常用脑卒中量表
- 格式:doc
- 大小:64.50 KB
- 文档页数:7


脑卒中的分级标准
脑卒中,也被称为脑血管意外,是一种急性脑血管疾病。
其分级标准有多种,包括脑卒中评估量表(NIHSS)等。
脑卒中评估量表(NIHSS)是一个包含11个方面的评估量表,包括唤醒水平、回答提问、执行命令、最佳凝视、视野、面瘫、上肢运动、下肢运动、协调运动、感觉、最佳语音、构音以及忽视。
NIHSS的评分范围为0-42分,分数越高,神经受损越严重。
具体的分级如下:0-1分:正常或近乎正常;1-4分:轻度卒中/小卒中;5-15分:中度卒中;15-20分:中-重度卒中;21-42分:重度卒中。
此外,肌力评估也是脑卒中的一种分级标准。
具体来说,零级是指无肌张力的增加;一级是指肌张力略微增加,受累关节被动活动时末端呈现最小阻力,或者突然卡住;二级是指肌张力明显增加,大部分肌肉呈现较大阻力,但是受累的关节被动活动比较容易;三级是指肌张力严重增高,受累关节被动活动困难。
以上信息仅供参考,脑卒中的分级应根据具体症状由专业医师进行判断,并在医生的指导下进行科学的治疗和护理。
1。


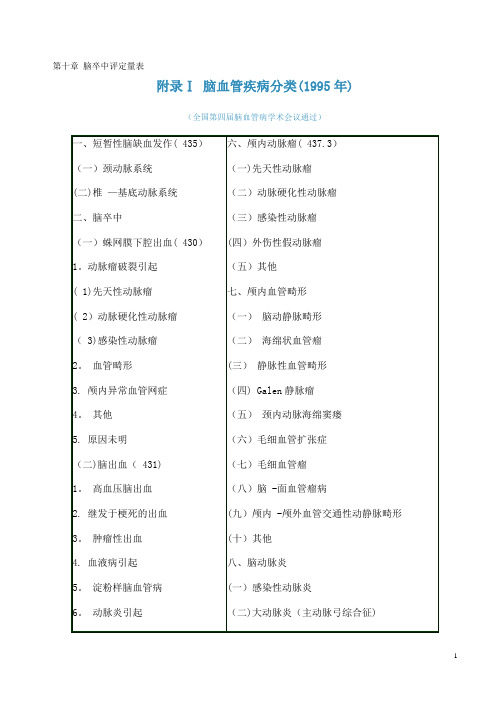
第十章脑卒中评定量表附录Ⅰ脑血管疾病分类(1995年)(全国第四届脑血管病学术会议通过)说明:一、本分类系经全国脑防办专家、在京专家和全国第四次脑血管病会议代表讨论,由王新德执笔,综合成此《脑血管疾病分类(1995年)》。
二、按病程发展可分为短暂性脑缺血发作、可逆性缺血发作(发作后3周内症状消失),进行性卒中和完全性卒中,仅列入短暂性脑缺血发作,其他未列入。
三、括号内数字为世界卫生组织第10版《国家疾病分类》的编号。
1.脑卒中结局评定的基本模式—ICF2001年5月22日,在日内瓦举行的第54届世界卫生大会上,根据近20年来的研究结果,世界卫生组织(WHO)提出并经会员国一致通过了一项WHA54.21决议:在会员国使用《国际功能、残疾和健康分类》(internatianal classification of functianing,disablity and health,简称ICF)。
从而,提出了一个全新的有关“功能”、“残疾”和“健康”概念的新模式(图1—1)一、身体的构成成分、活动和参与能力1.身体的构成成分在这里包括身体的“结构”和“功能”。
“身体结构”是指身体的解剖部位,如器官、肢体及其组成部分。
“身体功能”是指身体各系统的生理功能(包括心理功能),如精神功能、言语功能、感觉功能、心肺功能、消化功能、排泄功能、神经肌肉骨骼和运动功能等.2.活动能力是指个体执行一项任务和行动的能力,如学习和应用知识的能力、完成一般任务和要求的能力、交流的能力、个体的活动能力、生活自理能力等.3.参与能力指的是投人到一种生活情景中,如家庭生活的能力、人际交往和相处关系的能力、接受教育和工作就业的能力、参与社会和社区生活的能力等.图1-1 WHO关于“功能”、“残疾"和“健康"概念的新模式在ICF出台之前,有关康复医学的效果评定和质量控制的概念就已经有了很大的进展:在使用ICIDH 的年代,就己经逐步明确了不能只以“残损”(impairment)水平的积分改善来评定康复医疗的效果,而强调在“残疾”(disability)和“残障"(handicap)水平上积分的改善.通常,使用ADL(activity of daily living,日常生活活动能力)和IADL(instrumental activities of daily living,工具性日常生活活动能力)的积分(如巴氏指数—BI和功能独立性评定—FIM等)来定量“残疾"水平,使用QOL(生活质量)积分(如简表SF—36,世界卫生组织生活质量问卷WHOQOL—100,欧洲生活质量量表Euro—QOL,良好状态评定表QWB,诺丁汉健康量表NHP等)来定量“残障"水平积分。
脑卒中患者的评分标准
1. NIHSS评分,美国国立卫生研究院卒中量表(NIHSS)是评
估中风患者病情严重程度的常用工具,包括了11项测试,如意识状态、视觉、运动能力等,总分范围从0到42分,分数越高表示中风
越严重。
2. mRS评分,修正Rankin量表(mRS)是评估中风患者病后生
活质量和功能状态的常用工具,分为0-6级,0表示没有症状,6表
示死亡。
3. Barthel指数,用于评估患者的日常生活能力,包括如何进
行个人生活自理、移动、上下楼梯、穿衣、洗澡等,总分100分,
分数越高表示生活能力越强。
4. CHA2DS2-VASc评分,用于评估房颤患者中风危险的评分系统,包括年龄、性别、心衰、高血压、糖尿病等因素。
5. HAS-BLED评分,用于评估抗凝治疗下出血风险的评分系统,包括高血压、肝肾功能、中风史、出血史等因素。
这些评分标准能够帮助医生全面评估患者的病情和预后,指导治疗方案的制定和跟踪患者的病情变化,从而提高治疗效果和生活质量。
当然,具体的评分标准还会根据不同的临床情况和研究需求进行调整和补充。
第二十一节卒中相关量表目录一、缺血性卒中发生与复发风险评估量表1.缺血性卒中一级预防风险评估a)改良弗明汉卒中量表(表1)b)非瓣膜性心房颤动发生缺血性卒中风险的评分量表CHADS2和CHA2DS2-VASc(表3)2.缺血性卒中及TIA二级预防风险评估a)ABCD评估系统(表4)b)Essen量表(表5)c)卒中预测工具(SPI-2 表6)二、早期识别与诊断量表1.辛辛那提院前卒中量表(CPSS,表7)2.国际通用的快速识别脑卒中的FAST评估法(表8-1)3.中国版脑卒中简易识别法-中风120(表8-2)三、病因诊断评估量表1.STAF评分(表9)2.RoPE评分(表10)四、脑卒中后神经功能缺损与分级评估量表1.美国国立卫生研究所脑卒中(NIHSS表11)2.Glasgow 昏迷评分(表12)3.SAH临床分级:a)Hunt-Hess评分(表13)b)WFNS分级(表14)4.脑出血临床分级(ICH评分表15)5.动脉畸形分级:SPETZLER分级(表16)五、卒中分型:中国缺血性卒中亚型—CISS分型及临床干预六、卒中并发症发生风险评估量表1.深静脉血栓评估住院病人深静脉血栓形成(DVT)风险评估(表17)2.压疮风险评估Braden评估表及其评估指引细则(表18)3.营养风险筛查NRS-2002评估表(表19)4.卒中后肺炎a)AISAPS量表(表20)b)A2DS2 评分(表21)c)急性缺血性卒中相关性肺炎评分(Acute Ischemic Stroke-associated Pneumonia Score, AIS-APS)(计算相对复杂,较少使用)七、卒中并发症诊断评估量表1.中风后抑郁状态的评估a)综合医院焦虑/抑郁(HAD)情绪测定表(表22)b)汉密尔顿焦虑/抑郁量表(HAMA/D)(表23)c)PHQ-9(表24)2.中风后认知障碍的评估a)MMSE简易智能精神状态检查量表(表25)b)蒙特利尔认知评估量表(MoCA量表26)3.中风后吞咽障碍的评估a)进食评估问卷调查工具-10(EAT一10表27)b)洼田饮水试验(表28)4.中风后残疾评估a)功能残疾程度:mRS评分(表29)b)日常生活活动能力:Barthe指数(表30)八、各种治疗措施预后评估量表1.溶栓后出血风险的评估:HAT评分(表31-1)2.溶栓后出血风险的评估:SICH评分(表31-2)3.溶栓预后不良:DRAGON评分(表32)4.房颤抗凝治疗出血风险评估HAS-BLED评分(表33)5.缺血性卒中预后评估:IScore评(表34)九、其他量表1.ASPECTS评分(表35)2.Hachinski缺血指数量表(表36)3.匹茨堡睡眠质量指数量表(表37)4.大血管梗死的评估(表38)注:心血管疾病包括心肌梗死、心绞痛、冠状动脉功能不全、间歇性跛行、充血性心力衰竭等,左心室肥厚是指心电图诊断的心室肥厚。
Essen 脑卒中风险评分量表
(Essen stroke risk score, ESRS)
【使用说明】
1.该量表是目前少数基于缺血性卒中人群判断脑卒中复发风险的预测工具之一,可以很好地合理预测脑卒中和复合心血管事件的发生,是评估患者危险分层并指导用药的理想工具,简便且易于临床操作。
该量表适用于相对稳定的门诊就诊的缺血性卒中患者以及住院治疗的急性缺血性卒中患者的脑卒中复发风险预测评估,也可用于研究人群和个体患者的风险分层。
2.评估结果及应用:ESRS3〜6分者为高度风险,年脑卒中复发风险为7%〜9%; 6分以上者为极高度风险,年脑卒中复发风险达11%。
ESRS评分23分的患者再发脑卒中或心血管死亡的风险显著高于ESRS<3分的患者,应该实施氯毗格雷强化二级预防抗血小板治疗策略。
常用脑卒中量表1、改良Rankin量表(Modified Rankin Scale)Modified Rankin Scale(Internet Stroke Center at Washington University提供的Modified Rankin Scale)SCORE DESCRIPTION0 No symptoms at all1 No significant disability despite symptoms; able to carry out all usual duties and activities2 Slight disability; unable to carry out all previous activities, but able to look after own affairs without assistance3 Moderate disability; requiring some help, but able to walk without assistance4 Moderately severe disability; unable to walk without assistance and unable to attend to own bodily needs without assistance5 Severe disability; bedridden, incontinent and requiring constant nursing care and attention6 DeadScores:0-62、日常生活能力量表-巴氏指数(Barthel Index)THE Patient Name: ___________________________BARTHEL Rater Name: ___________________________ INDEX Date: ___________________________Activity ScoreFEEDING0 = unable5 = needs help cutting, spreading butter, etc., or requires modified diet10 = independent ______BATHING0 = dependent5 = independent (or in shower) ______GROOMING0 = needs to help with personal care5 = independent face/hair/teeth/shaving (implements provided) ______ DRESSING0 = dependent5 = needs help but can do about half unaided10 = independent (including buttons, zips, laces, etc.) ______BOWELS0 = incontinent (or needs to be given enemas)5 = occasional accident10 = continent ______BLADDER0 = incontinent, or catheterized and unable to manage alone5 = occasional accident10 = continent ______TOILET US E0 = dependent5 = needs some help, but can do something alone10 = independent (on and off, dressing, wiping) ______TRANSFERS (BED TO CHAIR AND BACK)0 = unable, no sitting balance5 = major help (one or two people, physical), can sit10 = minor help (verbal or physical)15 = independent ______MOBILITY (ON LEVEL S URFACES)0 = immobile or < 50 yards5 = wheelchair independent, including corners, > 50 yards10 = walks with help of one person (verbal or physical) > 50 yards15 = independent (but may use any aid; for example, stick) > 50 yards ______ STAIRS0 = unable5 = needs help (verbal, physical, carrying aid)10 = independent ______TOTAL (0–100): ______3、格拉斯哥昏迷量表(Glasgow Coma Scale)From Wikipedia, the free encyclopediaJump to: navigation, searchGlasgow Coma Scale or GCS is a neurological scale that aims to give a reliable, objective way of recording the conscious state of a person for initial as well as subsequent assessment. A patient is assessed against the criteria of the scale, and the resulting points give a patient score between 3 (indicating deep unconsciousness) and either 14 (original scale) or 15 (the more widely used modified or revised scale).GCS was initially used to assess level of consciousness after head injury, and the scale is now used by first aid, EMS, and doctors as being applicable to all acute medical and trauma patients. In hospitals it is also used in monitoring chronic patients in intensive care.The scale was published in 1974 by Graham Teasdale and Bryan J. Jennett, professors of neurosurgery at the University of Glasgow's Institute of Neurological Sciences at the city's Southern General Hospital.GCS is used as part of several ICU scoring systems, including APACHE II, SAPS II, and SOFA, to assess the status of the central nervous system. A similar scale, the Rancho Los Amigos Scale is used to assess the recovery of traumatic brain injury patients.Elements of the scaleGlasgow Coma Scale1 2 3 4 5 6Eyes DoesnotopeneyesOpens eyes inresponse topainfulstimuliOpens eyesinresponseto voicespontaneouslyVerb al MakesnosoundsIncomprehensible soundsUttersinappropriate wordsdisorientedMoto r MakesnoExtension topainfulAbnormalflexion toFlexion /WithdrawaLocalizesObeyscommanmoveme ntsstimuli(decerebrateresponse)painfulstimuli(decorticateresponse)l topainfulstimulipainfulstimulidsThe scale comprises three tests: eye, verbal and motor responses. The three values separately as well as their sum are considered. The lowest possible GCS (the sum) is 3 (deep coma or death), while the highest is 15 (fully awake person). Best eye response (E)There are 4 grades starting with the most severe:1.No eye opening2.Eye opening in response to pain. (Patient responds to pressure on the patient’s fingernailbed; if this does not elicit a response, supraorbital and sternal pressure or rub may beused.)3.Eye opening to speech. (Not to be confused with an awaking of a sleeping person; suchpatients receive a score of 4, not 3.)4.Eyes opening spontaneously[edit] Best verbal response (V)There are 5 grades starting with the most severe:1.No verbal response2.Incomprehensible sounds. (Moaning but no words.)3.Inappropriate words. (Random or exclamatory articulated speech, but no conversationalexchange)4.Confused. (The patient responds to questions coherently but there is some disorientationand confusion.)5.Oriented. (Patient responds coherently and appropriately to ques tions such as the patient’sname and age, where they are and why, the year, month, etc.)[edit] Best motor response (M)There are 6 grades starting with the most severe:1.No motor response2.Extension to pain (abduction of arm, internal rotation of shoulder, pronation of forearm,extension of wrist, decerebrate response)3.Abnormal flexion to pain (adduction of arm, internal rotation of shoulder, pronation offorearm, flexion of wrist, decorticate response)4.Flexion/Withdrawal to pain (flexion of elbow, supination of forearm, flexion of wristwhen supra-orbital pressure applied ; pulls part of body away when nailbed pinched)5.Localizes to pain. (Purposeful movements towards painful stimuli; e.g., hand crossesmid-line and gets above clavicle when supra-orbital pressure applied.)6.Obeys commands. (The patient does simple things as asked.)[edit] InterpretationIndividual elements as well as the sum of the score are important. Hence, the score is expressed in the form "GCS 9 = E2 V4 M3 at 07:35".Generally, brain injury is classified as:∙Severe, wit h GCS ≤ 8∙Moderate, GCS 9 - 12∙Minor, GCS ≥ 13.Tracheal intubation and severe facial/eye swelling or damage make it impossible to test the verbal and eye responses. In these circumstances, the score is given as 1 with a modifier attached e.g. 'E1c' where 'c' = closed, or 'V1t' where t = tube. A composite might be 'GCS 5tc'. This would mean, for example, eyes closed because of swelling = 1, intubated = 1, leaving a motor score of 3 for 'abnormal flexion'. Often the 1 is left out, so the scale reads Ec or Vt.The GCS has limited applicability to children, especially below the age of 36 months (where the verbal performance of even a healthy child would be expected to be poor). Consequently the Pediatric Glasgow Coma Scale, a separate yet closely related scale, was developed for assessing younger children.[edit] Revisions∙Glasgow Coma Scale: While the 15 point scale is the predominant one in use, this is in fact a modification and is more correctly referred to as the Modified Glasgow Coma Scale.The original scale was a 14 point scale, omitting the category of 'abnormal flexion'. Some centres still use this older scale, but most (including the Glasgow unit where the originalwork was done) have adopted the modified one.∙The Rappaport Coma/Near Coma Scale made other changes.[edit] See also∙Blantyre Coma Scale∙Rancho Los Amigos Scale∙Paediatric Glasgow Coma Scale∙Revised Trauma Score4、美国国立卫生研究院卒中量表(NIH Stroke Scale,NIHSS)5、斯堪的那维亚卒中量表(Scandinavian Stroke Scale,SSS)6、欧洲卒中量表(The European Stroke Scale,ESS)7、中国脑卒中临床神经功能缺损程度评分量表(1995)8、HAMILTON抑郁量表-21项评分标准9、HAMILTON焦虑量表。