Calculation of organ doses from breast cancer radiotherapy a Monte Carlo study
- 格式:pdf
- 大小:860.66 KB
- 文档页数:14

小学上册英语第2单元期中试卷(有答案)英语试题一、综合题(本题有100小题,每小题1分,共100分.每小题不选、错误,均不给分)1.Do you know my _____ (邻居)?2.The playground is ______ (fun) to play in.3.Dolphins are very _________. (聪明)4.The __________ (历史的启示作用) motivates individuals.5.The ______ can carry heavy loads on its back.6.What is the capital of Sri Lanka?A. ColomboB. KandyC. GalleD. Jaffna答案: A. Colombo7.The chemical formula for calcium oxide is ______.8.What is the largest organ in the human body?A. HeartB. BrainC. SkinD. Liver答案:C9.The __________ is known for its colorful coral reefs. (大堡礁)10. A _____ (植物) may have medicinal properties.11.The _______ can help with soil erosion.12.The process of separating liquids based on boiling points is called _______.13.What do you do with a pencil?A. EatB. WriteC. SleepD. Jump答案: B14.The chemical symbol for potassium is ________.15. A __________ is a natural opening in the earth, allowing molten rock to escape.16.The waves are _______ (crashing) on the shore.17.The _____ (笔记) is important.18.What do we call the place where we learn?A. HomeB. SchoolC. ParkD. Office答案: B19.The ________ (project) requires teamwork.20.Different types of matter can be classified into ______ and mixtures.21.The phone is _______ on the table.22.She is wearing a _____ hat. (green)23.The _______ (老虎) is a powerful animal.24.What do we call the stage of life after childhood?A. AdolescenceB. AdulthoodC. InfancyD. Elderly答案:B.Adulthood25.Listen and number.(听录音标号.)26.I like to pretend my toys are ________.27.I have a pet ______ (fish).28. A solid has a _____ shape and volume.29.I love _______ (和朋友一起)做手工。

小学上册英语第四单元真题(含答案)考试时间:90分钟(总分:140)B卷一、综合题(共计100题共100分)1. 选择题:What is the largest land animal?A. RhinocerosB. GiraffeC. ElephantD. Hippopotamus答案:C2. 听力题:The solid formed from a chemical reaction is called a ______.3. 听力题:The atomic number tells you the number of ______ in an atom.4. 听力题:Plants can grow in both _______ and dry conditions.5. 选择题:What do we call the process of a caterpillar turning into a butterfly?A. MetamorphosisB. EvolutionC. TransformationD. Development答案:A6. 听力题:The ______ helps us learn about science.7. 填空题:The first Olympic Games were held in ________ (古希腊).8. 听力题:The symbol for lanthanum is _____.9. 填空题:My favorite thing to do on a rainy day is _______ (阅读).10. 选择题:What is the name of the famous statue in Rio de Janeiro?A. Christ the RedeemerB. Statue of LibertyC. DavidD. Moai11. 选择题:What is the name of the famous street in New York City known for shopping?A. Rodeo DriveB. Fifth AvenueC. Wall StreetD. Broadway答案:B12. 选择题:What is the name of the famous ancient monument in Egypt?A. ColosseumB. Great WallC. PyramidsD. Stonehenge13. 选择题:What do we call a vehicle that flies?A. CarB. BoatC. AirplaneD. Train14. 选择题:What is the main ingredient in bread?A. SugarB. FlourC. RiceD. Salt答案:B15. 填空题:I like to write ______ (诗).16. 听力题:A chemical reaction can occur in _____ solutions.17. 听力填空题:I think it’s essential to take breaks. Taking time to relax helps recharge our minds and bodies. I like to __________ during my breaks to unwind.18. 填空题:The __________ (科学教育) promotes critical thinking.19. 听力题:The substance that is dissolved in a solution is called the _______.20. 填空题:I enjoy watching the _______ (小动物) in the park.21. 听力题:The girl is very ________.22. 选择题:What is the primary color of the sky on a clear day?A. GreenB. BlueC. GrayD. White答案: B23. 填空题:My favorite teacher knows how to _______ (动词). 她教我们 _______ (名词).24. 填空题:A horse can gallop very ________________ (快).25. 填空题:The _______ (蜗牛) leaves a slimy trail.26. 听力题:The ant builds a home called an _______.27. 听力题:The chemical formula for sodium sulfide is ______.28. 选择题:What is the name of the famous landmark in the USA?A. Statue of LibertyB. Washington MonumentC. Golden Gate BridgeD. All of the above答案: D. All of the above29. 填空题:A snail moves very ______ (慢).30. 选择题:What is 5 - 2?A. 2B. 3C. 4D. 531. 填空题:________ (叶片) can be broad or narrow.32. 选择题:What do we call the largest organ of the human body?A. HeartB. LiverC. SkinD. Brain答案:C33. 听力题:A bat uses ______ to navigate in the dark.34. 听力题:I like to collect ______ (stamps) from different countries.35. 选择题:What is the name of the famous ocean surrounding Antarctica?A. Atlantic OceanB. Arctic OceanC. Indian OceanD. Southern Ocean答案:D36. 填空题:The flowers smell _______ (甜美).37. 选择题:What is the capital of Saint Vincent and the Grenadines?a. Kingstownb. Arnos Valec. Calliaquad. Georgetown答案:a38. 填空题:A ________ is a fun stuffed animal.39. 听力题:Many stars are part of binary ______.40. 听力题:A chemical equation must be _______ to show that mass is conserved.41. 听力题:Many _______ lose their leaves in the fall.42. 听力题:I want to _____ (become/learn) an artist.43. 选择题:What is the name of the ocean between Africa and Asia?A. AtlanticB. IndianC. ArcticD. Pacific答案:B44. 选择题:What is the name of the fairy tale character who left a glass slipper?A. Snow WhiteB. CinderellaC. Sleeping BeautyD. Little Red Riding Hood答案: B45. 填空题:I love to play outside with my ________.46. 填空题:I enjoy _____ (discovering) new plants.47. 填空题:I feel _______ when I read.48. 听力题:A chemical reaction can produce _____ and heat.The _______ of a wave can change when it enters a new medium.50. 选择题:What is the color of a typical peach?A. GreenB. YellowC. PinkD. Orange答案:D51. 听力题:The _____ (汽车) is red.52. 选择题:What color is an orange?A. BlueB. OrangeC. GreenD. Red53. 听力题:A polymer is a large molecule made of many ______.54. 选择题:What is the opposite of "north"?A. EastB. WestC. SouthD. Up答案: C. South55. 填空题:My favorite character from a book is ______.56. 填空题:I like to help my ______ (父母) at home.57. 听力题:The _____ (花) smells good.58. 填空题:The writer, ______ (作家), creates amazing stories.59. 听力题:The bear catches a fish with its _____ strong paws.What is 5 + 7?A. 11B. 12C. 13D. 14答案:C61. 听力题:The ______ teaches us about international relations.62. 填空题:I like to __________ (动词) my __________ (玩具名) with friends after school.63. 填空题:My brother loves to __________ (玩耍) with his friends.64. 选择题:How do you say "yes" in Russian?A. DaB. NetC. OuiD. Si65. 选择题:What is the term for a baby kangaroo?A. JoeyB. CalfC. KitD. Cub答案:A66. 选择题:What do we breathe?A. WaterB. AirC. FoodD. Fire答案:B67. 听力题:The process by which plants make their food is called ______.68. 填空题:A flamingo's diet consists mainly of ________________ (浮游生物).What do we call the study of the human body?A. AnatomyB. BiologyC. ChemistryD. Physiology答案:A70. 填空题:My _______ (狗) likes to play fetch.71. 听力题:The ________ (research) provides valuable insights.72. 选择题:What is the main ingredient in sushi?A. NoodlesB. RiceC. BreadD. Pancakes73. 选择题:What do you call a person who creates art?A. ArtistB. ScientistC. EngineerD. Writer答案:A74. 填空题:The _______ (猪) is known for its intelligence.75. 听力题:The city of Nur-Sultan is the capital of _______.76. 听力题:The _______ is the center of an atom.77. 填空题:I enjoy playing ______ outside.78. Age is characterized by the use of ______ (石头) tools. 填空题:The StonI like to visit the ______ (农场) and see all the animals. Feeding the chickens is always a fun activity.80. 听力题:I like to ________ new things.81. 听力题:I love to ________ new things.82. 听力题:The chemical formula for undecanoic acid is ______.83. 填空题:A ______ (种子库) preserves genetic diversity in plants.84. 选择题:What is the main ingredient in salad dressing?A. OilB. VinegarC. WaterD. Milk85. 填空题:I enjoy watching ________ (动画) on Saturday mornings.86. 听力题:A compass helps us find ______ (direction).87. 听力题:The Earth is the _____ planet from the sun.88. 听力题:The capital of Ghana is __________.89. 填空题:The ancient Romans established ________ to govern their territories.90. 选择题:What is the capital of Lesotho?A. MaseruB. MaputoC. MbabaneD. Gaborone答案:AThis ________ (玩具) is great for developing skills.92. 听力题:Spectroscopy helps scientists determine the composition of _______.93. 选择题:What do we breathe?A. WaterB. FoodC. AirD. Fire94. 选择题:What is the hottest planet in our solar system?A. VenusB. MercuryC. MarsD. Jupiter答案:A95. 听力题:Rust is formed when iron reacts with ______.96. 听力题:The ______ is a popular author.97. 填空题:A ________ (鸽子) can be seen flying in the sky and often symbolizes peace.98. 填空题:The __________ (历史的传承) shapes our narrative.99. 选择题:What is the capital of Greece?A. AthensB. SpartaC. ThessalonikiD. Corinth100. 选择题:What is the capital of Tanzania?A. Dar es SalaamB. DodomaC. ZanzibarD. Arusha答案: B. Dodoma。

ANNEX ISUMMARY OF PRODUCT CHARACTERISTICS1. NAME OF THE MEDICINAL PRODUCTGRANUPAS4 g gastro-resistant granules2. QUALITATIVE AND QUANTITATIVE COMPOSITIONEach sachet contains 4 g of para-aminosalicylic acid.For the full list of excipients, see section 6.1.3. PHARMACEUTICAL FORMGastro-resistant granulesThe granules are small off white/ light brown coloured approximately 1.5mm diameter.4. CLINICAL PARTICULARS4.1 Therapeutic indicationsGRANUPAS is indicated for use as part of an appropriate combination regimen for multi-drug resistant tuberculosis in adults and paediatric patients from 28 days of age and older when an effective treatment regimen cannot otherwise be composed for reasons of resistance or tolerability (see section 4.4).Consideration should be given to official guidance on the appropriate use of antibacterial agents.4.2 Posology and method of administrationPosologyAdults4 g (one sachet) three times per day.The recommended schedule is 4 g every 8 hours. GRANUPAS can be taken with food.Maximum daily dose is 12 g. Usual duration of treatment is 24 months.Paediatric populationThe optimal dose regimen in children is uncertain. Limited pharmacokinetic data suggest no substantial difference between adults and children.For infants, children and adolescents the dosage will be adapted to the patient’s weight at 150 mg/kg per day, divided in two intakes. A dosing spoon is provided to measure small doses below 4g for young children.The safety and efficacy of GRANUPAS in neonates have not been established.No data are available. DesensitizationDesensitization can be accomplished by starting with 10 mg para-aminosalicylic acid given as a single dose. The dosage is doubled every 2 days until reaching a total of 1 gram after which the dosage is divided to follow the regular schedule of administration. If a mild temperature rise or skin reaction develops, the increment is to be dropped back one level or the progression held for one cycle. Reactions are rare after a total dosage of 1.5 g.Method of administrationOral use.The contents of the sachet should be added to a glass of orange or tomato juice. They will not dissolve, but swirling the juice in the glass will help re-suspend the granules if they sink. It should be drunk at once ensuring that the granules are not left in the glass. Any granules left-over at the bottom of the glass should be swallowed immediately by adding a small quantity of liquid. Smaller doses in children should be measured using the dosing spoon and given by sprinkling on apple sauce or yogurt.The medicinal product should be swallowed immediately after mixing with orange juice, tomato juice, apple sauce and yogurt whilst the granules are intact.The granules should not be crushed or chewed.4.3 ContraindicationsHypersensitivity to the active substance or to any of the excipients listed in section 6.1.Severe renal disease. Patients with severe renal impairment should not receive GRANUPAS. Patients with severe renal disease will accumulate the inactive acetyl metabolite of para-aminosalicylic acid. 4.4 Special warnings and precautions for useMild to moderate renal impairmentGiven that the metabolites of para-aminosalicylic acid are largely excreted via glomerular filtration, caution is warranted in patients with mild to moderate renal impairment (see also section 4.3). Gastric ulcerGRANUPAS should be used with caution in patients with peptic ulcer.Hepatic impairmentGRANUPAS should be used with caution in patients with hepatic impairment.Hepatic toxicityPara-aminosalicylic acid may cause hepatitis. The first symptoms usually appear within three months of the start of therapy with a rash as the most common adverse reaction followed by fever and much less frequently by gastrointestinal disturbances of anorexia, nausea or diarrhoea. Treatment should be stopped immediately in this case.HypersensitivityThe patient must be monitored carefully during the first three months of therapy and treatment must be discontinued immediately at the first sign of a rash, fever or other premonitory signs of intolerance. See section 4.2 for posology adjustements for desensitization.Patients should be advised that the skeletons of the granules may be seen in the stools.4.5 Interaction with other medicinal products and other forms of interactionNo interaction studies have been performed with GRANUPAS.Results from literature suggest the following:Vitamin B12Vitamin B12 absorption may be reduced by para-aminosalicylic acid with clinically significant erythrocyte abnormalities developing after depletion; patients on therapy of more than one month should be considered for maintenance of vitamin B12.Malabsorption syndromeA malabsorption syndrome can develop in patients on para-aminosalicylic acid, but is usually not complete. The complete syndrome includes steatorrhoea, an abnormal small bowel pattern on x-ray, villus atrophy, depressed cholesterol, reduced D-xylose and iron absorption. Triglyceride absorption is always normal.DigoxinPara-aminosalicylic acid may decrease the gastrointestinal absorption of digoxin, by inhibiting the absorption function of intestinal cells. Serum digoxin levels should be monitored in patients on concomitant therapy.EthionamideCo-administration of para- aminosalicylic acid and ethionamide may intensify adverse reactions of para-aminosalicylic acid, mainly the gastrointestinal effects, including jaundice, hepatitis, nausea, vomiting, diarrhoea, abdominal pain or anorexia. Ethionamide should be withdrawn if these effects are significant.DiphenylhydramineThis medicinal product decreases the gastrointestinal absorption of para-aminosalicylic acid, and should not be administered concomitantly.AntiretroviralsNo drug interaction studies have been conducted in patients with HIV infection taking antiretroviral agents and para-aminosalicylic acid.Given the metabolic pathway of GRANUPAS no significant drug interaction is anticipated.4.6 Fertility, pregnancy and lactationPregnancyThere are no or limited data from the use of para-aminosalicylic acid in pregnant women. Studies in animals have shown some embryologic toxicity (see section 5.3).Literature reports on para- aminosalicylic acid in pregnant women always report co-administration of other medicinal products. As there are no adequate and well controlled studies of para- aminosalicylic acid in humans, GRANUPAS should be given to a pregnant woman only if clearly needed. BreastfeedingPara-aminosalicylic acid is excreted into breast milk, therefore breastfeeding mothers should not breastfeed during treatment.FertilityThere is no evidence available on the effect of para-aminosalicylic acid on fertility.4.7 Effects on ability to drive and use machinesPara-aminosalicylic acid has negligeable influence on the ability to drive and use machines.4.8 Undesirable effectsSummary of the safety profileMost frequent adverse reactions were related to the gastrointestinal system. Cutaneous hypersensitivity reactions were also frequent as well as adverse reactions related to the nervous system.Tabulated list of adverse reactionsIn the table below all adverse reactions are listed by system organ class and by frequency. Frequency is defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.System Organ Class Frequency Adverse reactionBlood and lymphatic systemdisorders Very rareThrombocytopenia, purpura, leukopenia,anemia, methemoglobinemia, agranulocytosisMetabolism and nutritiondisordersRare hypothyroidism Very rare HypoglycemiaNervous system disorders Very rareTendon pain, headache, visual abnormalities,peripheral neuropathy, dizziness Common Giddiness, vestibular syndromeGastrointestinal disordersCommonabdominal pain, vomiting, nausea, bloating,diarrhea, soft stools, Uncommon anorexia,RareMalabsorption syndrome, peptic ulcer,gastrointestinal bleeding, jaundice, metallictasteSkin and subcutaneous tissuedisorders Common Cutaneous hypersensitivity, skin rash Rare urticariaRenal and urinary disorders Very rare crystalluriaInvestigations Very rare Decreased prothrombine level, hepatocytolysis.Increased blood alkaline phosphatase,transaminases. weight lossPaediatric populationFrequency, type and severity of adverse reactions in children are expected to be the same as in adults. Reporting of suspected adverse reactionsReporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system listed in Appendix V.4.9 OverdoseNo case of overdose in adults or paediatrics has been reported. Treatment is symptomatic and supportive.5. PHARMACOLOGICAL PROPERTIES5.1 Pharmacodynamic propertiesPharmacotherapeutic group: Antimycobacterials, drugs for treatment of tuberculosis ATC code: J04AA01Mechanism of actionAminosalicylic acid is bacteriostatic against Mycobacterium tuberculosis. It inhibits the onset of bacterial resistance to streptomycin and isoniazid.The mechanism of action of para-aminosalicylic acid resembles the sulfonamides, competing with paraminobenzoic acid (PABA) for dihydropteroate synthetase (DHP), a key enzyme in the biosynthesis of folates. However, para-aminosalicylic acid appears to be a weak inhibitor of DHP invitro, raising the possibility that it may have a different target. Para-aminosalicylic acid is acetylated in the liver and converted into the inactive metabolite, N-acetyl-para-aminosalicylic acid which is devoid of bacteriostatic activity. The plasma half-life of this agent is about 1 hour, the concentration is not substantially altered in hepatic dysfunction. The concentration of the metabolite may be increased in cases of renal failure.5.2 Pharmacokinetic propertiesAbsorptionGRANUPAS is a gastro-resistant preparation and, therefore, the acid-resistant coating of the granules protects against degradation in the stomach therefore preventing the formation of meta-aminophenol (a known hepatotoxin). The small granules are designed to escape the restriction on gastric emptying of large particles. Under neutral conditions as are found in the small intestine or in neutral foods, the acid-resistant coating is dissolved within one minute.Care must be taken in the administration of these granules to protect the acid-resistant coating by maintaining the granules in an acidic food during dosage administration.Because the granules are protected by an enteric coating, absorption does not commence until they leave the stomach. The soft skeletons of the granules remain and may be seen in the stools.In a single dose (4 grams) pharmacokinetic study in healthy adult volunteers (N=11) the initial time to a 2 µg/mL serum level of aminosalicylic acid was 2 hours with a range of 45 minutes to 24 hours; the median time to peak was 6 hours with a range of 1.5 to 24 hours; the mean peak level was 20 µg/mL with a range of 9 to 35µg/mL: a level of 2µg/mL was maintained for an average of 8 hours with a range of 5 to 9.5 a level of 1 µg/mL was maintained for an average of 8.8 hours with a range of 6 to 11.5 hours.DistributionPara-aminosalicylic acid is distributed in various tissues and fluids including the lungs, kidneys, liver and peritoneal fluid. Pleural or synovial fluid concentrations are approximately equal to plasma. The drug does not cross the blood brain barrier in patients unless the meninges are inflamed, when the concentration of para-aminosalicylic acid in cerebrospinal fluid is about 10 to 50% of the plasma. It is unknown whether it passes through the placental barrier. Small amounts of this agent are distributed in the milk and bile.Plasma protein binding is about 50 to 60%, the kinetic distribution has a half-life of 0.94 hours and a volume of distribution of 1.001 L/kg.BiotransformationThe major metabolites of PAS are produced by conjugation to glycine in para-aminosalicyluric acid (PASU) for up to 25% of the dose and to N-acetyl in N-acetyl para-aminosalicylic acid (Ac-PAS) for up to 70% of the dose. Together they constitute more than 90% of the total metabolites of PAS found in urine.EliminationIn a single dose study the plasma half-life of para-aminosalicylic acid administered as GRANUPAS was 1.62±0.85 h.Para-aminosalicylic acid and its metabolites are excreted by glomerular filtration and tubular secretion. The cumulative excretion of para-aminosalicylic after 24 hours is 84% of an oral dose of 4 g, 21% as para-aminosalicylic acid and 63% as the acetylated form. The acetylation process is not genetically determined as is the case for isoniazid.5.3 Preclinical safety dataNon-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology and repeated dose toxicity.The data available from a rat embrofetal development study, where animals were given sodium aminosalicylate (3.85 to 385 mg/kg) were limited. Bone defects were observed at 77 mg/kg only.and increased fetal weight was noted at the other doses. Other malformations were observed; however, the exact nature of these findings is unknown. The lack of a dose-response relationship suggests that the findings are not of clinical relevance, but it is noted that the findings were observed at doses below those proposed clinically. In the rabbit, sodium aminosalicylate had no effects on embryofetal development; however, the doses evaluated were below those proposed clinically.Sodium aminosalicylic acid was not mutagenic in Ames test strain TA 100. In human lymphocyte cultures in-vitro clastogenic effects of achromatic, chromatid, isochromatic breaks or chromatid translocations were not seen at 153 or 600 µg /mL but at 1500 and 3000 µg/mL there was a dose related increase in chromatid aberrations. No in vivo genotoxicity study has been conducted with GRANUPAS.6. PHARMACEUTICAL PARTICULARS6.1 List of excipientsColloidal silicon dioxideDibutyl sebacateMethacrylic acid – Ethyl acrylate Copolymer (1:1) Dispersion 30%HypromelloseMicrocrystalline celluloseTalc6.2 IncompatibilitiesNot applicable.6.3 Shelf life2 years.6.4 Special precautions for storageStore in a refrigerator (2°C – 8°C).The sachets can be stored below 25°C up to 24 hours after first opening.6.5 Nature and contents of containerSachets consisting of paper/low density polyethylene/aluminium foil/primer/low density polyethylene. Pack size of 30 sachets. A calibrated measuring spoon is provided.6.6 Special precautions for disposal and other handlingThe granules should not be crushed or chewed.DO NOT USE if sachet is swollen or if the granules have lost their light brown colour, and are turning dark brown or purple.Any unused product or waste material should be disposed in accordance with local requirements.7. MARKETING AUTHORISATION HOLDERLucane Pharma,172 rue de Charonne75011 ParisFrance8. MARKETING AUTHORISATION NUMBER(S)EU/1/13/896/0019. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATIONDate of first authorisation: 07 April 2014.10. DATE OF REVISION OF THE TEXTDetailed information on this medicinal product is available on the website of the European Medicines Agency: http://www.ema.europa.eu.ANNEX IIA. MANUFACTURER RESPONSIBLE FOR BATCH RELEASEB. CONDITIONS OR RESTRICTIONS REGARDING SUPPLY AND USEC. OTHER CONDITIONS AND REQUIREMENTS OF THE MARKETINGAUTHORISATIOND. CONDITIONS OR RESTRICTIONS WITH REGARD TO THE SAFE ANDEFFECTIVE USE OF THE MEDICINAL PRODUCTA. MANUFACTURER RESPONSIBLE FOR BATCH RELEASEName and address of the manufacturer responsible for batch releaseLucane Pharma,172 rue de Charonne75011 ParisFranceB. CONDITIONS OR RESTRICTIONS REGARDING SUPPLY AND USEMedicinal product subject to medical prescription.C. OTHER CONDITIONS AND REQUIREMENTS OF THE MARKETINGAUTHORISATION•Periodic safety update reportsThe marketing authorisation holder shall submit the first periodic safety update report for this product within 6 months following authorisation. Subsequently, the marketing authorisation holder shall submit periodic safety update reports for this product in accordance with the requirements set out in the list of Union reference dates (EURD list) provided for under Article 107c(7) of Directive 2001/83/EC and published on the European medicines web-portal.D. CONDITIONS OR RESTRICTIONS WITH REGARD TO THE SAFE ANDEFFECTIVE USE OF THE MEDICINAL PRODUCT•Risk Management Plan (RMP)The MAH shall perform the required pharmacovigilance activities and interventions detailed in the agreed RMP presented in Module 1.8.2 of the Marketing Authorisation and any agreed subsequent updates of the RMP.An updated RMP should be submitted:•At the request of the European Medicines Agency;•Whenever the risk management system is modified, especially as the result of new information being received that may lead to a significant change to the benefit/risk profile or as the result of an important (pharmacovigilance or risk minimisation) milestone beingreached.If the submission of a PSUR and the update of a RMP coincide, they can be submitted at the same time.•Additional risk minimisation measuresNone•Obligation to conduct post-authorisation measuresNoneANNEX IIILABELLING AND PACKAGE LEAFLETA. LABELLINGPARTICULARS TO APPEAR ON THE OUTER PACKAGINGCARTON BOX1. NAME OF THE MEDICINAL PRODUCTGRANUPAS 4 g gastro-resistant granulesPara-aminosalicylic acid2. STATEMENT OF ACTIVE SUBSTANCE(S)Each sachet contains 4 g of para-aminosalicylic acid3. LIST OF EXCIPIENTS4. PHARMACEUTICAL FORM AND CONTENTSGastro-resistant granules30 sachetsCalibrated measuring spoon5. METHOD AND ROUTE(S) OF ADMINISTRATIONRead the package leaflet before use.Oral use.Do not chew or crush.Warning: Do not use if sachet is swollen or the granules have lost their light brown color and are dark brown or purple6. SPECIAL WARNING THAT THE MEDICINAL PRODUCT MUST BE STORED OUT OF THE SIGHT AND REACH OF CHILDRENKeep out of the sight and reach of children.7. OTHER SPECIAL WARNING(S), IF NECESSARY8. EXPIRY DATEEXP9. SPECIAL STORAGE CONDITIONSStore in a refrigerator.10. SPECIAL PRECAUTIONS FOR DISPOSAL OF UNUSED MEDICINAL PRODUCTS OR WASTE MATERIALS DERIVED FROM SUCH MEDICINAL PRODUCTS, IF APPROPRIATE11. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER Lucane Pharma172 rue de Charonne75011 ParisFrance12. MARKETING AUTHORISATION NUMBER(S)EU/1/13/896/00113. BATCH NUMBERLot14. GENERAL CLASSIFICATION FOR SUPPLYMedicinal product subject to medical prescription.15. INSTRUCTIONS ON USE16. INFORMATION IN BRAILLEGRANUPAS 4gMINIMUM PARTICULARS TO APPEAR ON SMALL IMMEDIATE PACKAGING UNITS SACHET1. NAME OF THE MEDICINAL PRODUCT AND ROUTE(S) OF ADMINISTRATION GRANUPAS 4g gastro-resistant granulesPara aminosalicylic acidOral use2. METHOD OF ADMINISTRATION3. EXPIRY DATEEXP4. BATCH NUMBERLot5. CONTENTS BY WEIGHT, BY VOLUME OR BY UNIT4 g6. OTHERWarning: Do not use if sachet is swollen or the granules have lost their light brown color and are dark brown or purple.Do not chew or crush.Read the package leaflet before use.B. PACKAGE LEAFLETPackage leaflet: Information for the patientGRANUPAS 4 g gastro-resistant granulesPara-aminosalicylic acidRead all of this leaflet carefully before you start taking this medicine because it contains important information for you.•Keep this leaflet, you may need to read it again•If you have any further questions, ask your doctor or pharmacist.•This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours.•If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. See section 4.What is in this leaflet1. What GRANUPAS is and what it is used for2. What you need to know before you take GRANUPAS3. How to take GRANUPAS4. Possible side effects5.How to store GRANUPAS6. Contents of the pack and other information1.What GRANUPAS is and what it is used forGRANUPAS contains para-aminosalicylic acid which is used in adults and children aged 28 days and older to treat resistant tuberculosis in combination with other medicines, in cases of resistance or intolerability with other treatments.2.What you need to know before you take GRANUPASDo not take GRANUPAS if•you are allergic to para-aminosalicylic acid or any of the other ingredients of this medicine (listed in section 6)•you have severe kidney disease.If you are not sure, talk to your doctor or pharmacist before taking GRANUPAS.Warnings and precautionsTalk to your doctor or pharmacist before taking GRANUPAS•if you have liver problems or mild or moderate kidney disease•if you have a stomach ulcerChildrenUse of GRANUPAS is not recommended in newborn babies (under 28 days of age).Other medicines and GRANUPASTell your doctor or pharmacist if you are taking, have recently taken or are planning to take any other medicines.It is especially important to tell your doctor if you are taking any of the following: •Antituberculosis medicines or ethionamide (other treatments against tuberculosis) •Vitamin B12•Digoxin (for heart disease)•Diphenylhydramine (for allergic reactions)Pregnancy and breast-feedingIf you are pregnant or breast-feeding, think you may be pregnant or are planning to have a baby, ask your doctor or pharmacist for advice before taking this medicine.•GRANUPAS should only be used during pregnancy if advised by your physician•Do not breastfeed whilst taking GRANUPAS. This is because small amounts of the medicine can pass into mother’s milk.Driving and using machinesGRANUPAS is unlikely to affect your ability to drive and use machines.3.How to take GRANUPASAlways take this medicine exactly as your doctor has told you. Check with your doctor or pharmacist if you are not sure.AdultsThe recommended dose for adults is 1 sachet three times a day, with a schedule of 1 sachet every 8 hours. Your physician may need to start with a lower dose to prevent possible side effects.Do not take more than 3 sachets per day. Treatment is usually given for two years (24 months). •Add the contents of the sachet to a drink of tomato or orange juice.•Drink straight away•If some granules are left in the glass, add some more juice and drink straight away.Infants, children and adolescentsThe dose in infants, children and adolescents will be calculated by your doctor based on the patient’s body weight. The recommended total dose per day is 150 mg for each kg of body weight. This daily amount is divided into two doses spread out through the day.•Use the spoon that comes with the medicine to measure the dose.•To measure the dose:o Lines on the spoon indicate the amount (in milligrams of para-aminosalicylic acid).Take the correct amount as prescribed by your doctor.o Put granules directly into the spoon.o Tap the spoon once on a table to give a horizontal level of granules and continue filling if necessary.•Sprinkle the granules onto apple sauce or yogurt.•Make your child eat it straight away.Taking this medicine•Do not crush or chew the granules.•Do not use the sachet if it is swollen or the granules have lost their light brown colour. •You may notice granules appearing in your stools; this is normal.If you take more GRANUPAS than you shouldSpeak to a doctor or pharmacist.If you forget to take a dose of GRANUPASDo not take a double dose to make up for a forgotten dose. Wait until the next dose is due, then take your normal dose.If you have any further questions on the use of this medicine, ask your doctor or pharmacist.4. Possible side effectsLike all medicines, this medicine can cause side effects, although not everybody gets them.During the first 3 months of your treatment with GRANUPAS, you must be attentive to any sign of allergic reaction or hepatitis, like skin eruption and/or fever. If you experience any of these symptoms, you must talk to your doctor immediately.Common side effects (may affect more than 1 in 100 people): giddiness, stomach ache (abdominal pain), vomiting, nausea, bloating, diarrhoea, soft stools, skin redness or rash, disturbance of gait and equilibrium.Uncommon side effects (may affect more than 1 in 1,000 people): loss of appetite (anorexia)Rare side effects (may affect more than 1 in 10,000 people): thyroid gland problems, reduced ability to absorb nutrients from food ulcer, bleeding in the gut, yellowing of skin or eyes (jaundice), metallic taste, itchy rash.Very rare side effects (may affect less than 1 in 10,000 people): reduction in numbers of red or white blood cells, reduction in blood platelets, red spots on the skin, low levels of blood sugar, tendon pain, headache, visual abnormalities, nerve damage in the hands and feet, dizziness, prolonged bleeding time, elevated liver enzymes, weight loss, crystals in urine.Reporting of side effectsIf you get any side effects, talk to your doctor or pharmacist.This includes any possible side effects not listed in this leaflet.You can also report side effects directly via the national reporting system listed in Appendix V. By reporting side effects you can help provide more information on the safetyof this medicine.5. How to store GRANUPASKeep out of the sight and reach of children.Do not use after the expiry date which is stated on the carton and sachet after EXP. The expiry date refers to the last day of the month.Store in a refrigerator (2°C – 8°C). The sachets can be stored below 25°C up to 24 hours after opening.Do not use GRANUPAS if you notice the sachets are swollen or if the granules are dark brown or purple.Medicines should not be disposed of via wastewater or household waste. Ask your pharmacist how to dispose of medicines no longer required. These measures will help to protect the environment.6. Contents of the pack and other informationWhat GRANUPAS containsThe active substance is para-aminosalicylic acid.Each sachet of gastroresistant granules contains 4 g of para-aminosalicylic acid.The other ingredients are colloidal silicon dioxide, dibutyl sebacate, methacrylic acid – ethyl acrylate copolymer (1:1) dispersion 30%, hypromellose, microcrystalline cellulose, talc.What GRANUPAS looks like and contents of the packThis medicine is presented as light brown gastro-resistant granules in sachets.Each box contains 30 sachets. A calibrated measuring spoon is provided.Marketing Authorisation HolderLucane Pharma172 rue de Charonne75011 Paris - FranceManufacturerLucane Pharma,172 rue de Charonne75011 ParisFranceFor any information about this medicine, please contact the local representative of the Marketing Authorisation Holder:België/Belgique/Belgien Lucane PharmaTél/Tel: + 33 153 868 750 info@ LietuvaMedical Need Europe AB Tel: + 46 8 533 39 500 info@БългарияLucane PharmaTeл.: + 33 153 868 750 info@ Luxembourg/Luxemburg Lucane PharmaTél/Tel: + 33 153 868 750 info@Česká republika Medical Need Europe AB Tel: + 46 8 533 39 500 info@ MagyarországMedical Need Europe AB Tel.: + 46 8 533 39 500 info@DanmarkMedical Need Europe AB Tlf: + 46 8 533 39 500 info@ MaltaLucane PharmaTel: + 33 153 868 750 info@DeutschlandLucane PharmaTel: + 33 153 868 750 info@ NederlandLucane PharmaTel: + 33 153 868 750 info@EestiMedical Need Europe AB Tel: + 46 8 533 39 500 info@ NorgeMedical Need Europe AB Tlf: + 46 8 533 39 500 info@ΕλλάδαLucane PharmaΤηλ: + 33 153 868 750 info@ ÖsterreichLucane PharmaTel: + 33 153 868 750 info@。

左乳癌保乳术后放疗患者应用A-DIBH方法降低心脏剂量的研究作者:韩英陈科李强陈俊来源:《中国现代医生》2022年第09期[摘要] 目的本研究目的是在左侧乳腺癌保乳术后辅助放疗的患者中应用腹式呼吸深吸气屏气方法降低放疗时的心脏剂量,从而减少心脏远期不良事件的发生。
方法纳入2019年2月至2020年5月宁波大学附属人民医院左侧乳腺癌术后辅助调强放疗的患者30例,每位患者分别进行自由呼吸和腹式呼吸深吸气屏气,在两种不同呼吸模式下进行CT扫描,每位患者共生成两种治疗计划:自由呼吸和腹式呼吸深吸气屏气下的调强放疗计划。
使用t检验和Wilcoxon 秩和检验对计划靶区、心脏、左前降支冠状动脉和左肺的剂量进行评估和比较。
结果两种呼吸模式下的计划靶区平均剂量分别为(49.43±0.23)Gy和(49.39±0.46)Gy,差异无统计学意义(P>0.05)。
心脏平均剂量为(5.44±1.00)Gy和(2.02±0.66)Gy(P0.05)。
结论左侧乳腺癌保乳术后辅助调强放疗的患者中,使用腹式呼吸深吸气屏气计划相对于自由呼吸的计划能降低患者心脏和左前降支冠状动脉剂量。
腹式呼吸深吸气屏气模式的调强放疗计划可以作为左侧乳腺癌保乳术后辅助放疗患者的常规治疗模式,值得推广应用。
[关键词] 左乳癌;腹式呼吸深吸氣屏气;调强放射治疗;心脏剂量;数模[中图分类号] R737.9 [文献标识码] B [文章编号] 1673-9701(2022)09-0084-04Study on the application of A-DIBH method to reduce the cardiac dose in patients undergoing radiotherapy after breast-conserving surgery for left-sided breast cancerHAN Ying1 CHEN Ke1 LI Qiang2 CHEN Jun11.Center of Radiotherapy and Chemotherapy,the Affiliated People′s Hospital of Ningbo University, Ningbo 315100, China;2.Department of Radiology,the Affiliated People′s Hospital of Ningbo University, Ningbo 315100, China[Abstract] Objective To apply abdominal-deep inspiration breath hold (A-DIBH) to reduce the cardiac dose during radiotherapy in patients undergoing adjuvant radiotherapy after breast-conserving surgery for left-sided breast cancer, so as to reduce the occurrence of long-term adverse cardiac events. Methods Thirty patients undergoing adjuvant intensity-modulated radiotherapy after left-sided breast cancer surgery from February 2019 to May 2020 in the Affiliated People′s Hospital of Ningbo University were enrolled. Each patient was treated with free breathing and A-DIBH, and computed tomography (CT) scan was conducted in such two different breathing modes. Each patient received two treatment plans: intensity-modulated radiotherapy with free breathing and with A-DIBH. The doses to the planned target area, heart, left anterior descending (LAD) coronary artery and left lung were evaluated and compared using T test and signed rank test. Results The average doses to the planned target area under the two breathing modes were (49.43±0.23)Gy and (49.39±0.46) Gy, without statistically significant difference(P>0.05). The average doses to the heart were (5.44±1.00)Gy and (2.02±0.66) Gy (P0.05). Conclusion According to this study, for patients undergoing adjuvant intensity-modulated radiotherapy after breast-conserving surgery for left-sided breast cancer, the A-DIBH plan can reduce the doses to heart and LAD coronary artery for patients compared with free breathing plan. The intensity-modulated radiotherapy with A-DIBH plan can be used as a conventional treatment mode for patients undergoing adjuvant radiotherapy after breast-conserving surgery for left-sided breast cancer, and it is worthy of promotion and application.[Key words] Left-sided breast cancer; Abdominal-deep inspiration breath hold; Intensity-modulated radiotherapy; Cardiac dose; Digital simulation目前早期乳腺癌患者保乳手术联合术后辅助放疗已成为主流的治疗手段,保乳手术后全乳辅助放疗可以改善患者的局部控制率和总体生存率[1-2]。
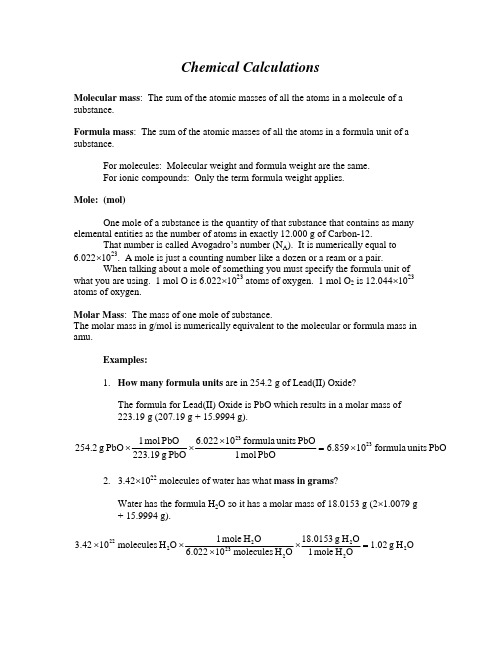
Chemical CalculationsMolecular mass : The sum of the atomic masses of all the atoms in a molecule of a substance.Formula mass : The sum of the atomic masses of all the atoms in a formula unit of a substance.For molecules: Molecular weight and formula weight are the same. For ionic compounds: Only the term formula weight applies.Mole: (mol)One mole of a substance is the quantity of that substance that contains as many elemental entities as the number of atoms in exactly 12.000 g of Carbon-12. That number is called Avogadro’s number (N A ). It is numerically equal to 6.022×1023. A mole is just a counting number like a dozen or a ream or a pair. When talking about a mole of something you must specify the formula unit of what you are using. 1 mol O is 6.022×1023 atoms of oxygen. 1 mol O 2 is 12.044×1023 atoms of oxygen.Molar Mass : The mass of one mole of substance.The molar mass in g/mol is numerically equivalent to the molecular or formula mass in amu.Examples:1. How many formula units are in 254.2 g of Lead(II) Oxide?The formula for Lead(II) Oxide is PbO which results in a molar mass of 223.19 g (207.19 g + 15.9994 g).PbO units formula 10859.6PbOmol 1PbO units formula 10022.6PbO g 19.223PbO mol 1PbO g 2.2542323×=×××2. 3.42×1022 molecules of water has what mass in grams ?Water has the formula H 2O so it has a molar mass of 18.0153 g (2×1.0079 g + 15.9994 g).O H g 02.1OH mole 1O H g 0153.18O H molecules 10022.6O H mole 1O H molecules 1042.32222232222=××××Chemical Equations and Stoichiometry Chemical EquationsA chemical equation is a shorthand way of indicating what is going on in a chemical reaction. We could do it the long way…Two molecules of Hydrogen gas react with one molecule of Oxygen gas to produce two molecule of liquid water.Or we can use the shorthand…2 H2 (g) + O2 (g) → 2 H2O (l)The second way is easier to read and keep track of everything going on. The equation above uses phase symbols. Phase symbols are used to denote the phase of substances in an equation.(g) gas(s) solid(l) liquid(aq)aqueous (water solution)The chemical equation must represent reality. The symbol, ∆, is sometimes used to denote a reaction that is heated and is written above the arrow. Catalyst symbols or formulas are also placed above the arrow.Balancing equationsAn equation is balanced when the number of atoms of each type present is the same on both sides of the equation. The chemical formulas CANNOT be changed in the process of balancing an equation. The process of balancing an equation can sometimes seem to be trial and error. In reality, there is a method to the madness. When we balance a chemical equation we are looking at the relationships between the elements on both sides of the equation. This relationship helps us to figure out what needs to be done. Some basic rules for balancing chemical equations are…1. Start with the most complicated chemical first and start with the element thatappears the most number of times in that compound.2. Save “free” elements for last.Example:CH4 (g) + O2 (g) → CO2 (g) + H2O (l)Here CH 4 is the most complicated and Hydrogen appears the most number of times so we will start with that element. O 2 is a “free” element (not combined with other elements) so we will leave that for last.There are 4 Hydrogens on the reactant side and 2 on the product side. Therefore, we multiply the water on the product side by 2 and the hydrogens balance.CH 4 (g ) + O 2 (g ) → CO 2 (g ) + 2 H 2O (l )The carbons are already balanced. Now we can balance the oxygen atoms. There are 2 on the reactant side and 4 on the product side. If we multiply the O 2 by 2 we balance the oxygen.CH 4 (g ) + 2 O 2 (g ) → CO 2 (g ) + 2 H 2O (l )Now the equation is balanced.Molar interpretation vs. Molecular interpretation of a chemical reactionThe balanced chemical reaction gives you a series of conversion factors to use in problem solving.CH 4 + 2 O 2 → CO 2 + 2 H 2OThe conversion factors are obtained from the coefficients in the balanced chemicalreaction. These conversion factors can be used to relate the amounts of reactant to other reactants or to amounts of products. It is this reason that, in order to solve a chemical problem, you first need to have a balanced chemical equation.Example:How many grams of solid Barium Sulfate can be produced from thereaction of 154.6 g of Barium Nitrate with Sodium Sulfate? The otherproduct of the reaction is Sodium Nitrate.First we need to write the balanced chemical equation:Ba(NO 3)2 + Na 2SO 4 → BaSO 4 + 2 NaNO 3Now we can proceed with the calculation.444234232323BaSO g 1.138BaSO mol 1BaSO g 233.391)Ba(NO mol 1BaSO mol 1)Ba(NO g 261.337)Ba(NO mol 1)Ba(NO g 6.154=×××。

Prescribing InformationDUPHASTONTabletsName of the medicinal productDuphaston 10mg film-coated tabletsQualitative and Quantitative CompositionDydrogesterone film-coated tablets contain 10 mg dydrogesterone per tablet. Pharmaceutical FormA round, biconvex, scored, white coloured film-coated tablet, one side bearing the inscription , the other side bearing the inscription ‘155’ on either side of the break markThe score line is only to facilitate breaking for ease of swallowing and not to divide into equal doses.IndicationsProgesterone deficienciesTreatment of progesterone deficiencies such as:-Treatment of dysmenorrhoea-Treatment of endometriosis-Treatment of secondary amenorrhoea-Treatment of irregular cycles-Treatment of dysfunctional uterine bleeding-Treatment of pre-menstrual syndrome.-Treatment of threatened and habitual abortion, associated with proven progesterone deficiency-Treatment of infertility due to luteal insufficiencyDosage and administrationDysmenorrhoea : 10 mg twice daily from day 5 to day 25 of thecycle.Endometriosis : 10 mg two or three times daily from day 5 today 25 of the cycle or continuously. Dysfunctional bleeding : 10 mg twice daily for five to seven days.(to arrest bleeding)Dysfunctional bleeding : 10 mg twice daily from day 11 to day 25 of the (to prevent bleeding) cycle.Amenorrhoea : an oestrogen once daily from day 1 to day 25 ofthe cycle, together with 10 mg dydrogesteronetwice daily from day 11 to day 25 of the cycle. Pre-menstrual syndrome : 10 mg twice daily from day 11 to day 25 of the cycle.Irregular cycles : 10 mg twice daily from day 11 to day 25 of the cycle.Threatened abortion : 40 mg at once, then 10 mg every eight hoursuntil symptoms remit.Habitual abortion : 10 mg twice daily until the twentieth week ofpregnancy. Infertility due to luteal : 10 mg daily from day 14 to 25 of the cycle. Insufficiency Treatment should be maintained for at least sixconsecutive cycles. It is advisable to continuetreatment for the first few months of pregnancyas described under 'Habitual abortion'. Duphaston is not recommended for use in children below age 18 due toinsufficient data on safety and efficacy.ContraindicationsHypersensitivity to the active substance or to any of the excipients.Known or suspected progestogen dependent neoplasms.Undiagnosed vaginal bleedingSpecial warnings and precautions for useBefore initiating treatment with dydrogesterone for abnormal bleeding, the etiology for the bleeding should be clarified.Treatment with dydrogesterone has infrequently been associated with alterations in liver function, sometimes accompanied by clinical symptoms. Thus, dydrogesterone should be used with caution in patients with acute liver disease or a history of liver disease as long as liver function tests have failed to return to normal. In cases of severe hepatic impairment treatment should be discontinued.Breakthrough bleeding may occur in a few patients.Conditions which need supervisionIf any of the following conditions are present, have occurred previously, and/orhave been aggravated during pregnancy or previous hormone treatment, thepatient should be closely supervised. It should be taken into account that these conditions may recur or be aggravated during treatment with Trademark, in particular:1. Porphyria2. DepressionOther conditionsPatients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine.Interaction with other medicinal products and other forms of interactionNo interaction studies have been performed.Pregnancy and lactationIt is estimated that altogether roughly 35 million women have been treated with dydrogesterone. Although the number of pregnancies is difficult to estimate, as an approximation it can be assumed that in utero foetuses were exposed to dydrogesterone in around 9 million pregnancies1. From spontaneous surveillance systems to date, there is no evidence that dydrogesterone can not be used during pregnancy.No other relevant epidemiological data on dydrogesterone are available.However, a recent US case-control study investigating 502 cases with hypospadias and 1286 healthy controls suggested at least a 2-fold increased risk of second/third degree hypospadias among boys born by mothers who took progestogens (predominantly progesterone) shortly prior or during early pregnancy (OR 2.2, 95% CI 1.0-5.0). The causality is unclear as the indication for progesterone in pregnancy may be potential risk factors for hypospadias. For dydrogesterone, the risk of hypospadias is unknown.Animal studies have been conducted, however, are insufficient with respect to pregnancy, embryonal /fetal, or postnatal development due to major difference in metabolism between rats and humans (for details see section “preclinical safety data”. The potential risk for humans is unknown.Limited animal safety data suggest that dydrogesterone has delaying effects on partuition, which is consistent with its progestogenic activity.Dydrogesterone is excreted in the milk of nursing mothers. A risk to the suckling child cannot be excluded. Dydrogesterone should not be used during breast-feeding.There is no evidence that dydrogesterone decreases fertility at therapeutic dose.Effects on ability to drive and use machinesDydrogesterone has no or negligible influence on the ability to drive and use machines.1This high exposure in pregnancy is due to the fact that dydrogesterone has pregnancy related indications inlarge parts of the world.Undesirable effectsThe undesirable effects reported in clinical trials and/or in post marketing experience following dydrogesterone therapy are:MedDRA system organ class Common>1/100, <1/10Uncommon>1/1,000,<1/100Rare>1/10,000,<1/1,000Very rare<1/10,000 incl.isolated reportsBlood and the lymphatic system disorders Haemolytic anaemiaImmune systemdisordersHypersensitivityNervous system disorders Migraines/ headacheHepatobiliary disorders hepaticfunctionabnormal (withjaundice,asthenia ormalaise, andabdominal pain)Skin and subcutaneous tissue disorders Dermatitisallergic (e.g.rash, pruritus,urticaria)AngioedemaReproductive system and breast disorders Metrorrhagia Breastpain/tendernessGeneraldisorders andadministrationsite conditionsOedemaOther adverse reactions obtained from the market with unknown frequency in association with dydrogesterone treatment:Neoplasms benign, malignant and unspecified (incl. cysts and polyps)Increase in size of progestogen dependent neoplasms (e.g.meningioma) (see section 4.3). Psychiatric disordersDepressed moodReproductive system and breast disordersBreast swellingOverdoseLimited data are available with regard to overdose in humans. Dydrogesterone was well tolerated after oral dosing (maximum daily dose taken to date in humans 360 mg). No reports of ill-effects from overdose have been recorded. If a large overdose is discovered within two or three hours and treatment seems desirable, gastric lavage is recommended. There are no specific antidotes and treatment should be symptomatic. Aforementioned information is also applicable for overdosing in children. Pharmacological propertiesPharmacodynamic propertiesPharmacotherapeutic group: Genito Urinary system and sex hormones,ATC code: G03DB01Dydrogesterone is an orally-active progestogen which produces a complete secretory endometrium in an oestrogen-primed uterus thereby providing protection for estrogen induced increased risk for endometrium hyperplasia and/or carcinogenesis. It is indicated in all cases of endogenous progesterone deficiency. Dydrogesterone has no estrogenic, no androgenic, no thermogenic, no anabolic and no corticoid activity. Pharmacokinetic propertiesAfter oral administration of labeled dydrogesterone on average 63% of the dose is excreted into the urine. Within 72 hours excretion is complete. Dydrogesterone is completely metabolized. The main metabolite of dydrogesterone is 20α-dihydrodydrogesterone (DHD) and is present in the urine predominantly as the glucuronic acid conjugate. A common feature of all metabolites characterized is the retention of the 4,6diene-3-one configuration of the parent compound and the absence of 17α-hydroxylation. This explains the lack of estrogenic and androgenic effects of dydrogesterone.After oral administration of dydrogesterone, plasma concentrations of DHD are substantially higher as compared to the parent drug. The AUC and C max ratios of DHD to dydrogesterone are in the order of 40 and 25, respectively. Dydrogesterone is rapidly absorbed. The T max values of dydrogesterone and DHD vary between 0.5 and 2.5 hours.Mean terminal half lives of dydrogesterone and DHD vary between 5 to 7 and 14 to 17 hours, respectively.Dydrogesterone is not excreted in urine as pregnanediol, like progesterone. Analysis of endogenous progesterone production based on pregnanediol excretion therefore remains possible.Preclinical safety dataReceptor binding studies and functional activity studies revealed antiandrogenic potency of progesterone, dydrogesterone and its metabolite dihydrodydrogesterone (DHD). The antiandrogenic potency of dydrogesterone and its metabolite DHD is probably noticeably weaker than that of progesterone. With regard to antiandrogenic effects mediated by inhibition of 5α-reductase type II, an important enzyme for differentiation of the maleexternal genitalia, progesterone is as potent as the synthetic enzyme inhibitor finasteride, whereas dydrogesterone and DHD are inactive.The overall potential to act as antiandrogenic endocrine disruptors may be rated as highest for Progesterone, lower for Dydrogesterone and lowest for DHD. Embryofoetal developmental studies were conducted in rats and rabbits using high dosages of dydrogesterone. No structural adverse effects were recorded in the foetal offspring. In a subsequent peripostnatal developmental study pregnant rats were treated with similar dosages of dydrogesterone during the period of gestation, and pups were raised. There were occasions of hypospadias in the male offspring but only at the highest dose. The next lower dose of dydrogesterone showed a sufficient safety margin in rat plasma exposure (>80 fold) compared to the estimated exposure at the maximum human daily dose of 60 mg. However, due to major species differences in metabolism between rats and humans, no adequate margin of exposure could be determined for the main human metabolite dihydrodydrogesterone.Limited animal safety data suggest that dydrogesterone has delaying effects on parturition, which is consistent with its progestogenic activity.Dydrogesterone has been used in several animal models and has been proven to be an entity with low toxicity, not having mutagenic or carcinogenic properties. Pharmaceutical particularsList of excipientsLactose monohydrate, methylhydroxypropylcellulose, maize starch, colloidal anhydrous silica, magnesium stearate, Opadry Y-1-7000 whiteIncompatibilitiesNone knownShelf-life5 years.Special precautions for storageDo not store above 30˚C. Keep in a dry place.Keep the blister in the outer carton, in order to protect from moisture.Nature and contents of container- Blister strips of aluminium foil and PVC film, coated with PVDCof 20 tabletsSpecial precautions for disposalAny unused product or waste material should be disposed of in accordance with local requirements.Manufacturer: Solvay PharmaceuticalsImporter: Perrigo Israel Agencies Ltd.22.2.2010 The format of this leaflet was determined by the Ministry of Health and its content was checked and approved by it in February 2010.。
PharmacologyNo pharmacological activity has been observed in the range of doses administered for diagnostic purposes. Pharmacokinetic PropertiesThe pertechnetate ion has similar biological distribution to iodide and perchlorate ions, concentrating temporarily in salivary glands, choroid plexus, stomach (gastric mucosa) and in the thyroid gland, from which it is released unchanged. The pertechnetate ion also tends to concentrate in areas with increased vascularisation or with abnormal vascular permeability, particularly when pre-treatment with blocking agents inhibits uptake in glandular structures. Technetium - 99m is selectively excluded from the cerebrospinal fluid. Following intravenous administration, pertechnetate [99m Tc] is distributed throughout the vascular system from which it is cleared by three main mechanisms:• rapid removal, depending on the diffusion equilibrium with interstitial fluid;• intermediate rate of removal, depending on the concentration of the pertechnetate in glandular tissue, mainly thyroid, salivary and gastric fundus glands which have an ionic pump mechanism;• slow removal, by glomerular filtration by the kidneys, dependent on rate of urinary excretion.Plasma clearance has a half-life of approximately 3 hours. Excretion during the first 24 hours following administration is mainly urinary (~25%) with faecal excretion occurring over the next 48 hours. Approximately 50% of the administration activity is excreted within the first 50 hours.When selective uptake of pertechnetate [99m Tc] in glandular structures is inhibited by the pre-administration of blocking agents, excretion follows the same pathways but there is a higher rate of renal clearance.When pertechnetate [99m Tc] is administered in association with pretreatment with reducing agents such as stannous/medronate which cause a “stannous leading” of red blood cells, up to approximately 95% of the administered activity is taken up bythe red blood cells where it becomes bound within the cells.Any unbound pertechnetate [99m Tc] is cleared by the kidneys. Radioactivity in the plasma normally constitutes less than 5% of the intravascular activity.The fate of technetium-99m follows that of the labelled erythrocyte themselves and the activity is cleared very slowly. A small level of elution of activity from the circulating red cells is thought to occur.Sodium pertechnetate injection may be reacted with a range of reagents (cold kits) to provide diagnostic agents for the imaging of specific organs.IndicationsSodium pertechnetate [99m Tc] is used for scintigraphy, principallyof the brain and thyroid. It can also be used to prepare various technetium-99m labelled injections for selective organ imaging especially of the liver, lung, bone and kidney. ContraindicationsSince Sodium Pertechnetate [99m Tc] is excreted through the kidneys and the gastrointestinal tract, its use in patients suffering obstructive pathology may give rise to a higher level of radiation exposure.PrecautionsGeneralRadiopharmaceuticals should be used only by physicians who are qualified by specific training in the safe use and handling of radionuclides produced by a nuclear reactor or particle accelerator and whose experience and training have been approved by the appropriate government agency authorised to license the use of radionuclides.Care should be taken to minimise radiation exposure to patients consistent with proper patient management. As with other radioactive drugs, Sodium Pertechnetate [99m Tc] must be handled with care and appropriate safety measures should be used to minimise radiation exposure to clinical personnel.Disposal of all radioactive wastes should be carried out in accordance with the NHMRC “Code of Practice for the Disposal of Radioactive Wastes by the User” 1985.Use with caution in the following circumstances Because the pertechnetate ion is concentrated in the thyroid gland, choroid plexus and salivary glands, a blocking dose of up to 1 gram of reagent grade potassium perchlorate in a suitable base of capsule may be given orally prior to the administration of Sodium pertechnetate [99m Tc] injection for brain scanning. Patients who have had scans performed on them in the previous 6 weeks with agents containing tin may show distribution artefacts and/or poor quality images in a subsequent Sodium pertechnetate [99m Tc] brain scan as a result of uptake of pertechnetate by the red blood cells. The physician should give special consideration in such cases to an alternative agent, eg. 99m Tc:DTPA.Check the following before useVerification of the dose to be administered and patient identification is necessary prior to administration. Parenteraldrug products should be inspected visually for particulate matter and discolouration prior to administration whenever solution or container permits.At the time of adminstration the solution should be crystal clear and should not be used if it is cloudy or if it contains particulate matter.Carcinogenesis, Mutagenesis, Impairment of FertilityAdequate reproduction studies have not been performed in animals to determine whether this drug affects fertility in males or females, has teratogenic potential, or has other adverse effectson the foetus.Use in PregnancyDirect administration of 800 MBq Sodium pertechnetate [99m Tc]to a patient results in an absorbed dose to the uterus of 6.5mGy. Following pretreatment of patients with a blocking agent, administration of 800 MBq Sodium pertechnetate [99m Tc] results in an absorbed dose to the uterus of 5.3 mGy.Administration of 925 MBq 99m Tc-labelled red blood cells results in an absorbed dose to the uterus of 4.3mGy. Doses above 0.5mGy should be regarded as a potential risk to the foetus.Use in LactationAs a general rule breast-feeding should not be undertaken when a patient is administered radioactive material.If the administration is considered necessary, breast-feeding should be interrupted and the expressed feeds discarded.Breast-feeding can be restarted when the activity level in the milk will not result in a radiation dose to the child greater than 1mSv. Paediatric UseSafety and effectiveness in children have not been established. Interactions with other drugsDrug interactions have been reported in brain scintigraphy where there can be increased uptake of [99m Tc] pertechnetate in the walls of cerebral ventricles as a result of methotrexate induced ventriculitis.In abdominal imaging, drugs such as atropine, isoprenalineand analgesics can result in a delay in gastric emptying and redistribution of pertechnetate.Adverse ReactionsThe following adverse reactions have been reported following intravenous injection of Sodium pertechnetate [99m Tc]: Hypersensitivity and Skin urticaria, pruritus Cardiovascular arrhythmia, vasodilationBody as a whole facial oedema, comaDosage and AdministrationSodium Pertechnetate [99m Tc] injection is administered by intravenous injection. The dosage employed varies for each diagnostic procedure with due allowances being made for patient body weight. The suggested intravenous dose range employed in the average adult (70kg) for the various diagnostic procedures is as follows:Brain Scan370-740 MBq (10-20 mCi) Thyroid Gland Scan37-185 MBq (1-5 mCi) Salivary Gland Scan37-185 MBq (1-5 mCi)Blood Pool Imaging370-740 MBq (10-20 mCi)In order to reduce radiation dose to the bladder the patient should be encouraged to drink fluids and to void as frequently as possible after the administration of the radiopharmaceutical for a period of four to six hours.OverdosageIn the event of an administration of a radiation overdose with Sodium pertechnetate [99m Tc], increasing the elimination of the radionuclide from the body should reduce the absorbed dose. Measures to reduce possible harmful effects include frequent voiding of urine and promotion of diureses and faecal excretion. Very little treatment can be undertaken in the event of an overdose of [99m Tc) labelled red blood cells since elimination is dependent on the normal haemolytic process.Radiation DosimetryThe estimated absorbed radiation doses to an average patient (70kg) from an intravenous injection of a maximum dose of 740 MBq of Sodium Pertechnetate [99m Tc] administered with and without a thyroid blocking agent is shown in Table 6.Table 6Dose (mGy)With Blocking Agent Without Blocking AgentStomach Wall 2.421.5Upper large Intestine 2.845.9Lower large Intestine 3.316.3Ovaries 3.57.4Red Marrow 3.3 4.5Testes 2.4 2.0Thyroid 1.617.0Bladder Wall23.714.1 Effective Dose 3.58.9 Reference:ICRP Publication 62 (Nov 1992) Radiation doses to patients from radiopharmaceuticals, Johansson L, Mattsson S, NosslinB and Leide-Svegborn S. Effective dose to patients from radiopharmaceuticals. Eur J Nucl Med (1992) 19:933-938How SuppliedThe generator is supplied in sizes ranging from 20 to 120 GBq and 370 GBq of 99Mo at 0900 hours Sydney time on the day of calibration.The generator pack contains the following items for use in its elution:(i) 1 Sterile generator.(ii) 2 kits each containing 5x5mL or 5x10mL or 5x20mL vials of Sodium Chloride for Injections BP.(iii) 2 kits each containing 5 x 30 evacuated vials, 5 sterile needles and 5 sterile mediswabs.(iv) Elution vial shield with viewing window supplied with initial order only.ExpiryThe Sodium Pertechnetate [99m Tc] Injection contains no bactericide and should not be used later than 8 hours after elution. The generator has an expiration time of 14 days after the date of calibration (shown on the generator label).StorageThe generator is designed to operate at normal room temerature (below 30°C). The yield of Sodium Pertechnetate [99m Tc] may be affected if the generator and the 0.9% sodium chloride solution are stored below room temperature.Disposal of the GeneratorThe generator (and packaging) should be kept and not disposed of as normal waste within 70 days of the calibration date. Users are encouraged to return their generators to ANSTO Health for recycling. A special set of instructions and labels are included with each generator.References1. European Commision Committee for Proprietary MedicinalProducts Ad hoc group on radiopharmaceuticals Technetium [99m Tc] Generator Dec 1994 111/3143/93-En Final.2. Walker, A.G., Effect of 99m Tc bone scan agent on subsequentbrainscans. Ad hoc J. Nucl. Med. 16:579, 1975.3. Richards, P. and O’Brien, M.J., Rapid determination of 99Mo inseparated 99m Tc. J. Nucl. Med., 10:517, 1969.TGA Approved date: 24th January 1994Amended: April 2014Contact Details:ANSTO HealthLocked Bag 2001Kirrawee DC NSW 2232Telephone: 1800 251 572Facsimile: 02 9543 6511ANSTO Health is a commercial enterpriseof the Australian Nuclear Science andTechnology Organisation (ANSTO),which is located at Lucas Heights,in Sydney, NSW.Product No: 10000AUST R: 72820, 75859.。
2024年11版小学英语第3单元期末试卷考试时间:100分钟(总分:100)B卷考试人:_________题号一二三四五总分得分一、综合题(共计100题)1、填空题:I love to eat fruit from the _____ (果园). It is fresh and delicious.我喜欢吃果园里的水果。
它新鲜美味。
2、What is the name of the fairy tale character who lost her glass slipper?A. Snow WhiteB. CinderellaC. BelleD. Ariel答案: B3、填空题:The ancient Greeks believed in the importance of ________ (艺术).4、听力题:A ______ is a collection of data gathered from observations.5、听力题:A _______ can attract butterflies.6、听力题:The chemical symbol for gallium is ______.7、填空题:The crab scuttles quickly across the _______ (沙滩).8、How many days are there in a week?A. 5B. 7C. 10D. 129、What do we call the fruit that is yellow and curved?A. AppleB. BananaC. PeachD. Grape10、填空题:The river flows ________ (快速).11、听力题:Trees produce oxygen during the process of ______.12、填空题:A _____ (社区花园) fosters cooperation and learning.13、What is 4 x 2?A. 6B. 8C. 10D. 12答案:B14、听力题:The _______ of sound can be measured using a sound level meter.15、What is the capital city of Italy?A. VeniceB. RomeC. FlorenceD. Naples16、填空题:I often tell my friends, "You can call me ______ anytime!"(我经常告诉我的朋友:“你随时可以叫我!”)17、填空题:A ________ (湿地) is important for biodiversity.18、听力题:The chemical formula for iron oxide is ______.19、听力题:A chemical formula shows the ratio of ______ in a compound.20、填空题:This boy, ______ (这个男孩), enjoys learning about space.The lamp is ___ (bright/dim).22、听力题:The process of plants making food is called ______.23、听力题:The chemical reaction of metals with oxygen produces __________.24、听力题:A reaction that produces a color change is a sign of a ______ reaction.25、What is the scientific study of living organisms?A. BiologyB. ChemistryC. PhysicsD. Geology答案:A26、听力题:We can ___ a fun game. (play)27、What is the primary ingredient in a traditional bagel?A. Rye flourB. Wheat flourC. CornmealD. Sourdough28、填空题:My sister loves to play with ______ (小猫).29、填空题:A _______ (小狐狸) has a bushy tail and sharp senses.30、听力题:The classroom is ___ (clean/messy).31、填空题:The __________ is known for its unique wildlife and ecosystems. (加拉帕戈斯群岛)32、填空题:In conclusion, my best friend is ______ because they make my life better. I am so grateful to have them by my side!33、听力题:A ______ has a long life cycle.A ________ is a place where an ocean meets land.35、填空题:I wish I could create my own ________ (名词) one day. It would be the most ________ (形容词) toy ever!36、How many hours are in a day?A. 12B. 24C. 36D. 48答案:B37、Which planet is known as the Red Planet?A. EarthB. MarsC. JupiterD. Saturn38、What do we call the period of time before written records?A. PrehistoricB. HistoricC. AncientD. Medieval答案:A39、听力题:The train is ______ (fast) and loud.40、填空题:The ______ (狮子) is known as the king of the jungle.41、What is the value of 5 + 5 3?A. 6B. 7C. 8D. 9答案:B42、ahal is a famous ________ (泰姬陵是著名的________) in India. 填空题:The Taj43、听力题:A gradient is a change in a variable over _____ distance.My favorite fruit is _______ (樱桃).45、听力题:The ______ helps educate young minds.46、听力题:The chemical symbol for water is ______.47、选择题:What is the capital of Italy?A. LisbonB. RomeC. AthensD. Paris48、oasis) is a fertile area in a desert. 填空题:The ____49、填空题:_____ (植物小组) can share gardening tips.50、听力题:A reaction that produces energy is called an ______ reaction.51、填空题:The ________ is a beautiful flower.52、听力题:Salt forms when an acid reacts with a ________.53、What is the capital of New Zealand?A. WellingtonB. AucklandC. ChristchurchD. Hamilton答案: A54、听力题:The movie was very _______ (interesting).55、What do we call the act of arranging flowers?A. FloristryB. GardeningC. LandscapingD. Horticulture答案:A56、Which animal is known as the king of the jungle?A. ElephantB. LionC. TigerD. Bear57、填空题:The __________ (战争的影响) shaped national identities.58、听力题:The element that is a gas at room temperature and essential for life is _______.59、听力题:The rabbit is ________ in the grass.60、填空题:I can play make-believe with my ________ (玩具).61、填空题:She is my __________ sister. (亲姐妹)62、填空题:A _____ is an area of low land between hills or mountains.63、选择题:How many legs does a cat have?A. 4B. 3C. 2D. 564、听力题:The capital of China is _______.65、听力题:I see a _____ (cloud/rock) in the sky.66、填空题:I enjoy _______ (看电影) on weekends.67、填空题:Plants can also help to clean the ______ (空气).The chemical symbol for gold is ______.69、填空题:We had a _________ (玩具交换) at school, and I got a new _________ (玩具).70、听力题:The letter is ________ in the mailbox.71、听力题:A saturated solution is one that can no longer ______.72、填空题:This girl, ______ (这个女孩), is a natural leader among her friends.73、填空题:The __________ (历史的纷争) can lead to reconciliation.74、How many hours are in a day?A. 12B. 24C. 36D. 4875、选择题:What is the capital of China?A. BeijingB. ShanghaiC. GuangzhouD. Shenzhen76、听力题:The clouds are ______ (fluffy) and white.77、填空题:The ancient Greeks contributed to the development of _____.78、听力题:I have a _____ (collection) of rocks.79、听力题:The ______ teaches us about different countries.80、听力题:The ____ makes a soft sound and is often seen in the garden.My dad is known for his __________ (智慧).82、听力题:The _____ (小猫) is playful.83、听力题:A ______ is a type of insect that can produce honey.84、填空题:The __________ (历史的复杂性) warrants careful study.85、听力题:The study of how rocks and minerals interact is called ______.86、sustainability conference) shares knowledge and strategies. 填空题:The ____87、What is the main purpose of a map?A. To tell timeB. To show directionsC. To draw picturesD. To write letters88、听力题:I found a ________ on the ground.89、What is the capital of Kenya?A. NairobiB. KampalaC. Addis AbabaD. Dar es Salaam答案: A90、填空题:_____ (自然) provides many resources for plants.91、What do we call the energy from the sun?A. Solar energyB. Wind energyC. Nuclear energyD. Geothermal energy答案:AA substance that speeds up a chemical reaction without being consumed is called a _______.93、听力题:A __________ is an animal that can survive in very hot environments.94、听力题:An acid-base reaction produces ______.95、填空题:My dad has a green ______ (摩托车). He rides it on the weekends.96、听力题:She always helps me with my __________.97、What do you call a person who swims?A. DiverB. SurferC. SwimmerD. Sailor答案:C98、填空题:A frog has webbed ______ (脚) for swimming.99、听力题:The _____ (山) is high.100、What do we call a baby elephant?A. CalfB. FawnC. CubD. Joey答案: A。
THE EMPIRICAL FORMULA OF A COMPOUNDINTRODUCTION-In a compound, the atoms of different elements are present in numbers whose ratio is usually expressed as an integer or a simple fraction. The simplest formula of the compound expresses that ratio and also, if the compound is non-molecular, serves to identify it. For example, the simplest formula for potassium chlorate, KClO3, tells us that in that compound, for every K atom there is a Cl atom and three O atoms. The K:Cl atom ratio is 1:1 and the K:O ratio is 1:3. An important job of the chemist is to find the simplest formulas of any new compound he or she discovers.Simplest formulas are determined by establishing the mass of each element present in a given mass of the compound. From those masses one finds the number of moles of each element. The mole ratio must be equal to the atom ratio in the compound and from that ratio the simplest (empirical) formula is easily found.To find the mass of each element in a compound, one must carry out at least one chemical reaction involving that compound and other known substances. Sometimes it is possible to form the compound directly from the elements. This is called a synthesis reaction (A+B=AB). In this experiment, you will form, or synthesize, magnesium oxide by burning magnesium in the oxygen of the air.Word EquationMagnesium + Oxygen → Magnesium oxideSkeletal EquationMg + O2 → MgOBalanced Equation2Mg + O2→ 2MgOBy weighing the magnesium before the reaction occurs and the magnesium oxide produced by the reaction, one can calculate the mass of oxygen that reacted with the magnesium. To do this we need to refer to the Law of Conservation of Mass. Which states that mass can be neither created nor destroyed. From the masses of magnesium and oxygen in the magnesium oxide we find the simplest (empirical) formula of that compound. To obtain good results in this exercise you must perform each step carefully. and must be particularly careful to make the “massings” as accurately as possible.YOU NEED TO KNOW:In order to successfully complete this lab, you should be skilled in the following areas:1. Calculation of empirical formulas (see page 271-279 in your text)2. The procedure for writing chemical equations.THE EXPERIMENT PURPOSE:1. To make a compound from its elements.2. To determine the empirical (simplest) formula of a compound.3. To describe a chemical reaction in terms of an equation.MATERIALS:-crucible and cover -clay triangle-ring stand -bunsen burner-heat resistant pad -electronic balance-magnesium ribbon (approx. 25 cm) -paper towelrod -tongs -stirring-wash bottle of water -strikerPROCEDURE:Wear safety goggles during this experiment1. Place a clean crucible and cover on a clay triangle on an iron support ring. The crucible cover should be slightly tilted on the top of the crucible leaving a small opening. Heat the crucible strongly for about three minutes to drive off any moisture. Allow the crucible and cover to cool on a heat resistant pad and then carefully mass them together to the nearest .01g and record on page 3.CAUTION: Crucibles and covers should be handled with tongs not hands.2. While the crucible is cooling, obtain a piece of magnesium ribbon approximately 25 cm long. Rub the ribbon with a piece of paper towel to remove any loose surface coating. Coil the ribbon around a pencil. After the cooled crucible has been massed, add the magnesium ribbon and mass the crucible, lid, and magnesium and record on page3.3. With the lid off, heat the crucible. Increase the temperature gradually. When the magnesium ribbon glows red, or ignites, cover the crucible quickly and reduce the amount of heat applied. If the magnesium actually ignites and burns, some of the compound vaporizes and leaves the crucible. Try not to let this occur, as this will increase your error. To prevent any loss the crucible must be immediately covered if you observe an orange or white flame. After about a minute, carefully remove the cover (to let more oxygen in) and heat until you observe that the magnesium is glowing, or ignites. At that point, replace the cover quickly and reduce the heat. Continue this procedure until no further reaction occurs when you heat the crucible. Then cover the crucible, leaving a small opening, and heat strongly for a few minutes. Let the crucible cool.4. When the crucible is cool, remove the cover and put it on the bench top. Use a stirring rod to grind the contents of the crucible into small particles. Rinse the particles off the stirring rod with about ten drops of water using the wash bottle. Replace the cover, leaving a small opening. Heat gently until the water begins to boil. Remove the burner, and waft the vapor to see if it has any odor. Then, continue heating until all the water is boiled off and the residue is thoroughly dry (about 5 minutes). Let the crucible cool, and then carefully mass the crucible, its lid, and the magnesium oxide.5. Clean the crucible with water as best as you can.DATA TABLE:-Mass of crucible and cover ....................................................................................................__________g. -Mass of crucible, cover, and Mg ribbon ................................................................................__________g. -Mass of crucible, cover, and magnesium oxide ......................................................................__________g. CALCULATIONS:1. (A) Calculate the mass of magnesium used in the reaction and the mass of magnesium oxide produced.(B) Calculate the mass of the oxygen that reacted with the magnesium sample.(C) What is the mass of one mole of magnesium oxide? (MgO)(D) What is the mass of one mole of oxygen? (O2)*(E) How many moles of magnesium atoms are in the magnesium oxide?*(F) How many moles of oxygen atoms are there in the oxide?(G) What is the Mg:O mole ratio from your data?(H) What is the Mg:O atom ratio in magnesium oxide?2. (A) Using the masses of magnesium and magnesium oxide obtained experimentally, calculate the % Mg in magnesium oxide.(B) Using the simplest formula obtained in 1(H) calculate the % Mg in magnesium oxide.(C) Calculate your % error, assuming the true value is that obtained from the formula.DISCUSSION QUESTIONS:1. Write a skeletal (balanced) equation for the reaction of magnesium with oxygen gas to form magnesium oxide. You should use “s” or “g” after the formulas of the molecules to denote solids or gases.2. Air is a mixture of gases. When magnesium is burned in air, a small amount of it forms a solid called magnesium nitride (Mg3N2), is formed along with the oxide. Write a skeletal equation for this reaction. Nitrogen occurs as N2 in the atmosphere.__________ + __________ → __________3. If water is added to the magnesium nitride and the mixture is heated, the nitride is converted to the oxide. This was done during the experiment to be sure that we got just magnesium oxide as a product. Ammonia gas, NH3 is also produced in this reaction, and you may have detected its odor when you heated the mixture to boiling. Balance the equation for the reaction between magnesium nitride and water._____Mg3N2 + _____H2O → _____NH3 + _____MgO4. Explain the effect on your % Mg answer if the following errors had been made.(A) A small amount of Mg had remained unheated.(B) Some of the product spilled after heating but before weighing.(C) All of the water added in procedure step 4 was not boiled off.(D) The product obtained contained some Mg3N2。
2016+ACR适宜性标准:乳腺癌筛查ORIGINAL ARTICLEACR Appropriateness Criteria BreastCancer ScreeningMartha B.Mainiero,MD a,Ana Lourenco,MD a,Mary C.Mahoney,MD b,Mary S.Newell,MD c, Lisa Bailey,MD d,e,LoraD.Barke,DO f,Carl D’Orsi,MD c,Jennifer A.Harvey,MD g,Mary K.Hayes,MD h,Phan Tuong Huynh,MD i,Peter M.Jokich,MD j,Su-Ju Lee,MD b, Constance D.Lehman,MD,PhD k,David A.Mankoff,MD,PhD k,l,Joshua A.Nepute,MD m, Samir B.Patel,MD n,Handel E.Reynolds,MD o,M.Linda Sutherland,MD p, Bruce G.Haffty,MD qa Rhode Island Hospital,Providence,Rhode Island.b University of Cincinnati,Cincinnati,Ohio.c Emory University Hospital,Atlanta,Georgia.d Imagimed,LLC,Rockville,Maryland.e American College of Surgeons,Chicago,Illinois.f Invision Sally Jobe,Englewood,Colorado.g University of Virginia Medical Center,Charlottesville,Virginia.h Memorial Regional Hospital,Hollywood,Florida.i St Luke’s Episcopal Hospital,Houston,Texas.j Rush Breast Imaging Center,Chicago,Illinois.k University of Washington,Seattle,Washington.l Society of Nuclear Medicine and Molecular Imaging,Reston,Virginia. m University of Cincinnati MedicalCenter,Cincinnati,Ohio.n Radiology Inc,Mishawaka,Indiana.o Radiology Association of Atlanta,Atlanta,Georgia.p Newport Diagnostic Center,Newport Beach,California.q University of Medicine and Dentistry of New Jersey–Robert Wood Johnson Medical School,New Brunswick,New Jersey. Corresponding author and reprints:Martha B.Mainiero,MD,American College of Radiology,1891Preston WhiteDrive,Reston,VA20191; e-mail:mmainiero@/doc/bf3745523d1ec5da50e2524de518964bcf84d210.html.The ACR seeks and encourages collaboration with other organizations on the development of the ACR Appropriateness Criteria through society representation on expert panels.Participation by representatives from collaborating societies on the expert panel does not necessarily imply in-dividual or society endorsement of the?nal document.Dr Harvey reported that she is a shareholder in and has a research agree-ment with Hologic(Marlborough,Massachusetts).Dr Hayes reported that she is an international speaker for Hologic.a2013American College of Radiology 1546-1440/16/$36.00nSUMMARY OF LITERATURE REVIEW MammographyMammography is the only method of screening for breast cancer shown to decrease mortality[1-4]. Annual screening mammography is recommended starting at(1)40years of age for the general population;(2)25to30years of age for carriers of the breast cancer1gene and untested relatives of carriers;(3)25to30years of age or10years earlier than the age of the affected relatives at diagnosis (whichever is later)for women with?rst degree relatives with premenopausal breast cancer or for women with lifetime risk for breast cancer20%on the basis of family history;(4)8years afterradiation therapy but not before25years of age for women who received mantle radiation between the agesof10and30years;and(5)any age for women with biopsy-proven lobular neoplasia,atyp-ical ductal hyperplasia,ductal carcinoma in situ,or invasive breast cancer[5](see Variant1).However, mammography alone does not perform as well as mammography plus supplemental screening in certain subsets of women,particularly those with genetic predispositions to the disease and those with dense breasts[6-11].Therefore,supplemental screening is recommended in selected high-risk populations.MRIBreast MRI in high-risk women has been shown to have higher sensitivity than mammography,and the combina-tion of mammography and MRI in this population has the highest sensitivity[12-19].In a high-risk population, MRI and mammography combined have higher sensitivity (92.7%)than ultrasound and mammography combined (52%)[6].Therefore,in high risk women for whom supplemental screening is indicated,MRI is recommended when possible(see Variant2). Screening high-risk women using breast MRI is cost-effective[20,21],and the cost-effectiveness of screening MRI rises with increasing breast cancer risk. The American Cancer Society recommends screening breast MRI in certain high-risk women[22],and the ACR and the Society of Breast Imaging endorse those recommendations[5].Screening MRI is recommended in women with breast cancer1gene mutations and their untested?rst-degree relatives as well as women with lifetime risk for breast cancer 20%.Also included in this high-risk group are women who received radiation therapy to the chest between the ages of10and30years as well as women with other genetic syndromes that increase the risk for breast cancer(eg,Li-Fraumeni syndrome).For other women with intermediate risk for breast cancer,such as those with lifetime risk of15%to20%,personal histories of breast cancer,or histories of lobular neoplasia or atypical ductal hyperplasia,the use of screening MRI is an area of ongoing investigation [5,22].However,recent literature supports the use of screening MRI in addition to mammography in patients with personal histories of breast cancer[23] and lobular neoplasia[24](see Variant3). UltrasoundScreening ultrasound is indicated in high-risk patients who cannot tolerate MRI.Supplemental screening with ultrasound for women with intermediate risk and dense breasts is an option to increase cancer detection.However,handheld ultrasound screening by radiologists has a high false-positive rate and is time-consuming[25].Therefore,this may not be a cost-effective practice.The balance between cancer detection and the risk of a false positive result should be considered by women and their health care providers when considering the use of screening US or other ancillary screening examinations.Other Imaging ModalitiesThere is insuf?cient evidence to support the use of other imaging modalities,such as thermography, breast-speci?c gamma imaging,positron emission mammography,and optical imaging,for breast cancer screening[5].Radiation doses from breast-speci?c Radiologic Procedure Rating Comments RRL Mammographic screening9??MRI breast without and withcontrast3B Ultrasound breast2B MRI breast without contrast1B FDG-PEM199m T c sestamibi BSGI16?may be appropriate;7,8,and9?usually appropriate.BSGI?breast-speci?c gamma imaging;FDG?2-[18F]?uoro-2-deoxyglucose;PEM?positron emission mammography;RRL?relative radiation level.gamma imaging and positron emission mammography are 15to 30times higher than the dose from digital mammography [26,27],and they are not indicated for screening in their present form.SUMMARYn For high-risk women,annual screening mammo-graphy and contrast-enhanced MRI are both indicated.Ultrasound can be used for patients with contraindi-cations to MRI.n For intermediate-risk women,annual screening mammography is indicated.Contrast-enhanced MRI may be indicated in some patients.nFor average-risk women,annual screening mammog-raphy is indicated.ANTICIPATED EXCEPTIONSNephrogenic systemic ?brosis is a disorder with a scleroderma like presentation and a spectrum of manifestations that can range from limited clinical sequelae to fatality.It seems to be related to both underlying severe renal dysfunction and the admin-istration of gadolinium-based contrast agents.It has occurred primarily in patients on dialysis,rarely in patients with very limited glomerular ?ltration rates (ie,<30mL/min/1.73m 2),and almost never in other patients.There is growing literatureregardingRadiologic Procedure Rating CommentsRRL Mammographic screening 9??MRI breast without and with contrast7See statement regarding contrast,in text under “Anticipated Exceptions.”BUltrasound breast 5B FDG-PEM 299mT c sestamibi BSGI2MRI breast without contrast1Bspeci ?c gamma imaging;FDG ?2-[18F]?uoro-2-deoxyglucose;PEM ?positron emission mammography;RRL ?relative radiationlevel.Radiologic Procedure Rating CommentsRRL Mammographic screening9Beginning at age 25-30y or 10y before age of ?rst-degree relative when diagnosed with breast cancer or 8y after radiation therapy,but not before age 25y.Mammography and MRI are complementary examinations;both should be performed.??MRI breast without and with contrast9Mammography and MRI arecomplementary examinations;both should be performed.See statement regarding contrast,in text under “Anticipated Exceptions.”BUltrasound breast 6If patient cannot undergo MRI.B FDG-PEM 299mT c sestamibi BSGI2MRI breast without contrast 1B1;BSGI ?breast-speci ?c gamma imaging;FDG ?2-[18F]?uoro-2-deoxyglucose;PEM ?positron emission mammography;RRL relative radiation level.nephrogenic systemic ?brosis.Although some con-troversy and lack of clarity remain,there is a consensus that it is advisable to avoid all gadolinium-based contrast agents in dialysis-dependent patients unless the possible bene ?ts clearly outweigh the risk and to limit the type and amount in patients with estimated glomerular ?ltration rates <30mL/min/1.73m 2.For more information,please see the ACR ’s Manual on Contrast Media [28].RELATIVE RADIATION LEVEL INFORMATION Potential adverse health effects associated with radia-tion exposure are an important factor to consider when selecting the appropriate imaging procedure.Because there is a wide range of radiation exposures associated with different diagnostic procedures,a relative radia-tion level indication has been included for each im-aging examination.The relative radiation levels are based on effective dose,which is a radiation dose quantity that is used to estimate population total ra-diation risk associated with an imaging procedure.Patients in the pediatric age group are at inherently higher risk from exposure,both because of organ sensitivity and longer life expectancy (relevant to the long latency that appears to accompany radiation exposure).For these reasons,the relative radiation level dose estimate ranges for pediatric examinations are lower compared with those speci ?ed for adults (Table 1).Additional information regarding radiation dose assessment for imaging examinations can be found in ACR Appropriateness Criteria ò:Radiation Dose Assessment Introduction [29].For additional information on ACR Appropriateness Criteria,refer to/doc/bf3745523d1ec5da50e2524de518964bcf84d210.html /ac .REFERENCES1.Reduction in breast cancer mortality from organized service screening with mammography:1.Further con ?rmation with extended data.Cancer Epidemiol Biomarkers Prev 2006;15:45-51.2.Duffy SW,Tabar L,Chen HH,et al.The impact of organized mammography service screening on breast carcinoma mortality in seven Swedish counties.Cancer 2002;95:458-69.3.Hendrick RE,Smith RA,Rutledge JH III,Smart CR.Bene ?t of screening mammography in women aged 40-49:a new meta-analysis of randomized controlled trials.J Natl Cancer Inst Monogr 1997:87-92.4.Tabar L,Vitak B,Chen HH,Yen MF,Duffy SW,Smith RA.Beyond randomized controlled trials:organized mammographic screening sub-stantially reduces breast carcinoma mortality.Cancer 2001;91:1724-31.5.Lee CH,Dershaw DD,Kopans D,et al.Breast cancer screening with imaging:recommendations from the Society of Breast Imaging and the ACR on the use of mammography,breast MRI,breast ultrasound,and other technologies for the detection of clinically occult breast cancer.JAm Coll Radiol 2010;7:18-27.6.Berg WA.Tailored supplemental screening for breast cancer:what now and what next?Am J Roentgenol 2009;192:390-9.7.Brekelmans CT,Seynaeve C,Bartels CC,et al.Effectiveness of breast cancer surveillance in BRCA1/2gene mutation carriers and women with high familial risk.J Clin Oncol 2001;19:924-30.8.Chart PL,Franssen E.Management of women at increased risk for breast cancer:preliminary results from a new program.CMAJ 1997;157:1235-42.9.Macmillan RD.Screening women with a family history of breast cancer —results from the British Familial Breast Cancer Group.Eur J Surg Oncol 2000;26:149-52.10.Scheuer L,Kauff N,Robson M,et al.Outcome of preventive surgeryand screening for breast and ovarian cancer in BRCA mutation carriers.J Clin Oncol 2002;20:1260-8.11.Warner E,Plewes DB,Shumak RS,et /doc/bf3745523d1ec5da50e2524de518964bcf84d210.html parison of breast magnetic resonance imaging,mammography,andultrasound for sur-veillance ofwomenat high risk for hereditary breast cancer.J Clin Oncol 2001;19:3524-31.12.Hagen AI,Kvistad KA,Maehle L,et al.Sensitivity of MRI versusconventional screening in the diagnosis of BRCA-associated breast cancer in a national prospective series.Breast2007;16:367-74.13.Hartman AR,Daniel BL,Kurian AW,et al.Breast magnetic resonanceimage screening and ductal lavage in women at high genetic risk for breast carcinoma.Cancer 2004;100:479-89.14.Kriege M,Brekelmans CT,Boetes C,et al.Differences between ?rstand subsequent rounds of the MRISC breast cancer screening program for women with a familial or genetic predisposition.Cancer 2006;106:2318-26.15.Kuhl CK,Schrading S,Leutner CC,et al.Mammography,breastultrasound,and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer.J Clin Oncol 2005;23:8469-76.16.Leach MO,Boggis CR,Dixon AK,et al.Screening with magneticresonance imaging and mammography of a UK population at high familial risk of breast cancer:a prospective multicentre cohort study (MARIBS).Lancet 2005;365:1769-78.17.Lehman CD,Isaacs C,Schnall MD,et al.Cancer yield ofmammography,MR,and US in high-risk women:prospective multi-institution breast cancer screening study.Radiology 2007;244:381-8.18.Sardanelli F,Podo F,D ’Agnolo G,et al.Multicenter comparative mul-timodality surveillance of women at genetic-familial high risk for breast cancer (HIBCRIT study):interim results.Radiology 2007;242:698-715.19.Warner E,Plewes DB,Hill KA,et al.Surveillance of BRCA1and BRCA2mutation carriers with magnetic resonanceimaging,Relative Radiation Level Adult Effective Dose Estimate Range (mSv)Effective Dose Estimate Range(mSv)B 00?<0.1<0.03??0.1-10.03-0.31-100.3-3?10-303-10??30-10010-30tions cannot be made because the actual patient doses in these procedures vary as a function of a number of factors (eg,region of the body exposed to ionizing radiation,the imaging guidance that is used).The relative radiation levels for these examinations are designated as “varies.”ultrasound,mammography,and clinical breast examination.JAMA 2004;292:1317-25.20.Plevritis SK,Kurian AW,Sigal BM,et al.Cost-effectiveness ofscreening BRCA1/2mutation carriers with breast magnetic resonance imaging.JAMA2006;295:2374-84.21.Taneja C,Edelsberg J,Weycker D,Guo A,Oster G,Weinreb J.Costeffectiveness of breast cancer screening with contrast-enhanced MRI in high-risk women.J Am Coll Radiol2009;6:171-9. 22.Saslow D,Boetes C,Burke W,et al.American Cancer Societyguidelines for breast screening with MRI as an adjunct to mammog-raphy.CA Cancer J Clin2007;57:75-89.23.Brennan S,Liberman L,Dershaw DD,Morris E.Breast MRIscreening of women with a personal history of breast cancer.AJR Am J Roentgenol2010;195:510-6.24.Sung JS,Malak SF,Bajaj P,Alis R,Dershaw DD,Morris EA.Screening breast MR imaging in women with a history of lobular carcinoma in situ.Radiology2011;261:414-20.25.Berg WA,Blume JD,Cormack JB,et /doc/bf3745523d1ec5da50e2524de518964bcf84d210.html bined screening withultrasound and mammography vs mammography alone in women at elevated risk of breast cancer.JAMA2008;299:2151-63.26.Hendrick RE.Radiation doses and cancer risks from breast imagingstudies.Radiology2010;257:246-53.27.O’Connor MK,Li H,Rhodes DJ,Hruska CB,Clancy CB,Vetter RJ.Comparison of radiation exposure and associated radiation-induced cancer risks from mammography and molecular imaging of the breast.Medical physics2010;37:6187-98.28.American College of Radiology.Manual on contrast media v7.Available at:/doc/bf3745523d1ec5da50e2524de518964bcf84d210.html/w/media/ACR/Documents/PDF/ QualitySafety/Resources/Contrast%20Manual/FullManual.pdf.Accessed November14,2012.29.American College of Radiology.ACR Appropriateness Criteriaò:ra-diation dose assessment introduction.Availableat:/doc/bf3745523d1ec5da50e2524de518964bcf84d210.html /w/media/A27A29133302408BB86888EAFD460A1F.pdf.Accessed September19,2012.。
aCorresponding author: John Damilakis, Department of Medical Physics, Faculty of Medicine, University of Crete, P .O. Box 2208, 71003 Heraklion, Crete, Greece; phone: +30 2810 392569; fax: +30 2810 394933; email: john.damilakis@med.uoc.grCalculation of organ doses from breast cancer radiotherapy: a Monte Carlo studyT. Berris,1 M. Mazonakis,1 J. Stratakis,1 A. Tzedakis,2 A. Fasoulaki,3 J. Damilakis 1aDepartment of Medical Physics,1 Faculty of Medicine, University of Crete, Heraklion, Crete, Greece; Department of Medical Physics,2 University Hospital of Heraklion,H eraklion, Crete, Greece; Department of Radiotherapy and Oncology,3 UniversityH ospital of Heraklion, Heraklion, Crete, Greece john.damilakis@med.uoc.grReceived 28 April, 2012; accepted 16 August, 2012The current study aimed to: a) utilize Monte Carlo simulation methods for the assessment of radiation doses imparted to all organs at risk to develop secondary radiation induced cancer, for patients undergoing radiotherapy for breast cancer; and b) evaluate the effect of breast size on dose to organs outside the irradiation field. A simulated linear accelerator model was generated. The in-field accuracy of the simulated photon beam properties was verified against percentage depth dose (PDD) and dose profile measurements on an actual water phantom. Off-axis dose calculations were verified with thermoluminescent dosimetry (TLD) measurements on a humanoid physical phantom. An anthropomorphic mathematical phantom was used to simulate breast cancer radiotherapy with medial and lateral fields. The ef-fect of breast size on the calculated organ dose was investigated. Local differences between measured and calculated PDDs and dose profiles did not exceed 2% for the points at depths beyond the depth of maximum dose and the plateau region of the profile, respectively. For the penumbral regions of the dose profiles, the distance to agreement (DTA) did not exceed 2 mm. The mean difference between calculated out-of-field doses and TLD measurements was 11.4% ± 5.9%. The calculated doses to peripheral organs ranged from 2.32 cGy up to 161.41 cGy depending on breast size and thus the field dimensions applied, as well as the proximity of the organs to the primary beam. An increase to the therapeutic field area by 50% to account for the large breast led to a mean organ dose elevation by up to 85.2% for lateral exposure. The contralateral breast dose ranged between 1.4% and 1.6% of the prescribed dose to the tumor. Breast size affects dose deposition substantially.PACS numbers: 87.10.rt, 87.56.bd, 87.53.Bn, 87.55.K-, 87.55.ne, 87.56.jf, 87.56.J-Key words: breast cancer, radiotherapy, Monte Carlo simulation, organ dosesI. IntroduCtIonBreast tumors are the most common form of cancer in female patients of European countries, accounting for 30.9% of all incident cases.(1) The early cancer diagnosis with screening mam-mography and the recent advances in adjuvant therapy have reduced the mortality from breast malignancies.(2,3) The five-year survival rate of women suffering from breast carcinomas has reached to 79% in Europe.(4) Radiation therapy has a major role in the adjuvant management of breast carcinoma.(5) However, radiotherapy inevitably exposes to ionizing radiation the organs/tissues that are entirely or partially excluded from the treatment volume. Berrington et al.(6)JournAL oF APPLIEd CLInICAL MEdICAL PHYSICS, VoLuME 14, nuMBEr 1, 2013133133found a high relative risk for lung and esophageal cancer induction due to the high radiation dose of more than 1 Gy received by these organs. Stovall et al.(7) showed that women below 40 years of age have an elevated risk for developing contralateral breast cancer when the healthy breast dose exceeds 1 Gy. Huang and Mackillop(8) reported a high risk for radiotherapy-induced soft tissue sarcomas in the vicinity of the treated anatomic region. Therapeutic irradiation might be associated with a relatively increased risk for carcinogenesis in distant sites from the breast, such as salivary glands and ovaries, and it also has a significant effect on gynecological cancer incidence.(8,9)Scarce information exists in the literature about organ doses due to breast cancer radio-therapy. Previous studies dealing with healthy organ dose calculation from breast radiotherapy were performed using treatment planning systems and, therefore, their results were restricted to anatomic sites located very close to the treatment field.(10-12) Both in vivo and phantom measurements with thermoluminescent dosimeters (TLD) have also been employed for organ dose determination from breast cancer treatment.(6,7,13,14)In vivo experiments are limited to surface dose estimation. Phantom measurements require the placement of numerous TLD chips in a tissue-equivalent phantom to detect either the dose variation across each organ volume or the steep dose gradients observed in organs that were partly included in the primary beam. Thermoluminescent dosimetry may be considered as a time-consuming and labor-intensive procedure, often prone to high uncertainties. Furthermore, to the best of our knowledge, no study has yet dealt with the assessment of radiation dose to all organs at risk (OAR) to develop radiation induced cancer as recently defined by the International Commission on Radiologi-cal protection (ICRP).(15) The computerized Monte Carlo (MC) technique uses mathematical phantoms with realistic anatomic proportions, and it can provide a mean organ dose value by taking into account the radiation exposure inside the entire organ volume. Depending on the phantom employed, dose to all OARs for radiation induced cancer is feasible. Such dose estimations are useful from a radiation protection perspective.The current study was conducted to: a) simulate breast radiotherapy with a megavoltage beam using the Monte Carlo N-particle (MCNP) transport code in order to calculate the radiation dose to all OARs of patients undergoing radiotherapy for breast cancer, and b) evaluate the effect of breast size, and subsequently irradiation field size, on peripheral organ doses.II. MAtErIALS And MEtHodSA. Linear accelerator modelingA simulated model of a 6 MV medical linear accelerator (linac) (Philips SL 75/5, Philips/ Elekta, The Netherlands) was generated using the MCNP radiation transport code.(16) The model incorporated the basic beam modifying components, namely the heavy metal target, primary collimator, flattening filter, flattening filter holder, and secondary collimator. The ex-act geometry and materials specification of the linac head was derived by detailed blueprints provided exclusively by the manufacturer of the radiotherapeutic unit. To save simulation time, the implementation of the MC model was performed in two steps.(17) The linac parts included in the simulation are depicted in Fig. 1.In the first step of the linac simulation, a 6 MeV electron beam impinged perpendicularly on the heavy metal target. The energy spread and the radial intensity distribution of the electron beam were supposed to be 1 MeV and 1 mm full width at half maximum (FWHM), respec-tively.(18) The produced bremsstrahlung photons passed through the primary collimator and their forward peaked intensity distribution was compensated by the flattening filter. A circular tallying surface was defined just under the flattening filter holder. The surface was divided into 13 annular rings using the tally segmentation feature of the MCNP code. The width of each ring was 0.2 cm. The outer annular ring extended to the boundaries of the photon field defined by the extension of the conical surface, which incorporated the inner surface of the primaryJournal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013collimator. An F2 type tally was assigned to every annular ring. The flux of the photons cross-ing each ring was calculated and registered separately for 250 keV energy bins that spanned an energy range from 0 to 8 MeV . The energy cutoff feature of the MCNP code was used as a variance reduction technique. The cutoff energies were set to 10 and 500 keV for photons and electrons, respectively.(17) The number of source electrons needed for the detectors to produce statistically meaningful results with a relative error below 1% was 109. Many of those electrons performed more than 104 individual interactions before any kind of a cutoff occurred. An equal number of calculations was performed by the code in order to track their histories.In the second step of the simulation, the photon spectra calculated by each annular ring were re-emitted by a point source at the azimuthal angular intervals corresponding to each ring. The MCNP code provides an automatically uniform polar sampling for photon emission directions and, therefore, no polar photon emission parameters were specified. The secondary collimator was also included in the second part of the simulation. The distance between the blocks of the simulated secondary collimator and the point source was equal to the distance between the actual secondary collimator blocks and the upper surface of the target where the electron beam strikes. The conical beam emitted from the point source could be shaped into rectangular fields of any dimension with the aid of the simulated secondary collimator.B. Mathematical phantomThe BodyBuilder commercial software (version 1.30, White Rock Science, Los Alamos, NM) was used for the generation of an androgynous mathematical phantom with a height of 1.79m and weight of 73.54 kg.(19) The mathematical phantom included 21 of the 29 “main” and “re-mainder” OARs recently defined by the ICRP.(15) The eight missing organs were the following: prostate gland, salivary glands, lymph nodes, red bone marrow (RBM), bone surface (BS), extra-thoracic tissue, muscle, and oral mucosa.The radiation exposure of salivary glands was estimated by appropriate tally cells added to the three-dimensional geometry in accordance with the Van Ripper et al. report.(20) The radiation dose imparted to the soft tissue of the neck of the mathematical phantom was taken as the extrathoracic tissue dose. Muscle exposure was determined by the mass weighted mean doses imparted to all phantom’s tissues, excluding those of specifically defined organs.(21)TheF ig . 1. Descriptive representation of the linear accelerator (linac) simulation. The dashed line divides the geometryc onceptually and specifies the linac parts included in each simulation step.Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013mean radiation dose to the oral mucosa was assumed to be equal to the dose received by the sublingual salivary glands.The cells of the mathematical phantom corresponding to the skeleton consisted of solid bone tissue. There were no soft tissue structures to represent the RBM tissue. The mean dose imparted to the RBM, RBM was approximated by the equation:(1)BoneRBM D D where Bone is the mean dose to the solid osseous tissue, and the notationµencorresponds tothe mass-energy absorption coefficient of a material.(22) RBM tissue was considered to match the composition of soft tissue. The selected values of the mass-energy absorption coefficients for bone and soft tissue corresponded to the mean energy of the photon beam. The mean energy of the photon spectrum was calculated in the previously described first step of the linac simulation. The fractions of active RBM residing in various osseous structures needed for the calculation of the total organ dose were obtained by a previously published report.(21)The mathematical phantom had no specifically defined cells to represent the BS (i.e., the approximately 50 μm thick layer of trabecular endosteum of each bone (23)). The BS dose was considered to be equal to the dose received by the solid osseous tissue. This approach should give a relatively accurate dose estimate in the photon energy range above about 100 keV .(24) BS was considered to be uniformly distributed throughout the skeleton.The lymph node distribution in the mathematical phantom was approximated with the aid of a three-dimensional atlas of lymph node topography.(25) The dose to the lymph nodes was estimated either by the mass-weighted radiation doses received by organs or by specifically de-fined tally cells distributed in the lymphoid regions of the simulated human body (Table 1).The arms of the mathematical phantom used in this study were incorporated in the trunk. To represent the real irradiation of the left breast, a left arm was designed and positioned over the mathematical phantom’s head. The osseous tissue of the left arm bone which was originally inside the trunk was substituted with soft tissue.T able 1. Lymphatic distribution in the mathematical phantom and regions of dose calculation to lymph nodes. Lymph Node Cluster % of the Total Lymph Node VolumeRegion of Dose Calculation Head & neck 1% Parotid salivary glands, thyroid a Head & neck 24.1% Neck soft tissue a Chest 8.8% Heart aAxilla 6% Left and right axilla b Abdomen 2.5% Stomach aAbdomen 41.1% Small intestine a Pelvis 13.5% Upper pelvis bPelvis3%Upper leg muscle baThe radiation dose to lymph nodes was approximated by the mass-weighted organ doses.b Tally cells were added for lymph node dose calculation.C. Verification of the simulated beam modelC.1 Comparison of Monte Carlo results with ionization chamber measurements The setup of the second part of the simulation was utilized for the calculation of percent depth dose (PDD) of the MC beam model. Depth dose curves were calculated for square 10 × 10 cm2 and 20 × 20 cm2 radiation fields on a simulated 50 × 50 × 50 cm3 water phantom. The SSD was set to 100 cm and *F8 type tally cells were embedded in regular distances inside the water phantom volume to score the energy deposition at various depths. The tally cells were cylindri-cal and coaxial with the simulated therapeutic beam. Their height was equal to 0.2 cm. A radius of 1 cm was chosen to increase tally cell surfaces that were perpendicular to the beam’s axis and to subsequently improve the simulation efficiency. The number of source photon histories needed to achieve a relative error less than 1% for all detectors was 2.4 × 108.For the same field sizes, beam profiles were calculated using an array of cylindrical F6 type tallies embedded in the water volume. F6 tallies calculate collision kerma, which is a quantity proportional to the dose at depths equal to the depth of maximum dose (d max) and beyond. The axes of the tally cells were laid on the middle plane of the water phantom and they were parallel to the beam’s axis. The cylinders had a radius of 0.5 cm and they were 1 cm long. The array could be moved along the direction of the beam’s axis, and dose profiles were calculated at d max and at a depth of 10 cm (d10). The d max was determined based on the previously described PDD calculations. A detector error below 1% was obtained by using 2 × 108 source photon histories. The calculated PDDs and dose profiles were directly compared with corresponding curves generated on a physical water phantom (RFA-300, Scanditronix Wellhofer, Uppsala, Sweden) with dimensions 49.5 × 49.5 × 49.5 cm3. Ionization measurements were made with a 0.13 cc calibrated chamber (CC13-S, Scanditronix Wellhofer). The dose evaluation to the penumbral, high-dose gradient parts of the beam profiles was performed with the distance to agreement (DTA) method.(26)C.2 Comparison of Monte Carlo results with TLD measurementsA RANDO humanoid phantom (Alderson Research Labs, Stanford, CA) and thermolumines-cence dosimetry were employed to measure out-of-field radiation doses. The phantom has been constructed by tissue-equivalent material and it represents a human body trunk from the upper third of the thighs to the vertex of an average individual with a height of 173 cm and a weight of 73.5 kg. A left breast made of wax was placed on the RANDO phantom.(27) The dimensions of the breast were similar with those of the tissue in the mathematical phantom. The physical phantom was irradiated with the same setup used in MC simulations. The tangential field size used was 10 × 16 cm2.Calcium fluoride thermoluminescent dosimeters (TLD-200, Harshaw, Solon, OH), suitable for scattered dose measurements, were positioned in the RANDO phantom. The calibration of the crystals was made on the same linear accelerator with that used for direct measurements and modeled by the MCNP code. The procedure of the TLD calibration and reading has been previously described.(28) The standard deviation of the sensitivity factors was less than 4% for the TLD batch used in this study. The crystals were positioned at distances of 15 cm, 20 cm, 25cm, 30 cm, 35 cm, and 40 cm from the field isocenter. The depth from the anterior phantom’s surface varied from 9 to 11 cm. The TLD measurements were compared with out-of-field dose calculations. Six spherical MCNP F6 tallies with a radius of 1 cm were positioned inside the mathematical phantom at the same distances and depths with those referred for TLD crys-tals. The simulations performed needed 2 × 108 histories to achieve an error less than 7% for all tallies.d. Breast radiation therapy simulationThe second part of the linac beam simulation in conjunction with the mathematical phantom was used to determine organ doses attributable to tangential irradiation of the left breast c onsistingJournal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013of a pair of medial and lateral fields. The effect of the breast size on the out-of-field organ was investigated in our study. Dose calculations were initially carried out using the standard field dimensions of 10 × 16 cm2. Moreover, organ doses were determined using an increased field size of 12 × 20 cm2 coupled to a large-sized breast to evaluate the effect of scattering on a larger breast to the peripheral organ doses. To achieve this simulation, the original breast size of the phantom, which represents a small breast of 168.50 cm3, was changed to 1354.4 cm3 to represent very closely the average large breast size.(29) Similar ranges of breast sizes, as well as irradiation field sizes, have been documented elsewhere in the literature.(30,31) For both breast sizes, the tumor site was located at the center of the left breast tissue and the source-to-skin distance (SSD) was set to 100 cm. The gantry angles for the medial and the lateral treatment field corresponding to the small breast size were 286° and 115°, respectively. Due to the dif-ferent anatomy of the phantom with large breast size, the respective medial and lateral field angles were 301° and 128°. In all cases the opposing posterior field borders were aligned. The contralateral breast was very close, but not exposed, to the primary beam. This setup ensured the detection of the maximum scattered dose to the contralateral breast. The treatment setup was defined by a radiotherapist experienced in the management of breast carcinoma. Organ doses were calculated for equally weighted field irradiations giving 50.4 Gy to the tumor site. Doses to OARs were calculated by assigning an F6 type tally to each geometrical cell rep-resenting an organ or a part of it. The F6 tally calculates the average collision kerma at every geometrical cell. In this study, the approach of Gu et al.(32) was followed and collision kerma was considered equal to absorbed dose for the relatively low energy of 6 MV photons. The dose to each organ was calculated as a weighted average of the doses received by the various fractions of the organ throughout the phantom’s body. Organs or organ parts exposed by the primary beam were excluded from dose calculation.(33) The dose to the RBM and the BS was calculated excluding the dose received by the ribs. Lung exposure was approximated by the dose to the right lung, since the left lung was partially inside the primary beam. The dose to the trunk and left breast skin was not taken into account for the total skin dose calculation. The radiation dose to tissues between the ribs and skin was also excluded from the determination of muscle exposure. The breast dose corresponded to the contralateral breast, which was outside the primary photon beam. The relative error of all dose calculations was kept below 7% even for cells far outside the primary beam. To keep the error that low, the number of source photon histories was 2 × 108 for each projection.III. rESuLtSA. Linear accelerator modelingThe photon spectrum passing through the flattening filter holder was found to be “softer” as the distance from the central beam axis increased. Figure 2 shows the spectrum obtained by the central circular detector and the outer annular detector to illustrate the variation of the photon spectrum as a function of the distance from the beam’s axis. The outmost annular detector received relatively more low-energy photons than the central detector. In contrast, the central detector collected more high-energy photons than the outer ring. Figure 3 shows the mean photon energy observed at various distances from the beam’s axis at the detectors level exem-plifying the radial softening of the spectrum. The mean energy of the spectrum calculated by the outmost detector was found to be 11.7% lower than that calculated by the central circular tally. The total photon fluence just below the flattening filter holder was 3.5 photons for every 100 source electrons. These results are in agreement with previously published data.(17)Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013B. Verification of the simulated beam modelFigure 4 shows a comparison of the calculated and measured PDD curve for the 20 × 20 cm 2 field. The doses were normalized to d 10. Local differences at depths beyond d max were less than 2%. Similar results were also obtained for the smaller field size of 10 × 10 cm 2. Figures 5 and 6 present superimposed measured and calculated dose profiles for the 20 × 20 cm 2 radiation field at d max and d 10, respectively. In the plateau region of the profiles, the local differences did not exceed the value of 2%. For the collimated field of 10 × 10 cm 2, the maximum local differ-ence between measured and calculated profiles was also less than 2% in the plateau region. In the penumbra region of all profiles considered, spatial differences (DTA) up to 2 mm were observed between calculations and measurements. The above discrepancy should be consid-ered as acceptable.(34) Regarding the out-of-field point doses, no systematic differences were observed between the MCNP calculations and TLD measurements. The mean difference was equal to 11.4% ± 5.9%.F ig . 2. Photon spectra calculated by the central circular and the outmost annular detector. The photon spectrum was “softer” towards the edges of the field.ig filter holder.Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013F ig . 4. Superimposed measured and calculated percentage depth dose (PDD) curves for the 20 × 20 cm 2 photon field. The inset shows the local differences of the calculated values from the corresponding measured PDD values. The horizontal dashed lines mark the ± 2% limit of acceptance. The vertical dashed line marks the depth of maximum dose.F ig . 5. Superimposed measured and calculated lateral dose profiles for the 20 × 20 cm 2 photon field at depth of maximum dose (d max ). The inset shows the local differences of the calculated values from the corresponding measured dose profile values. The horizontal dashed lines mark the ± 2% limit of acceptance. The vertical dashed lines limit the plateau regionof the profiles.Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013C. Breast radiation therapy simulationThe mean radiation doses to all OARs associated with radiotherapy for breast cancer with tan-gential lateral and medial fields are summarized in Table 2. These tabular data show the organ dose variation with the breast size and the field size employed. The mean dose increase was found to be equal to 67.4% and 85.2% for the medial and lateral field irradiations, respectively. For a treatment course delivering 50.4 Gy to the tumor site with a field size of 10 × 16 cm 2, organ dose varied from 2.32 cGy in urinary bladder to 161.41 cGy in heart. Dose variation with the increased field dimensions of 12 × 20 cm 2 ranged from 4.06 cGy in urinary bladder to 141.59 cGy to the thymus. The heart and thymus were the remainder organs receiving the largest amounts of radiation. The highest exposure to a main organ was observed for the con-tralateral breast with an absorbed dose of 69.57 cGy to 83.10 cGy, depending upon the breast size and the matching field size employed. The absorbed dose to the contralateral breast was 1.4% and 1.6% of the prescribed dose to the tumor for the small and large breast radiotherapy simulation, respectively.F ig . 6. Superimposed measured and calculated lateral dose profiles for the 20 × 20 cm 2 photon field at 10 cm depth (d 10). The inset shows the local differences of the calculated values from the corresponding measured dose profile values. The hori-zontal dashed lines mark the ± 2% limit of acceptance. The vertical dashed lines limit the plateau region of theprofiles.Journal of Applied Clinical Medical Physics, Vol. 14, no. 1, 2013IV. dISCuSSIonIn this study, a MC method was employed to produce a model of a 6 MV medical linac photon beam. The two-step implementation of the model provided a photon beam that could be used for any radiotherapy simulation without the need to resimulate the whole linac geometry. The measured and calculated PDD values were in a very good agreement at depths beyond d max , with local differences not exceeding 2%. Relatively large discrepancies up to 16% were ob-served at depths shallower than d max . Similar discrepancies reaching up to 15%, attributed to perturbations caused by the measurement chamber and inaccurate simulation of the treatment head, have been previously observed.(18,35-38) The calculated dose values agreed very well with the measured ones in the plateau regions of the profiles with differences of less than 2%. The discrepancies observed at the abrupt dose fall-off regions of the profiles might be due to the poor sampling achieved by the relatively large tally detector sizes used in MC simulations. It should be noticed that the differences between measurements and calculations in the profile regions with high-dose gradients were found to be acceptable based on the 2 mm criterion that was also used by Bednarz and Xu.(34) The moderate agreement between the measured and calculated out-of-field doses should be attributed to the uncertainty of TLD dosimetry, to error in MC calculations, and to differences in size and composition of the RANDO phantom with the mathematical humanoid phantom.The absorbed dose to OARs from left breast radiotherapy was calculated in this study. Treat-ment of the right breast may lead to different dose values, especially for organs not located inT able 2. Organ doses due to radiotherapy for breast cancer using two different field sizes. Organ Dose (cGy)Lateral FieldMedial Field10×16 cm 2 12×20 cm 210×16 cm 2 12×20 cm 2Main organs Female breast 37.05 50.18 32.53 32.92Stomach 16.63 41.89 14.77 36.25Esophagus 17.98 33.00 13.94 20.49Thyroid 9.97 21.58 11.28 16.93Liver9.22 16.20 7.55 10.18Red bone marrow 7.28 13.20 5.93 9.61Lung4.90 7.06 4.825.04Bone surface 4.22 7.48 3.766.08Salivary glands 4.357.65 3.87 5.98Colon 2.39 4.39 2.43 4.01Skin 1.96 6.73 2.05 7.95Brain 2.06 3.38 1.64 2.63Ovaries1.58 3.14 1.512.53Urinary bladder 1.04 1.73 1.28 2.33Remainder Organs Heart 83.49 86.18 77.93 44.84Thymus 84.24 102.88 41.67 38.71Pancreas 12.24 25.39 10.04 19.83Spleen11.27 24.23 10.48 25.26Lymphatic nodes 10.96 14.83 10.42 10.60Adrenals 8.83 17.46 6.69 11.63Gall bladder5.82 11.04 5.90 8.52Extra-thoracic tissue 5.70 10.82 5.12 8.00Kidneys 4.87 9.27 3.656.55Oral mucosa 3.637.12 3.59 5.61Small intestine 2.66 4.90 2.67 4.41Uterus 1.56 2.71 1.59 2.66Muscle1.242.441.273.34。