his assistance and advice with statistical and data analysis.Dr.S.Rao holds a joint patent with Inamed Corporation for the FECOM device. STUDY HIGHLIGHTSWhat Is Current Knowledger Symptoms of constipation are poor predictors of un-derlying pathophysiology hence,physiological testingis recommended.r The left lateral position,although convenient for phys-iologic testing is unnatural and may lead to higher in-cidence of dyssynergia but the effects of body positionand stool consistency on anorectal function are poorlyunderstood.We assessed defecation dynamics undervarious controlled conditions.What Is New Herer A higher proportion of healthy subjects demonstrateda dyssynergic pattern of defecation with a low defeca-tion index,and had difficulty with expelling simulatedstools in the lying position when compared to the sittingposition.r A silicone-filled stool-like device was more likely toevoke a sensation of stooling and was more easily ex-pelled than a water-filled balloon.r Defecation dynamics are best assessed in the sitting po-sition and after evoking a stool-like sensation in rectum.Reprint requests and correspondence:Satish S.C.Rao,M.D., Ph.D.,F.R.C.P.,Department of Internal Medicine,Division of Gas-troenterology/Hepatology,4612JCP,200Hawkins Drive,Iowa City, IA52242-1009.Received February17,2006;accepted June10,2006. REFERENCES1.Pare P,Ferrazzi S,Thompson WG,et al.A longitudinalsurvey of self-reported bowel habits in the United States.Dig Dis Sci1989;34:1153–62.2.Walter F,Stewart WF,Liberman J,et al.Epidemiology ofconstipation(EPOC)study in the United States:Relation of clinical subtypes to sociodemographic features.Am J Gastroenterol1999;94:3530–40.3.Grotz RL,Pemberton JH,Talley NJ,et al.Discriminantvalue of psychological distress,symptom profiles,and seg-mental colonic dysfunction in outpatients with severe idio-pathic constipation.Gut1994;35:798–802.4.Rao S,Tuteja AK,Vellema T,et al.Dyssynergic defecation:Demographics,symptoms,stool patterns,and quality of life.J Clin Gastroenterol2004;38:1–6.5.Thompson WG,Longstreth GF,Drossman DA,et al.Func-tional bowel disorders and functional abdominal pain.Gut 1999;45:1143–7.6.Rao SSC,Mudipalli RS,Stessman M,et al.Investigation ofthe utility of colorectal function tests and Rome II criteria in dyssynergic defecation(Anismus).Neurogastroenterol Motil2004;16:589–96.7.Rao SSC,Ozturk R,Laine L.Clinical utility of diagnostictests for constipation in adults:A systematic review.Am J Gastroenterol2005;100:1605–15.8.Mertz H,Naliboff B,Mayer E.Physiology of refractorychronic constipation.Am J Gastroenterol1983;85:306–12.9.Surrenti E,Rath DM,Pemberton JH,et al.Audit of consti-pation in a tertiary referral gastroenterology practice.Am J Gastroenterol1995;90:1471–5.10.Diamant ND,Kamm MA,Wald A,et al.AGA technicalreview on anorectal testing techniques.Gastroenterology 1999;116:736–60.11.Rao SSC,Diamant N,Enck P,et al.Current methods ofperforming anorectal manometry(ARM):An inter-center comparison.Gastroenterology1999;116:G4633.12.Bannister JJ,Timms JM,Barfield LJ,et al.Physiologicalstudies in young women with chronic constipation.Int J Colorect Dis1986;1:175–82.13.Siproudhis L,Dautreme S,Ropert A,et al.Anismus andbiofeedback;who benefits?Eur J Gastroenterol Hepatol 1995;7:547–52.14.Rao SSC,Hatfield R,Soffer E,et al.Manometric test ofanorectal function in healthy adults.Am J Gastroenterol 1999;94:773–83.15.Duthie GS,Barolo DCC.Anismus:The cause of constipa-tion?Results of investigation and treatment.World J Surg 1992;16:831–5.16.Rao SSC.Constipation.Gastroenterol Clin North Am2003;32:659–83.17.Whitehead WE,Wald A,Diamant NE,et al.Functionaldisorders of the anus and rectum.Gut1999;45:55–9. 18.Minguiz M,Herreros B,Sanchiz V,et al.Predictive valueof the balloon expulsion test for excluding the diagnosis of pelvicfloor dyssynergia in constipation.Gastroenterology 2004;126:57–62.19.Rao SSC,Azpiroz F,Diamant N,et al.Minimum stan-dards of anorectal manometry.Neurogastroenterol Motil 2002;14:553–9.2796Rao et al.20.Pelsang RE,Rao SSC,Welcher K.FECOM:A new arti-ficial stool for assessing defecation.Am J Gastroenterol 1999;94:183–6.21.Barnes PRH,Lennard-Jones JE.Balloon expulsion from therectum in constipation of different types.Gut1985;26:1049–52.22.Bannister JJ,Davis P,Timms JM.Effect of stool size andconsistency on defecation.Gut1987;28:1246–50.23.Chiaroni G,Salandini L,Whitehead WE.Biofeedback ben-efits only patients with outlet dysfunction,not patients with isolated slow transit constipation.Gastroenterology 2005;129:86–97.24.Fernandez-Fraga X,Azpiroz F,Malagelada JR.Signif-icance of pelvicfloor muscles in anal incontinence.Gastroenterology2002;123:1441–50.CONFLICT OF INTERESTGuarantor of the article:Satish S.C.Rao,M.D.Specific author contributions:Satish S.C.Rao:writing of manuscript.Renae Kavlock:data analysis and research. Sheila Rao:research.Financial support:In part by grant RO DK57100-03 Potential competing interests:None。