盐酸纳美芬注射液说明书
- 格式:docx
- 大小:59.63 KB
- 文档页数:9
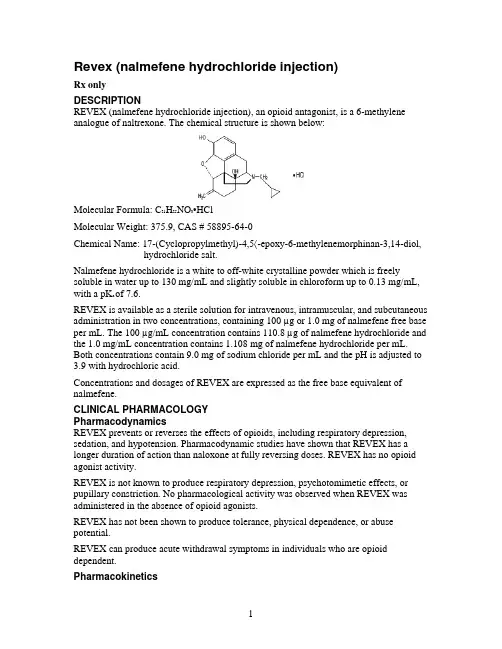
Revex (nalmefene hydrochloride injection)Rx onlyDESCRIPTIONREVEX (nalmefene hydrochloride injection), an opioid antagonist, is a 6-methylene analogue of naltrexone. The chemical structure is shown below:Molecular Formula: C21H25NO3•HClMolecular Weight: 375.9, CAS # 58895-64-0Chemical Name: 17-(Cyclopropylmethyl)-4,5〈-epoxy-6-methylenemorphinan-3,14-diol, hydrochloride salt.Nalmefene hydrochloride is a white to off-white crystalline powder which is freely soluble in water up to 130 mg/mL and slightly soluble in chloroform up to 0.13 mg/mL, with a pK a of 7.6.REVEX is available as a sterile solution for intravenous, intramuscular, and subcutaneous administration in two concentrations, containing 100 µg or 1.0 mg of nalmefene free base per mL. The 100 µg/mL concentration contains 110.8 µg of nalmefene hydrochloride and the 1.0 mg/mL concentration contains 1.108 mg of nalmefene hydrochloride per mL. Both concentrations contain 9.0 mg of sodium chloride per mL and the pH is adjusted to 3.9 with hydrochloric acid.Concentrations and dosages of REVEX are expressed as the free base equivalent of nalmefene.CLINICAL PHARMACOLOGYPharmacodynamicsREVEX prevents or reverses the effects of opioids, including respiratory depression, sedation, and hypotension. Pharmacodynamic studies have shown that REVEX has a longer duration of action than naloxone at fully reversing doses. REVEX has no opioid agonist activity.REVEX is not known to produce respiratory depression, psychotomimetic effects, or pupillary constriction. No pharmacological activity was observed when REVEX was administered in the absence of opioid agonists.REVEX has not been shown to produce tolerance, physical dependence, or abuse potential.REVEX can produce acute withdrawal symptoms in individuals who are opioid dependent.PharmacokineticsNalmefene exhibited dose proportional pharmacokinetics following intravenousadministration of 0.5 mg to 2.0 mg. Pharmacokinetic parameters for nalmefene after a 1mg intravenous administration in adult male volunteers are listed in Table 1.Table 1: Mean (CV%) Nalmefene Pharmacokinetic ParametersIn Adult Males Following a 1 mg Intravenous DoseParameter Young, N=18 Elderly, N=1162-80 Age 19-32Cp at 5 min. (ng/mL) 3.7 (29) 5.8 (38)Vdss (L/kg) 8.6 (19) 8.6 (29)Vc (L/kg) 3.9 (29) 2.8 (41)AUC0-inf (ng-hr/mL) 16.6 (27) 17.3 (14)Terminal T1/2 (hr) 10.8 (48) 9.4 (49)Clplasma (L/hr/kg) 0.8 (23) 0.8 (18)ABSORPTIONNalmefene was completely bioavailable following intramuscular or subcutaneousadministration in 12 male volunteers relative to intravenous nalmefene. The relativebioavailabilities of intramuscular and subcutaneous routes of administration were 101.5%± 8.1% (Mean ± SD) and 99.7% ± 6.9%, respectively. Nalmefene will be administeredprimarily as an intravenous bolus, however, nalmefene can be given intra-muscularly(IM) or subcutaneously (SC) if venous access cannot be established. While the time tomaximum plasma nalmefene concentration was 2.3 ± 1.1 hours following intramuscularand 1.5 ± 1.2 hours following subcutaneous administrations, therapeutic plasmaconcentrations are likely to be reached within 5-15 minutes after a 1 mg dose in anemergency. Because of the variability in the speed of absorption for IM & SC dosing, andthe inability to titrate to effect, great care should be taken if repeated doses must be givenby these routes.DISTRIBUTIONFollowing a 1 mg parenteral dose, nalmefene was rapidly distributed. In a study of brainreceptor occupancy, a 1 mg dose of nalmefene blocked over 80% of brain opioidreceptors within 5 minutes after administration. The apparent volumes of distributioncentrally (Vc) and at steady-state (Vdss) are 3.9 ± 1.1 L/kg and 8.6 ± 1.7 L/kg,respectively. Ultrafiltration studies of nalmefene have demonstrated that 45% (CV 4.1%)is bound to plasma proteins over a concentration range of 0.1 to 2 µg/mL. An in vitrodetermination of the distribution of nalmefene in human blood demonstrated thatnalmefene distributed 67% (CV 8.7%) into red blood cells and 39% (CV 6.4%) intoplasma. The whole blood to plasma ratio was 1.3 (CV 6.6%) over the nominalconcentration range in whole blood from 0.376 to 30 ng/mL.METABOLISMNalmefene is metabolized by the liver, primarily by glucuronide conjugation, andexcreted in the urine. Nalmefene is also metabolized to trace amounts of an N-dealkylated metabolite. Nalmefene glucuronide is inactive and the N-dealkylatedmetabolite has minimal pharmacological activity. Less than 5% of nalmefene is excretedin the urine unchanged. Seventeen percent (17%) of the nalmefene dose is excreted in thefeces. The plasma concentration-time profile in some subjects suggests that nalmefene undergoes enterohepatic recycling..ELIMINATIONAfter intravenous administration of 1 mg REVEX to normal males (ages 19-32), plasma concentrations declined biexponentially with a redistribution and a terminal elimination half-life of 41 ± 34 minutes and 10.8 ± 5.2 hours, respectively. The systemic clearance of nalmefene is 0.8 ± 0.2 L/hr/kg and the renal clearance is 0.08 ± 0.04 L/hr/kg.Special PopulationsELDERLYDose proportionality was observed in nalmefene AUC0-inf following 0.5 to 2 mg intravenous administration to elderly male subjects. Following a 1 mg intravenous nalmefene dose, there were no significant differences between young (19-32 years) and elderly (62-80 years) adult male subjects with respect to plasma clearance, steady-state volume of distribution, or half-life. There was an apparent age-related decrease in the central volume of distribution (young: 3.9 ± 1.1 L/kg, elderly: 2.8 ± 1.1 L/kg) that resulted in a greater initial nalmefene concentration in the elderly group. While initial nalmefene plasma concentrations were transiently higher in the elderly, it would not be anticipated that this population would require dosing adjustment. No clinical adverse events were noted in the elderly following the 1 mg intravenous nalmefene dose. PATIENTS WITH HEPATIC IMPAIRMENTSubjects with hepatic disease, when compared to matched normal controls, had a 28.3% decrease in plasma clearance of nalmefene (0.56 ± 0.21 L/hr/kg versus 0.78 ± 0.24L/hr/kg, respectively). Elimination halflife increased from 10.2 ± 2.2 hours to 11.9 ± 2.0 hours in the hepatically impaired. No dosage adjustment is recommended since nalmefene will be administered as an acute course of therapy.PATIENTS WITH RENAL IMPAIRMENTThere was a statistically significant 27% decrease in plasma clearance of nalmefene in the end-stage renal disease (ESRD) population during interdialysis (0.57 ± 0.20 L/hr/kg) and a 25% decreased plasma clearance in the ESRD population during intradialysis (0.59 ± 0.18 L/hr/kg) compared to normals (0.79 ± 0.24 L/hr/kg). The elimination half-life was prolonged in ESRD patients from 10.2 ± 2.2 hours in normals to 26.1 ± 9.9 hours. (See DOSAGE AND ADMINISTRATION.)GENDER DIFFERENCESThere has not been sufficient pharmacokinetic study to make a definitive statement as to whether the pharmacokinetics of nalmefene differs between the genders.CLINICAL TRIALSREVEX has been administered to reverse the effects of opioids after general anesthesia and in the treatment of overdose. It has also been used to reverse the systemic effects of intrathecal opioids.Reversal of Postoperative Opioid DepressionREVEX (nalmefene hydrochloride injection) (N=326) was studied in 5 controlled trials in patients who had received morphine or fentanyl intraoperatively. The primary efficacy criterion was the reversal of respiratory depression. A positive reversal was defined asboth an increase in respiratory rate by 5 breaths per minute and a minimum respiratory rate of 12 breaths per minute. Five minutes after administration, initial single REVEX doses of 0.1, 0.25, 0.5, or 1.0 µg/kg had effectively reversed respiratory depression in a dose-dependent manner. Twenty minutes after initial administration, respiratory depression had been effectively reversed in most patients receiving cumulative doses within the recommended range (0.1 to 1.0 µg/kg). Total doses of REVEX above 1.0µg/kg did not increase the therapeutic response. The postoperative administration of REVEX at the recommended doses did not prevent the analgesic response to subsequently administered opioids.Reversal of the Effect of Intrathecally Administered OpioidsIntravenous REVEX at doses of 0.5 and 1.0 µg/kg was administered to 47 patients given intrathecal morphine. One to 2 doses of 0.5 and 1.0 µg/kg REVEX reversed respiratory depression in most patients. The administration of REVEX at the recommended doses did not prevent the analgesic response to subsequently administered opioids. Management of Known or Suspected Opioid OverdoseREVEX (N=284) at doses of 0.5 mg to 2.0 mg was studied in 4 trials of patients who were presumed to have taken an opioid overdose. REVEX doses of 0.5 mg to 1.0 mg effectively reversed respiratory depression within 2 to 5 minutes in most patients subsequently confirmed to have opioid overdose. A total dose greater than 1.5 mg did not increase the therapeutic response.INDICATIONS AND USAGEREVEX is indicated for the complete or partial reversal of opioid drug effects, including respiratory depression, induced by either natural or synthetic opioids.REVEX is indicated in the management of known or suspected opioid overdose. CONTRAINDICATIONSREVEX is contraindicated in patients with a known hypersensitivity to the product. WARNINGSUse of REVEX in EmergenciesREVEX, like all drugs in this class, is not the primary treatment for ventilatory failure. In most emergency settings, treatment with REVEX should follow, not precede, the establishment of a patent airway, ventilatory assistance, administration of oxygen, and establishment of circulatory access.Risk of Recurrent Respiratory DepressionAccidental overdose with long acting opioids [such as methadone and levo-alpha-acetylmethadol (LAAM)] may result in prolonged respiratory depression. Respiratory depression in both the postoperative and overdose setting may be complex and involve the effects of anesthetic agents, neuromuscular blockers, and other drugs. While REVEX has a longer duration of action than naloxone in fully reversing doses, the physician should be aware that a recurrence of respiratory depression is possible, even after an apparently adequate initial response to REVEX treatment.Patients treated with REVEX should be observed until, in the opinion of the physician, there is no reasonable risk of recurrent respiratory depression. PRECAUTIONSGeneralCARDIOVASCULAR RISKS WITH NARCOTIC ANTAGONISTSPulmonary edema, cardiovascular instability, hypotension, hypertension, ventricular tachycardia, and ventricular fibrillation have been reported in connection with opioid reversal in both postoperative and emergency department settings. In many cases, these effects appear to be the result of abrupt reversal of opioid effects.Although REVEX has been used safely in patients with pre-existing cardiac disease, all drugs of this class should be used with caution in patients at high cardiovascular risk or who have received potentially cardiotoxic drugs. (See DOSAGE AND ADMINISTRATION.)RISK OF PRECIPITATED WITHDRAWALREVEX, like other opioid antagonists, is known to produce acute withdrawal symptoms and, therefore, should be used with extreme caution in patients with known physical dependence on opioids or following surgery involving high doses of opioids. Imprudent use or excessive doses of opioid antagonists in the postoperative setting has been associated with hypertension, tachycardia, and excessive mortality in patients at high risk for cardiovascular complications. (See PRECAUTIONS.)INCOMPLETE REVERSAL OF BUPRENORPHINEPreclinical studies have shown that nalmefene at doses up to 10 mg/kg (437 times the maximum recommended human dose) produced incomplete reversal of buprenorphine-induced analgesia in animal models. This appears to be a consequence of a high affinity and slow displacement of buprenorphine from the opioid receptors. Hence, REVEX may not completely reverse buprenorphine-induced respiratory depression.Drug InteractionsREVEX has been administered after benzodiazepines, inhalational anesthetics, muscle relaxants, and muscle relaxant antagonists administered in conjunction with general anesthesia. It also has been administered in outpatient settings, both in trials in conscious sedation and in the emergency management of overdose following a wide variety of agents. No deleterious interactions have been observed.Preclinical studies have shown that both flumazenil and nalmefene can induce seizures in animals. The coadministration of both flumazenil and nalmefene produced fewer seizures than expected in a study in rodents, based on the expected effects of each drug alone. Based on these data, an adverse interaction from the coadministration of the two drugs is not expected, but physicians should remain aware of the potential risk of seizures from agents in these classes.Carcinogenesis, Mutagenesis, Impairment of FertilityNalmefene did not have mutagenic activity in the Ames test with five bacterial strains or the mouse lymphoma assay. Clastogenic activity was not observed in the mouse micronucleus test or in the cytogenic bone marrow assay in rats. However, nalmefene did exhibit a weak but significant clastogenic activity in the human lymphocyte metaphase assay in the absence but not in the presence of exogenous metabolic activation. Oral administration of nalmefene up to 1200 mg/m2/day did not affect fertility, reproductive performance, and offspring survival in rats.Use in PregnancyPREGNANCY CATEGORY BReproduction studies have been performed in rats (up to 1200 mg/m2/day) and rabbits (up to 2400 mg/m2/day) by oral administration of nalmefene and in rabbits by intravenous administration up to 96 mg/m2/day (114 times the human dose). There was no evidence of impaired fertility or harm to the fetus. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.Nursing MothersNalmefene and its metabolites were secreted into rat milk, reaching concentrations approximately three times those in plasma at one hour and decreasing to about half the corresponding plasma concentrations by 24 hours following bolus administration. As no clinical information is available, caution should be exercised when REVEX is administered to a nursing woman.Use in Pediatric PatientsSafety and effectiveness of REVEX in pediatric patients have not been established.Use in NeonatesThe safety and effectiveness of REVEX in neonates have not been established in clinical studies. In a preclinical study, nalmefene was administered by subcutaneous injection to rat pups at doses up to 205 mg/m2/day throughout maternal lactation without producing adverse effects. A preclinical study evaluating the irritancy of the dosage form following arterial and venous administration in animals showed no vascular irritancy.REVEX (nalmefene hydrochloride injection) should only be used in the resuscitation of the newborn when, in the opinion of the treating physician, the expected benefits outweigh the risks.Geriatric UseClinical studies of Revex did not include sufficient number of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.ADVERSE REACTIONSAdverse event information was obtained following administration of REVEX to 152 normal volunteers and in controlled clinical trials to 1127 patients for the treatment of opioid overdose or for postoperative opioid reversal.Nalmefene was well tolerated and showed no serious toxicity during experimental administration to healthy individuals, even when given at 15 times the highest recommended dose. In a small number of subjects, at doses exceeding the recommendedREVEX dose, nalmefene produced symptoms suggestive of reversal of endogenousopioids, such as have been reported for other narcotic antagonist drugs. These symptoms(nausea, chills, myalgia, dysphoria, abdominal cramps, and joint pain) were usuallytransient and occurred at very low frequency.Such symptoms of precipitated opioid withdrawal at the recommended clinical doseswere seen in both postoperative and overdose patients who were later found to have hadhistories of covert opioid use. Symptoms of precipitated withdrawal were similar to thoseseen with other opioid antagonists, were transient following the lower doses used in thepostoperative setting, and more prolonged following the administration of the largerdoses used in the treatment of overdose.Tachycardia and nausea following the use of nalmefene in the postoperative setting werereported at the same frequencies as for naloxone at equivalent doses. The risk of boththese adverse events was low at doses giving partial opioid reversal and increased withincreases in dose. Thus, total doses larger than 1.0 µg/kg in the postoperative setting and1.5 mg/70 kg in the treatment of overdose are not recommended.Relative Frequencies of Common Adverse ReactionsWith an Incidence Greater than 1%(all patients, all clinical settings)Adverse EventNalmefene Naloxone PlaceboN=1127N=369N=776% Nausea 18%18%Vomiting 9% 7% 4%- Tachycardia 5%8%- Hypertension 5%7%Postoperative pain 4% 4% N/A- Fever 3%4%Dizziness 3% 4% 1%Headache 1% 1% 4%Chills 1%-1%- Hypotension 1%1%- Vasodilatation 1%1%Incidence less than 1%CARDIOVASCULAR: Bradycardia, arrhythmiaDIGESTIVE: Diarrhea, dry mouthNERVOUS SYSTEM: Somnolence, depression, agitation, nervousness, tremor,confusion, withdrawal syndrome, myoclonusRESPIRATORY: PharyngitisSKIN: PruritusUROGENITAL: Urinary retentionThe incidence of adverse events was highest in patients who received more than therecommended dose of REVEX.Laboratory findings: Transient increases in CPK were reported as adverse events in 0.5%of the postoperative patients studied. These increases were believed to be related tosurgery and not believed to be related to the administration of REVEX. Increases in AST were reported as adverse events in 0.3% of the patients receiving either nalmefene or naloxone. The clinical significance of this finding is unknown. No cases of hepatitis or hepatic injury due to either nalmefene or naloxone were observed in the clinical trials. DRUG ABUSE AND DEPENDENCEREVEX is an opioid antagonist with no agonist activity. It has no demonstrated abuse potential, is not addictive, and is not a controlled substance.OVERDOSAGEIntravenous doses of up to 24 mg of nalmefene, administered to healthy volunteers in the absence of opioid agonists, produced no serious adverse reactions, severe signs or symptoms, or clinically significant laboratory abnormalities. As with all opioid antagonists, use in patients physically dependent on opioids can result in precipitated withdrawal reactions that may result in symptoms that require medical attention. Treatment of such cases should be symptomatic and supportive. Administration of large amounts of opioids to patients receiving opioid antagonists in an attempt to overcome a full blockade has resulted in adverse respiratory and circulatory reactions.DOSAGE AND ADMINISTRATIONImportant Information - Dosage FormsREVEX is supplied in two concentrations that can be identified by their color coded container labels: a concentration suitable for postoperative use (100 µg/mL) in a blue labeled ampul containing ONE (1) mL and a concentration suitable for the management of overdose (1 mg/mL, 10 times as concentrated, 20 times as much drug) in a green labeled ampul containing TWO (2) mL. Proper steps should be taken to prevent use of the incorrect concentration.General PrinciplesREVEX should be titrated to reverse the undesired effects of opioids. Once adequate reversal has been established, additional administration is not required and may actually be harmful due to unwanted reversal of analgesia or precipitated withdrawal.Duration of ActionThe duration of action of REVEX is as long as most opioid analgesics. The apparent duration of action of REVEX will vary, however, depending on the half-life and plasma concentration of the narcotic being reversed, the presence or absence of other drugs affecting the brain or muscles of respiration, and the dose of REVEX administered. Partially reversing doses of REVEX (1 µg/kg) lose their effect as the drug is redistributed through the body, and the effects of these low doses may not last more than 30-60 minutes in the presence of persistent opioid effects. Fully reversing doses (1 mg/70 kg) have been shown to last many hours in both experimental and clinical studies, but may complicate the management of patients who are in pain, at high cardiovascular risk, or who are physically dependent on opioids.The recommended doses represent a compromise between a desirable controlled reversal and the need for prompt response and adequate duration of action. Using higher dosages or shorter intervals between incremental doses is likely to increase the incidence and severity of symptoms related to acute withdrawal such as nausea, vomiting, elevated blood pressure, and anxiety.Patients Tolerant to or Physically Dependent on OpioidsREVEX may cause acute withdrawal symptoms in individuals who have some degree of tolerance to and dependence on opioids. These patients should be closely observed for symptoms of withdrawal following administration of the initial and subsequent injections of REVEX. Subsequent doses should be administered with intervals of at least 2-5 minutes between doses to allow the full effect of each incremental dose of REVEX to be reached.Recommended Doses for Reversal of Postoperative Opioid Depression Use 100 µg/mL dosage strength (blue label) and see Table 2 for initial doses.The goal of treatment with REVEX in the postoperative setting is to achieve reversal of excessive opioid effects without inducing a complete reversal and acute pain. This is best accomplished with an initial dose of 0.25 µg/kg followed by 0.25 µg/kg incremental doses at 2-5 minute intervals, stopping as soon as the desired degree of opioid reversal is obtained. A cumulative total dose above 1.0 µg/kg does not provide additional therapeutic effect.Table 2: Reversal of Postoperative Opioid DepressionmL of REVEXBody Weight100 µg/mL Solution50 kg 0.12560 kg 0.15070 kg 0.17580 kg 0.20090 kg 0.225100 kg 0.250In cases where the patient is known to be at increased cardiovascular risk, it may be desirable to dilute REVEX 1:1 with saline or sterile water and use smaller initial and incremental doses of 0.1 µg/kg.Management of Known or Suspected Opioid OverdoseUse 1.0 mg/mL dosage strength (green label).The recommended initial dose of REVEX for non-opioid dependent patients is 0.5 mg/70 kg. If needed, this may be followed by a second dose of 1.0 mg/70 kg, 2-5 minutes later. If a total dose of 1.5 mg /70 kg has been administered without clinical response, additional REVEX (nalmefene hydrochloride injection) is unlikely to have an effect. Patients should not be given more REVEX than is required to restore the respiratory rate to normal, thus minimizing the likelihood of cardiovascular stress and precipitated withdrawal syndrome.If there is a reasonable suspicion of opioid dependency, a challenge dose of REVEX 0.1 mg/70 kg should be administered initially. If there is no evidence of withdrawal in 2 minutes, the recommended dosing should be followed.REVEX had no effect in cases where opioids were not responsible for sedation and hypoventilation. Therefore, patients should only be treated with REVEX when thelikelihood of an opioid overdose is high, based on a history of opioid overdose or the clinical presentation of respiratory depression with concurrent pupillary constriction. Repeated DosingREVEX is the longest acting of the currently available parenteral opioid antagonists. If recurrence of respiratory depression does occur, the dose should again be titrated to clinical effect using incremental doses to avoid over-reversal.Hepatic and Renal DiseaseHepatic disease and renal failure substantially reduce the clearance of nalmefene (see Pharmacokinetics). For single episodes of opioid antagonism, adjustment of REVEX dosage is not required. However, in patients with renal failure, the incremental doses should be delivered slowly (over 60 seconds) to minimize the hypertension and dizziness reported following the abrupt administration of nalmefene to such patients.Loss of Intravenous AccessShould intravenous access be lost or not readily obtainable, a pharmacokinetic study has shown that a single dose of REVEX should be effective within 5-15 minutes after intramuscular or subcutaneous doses of 1.0 mg. (See Pharmacokinetics.)SAFETY AND HANDLINGREVEX is distributed in sealed ampuls which represent no known risk to health care workers. As with all parenterals, care should be taken to prevent the generation and inhalation of aerosols during preparation and use. Dermal absorption of spilled REVEX should be prevented by prompt removal of contaminated clothing and rinsing the skin thoroughly with cool water.Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.HOW SUPPLIEDREVEX (nalmefene hydrochloride injection) is available in the following presentations: An ampul containing 1 mL of 100 µg/mL nalmefene base (Blue Label) Box of 10 (NDC 10019-315-21)An ampul containing 2 mL of 1 mg/mL nalmefene base (Green Label) Box of 10 (NDC 10019-311-22)Store at controlled room temperature.REVEX is a registered trademark of Ivax Laboratories, Inc.Baxter is a trademark of Baxter International, Inc.Manufactured forBaxter Healthcare CorporationDeerfield, IL 60015 USAby: Taylor PharmaceuticalsDecatur, IL 62525For Product Inquiry 1 800 ANA DRUG (1-800-262-3784)U.S. Patent No. 4,535,157MLT-01167/1.011。
盐酸纳美芬注射液说明书乐萌SANY标准化小组 #QS8QHH-HHGX8Q8-GNHHJ8-HHMHGN#盐酸纳美芬注射液说明书【药品名称】通用名称:盐酸纳美芬注射液汉语拼音: Yansuan Nameifen Zhusheye商品名:乐萌英文名: Nalmefene Hydrochloride Injection【成份】1. 本品主要成份为盐酸纳美芬,化学名称: 17-环丙甲基-4,5α-环氧-6-亚甲基吗啡喃-3,14-二醇盐酸盐化学结构式:分子式: C21H25NO3·HCl分子量:375.9CAS No.:58895-64-02. 辅料:氯化钠、注射用水【性状】本品为无色的澄明液体。
【适应症】纳美芬用于完全或部分逆转阿片类药物的作用,包括由天然的或合成的阿片类药物引起的呼吸抑制。
【规格】1ml:0.1mg(以C21H25NO3计)【用法用量】纳美芬注射液一般为静注,也可肌注或皮下注射。
一般原则:本品可通过剂量滴定逆转不期望的阿片类作用。
因为不期望逆转痛觉缺失而引起危害或产生撤药反应,一旦达到了足够的逆转效果,就不应继续用药。
逆转术后阿片类药物抑制的推荐剂量:使用100μg/mL的剂量浓度,见表1的初始剂量。
术后使用纳美芬治疗的目的是为了逆转阿片类药物过度的抑制作用,而不是引起完全的逆转和急性疼痛。
初始剂量为0.25μg/kg,2-5分钟后可增加剂量0.25μg/kg,当达到了预期的阿片类药物逆转作用后立即停药。
累积剂量大于1.0μg/kg不会增加疗效。
对已知的心血管高危患者用药时,应将本品与氯化钠注射液或无菌注射用水按1:1的比例稀释,并使用0.1μg/kg作为初始剂量和增加剂量。
对阿片类药物耐受或产生躯体依赖的患者:纳美芬对阿片类药物耐受或躯体依赖的患者能引起急性戒断症状。
在初次或持续用药时应密切观察这些患者是否出现戒断症状。
至少应在2-5分钟后再次用药,以增加剂量达到最大疗效。
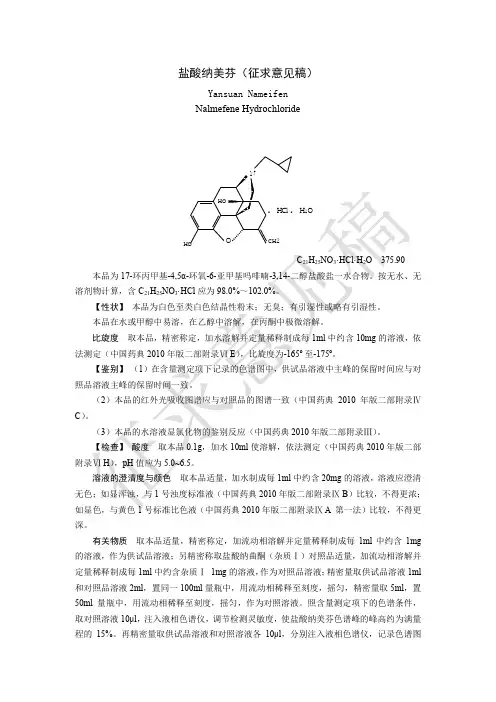
盐酸纳美芬(征求意见稿)Yansuan NameifenNalmefene Hydrochloride. H Cl . H 2ONHOCH2O HOC 21H 25NO 3·HCl·H 2O 375.90 本品为17-环丙甲基-4,5α-环氧-6-亚甲基吗啡喃-3,14-二醇盐酸盐一水合物。
按无水、无溶剂物计算,含C 21H 25NO 3·HCl 应为98.0%~102.0%。
【性状】 本品为白色至类白色结晶性粉末;无臭;有引湿性或略有引湿性。
本品在水或甲醇中易溶,在乙醇中溶解,在丙酮中极微溶解。
比旋度 取本品,精密称定,加水溶解并定量稀释制成每1ml 中约含10mg 的溶液,依法测定(中国药典2010年版二部附录Ⅵ E ),比旋度为-165º至-175º。
【鉴别】 (1)在含量测定项下记录的色谱图中,供试品溶液中主峰的保留时间应与对照品溶液主峰的保留时间一致。
(2)本品的红外光吸收图谱应与对照品的图谱一致(中国药典2010年版二部附录ⅣC )。
(3)本品的水溶液显氯化物的鉴别反应(中国药典2010年版二部附录Ⅲ)。
【检查】 酸度 取本品0.1g ,加水10ml 使溶解,依法测定(中国药典2010年版二部附录Ⅵ H ),pH 值应为5.0~6.5。
溶液的澄清度与颜色 取本品适量,加水制成每1ml 中约含20mg 的溶液,溶液应澄清无色;如显浑浊,与1号浊度标准液(中国药典2010年版二部附录Ⅸ B )比较,不得更浓;如显色,与黄色1号标准比色液(中国药典2010年版二部附录Ⅸ A 第一法)比较,不得更深。
有关物质 取本品适量,精密称定,加流动相溶解并定量稀释制成每1ml 中约含1mg 的溶液,作为供试品溶液;另精密称取盐酸纳曲酮(杂质Ⅰ)对照品适量,加流动相溶解并定量稀释制成每1ml 中约含杂质Ⅰ 1mg 的溶液,作为对照品溶液;精密量取供试品溶液1ml 和对照品溶液2ml ,置同一100ml 量瓶中,用流动相稀释至刻度,摇匀,精密量取5ml ,置50ml 量瓶中,用流动相稀释至刻度,摇匀,作为对照溶液。
我院盐酸纳美芬注射液合理使用的干预研究摘要】目的了解盐酸纳美芬注射液在我院的使用情况并进行合理干预,规范纳美芬临床使用。
方法调取本院2009年08、09两个月内盐酸纳美芬注射液的使用情况进行统计,从消耗量,使用人数,开药医生人数,诊断分布等进行分析,分析结果通过院内网发布等方式对临床用药进行合理干预;并持续追踪8~12月的盐酸纳美芬注射液使用情况以了解干预效果。
结果临床上存在超适应症和超剂量使用的情况;药师合理干预后,不合理使用情况得到了明显纠正。
结论药师通过有效途径进行用药合理性干预有助于减少临床不合理用药。
【关键词】纳美芬用药干预合理用药【中图分类号】R969.3 【文献标识码】A 【文章编号】2095-1752(2013)27-0109-02纳美芬(nalmefene)为特异性吗啡受体阻断剂,是纳曲酮的6-亚甲基类似物,该药系1975年合成,1995年上市。
SFDA批准的盐酸纳美芬注射液说明书中的适应症为“用于完全或部分逆转阿片类药物的作用,包括由天然的或合成的阿片类药物引起的呼吸抑制”。
近年来,部分宣传资料夸大了纳美芬的作用,强调其可以用于各种原因引起的昏迷、休克患者,或颅脑损伤等患者,导致我院纳美芬注射液超适应症、超剂量使用的情况比较严重。
为了解该药物临床使用现状,规范纳美芬在我院的使用,我们通过HIS系统对2009年8月和9月全院盐酸纳美芬注射液使用情况进行了连续调查,调查结果发布于院内网及2009年第五期药讯。
并通过8月至12月盐酸纳美芬注射液的发放量的持续追踪,了解药师干预效果,旨在规范我院用药的合理性。
1. 资料与方法1.1 资料从医院管理系统(浙江联众卫生信息科技有限公司开发)调取我院2009年8月和9月盐酸纳美芬注射液的相关数据,包括药品数量、销售金额、使用科室、使用人数、开方医师、疾病诊断等;持续统计8~12月盐酸纳美芬注射液的销售数量。
1.2 方法制定盐酸纳美芬注射液使用调查表,纪录患者姓名、性别、年龄、临床诊断分布、使用情况(应用时间、用法用量、持续时间)、开方医生等。
盐酸纳美芬注射液说明书【药品名称】通用名称:盐酸纳美芬注射液汉语拼音:Yan sua n Nameife n Zhusheye商品名:乐萌英文名:Nalmefe ne Hydrochloride Injection【成份】1.本品主要成份为盐酸纳美芬,化学名称:二醇盐酸盐化学结构式:分子式:C21H25NO3 HCI分子量:375.9CAS No. : 58895-64-02.辅料:氯化钠、注射用水【性状】本品为无色的澄明液体。
【适应症】纳美芬用于完全或部分逆转阿片类药物的作用,包括由天然的或合成的阿片类药物引起的呼吸抑制。
【规格】1ml:0.1mg (以C21H25NO3 计)【用法用量】纳美芬注射液一般为静注,也可肌注或皮下注射。
一般原则:本品可通过剂量滴定逆转不期望的阿片类作用。
因为不期望逆转痛觉缺失而引起危害或产生撤药反应,一旦达到了足够的逆转效果,就不应继续用药。
逆转术后阿片类药物抑制的推荐剂量:使用100卩g/mL的剂量浓度,见表1的初始剂量。
术后使用纳美芬治疗的目的是为了逆转阿片类药物过度的抑制作用,而不是引起完全的逆转和急性疼痛。
初始剂量为0.25卩g/kg 2-5分钟后可增加剂量0.25卩g/kg当达到了预期的阿片类药物逆转作用后立即停药。
累积剂量大于1.0卩g/k环会增加疗效。
0. L2&(\ inf)0. 175u jjn0.2250.25017-环丙甲基-4,5 «环氧-6-亚甲基吗啡喃-3,14-对已知的心血管高危患者用药时,应将本品与氯化钠注射液或无菌注射用水按1:1 的比例稀释,并使用0.1卩g/kg乍为初始剂量和增加剂量。
对阿片类药物耐受或产生躯体依赖的患者:纳美芬对阿片类药物耐受或躯体依赖的患者能引起急性戒断症状。
在初次或持续用药时应密切观察这些患者是否出现戒断症状。
至少应在2-5 分钟后再次用药,以增加剂量达到最大疗效。
重复用药:如果复发呼吸抑制,应再增加剂量来达到临床治疗效果,增加剂量时应避免过度逆转。
盐酸纳美芬注射液说明书【药品名称】通用名称:盐酸纳美芬注射液汉语拼音:Yansuan Nameifen Zhusheye商品名:乐萌英文名:Nalmefene Hydrochloride Injection【成份】本品主要成份为盐酸纳美芬,辅料为氯化钠、注射用水化学名称:17-环丙甲基-4,5α-环氧-6-亚甲基吗啡喃-3,14-二醇盐酸盐化学结构式:分子式:C21H25NO3·HCl分子量:375.9【性状】本品为无色的澄明液体。
【适应症】纳美芬用于完全或部分逆转阿片类药物的作用,包括由天然的或合成的阿片类药物引起的呼吸抑制。
【规格】1ml:0.1mg(以C21H25NO3计)【用法用量】纳美芬注射液一般为静注,也可肌注或皮下注射。
一般原则:本品可通过剂量滴定逆转不期望的阿片类作用。
因为不期望逆转痛觉缺失而引起危害或产生撤药反应,一旦达到了足够的逆转效果,就不应继续用药。
逆转术后阿片类药物抑制的推荐剂量:使用100μg/mL的剂量浓度,见表1的初始剂量。
术后使用纳美芬治疗的目的是为了逆转阿片类药物过度的抑制作用,而不是引起完全的逆转和急性疼痛。
初始剂量为0.25μg/kg,2-5分钟后可增加剂量0.25μg/kg,当达到了预期的阿片类药物逆转作用后立即停药。
累积剂量大于1.0μg/kg不会增加疗效。
表1对已知的心血管高危患者用药时,应将本品与氯化钠注射液或无菌注射用水按1:1的比例稀释,并使用0.1μg/kg作为初始剂量和增加剂量。
对阿片类药物耐受或产生躯体依赖的患者:纳美芬对阿片类药物耐受或躯体依赖的患者能引起急性戒断症状。
在初次或持续用药时应密切观察这些患者是否出现戒断症状。
至少应在2-5分钟后再次用药,以增加剂量达到最大疗效。
重复用药:如果复发呼吸抑制,应再增加剂量来达到临床治疗效果,增加剂量时应避免过度逆转。
【不良反应】对健康者用药者,即使剂量达到推荐剂量的15倍或15倍以上,纳美芬的耐受性都很好、没有出现严重的不良反应。
纳美芬是一种新型纯阿片受体拮抗剂,对各种阿片受体(μ、κ、α受体)均有作用,与阿片受体结合效能是纳洛酮的4倍,且单次静脉等效剂量给药可获得更长的作用时间,即在完全逆转剂量下纳美芬的作用持续时间长于纳洛酮[1]。
由于其在拮抗阿片药物的呼吸抑制、镇静和低血压作用方面有明显优势,目前广泛用于临床,尤其是术后促醒和神经外科领域。
该药于1995年获得美国食品药品监督管理局(FDA)批准上市,但因商业原因已在美国退市。
然而,该药在我国用量较大,应用范围之广需引起警惕。
为了解该药物目前的使用现状,规范盐酸纳美芬注射液在我院的合理使用,笔者采用回顾性分析方法,调取2019年6月– 12月在我院使用盐酸纳美芬注射液患者的病例资料并进行合理性评价,旨在促进该药在临床的合理使用。
1 资料与方法采用回顾性研究的方法,调取我院2019年6月1日– 12月31日使用盐酸纳美芬注射液的住院患者病例资料,共纳入279例患者,收集患者的性别、年龄、体质量、住院时间、科室和出院诊断等信息,排除医嘱作废的患者资料。
通过查阅电子病历,提取患者使用盐酸纳美芬注射液的剂量、给药方法,根据国家药品监督管理局(National Medical Products Administration,NMPA)批准的盐酸纳美芬注射液药品说明书(商品名称:乐萌,规格为1 mL∶500 μg,成都天台山制药有限公司)进行合理性评价,主要包括用药适应证、疗程、用法用量等。
2 结果2.1 一般情况我院自2019年6月1日– 12月31日使用盐酸·药物利用分析·279例盐酸纳美芬注射液临床使用分析安胜男,任文静,付桂英(解放军总医院医疗保障中心派驻第五医学中心药剂科,北京 100073)[摘要] 目的:了解并评价盐酸纳美芬注射液在我院住院患者中临床应用的合理性,为临床合理用药提供参考。
方法:采用回顾性分析方法,调取我院2019年6月– 12月期间使用盐酸纳美芬注射液住院患者的信息,收集患者性别、年龄、科室、临床诊断、药物用法用量、疗程等数据,对上述指标进行统计分析,评价用药合理性。

盐酸纳美芬注射液说明书一金美芬
逆转术后阿片类药物抑制的推荐剂量:
使用100 g/ml的剂量浓度,见表1的初始剂量
表1 :逆转术后阿片类药物的抑制作用
术后使用纳美芬治疗的目的是为了逆转阿片类药物过度的抑制作用,而不是引起完全的逆转和急性疼痛。
初始剂量为0.25 g/kg , 2〜5min后可增加剂量
0.25 g/kg,当达到了预期的阿片类药物逆转作用后立即停药。
累计剂量大于1.0 g/kg不会增加疗效。
对已知的心血管高危患者用药时,应将本品与氯化钠注射液或无菌注射用水按 1 :1的比例稀释,并使用0.1 g/kg作为初始剂量和增加剂量。
对阿片类药物耐受或产生躯体依赖的患者:
纳美芬对阿片类药物耐受或躯体依赖的患者能引起急性戒断症状。
在初次或持续用药时应密切观察这些患者是否出现戒断症状。
至少应在2〜5分钟后再次用药, 以增加剂量达到最大疗效。
床病例)。
盐酸纳布啡注射液说明书 Ting Bao was revised on January 6, 20021盐酸纳布啡注射液核准日期:2013年11月27日修改日期:2014年04月28日【药品名称】通用名称:盐酸纳布啡注射液?商品名:瑞静英文名:NalbuphineHydrochlorideInjection【成份】本品主要成份为盐酸纳布啡。
化学名称:(-)-17-(环丁烷甲基)-4,5α-环氧吗啡-3,6α,14-羟基盐酸盐倍半水合物。
化学结构式为:分子式:C21H27NO4·HCl·11/2H2O分子量:420.93本品的辅料:枸橼酸,枸橼酸钠,氯化钠。
【性状】本品为无色的澄明液体。
【适应症】盐酸纳布啡作为复合麻醉时诱导麻醉的辅助用药。
【规格】2ml:20mg【用量用法】诱导麻醉时,盐酸纳布啡的用量为0.2mg/kg,应在10---15分钟内静脉输注完。
使用盐酸纳布啡注射液过程中,若出现呼吸抑制现象,可用阿片受体拮抗剂纳洛酮逆转。
【不良反应】据国外文献报道,临床用纳布啡治疗中,最常见的不良反应为镇静,临床1066例接受该药治疗的患者381例出现了镇静(发生率为36%)。
不常见的不良反应包括:多汗99例(9%),恶心/呕吐68例(6%)、眩晕58例(5%)、口干44例(4%)和头痛27例(3%)。
此外还可发生一些罕见的不良反应(报道的发生率为1%或更低)中枢神经系统效应:神经质、抑郁、坐立不安、烦躁尖叫、欣快、敌意、多梦、精神错乱、晕厥、幻觉、焦虑、悲观、麻木、麻刺感,心理反应,如非真实感、人格解体、妄想、焦虑和幻觉的发生率较使用喷他佐辛时低。
心血管系统:高血压、低血压、心动过缓、心动过速;消化系统:胃肠绞痛、消化不良、口苦;呼吸系统:呼吸抑制、呼吸困难、哮喘;皮肤:瘙痒、干燥、荨麻疹;其他症状:吐字不清、尿急、视物模糊、面部潮红;过敏反应:在使用纳布啡过程中可出现过敏反应。