奥瑞那说明书
- 格式:pdf
- 大小:6.49 MB
- 文档页数:12

Ordering Information Cat. No. Product ***********MagNA Lyser Instrument (230 Volt)***********MagNA Lyser Instrument (110 Volt)(Instruments supplied with rotor and rotor cooling block)***********MagNA Lyser Green Beads (100 tubes)Related Products Cat. No. Product***********MagNA Pure LC DNA Isolation Kit II (Tissue)***********MagNA Pure LC mRNA Isolation Kit II (Tissue)03 330 591 001MagNA Pure LC RNA Isolation Kit III (Tissue)***********MagNA Pure LC DNA Isolation Kit III (Bacteria, Fungi)***********MagNA Pure LC RNA Isolation Tissue Lysis Buffer – Refill (70 ml)System DescriptionHomogenize up to 16 samples in just a few seconds.Save valuable lab space with a small benchtop instrument.Reduce hands-on time by replacing the mortar and pestle and other manual methods.Integrate your workflow with the automated nucleic acid isolation of the MagNA Pure LC Instrument.Perform consistent and reproducible sample disruption.Process many different sample types.Prevent nucleic acid degradation with the benchtop cooling unit.Ease your setup with a removable rotor and prefilled disposable vials.Automate with an easy-to-use instrumentVersatile, efficient, and rapid pre-preparationFigure 71. Add your sample and lysis buffer to the MagNA Lyser Green Beads.2. Homogenize with the MagNA Lyser Instrument.3. Centrifuge to pellet the debris.4. Proceeed with the supernatant to prepare nucleic acids or proteins.For detailed information,visit or contact your local representative.Trademarks:MagNA Pure, MagNA Lyser, LightCycler, and the MagNA Pure Logo are trademarks of a member of the Roche Group.The technology used for the LightCycler System is licensed from Idaho Technology Inc., Salt Lake City, UT, USA.Fully automated sample preparationon the PCR Workflow SystemRoche Diagnostics GmbH Roche Applied Science Nonnenwald 282372 Penzberg Germany0000Roche Applied Science Part of Roche DiagnosticsMagNA Lyser InstrumentStart the Ball Rollingwith Automated Tissue HomogenizationᕤᕣᕢᕡFigure 6Components of the system.The MagNA Lyser InstrumentAutomated tissue homogenizationProcessing conditionsRefer to the following tables for guidelines on setting up your homogenizationSample material(10 mg)*Time settings(seconds)Cooling(between the runs)Speed Average yield(µg)***Average purity(OD 280/260 nm)***Spleen 2 x 25 906,00030–40 1.9Liver 25-6,00016–18 1.8Lung 2 x 25906,00025 1.8Kidney25-6,000201.8Maize leaves **20-5,00010n.d.Maize polenta **20-5,0008n.d.Tortilla chips **20-5,0001n.d.*Aliqout containing 10 mg sample material (here mouse and food samples) was taken for the DNA purificationusing the MagNA Pure LC DNA Isolation Kit II (Tissue), (see pack insert)**Centrifugation after the homogenization for 5 minutes at 2,200 x g*** Yield and purity strongly depend on the condition of the sample material n.d.not determinedData kindly provided by Dr. Peterhänsel, RWTH Aachen, GermanyFigure 1Gel electrophoresis from genomic DNA isolated from tissue homogenized with the MagNA LyserInstrument, using the MagNA Pure LC DNA Kit II (Tissue).Marker: DNA Marker III*Aliquot containing 10 mg sample material (here mouse and human research samples) was taken to purify RNAeither with the MagNA Pure LC RNA Isolation Kit III (Tissue) or the MagNA Pure LC mRNA Isolation Kit II (Tissue) homogenized with the MagNA Lyser Instrument.** Yield and purity strongly depend on the condition of the sample material. The yield for mRNA was not determined.Sample material(10 mg)*Time settings(cycles/seconds)Cooling(between/afterthe runs in seconds)SpeedAverage yield (mg)(total RNA)**Average purity(OD 280/260 nm)**RNA/mRNARarely expressed targets in small numbers of target cells,as seen in experiments about minimalresidual diseases,are difficult to detect.Increasing the cell number can improve sensitivity and lead to accurate results.Without the MagNA Lyser pre-processing,the MagNA Pure mRNA HS Kit can efficiently obtain mRNA from a maximum of 1 x 107white blood cells (WBCs),as shown in research studies with human samples.However,using greater cell numbers results in a saturation effect with quantitative assays (Figure 3).Homogenization of the lysate with the MagNA Lyser Instrument prior to the purification eliminatesthe amplification saturation at 1 x 107cells and allows the use of up to 2.5 x 107WBCs (Figure 4 and 5),enhancing the analytical sensitivity of the assay.Eliminate sensitivity barriers with increased sample inputFigure 3mRNA was purified from different amounts of human white blood cells with the MagNA Pure mRNA HS Kit. G6PDH was amplified using the LightCycler t(9;22) Quantification Kit (see text beside).Figure 4mRNA was purified from different amounts of human white blood cells with the MagNA Pure mRNA HS Kit. The lysates from 2.5 x 107cells and 5 x 107cells were homogenized with the MagNA Lyser Instrument (2x50 seconds with 90 seconds cooling in between) prior to the mRNA purification. G6PDH was amplified using the LightCycler t(9;22) Quantification Kit (see text beside).Figure 5Scalability from 1 x 106cells to 2.5 x 107cells is represented in the graph and the table of the relationship between crossing points and cell numbers. The limitation of cell input is indicated by no change in crossing point with increased cell number (see text beside).Cell number 5 x 1072.5 x 1071 x 1075 x 1061 x 106Log (cell number)7.77.47.06.76.0Crossing point 20.320.321.822.424.4crossingpointLog(cell number)252423222120195.86.36.87.37.8Figure 2Gel electrophoresis from total RNA isolated from tissue homogenized with the MagNA Lyser Instrument, using the MagNA Pure LC RNA Kit III (Tissue).Ma r k e rS p l e e nL i v e rL u n gK i d n e yM a r k e rMa i z e l e a v e sMa i z e l e a v e sS p l e e nL i v e r11 kb5 kb5 kb28 S rRNA 18 S rRNASpleen 2 x 50 90 6,500–7,000 30–40 1.9Liver 50 - 6,500–7,000 13–17 2.0Thymoid tissue60906,500n.d.n.d.Heart 60 90 6,500 n.d. n.d.Abdominal fat 60 90 6,500 n.d. n.d.Aorta 60 90 6,500 n.d. n.d. Other samples1+n x 50 90 6,500–7,000- -1 x 105 x 101 x 10- 5 x 101 x 105 x 105 x 10- 5 x 102.5 x 10 5 x 10。

ORENA火灾报警及消防联动控制系统产品设计应用手册彩页:产品技术特点和优势控制器大容量,全系列控制器单机容量从64点、128点、192点、384点、768点、1536点、2304点……直至11520点,可多台控制器联网通讯,完全满足各种工程的需要,具有较高的性能价格比。
双向分布智能回路器件(探测器、模块、手报按钮)采用MCU微处理器,具有独立的智能分析和判断能力,内含智能软件,可根据现场环境的变化(温度、湿度、灰尘污染)自动调整报警阈值、滤除干扰,并与控制器双向传输信息,大大降低了误报率,加快了报警响应时间,最大限度地保证了报警的准确性。
真正的全总线系统结构系统内所有的各种探测器、模块、报警按钮、楼层火灾显示盘、回路扩展单元等外部设备全部挂接在总线上,不需额外的信号线。
系统结构简洁,节省大量线材和布线工时。
数字化信号传输二总线电流量脉宽数字化信号传输技术,通讯可靠,抗干扰性能强。
先进的自动编址功能无需人工设定地址,所有外部设备在线自动识别,自动编址,节省大量安装调试时间,提高了可靠性。
安装调试简便无极性两总线,避免了由于接线不当而引起的系统损坏。
可T形/环形任意布线,任意分支,节省大量线材和布线工时。
控制器上可显示回路器件的供电电压,方便系统调试。
大容量事件记录事件记录簿的容量为4096条,为用户日常使用管理和物业管理部门对使用情况的监督以及万一发生火灾后事故成因的分析都提供一个超长时间的可靠数据记录。
系统结构图前言奥瑞那公司成立于1995年,一直专业从事火灾自动报警设备的研发、生产、销售和服务。
200余名高素质员工、5000m2现代化厂房、众多自动化生产检测设备,严谨完善的质量管理体系,充分保证了产品的先进性和可靠性。
先进的技术和设备、严格的质量控制、优良的售后服务,是奥瑞那向客户提供可靠产品并让客户放心满意的有力保证。
奥瑞那的产品具有外形美观、质量可靠、服务优良的特点,主导产品火灾报警及消防联动控制系统已成功应用于数千项工程,在广东省消防指挥中心、广东省政协办公楼、甘肃省政府办公楼、江西省政协大厦、天健世纪花园、天然居(6栋32层住宅楼)、绿景蓝湾畔岛(8栋33层商住楼)、天鸿安柏丽晶、万科东海岸等许多重大工程中发挥着重要作用。

J B-Q B-O Z H200火灾报警控制器使用说明书(V1.0)-CAL-FENGHAI.-(YICAI)-Company One1目录第一章产品介绍 (2)概述 (2)主要技术指标 (2)产品功能特点 (2)第二章安装与接线.......................................................................................... 错误!未定义书签。
设备外观与机箱安装.. (3)部件组成 (3)电源连接 (3)端子说明 (4)第三章键盘及主界面说明.............................................................................. 错误!未定义书签。
键盘说明. (4)主界面说明 (5)第四章菜单界面.............................................................................................. 错误!未定义书签。
设置菜单. (5)操作菜单 (6)编程菜单 (6)查询菜单 (7)编码菜单 (7)帮助菜单 (7)第五章部件类型对照表.................................................................................. 错误!未定义书签。
第六章常见故障排除方法.............................................................................. 错误!未定义书签。
第七章联系方式.............................................................................................. 错误!未定义书签。

1.4 火灾报警控制器概述OZH4800系列火灾报警控制器是消防报警及联动系统的核心设备,它负责检测各探测器、模块等部件的状态,及时将回路总线上各部件的火警信息以声、光形式反应出来,并按预先编制的联动关系以总线形式联动相应设备,完成报警及联动灭火任务。
奥瑞那公司的OZH4800系列火灾报警控制器具有强大的功能和可靠的长期稳定性,完全符合国家技术标准规定和用户的实际要求。
产品特点及功能z容量:单机最大容量11520地址,可以1~8台控制器联网组成超大系统;每回路总线监控容量 192地址;每块回路扩展卡配置4个回路,共768地址;单机基本配置1块回路扩展卡,可最多扩展到15块回路扩展卡。
z总线:1)探测器、手报:2总线,无极性,允许枝状布线,总线长度可达1500m;2)总线联动、楼层显示器:4总线,除与探测器、手报按钮共享信号2总线 外,另加两根电源线(24V,0V);3) 多线联动:N+1线制z地址:由控制器自动编址,探测器和总线联动模块统一编址;火灾显示盘独立编址,不占用整机容量空间。
z显示器:1)主显示器:320X240点阵液晶屏,显示汉字、表格和图形;2)时钟显示器:VFD真空荧光数码管。
z事件记录:可循环记录4096条事件,如:开机、关机、火警、故障、反馈、编程操作、复位等;记录信息掉电或脱机可保存10年;为分析事件提供证据。
z高速微打:可选配热敏或针式微型汉字打印机。
z操作灵活:可测试探测器等部件的电压、电流,反应烟温信息的各种参数。
z自动编址:通过登记操作,对探测器等部件自动编址。
z 外形:壁挂式、立柜式和琴台式三种外型结构,符合不同场所的空间要求。
配壁挂式、柜式和琴台式照片主要技术参数主电源 AC187~242V 50Hz备电源 DC24V 7Ah功耗 监视状态:2.2W 报警状态 :10W巡检周期 3.5秒外形尺寸 壁挂式:700mm(高)×520mm(宽)×140mm立柜式:500mm(长)×610mm(宽)×1860mm(高)标准单琴台式:1040mm(长)×610mm(宽)×1115mm(高)标准单琴台式:1040mm(长)×610mm(宽)×1115mm(高)技术标准 GB4717-93、GB16806-1997配置参考z JB-QB-OZH5800/64 智能火灾报警控制器(联动型) 壁挂64点z JB-QB-OZH5800/128 智能火灾报警控制器(联动型)壁挂128点z JB-QB-OZH5800/192 智能火灾报警控制器(联动型)壁挂192点z JB-QB-OZH5800/384 智能火灾报警控制器(联动型)壁挂384点z JB-QB-OZH5800/768 智能火灾报警控制器(联动型)壁挂768点z JB-QG/T-OZH5800/768 智能火灾报警控制器(联动型) 柜式/台式768点z JB-QG/T-OZH5800/1536 智能火灾报警控制器(联动型) 柜式/台式1536点 z JB-QG/T-OZH5800/2304 智能火灾报警控制器(联动型) 柜式/台式2304点 z JB-QG/T-OZH5800/3072 智能火灾报警控制器(联动型) 柜式/台式3072点 z JB-QG/T-OZH5800/3840 智能火灾报警控制器(联动型) 柜式/台式3840点 每增加一块回路扩展卡,容量增加768点。
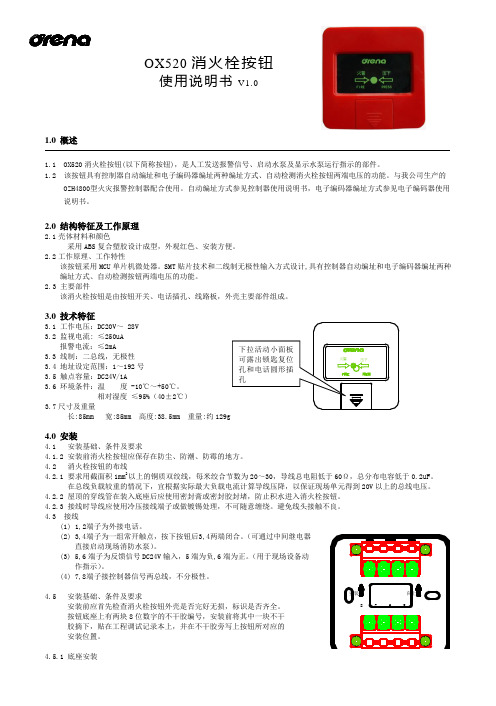
OX520消火栓按钮使用说明书V1.01.0 概述1.1 OX520消火栓按钮(以下简称按钮),是人工发送报警信号、启动水泵及显示水泵运行指示的部件。
1.2 该按钮具有控制器自动编址和电子编码器编址两种编址方式、自动检测消火栓按钮两端电压的功能。
与我公司生产的OZH4800型火灾报警控制器配合使用。
自动编址方式参见控制器使用说明书,电子编码器编址方式参见电子编码器使用说明书。
2.0 结构特征及工作原理2.1壳体材料和颜色采用ABS 复合塑胶设计成型,外观红色、安装方便。
2.2工作原理、工作特性该按钮采用MCU 单片机微处器。
SMT 贴片技术和二线制无极性输入方式设计,具有控制器自动编址和电子编码器编址两种编址方式、自动检测按钮两端电压的功能。
2.3 主要部件该消火栓按钮是由按钮开关、电话插孔、线路板,外壳主要部件组成。
3.0 技术特征3.1 工作电压:DC20V ~ 28V3.2 监视电流: ≤250uA报警电流:≤2mA3.3 线制:二总线,无极性3.4 地址设定范围:1~192号3.5 触点容量:DC24V/1A3.6 环境条件:温 度 -10℃~+50℃。
相对湿度 ≤95%(40±2℃)3.7尺寸及重量长:85mm 宽:85mm 高度:38.5mm 重量:约129g4.0 安装4.1 安装基础、条件及要求4.1.2 安装前消火栓按钮应保存在防尘、防潮、防霉的地方。
4.2 消火栓按钮的布线4.2.1 要求用截面积1mm 2以上的铜质双绞线,每米绞合节数为20~30,导线总电阻低于60Ω,总分布电容低于0.2uF 。
在总线负载较重的情况下,宜根据实际最大负载电流计算导线压降,以保证现场单元得到20V 以上的总线电压。
4.2.2 屋顶的穿线管在装入底座后应使用密封膏或密封胶封堵,防止积水进入消火栓按钮。
4.2.3 接线时导线应使用冷压接线端子或做镀锡处理,不可随意缠绕。
避免线头接触不良。

乐奥苏奥美拉唑肠溶胶囊说明书乐奥苏奥美拉唑肠溶胶囊适用于胃溃疡、十二指肠溃疡、应激性溃疡、返流性食管炎和卓一艾氏综合症(胃泌素瘤),那么乐奥苏奥美拉唑肠溶胶囊说明书你看过吗?下面是店铺为你整理的乐奥苏奥美拉唑肠溶胶囊说明书的相关内容,希望对你有用!乐奥苏奥美拉唑肠溶胶囊说明书【药品名称】通用名称:奥美拉唑肠溶胶囊商品名称:奥美拉唑肠溶胶囊(乐奥苏)英文名称:Omeprazole Enteric Capsules【主要成份】奥美拉唑。
【成份】化学名:5-甲氧基-2-[(4-甲氧基-3,5-二\n甲基-2-吡啶基)-甲基]-亚砜-1H-苯并咪唑分子式:C17H19N3O3S分子量:345.41【性状】本品为胶囊,内含类白色肠衣小颗粒。
【适应症/功能主治】适用于胃溃疡、十二指肠溃疡、应激性溃疡、返流性食管炎和卓一艾氏综合症(胃泌素瘤)。
【规格型号】20mg*14s【用法用量】口服,不可咀嚼。
1.消化性溃疡:一次20mg(一次1片),一日1~2次。
每日晨起吞服或早晚各一次,胃溃疡疗程通常为4~8周,十二指肠溃疡疗程通常2~4周。
2.反流性食管炎:一次20~60 mg(一次1~3片),一日1~2次。
晨起吞服或早晚各一次,疗程通常为4~8周。
3.卓-艾综合征:一次60mg(一次3粒),一日1次,以后每日总剂量可根据病情调整为20~120mg(1~6粒),若一日总剂量需超过80mg(4粒)时,应分为两次服用。
【不良反应】奥美拉唑肠溶胶囊耐受性良好、常见不良反应是腹泻、头痛、恶心。
腹痛、胃肠胀气及便秘。
偶见血清氨基转移酶(ALT,AST)增高。
皮疹。
眩晕、嗜睡、失眠等。
这些不良反应通常是轻微的。
可自动消失。
与剂量无关。
长期治疗未见严重的不良反应。
但在有些病例中可发生胃煔膜细胞增生和萎缩性胃炎。
【禁忌】对本品过敏者和严重肾功能不全者及婴幼儿禁用。
【注意事项】1.治疗胃溃疡时,应首先排除溃疡型胃癌的可能,因用本品治疗可减轻其症状,从而延误治疗。
奥瑞那QZH280消防主机说明书奥瑞那QZH280消防主机操作说明书:一、消音:当主机发生报警信息,联动信息,故障信息时声响,按“消音”键即可消音。
二、复位:当主机屏幕显示有火警,联动,故障信息且该火警信息,联信息或故障信息已被排除时,按“复位”键可将主机恢复至正常监控状态。
三、隔离/释放设备隔离设备:此操作用于发生误报警的或故障的设备,但又不能及时处理的情况。
释放设备:当被隔离的设备经处理恢复正常即可对其进行释放操作,使其恢复正常工作。
操作方法如下:按“设置”键→输入密码“111”→选择2项“故障部件隔离”即按数字键2→根据提示输入回路号和地址号→按“隔离”键将设备隔离,按“解除”键将被隔离设备释放→按“退出”键四、打印机的控制及换纸开关打印机:按“设置”键→输入密码“111”→选择3项“打印机开关设置”即按数字键“3”→按“开”或“关”键→退出老主机换纸:1 将打印机设置在开启状态2 先按打印机上“SEL”,再按“LF”键,使打印机在进纸状态(打印机有呼呼声响)3 将打印纸的端部剪成20度左右插入打印机的进纸口,让纸慢慢的进入4 待纸从打印口出来后,按“SEL”即完成打印纸的安装新主机换纸:1 将打印右边按钮按下,打印机会自动打开,然后将热敏打印纸(超市收银纸)光滑一面朝上,放入打印机,闭合打印机即可。
五、校对时间按“设置”键→密码“111”→选1项“日期和时钟”→根据提示输入准确的日期和时间,按“确认”键→退出六、气体灭火方式和设置按“设置”键→密码“111”→选X项“气体灭火控制方式”→根据提示输入准确的控制状态。
七、主机控制方式和设置1、有多线盘的控制方式由第一块多线控制盘决定。
2、没有多控制盘,按“设置”键→密码“111”→选X项“控制方式”→根据提示输入准确的控制状态。
八、消防控制主机自检按“设置”键→密码“111”→选X项“主机自检”→根据提示输入机器号00,按确定键即可。
注:安装设置,系统设置菜单中禁止操作;如果进行不当的操作造成的后果自负。
目录一、OZH280火灾报警控制器容量、配置、线制及设置 (1)二、OZH280火灾报警控制器操作方法 (3)三、附A: OZH280火灾报警控制器字符区位码对照表 (14)四、附B: OZH280火灾报警控制器汉字区位码对照表 (15)OZH280火灾报警控制器容量、配置、线制及设置一、主要技术指标1、交流输入电压:220V±10%, 50Hz±1%。
2、备用电源:24V 4Ah, 全密封免维护蓄电池。
3、使用环境:温度:0℃~+50℃;相对湿度:≤95% ( 40℃±2℃)。
4、容量:共2回路总线,每回路总线带192地址,整机最大容量为384个地址点。
1回路地址范围1~192;2回路地址范围201~392。
二、配置该设备由主机、电源和多线联动控制部分组成。
1、主机部分:(1)主机面板:液晶屏,键盘,指示灯,扬声器等。
(2)主机主板:(主机板包括回路部分)。
(3)主机电源:(电源板)。
三、线制(1)报警单元:两总线(无极性)(2)接口模块:四总线,两根信号线(无极性),两根电源线(24V,0V)。
(3)复示盘:四总线,两根信号线(无极性),两根电源线(24V,0V)。
(4)线制要求:a. 信号二总线(无极性),采用RVS双绞线,截面积≥1.0mm2。
根据工程具体情况配置。
b. DC24V输出线采用BV线,截面积≥2.5mm2。
c.信号二总线的主干线≥1.5mm2d. 控制器每路总线的往返电阻<20Ω.四、设置(1)系统刷新:首次使用应进行刷新操作,将以前的信息、记录、安装位置、联动编程、综合编程等全部清除;然后再进行登记操作、安装位置编程、联动编程、综合编程、多线联动设置等操作。
操作密码为:11111111。
(2)登记操作:首次加电或总线上部件变更时,需进行登记操作。
登记过程是自动完成的。
登记是按回路号进行的,登记后显示总数信息。
操作密码为:44441111。
Arzerra® (ofatumumab)(Intravenous)Document Number: IC‐0208 Last Review Date: 04/04/2022Date of Origin: 08/26/2014Dates Reviewed: 03/2015, 05/2015, 08/2015, 11/2015, 02/2016, 05/2016, 08/2016, 11/2016, 02/2017,05/2017, 08/2017, 11/2017, 02/2018, 05/2018, 04/2019, 04/2020, 04/2021, 04/2022I.Length of Authorization 1,10Coverage will be provided for 6 months with renewal subject to the following:∙CLL/SLL (first-line) may be renewed to allow for a total of 12 cycles∙CLL/SLL (relapsed) may not be renewed (unless the provisions for extended treatment have been met)∙CLL/SLL (single agent subsequent therapy) may not be renewed (unless the provisions for extended treatment have been met)∙CLL/SLL (extended treatment) may be renewed to provide for a total of 2 years of therapy ∙Waldenström’s Macroglobulinemia/Lymphoplasmacytic lymphoma may be renewed to allow for up to a total of 3 cyclesII.Dosing LimitsA.Quantity Limit (max daily dose) [NDC Unit]:∙Arzerra 100 mg/5 mL single-use vial: 3 vials Day 1∙Arzerra 1000 mg/50 mL single-use vial: 2 vials weekly x 7 doses, then 2 vials every 4 weeks, then 1 vial every 8 weeks for up to 24 monthsB.Max Units (per dose and over time) [HCPCS Unit]:CLL/SLL First‐Line▪30 billable units on day 1 and 100 billable units on day 8; then▪100 billable units every 28 days for up to 11 dosesSingle agent subsequent therapy▪30 billable units on day 1; then▪200 billable units weekly x 7 doses; then▪200 billable units every 28 days x 4 dosesRelapsed▪30 billable units on day 1 and 100 billable units on day 8; then▪100 billable units every 28 days for up to 5 dosesExtended Treatment▪30 billable units on day 1 and 100 billable units on day 8; then▪100 billable units 7 weeks later and every 8 weeks thereafterWaldenström’s Macroglobulinemia / Lymphoplasmacytic Lymphoma ▪30 billable units on day 1; then▪200 billable units every 7 days x 4 dosesIII.Initial Approval Criteria 1Coverage is provided in the following conditions:∙Patient is at least 18 years of age; ANDUniversal Criteria 1∙Patient has been screened for the presence of hepatitis B (HBV) infection (i.e., HBsAg and anti-HBc) prior to initiating therapy and patients with evidence of current or prior HBVinfection will be monitored for HBV reactivation during treatment; AND∙Must not be administered concurrently with live vaccines; ANDChronic Lymphocytic Leukemia (CLL)/Small Lymphocytic Lymphoma (SLL) † Ф1-3∙Used as first-line therapy; ANDo Used in combination with chlorambucil in patients considered inappropriate for fludarabine-based therapy (Note: only applies to CLL);ORo Used in combination with bendamustine ‡; AND▪Patient does not have del(17p)/TP53 mutation (patients ≥ 65 years, or younger patients with or without significant comorbidities; excluding use in frail patients[i.e., creatine clearance (CrCl) <70 mL/min]); OR∙Used as subsequent therapy; ANDo Used as a single agent; ORo Used in combination with fludarabine and cyclophosphamide (FC) for relapsed disease (Note: only applies to CLL);OR∙Used as extended treatment in patients with complete or partial response after at least 2 lines of therapy for recurrent or progressive disease (Note: only applies to CLL) Waldenström’s Macroglobulinemia/Lymphoplasmacytic Lymphoma ‡ 2,4∙Used as a single agent OR as part of combination therapy; AND∙Patient is intolerant to rituximab; ANDo Patient has previously failed primary therapy; ORo Patient has progressive or relapsed disease† FDA Approved Indication(s); ‡ Compendia Recommended Indication(s); Ф Orphan Drug IV.Renewal Criteria 1Coverage may be renewed based on the following criteria:∙Patient continues to meet universal and other indication-specific relevant criteria such as concomitant therapy requirements (not including prerequisite therapy), performancestatus, etc.identified in section III; AND∙Disease response with treatment as defined by stabilization of disease or decrease in size of tumor or tumor spread; AND∙Absence of unacceptable toxicity from the drug. Examples of unacceptable toxicity include: Hepatitis B virus reactivation/infection, progressive multifocal leukoencephalopathy, severe infusion reactions, tumor lysis syndrome, cytopenias (neutropenia, anemia, andthrombocytopenia), etc.V.Dosage/Administration 1,10CLL/SLL (First-line)Administer 300 mg on Day 1, then 1,000 mg on Day 8, followed by 1,000 mg on Day 1 of subsequent 28-day cycles for a minimum of 3 cycles until best response or amaximum of 12 cyclesCLL/SLL (Single agent subsequent therapy)Administer 300 mg on Day 1, followed 1 week later by 2,000 mg given weekly x 7 doses (infusions 2 through 8), followed 4 weeks later by 2,000 mg every 4 weeks for 4 doses (infusions 9 through 12) for a total of 12 dosesCLL/SLL (Relapsed) Administer 300 mg on Day 1, then 1,000 mg on Day 8, followed by 1,000 mg on Day 1 of subsequent 28-day cycles for a maximum of 6 cyclesCLL/SLL (Extended treatment)Administer 300 mg on Day 1, then 1,000 mg on Day 8, followed by 1,000 mg 7 weeks later and every 8 weeks thereafter for up to a maximum of 2 yearsWaldenström’s/ Lymphoplasmacytic lymphoma Cycle 1:∙Administer 300 mg on day 1, then 1,000 mg weekly for weeks 2 through 4; OR∙Administer 300 mg on day 1, then 2,000 mg weekly for weeks 2 through 5Cycle 2-3:∙Patients with stable disease or a minor response at week 16 of cycle 1 are eligible to receive a re-dosing cycle of 300 mg on day 1, then 2,000 mg for weeks 2 through5.Patients responding to cycle 1 or the redosing cycle who developed diseaseprogression within 36 months can receive treatment with 300 mg on day 1, then2,000 mg for weeks 2 through 5.VI.Billing Code/Availability InformationHCPCS Code:•J9302 – Injection, ofatumumab, 10 mg; 1 billable unit = 10 mgNDC:•Arzerra 1000 mg/50 mL single-use vial: 00078-0690-xx•Arzerra 100 mg/5 mL single-use vial: 00078-0669-xxVII.References1.Arzerra [package insert]. East Hanover, NJ; Novartis Pharmaceuticals Corporation, August2016. Accessed March 2022.2.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) ofatumumab. National Comprehensive Cancer Network, 2022. The NCCNCompendium® is a derivative work of the NCCN Guidelines®. NATIONALCOMPREHENSIVE CANCER NETWORK®, NCCN®, and NCCN GUIDELINES® aretrademarks owned by the National Comprehensive Cancer Network, Inc. To view the mostrecent and complete version of the Compendium, go online to . Accessed March2022.3.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Version2.2022. National Comprehensive Cancer Network, 2022. The NCCN Compendium® is aderivative work of the NCCN Guidelines®. NATIONAL COMPREHENSIVE CANCERNETWORK®, NCCN®, and NCCN GUIDELINES® are trademarks owned by the NationalComprehensive Cancer Network, Inc. To view the most recent and complete version of theCompendium, go online to . Accessed March 2022.4.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) Waldenstrom’s Macroglobulinemia/Lymphoplasmacytic Lymphoma. Version2.2022. National Comprehensive Cancer Network, 2022. The NCCN Compendium® is aderivative work of the NCCN Guidelines®. NATIONAL COMPREHENSIVE CANCERNETWORK®, NCCN®, and NCCN GUIDELINES® are trademarks owned by the NationalComprehensive Cancer Network, Inc. To view the most recent and complete version of theCompendium, go online to . Accessed March 2022.5.Furman RR, Eradat H, DiRienzo CG, et al. A phase II trial of ofatumumab in subjects withWaldenstrom's macroglobulinemia. Blood. 2011;118:37016.Wierda WG, Kipps TJ, Mayer J, et al. Ofatumumab as single-agent CD20 immunotherapyin fludarabine-refractory chronic lymphocytic leukemia. J Clin Oncol 2010;28:1749-17557.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) B-Cell Lymphomas. Version 1.2022. National Comprehensive CancerNetwork, 2022. The NCCN Compendium® is a derivative work of the NCCN Guidelines®.2NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®, and NCCNGUIDELINES® are trademarks owned by the National Comprehensive Cancer Network,Inc. To view the most recent and complete version of the Compendium, go online to. Accessed March 2022.8.Rosenbaum CA, Jung SH, Pitcher B, et al. Phase 2 multicentre study of single-agentofatumumab in previously untreated follicular lymphoma: CALGB 50901 (Alliance). Br JHaematol. 2019 Feb 5.9.Van Imhoff GW, McMillan A, Matasar MJ et al. Ofatumumab Versus Rituximab SalvageChemoimmunotherapy in Relapsed or Refractory Diffuse Large B-Cell Lymphoma: TheORCHARRD Study. J Clin Oncol 2017;35 (5):544-551.10.Furman RR, Eradat HA, DiRienzo CG, et al. Once-weekly ofatumumab in untreated orrelapsed Waldenström's macroglobulinaemia: an open-label, single-arm, phase 2 study.Lancet Haematol. 2017 Jan;4(1):e24-e34. doi: 10.1016/S2352-3026(16)30166-1. Epub 2016Dec 1.11.Hillmen P, Robak T, Janssens A, et al. Chlorambucil plus ofatumumab versus chlorambucilalone in previously untreated patients with chronic lymphocytic leukaemia(COMPLEMENT 1): a randomised, multicentre, open-label phase 3 trial. Lancet. 2015 May 9;385(9980):1873-83. doi: 10.1016/S0140-6736(15)60027-7. Epub 2015 Apr 14.12.Robak T, Warzocha K, Govind Babu K, et al. Ofatumumab plus fludarabine andcyclophosphamide in relapsed chronic lymphocytic leukemia: results from theCOMPLEMENT 2 trial. Leuk Lymphoma. 2017 May;58(5):1084-1093. doi:10.1080/10428194.2016.1233536. Epub 2016 Oct 12.13.van Oers MH, Kuliczkowski K, Smolej L, et al. Ofatumumab maintenance versusobservation in relapsed chronic lymphocytic leukaemia (PROLONG): an open-label,multicentre, randomised phase 3 study. Lancet Oncol. 2015 Oct;16(13):1370-9. doi:10.1016/S1470-2045(15)00143-6. Epub 2015 Sep 13.14.Lemery SJ, Zhang J, Rothmann MD, et al. U.S. Food and Drug Administration Approval:Ofatumumab for the Treatment of Patients with Chronic Lymphocytic Leukemia Refractory to Fludarabine and Alemtuzumab. 10.1158/R-10-0570 Published September2010.15.Chen L, Shah R, Cwynarski K. et al. Ofatumumab is a feasible alternative anti-CD20therapy in patients intolerant of rituximab. Br J Haematol. 2019 Feb;184(3):462-465.doi: 10.1111/bjh.15110. Epub 2018 Jan 24.Appendix 1 – Covered Diagnosis Codes1010C83.00 Small cell B-cell lymphoma, unspecified siteC83.01 Small cell B-cell lymphoma, lymph nodes of head, face and neckC83.02 Small cell B-cell lymphoma, intrathoracic lymph nodes1010C83.03 Small cell B-cell lymphoma, intra-abdominal lymph nodesC83.04 Small cell B-cell lymphoma, lymph nodes of axilla and upper limbC83.05 Small cell B-cell lymphoma, lymph nodes of inguinal region and lower limbC83.06 Small cell B-cell lymphoma, intrapelvic lymph nodesC83.07 Small cell B-cell lymphoma, spleenC83.08 Small cell B-cell lymphoma, lymph nodes of multiple sitesC83.09 Small cell B-cell lymphoma, extranodal and solid organ sitesC88.0 Waldenström macroglobulinemiaC91.10 Chronic lymphocytic leukemia of B-cell type not having achieved remissionC91.12 Chronic lymphocytic leukemia of B-cell type in relapseAppendix 2 – Centers for Medicare and Medicaid Services (CMS)Medicare coverage for outpatient (Part B) drugs is outlined in the Medicare Benefit Policy Manual (Pub. 100-2), Chapter 15, §50 Drugs and Biologicals. In addition, National Coverage Determination (NCD), Local Coverage Determinations (LCDs), and Local Coverage Article (LCAs) may exist and compliance with these policies is required where applicable. They can be found at: https:///medicare-coverage-database/search.aspx. Additional indications may be covered at the discretion of the health plan.Medicare Part B Covered Diagnosis Codes (applicable to existing NCD/LCA/LCD): N/AJurisdiction Applicable State/US Territory ContractorE (1) CA, HI, NV, AS, GU, CNMI Noridian Healthcare Solutions, LLCF (2 & 3) AK, WA, OR, ID, ND, SD, MT, WY, UT, AZ Noridian Healthcare Solutions, LLC5 KS, NE, IA, MO Wisconsin Physicians Service Insurance Corp (WPS)6 MN, WI, IL National Government Services, Inc. (NGS)H (4 & 7) LA, AR, MS, TX, OK, CO, NM Novitas Solutions, Inc.8 MI, IN Wisconsin Physicians Service Insurance Corp (WPS) N (9) FL, PR, VI First Coast Service Options, Inc.J (10) TN, GA, AL Palmetto GBA, LLCM (11) NC, SC, WV, VA (excluding below) Palmetto GBA, LLCNovitas Solutions, Inc.L (12) DE, MD, PA, NJ, DC (includes Arlington &Fairfax counties and the city of Alexandria in VA)K (13 & 14) NY, CT, MA, RI, VT, ME, NH National Government Services, Inc. (NGS)15 KY, OH CGS Administrators, LLC。
目录一、OZH4800火灾报警控制器(联动型) Ver 2003容量、配置、线制及设置 (1)二、OZH4800火灾报警控制器(联动型) Ver 2003操作方法 (3)三、总线联动控制盘 (24)四、OZH4800火灾报警控制器(联动型)Ver 2003汉字字符区位码对照表 (25)OZH4800火灾报警控制器(联动型) Ver 2003容量、配置、线制及设置一、主要技术指标1、交流输入电压:220V±10%, 50Hz±1%。
2、备用电源:24V 7.0Ah, 全密封免维护蓄电池;3、使用环境:温度:0℃~40℃;相对湿度:≤95% ( 40℃)。
4、容量:基本配置可管理4路总线,每路总线带192地址,可扩展为60路总线,整机最大容量为11520地址。
5、联动与报警统一编址,可根据实际要求设置。
二、配置该设备由主机、分机和总线联动控制部分、多线联动控制部分组成,基本配置为一台主机、一台分机、一块总线联动盘和一套多线联动控制盘。
其中分机可扩展到十五台,多线联动控制盘最大可容纳127个地址。
1、主机部分包括:(1)主机面板:液晶屏,键盘,指示灯,扬声器等。
(2)主机主板:(内装与电源板靠近)(3)主机电源:(电源板)。
2、分机部分包括:(1)分机回路板:可连接四路总线。
(2)分机总线联动板:有8点、32点、64点、96点四种。
3、多线联动控制盘:可直接手动控制127台设备。
三、线制(1)报警单元:两总线(ZX+、ZX-),无极性。
1(2)接口模块:四总线,两根信号线(ZX+、ZX-),两根电源线(24V,0V),信号线无极性。
(3)复示盘:四总线,两根信号线(ZX+、ZX-),两根电源线(24V,0V),信号线无极性。
四、设置(1)主机板上8位拨码开关的设置1~4位备用5位ON 手动允许OFF 自动允许6位ON 自动打印OFF 禁止打印7位ON 不检测电源OFF 检测电源8位ON 键盘锁定,只有【消音】、【上页】、【下页】键开放OFF 键盘开放(2)分机板上8位拨码开关的设置1~4位设置分机地址,有效范围为1~155位ON 手动允许OFF 自动允许6位ON 装有32点总线联动板OFF 无32点总线联动板7位ON 装有64点总线联动板OFF 无64点总线联动板28位ON 开机自动登记OFF 开机不自动登记(3)登记:首次加电或总线上部件变更时,需进行登记操作。