房颤抗栓治疗ACCP9
- 格式:pptx
- 大小:111.75 KB
- 文档页数:19
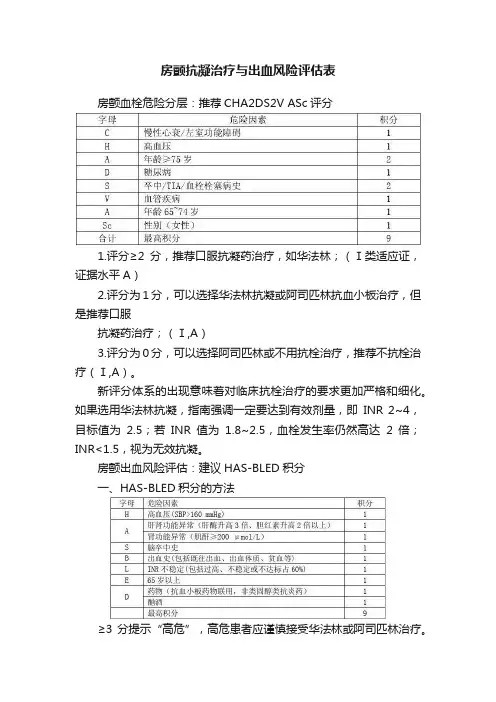
房颤抗凝治疗与出血风险评估表
房颤血栓危险分层:推荐CHA2DS2V ASc评分
1.评分≥2分,推荐口服抗凝药治疗,如华法林;(Ⅰ类适应证,证据水平A)
2.评分为1分,可以选择华法林抗凝或阿司匹林抗血小板治疗,但是推荐口服
抗凝药治疗;(Ⅰ,A)
3.评分为0分,可以选择阿司匹林或不用抗栓治疗,推荐不抗栓治疗(Ⅰ,A)。
新评分体系的出现意味着对临床抗栓治疗的要求更加严格和细化。
如果选用华法林抗凝,指南强调一定要达到有效剂量,即INR 2~4,目标值为2.5;若INR值为1.8~2.5,血栓发生率仍然高达2倍;INR<1.5,视为无效抗凝。
房颤出血风险评估:建议HAS-BLED积分
一、HAS-BLED积分的方法
≥3分提示“高危”,高危患者应谨慎接受华法林或阿司匹林治疗。
并在开始抗栓治疗之后,加强复查PT、INR
但实际上需要注意的是,高龄、高血压、卒中病史等既是卒中的危险因素,又是出血的危险因素,故新指南对高危患者抗栓治疗的建议虽然更加全面,可操作性也更强,但部分情况下抗栓治疗仍然会是一个较为棘手的选择。
2012 ACCP 抗栓治疗与血栓预防临床实践指南(第9 版)美国胸科医师协会(ACCP )于2012 年 2 月7 日公布了第9 版《抗栓与血栓预防》临床实践指南,发表于《胸》杂志的增刊:Chest 2012, 141 ( 2 Suppl )。
与上一版指南(2008 年发布)相比,新版指南更为简洁明了,首次加入了关于深静脉血栓形成(DVT)的诊断章节。
指南目录1、Disclaimer2、Panel List3、Executive Summary (执行摘要)4、Introduction to the Ninth Edition (第九版简介)点击下载全文5、Methodology for the Development of AntithromboticTherapy and Prevention of Thrombosis Guidelines (抗栓和溶栓治疗指南制定方法)点击下载全文6、Patient Values and Preferences in DecisionMaking for Antithrombotic Therapy (抗凝治疗决策中的患者评估和参数)点击下载全文7、Parenteral Anticoagulants (肠外抗凝治疗)点击下载全文8、Oral Anticoagulant Therapy (口服抗凝药的使用)点击下载全文9、Antiplatelet Drugs(抗血小板药物)点击下载全文10、New Antithrombotic Drugs (抗栓新药)点击下载全文11、Evidence-Based Management of AnticoagulantTherapy(抗栓治疗管理的循证基础)点击下载全文12、Approach to Outcome Measurement in thePrevention of Thrombosis in Surgical and MedicalPatients (外科治疗患者预防血栓形成预后管理措施)点击下载全文13、Prevention of VTE in Nonsurgical Patients(非手术患者的VTE 预防)点击下载全文14、Prevention of VTE in Nonorthopedic SurgicalPatients(非骨科手术的VTE 预防)点击下载全文15、Prevention of VTE in Orthopedic Surgery Patients (骨科手术患者的VTE 预防)点击下载全文16、Perioperative Management of Antithrombotic Therapy (围手术期的抗栓治疗管理)点击下载全文17 、Diagnosis of DVT (深静脉血栓形成的诊断)点击下载全文18、Antithrombotic Therapy for VTE Disease (静脉血栓栓塞性疾病的抗栓治疗)点击下载全文19、Treatment and Prevention of Heparin-Induced Thrombocytopenia(肝素诱导的血小板减少症的治疗与预防)点击下载全文20、Antithrombotic Therapy for AtrialFibrillation(房颤的抗栓治疗)点击下载全文21、Antithrombotic and Thrombolytic Therapy for Valvular Disease(心瓣膜病的抗栓和溶栓治疗)点击下载全文22、Antithrombotic and Thrombolytic Therapy for Ischemic Stroke(缺血性卒中的抗栓和溶栓治疗)点击下载全文23、Primary and Secondary Prevention of Cardiovascular Disease(心血管疾病的一级和二级预防)点击下载全文24 、Antithrombotic Therapy in Peripheral Artery Disease(周围动脉疾病的抗栓治疗)点击下载全文25、VTE, Thrombophilia, Antithrombotic Therapy, andPregnancy(静脉血栓栓塞、血栓形成倾向、抗栓治疗与妊娠)点击下载全文26 、Antithrombotic Therapy in Neonates and Children(新生儿和儿童的抗栓治疗)点击下载全文更多内容请点击:DVT 病因新指南:经济舱综合征缺乏证据ACCP 新指南:并非所有患者适用DVT 预防另外,非常感谢fxjj 医友为大家提供该指南的部分内容,期待在大家共同努力下,能在该频道分享到更多更新的指南温馨提示:由于该指南的内容较为丰富,文档较多(共26 个文档),所以,完整指南内容包括了附件中的 3 个压缩包和2 个pdf 文档。

DOI 10.1378/chest.1412S3 2012;141;7S-47S ChestPhysicians Antithrombotic Therapy and Prevention of Thrombosis Panel Holger J. Schuünemann and for the American College of ChestGordon H. Guyatt, Elie A. Akl, Mark Crowther, David D. Gutterman,Evidence-Based Clinical Practice Guidelinesed: American College of Chest Physicians Therapy and Prevention of Thrombosis, 9th Executive Summary : Antithrombotic/content/141/2_suppl/7S.full.html services can be found online on the World Wide Web at:The online version of this article, along with updated information and7S.DC1.html/content/suppl/2012/02/06/141.2_suppl.Supplemental material related to this article is available at:ISSN:0012-3692)/site/misc/reprints.xhtml (written permission of the copyright holder.this article or PDF may be reproduced or distributed without the prior Dundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright2012by the American College of Chest Physicians, 3300Physicians. It has been published monthly since 1935.is the official journal of the American College of Chest ChestCHEST / 141 / 2 / FEBRUARY , 2012 SUPPLEMENT 7ST he eighth iteration of the American College of Chest Physicians Antithrombotic Guidelines pre-sented, in a paper version, a narrative evidence sum-mary and rationale for the recommendations, a small number of evidence profi les summarizing bodies ofevidence, and some articles with quite extensivesummary tables of primary studies. In total, this represented 600 recommendations summarized in 968 pages of text. Many readers responded that the result was too voluminous for their liking or prac-tical use. C ognizant of this feedback, we worked hard to minimize the length of the text for the ninth iteration of the guidelines Antithrombotic Therapy and Pre-vention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (AT9) without sacrifi cing key content. A number of topic editors found our shortening edits draconian, but we were determined to produce the leanest product possible.T here were, however, a number of obstacles. In what we believe is a key advance in AT9, we con-ducted a systematic review of what is known about patients’ values and preferences regarding antithrom-botic therapy and included the results as an article in AT9. In another forward step, we recognized the problems with asymptomatic thrombosis as a surro-gate outcome, and devised strategies to estimate reductions in symptomatic DVT and pulmonary embolism with antithrombotic prophylaxis. We felt it important to explain this innovation to users of AT9, and this meant another article. W e included, for the fi rst time, an article on diag-nosis addressing patients with symptoms and signs suggesting DVT. We increased the range of interven-tions we have covered, resulting in additional recom-mendations. Finally, we produced many summary of fi ndings tables, which offer extremely succinct and informative presentations of best estimates of effect and the confi dence associated with those estimates.I f published in the same fashion as the Antithrom-botic and Thrombolytic Therapy, 8th ed: AmericanA bbreviations:ACS 5 acute coronary syndrome; AF 5 atrialfi brillation; AIS 5 arterial ischemic stroke; APLA 5antiphospolipidantibodies; ASA 5 acetylsalicylic acid; AT9 5 Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines; BMS 5 bare-metal stent; CABG 5 coronary artery bypass graft; CAD 5coronary artery disease; CDT 5catheter-directed thrombosis; CHADS 2 5 congestive heart failure, hyperten-sion, age Ն 75 years, diabetes mellitus, prior stroke or transient ischemic attack; CSVT 5 cerebral sinovenous thrombosis; CTPH 5 chronic thromboembolic pulmonary hypertension; CUS 5 com-pression ultrasound; CVAD 5 central venous access device; DES 5 d rug-eluting stent; GCS 5 g raduated compression stockings; H FS 5 hip fracture surgery; HIT 5 heparin-induced thrombocy-topenia; HITT 5 heparin-induced thrombocytopenia complicated by thrombosis; IA 5 intraarterial; ICH 5intracerebral hemor-rhage; IE 5 infective endocarditis; INR 5 international normalized ratio; IPC 5 intermittent pneumatic compression; IPCD 5 inter-mittent pneumatic compression device; IVC 5 inferior vena cava; LDUH 5 low-dose unfractionated heparin; LMWH 5 low-molecular-weight heparin; LV 5 left ventricular; MBTS 5 modifi ed Blalock-Taussig shunt; MR 5 magnetic resonance; PAD 5peripheral artery disease; PCI 5 percutaneous coronary inter v ention; PE 5 pul-monary embolism; PFO 5 patent foramen ovale; PMBV 5 p ercuta-neous mitral balloon valvotomy; PTS 5postthrombotic syndrome; PVT 5 prosthetic valve thrombosis; r-tPA 5 recombinant tissue plas-minogen activator; RVT 5 renal vein thrombosis; SC 5 subcuta-neous; TEE 5 transesophageal echocardiography; THA 5 total hip arthroplasty; TIA 5 transient ischemic attack; TKA 5 total knee arthroplasty; UAC 5umbilical arterial catheter; UEDVT 5 upper-extremity DVT; UFH 5 unfractionated heparin; US 5 ultrasound; UVC 5 umbilical venous catheter; VAD 5 ventricular assist device; VKA 5 vitamin K antagonistAntithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice GuidelinesG ordon H. G uyatt ,M D, FCCP ;E lie A. A kl ,M D, PhD, M PH ;M ark C rowther ,M D ;D avid D. G utterman ,M D, FCCP ;H olger J. S chü n emann ,M D, PhD, FCCP ;f or the American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Panel *CHEST 2012; 141(2)(Suppl):7S–47S8SExecutive Summarytables) and some tables summarizing the methodsand results, and the risk of bias, associated with the individual studies that contributed to the evidence profi les and summary of fi ndings tables.T he world of medical information is rapidly becom-ing a world of electronic storage and presentation of primary studies, recommendations, and a wide variety of other information of interest to health care prac t itioners. Although our abbreviated paper copy presentation represents a necessary response to a challenging situation, it is also a harbinger of the increasingly electronic world of medical information into which future editions of guidelines are destined to move.S ummary of Recommendations Note on Shaded Text: Throughout this guideline, shading is used within the summary of recommenda-tions sections to indicate recommendations that are newly added or have been changed since the publica-tion of Antithrombotic and Thrombolytic Therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Rec-ommendations that remain unchanged are not shaded.E vidence-Based Management of Anticoagulant TherapyF or further details, see Holbrook et al. 1 2.1 Loading Dose for Initiation of Vitamin K Antagonist(VKA) Therapy2.1. For patients suffi ciently healthy to be treated as outpatients, we suggest initiating VKA therapy with warfarin 10 mg daily for the fi rst 2 days followed by dosing based on international normalized ratio (INR) measurements rather than starting with the estimated maintenance dose (Grade 2C) .2.2 Initial Dose Selection and Pharmacogenetic Testing2.2. For patients initiating VKA therapy, we recommend against the routine use of pharma-cogenetic testing for guiding doses of VKA (Grade 1B) . 2.3 Initiation Overlap for Heparin and VKA2.3. For patients with acute VTE, we suggest that VKA therapy be started on day 1 or 2 of low-molecular-weight heparin (LMWH) or low-dose unfractionated heparin (UFH) therapy rather than waiting for several days to start (Grade 2C) .College of Chest Physicians Antithrombotic Guide-lines, this would have resulted in a document with . 850 pages of paper text, an unacceptable length. Given this and with the advice of the journal, we decided to adopt a highly focused print version that includes only this executive summary and the following articles:• An introduction describing the major innovations in AT9 • A methods article explaining how we devel-oped the guidelines (a potential model for other guideline groups interested in optimal rigor) • Recommendations and grading from each arti-cle embedded in the table of contents of each article T hose seeking the rationale for the recommenda-tions, including the supporting evidence, should access the online version of the guideline ( h ttp:///content/141/2_suppl )that includes a narrative summaries and support-ing summary of fi ndings tables. The numbering indi-cated beside the recommendations in this summary is aligned with the sections and tables found in the full articles. Those interested in a deeper under-standing of the evidence can turn to online data supplements for each of the articles that include rec-ommendations. There, they will fi nd evidence pro-fi les (expanded versions of the summary of fi ndingsR evision accepted August 31, 2011. A ffi liations: From the Department of Clinical Epidemiology and Biostatistics (Drs Guyatt, Akl, and Schü n emann) and Depart-ment of Medicine (Drs Guyatt, Crowther, and Schü n emann), McMaster University Faculty of H ealth Sciences, H amilton, ON, Canada; Departments of Medicine and Family Medicine (Dr Akl), State University of New York, Buffalo, NY; Cardiovascular Research Center (Dr Gutterman), Medical College of Wisconsin, Milwaukee, WI.*For complete panel list, see: /content/141/2_suppl/2S F unding/Support : The Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines received support from the National Heart, Lung, and Blood Institute [R13 HL104758] and Bayer Schering Pharma AG. Support in the form of educa-tional grants were also provided by Bristol-Myers Squibb; Pfi zer, Inc; Canyon Pharmaceuticals; and sanofi -aventis US.D isclaimer: American College of Chest Physician guidelines are intended for general information only, are not medical advice, and do not replace professional medical care and physician advice, which always should be sought for any medical condition. The complete disclaimer for this guideline can be accessed at /content/141/2_suppl/1SC orrespondence to: Gordon H . Guyatt, MD, FCCP , Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, ON, L8N 3Z5, Canada; e-mail: guyatt@mcmaster.ca© 2012 American College of Chest Physicians.Reproduction of this article is prohibited without written permission from the American College of Chest Physicians ( h ttp:///site/misc/reprints.xhtml ).D OI: 10.1378/chest.1412S3CHEST / 141 / 2 / FEBRUARY , 2012 SUPPLEMENT 9S3.8 VKA Drug Interactions to Avoid3.8. For patients taking VKAs, we suggest avoid-ing concomitant treatment with nonsteroidal antiinfl ammatory drugs, including cyclooxyge-nase-2-selective nonsteroidal antiinfl ammatory drugs, and certain antibiotics (see Table 8 in mainarticle1 ) (Grade 2C) .F or patients taking VKAs, we suggest avoiding concomitant treatment with antiplatelet agents except in situations where benefi t is known or is highly likely to be greater than harm from bleeding, such as patients with mechanical valves, patients with acute coronary syndrome, or patients with recent coronary stents or bypass surgery (Grade 2C) .4.1 Optimal Therapeutic INR Range4.1. For patients treated with VKAs, we recom-mend a therapeutic INR range of 2.0 to 3.0 (tar-get INR of 2.5) rather than a lower (INR , 2) or higher (INR 3.0-5.0) range (Grade 1B) . 4.2 Therapeutic Range for High-Risk Groups 4.2. For patients with antiphospholipid syn d rome with previous arterial or venous thromboembolism, we suggest VKA therapy titrated to a moderate-intensity INR range (INR 2.0-3.0) rather than higher intensity (INR 3.0-4.5) (Grade 2B). 5.0 Discontinuation of Therapy5.0. For patients eligible to discontinue treat-ment with VKA, we suggest abrupt discontinua-tion rather than gradual tapering of the dose to discontinuation (Grade 2C) .6.1 Unfractionated Heparin (UFH) Dose Adjustment by Weight6.1. For patients starting IV UFH, we suggest that the initial bolus and the initial rate of the continuous infusion be weight adjusted (bolus 80 units/kg followed by 18 units/kg per h for VTE; bolus 70 units/kg followed by 15 units/kg per h for cardiac or stroke patients) or use of a fi xed dose (bolus 5,000 units followed by 1,000 units/h) rather than alternative regimens (Grade 2C) . 6.2 Dose Management of Subcutaneous (SC) UFH6.2. For outpatients with VTE treated with SC UFH, we suggest weight-adjusted dosing (fi rst dose 333 units/kg, then 250 units/kg) with-out monitoring rather than fi xed or weight-adjusted dosing with monitoring (Grade 2C) .3.1 Monitoring Frequency for VKAs3.1. For patients taking VKA therapy with con-sistently stable INRs, we suggest an INR testing frequency of up to 12 weeks rather than every 4 weeks (Grade 2B) .3.2 Management of the Single Out-of-Range INR3.2. For patients taking VKAs with previously stable therapeutic INRs who present with a single out-of-range INR of Յ 0.5 below or above therapeutic, we suggest continuing the current dose and testing the INR within 1 to 2 weeks (Grade 2C) .3.3 Bridging for Low INRs3.3. For patients with stable therapeutic INRs presenting with a single subtherapeutic INR value, we suggest against routinely adminis-tering bridging with heparin (Grade 2C) . 3.4 Vitamin K Supplementation3.4. For patients taking VKAs, we suggest against routine use of vitamin K supplementa-tion (Grade 2C) .3.5 Anticoagulation Management Services for VKAs 3.5. (Best Practices Statement) We suggest that health-care providers who manage oral antico-agulation therapy should do so in a systematic and coordinated fashion, incorporating patient education, systematic INR testing, tracking, follow-up, and good patient communication of results and dosing decisions.3.6 Patient Self-Testing and Self-Management3.6. For patients treated with VKAs who are motivated and can demonstrate competency in self-management strategies, including the self-testing equipment, we suggest patient self-management rather than usual outpatient INR monitoring (Grade 2B) . For all other patients, we suggest monitoring that includes the safe-guards in our best practice statement 3.5. 3.7 Dosing Decision Support3.7. For dosing decisions during maintenance VKA therapy, we suggest using validated deci-sion support tools (paper nomograms or com-puterized dosing programs) rather than no decision support (Grade 2C) .Remarks: Inexperienced prescribers may be more likely to improve prescribing with use of decision sup-port tools than experienced prescribers.10SExecutive Summaryunfractionated heparin (L DUH) bid, LDUHtid, or fondaparinux (Grade 1B) .R emarks: In choosing the specifi c anticoagulant drug to be used for pharmacoprophylaxis, choices should be based on patient preference, compliance, and ease of administration (eg, daily vs bid vs tid dosing), as well as on local factors affecting acquisition costs (eg, prices of various pharmacologic agents in individual hospital formularies).2.4. For acutely ill hospitalized medical patients at low risk of thrombosis, we recommend against the use of pharmacologic prophylaxis or mechan-ical prophylaxis (Grade 1B) .2.7.1. For acutely ill hospitalized medical patients who are bleeding or at high risk for bleeding, we recommend against anticoagulant thromboprophylaxis (Grade 1B) .2.7.2. For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleeding or at high risk for major bleeding, we suggest the optimal use of mechanical thromboprophylaxis with graduated compression stockings (GCS) (Grade 2C) or intermittent pneumatic compres-sion (IPC) (Grade 2C) , rather than no mechan-ical thromboprophylaxis. When bleeding risk decreases, and if VTE risk persists, we sug-gest that pharmacologic thromboprophylaxis be substituted for mechanical thromboprophy-laxis (Grade 2B) .R emarks: Patients who are particularly averse to the potential for skin complications, cost, and need for clinical monitoring of GCS and IPC use are likely to decline mechanical prophylaxis.2.8. In acutely ill hospitalized medical patients who receive an initial course of thrombopro-phylaxis, we suggest against extending the dura-tion of thromboprophylaxis beyond the period of patient immobilization or acute hospital stay (Grade 2B) .3.0 Critically Ill Patients3.2. In critically ill patients, we suggest against routine ultrasound screening for DVT (Grade 2C) .3.4.3. For critically ill patients, we suggest using LMWH or LDUH thromboprophylaxis over no prophylaxis (Grade 2C) .3.4.4. For critically ill patients who are bleeding, or are at high risk for major bleeding, we suggest mechanical thromboprophylaxis with GCS (Grade 2C) o r IPC (Grade 2C) u ntil the7.1 Therapeutic Dose of LM WH in Patients With Decreased Renal Function7.1. For patients receiving therapeutic LMWH who have severe renal insuffi ciency (calculated creatinine clearance , 30 mL/min), we suggest a reduction of the dose rather than using stan-dard doses (Grade 2C) .8.1 Fondaparinux Dose Management by Weight8.1. For patients with VTE and body weight over 100 kg, we suggest that the treatment dose of fondaparinux be increased from the usual 7.5 mg to 10 mg daily SC (Grade 2C) .9.1 Vitamin K for Patients Taking VKAs With High INRs Without Bleeding9.1.(a) For patients taking VKAs with INRs between 4.5 and 10 and with no evidence of bleeding, we suggest against the routine use of vitamin K (Grade 2B) .(b) For patients taking VKAs with INRs . 10.0 and with no evidence of bleeding, we suggest that oral vitamin K be administered (Grade 2C) . 9.2 Clinical Prediction Rules for Bleeding While Taking VKA9.2. For patients initiating VKA therapy, we suggest against the routine use of clinical pre-diction rules for bleeding as the sole criterion to withhold VKA therapy (Grade 2C) .9.3 Treatment of Anticoagulant-Related Bleeding9.3. For patients with VKA-associated major bleeding, we suggest rapid reversal of antico-agulation with four-factor prothrombin complex concentrate rather than with plasma. (Grade 2C) .W e suggest the additional use of vitamin K 5 to 10 mg administered by slow IV injection rather than reversal with coagulation factors alone (Grade 2C) .P revention of VTE in Nonsurgical PatientsF or further details, see Kahn et al. 2 2.0 Hospitalized Acutely Ill Medical Patients2.3. For acutely ill hospitalized medical patients at increased risk of thrombosis, we recom m end anticoagulant thromboprophylaxis with low-molecular-weight heparin [LMWH], low-doseCHEST / 141 / 2 / FEBRUARY , 2012 SUPPLEMENT 11Sknee GCS providing 15 to 30 mm Hg of pressureat the ankle during travel (Grade 2C) . F or all other long-distance travelers, we suggest against the use of GCS (Grade 2C) .6.1.3. For long-distance travelers, we suggest against the use of aspirin or anticoagulants to prevent VTE (Grade 2C) .7.0 Persons With Asymptomatic Thrombophilia7.1. In persons with asymptomatic thrombo-philia (ie, without a previous history of VTE), we recommend against the long-term daily use of mechanical or pharmacologic thrombopro-phylaxis to prevent VTE (Grade 1C) .P revention of VTE in Nonorthopedic Surgical PatientsF or further details, see Gould et al. 3 3.6 Patients Undergoing General, GI, Urological,Gynecologic, Bariatric, Vascular, Plastic, or Recon-structive Surgery3.6.1. For general and abdominal-pelvic sur-gery patients at very low risk for VTE ( , 0.5%; Rogers score, , 7; Caprini score, 0), we recom-mend that no specifi c pharmacologic (Grade 1B) o r mechanical (Grade 2C) p rophylaxis be used other than early ambulation.3.6.2. For general and abdominal-pelvic sur-gery patients at low risk for VTE ( ف 1.5%; Rog-ers score, 7-10; Caprini score, 1-2), we suggest mechanical prophylaxis, preferably with inter-mittent pneumatic compression (IPC), over no prophylaxis (Grade 2C) .3.6.3. For general and abdominal-pelvic sur-gery patients at moderate risk for VTE ( ف 3.0%; Rogers score, . 10; Caprini score, 3-4) who are not at high risk for major bleeding complica-tions, we suggest L MWH (Grade 2B ), L DUH (Grade 2B) , o r mechanical prophylaxis, prefer-ably with IPC (Grade 2C) ,o ver no prophylaxis. R emarks: T hree of the seven authors favored a strong (Grade 1B) recommendation in favor of LMWH or LDUH over no prophylaxis in this group.3.6.4. For general and abdominal-pelvic sur-gery patients at moderate risk for VTE (3.0%; Rogers score, . 10; Caprini score, 3-4) who are at high risk for major bleeding complications or those in whom the consequences of bleed-ing are thought to be particularly severe, webleeding risk decreases, rather than no mechan-ical thromboprophylaxis. When bleeding risk decreases, we suggest that pharmacologic throm-boprophylaxis be substituted for mechanical thromboprophylaxis (Grade 2C) . 4.0 Patients With Cancer in the Outpatient Setting4.2.1. In outpatients with cancer who have no additional risk factors for VTE, we suggest against routine prophylaxis with L MWH or LDUH (Grade 2B) and recommend against the prophylactic use of VKAs (Grade 1B) .R emarks: Additional risk factors for venous throm-bosis in cancer outpatients include previous venous thrombosis, immobilization, hormonal therapy, angio-genesis inhibitors, thalidomide, and lenalidomide.4.2.2. In outpatients with solid tumors who have additional risk factors for VTE and who are at low risk of bleeding, we suggest prophylactic-dose L MWH or L DUH over no prophylaxis (Grade 2B) .R emarks: Additional risk factors for venous thrombo-sis in cancer outpatients include previous venous thrombosis, immobilization, hormonal therapy, angio-genesis inhibitors, thalidomide, and lenali d omide.4.4. In outpatients with cancer and indwelling central venous catheters, we suggest againstroutine prophylaxis with L MWH or L DUH (Grade 2B) and suggest against the prophylactic use of VKAs (Grade 2C) .5.0 Chronically Immobilized Patients5.1. In chronically immobilized persons residing at home or at a nursing home, we suggest against the routine use of thromboprophylaxis (Grade 2C) .6.0 Persons Traveling Long-Distance6.1.1. For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery or trauma, active malignancy, preg-nancy, estrogen use, advanced age, limited mobility, severe obesity, or known thrombo-philic disorder), we suggest frequent ambula-tion, calf muscle exercise, or sitting in an aisle seat if feasible (Grade 2C) .6.1.2. For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery or trauma, active malignancy, pregnancy, estrogen use, advanced age, limited mobility, severe obesity, or known thrombophilic disor-der), we suggest use of properly fi tted, below-12SExecutive Summarygest use of mechanical prophylaxis, preferably with optimally applied IPC, over either no pro-phylaxis (Grade 2C) o r pharmacologic prophy-laxis (Grade 2C) .4.4.2. For cardiac surgery patients whose hos-pital course is prolonged by one or more non-hemorrhagic surgical complications, we suggest adding pharmacologic prophylaxis with LDUH or LMWH to mechanical prophylaxis (Grade 2C) .5.0 Patients Undergoing Thoracic Surgery5.4.1. For thoracic surgery patients at mod-erate risk for VTE who are not at high risk for perioperative bleeding, we suggest L DUH (Grade 2B) , L MWH (Grade 2B) , o r mechanical prophylaxis with optimally applied IPC (Grade 2C)o ver no prophylaxis. R emarks: T hree of the seven authors favored a strong (Grade 1B) recommendation in favor of LMWH or LDUH over no prophylaxis in this group.5.4.2. For thoracic surgery patients at high risk for VTE who are not at high risk for periopera-tive bleeding, we suggest LDUH (Grade 1B) o r LMWH (Grade 1B) o ver no prophylaxis. In addi-tion, we suggest that mechanical prophylaxis with elastic stockings or IPC should be added to pharmacologic prophylaxis (Grade 2C) .5.4.3. For thoracic surgery patients who are at high risk for major bleeding, we suggest use of mechanical prophylaxis, preferably with opti-mally applied IPC, over no prophylaxis until the risk of bleeding diminishes and pharmacologic prophylaxis may be initiated (Grade 2C) .6.0 Patients Undergoing Craniotomy6.4.1. For craniotomy patients, we suggest that mechanical prophylaxis, preferably with IPC, be used over no prophylaxis (Grade 2C) o r phar-macologic prophylaxis (Grade 2C) .6.4.2. For craniotomy patients at very high risk for VTE (eg, those undergoing craniotomy for malignant disease), we suggest adding pharma-cologic prophylaxis to mechanical prophylaxis once adequate hemostasis is established and the risk of bleeding decreases (Grade 2C) .7.0 Patients Undergoing Spinal Surgery7.4.1. For patients undergoing spinal surgery, we suggest mechanical prophylaxis, prefer-ably with IPC, over no prophylaxis (Grade 2C) , u nfractionated heparin (Grade 2C) , o r LMWH (Grade 2C) .suggest mechanical prophylaxis, preferably with IPC, over no prophylaxis (Grade 2C) .3.6.5. For general and abdominal-pelvic sur-gery patients at high risk for VTE ( ف 6.0%; Caprini score, Ն 5) who are not at high risk for major bleeding complications, we recommend pharmacologic prophylaxis with LMWH (Grade 1B) o r L DUH (Grade 1B) o ver no prophylaxis. We suggest that mechanical prophylaxis with elastic stockings or IPC should be added to phar-macologic prophylaxis (Grade 2C) .3.6.6. For high-VTE-risk patients undergoing abdominal or pelvic surgery for cancer who are not otherwise at high risk for major bleeding complications, we recommend extended-duration pharmacologic prophylaxis (4 weeks) with LMWH over limited-duration prophylaxis (Grade 1B) .R emarks: Patients who place a high value on mini-mizing out-of-pocket health-care costs might prefer limited-duration over extended-duration prophylaxis in settings where the cost of extended-duration pro-phylaxis is borne by the patient.3.6.7. For high-VTE-risk general and abdominal-pelvic surgery patients who are at high risk for major bleeding complications or those in whom the consequences of bleeding are thought to be particularly severe, we suggest use of mechan-ical prophylaxis, preferably with IPC, over no prophylaxis until the risk of bleeding diminishes and pharmacologic prophylaxis may be initiated (Grade 2C) .3.6.8. For general and abdominal-pelvic sur-gery patients at high risk for VTE (6%; Caprini score, Ն 5) in whom both L MWH and unfrac-tionated heparin are contraindicated or unavail-able and who are not at high risk for major bleeding complications, we suggest low-dose aspirin (Grade 2C) , f ondaparinux (Grade 2C) , o r mechanical prophylaxis, preferably with IPC (Grade 2C) ,o ver no prophylaxis.3.6.9. For general and abdominal-pelvic sur-gery patients, we suggest that an inferior vena cava (IVC) fi lter should not be used for primary VTE prevention (Grade 2C) .3.6.10. For general and abdominal-pelvic surgery patients, we suggest that periodic surveillance with venous compression ultrasound should not be performed (Grade 2C) .4.0 Patients Undergoing Cardiac Surgery4.4.1. For cardiac surgery patients with an uncomplicated postoperative course, we sug-CHEST / 141 / 2 / FEBRUARY , 2012 SUPPLEMENT 13Sigatran, rivaroxaban, low-dose unfractionatedheparin (LDUH), adjusted-dose VKA, aspirin (all Grade 1B) , or an intermittent pneumatic com-pression device (IPCD) (Grade 1C) .R emarks: We recommend the use of only portable, battery-powered IPCDs capable of recording and reporting proper wear time on a daily basis for inpa-tients and outpatients. Efforts should be made to achieve 18 h of daily compliance. One panel member believed strongly that aspirin alone should not be included as an option.2.1.2. In patients undergoing HFS, we recom-mend use of one of the following rather than no antithrombotic prophylaxis for a minimum of 10 to 14 days: L MWH, fondaparinux, L DUH, adjusted-dose VKA, aspirin (all Grade 1B) , or an IPCD (Grade 1C) .R emarks: We recommend the use of only portable, battery-powered IPCDs capable of recording and reporting proper wear time on a daily basis for inpa-tients and outpatients. Efforts should be made to achieve 18 h of daily compliance. One panel member believed strongly that aspirin alone should not be included as an option.2.2. For patients undergoing major orthopedic surgery (THA, TKA, HFS) and receiving LMWH as thromboprophylaxis, we recommend starting either 12 h or more preoperatively or 12 h or more postoperatively rather than within 4 h or less pre-operatively or 4 h or less postoperatively (Grade 1B) .2.3.1. In patients undergoing THA or TKA, irrespective of the concomitant use of an IPCD or length of treatment, we suggest the use of L MWH in preference to the other agents we have recommended as alternatives: fonda-parinux, apixaban, dabigatran, rivaroxaban, LDUH (all Grade 2B) , adjusted-dose VKA, or aspirin (all Grade 2C) .R emarks: If started preoperatively, we suggest admin-istering LMWH Ն 12 h before surgery. Patients who place a high value on avoiding the inconvenience of daily injections with LMWH and a low value on the limitations of alternative agents are likely to choose an alternative agent. Limitations of alter-native agents include the possibility of increased bleeding (which may occur with fondaparinux, rivar-oxaban, and VKA), possible decreased effi cacy (LDUH, VKA, aspirin, and IPCD alone), and lack of long-term safety data (apixaban, dabigatran, and rivaroxaban). Furthermore, patients who place a high value on avoiding bleeding complications and a low value on7.4.2. For patients undergoing spinal surgery at high risk for VTE (including those with malig-nant disease or those undergoing surgery with a combined anterior-posterior approach), we suggest adding pharmacologic prophylaxis to mechanical prophylaxis once adequate hemo-stasis is established and the risk of bleeding decreases (Grade 2C) . 8.0 Patients With Major Trauma: Traumatic Brain Injury, Acute Spinal Injury, and Traumatic Spine Injury8.4.1. For major trauma patients, we suggest use of LDUH (Grade 2C) , L MWH (Grade 2C) , o r mechanical prophylaxis, preferably with IPC (Grade 2C) ,o ver no prophylaxis.8.4.2. For major trauma patients at high risk for VTE (including those with acute spinal cord injury, traumatic brain injury, and spinal sur-gery for trauma), we suggest adding mechan-ical prophylaxis to pharmacologic prophylaxis (Grade 2C) w hen not contraindicated by lower-extremity injury.8.4.3. For major trauma patients in whom LMWH and LDUH are contraindicated, we sug-gest mechanical prophylaxis, preferably with IPC, over no prophylaxis (Grade 2C) w hen not contraindicated by lower-extremity injury. We suggest adding pharmacologic prophylaxis with either L MWH or L DUH when the risk of bleeding diminishes or the contraindication to heparin resolves (Grade 2C) .8.4.4. For major trauma patients, we suggest that an IVC fi lter should not be used for pri-mary VTE prevention (Grade 2C) .8.4.5. For major trauma patients, we suggest that periodic surveillance with venous compression ultrasound should not be performed (Grade 2C) .P revention of VTE in Orthopedic Surgery PatientsF or further details, see Falck-Ytter et al. 4 2.0 Patients Undergoing Major Orthopedic Surgery: Total Hip Arthroplasty (THA), Total Knee Arthroplasty (TKA), Hip Fracture Surgery (HFS)2.1.1. In patients undergoing THA or TKA, we recommend use of one of the following for a minimum of 10 to 14 days rather than no anti-thrombotic prophylaxis: low-molecular-weight heparin (LMWH), fondaparinux, apixaban, dab-。