2004 Circ J 改善ST段抬高MI微血管痉挛病例报告(冠脉)
- 格式:pdf
- 大小:302.73 KB
- 文档页数:3

急性心肌梗死溶栓治疗后ST段再抬高的临床分析
邓俊萍
【期刊名称】《实用医技杂志》
【年(卷),期】2004(011)12A
【摘要】目的:探讨急性心肌梗死(AMI)静脉溶栓治疗后ST段再抬高的临床特点。
方法:将AMI患者90例,根据溶栓后有无ST段再抬高分为ST段抬高组(A组)
和ST段未抬高组(B组),比较两组间伴发疾病、冠脉病变、再通率、心律失常、
心功能变化(Killp分级等)。
结果:A组伴发糖尿病、高血压病、高脂血症、冠脉多支病变、心功能不全、心律失常发生率均高于B组,而冠脉再通率明显低于B组。
结论:溶栓治疗后ST段再抬高与患者并发糖尿病、高血压病、高脂血症密切相关,冠状动脉存在多支病变,该类患者溶栓再通率低,心肌受损严重,心功能不全、心律失常发生率高。
【总页数】2页(P2578-2579)
【作者】邓俊萍
【作者单位】临汾市人民医院,山西临汾044100
【正文语种】中文
【中图分类】R542.22
【相关文献】
1.急性心肌梗死溶栓治疗后ST段再抬高临床分析 [J], 韩凤波
2.急性心肌梗死溶栓治疗后ST段再抬高21例分析 [J], 剧仲华
3.急性心肌梗死静脉溶栓治疗后ST段再抬高临床意义探讨 [J], 杨发;解彦炯;方俊平;肖丽;于新丽;田江
4.急性心肌梗死溶栓治疗后ST段再抬高的临床分析 [J], 邓俊萍
5.急性心肌梗死溶栓治疗后迟发性ST段再抬高的临床意义 [J], 郭任维;任艳琴;王春玲;邹阳春
因版权原因,仅展示原文概要,查看原文内容请购买。

冠脉痉挛治愈案例
以下是一个冠脉痉挛治愈的案例:
一名患者因冠脉痉挛接受了抗血管痉挛治疗,但症状未缓解。
之后接受了冠脉造影和乙酰胆碱激发试验,结果发现冠脉痉挛和患者症状在冠脉内注射硝酸甘油后得到缓解。
然而,尽管接受了当前指南推荐的药物治疗,患者的症状仍未得到解决。
在这种情况下,医生决定尝试一种新的治疗方法——riociguat,这是一种可溶性鸟苷酸环化酶(sGC)激动剂,原本用于治疗肺动脉高压。
给予患者riociguat后,患者逐渐改善,生活质量明显提高。
在随后的乙酰胆碱激试验中,未能诱发冠脉痉挛。
以上案例仅供参考,每个患者的病情都不同,治疗方法也会因人而异。
如有相关症状,建议及时就医。
ST段抬高型急性心肌梗死急诊经皮冠状动脉介入治疗中欣维宁应用的临床观察摘要】目的探讨ST段抬高型急性心肌梗死患者在介入治疗中使用欣维宁的安全性有效性及并发症。
方法选择19例ST段抬高型急性心肌梗死患者于术前开始使用欣维宁,6例患者同时冠脉内注射。
结果18例(94.7%)患者成功介入治疗,17例(89.5%)达到TIMI血流3级。
1例(5.3%)TIMI血流2级,1例(5.3%)TIMI血流0级。
结论欣维宁能减少冠脉内血栓、改善心肌灌注、减少主要心脏不良事件发生,疗效确切,安全性好。
【关键词】欣维宁急性心肌梗死血栓ST段抬高型急性心肌梗死主要病理改变是在冠状动脉粥样硬化不稳定斑块基础上破裂继发血栓完全阻塞冠状动脉所致,而经皮冠状动脉介入治疗作为ST段抬高型急性心肌梗死最直接最有效的治疗手段得到越来越广泛的应用。
血小板糖蛋白(glycoprotein,GP)Ⅱb -Ⅲa 受体拮抗剂因其抑制血小板聚集的最后通路,有效地抑制血小板聚集抑制血栓形成的作用应用于急诊冠脉介入治疗已写入临床指南,我科自2009年10月开展急性心梗急诊介入治疗以来共19例患者使用血小板糖蛋白Ⅱ b-Ⅲ a 受体拮抗剂—欣维宁,效果满意,特总结如下。
1、资料与方法1.1 一般资料:2009年10月-2010年9月在我院心内科就诊的ST段抬高型急性心肌梗死共19例,其中男18例,女1例,年龄38-75岁,平均年龄54±3岁,从首发胸痛症状到就诊时间7小时内,从就诊到冠脉开通时间2小时内。
初发心梗17例,再发心梗1例。
合并糖尿病者6例,合并高血压病者5例。
1.2 方法:全部患者同意介入治疗后在心内科病房即开始给予阿司匹林300mg、70岁以上者氯吡格雷450mg, 70岁以下者氯吡格雷600mg,欣维宁剂量为10μg/kg在3 分钟内推注后,以0.15 μ g/kg·min 维持静点,其中6人因造影并球囊扩张后显示血栓负荷重,遂于冠状动脉内10μg/kg注射,全部患者均以0.15 μ g/kg·min维持静点18-24小时。

・标准与规范・作者单位:250012济南,山东大学齐鲁医院心内科美国心脏病学会和美国心脏病协会发布关于ST 段抬高型急性心肌梗死治疗指南(2004年修订版)蒋世亮 季晓平 张运 美国心脏病学会和美国心脏病协会(ACC /AHA )修订的ST 段抬高型急性心肌梗死(STE M I )处理新指南于2004年8月发表。
与1999年版指南相比,新指南作了较大修改[1],现将主要内容简介如下。
一、院前处理胸痛患者在含化硝酸甘油014mg 无效后(观察时间为5m in ),应立即与当地急救中心联系。
疑诊为STE M I 且无阿司匹林禁忌证的患者应立即口服阿司匹林(非肠衣片)162mg ~325mg 。
急救人员应尽快赶到发病现场(目标时间为8m in )行心电图(ECG )等检查,在具备心内科医师和护理人员的救护车中可对STE M I 患者行院前溶栓治疗,从接诊到开始溶栓的时间应控制在30m in 内。
若不能行院前溶栓,应尽快转送至附近医院行再灌注治疗。
若行溶栓治疗,从送达医院至开始溶栓的时间应控制在30m in 内;如行直接PC I 治疗,从院前开始转送至球囊扩张的时间应控制在90m in 内。
有下列情况的STE M I 患者应迅速转送至条件较好的医疗中心行血管成形术(PC I 或CABG ):(1)心源性休克;(2)有溶栓禁忌证;(3)死亡危险性特别高。
强化院前急救的目标是将患者的总缺血时间控制在120m in 内。
二、急诊室处理11诊断程序:应在10m in 内完成病史采集、体检和12导联ECG 描记,若有适应证,应在接诊30m in 内开始溶栓治疗或90m in 内开始直接PC I 治疗。
应常规行心肌肌钙蛋白、心肌酶谱等实验室检查,但不应因之延误再灌注治疗的实行。
疑有主动脉夹层的患者,应行床旁X 线、经胸或经食管超声、胸部CT 、MR I 等检查明确诊断。
21一般治疗和药物治疗:(1)吸氧:低氧血症的患者(SaO 2<90%)应吸氧。
・实践与交流・Practice and Communication 美国心脏病学会/美国心脏协会ST段抬高心肌梗死治疗指南(2004年版)要点解读李瑞杰1 卢 全1 胡大一21.北京市垂杨柳医院心血管疾病中心(北京100022);2.同济大学医学院(上海200092) 【摘要】介绍ACC/AHA关于ST段抬高心肌梗死治疗指南(2004年版)中有关流行病学、急诊科处理和住院治疗的主要内容并加以解读。
【关键词】ST段抬高心肌梗死,临床治疗指南 【中图分类号】R542.22 【文献标识码】A 【文章编号】16722531(2005)02016704ACC/AHA G uidelines for the Management of P atients with ST2E levation Myocardial I n2 farction:Essential I ntroduction LI Rui2jie1,LU Quan1,H U Da2yi2. 1.The H eart Center o f Beijing Chuiyangliu Hospital,Beijing100022,China; 2.Medical College o f Tongji Univer sity,Shanghai200092,China 【Abstract】The E ssential of ACC/AHA Guidelines for the Management of Patients with ST2Elevation Myocardial Infarc2tion was introduced,including epidemology,initial management in the emergency department and hospital management. 【K ey w ords】 ST2Elevation myocardial infarction,Practice guidelines 美国心脏病学会(ACC)和美国心脏协会(AHA)早在1990年就推出“急性心肌梗死病人早期治疗指南”,又于1999年再版“急性心肌梗死治疗指南”。

急性ST段抬高型心肌梗死静脉溶栓再通的患者采取择期PCI
术治疗的临床分析
高振军;张莉;周殷;陈志琳
【期刊名称】《航空航天医学杂志》
【年(卷),期】2011(022)002
【摘要】目的:观察择期经皮冠脉介入治疗(PCI)治疗急性ST抬高型心肌梗死(STAMI)的疗效.方法:回顾性分析我科2007-06~2010-06期间收治的急性ST抬高型心肌梗死患者接受静脉溶栓后再通的患者116例,其中接受择期PCI治疗者53例,未行PCI者65例为对照组,两组患者出院后均选用β受体阻滞剂氯吡格雷阿斯匹林、调脂类等药物,随访6个月,观察心血管事件的发生情况.结果:接受PCI治疗组心血管事件明显减少,随访期间无心源性猝死及再梗发生,心绞痛的发生率亦明显低于对照组(P<0.01).结论:静脉溶栓冠脉完全再通率低,此类患者择期PCI术能取得良好疗效.
【总页数】2页(P207-208)
【作者】高振军;张莉;周殷;陈志琳
【作者单位】
【正文语种】中文
【中图分类】R541.1
【相关文献】
1.急性 ST 段抬高型心肌梗死静脉溶栓再通的患者采取择期 PCI 术治疗探讨 [J], 解永芳
2.急性ST段抬高型心肌梗死静脉溶栓再通的患者采取择期PCI术治疗的临床分析[J], 高振军;张莉;周殷;陈志琳
3.静脉溶栓再通的急性心梗患者择期PCI治疗的临床分析 [J], 高振军;张莉;周殷
4.静脉溶栓再通的急性心梗患者择期PCI治疗的临床分析 [J], 高振军;张莉;周殷
5.rt-PA静脉溶栓联合依诺肝素钠注射液对急性ST段抬高型心肌梗死患者心电图变化及血管再通率的影响 [J], 毛绍英
因版权原因,仅展示原文概要,查看原文内容请购买。
ised,double 2blind,p lacebocontr olled,multicentre trial (the EU 2ROP A study )[J ].Lancet,2003,362:782-788.2006-09-10收稿 本文编辑:李允德作者单位:中国医学科学院中国协和医科大学阜外心血管病医院冠心病诊疗中心,北京100037E 2mail:yyj@fuwihos p ital .org【文章编号】1005-2194(2007)12-0907-042004年ACC /AHA ST 段抬高急性心肌梗死治疗指南评介杨跃进,赵京林【中图分类号】R5 【文献标志码】A 杨跃进,男,医学博士,主任医师,教授,博士生导师。
现任中国医学科学院阜外心血管病医院副院长、心内科主任。
兼任中华医学会心血管分会委员和北京分会心血管专业委员会委员、《中华心血管病杂志》、《中国医学科学杂志》、《中国循环杂志》、《中国实用内科杂志》等9家杂志的编委、副主编。
主持国家自然科学基金、科技部“863”分课题,教育部、卫生部等基金课题12项。
获得部级成果奖1项、医科院级1项、医科院级的医疗成就奖4项,并获得1999年度赛克勒基金青年医师奖。
已发表学术论文100余篇。
【关键词】 心肌梗死;ST 段抬高;指南Keywords Myocardial infarcti on;ST seg ment elevated;Guideline美国心脏病学会(ACC )和美国心脏协会(AHA )于2004发布了新版ST 段抬高急性心肌梗死(STE M I )治疗指南,该指南以临床实践为导向,全面综合了近几年大量的循证医学新证据,就STE M I 的预防、诊断、鉴别诊断、治疗和随访等方面进行了全面的原则论述,对指导临床医师在临床实践中的正确决策具有重要价值,发表后受到广泛关注[1]。
现评介如下。
1 分类定义STE M I 治疗指南将疗效指征和证据水平定义如下:疗效指征分为Ⅰ、Ⅱa 、Ⅱb 、Ⅲ类,主要依据治疗的获益和风险相比较,而确定是否应该手术或应该给予药物治疗。
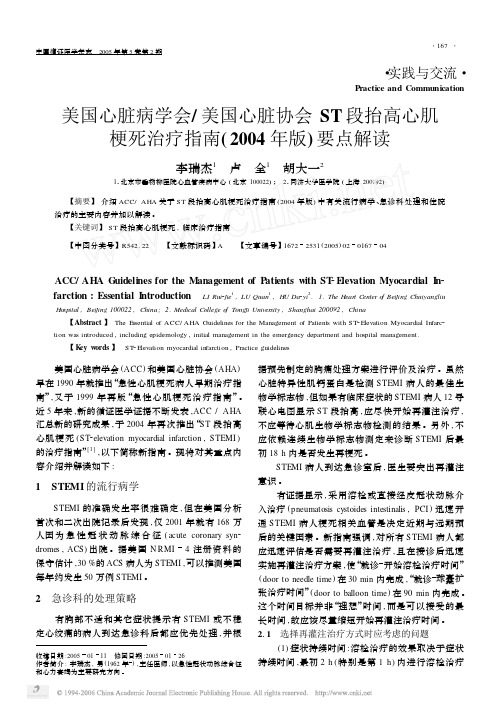
depression during exercise or atrial pacing despite normal coronary angiograms are diagnosed as ‘syndrome X’.3,4 From the therapeutic point of view, calcium channel block-ers are extremely effective for epicardial coronary spasm, but have limited efficacy in patients with syndrome X.5,6 Several cases with spontaneous electrocardiographic (ECG) changes and normal coronary angiograms have been recently reported in Japan7,8and this rare phenome-non is thought to be caused by coronary microvascular spasm. Very recently, it has been suggested that coronary microvascular spasm may also contribute to the anginal pain of vasospastic angina9and syndrome X.10We describe a case of spontaneous microvascular spasm during coro-nary angiography with ST segment elevation for which intracoronary administration of nicorandil was extremely useful.Case ReportA 64-year-old man with a history of previous coronary intervention of the left anterior descending artery was admitted because of recurrent chest pain at rest. Physical examination on admission showed a blood pressure of 124/60mmHg, a heart rate of 68beats/min and no abnor-malities of the chest and abdomen. Admission ECG at rest showed no significant ischemic changes; ECG during exer-cise was not performed. After obtaining written informed consent, cardiac catheterization was performed. Left ven-Circulation Journal Vol.68, March 2004ECG showed ST segment elevation in leads II, III and aV F (Fig1). Immediate right coronary angiography revealed no significant coronary artery stenosis, but markedly delayed contrast medium washout. The thrombolysis-in-myocar-dial-infarction (TIMI) frame count11,12from the ostium to the distal landmark increased to 116 (Fig2). Because the chest pain, ST segment elevation and delayed washout of the right coronary artery continued for 2min after intra-coronary administration of nitroglycerin, we administrated 2mg of nicorandil into the right coronary artery. One minute later, the chest pain and ST segment elevation disappeared. Repeat right coronary angiography revealed normal contrast medium washout, and the TIMI frame count decreased to 42 (Fig3). The patient was diagnosed as having microvascular spasm for which intracoronary administration of nicorandil was extremely useful.DiscussionThere are a few reports of patients experiencing sponta-neous microvascular spasm during coronary angiography. Yamagishi et al7reported a case of delayed contrast medi-um washout in the left anterior descending artery and ST segment elevation. As the onset of chest pain occurred more than 10min after the administration of acetylcholine into the right coronary artery, they believed that microvas-cular spasm in the left anterior descending artery occurred spontaneously and was not induced by intracoronary administration of acetylcholine. Mohri et al8reported 2 cases with spontaneous microvascular spasm as evidenced by the typical chest pain during catheterization and which was associated with ST segment elevation in one patient and ST segment depression in the other.In the current case, we did not use either ergonovine or acetylcholine to induce coronary spasm during coronaryCirc J2004; 68:267–269268KURISU S et al.Circulation Journal Vol.68, March 2004angiography. An increase in demand for myocardial oxygen was unlikely to have caused myocardial ischemia because the rate –pressure product did not change during ST segment elevation. In addition, it is unlikely that the contrast medium was associated with the myocardial ischemia because the ECG changes did not occur during left coronary angiography. We could not perform left coro-nary angiography during the ST segment elevation in leads II, III and aV F , but observed markedly delayed contrast medium washout in the right coronary artery, which sug-Fig 1.Serial electrocardiograms (ECGs) during coronary angiography. ST segment elevation was observed in leads II,III and aV F even after intracoronary administration of nitroglycerin. Intracoronary administration of nicorandil resolved the ECGs change.Fig 2.Left ventriculography revealed normal wall motion, and coronary angiography revealed no significant coronary artery stenosis. Contrast medium, which used for the first image of the right coronary artery, remained in the mid portion.The second image of the right coronary artery revealed markedly delayed contrast medium washout, and the TIMI frame count increased to 116. Numbers show TIMI frame count from the ostium.Fig 3.Intracoronary administration of nicorandil attenuated the delayed washout of the right coronary artery, and the TIMI frame count decreased to 42.Numbers show TIMI frame count from the ostium.269Nicorandil in Microvascular SpasmCirculation Journal Vol.68, March 2004gested that the microvascular spasm occurred spontaneous-ly in the right coronary artery. It has been demonstrated that nitroglycerin produces a dose-related dilation of coro-nary microvessels greater than 200 m in diameter and has little or no effect on smaller coronary microvessels. In the current case, intracoronary administration of nitroglycerin did not attenuate chest symptoms or the ST segment eleva-tion, suggesting that the major responsible site was vessels of less than 200 m in diameter.13Nicorandil is a hybrid of a nitrate and an ATP-sensitive potassium channel opener,and has a potent vasodilator effect on coronary arteries.14–17It has been shown that coronary microvascular resistance is largely regulated by ATP-sensitive potassium channels. Ito et al recently reported 2 patients in whom intracoronary administration of diltiazem or nicorandil markedly attenu-ated delayed contrast medium washout with ST segment depression refractory to nitroglycerin.18We have shown that intracoronary administration of nicorandil can attenu-ate spontaneous microvascular spasm even with ST seg-ment elevation. It is an important but unresolved question why the ECG reveals ST segment elevation in one patient with microvascular spasm and ST segment depression in the other. It may depend on the degree of myocardial ischemia caused by the microvascular spasm or the micro-vascular level at which the spasm occurs. Further clinical studies and basic experiments are required to clarify the mechanism. In conclusion, nicorandil should be considered in patients with microvascular spasm.References1.Maseri A, Pesola A, Marzilli M, Severi S, Parodi O, L’Abbate A, et al. Coronary vasospasm in angina pectoris. Lancet 1977; 1:713–718.2.Ozaki Y, Keane D, Serruys PW. Progression and regression of coro-nary stenosis in the long-term follow-up of vasospastic angina.Circulation 1995; 92:2446–2456.3.K aski JC, Crea F, Nihoyannopoulus P, Hacket D, Maseri A.Transient myocardial ischemia during daily life in patients with syndrome X. Am J Cardiol 1986; 58:1242–1247.4.Maseri A, Crea F, Kaski JC, Crake T. Mechanisms of angina pectoris in syndrome X. J Am Coll Cardiol 1991; 17:499–506.nza GA, Colonna G, Pasceri V, Maseri A. Atenolol versus amlodipine versus isosorbide-5-mononitrate on anginal symptoms in syndrome X. Am J Cardiol 1999; 84:854–856.6.Matsumoto A, Mohri M, Takeshita A. Three-year follow-up of Japanese patients with microvascular angina attributable to coronary microvascular spasm. Int J Cardiol 2001; 81:151–156.7.Yamagishi H, Itagane H, Hato K, Suto Y, Minami S, Otsuka M, et al.A case of rest angina due to microvascular spasm. Jpn Circ J 1997;61:87–89.8.Mohri M, Koyanagi M, Egashira K, Tagawa H, Ichiki T, Shimokawa H, et al. Angina pectoris caused by coronary microvascular ncet 1998; 351:1165–1169.9.Sun H, Mohri M, Shimokawa H, Usui M, Urakami L, Takeshita A.Coronary microvascular spasm causes myocardial ischemia in patients with vasospastic angina. J Am Coll Cardiol 2002; 39:847–851.10.Murakami H, Urabe K, Nishimura M. Inappropriate microvascular constriction produced transient ST-segment elevation in patients with syndrome X. J Am Coll Cardiol 1998; 32:1287–1294.11.Gibson CM, Cannon CP, Daley WL, Dodge JT, Alexander B,Marble SJ, et al. TIMI frame count: A quantitative method of assess-ing coronary artery flow. Circulation 1996; 93:879–888.12.Gibson CM, Murphy SA, Rizzo MJ, Ryan KA, Marble SJ, McCabe CH, et al. Relationship between TIMI frame count and clinical outcomes after thrombolytic administration. Circulation 1999; 99:1945–1950.13.Marcus ML, Chilian WM, Kanatsuka H, Dellsperger KD, Eastham CL, Lamping K G. Understanding the coronary circulation through studies at the microvascular level. Circulation 1990; 82:1–7.14.Noguchi T, Nonogi H, Yasuda S, Daikoku S, Morii I, Itoh A, et al.Refractory coronary spasm relieved by intracoronary administration of nicorandil. Jpn Circ J 2000; 64:396–398.15.Yasuda T, Hashimura K, Matsu–ura Y, Kato Y, Ueda T, Mori I, et al.Nicorandil, a hybrid between nitrate and ATP-sensitive potassium channel opener, preconditions human heart to ischemia during percu-taneous transluminal coronary angioplasty. Jpn Circ J 2001; 65:526–530.16.Ashikaga T, Nishizaki M, Arita M, Yamawake N, Fujii H, Kishi Y,et al. Opening of K (ATP) channel attenuates the increase in QT dispersion produced by the first balloon inflation during coronary angioplasty. Circ J 2002; 66: 469–472.17.Sakai K , Yamagata T, Teragawa H, Matsuura H, Chayama K.Nicorandil enhances myocardial tolerance to ischemia without progressive collateral recruitment during coronary angioplasty. Circ J 2002; 66:317–322.18.Ito K, Sugihara H, Zen K, Hikosaka T, Adachi Y, Yoneyama S, et al.Two cases of microvascular vasospastic angina: Usefulness of 99m Tc-tetrofosmin myocardial SPECT in clinical diagnosis. Kaku-igaku 2000; 37:23–29.。