oral contraceptives-very low estrogen dosagespros and
- 格式:rtf
- 大小:39.04 KB
- 文档页数:6
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use YASMIN safely and effectively. See full prescribing information for YASMIN.YASMIN (drospirenone/ethinyl estradiol) tablets, for oral useInitial U.S. Approval: 2001WARNING: CIGARETTE SMOKING AND SERIOUSCARDIOVASCULAR EVENTSSee full prescribing information for complete boxed warning• Women over 35 years old who smoke should not use Yasmin. (4) • Cigarette smoking increases the risk of serious cardiovascular events from combination oral contraceptive (COC) use. (4)----------------------------RECENT MAJOR CHANGES-------------------------Warnings and Precautions, Hyperkalemia (5.2) 5/2015----------------------------INDICATIONS AND USAGE---------------------------Yasmin is an estrogen/progestin COC indicated for use by women to prevent pregnancy. (1)---------------------DOSAGE AND ADMINISTRATION---------------------• Take one tablet daily by mouth at the same time every day. (2.1)• Tablets must be taken in the order directed on the blister pack. (2.1)---------------------DOSAGE FORMS AND STRENGTHS----------------------Yasmin consists of 28 film-coated, biconvex tablets in the following order (3): • 21 yellow tablets, each containing 3 mg drospirenone (DRSP) and0.03 mg ethinyl estradiol (EE)• 7 inert white tablets-------------------------------CONTRAINDICATIONS-----------------------------• Renal impairment (4)• Adrenal insufficiency (4)• A high risk of arterial or venous thrombotic diseases (4)• Undiagnosed abnormal uterine bleeding (4)• Breast cancer or other estrogen-or progestin-sensitive cancer (4)• Liver tumors or liver disease (4)• Pregnancy (4)-----------------------WARNINGS AND PRECAUTIONS-----------------------• Vascular risks: Stop Yasmin if a thrombotic event occurs. Stop at least 4 weeks before and through 2 weeks after major surgery. Start no earlierthan 4 weeks after delivery, in women who are not breastfeeding (5.1).COCs containing DRSP may be associated with a higher risk of venous thromboembolism (VTE) than COCs containing levonorgestrel or some other progestins. Before initiating Yasmin in a new COC user or awoman who is switching from a contraceptive that does not containDRSP, consider the risks and benefits of a DRSP-containing COC inlight of her risk of a VTE (5.1).•Hyperkalemia: DRSP has anti-mineralocorticoid activity. Do not use in patients predisposed to hyperkalemia. Check serum potassiumconcentration during the first treatment cycle in women on long-termtreatment with medications that may increase serum potassiumconcentration. (5.2, 7.1, 7.2)•Liver disease: Discontinue Yasmin if jaundice occurs. (5.4)•High blood pressure: Do not prescribe Yasmin for women with uncontrolled hypertension or hypertension with vascular disease. (5.5) •Carbohydrate and lipid metabolic effects: Monitor prediabetic and diabetic women taking Yasmin. Consider an alternate contraceptivemethod for women with uncontrolled dyslipidemia. (5.7) •Headache: Evaluate significant change in headaches and discontinue Yasmin if indicated. (5.8)•Uterine bleeding: Evaluate irregular bleeding or amenorrhea. (5.9)------------------------------ADVERSE REACTIONS------------------------------The most frequent adverse reactions (≥2%) are premenstrual syndrome (13.2%), headache /migraine (10.7%), breast pain/tenderness/discomfort (8.3%), nausea/vomiting (4.5%), abdominal pain/tenderness/discomfort(2.3%), mood changes (2.3%). (6.1)To report SUSPECTED ADVERSE REACTIONS, contact Bayer HealthCare Pharmaceuticals Inc. at 1-888-842-2937 or FDA at 1-800FDA-1088 or /medwatch------------------------------DRUG INTERACTIONS------------------------------Drugs or herbal products that induce certain enzymes (for example, CYP3A4) may decrease the effectiveness of COCs or increase breakthrough bleeding. Counsel patients to use a back-up or alternative method of contraception when enzyme inducers are used with COCs. (7.1)-----------------------USE IN SPECIFIC POPULATIONS-----------------------Nursing mothers: Not recommended; can decrease milk production. (8.3) See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.Revised: 5/2015FULL PRESCRIBING INFORMATION: CONTENTS*WARNING: CIGARETTE SMOKING AND SERIOUS CARDIOVASCULAR EVENTS1 INDICATIONS AND USAGE2 DOSAGE AND ADMINISTRATION2.1 How to Take Yasmin2.2 How to Start Yasmin2.3 Advice in Case of Gastrointestinal Disturbances3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 Thromboembolic Disorders and Other Vascular Problems5.2 Hyperkalemia5.3 Carcinoma of the Breasts and Reproductive Organs5.4 Liver Disease5.5 High Blood Pressure5.6 Gallbladder Disease5.7 Carbohydrate and Lipid Metabolic Effects5.8 Headache5.9 Bleeding Irregularities5.10 COC Use Before or During Early Pregnancy5.11 Depression5.12 Interference with Laboratory Tests5.13 Monitoring5.14 Other Conditions6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Postmarketing Experience7 DRUG INTERACTIONS7.1 Effects of Other Drugs on Combined Oral Contraceptives7.2 Effects of Combined Oral Contraceptives on Other Drugs7.3 Interference with Laboratory Tests8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use8.6 Patients with Renal Impairment8.7 Patients with Hepatic Impairment8.8 Race10 OVERDOSAGE11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility14 CLINICAL STUDIES15 REFERENCES16 HOW SUPPLIED/STORAGE AND HANDLING16.1 How Supplied16.2 Storage17 PATIENT COUNSELING INFORMATION*Sections or subsections omitted from the full prescribing information are not listed__________________________________________________________________________________________________ FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGEYasmin® is indicated for use by women to prevent pregnancy.2 DOSAGE AND ADMINISTRATION2.1 How to Take YasminTake one tablet by mouth at the same time every day. The failure rate may increase when pills are missed or taken incorrectly.To achieve maximum contraceptive effectiveness, Yasmin must be taken as directed, in the order directed on the blister pack. Single missed pills should be taken as soon as remembered.2.2 How to Start YasminInstruct the patient to begin taking Yasmin either on the first day of her menstrual period (Day 1 Start) or on the first Sunday after the onset of her menstrual period (Sunday Start).Day 1 StartDuring the first cycle of Yasmin use, instruct the patient to take one yellow Yasmin daily, beginning on Day 1 of her menstrual cycle. (The first day of menstruation is Day 1.) She should take one yellow Yasmin daily for 21 consecutive days, followed by one white tablet daily on Days 22 through 28. Yasmin should be taken in the order directed on the package at the same time each day, preferably after the evening meal or at bedtime with some liquid, as needed. Yasmin can be taken without regard to meals. If Yasmin is first taken later than the first day of the menstrual cycle, Yasmin should not be considered effective as a contraceptive until after the first 7 consecutive days of product administration. Instruct the patient to use a non-hormonal contraceptive as back-up during the first 7 days. The possibility of ovulation and conception prior to initiation of medication should be considered.Sunday StartDuring the first cycle of Yasmin use, instruct the patient to take one yellow Yasmin daily, beginning on the first Sunday after the onset of her menstrual period. She should take one yellow Yasmin daily for 21 consecutive days, followed by one white tablet daily on Days 22 through 28. Yasmin should be taken in the order directed on the package at the same time each day, preferably after the evening meal or at bedtime with some liquid, as needed. Yasmin can be taken without regard to meals. Yasmin should not be considered effective as a contraceptive until after the first 7 consecutive days of product administration. Instruct the patient to use a non-hormonal contraceptive as back-up during the first 7 days. The possibility of ovulation and conception prior to initiation of medication should be considered.The patient should begin her next and all subsequent 28-day regimens of Yasmin on the same day of the week that she began her first regimen, following the same schedule. She should begin taking her yellow tablets on the next day after ingestion of the last white tablet, regardless of whether or not a menstrual period has occurred or is still in progress. Anytime a subsequent cycle of Yasmin is started later than the day following administration of the last white tablet, the patient should use another method of contraception until she has taken a yellow Yasmin daily for seven consecutive days. When switching from a different birth control pillWhen switching from another birth control pill, Yasmin should be started on the same day that a new pack of the previous oral contraceptive would have been started.When switching from a method other than a birth control pillWhen switching from a transdermal patch or vaginal ring, Yasmin should be started when the next application would have been due. When switching from an injection, Yasmin should be started when the next dose would have been due. When switching from an intrauterine contraceptive or an implant, Yasmin should be started on the day of removal. Withdrawal bleeding usually occurs within 3 days following the last yellow tablet. If spotting or breakthrough bleeding occurs while taking Yasmin, instruct the patient to continue taking Yasmin by the regimen described above. Counsel her that this type of bleeding is usually transient and without significance; however, advise her that if the bleeding is persistent or prolonged, she should consult her healthcare provider.Although the occurrence of pregnancy is low if Yasmin is taken according to directions, if withdrawal bleeding does not occur, consider the possibility of pregnancy. If the patient has not adhered to the prescribed dosing schedule (missed one or more active tablets or started taking them on a day later than she should have), consider the possibility of pregnancy at the time of the first missed period and take appropriate diagnostic measures. If the patient has adhered to the prescribed regimen and misses two consecutive periods, rule out pregnancy. Discontinue Yasmin if pregnancy is confirmed.The risk of pregnancy increases with each active yellow tablet missed. For additional patient instructions regarding missed pills, see the “WHAT TO DO IF YOU MISS PILLS” section in the FDA-Approved Patient Labeling. If breakthrough bleeding occurs following missed tablets, it will usually be transient and of no consequence. If the patient misses one or more white tablets, she should still be protected against pregnancy provided she begins taking a new cycle of yellow tablets on the proper day.For postpartum women who do not breastfeed or after a second trimester abortion, start Yasmin no earlier than 4 weeks postpartum due to the increased risk of thromboembolism. If the patient starts Yasmin postpartum and has not yet had a period, evaluate for possible pregnancy, and instruct her to use an additional method of contraception until she has taken Yasmin for 7 consecutive days.2.3 Advice in Case of Gastrointestinal DisturbancesIn case of severe vomiting or diarrhea, absorption may not be complete and additional contraceptive measures should be taken. If vomiting occurs within 3-4 hours after tablet-taking, this can be regarded as a missed tablet.3 DOSAGE FORMS AND STRENGTHSYasmin (drospirenone/ethinyl estradiol) tablets are available in blister packs.Each blister pack contains 28 film-coated, round, bi-convex tablets in the following order:• 21 yellow tablets each containing 3 mg drospirenone (DRSP) and 0.03 mg ethinyl estradiol (EE) embossed with a “DO” in a regular hexagon on one side• 7 inert white tablets embossed with a “DP” in a regular hexagon on one side4 CONTRAINDICATIONSDo not prescribe Yasmin to women who are known to have the following:• Renal impairment• Adrenal insufficiency• A high risk of arterial or venous thrombotic diseases. Examples include women who are known to: o Smoke, if over age 35 [see Boxed Warning and Warnings and Precautions (5.1)]o Have deep vein thrombosis or pulmonary embolism, now or in the past [see Warnings and Precautions (5.1)] o Have cerebrovascular disease [see Warnings and Precautions (5.1)]o Have coronary artery disease [see Warnings and Precautions (5.1)]o Have thrombogenic valvular or thrombogenic rhythm diseases of the heart (for example, subacute bacterial endocarditis with valvular disease, or atrial fibrillation) [see Warnings and Precautions (5.1)] o Have inherited or acquired hypercoagulopathies [see Warnings and Precautions (5.1)]o Have uncontrolled hypertension [see Warnings and Precautions (5.5)]o Have diabetes mellitus with vascular disease [see Warnings and Precautions (5.7)]o Have headaches with focal neurological symptoms or have migraine headaches with or without aura if over age 35 [see Warnings and Precautions (5.8)]• Undiagnosed abnormal uterine bleeding [see Warnings and Precautions (5.9)]• Breast cancer or other estrogen-or progestin-sensitive cancer, now or in the past [see Warnings and Precautions(5.3)]• Liver tumor (benign or malignant) or liver disease [see Warnings and Precautions (5.4) and Use in Specific Populations (8.7)]• Pregnancy, because there is no reason to use COCs during pregnancy [see Warnings and Precautions (5.10) and Use in Specific Populations (8.1)]5 WARNINGS AND PRECAUTIONS5.1 Thromboembolic Disorders and Other Vascular ProblemsStop Yasmin if an arterial or venous thrombotic (VTE) event occurs.Based on presently available information on Yasmin, DRSP-containing COCs may be associated with a higher risk of venous thromboembolism (VTE) than COCs containing the progestin levonorgestrel or some other progestins. Epidemiologic studies that compared the risk of VTE reported that the risk ranged from no increase to a three-fold increase. Before initiating use of Yasmin in a new COC user or a woman who is switching from a contraceptive that does not contain DRSP, consider the risks and benefits of a DRSP-containing COC in light of her risk of a VTE. Known risk factors for VTE include smoking, obesity, and family history of VTE, in addition to other factors that contraindicate use of COCs [see Contraindications (4)].A number of studies have compared the risk of VTE for users of Yasmin to the risk for users of other COCs, including COCs containing levonorgestrel. Those that were required or sponsored by regulatory agencies are summarized in Table 1.Table 1: Estimates (Hazard Ratios) of Venous Thromboembolism Risk in Current Users of Yasmin Compared to Users of Oral Contraceptives that Contain Other Progestins Epidemiologic Study Comparator Product Hazard Ratio (HR) (Author, Year of (all are low-dose COCs; with (95% CI) Publication) ≤0.04 mg of EE)Population Studiedi3 Ingenix All COCs available in the US HR: 0.9 (Seeger 2007)Initiators, including newusers aduring the conduct of the study b (0.5-1.6)All COCs available in Europe HR: 0.9 EURAS during the conduct of the study c (0.6-1.4) (Dinger 2007)Initiators, including new users a Levonorgestrel/EE HR: 1.0(0.6-1.8)“FDA-funded study” (2011)New users aAll users(i.e., initiation and continuing use of study combination hormonal contraception) Other COCs available during thecourse of the study dLevonorgestrel/0.03 mg EEOther COCs available during thecourse of the study dLevonorgestrel/0.03 mg EEHR: 1.8(1.3-2.4)HR: 1.6(1.1-2.2)HR: 1.7(1.4-2.1)HR: 1.5(1.2-1.8)a) “New users” -no use of combination hormonal contraception for at least the prior 6 monthsb) Includes low-dose COCs containing the following progestins: norgestimate, norethindrone, levonorgestrel,desogestrel, norgestrel, medroxyprogesterone, or ethynodiol diacetatec) Includes low-dose COCs containing the following progestins: levonorgestrel, desogestrel, dienogest, chlormadinoneacetate, gestodene, cyproterone acetate, norgestimate, or norethindroned) Includes low-dose COCs containing the following progestins: norgestimate, norethindrone, or levonorgestrelIn addition to these “regulatory studies,” other studies of various designs have been conducted. Overall, there are two prospective cohort studies (see Table 1): the US post-approval safety study Ingenix [Seeger 2007], the European post-approval safety study EURAS (European Active Surveillance Study) [Dinger 2007]. An extension of the EURAS study, the Long-Term Active Surveillance Study (LASS), did not enroll additional subjects, but continued to assess VTE risk. There are three retrospective cohort studies: one study in the US funded by the FDA (see Table 1), and two from Denmark [Lidegaard 2009, Lidegaard 2011]. There are two case-control studies: the Dutch MEGA study analysis [van Hylckama Vlieg 2009] and the German case-control study [Dinger 2010]. There are two nested case-control studies that evaluated the risk of non-fatal idiopathic VTE: the PharMetrics study [Jick 2011] and the GPRD study [Parkin 2011]. The results of all of these studies are presented in Figure 1.Figure 1: VTE Risk with Yasmin Relative to LNG-Containing COCs (adjusted risk#)Risk ratios displayed on logarithmic scale; risk ratio < 1 indicates a lower risk of VTE for DRSP, > 1 indicates an increased risk of VTE for DRSP.*Comparator “Other COCs”, including LNG-containing COCs† LASS is an extension of the EURAS study#Some adjustment factors are indicated by superscript letters: a) Current heavy smoking, b) hypertension, c) obesity, d) family history, e) age, f) BMI, g) duration of use, h) VTE history, i) period of inclusion, j) calendar year, k) education, l) length of use, m) parity, n) chronic disease, o) concomitant medication, p) smoking, q) duration of exposure, r) site(References: Ingenix [Seeger 2007]1, EURAS (European Active Surveillance Study) [Dinger 2007]2, LASS (Long-Term Active Surveillance Study) [Dinger, unpublished document on file], FDA-funded study [Sidney 2011]3, Danish [Lidegaard 2009]4, Danish reanalysis [ Lidegaard 2011]5, MEGA study [van Hylckama Vlieg 2009]6, German Case-Control study [Dinger 2010]7, PharMetrics [Jick 2011]8, GPRD study [Parkin 2011]9)Although the absolute VTE rates are increased for users of hormonal contraceptives compared to non-users, the rates during pregnancy are even greater, especially during the post-partum period (see Figure 2). The risk of VTE in women using COCs has been estimated to be 3 to 9 per 10,000 woman-years. The risk of VTE is highest during the first year of use. Data from a large, prospective cohort safety study of various COCs suggest that this increased risk, as compared to that in non-COC users, is greatest during the first 6 months of COC use. Data from this safety study indicate that the greatest risk of VTE is present after initially starting a COC or restarting (following a 4 week or greater pill-free interval) the same or a different COC.The risk of thromboembolic disease due to oral contraceptives gradually disappears after COC use is discontinued. Figure 2 shows the risk of developing a VTE for women who are not pregnant and do not use oral contraceptives, for women who use oral contraceptives, for pregnant women, and for women in the postpartum period. To put the risk of developing a VTE into perspective: If 10,000 women who are not pregnant and do not use oral contraceptives are followed for one year, between 1 and 5 of these women will develop a VTE.Figure 2 Likelihood of Developing a VTEIf feasible, stop Yasmin at least 4 weeks before and through 2 weeks after major surgery or other surgeries known to have an elevated risk of thromboembolism.Start Yasmin no earlier than 4 weeks after delivery, in women who are not breastfeeding. The risk of postpartum thromboembolism decreases after the third postpartum week, whereas the risk of ovulation increases after the third postpartum week.Use of COCs also increases the risk of arterial thromboses such as strokes and myocardial infarctions, especially in women with other risk factors for these events.COCs have been shown to increase both the relative and attributable risks of cerebrovascular events (thrombotic and hemorrhagic strokes), although, in general, the risk is greatest among older (>35 years of age), hypertensive women who also smoke. COCs also increase the risk for stroke in women with other underlying risk factors.Oral contraceptives must be used with caution in women with cardiovascular disease risk factors.Stop Yasmin if there is unexplained loss of vision, proptosis, diplopia, papilledema, or retinal vascular lesions. Evaluate for retinal vein thrombosis immediately. [See Adverse Reactions (6).]5.2 HyperkalemiaYasmin contains 3 mg of the progestin DRSP, which has anti-mineralocorticoid activity, including the potential for hyperkalemia in high-risk patients, comparable to a 25 mg dose of spironolactone. Yasmin is contraindicated in patients with conditions that predispose to hyperkalemia (that is, renal impairment, hepatic impairment, and adrenal insufficiency). Women receiving daily, long-term treatment for chronic conditions or diseases with medications that may increase serum potassium concentration should have their serum potassium concentration checked during the first treatment cycle. Medications that may increase serum potassium concentration include ACE inhibitors, angiotensin–II receptor antagonists, potassium-sparing diuretics, potassium supplementation, heparin, aldosterone antagonists, and NSAIDs. Consider monitoring serum potassium concentration in high-risk patients who take a strong CYP3A4 inhibitor long-term and concomitantly. Strong CYP3A4 inhibitors include azole antifungals (e.g. ketoconazole, itraconazole, voriconazole), HIV/HCV protease inhibitors (e.g., indinavir, boceprevir), and clarithromycin [see Clinical Pharmacology (12.3)].5.3 Carcinoma of the Breasts and Reproductive OrgansWomen who currently have or have had breast cancer should not use Yasmin because breast cancer is a hormonallysensitive tumor.There is substantial evidence that COCs do not increase the incidence of breast cancer. Although some past studies have suggested that COCs might increase the incidence of breast cancer, more recent studies have not confirmed such findings. Some studies suggest that COCs are associated with an increase in the risk of cervical cancer or intraepithelial neoplasia. However, there is controversy about the extent to which these findings may be due to differences in sexual behavior and other factors.5.4 Liver DiseaseDiscontinue Yasmin if jaundice develops. Steroid hormones may be poorly metabolized in patients with impaired liver function. Acute or chronic disturbances of liver function may necessitate the discontinuation of COC use until markers of liver function return to normal and COC causation has been excluded.Hepatic adenomas are associated with COC use. An estimate of the attributable risk is 3.3 cases/100,000 COC users. Rupture of hepatic adenomas may cause death through intra-abdominal hemorrhage.Studies have shown an increased risk of developing hepatocellular carcinoma in long-term (> 8 years) COC users. However, the attributable risk of liver cancers in COC users is less than one case per million users.Oral contraceptive-related cholestasis may occur in women with a history of pregnancy-related cholestasis. Women with a history of COC-related cholestasis may have the condition recur with subsequent COC use.5.5 High Blood PressureFor women with well-controlled hypertension, monitor blood pressure and stop Yasmin if blood pressure rises significantly. Women with uncontrolled hypertension or hypertension with vascular disease should not use COCs.An increase in blood pressure has been reported in women taking COCs, and this increase is more likely in older women and with extended duration of use. The incidence of hypertension increases with increasing concentration of progestin. 5.6 Gallbladder DiseaseStudies suggest a small increased relative risk of developing gallbladder disease among COC users.5.7 Carbohydrate and Lipid Metabolic EffectsCarefully monitor prediabetic and diabetic women who are taking Yasmin. COCs may decrease glucose tolerance in a dose-related fashion.Consider alternative contraception for women with uncontrolled dyslipidemia. A small proportion of women will have adverse lipid changes while on COCs.Women with hypertriglyceridemia, or a family history thereof, may be at an increased risk of pancreatitis when using COCs.5.8 HeadacheIf a woman taking Yasmin develops new headaches that are recurrent, persistent, or severe, evaluate the cause and discontinue Yasmin if indicated.An increase in frequency or severity of migraine during COC use (which may be prodromal of a cerebrovascular event) may be a reason for immediate discontinuation of the COC.5.9 Bleeding IrregularitiesUnscheduled (breakthrough or intracyclic) bleeding and spotting sometimes occur in patients on COCs, especially during the first three months of use. If bleeding persists or occurs after previously regular cycles, check for causes such as pregnancy or malignancy. If pathology and pregnancy are excluded, bleeding irregularities may resolve over time or with a change to a different COC.Data from ten contraceptive efficacy clinical trials (N=2,467) show that the percent of women who took Yasmin and experienced unscheduled bleeding decreased over time from 12% at cycle 2 to 6% (cycle 13). A total of 24 subjects out of 2,837 in the Yasmin trials (<1%) discontinued due to bleeding complaints. These are described as metrorrhagia, vaginal hemorrhage, menorrhagia, abnormal withdrawal bleeding, and menometrorrhagia.The average duration of scheduled bleeding episodes in the majority of subjects (86%-88%) was 4-7 days. Women who use Yasmin may experience absence of withdrawal bleeding, even if they are not pregnant. Based on subject diaries fromcontraceptive efficacy trials, during cycles 2–13, 1-11% of women per cycle experienced no withdrawal bleeding. Some women may encounter post-pill amenorrhea or oligomenorrhea, especially when such a condition was pre-existent.If withdrawal bleeding does not occur, consider the possibility of pregnancy. If the patient has not adhered to the prescribed dosing schedule (missed one or more active tablets or started taking them on a day later than she should have), consider the possibility of pregnancy at the time of the first missed period and take appropriate diagnostic measures. If the patient has adhered to the prescribed regimen and misses two consecutive periods, rule out pregnancy.5.10 COC Use Before or During Early PregnancyExtensive epidemiological studies have revealed no increased risk of birth defects in women who have used oral contraceptives prior to pregnancy. Studies also do not suggest a teratogenic effect when COCs are taken inadvertently during early pregnancy, particularly in so far as cardiac anomalies and limb-reduction defects are concerned.The administration of oral contraceptives to induce withdrawal bleeding should not be used as a test for pregnancy [see Use in Specific Populations (8.1)].5.11 DepressionWomen with a history of depression should be carefully observed and Yasmin discontinued if depression recurs to a serious degree.5.12 Interference with Laboratory TestsThe use of COCs may change the results of some laboratory tests, such as coagulation factors, lipids, glucose tolerance, and binding proteins. Women on thyroid hormone replacement therapy may need increased doses of thyroid hormone because serum concentrations of thyroid-binding globulin increase with use of COCs [see Drug Interactions (7.2)].DRSP causes an increase in plasma renin activity and plasma aldosterone induced by its mild anti-mineralocorticoid activity.5.13 MonitoringA woman who is taking COCs should have a yearly visit with her healthcare provider for a blood pressure check and for other indicated healthcare.5.14 Other ConditionsIn women with hereditary angioedema, exogenous estrogens may induce or exacerbate symptoms of angioedema. Chloasma may occasionally occur, especially in women with a history of chloasma gravidarum. Women with a tendency to chloasma should avoid exposure to the sun or ultraviolet radiation while taking COCs.6 ADVERSE REACTIONSThe following serious adverse reactions with the use of COCs are discussed elsewhere in the labeling:•Serious cardiovascular events and stroke [see Boxed Warning and Warnings and Precautions (5.1)]•Vascular events [see Warnings and Precautions (5.1)]•Liver disease [see Warnings and Precautions (5.4)]Adverse reactions commonly reported by COC users are:•Irregular uterine bleeding•Nausea•Breast tenderness•Headache6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, the adverse reaction rates observed cannot be directly compared to rates in other clinical trials and may not reflect the rates observed in practice.。

732015 V ol.36 No.273·综 述·口服避孕药避孕效果可靠,应用广泛。
自第一个复方口服避孕药Enovid 于上世纪60年代面世以来,人们不断研发雌激素含量更低的避孕药以及各种新型孕激素,以降低药物不良反应,提高避孕效果。
口服避孕药主要成分为合成雌激素和孕激素,前者主要为高效乙炔雌二醇(炔雌醇)和炔雌醚。
不同种类和性能各异的孕激素组成的各种避孕药,作用机制包括:抑制排卵、改变宫颈黏液的黏稠度、改变输卵管蠕动、改变子宫内膜形态及功能等多个方面[1]。
其能抑制垂体分泌促性腺激素从而抑制排卵。
目前口服避孕药中的孕激素主要是人工合成的甾体激素。
按化学结构可分为:17α-羟孕酮类、19-去甲睾酮类以及17α-螺甾内酯类等新型孕激素。
本文按孕激素的种类及特点简要概述各种口服避孕药孕激素在口服避孕药中应用王蓓颖,王海云(同济大学附属第一妇婴保健院计划生育科,上海 200040)摘要:口服避孕药对人类的计划生育作出了巨大贡献,其主要成分为合成雌激素和孕激素,前者主要为高效的乙炔雌二醇 (炔雌醇)和炔雌醚。
本文简要综述不同种类和性能各异的孕激素组成的多种避孕药的特点,以便临床合理选用。
关键词:口服避孕药;雌激素;孕激素;计划生育中图分类号:R977.1+2 文献标志码:A 文章编号:1672-9188(2015)02-0073-04收稿日期:2014-08-29;修回日期:2014-10-29作者简介:王蓓颖,主治医师,现主要从事计划生育和女性内分泌疾病的诊治工作。
Progestin used for steroid oral contraceptivesWANG Bei-yin, WANG Hai-yun(Department of Family Planning, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai 200040, China )Abstract: The steroid oral contraceptives contribute enormous merit for family planning. It consists of syntheticestrogen and progestin, such as ethinly estradiol (EE) and different progestin. This review describes different oral contraceptives for rational selective usage.Key words: oral contraceptive; estrogen; progestin; family planning的特点和临床应用。


Unit 10 Gynecological Diseases第10单元妇科疾病Pre-reading Activitiesang预习工作. Read the following clinical situation and decide what kind of intervention you will suggest and what disease the patient might be suffering from.阅读下面的临床表现然后决定你将建议做那些干预,病人可能患了那种疾病。
A 55-year-old woman comes to the outpatient office complaining of pelvic pressure and ab-dominal fullness. Her last menstrual period (LMP) was 3 years ago.A、女性,55岁,门诊病人,住宿骨盆压迫感,腹部胀满。
末次月经为3年前。
在阅读这个文章前先理解一下术语。
Try to understand the following terms before you read the text.gynecological [ igainiks'bc^ikal] adj. of or relating to or practicing gynecology $3产科医学的n.ovarian [ ou'vesrisn] adj. of or involving the ovaries [解音I门卵巢的malignancy [ ms'lignsnsi]( medicine) a malignant state ;progressive and resistant to treatment and tending to cause "death 恶性(肿瘤等)salpingectomy [ iS2elpin'd3ekt3mi J surgical removal of one or both Fallopian tubes [妇产]输卵管切除术hysterectomy [ ihista'rektsmi] n. surgical removal of the uterus 子宫切除Text A Ovarian Gancort FocusAbout Ovarian Cancer iSigns and Symptomst Causes| DiagnosisClassificationStaging | Treatment+ Prevention主题A 卵巢癌重点:卵巢癌的相关体征和症状病因诊断分级分期|治疗预防About Ovarian Cancer关于卵巢癌Ovarian cancer is a cancerous growth arising from the ovary. Ovarian Cancer is the second most• 1 •• 2 •新编临床实用医学英语commonly diagnosed gynecologic malignancy,the deadliest gynecologic malignancy,and the fourth leading cause of cancer-related deaths in women in the USA. About 1 in 70 women eventually develop ovarian cancer,and 1 in 100 women dies of it. Ovarian cancer affects pre-dominantly perimenopausal and postmenopausal women.卵巢癌是一种子宫增生性癌。

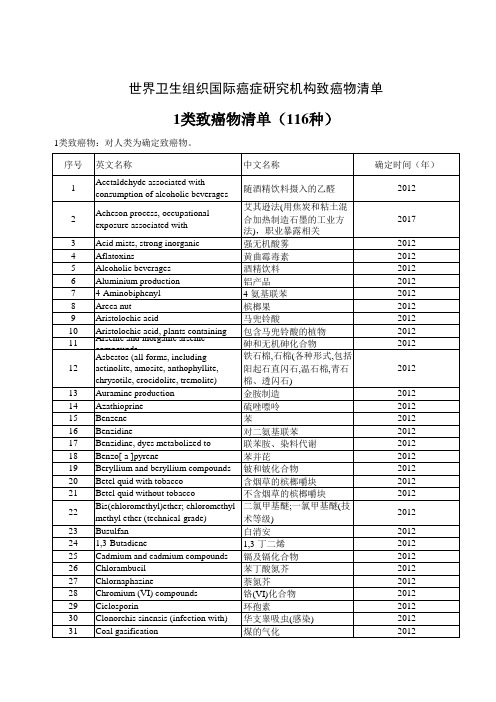
致癌物分类IARC根据对人类和对实验动物致癌性资料,以及在实验系统和人类其他有关的资料(包括癌前病变、肿瘤病理学、遗传毒性、结构—活性关系,代谢和动力学,理化参数及同类的生物因子)进行综合评价,将环境因子和类别、混合物及暴露环境与人类癌症的关系分为下列五类四组:第一类:致癌组1,对人类是致癌物。
对人类致癌性证据充分者属于本组。
如吸烟和二手烟。
第二类:很可能致癌组2,对人类是很可能或可能致癌物。
又分为两组,即组2A和组2B。
组2A,对人类很可能(probably)是致癌物,指对人类致癌性证据有限。
对实验动物致癌性证据充分。
如生产艺术玻璃、常用电吹风的理发师。
第三类:可能致癌组2B,对人类是可能(possible)致癌物,指对人类致癌性证据有限,对实验动物致癌性证据并不充分;或指对人类致癌性证据不足,对实验动物致癌性证据充分。
第四类:未知组3,现有的证据不能对人类致癌性进行分类。
第五类:很可能不致癌组4,对人类可能是非致癌物。
编辑本段致癌物五类明细表IARC专家组在2010年1月最新报告对834种环境因子和类别、混合物及暴露环境与人类癌症关系评价结果,其中组1有100种,组1B有68种,组2B有246种,组3有516种,组4有1种。
IARC对化学物质引起人类癌症危险性评价,是目前公认的权威性资料。
在要了解某种化学物的致癌性时,应首先查阅IARC的资料(网址http:193.51.164.11/monoeval/crthgr01.html)。
毒理学网 2010年1月12日Overall Evaluations of Carcinogenicity to HumansGroup 1: Carcinogenic to humans (100)Agents and groups of agents4-Aminobiphenyl [92-67-1] (Vol. 1, Suppl. 7; 1987)Arsenic [7440-38-2] and arsenic compounds (Vol. 23, Suppl. 7; 1987) (NB:This evaluation applies to the group of compounds as a whole and notnecessarily to all individual compounds within the group)Asbestos [1332-21-4] (Vol. 14, Suppl. 7; 1987)Azathioprine [446-86-6] (Vol. 26, Suppl. 7; 1987)Benzene [71-43-2] (Vol. 29, Suppl. 7; 1987)Benzidine [92-87-5] (Vol. 29, Suppl. 7; 1987)Benzo[a]pyrene [50-32-8] (Vol. 32, Suppl. 7, Vol. 92; in preparation)(NB: Overall evaluation upgraded from 2B to 1 based on mechanistic andother relevant data)Beryllium [7440-41-7] and beryllium compounds (Vol. 58; 1993) N,N-Bis(2-chloroethyl)-2-naphthylamine (Chlornaphazine)[494-03-1] (Vol.4, Suppl. 7; 1987)Bis(chloromethyl)ether [542-88-1] and chloromethyl methyl ether [107-30-2](technical-grade)(Vol. 4, Suppl. 7; 1987)1,4-Butanediol dimethanesulfonate (Busulphan; Myleran)[55-98-1] (Vol. 4,Suppl. 7; 1987)Cadmium [7440-43-9] and cadmium compounds (Vol. 58; 1993)Chlorambucil [305-03-3] (Vol. 26, Suppl. 7; 1987)1-(2-Chloroethyl)-3-(4-methylcyclohexyl)-1-nitrosourea (Methyl-CCNU;Semustine) [13909-09-6] (Suppl. 7; 1987)Chromium[VI] (Vol. 49; 1990)Ciclosporin [79217-60-0] (Vol. 50; 1990)Cyclophosphamide [50-18-0] [6055-19-2] (Vol. 26, Suppl. 7; 1987)Diethylstilboestrol [56-53-1] (Vol. 21, Suppl. 7; 1987)Epstein-Barr virus (Vol. 70; 1997)Erionite [66733-21-9] (Vol. 42, Suppl. 7; 1987)Estrogen-progestogen menopausal therapy (combined) (Vol. 72, Vol. 91; inpreparation)Estrogen-progestogen oral contraceptives (combined) (Vol. 72, Vol. 91; inpreparation)(NB: There is also convincing evidence in humans that these agents confera protective effect against cancer in the endometrium and ovary)Estrogens, nonsteroidal (Suppl. 7; 1987) (NB: This evaluation applies tothe group of compounds as a whole and not necessarily to all individualcompounds within the group)Estrogens, steroidal (Suppl. 7; 1987) (NB: This evaluation applies tothe group of compounds as a whole and not necessarily to all individualcompounds within the group)Estrogen therapy, postmenopausal (Vol. 72; 1999)Ethylene oxide [75-21-8] (Vol. 60; 1994) (NB: Overall evaluation upgradedfrom 2A to 1 with supporting evidence from other relevant data) Etoposide [33419-42-0] in combination with cisplatin and bleomycin (Vol.76; 2000)Formaldehyde [50-00-0] (Vol. 88; 2006)Gallium arsenide [1303-00-0] (Vol. 86; 2006)[Gamma Radiation: see X- and Gamma (g)-Radiation]Helicobacter pylori (infection with) (Vol. 61; 1994)Hepatitis B virus (chronic infection with) (Vol. 59; 1994)Hepatitis C virus (chronic infection with) (Vol. 59; 1994)Human immunodeficiency virus type 1 (infection with) (Vol. 67; 1996)Human papillomavirus types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59and 66 (Vol. 64, Vol. 90; in preparation) (NB: The HPV types that havebeen classified as carcinogenic to humans can differ by an order ofmagnitude in risk for cervical cancer)Human T-cell lymphotropic virus type I (Vol. 67; 1996)Melphalan [148-82-3] (Vol. 9, Suppl. 7; 1987)8-Methoxypsoralen (Methoxsalen) [298-81-7] plus ultraviolet A radiation(Vol. 24, Suppl. 7; 1987)MOPP and other combined chemotherapy including alkylating agents (Suppl.7; 1987)Mustard gas (Sulfur mustard) [505-60-2] (Vol. 9, Suppl. 7; 1987) 2-Naphthylamine [91-59-8] (Vol. 4, Suppl. 7; 1987)Neutrons (Vol. 75; 2000) (NB: Overall evaluation upgraded from 2B to 1with supporting evidence from other relevant data)Nickel compounds (Vol. 49; 1990)N‘-Nitrosonornicotine (NNN) [16543-55-8] and4-(N-Nitrosomethylamino)-1-(3-pyridyl)- 1-butanone (NNK) [64091-91-4](Vol. 37, Suppl. 7, Vol. 89; in preparation) (NB: Overall evaluationupgraded from 2B to 1 based on mechanistic and other relevant data)[Oestrogen: see Estrogen]Opisthorchis viverrini (infection with) (Vol. 61; 1994)[Oral contraceptives, combined estrogen-progestogen: seeEstrogen-progestogen oral contraceptives (combined)]Oral contraceptives, sequential (Suppl. 7; 1987)Phosphorus-32, as phosphate (Vol. 78; 2001)Plutonium-239 and its decay products (may contain plutonium-240 and otherisotopes), as aerosols (Vol. 78; 2001)Radioiodines, short-lived isotopes, including iodine-131, from atomicreactor accidents and nuclear weapons detonation (exposure duringchildhood) (Vol. 78; 2001)Radionuclides, a-particle-emitting, internally deposited (Vol. 78; 2001)(NB: Specific radionuclides for which there is sufficient evidence forcarcinogenicity to humans are also listed individually as Group 1 agents)Radionuclides, b-particle-emitting, internally deposited (Vol. 78; 2001)(NB: Specific radionuclides for which there is sufficient evidence forcarcinogenicity to humans are also listed individually as Group 1 agents)Radium-224 and its decay products (Vol. 78; 2001)Radium-226 and its decay products (Vol. 78; 2001)Radium-228 and its decay products (Vol. 78; 2001)Radon-222 [10043-92-2] and its decay products (Vol. 43, Vol. 78; 2001)Schistosoma haematobium (infection with) (Vol. 61; 1994)Silica [14808-60-7], crystalline (inhaled in the form of quartz orcristobalite from occupational sources) (Vol. 68; 1997)Solar radiation (Vol. 55; 1992)Talc containing asbestiform fibres (Vol. 42, Suppl. 7; 1987) Tamoxifen [10540-29-1] (Vol. 66; 1996) (NB: There is also conclusiveevidence that tamoxifen reduces the risk of contralateral breast cancer)2,3,7,8-Tetrachlorodibenzo-para-dioxin [1746-01-6] (Vol. 69; 1997) (NB:Overall evaluation upgraded from 2A to 1 with supporting evidence fromother relevant data)Thiotepa [52-24-4] (Vol. 50; 1990)Thorium-232 and its decay products, administered intravenously as acolloidal dispersion of thorium-232 dioxide (Vol. 78; 2001) Treosulfan [299-75-2] (Vol. 26, Suppl. 7; 1987)Vinyl chloride [75-01-4] (Vol. 19, Suppl. 7; 1987)X- and Gamma (g)-Radiation (Vol. 75; 2000)MixturesAflatoxins (naturally occurring mixtures of) [1402-68-2] (Vol. 56, Vol.82; 2002)Alcoholic beverages (Vol. 44; 1988)Areca nut (Vol. 85; 2004) (NB: Overall evaluation based on human data,animal data, and mechanistic and other relevant data)Betel quid with tobacco (Vol. 85; 2004)Betel quid without tobacco (Vol. 85; 2004)Coal-tar pitches [65996-93-2] (Vol. 35, Suppl. 7; 1987)Coal-tars [8007-45-2] (Vol. 35, Suppl. 7; 1987)Herbal remedies containing plant species of the genus Aristolochia (Vol.82; 2002)Household combustion of coal, indoor emissions from (Vol. 95; inpreparation)Mineral oils, untreated and mildly treated (Vol. 33, Suppl. 7; 1987)Phenacetin, analgesic mixtures containing (Suppl. 7; 1987) Salted fish (Chinese-style) (Vol. 56; 1993)Shale-oils [68308-34-9] (Vol. 35, Suppl. 7; 1987)Soots (Vol. 35, Suppl. 7; 1987)Tobacco烟草, smokeless (Vol. 37, Suppl. 7, Vol. 89; in preparation)Wood dust (Vol. 62; 1995)Exposure circumstancesAluminium production (Vol. 34, Suppl. 7; 1987)Arsenic in drinking-water (Vol. 84; 2004)Auramine, manufacture of (Suppl. 7; 1987)Boot and shoe manufacture and repair (Vol. 25, Suppl. 7; 1987)Chimney sweeping (Vol. 92; in preparation)Coal gasification (Vol. 34, Suppl. 7, Vol. 92; in preparation) Coal-tar distillation (Vol. 92; in preparation)Coke production (Vol. 34, Suppl. 7, Vol. 92; in preparation) Furniture and cabinet making (Vol. 25, Suppl. 7; 1987)Haematite mining (underground) with exposure to radon (Vol. 1, Suppl. 7;1987)Involuntary smoking (exposure to secondhand or‘environmental‘ tobaccosmoke) (Vol. 83; 2004)Iron and steel founding (Vol. 34, Suppl. 7; 1987)Isopropyl alcohol manufacture (strong-acid process) (Suppl. 7; 1987)Magenta, manufacture of (Vol. 57; 1993)Painter (occupational exposure as a) (Vol. 47; 1989)Paving and roofing with coal-tar pitch (Vol. 92; in preparation) Rubber industry (Vol. 28, Suppl. 7; 1987)Strong-inorganic-acid mists containing sulfuric acid (occupationalexposure to) (Vol. 54; 1992)Tobacco smoking 吸烟and tobacco smoke 二手烟(Vol. 83; 2004) Last updated: 13 December 2006Group 2A: Probably carcinogenic to humans(68)Agents and groups of agentsAcrylamide [79-06-1] (Vol. 60; 1994) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Adriamycin [23214-92-8] (Vol. 10, Suppl. 7; 1987) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)Androgenic (anabolic) steroids (Suppl. 7; 1987)Aristolochic acids (naturally occurring mixtures of) (Vol. 82; 2002)Azacitidine [320-67-2] (Vol. 50; 1990) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data)Benzidine-based dyes (Suppl. 7; 1987) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Bischloroethyl nitrosourea (BCNU) [154-93-8] (Vol. 26, Suppl.7; 1987)1,3-Butadiene [106-99-0] (Vol. 71; 1999)Captafol [2425-06-1] (Vol. 53; 1991) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Chloramphenicol [56-75-7] (Vol. 50; 1990) (NB: Overall evaluationupgraded from 2B to 2A with supporting evidence from other relevant data)a-Chlorinated toluenes (benzal chloride [98-87-3], benzotrichloride[98-07-7], benzyl chloride [100-44-7]) and benzoyl chloride [98-88-4](combined exposures) (Vol. 29, Suppl. 7, Vol. 71; 1999)1-(2-Chloroethyl)-3-cyclohexyl-1-nitrosourea (CCNU)[13010-47-4](Vol. 26,Suppl. 7; 1987)(NB: Overall evaluation upgraded from 2B to 2A with supporting evidencefrom other relevant data)4-Chloro-ortho-toluidine [95-69-2] (Vol. 77; 2000)Chlorozotocin [54749-90-5] (Vol. 50; 1990) (NB: Overall evaluationupgraded from 2B to 2A with supporting evidence from other relevant data)Cisplatin [15663-27-1] (Vol. 26, Suppl. 7; 1987) (NB: Overall evaluationupgraded from 2B to 2A with supporting evidence from other relevant data)Clonorchis sinensis (infection with) (Vol. 61; 1994) (NB: Overallevaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)Cyclopenta[cd]pyrene [27208-37-3] (Vol. 32, Suppl. 7, Vol. 92; inpreparation) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence from other relevant data)Dibenz[a,h]anthracene [53-70-3] (Vol. 32, Suppl. 7, Vol. 92; in preparation) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence from other relevant data)Dibenzo[a,l]pyrene [191-30-0] (Vol. 32, Suppl. 7, Vol. 92; in preparation)(NB: Overall evaluation upgraded from 2B to 2A with supporting evidencefrom other relevant data)Diethyl sulfate [64-67-5] (Vol. 54, Vol. 71; 1999) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)Dimethylcarbamoyl chloride [79-44-7] (Vol. 12, Suppl. 7, Vol. 71; 1999)(NB: Overall evaluation upgraded from 2B to 2A with supporting evidencefrom other relevant data)1,2-Dimethylhydrazine [540-73-8] (Vol. 4, Suppl. 7, Vol. 71; 1999) (NB:Overall evaluation upgraded from 2B to 2A with supporting evidence fromother relevant data)Dimethyl sulfate [77-78-1] (Vol. 4, Suppl. 7, Vol. 71; 1999) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence fromother relevant data)Epichlorohydrin [106-89-8] (Vol. 11, Suppl. 7, Vol. 71; 1999) (NB:Overall evaluation upgraded from 2B to 2A with supporting evidence fromother relevant data)Ethylene dibromide [106-93-4] (Vol. 15, Suppl. 7, Vol. 71; 1999) (NB:Overall evaluation upgraded from 2B to 2A with supporting evidence fromother relevant data)N-Ethyl-N-nitrosourea [759-73-9] (Vol. 17, Suppl.7; 1987) (NB: Overallevaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)Etoposide [33419-42-0] (Vol. 76; 2000) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Glycidol [556-52-5] (Vol. 77; 2000) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Indium phosphide [22398-80-7] (Vol. 86; 2006) (NB: Overall evaluationupgraded from 2B to 2A)IQ (2-Amino-3-methylimidazo[4,5-f]quinoline) [76180-96-6] (Vol. 56; 1993)(NB: Overall evaluation upgraded from 2B to 2A with supporting evidencefrom other relevant data)Kaposi‘s sarcoma herpesvirus/human herpesvirus 8 (Vol. 70; 1997)Lead compounds, inorganic (Vol. 87; 2006)5-Methoxypsoralen [484-20-8] (Vol. 40, Suppl. 7; 1987) (NB: Overallevaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)4,4′-Methylene bis(2-chloroaniline) (MOCA) [101-14-4] (Vol.57; 1993)(NB: Overall evaluation upgraded from 2B to 2A with supporting evidencefrom other relevant data)Methyl methanesulfonate [66-27-3] (Vol. 7, Suppl. 7, Vol. 71; 1999)(NB: Overall evaluation upgraded from 2B to 2A with supporting evidencefrom other relevant data)N-Methyl-N′-nitro-N-nitrosoguanidine(MNNG) [70-25-7] (Vol. 4, Suppl. 7;1987) (NB: Overall evaluation upgraded from 2B to 2A with supportingevidence from other relevant data)N-Methyl-N-nitrosourea [684-93-5] (Vol. 17, Suppl.7; 1987) (NB: Overallevaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)Nitrate or nitrite (ingested) under conditions that result in endogenousnitrosation (Vol. 94; in preparation)Nitrogen mustard [51-75-2] (Vol. 9, Suppl. 7; 1987)N-Nitrosodiethylamine [55-18-5] (Vol. 17, Suppl. 7; 1987) (NB: Overallevaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)N-Nitrosodimethylamine [62-75-9] (Vol. 17, Suppl. 7; 1987) (NB: Overallevaluation upgraded from 2B to 2A with supporting evidence from otherrelevant data)Phenacetin [62-44-2] (Vol. 24, Suppl. 7; 1987)Procarbazine hydrochloride [366-70-1] (Vol. 26, Suppl. 7; 1987) (NB:Overall evaluation upgraded from 2B to 2A with supporting evidence fromother relevant data)Styrene-7,8-oxide [96-09-3] (Vol. 60; 1994) (NB: Overall evaluationupgraded from 2B to 2A with supporting evidence from other relevant data)Teniposide [29767-20-2] (Vol. 76; 2000) (NB: Overall evaluationupgraded from 2B to 2A with supporting evidence from other relevant data)Tetrachloroethylene [127-18-4] (Vol. 63; 1995)ortho-Toluidine [95-53-4] (Vol. 77; 2000)Trichloroethylene [79-01-6] (Vol. 63; 1995)1,2,3-Trichloropropane [96-18-4] (Vol. 63; 1995)Tris(2,3-dibromopropyl) phosphate [126-72-7] (Vol. 20, Suppl. 7, Vol.71;1999) (NB: Overall evaluation upgraded from 2B to 2A with supportingevidence from other relevant data)Ultraviolet radiation A (Vol. 55; 1992) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Ultraviolet radiation B (Vol. 55; 1992) (NB: Overall evaluation upgradedfrom 2B to 2A with supporting evidence from other relevant data) Ultraviolet radiation C (Vol. 55; 1992) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence from other relevant data)Vinyl bromide [593-60-2] (Vol. 39, Suppl. 7, Vol. 71; 1999) (NB: Overall evaluation upgraded from 2B to 2A with supporting evidence fromother relevant data)Vinyl fluoride [75-02-5] (Vol. 63; 1995)MixturesCreosotes [8001-58-9] (Vol. 35, Suppl. 7, Vol. 92; in preparation)Diesel engine exhaust (Vol. 46; 1989)High-temperature frying, emissions from (Vol. 95; in preparation)Hot mate (Vol. 51; 1991)Household combustion of biomass fuel (primarily wood), indoor emissionsfrom (Vol. 95; in preparation)Non-arsenical insecticides (occupational exposures in spraying andapplication of) (Vol. 53; 1991)Polychlorinated biphenyls [1336-36-3] (Vol. 18, Suppl. 7; 1987) Exposure circumstancesArt glass, glass containers and pressed ware (manufacture of) (Vol. 58;1993)Carbon electrode manufacture (Vol. 92; in preparation)Cobalt metal with tungsten carbide (Vol. 86; 2006)Hairdresser or barber (occupational exposure as a) (Vol. 57; 1993)Petroleum refining (occupational exposures in) (Vol. 45; 1989) Sunlamps and sunbeds (use of) (Vol. 55; 1992)Last updated: 29 November 2006Group 2B: Possibly carcinogenic to humans (246)Agents and groups of agentsA-a-C (2-Amino-9H-pyrido[2,3-b]indole) [26148-68-5] (Vol. 40, Suppl. 7;1987)Acetaldehyde [75-07-0] (Vol. 36, Suppl. 7, Vol. 71; 1999)Acetamide [60-35-5] (Vol. 7, Suppl. 7, Vol. 71; 1999)Acrylonitrile [107-13-1] (Vol. 71; 1999)AF-2 [2-(2-Furyl)-3-(5-nitro-2-furyl)acrylamide] [3688-53-7] (Vol.31,Suppl. 7; 1987)Aflatoxin M1 [6795-23-9] (Vol. 56; 1993)para-Aminoazobenzene [60-09-3] (Vol. 8, Suppl. 7; 1987)ortho-Aminoazotoluene [97-56-3] (Vol. 8, Suppl. 7; 1987)2-Amino-5-(5-nitro-2-furyl)-1,3,4-thiadiazole [712-68-5] (Vol. 7, Suppl.7; 1987)Amsacrine [51264-14-3] (Vol. 76; 2000)ortho-Anisidine [90-04-0] (Vol. 73; 1999)Antimony trioxide [1309-64-4] (Vol. 47; 1989)Aramite? [140-57-8] (Vol. 5, Suppl. 7; 1987)Auramine [492-80-8] (technical-grade) (Vol. 1, Suppl. 7; 1987) Azaserine [115-02-6] (Vol. 10, Suppl. 7; 1987)Aziridine [151-56-4] (Vol. 9, Suppl. 7, Vol. 71; 1999) (NB: Overallevaluation upgraded from 3 to 2B with supporting evidence from otherrelevant data)Benz[j]aceanthrylene [202-33-5] (Vol. 92; in preparation) (NB: Overallevaluation upgraded from 3 to 2B with supporting mechanistic and otherrelevant data)Benz[a]anthracene [56-55-3] (Vol. 32, Suppl. 7, Vol. 92; in preparation)Benzo[b]fluoranthene [205-99-2] (Vol. 32, Suppl. 7, Vol. 92; in preparation)Benzo[j]fluoranthene [205-82-3] (Vol. 32, Suppl. 7, Vol. 92; in preparation)Benzo[k]fluoranthene [207-08-9] (Vol. 32, Suppl. 7, Vol. 92; in preparation)Benzofuran [271-89-6] (Vol. 63; 1995)Benzo[c]phenanthrene [195-19-7] (Vol. 32, Suppl. 7, Vol. 92; in preparation) (NB: Overall evaluation upgraded from 3 to 2B with supporting evidence from other relevant data)Benzyl violet 4B [1694-09-3] (Vol. 16, Suppl. 7; 1987)2,2-Bis(bromomethyl)propane-1,3-diol [3296-90-0] (Vol. 77; 2000)Bleomycins [11056-06-7] (Vol. 26, Suppl. 7; 1987) (NB: Overall evaluation upgraded from 3 to 2B with supporting evidence from otherrelevant data)Bracken fern (Vol. 40, Suppl. 7; 1987)Bromodichloromethane [75-27-4] (Vol. 52, Vol. 71; 1999)Butylated hydroxyanisole (BHA) [25013-16-5] (Vol. 40, Suppl. 7;1987)b-Butyrolactone [3068-88-0] (Vol. 11, Suppl. 7, Vol. 71; 1999) Caffeic acid [331-39-5] (Vol. 56; 1993)Carbon black [1333-86-4] (Vol. 65, Vol. 93; in preparation) Carbon tetrachloride [56-23-5] (Vol. 20, Suppl. 7, Vol. 71; 1999) Catechol [120-80-9] (Vol. 15, Suppl. 7, Vol. 71; 1999)Chlordane [57-74-9] (Vol. 79; 2001)Chlordecone (Kepone) [143-50-0] (Vol. 20, Suppl. 7; 1987)Chlorendic acid [115-28-6] (Vol. 48; 1990)para-Chloroaniline [106-47-8] (Vol. 57; 1993)3-Chloro-4-(dichloromethyl)-5-hydroxy-2(5H)-furanone[77439-76-0] (Vol.84; 2004)Chloroform [67-66-3] (Vol. 73; 1999)1-Chloro-2-methylpropene [513-37-1] (Vol. 63; 1995)Chlorophenoxy herbicides (Vol. 41, Suppl. 7; 1987)4-Chloro-ortho-phenylenediamine [95-83-0] (Vol. 27, Suppl.7; 1987)Chloroprene [126-99-8] (Vol. 71; 1999)Chlorothalonil [1897-45-6] (Vol. 73; 1999)Chrysene [218-01-9] (Vol. 32, Suppl. 7, Vol. 92; in preparation) CI Acid Red 114 [6459-94-5] (Vol. 57; 1993)CI Basic Red 9 [569-61-9] (Vol. 57; 1993)CI Direct Blue 15 [2429-74-5] (Vol. 57; 1993)Citrus Red No. 2 [6358-53-8] (Vol. 8, Suppl. 7; 1987)Cobalt [7440-48-4] and cobalt compounds (Vol. 52; 1991) (NB: Evaluatedas a group)Cobalt sulfate [10026-24-1] and other soluble cobalt(II) salts (Vol. 86;2006)para-Cresidine [120-71-8] (Vol. 27, Suppl. 7; 1987)Cycasin [14901-08-7] (Vol. 10, Suppl. 7; 1987)Dacarbazine [4342-03-4] (Vol. 26, Suppl. 7; 1987)Dantron (Chrysazin; 1,8-Dihydroxyanthraquinone) [117-10-2] (Vol. 50; 1990)Daunomycin [20830-81-3] (Vol. 10, Suppl. 7; 1987)DDT [p,p‘-DDT, 50-29-3] (Vol. 53; 1991)N,N‘-Diacetylbenzidine [613-35-4] (Vol. 16, Suppl.7; 1987) 2,4-Diaminoanisole [615-05-4] (Vol. 79; 2001)4,4‘-Diaminodiphenyl ether [101-80-4] (Vol. 29, Suppl. 7; 1987) 2,4-Diaminotoluene [95-80-7] (Vol. 16, Suppl. 7; 1987)Dibenz[a,h]acridine [226-36-8] (Vol. 32, Suppl. 7; 1987)Dibenz[a,j]acridine [224-42-0] (Vol. 32, Suppl. 7; 1987)7H-Dibenzo[c,g]carbazole [194-59-2] (Vol. 32, Suppl.7; 1987)Dibenzo[a,h]pyrene [189-64-0] (Vol. 32, Suppl. 7, Vol. 92; in preparation)Dibenzo[a,i]pyrene [189-55-9] (Vol. 32, Suppl. 7, Vol. 92; in preparation)1,2-Dibromo-3-chloropropane [96-12-8] (Vol. 20, Suppl. 7, Vol. 71; 1999)2,3-Dibromopropan-1-ol [96-13-9] (Vol. 77; 2000)Dichloroacetic acid [79-43-6] (Vol. 84; 2004)para-Dichlorobenzene [106-46-7] (Vol. 73; 1999)3,3‘-Dichlorobenzidine [91-94-1] (Vol. 29, Suppl. 7; 1987) 3,3‘-Dichloro-4,4‘-diaminodiphenyl ether [28434-86-8] (Vol. 16,Suppl. 7;1987)1,2-Dichloroethane [107-06-2] (Vol. 20, Suppl. 7, Vol. 71; 1999) Dichloromethane (methylene chloride) [75-09-2] (Vol. 71; 1999) 1,3-Dichloropropene [542-75-6] (technical-grade) (Vol. 41, Suppl.7, Vol.71; 1999)Dichlorvos [62-73-7] (Vol. 53; 1991)1,2-Diethylhydrazine [1615-80-1] (Vol. 4, Suppl. 7, Vol. 71; 1999)Diglycidyl resorcinol ether [101-90-6] (Vol. 36, Suppl. 7, Vol. 71; 1999)Dihydrosafrole [94-58-6] (Vol. 10, Suppl. 7; 1987)Diisopropyl sulfate [2973-10-6] (Vol. 54, Vol. 71; 1999)3,3‘-Dimethoxybenzidine (ortho-Dianisidine) [119-90-4] (Vol. 4, Suppl. 7;1987)para-Dimethylaminoazobenzene [60-11-7] (Vol. 8, Suppl. 7; 1987)trans-2-[(Dimethylamino)methylimino]-5-[2-(5-nitro-2-furyl)-vinyl]-1,3,4-oxadiazole[25962-77-0] (Vol. 7, Suppl. 7; 1987)2,6-Dimethylaniline (2,6-Xylidine) [87-62-7] (Vol. 57; 1993) 3,3‘-Dimethylbenzidine (ortho-Tolidine) [119-93-7] (Vol.1, Suppl. 7; 1987)1,1-Dimethylhydrazine [57-14-7] (Vol. 4, Suppl. 7, Vol. 71; 1999)3,7-Dinitrofluoranthene [105735-71-5] (Vol. 65; 1996)3,9-Dinitrofluoranthene [22506-53-2] (Vol. 65; 1996)1,6-Dinitropyrene [42397-64-8] (Vol. 46; 1989)1,8-Dinitropyrene [42397-65-9] (Vol. 46; 1989)2,4-Dinitrotoluene [121-14-2] (Vol. 65; 1996)2,6-Dinitrotoluene [606-20-2] (Vol. 65; 1996)1,4-Dioxane [123-91-1] (Vol. 11, Suppl. 7, Vol. 71; 1999)Disperse Blue 1 [2475-45-8] (Vol. 48; 1990)1,2-Epoxybutane [106-88-7] (Vol. 47, Vol. 71; 1999) (NB: Overall evaluation upgraded from 3 to 2B with supporting evidence from otherrelevant data)Ethyl acrylate [140-88-5] (Vol. 39, Suppl. 7, Vol. 71; 1999) Ethylbenzene [100-41-4] (Vol. 77; 2000)Ethyl methanesulfonate [62-50-0] (Vol. 7, Suppl. 7; 1987)[Foreign bodies: see Surgical implants and other foreign bodies] 2-(2-Formylhydrazino)-4-(5-nitro-2-furyl)thiazole [3570-75-0] (Vol. 7,Suppl. 7; 1987)Fumonisin B1 [116355-83-0] (Vol. 82; 2002)Furan [110-00-9] (Vol. 63; 1995)Glu-P-1 (2-Amino-6-methyldipyrido[1,2-a:3‘,2‘-d]imidazole) [67730-11-4](Vol. 40, Suppl. 7; 1987)Glu-P-2(2-Aminodipyrido[1,2-a:3‘,2‘-d]imidazole)[67730-10-3] (Vol. 40, Suppl. 7; 1987)Glycidaldehyde [765-34-4] (Vol. 11, Suppl. 7, Vol. 71; 1999) Griseofulvin [126-07-8] (Vol. 79; 2001)HC Blue No. 1 [2784-94-3] (Vol. 57; 1993)Heptachlor [76-44-8] (Vol. 79; 2001)Hexachlorobenzene [118-74-1] (Vol. 79; 2001)Hexachloroethane [67-72-1] (Vol. 73; 1999)Hexachlorocyclohexanes (Vol. 20, Suppl. 7; 1987)Hexamethylphosphoramide [680-31-9] (Vol. 15, Suppl. 7, Vol. 71; 1999)Human immunodeficiency virus type 2 (infection with) (Vol. 67; 1996)Human papillomavirus types 6 and 11 (Vol. 90; in preparation) Human papillomavirus genus beta (some types) (Vol. 90; in preparation)Hydrazine [302-01-2] (Vol. 4, Suppl. 7, Vol. 71; 1999)1-Hydroxyanthraquinone [129-43-1] (Vol. 82; 2002)Indeno[1,2,3-cd]pyrene [193-39-5] (Vol. 32, Suppl. 7, Vol. 92; inpreparation)Iron-dextran complex [9004-66-4] (Vol. 2, Suppl. 7; 1987)Isoprene [78-79-5] (Vol. 60, Vol. 71; 1999)Lasiocarpine [303-34-4] (Vol. 10, Suppl. 7; 1987)Lead [7439-92-1] (Vol. 23, Suppl. 7; 1987)Magenta [632-99-5] (containing CI Basic Red 9) (Vol. 57; 1993) Magnetic fields (extremely low-frequency) (Vol. 80; 2002)MeA-a-C (2-Amino-3-methyl-9H-pyrido[2,3-b]indole) [68006-83-7] (Vol. 40,Suppl. 7; 1987)Medroxyprogesterone acetate [71-58-9] (Vol. 21, Suppl. 7; 1987) MeIQ (2-Amino-3,4-dimethylimidazo[4,5-f]quinoline)[77094-11-2] (Vol. 56;1993)MeIQx (2-Amino-3,8-dimethylimidazo[4,5-f]quinoxaline)[77500-04-0] (Vol.56; 1993)Merphalan [531-76-0] (Vol. 9, Suppl. 7; 1987)2-Methylaziridine (Propyleneimine) [75-55-8] (Vol. 9, Suppl. 7, Vol. 71;1999)Methylazoxymethanol acetate [592-62-1] (Vol. 10, Suppl. 7; 1987) 5-Methylchrysene [3697-24-3] (Vol. 32, Suppl. 7, Vol. 92; in preparation)4,4‘-Methylene bis(2-methylaniline) [838-88-0] (Vol. 4, Suppl.7; 1987)4,4‘-Methylenedianiline [101-77-9] (Vol. 39, Suppl. 7; 1987) Methylmercury compounds (Vol. 58; 1993) (NB: Evaluated as a group)2-Methyl-1-nitroanthraquinone [129-15-7] (uncertain purity) (Vol.27,Suppl. 7; 1987)N-Methyl-N-nitrosourethane [615-53-2] (Vol. 4, Suppl.7; 1987) Methylthiouracil [56-04-2] (Vol. 79; 2001)Metronidazole [443-48-1] (Vol. 13, Suppl. 7; 1987)Microcystin-LR [101043-37-2] (Vol. 94; in preparation) (NB: Overallevaluation upgraded from 3 to 2B based on mechanistic and other relevantdata)Mirex [2385-85-5] (Vol. 20, Suppl. 7; 1987)Mitomycin C [50-07-7] (Vol. 10, Suppl. 7; 1987)Mitoxantrone [65271-80-9] (Vol. 76; 2000)Monocrotaline [315-22-0] (Vol. 10, Suppl. 7; 1987)5-(Morpholinomethyl)-3-[(5-nitrofurfurylidene)amino]-2-oxazolidi none[3795-88-8] (Vol. 7, Suppl. 7; 1987)Nafenopin [3771-19-5] (Vol. 24, Suppl. 7; 1987)Naphthalene [91-20-3] (Vol. 82; 2002)Nickel, metallic [7440-02-0] and alloys (Vol. 49; 1990)Niridazole [61-57-4] (Vol. 13, Suppl. 7; 1987)Nitrilotriacetic acid [139-13-9] and its salts (Vol. 73; 1999) (NB:Evaluated as a group)5-Nitroacenaphthene [602-87-9] (Vol. 16, Suppl. 7; 1987)2-Nitroanisole [91-23-6] (Vol. 65; 1996)Nitrobenzene [98-95-3] (Vol. 65; 1996)6-Nitrochrysene [7496-02-8] (Vol. 46; 1989)Nitrofen [1836-75-5] (technical-grade) (Vol. 30, Suppl. 7; 1987) 2-Nitrofluorene [607-57-8] (Vol. 46; 1989)1-[(5-Nitrofurfurylidene)amino]-2-imidazolidinone [555-84-0] (Vol.7,Suppl. 7; 1987)N-[4-(5-Nitro-2-furyl)-2-thiazolyl]acetamide [531-82-8] (Vol. 7, Suppl. 7;1987)Nitrogen mustard N-oxide [126-85-2] (Vol. 9, Suppl. 7;1987) Nitromethane [75-52-5] (Vol. 77; 2000)。
内分泌治疗英语Endocrine TherapyThe endocrine system is a complex network of glands and hormones that play a crucial role in regulating various physiological processes within the human body. Hormones, the chemical messengers produced by these glands, are responsible for maintaining homeostasis, controlling growth and development, and influencing a wide range of bodily functions, from metabolism to mood. When the endocrine system malfunctions, it can lead to a variety of health issues, ranging from hormonal imbalances to chronic diseases. In such cases, endocrine therapy emerges as a vital treatment approach, aiming to restore the delicate balance of hormones and alleviate the associated symptoms.Endocrine therapy, also known as hormone therapy, is a medical treatment that involves the administration of synthetic or natural hormones to address hormonal imbalances or to target specific hormone-dependent conditions. This therapeutic approach is particularly effective in the management of various endocrine-related disorders, including thyroid dysfunction, diabetes, and certain types of cancer.One of the primary applications of endocrine therapy is in the treatment of thyroid disorders. The thyroid gland, located in the neck, is responsible for producing hormones that regulate metabolism, body temperature, and other vital functions. When the thyroid gland becomes underactive (hypothyroidism) or overactive (hyperthyroidism), it can lead to a range of symptoms, such as fatigue, weight changes, and mood disturbances. Endocrine therapy, typically in the form of synthetic thyroid hormones (e.g., levothyroxine), can be used to restore the proper balance of thyroid hormones, effectively managing the symptoms and preventing long-term complications.Another significant application of endocrine therapy is in the treatment of diabetes, a chronic condition characterized by thebody's inability to regulate blood sugar levels effectively. In type 1 diabetes, the pancreas fails to produce insulin, a hormone essential for glucose metabolism. In type 2 diabetes, the body becomes resistant to the effects of insulin. Endocrine therapy in the form of insulin administration or the use of other antidiabetic medications (e.g., metformin, GLP-1 agonists) can help maintain healthy blood sugar levels, reducing the risk of diabetic complications such as nerve damage, kidney disease, and cardiovascular problems.Endocrine therapy also plays a crucial role in the management ofhormone-dependent cancers, such as breast cancer and prostate cancer. These types of cancers are fueled by the presence of specific hormones, which promote the growth and proliferation of cancer cells. Endocrine therapy in this context aims to disrupt the cancer's dependence on hormones, either by blocking the production or action of these hormones or by directly targeting the cancer cells. This approach can be highly effective in slowing the progression of the disease, improving patient outcomes, and enhancing quality of life.In the case of breast cancer, endocrine therapy may involve the use of selective estrogen receptor modulators (SERMs), such as tamoxifen, or aromatase inhibitors, which block the conversion of androgens to estrogens. These medications can significantly reduce the risk of recurrence and improve survival rates in patients with hormone-receptor-positive breast cancer. Similarly, in prostate cancer, endocrine therapy may involve the use of androgen-deprivation therapies, which suppress the production or action of testosterone, the primary male sex hormone.Beyond these well-established applications, endocrine therapy is also being explored for the management of other health conditions, such as polycystic ovary syndrome (PCOS), infertility, and certain endocrine-related mental health disorders. In PCOS, for instance, endocrine therapy may involve the use of oral contraceptives orinsulin-sensitizing medications to regulate hormonal imbalances and alleviate symptoms like irregular menstrual cycles, acne, and excessive hair growth.The success of endocrine therapy is largely dependent on the accurate diagnosis and monitoring of the underlying endocrine condition. Healthcare providers, such as endocrinologists, work closely with patients to develop personalized treatment plans, which may involve a combination of medication, lifestyle modifications, and regular monitoring of hormone levels. Patients play a crucial role in the treatment process, as adherence to the prescribed regimen and regular follow-up appointments are essential for achieving optimal outcomes.In conclusion, endocrine therapy is a vital component of modern healthcare, providing effective solutions for a wide range of endocrine-related disorders. By leveraging the power of hormones and targeted interventions, healthcare professionals can help patients restore hormonal balance, manage chronic conditions, and improve their overall health and well-being. As research in this field continues to evolve, the potential of endocrine therapy to address complex health challenges is expected to grow, offering new hope and improved quality of life for those affected by endocrine system disorders.。
IARE一类致癌物D-F字母打头部分I . D字母开头部分:1. 1,2-Dichloropropane 1,2-二氯丙烷。
也有人简称作二氯丙烷,这应该是2017年刚加入到目录中的,补充材料引用的文献也比较新。
总之它是这样子的:它的用途主要是纺织品去污剂、油和石蜡萃等。
1,2-二氯丙烷和1,3-二氯丙烯,作为农药即滴滴混剂(D-D、Vidden D)。
D-D为播前杀线虫剂,能有效地防治土壤线虫,包括根瘤线虫、草地线虫、刺线虫、剑线虫、螺旋线虫和甜菜线虫,但是这个东西在美国1989年就禁用了,欧盟在2003年也禁用了,就连日本也不用这个做农药了。
在日本,1,2-二氯丙烷主要用于印刷业的清洁溶剂,但也正在慢慢退出历史舞台。
IARC的补充材料里面有日本印刷工人得胆管癌的资料,有兴趣的可以看看官网补充材料:http://monographs.iarc.fr/ENG/Monographs/vol110/mono110-03.pdf2. Diethylstilbestrol己烯雌酚。
这个可是大名鼎鼎啊,没听过的确实应该补补课了。
这是一种雌激素,上世纪人们没有意识到它的危害前还用作避孕药,结果自己得肿瘤不说,生下的后代还有不同程度的病变。
(这再一次说明人类的认识是不停发展的,所以我再一次支持人们反对P那个什么什么X项目的行动。
)当然是不是需要服用这个药还是要听医生的了。
我曾经用液相色谱测过这个,因为这东西作为兽药是被国家禁用的。
II. E字母开头部分1. Engine exhaust, diesel 柴油机排气。
这个不多解释,这个里面致癌的是氮氧化物NO x和PM颗粒。
可以参考官网补充材料:http://monographs.iarc.fr/ENG/Monographs/vol105/mono105.pdf2. Epstein-Barr virus EB病毒,这是一种致癌病毒,为疱疹病毒科嗜淋巴细胞病毒属的成员。
Oral Contraceptives- Very Low Estrogen Dosages: Pros andConsG. Creatsas and A. Elsheikh2nd Department of Obstetrics and Gynecology University of Athens, Aretaieion Hospital, Athens,GreeceSummaryThe latest development in oral contraceptive preparations has focused on further reductions in estrogen and progestin doses in order to improve safety and tolerability. Currently the lowest estrogen dose used in combined oral contraceptives, is: a 15 μg ethinylestradiol and 60 μg gestodene combination, utilizing a 24- day regimen. This regimen has been shown to enhanced ovarian suppression and consistent lower serum estrogen levels. The shorter pill-free interval can be particulary relevant to the maintenance of the efficacy. The overall incidence of normal cycles is reported 72%, which was found to increase with the duration of use. All treatment- emergent adverse events were either mild or moderate. The most common adverse events were headache and abdominal pain. The current evidence is that the ultra low estrogen- dose pill provides uncompromised contraceptive efficacy and reduces unwanted side-effects.IntroductionBirth control is a major factor in public health and welfare, preserving the general and reproductive health of women and allowing them to choose the moment of a planned pregnancy. Furthermore, it opens up a remarkable sense of freedom, and has increased couple’s responsibility regarding the exercise of their sexuality. Combined oral contraceptives (COCs) were the first medicine ever destined for a purely social, rather than a therapeutic purpose. Over the past four decades COCs have become the most widely used drugs, providing millions of women world-wide with a convenient means of birth control that is both highly reliable and cost effective. Therefore minimizing any associated side-effects is especially important. Today, choosing a contraceptive method means examining a host of issues related to efficacy, side-effects and cost, plus those related to future fertility, cardiovascular disease, malignancies and sexually transmitted diseases.New FormulationsThe latest development in oral contraceptive technology have focused on further reductions in estrogen and progestin doses to improve safety and tolerability1. The aim of this new formulations is to alter steroid levels in an effort to achieve lesser metabolic effects and minimize the occurrence of breakthrough bleeding and amenorrhea, while maintaining contraceptive efficacy 2. Currently the very low COCs carries, the lowest estrogen-dose i.e. 15 μg ethinylestradiol and 60 μg gestodene, utilizing a 24-day regimen, which assures contraceptive efficacy and acceptable cycle control 3. This regimen has been shown to enhance ovarian suppression and maintains a consistent lower serum estrogen level, which may result in a lower incidence of estrogenic side-effects 4,5. The 24-day regimen on the other hand may be particularly relevant to the maintenance of efficacy due to the shorter pill-free interval 6.EfficacyThe new 24-day regimen ultra low estrogen- dose pill was found to be an effective method. The Pearl index was found to be between 0.21 to 0.24 4,5 which compares favorably with those of other COCs containing higher hormonal doses for which the Pearl index values ranged from 0.1 to 3.0 during the first years of use 2,7.Ovulation and Ovarian ActivityNormal ovulation observed in all studied subjects was inhibited in all cycles using the above mentioned 24- day regimen. In addition no luteinized unruptured follicles were seen.The mean diameter of the largest follicle- like structure remained < 10mm throughout 3 treatment cycles, while during treatment a reduction was noted in the 17β- estradiol plasma levels (<50 pg/ml). LH levels were suppressed (<10 mlU/ml) with only a small rise seen during the pill-free intervals, while FSH levels were found suppressed only during active treatment and rose nearly to normal levels during the pill- free interval 4,5,8.Cycle ControlUsing the ultra low estrogen- doses, cycle control was found to be efficient. The overall incidence of normal cycles was 72%, indicating that the 24-day regimen was able to maintain acceptable cycle control. The mean cycle length was found to be 25.8 days and 30.9 at cycles 1 and 19, respectively. Some reports howevershow that the incidence of normal cycles was lower than that of the other low dose pills, due to the lower progestin and estrogen content. The main cycle- control difference was a somewhat higher incidence of breakthrough bleeding and spotting 4,5 (Fig. 1). Furthermore, the incidence of normal cycles were found to increase with the duration of use 4. The cycle characteristics produced a bleeding pattern that was acceptable to subjects and were not associated with a significantly different rate of discontinuation due to irregular bleeding.SafetyThe safety profile of ultra low estrogen- dose was similar to those of the other low dose COCs. All treatment- emergent adverse events were either mild or moderate. The most common adverse events were headache, abdominal and breast pain (Table 1). No clinically important changes in physical examinations, laboratory parameters, cervical smear results, blood pressure and body weight measurements were noted. On the contrary other studies showed an increase in mean body weight observed at cycle 6 (+0.25 kg), cycle 13 (+0.54 kg) and cycle 19 (+0.68 kg) which despite their statistical significance (p<0.001) were not considered to be clinically important3,5.EndometriumThe results of studies undertaken to evaluate the effects of ultra low estrogen-dose COCs on the endometrium pattency, showed that the 24-day regimen produced effective endometrial suppression 3,9. As the estrogen dose is reduced, endometrial support is lessened and more irregular bleeding occurs. However potent progestogens such as gestodene possess greater progestational, antiestrogenic and antiovulatory activity 10.11.Endometrial suppression appeard to occur sooner than with the 21-day regimen of the 20 μg ethinylestradiol dose preparations 9. This difference may partially correlated to the higher progestogen-to-estrogen ratio (4.0) with gestodene 60 μg/ ethinylestradiol 15 μg versus a ratio of 3.75 with the gestodene 75 μg/ ethinylestradiol 20 μg combination. The contribution of the additional 3 days of active pills to the endometrial suppression is unclear, since no comparative trial utilizing endometrial biopsies have studied the 21- and 24-day regimens 3. Metabolic ProfileIn a few studies COCs have been associated with an increased risk of thromboembolic disease 2,12, altered lipid metabolism 13and abnormal glucosetolerance 14. The ultra low estrogen-dose preparations have been introduced as an effort to reduce further the unwanted side-effects.Lipid and Carbohydrate MetabolismReports show that the ultra low estrogen-dose have a minimal impact on the lipid profile. Cholesterol and LDL-C levels were found to be decreased at the third and sixth cycles, respectively. Triglyceride and Apoprotein levels were noted to be significantly increased. The results of the glucose tolerance tests showed that mean glucose AUC and mean insulin AUC were significantly increased 15,16, while C-peptide AUC was found to remain unchanged 15. HemostasisAn increase in the levels of fibrin degradation products has been noted. Also a significant increase in D-dimer levels was found. Mean levels of fibrinogen, factors VIIt, VIIa and F1 + 2 showed significant increases. Significant increases were also reported in mean plasminogen activity, fibrinolytic activity (PAP) values and angiotensinogen plasma levels. In the mean time, there were significant decreases in the mean levels of tPA ag and PAI-1 ag have been reported 15,17.Cardiovascular DiseaseEpidemiological studies in the ‘60s showed that COCs increased th e risk of cardiovascular disease 18.19. Research was directed in reducing this risk via changes of the estrogen- doses 13. The continuing decrease in the estrogen- doses has resulted in a further reduction of the COCs- related risks on cardiovascular, cerebrovascular and thromboembolic diseases. The overall minimal changes in the lipid profile were sufficiently small to maintain normal or beneficial levels and thereof would not be expected to adversely affect cardiovascular risk in healthy women 20.ComplianceThe ultra low dose pill was found to be well tolerated and there were no serious drug-related adverse events. No discontinuation of treatment due to adverse related events was reported 3.References1.Dusterberg B, Ellman H, Muller U. A three-year clinical investigationinto efficacy, cycle control and tolerability of a new low-dose monophasicoral contraceptive containing gestodene. Gynecol Endocrinol 10:33-39;19962.Speroff L, DeCherney A. Evaluation of a new generation of oralcontraceptives. Obstet Gynecol 81:1034-47;19933.Oosterbaan H.P. An open-label study of the effects of a 24-day regimen ofgestodene 60 μg/ ethinylestradiol 15 μg on endometrial histological findings in healthy women. Eur J Contracept Reprod Health Care 4 (suppl 2):3-8;19994.Gestodene Study Group 322. The safety and contraceptive efficacy of a24-day low- dose OC regimen containing gestodene 60 μg and ethinylestradiol 15 μg. Eur J Contracept Reprod Health Care 4:9-15;1999 5.Gestodene Study Group 324. Cycle control, safety and efficacy of a 24-dayregimen of gestodene 60 μg/ ethinylestradiol 15 μg and a 21-day regimen of desogestrel 150 μg/ ethinylestradiol 20 μg. Eur J Contracept Reprod Health Care 4:17-25; 19996.Spona J, Elstein M, Feichtinger W. Shorter pill-free interval in combinedoral contraceptives decreases follicular development. Contraception 54:71-77;19967.Kirkman RJ, Pedersen JH, Fioretti P, Roberts HE. Clinical comparisonof two low-dose oral contraceptives, Mimulet and Mercilon, in women over 30 years of age. Contraception 49:33-46;19948.Sullivan H, Furniss H, Spona J, Elstein M. Effect of 21-day and 24-dayoral contraceptive regimens containing gestodene (60 μg) and ethinylestradiol (15 μg) on ovarian activity. Fertil Steril 72:115-120;1999 9.Coenen CMH, Hollanders JMG, Rolland R. The effects of a low-dosegestodene-containing oral contraceptive on endometrial histology in healthy women. Eur J Contracept Reprod Health Care 1:325-329;1996 10.Kaplan B. Desogestrel, norgestimate and gestodene: the newer progestins.Ann Pharmacother 29:736-742;199511.Wilde MI, Balfour JA. Gestodene: A review of its pharmacology, efficacyand tolerability in combined contraceptive preparations. Drugs 50:364-395;199512.Daly L, Bonnar J. Comparative studies of 30 micrograms ethinylestradiolcombined with gestodene and desogestrel on blood coagulation, fibrinolysis and platelets. Am J Obstet Gynecol 163:430-437;199013.Fotherby K, Caldwell A. New progestogens in oral contraception.Contraception 49:1-32;199414.Wynn V, Doar J. Some effects of oral contraceptives on carbohydratemetabolism. Lancet 2:715-719;199615.van der Mooren MJ, Klipping C, van Aken B, Helmerhorst FM. Acomparative study of the effects of gestodene 60 μg / ethinylestradiol 15 μg and desogestrel 150 μg/ ethinylestradiol 20 μg on hemostatic balance, blood lipid levels and carbohydrate metabolism. Eur J Contracept Reprod Health Care 4:27-35;199916.Spellacy WN, Tsibris AM, Tsibris JC. Carbohydrate metabolism studiesafter one year of using an oral contraceptive containing gestodene and ethinylestradiol. Contraception 49:125-130;199417.Kluft C, Lunsink M. Effect of oral contraceptives on haemostasisvariables. Thromb Haemost 78:315-326;199718.Stadd BV. Oral contraceptives and cardiovascular disease. N Engl J Med305:612-617, 672-677;198119.Carr BR. Re-evaluation of oral contraceptive classifications. Int J Fertil42:133-144;199720.Lewis MA, Heinemann LA, Spitzer WD. The use of oral contraceptivesand the occurence of acute myocardial infarction in young women.Results from the transnational study on oral contraceptives and the health of young women. Contraception 56:129-140;1997Figure 1: Bleeding classification in percentage of total number of cycles (adapted from Gestodene Study Group 324,1999)Table 1. Percentage of adverse events reported by different authors。