支架内血栓In-Stent Thrombosis
- 格式:ppt
- 大小:2.12 MB
- 文档页数:41
冠状动脉介入治疗新里程碑--生物可吸收支架刘兵;何青【摘要】现代药物洗脱支架的术后再狭窄率及支架内血栓风险显著下降,明显改善了冠状动脉介入治疗后的远期预后,但是为了保持狭窄动脉的通畅,血管内不得不置入永久支架;永久支架置入所致的血管炎性反应、支架内再狭窄、支架内血栓形成及支架区域血管生理功能的部分丧失都是无法避免的“陷阱”。
生物可吸收支架仅仅提供暂时的血管管腔支撑随之便逐渐消失,目前市场已经有多种生物可吸收支架正在进行临床评估及临床前期评估,其中两种已获得了欧盟认证,一种已获得了美国食品和药物管理局认证。
本文旨在对目前主要生物可吸收支架进行系统介绍。
%The current generation of drug-eluting stents has significantly improved the outcomes of percutaneous coronary intervention by substantially reducing stent restenosis and stent thrombosis. However, the concept of using a permanent metallic stent to keep the patency of a stenotic artery has inevitable“traps”,the presence of a foreign body within the artery induces vascular inflammation,in-stent restenosis, stent thrombosis, and impeding the restoration of the physiologic function of the stented segment. Bioresorbable scaffolds (BRS) were introduced to potentially overcome these limitations,as they provide only temporary support the vascular lumens and then gradually disappear,liberating the treated vessel from its cage. Currently, several BRSs are undergoing evaluations either in clinical trials or in preclinical settings. Two devices with substantial clinical data have received a EU certification and one hasreceived a US FDA approval. This review article presents the current status of these devices.【期刊名称】《中国心血管杂志》【年(卷),期】2016(021)004【总页数】5页(P314-318)【关键词】冠状动脉疾病;血管成形术,经腔,经皮冠状动脉;生物可吸收支架【作者】刘兵;何青【作者单位】100730 中国医学科学院北京协和医学院北京医院心内科国家老年医学中心;100730 北京医院心内科国家老年医学中心【正文语种】中文1977年,Gruentzig在完成了世界上第一例经皮冠状动脉腔内成形术后[1],冠状动脉介入治疗在短短30多年间经历了三个里程碑,即单纯球囊扩张、金属裸支架和药物洗脱支架(drug eluting stent,DES),改善了冠状动脉介入治疗(percutaneous coronary intervention,PCI)的短期及长期预后。
颈动脉支架置入术后支架内血栓形成研究进展(全文)颈动脉支架置入术(carotid artery stenting,CAS)作为中到重度颈动脉狭窄患者的治疗方式之一,越来越受到人们的重视,而围手术期的血栓栓塞事件,作为CAS的严重并发症,可导致患者围手术期致残甚至死亡。
有学者将颈动脉支架内血栓形成分为早期(≤30d)、晚期(>30d)及极晚期(>12个月)3种情况,而早期支架内血栓形成又可分为急性支架内血栓形成(<24h)和亚急性支架内血栓形成(1-30d)。
目前,研究中对颈动脉支架内血栓形成的报道较少,本文回顾了2018年以前在MEDLINE、EMBAST及Ovid等数据库中以英文形式发表的关于颈动脉支架内血栓形成的文章,对颈动脉支架内血栓形成的特点、可能原因及治疗等进行汇总,以期为今后颈动脉支架内血栓形成的及早发现及治疗提供参考。
这些研究共21项,报道了32例CAS后颈动脉支架内血栓形成的病例。
01流行病学及病因颈动脉支架内血栓形成是CAS的少见并发症,发病率在0.5%-0.8%。
大多数颈动脉支架内血栓形成与手术相关,具体有:保护伞装置堵塞、2个重叠的支架、支架后扩张后的颈动脉夹层、球囊破裂、支架贴壁不良等。
保护伞装置堵塞是经报道最多的与手术相关的颈动脉支架内血栓形成。
Yong-Won Kim等曾报道了3例由于保护伞装置堵塞造成的颈动脉支架内血栓形成。
Stephan Munich等也报道了1例由于保护伞装置堵塞所造成的颈动脉支架内血栓形成。
再次接受CAS,可能也是导致术中颈动脉支架内血栓形成的重要原因。
Konstantinos G. Moulakakis等报道了2例由于2个重叠的支架所导致的颈动脉支架内血栓形成。
抗血小板治疗不充分或术后停止抗血小板治疗,也是导致围手术期颈动脉支架内血栓形成的主要原因之一。
G. F. Hamann等及Fotis Markatis 等均报道了由于失误导致患者停止抗血小板治疗,从而引发颈动脉支架内血栓形成。
支架血栓形成是严重问题发表时间:2014-08-22T10:58:52.480Z 来源:《医药前沿》2014年第19期供稿作者:陈艺娜王辉宇[导读] 目前,冠状动脉粥样硬化性心脏病血运重建术治疗中,支架植入术被广泛应用于临床,明显优于球囊扩张术。
陈艺娜王辉宇 (三门峡市中心医院心血管内科 472000) 【摘要】目的为研究三门峡地区行经皮冠状动脉介入治疗(percutaneous coronary intervention, PCI)术患者,药物洗脱支架(drug-eluting stents DES)和金属裸支架(bare metal stents BMS)支架内血栓形成(stent thrombosis ST)的发生率。
急性血栓在24h小时发生,亚急性血栓在30天内、一年或者超过一年发生。
方法所有患者患有急性冠脉综合症或者不稳定心绞痛,所有患者病情是PCI术适应症,无禁忌症。
均在介入中心行PCI治疗。
结果全部1386个行PCI术患者中,有19个(1.3%)有支架内血栓形成,其中4个人(21%)植入DES,15人(79%)植入BMS。
4个人有支架内急性血栓形成,5个人有亚急性血栓形成,8个人有晚期血栓形成。
同时9个病人有糖尿病,8个病人有高血压。
结论三门峡地区在我们介入中心植入DES的患者支架内血栓形成的发生率与国际上报道的人数相似。
支架内血栓形成的病人当中几乎一半患有糖尿病。
倍受医生关注的是晚期支架内血栓形成的风险DES偏高于BMS。
【关键词】药物洗脱支架支架内血栓形成经皮冠状动脉介入治疗支架内再狭窄【中图分类号】R608 【文献标识码】A 【文章编号】2095-1752(2014)19-0265-02 Stent thrombosis is a major concern in clinical practice: A single Saudi center experience 目前,冠状动脉粥样硬化性心脏病血运重建术治疗中,支架植入术被广泛应用于临床,明显优于球囊扩张术。
临床研究早期与晚期支架内血栓致4b型急性心肌梗死患者临床结局比较李晓卫1,2,高静1,2,3△,刘寅1,高明东1,肖健勇1摘要:目的 比较早期与晚期支架内血栓(ST)致4b型急性心肌梗死(AMI)患者院内及出院1年生存及预后情况。
方法 入选2015年1月—2018年2月冠状动脉造影确定ST致4b型AMI患者共302例。
根据ST发生时间分为早期ST组(≤30 d)26例和晚期ST组(>30 d)276例,对比2组患者住院期间及出院1年内的终点事件。
主要研究终点包括心源性死亡和再发AMI;次要研究终点包括靶病变血运重建(TLR)、再次ST、心力衰竭及卒中。
采用Kaplan-Meier法绘制生存曲线并比较2组患者无终点事件发生率;采用Cox回归分析4b型AMI患者发生终点事件的危险因素。
结果 住院期间2组主要研究终点事件发生率差异无统计学意义(7.7% vs. 3.3%,P=0.243);早期ST组院内心力衰竭发生率高于晚期ST组(11.5% vs. 1.4%,P=0.016),其他次要终点事件发生率差异无统计学意义(P>0.05)。
平均随访1年,早期ST组主要(20.0% vs. 5.9%,P<0.05)及次要(36.0% vs. 11.5%,P<0.05)研究终点事件发生率均高于晚期ST组。
Kaplan-Meier生存分析表明,早期ST组1年累积无主要(P=0.022)及次要(P<0.001)终点事件发生率均低于晚期ST组。
Cox回归分析表明高血压、冠状动脉旁路移植术史是4b型AMI患者发生主要终点事件的独立危险因素,术中植入主动脉内气囊泵(IABP)、缩短支架内血栓至球囊扩张(ST to B)时间是其发生次要终点事件的独立保护因素。
结论 与晚期ST致4b型AMI患者相比,早期ST患者院内结局相似,长期预后差。
术中植入IABP、缩短ST to B时间可能改善4b型AMI患者预后。
关键词:心肌梗死;主动脉内气囊泵;支架内血栓;靶病变血运重建中图分类号:R541.4 文献标志码:A DOI:10.11958/20230488Comparison of clinical outcomes in patients with 4b acute myocardial infarction caused by earlyand late stent thrombosisLI Xiaowei1, 2, GAO Jing1, 2, 3△, LIU Yin1, GAO Mingdong1, XIAO Jianyong11 Department of Coronary Care Unit, Chest Hospital, Tianjin University, Tianjin 300222, China;2 Tianjin Medical University;3 Tianjin Cardiovascular Diseases Institute△Corresponding Author E-mail:*******************Abstract: Objective To observe and compare in-hospital and 1-year survival and prognosis of patients with 4b acute myocardial infarction (AMI) caused by early and late stent thrombosis (ST). Methods A total of 302 patients with 4b acute myocardial infarction caused by ST were enrolled in this study from January 2015 to February 2018. ST patients were confirmed by coronary angiography. These patients were divided into two groups: the early ST group (n=26) and the late ST group (n=276) according to the time of ST occurrence. Endpoint events during hospitalization and one year of follow up were compared between the two groups of patients. The primary endpoint events included cardiac death and recurrent AMI. The secondary endpoint events included target lesion revascularization (TLR), re-stent thrombosis, heart failure and stroke. The incidence of no endpoint events was compared between two groups of patients by Kaplan and Meier survival analysis. Cox regression analysis was used to analyze risk factors for endpoint events in patients with type 4b AMI. Results There was no significant difference in the incidence of the primary endpoint events during hospitalization between the two groups (7.7% vs.3.3%,P=0.243). The incidence of heart failure was higher in the early ST group than that of the late ST group (11.5%vs.1.4%, P=0.016). There was no significant difference in the incidence rates of other secondary endpoint events between the two groups (P>0.05). After a mean follow-up of 1 year, the incidence rates of primary endpoint events and the secondary eendpoint events were higher in the early ST group (20.0% vs. 5.9%,P<0.05 and 36.0% vs. 11.5%,P<0.01)than that of the late ST group. Kaplan and Meier survival analysis showed that the 1-year cumulative incidences of non-primary (P= 0.022) and non-secondary events (P<0.001) were lower in the early ST group than those of the late ST group. Cox regression 基金项目:天津市卫健委重点学科项目(TJWJ2022XK032);天津市卫健委科技基金项目(TJWJ2021MS027);天津市科技计划项目(22JCZDJC00130);天津市科委重点项目(20YFZCSY00820);天津市医学重点建设学科项目(TJYXZDXK-055B) 作者单位:1天津大学胸科医院冠心病监护病房(邮编300222);2天津医科大学;3天津市心血管病研究所 作者简介:李晓卫(1982),男,副主任医师,主要从事急性心肌梗死相关研究。
药物洗脱支架血栓形成[摘要]药物洗脱支架内血栓形成是支架置入术后非常少见,但后果非常严重的并发症。
药物洗脱支架内血栓导致的心肌梗死发生率和死亡率相当高,这不得不引起人们对药物洗脱支架安全性的高度重视。
现对药物洗脱支架内血栓的定义、病因、临床证据和预防等进行简要综述。
[关键词]药物洗脱支架;血栓形成;支架;文献综述2001年9月REV AL实验结果在欧洲心脏病学会上公布,标志着药物洗脱支架(DES)新纪元的开始。
随后DES,尤其是雷帕霉素洗脱支架(SEs)和紫杉醇洗脱支架(PES),因其可减少支架内再狭窄而越来越多地被使用,但其支架内血栓(stent thrombosis,ST)发生率却没有减少。
ESTROFA注册研究显示,23500例病人34075只DES植入后3年随访ST累计发病率为2%。
虽然ST发生率并不高,但庞大的冠脉介入治疗数量及ST相关的心肌梗死发生率和死亡率很高,因而备受关注。
1.ST的定义和分类1.1明确的ST明确的ST是经血管造影术或病理检查确诊的。
血管造影术确诊是指支架段(含近端和远端5mm内)发生的血栓,并且48h内有以下至少1种情况发生:休息时有急性缺血症状(典型胸痛>20min)、心电图提示急性心肌缺血或心肌标志物的典型改变。
病理确诊是尸检报告确定支架内有新近血栓形成。
1.2可能的ST可能的ST:30d内不明原因死亡或血管造影术后任何时期发生急性缺血症状,且血管造影不能确诊为ST并排除其他原因导致的心肌缺血。
1.3不能排除的ST不能排除的ST:术后30d到随访结束这段时间内不明原因的死亡。
根据ST形成发生的时间分为4类:(1)急性ST,发生于介入术后24h内;(2)亚急性ST,发生在介入术后24h~30d;(3)晚期ST,发生在介入术后30d~1年;(4)极晚期ST,发生在介入术后1年以上。
2.ST的病因多变量分析显示,明确的早期ST(30d内)最重要的危险因素是术后支架内面积小、术前未服用氯吡格雷、冠脉病变程度重以及基础血红蛋白水平高;明确的或者可能的早期ST的独立危险因素为胰岛素依赖型糖尿病、杜克危险积分、术前未服用氯吡格雷、肾功能不全;晚期和极晚期独立危险因素包括血液透析、终末期肾病[GFR31.5mm的病人更容易发生ST、心肌梗死及死亡。

极晚期支架内血栓形成原因及处理作者:刘睿方徐方兴周玉杰刘同库徐丽华来源:《中西医结合心血管病电子杂志》2017年第01期【摘要】目的探讨极晚期支架内血栓(LVST)形成原因及处理。
方法回顾性分析2005年6月~2010年6月植入雷帕霉素药物洗脱支架(DES)治疗冠状动脉狭窄1548例(共植入2642枚支架)中发生LVST病例的发病和处理的具体情况。
结果 1548例中发生2例LVST,LVST发生率为0.13%,1例LVST发生在支架术后41个月(三年半),另1例LVST发生在支架术后26个月(二年两个月)。
两例均为停止用双联抗血小板治疗后发生支架内血栓。
经过充分的抗栓治疗同时行球囊扩张治疗,血栓影消失,无残余狭窄,未再植入支架。
随访75个月,病人无不适症状。
结论 LVST形成原因复杂,与停用双抗有关。
充分的抗栓同时行球囊扩张治疗是有效的方法。
【关键词】极晚期支架血栓,原因,处理方法【中图分类号】R541.4 【文献标识码】A 【文章编号】ISSN.2095-6681.2017.01..02The causes and the treatment of very late stent thrombosisLIURui-fang1, XUFang-xing1, ZHOUYu-jie1, LIUTong-ku2, XU-Lihua2(1.Beijing Anzhen Hospital, Capital Medical University,Beijing 100029,China;2.Affiliated Hospital,Beihua University,JiLin JiLin 132011,China)【Abstract】Objective To explore the causes and the treatment of very late stent thrombosis.Methods Among 1548 cases with coronary stenosis lesions undergoing 2642 rapamycin drug-eluting stents (DES) implantation two patients with LVST were retrospectively analyzed from June 2005 to June 2010.Results Among 1548 cases with coronary stents implantation two cases suffered from LVST. The incidence rate of LVST was 0.13%. 1 case with in-stent thrombosis occurred in 41 months after stenting (three and a half years), and the other case with LVST occurred in 26 months after stenting.Two cases with LVST all occurred in stop using dual antiplatelet therapy.For those patients full antithrombotic treatment and balloon expansion were performed at the same time.The thrombus shadow in-stent disappeared.There was no residual stenosis in target coronary vessels.Stent implantation was not performed again. The patients were Follow-up of 75 months and without symptoms.Conclusion The causes of LVST is complex and related to stop using double antiplatelet.The balloon expansion and at the same time fully antithrombotic therapy are effective method.【Keyword】Very late stent thrombosis;causes;treatment经皮冠状动脉介入治疗(PCI)植入雷帕霉素洗脱支架(DES),可发生支架内血栓形成,引起急性心肌梗死或猝死。
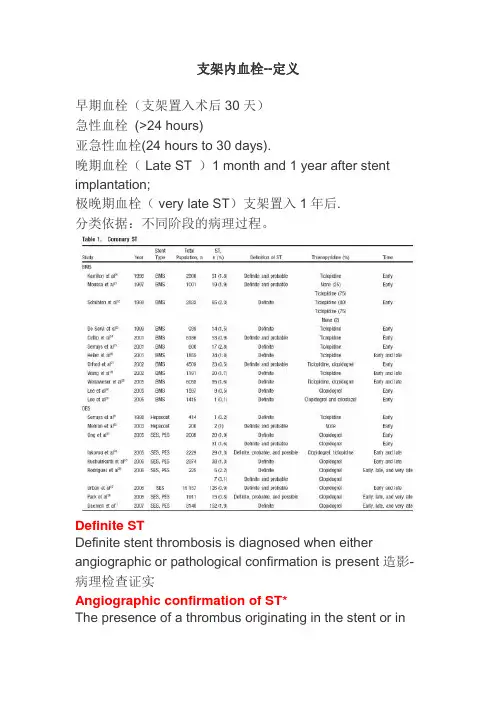
支架内血栓--定义早期血栓(支架置入术后30天)急性血栓(>24 hours)亚急性血栓(24 hours to 30 days).晚期血栓( Late ST )1 month and 1 year after stent implantation;极晚期血栓( very late ST)支架置入1年后.分类依据:不同阶段的病理过程。
Definite STDefinite stent thrombosis is diagnosed when either angiographic or pathological confirmation is present造影-病理检查证实Angiographic confirmation of ST*The presence of a thrombus originating in the stent or inthe segment 5 mm proximal or distal to the stented region and at least one of the following 支架内血栓支架5mm节段内血栓criteria within a 48-h time window:48小时内Acute onset of ischemic symptoms at rest (typical chest pain >20 min)静息缺血症状>20分钟New ischemic ECG changes suggestive of acute ischemia 新的缺血性心电图改变Typical rise and fall in cardiac biomarkers典型的心脏生物学标记物升高和降低Pathological confirmation of stent thrombosis Evidence of recent thrombus within the stent determined at autopsyProbable STClinical definition of probable ST is diagnosed after intracoronary stenting in the following casesAny unexplained death within the first 30 dRegardless of the time after the index procedure, any MI that is related to documented acute ischemia in the territory of the implanted stent withoutangiographic confirmation of ST and in the absence of any other obvious causePossible STClinical definition of possible ST is diagnosed with any unexplained death from 30 d after intracoronary stenting until the end of trial follow-up*The incidental angiographic documentation of stent occlusion in the absence of clinical signs or symptoms (silent occlusion) is (for this purpose) not considered a confirmed stent thrombosis.Multifactorial Origin of ST 血栓形成原因Patient factorsThickness and robustness of neointimal stent coverage Drug response/interactionsGene polymorphismLeft ventricular functionAcute coronary syndromeRenal failureDiabetes mellitusAntithrombotic and anticoagulation therapy Coagulation activityInhibition of platelet aggregationProcedural factorsDissectionIncomplete stent appositionStent expansionLesion factorsVessel sizeLesion lengthThrombusPlaque characteristicsBifurcationDevice factorsStent surfaceDrugsPolymerPrevention of STAntiplatelet Therapyit appears reasonable to maintain patients treated with (first-generation) DES for >1 year on dual antiplatelet therapy if they tolerate it and are at low risk of bleeding. Whether prolonged dual antiplatelet therapy prevents late and very late ST after DES implantation, is associated with a lower rate of ischemic cardiovascular events, and has a favorable net clinical benefit requires confirmation in randomized, prospective trials.Patient and Lesion SelectionSelection of patients suitable for DES implantation is another measure to reduce the risk of ST.Technique。
冠脉介入术后支架内再狭窄治疗进展冠脉介入术(Percutaneous Coronary Intervention,PCI)是一种治疗心脏病的有效手段,通过在狭窄或闭塞的冠状动脉内放置支架来恢复血流,缓解心肌缺血和心绞痛症状。
然而,在支架植入后,患者仍有可能出现支架内再狭窄(In-Stent Restenosis,ISR)的情况,这会影响血流恢复效果,增加血栓形成和再次心血管事件的风险。
因此,治疗ISR具有重要的临床意义。
ISR的发生机制复杂多样,涉及多种细胞因子、细胞增殖和细胞凋亡等生物学过程。
治疗ISR的方法也多种多样,包括药物治疗、再介入术、放射性支架、药物涂层支架等。
近年来,各类新技术也不断涌现,如经皮冠状动脉取支架术(Percutaneous Coronary Atherectomy,PCA)、分叉支架、仿生支架等,为ISR治疗带来了新的进展和选择。
药物治疗是治疗ISR的经典方法,常用的药物包括抗增殖药物(如西罗莫司、乐纳普利)、抗炎药物(如甲泼尼龙)、抗血小板药物(如阿司匹林、氯吡格雷)等。
这些药物可以降低细胞增殖和炎症反应,减少血小板聚集和血栓形成,从而减轻支架内再狭窄的程度,并降低血栓形成和再次心血管事件的风险。
药物治疗的优点在于较为简便、经济、安全,缺点在于缓解程度有限,不能完全消除狭窄。
再介入术是一种常用的治疗ISR的方法,包括球囊扩张术、球切术、激光扩张术等。
这些方法通过直接扩张和切割支架内再狭窄的部位,恢复狭窄段的通畅度,减轻心肌缺血和心绞痛症状。
再介入术的优点在于可直接消除狭窄,缺点在于易造成支架损伤、内皮细胞损伤以及血栓形成的风险。
放射性支架是一种近年来新兴的治疗ISR的方法,其特点在于支架表面涂覆放射性物质,发射放射线破坏狭窄部位的细胞和基质,从而减少再次狭窄的风险。
这种方法可以达到较好的疗效,但也存在较高的辐射风险和复发风险。
药物涂层支架(Drug-Eluting Stent,DES)是一种将药物涂层于支架表面的特殊支架,可以在支架植入后缓慢释放药物,防止血管再次狭窄。
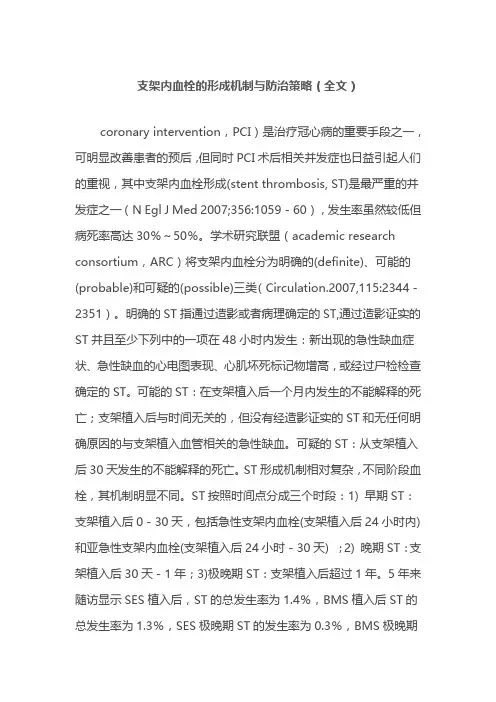
支架内血栓的形成机制与防治策略(全文)coronary intervention,PCI)是治疗冠心病的重要手段之一,可明显改善患者的预后,但同时PCI术后相关并发症也日益引起人们的重视,其中支架内血栓形成(stent thrombosis, ST)是最严重的并发症之一(N Egl J Med 2007;356:1059-60),发生率虽然较低但病死率高达30%~50%。
学术研究联盟(academic research consortium,ARC)将支架内血栓分为明确的(definite)、可能的(probable)和可疑的(possible)三类(Circulation.2007,115:2344-2351)。
明确的ST指通过造影或者病理确定的ST,通过造影证实的ST并且至少下列中的一项在48小时内发生:新出现的急性缺血症状、急性缺血的心电图表现、心肌坏死标记物增高,或经过尸检检查确定的ST。
可能的ST:在支架植入后一个月内发生的不能解释的死亡;支架植入后与时间无关的,但没有经造影证实的ST和无任何明确原因的与支架植入血管相关的急性缺血。
可疑的ST:从支架植入后30天发生的不能解释的死亡。
ST形成机制相对复杂,不同阶段血栓,其机制明显不同。
ST按照时间点分成三个时段:1) 早期ST:支架植入后0-30天,包括急性支架内血栓(支架植入后24小时内)和亚急性支架内血栓(支架植入后24小时-30天) ;2) 晚期ST:支架植入后30天-1年;3)极晚期ST:支架植入后超过1年。
5年来随访显示SES植入后,ST的总发生率为1.4%,BMS植入后ST的总发生率为1.3%,SES极晚期ST的发生率为0.3%,BMS极晚期发生率为0.04%(N Egl J Med 2007;356:1030-9)。
ST主要归因于手术操作、血小板抵抗、患者用药依从性差、支架贴壁不良、内皮化不良、过敏反应及新生斑块破裂。
然而在不同阶段,影响ST发生的因素有明显的区别,目前认为急性期ST主要与介入操作相关,包括支架膨胀不全、长支架植入、多支架植入及重叠支架等均有可能增加ST发生的风险。
pci支架内血栓定义
听说PCI支架里还会长血栓?这可是真事儿。
做了心脏支架手
术后,有时候支架里面或者周围可能会形成血栓。
这血栓一堵,心
脏可就受不了了,严重的还可能导致心肌梗死。
说到这血栓的形成,原因可不少。
支架材料、手术操作,还有
病人自身的身体状况都可能有关系。
有时候,就算支架做得再好,
也难免会出现问题。
毕竟,这东西是放在心脏里的,稍微出点差错
都可能引发大问题。
你问我什么是PCI支架内血栓?简单来说,就是在做了PCI手
术后,支架里面或者周围出现了血栓。
这血栓有急性的、亚急性的,还有晚期的,每种情况都不一样。
医生得根据具体情况来判断怎么
处理。
所以啊,这PCI支架内血栓可不是小事儿。
做了手术的朋友们,一定得注意身体状况,有什么不舒服的赶紧去医院。
医生会根据情
况给你最好的建议和治疗。
记住,健康最重要,别拿自己的生命开
玩笑!。
支架内血栓--定义早期血栓(支架置入术后30天)急性血栓(>24 hours)亚急性血栓(24 hours to 30 days).晚期血栓( Late ST )1 month and 1 year after stent implantation;极晚期血栓( very late ST)支架置入1年后.分类依据:不同阶段的病理过程。
Definite STDefinite stent thrombosis is diagnosed when either angiographic or pathological confirmation is present造影-病理检查证实Angiographic confirmation of ST*The presence of a thrombus originating in the stent or inthe segment 5 mm proximal or distal to the stented region and at least one of the following 支架内血栓支架5mm节段内血栓criteria within a 48-h time window:48小时内Acute onset of ischemic symptoms at rest (typical chest pain >20 min)静息缺血症状>20分钟New ischemic ECG changes suggestive of acute ischemia 新的缺血性心电图改变Typical rise and fall in cardiac biomarkers典型的心脏生物学标记物升高和降低Pathological confirmation of stent thrombosis Evidence of recent thrombus within the stent determined at autopsyProbable STClinical definition of probable ST is diagnosed after intracoronary stenting in the following casesAny unexplained death within the first 30 dRegardless of the time after the index procedure, any MI that is related to documented acute ischemia in the territory of the implanted stent withoutangiographic confirmation of ST and in the absence of any other obvious causePossible STClinical definition of possible ST is diagnosed with any unexplained death from 30 d after intracoronary stenting until the end of trial follow-up*The incidental angiographic documentation of stent occlusion in the absence of clinical signs or symptoms (silent occlusion) is (for this purpose) not considered a confirmed stent thrombosis.Multifactorial Origin of ST 血栓形成原因Patient factorsThickness and robustness of neointimal stent coverage Drug response/interactionsGene polymorphismLeft ventricular functionAcute coronary syndromeRenal failureDiabetes mellitusAntithrombotic and anticoagulation therapy Coagulation activityInhibition of platelet aggregationProcedural factorsDissectionIncomplete stent appositionStent expansionLesion factorsVessel sizeLesion lengthThrombusPlaque characteristicsBifurcationDevice factorsStent surfaceDrugsPolymerPrevention of STAntiplatelet Therapyit appears reasonable to maintain patients treated with (first-generation) DES for >1 year on dual antiplatelet therapy if they tolerate it and are at low risk of bleeding. Whether prolonged dual antiplatelet therapy prevents late and very late ST after DES implantation, is associated with a lower rate of ischemic cardiovascular events, and has a favorable net clinical benefit requires confirmation in randomized, prospective trials.Patient and Lesion SelectionSelection of patients suitable for DES implantation is another measure to reduce the risk of ST.Technique。
STEMI支架植入术后发生支架内血栓形成患者影响因素的临床分析作者:王培翠武文辉来源:《中西医结合心血管病电子杂志》2020年第02期【摘要】目的探讨急性ST段抬高性心肌梗死(STEMI)冠状动脉腔内药物洗脱支架(DES)置入后围手术期支架内血栓形成的影响因素、解决办法和效果。
方法应用回顾性的方法分析实施冠状动脉腔内DES置入术的冠心病急性ST段抬高性心肌梗死患者冠脉内支架置入术后发生支架内血栓患者(26例)的临床特点、再次冠状动脉介入干预及术后治疗情况。
结果 26例支架内血栓患者中16例患者于支架置入术后24 h内出现支架内血栓,7例患者于支架置入术后24 h~30 d内出现支架内血栓,有2例患者于支架置入术后31 d~1年内内出现支架内血栓,1例患者患者于支架置入术后1年出现支架内血栓,有1例高龄患者因再次急性心肌梗死心力衰竭死亡,死亡率7.7%。
结论支架内血栓形成是冠状动脉腔内支架置入术后的常见并发症,其发生率为2%左右,其中直接PCI术后的血栓形成的几率较高,多于术后3d内发生,对于危险因素控制、强化抗栓、规范手术操作是预防支架内血栓形成的主要手段。
【关键词】急性心肌梗死;支架内血栓;心肌梗死;危险因素【中图分类号】R541 【文献标识码】A 【文章编号】ISSN.2095.6681.2020.2..02冠脉内支架置入(PCI)术是冠心病急性心肌梗死治疗最迅速、安全、有效的方法之一,支架内血栓形成(stent thrombosis ST)是通过皮冠状动脉进行治疗percutaneou$coronary intervention PCI)中多发的并发症,也是影响冠脉支架置入术预后的主要因素,虽然发生率只有l%~3%[1],但后果却很严重,容易导致患者术后死亡,虽然目前抗栓治疗不断改进,但是不论是强化抗血小板制剂治疗还是低分子肝素抗凝剂的延长使用,一部分患者依然会发生支架内血栓问题[2]。
我院心内科自2012年8月~2018年8月951例急性ST段抬高性的心肌梗死(STEMI)药物洗脱支架(DES)置入患者中有26例出现围手术期支架内血栓形成现象,现报道如下。
于波:支架内血栓的研究进展冠状动脉支架置人治疗作为冠心病治疗的主要手段在全球范围内得到了迅速发展,在临床上得到越来越广泛的应用。
而支架内血栓(Intro stent thrombosis,IST)作为冠状动脉支架置入术后的严重甚至致命的并发症也日益受到临床医生的关注,对其安全性的质疑及防治成为当今学术界研究的热点之一。
一、支架内血栓的定义和分类2006年美国学术研究联合会(ARC)统一了支架内血栓的定义(图1)。
根据介入治疗后支架内血栓发生的时间窗可以将其分为3类。
急性期支架内血栓,发生于支架置入后0~30天,包括急性支架内血栓(支架置入后24小时内)和亚急性支架内血栓(支架置人后24小时~30天);晚期支架内血栓,发生于支架置入30天~1年;极晚期支架内血栓,发生于支架置入后超过1年[1]。
根据造影结果和临床情况对支架内血栓发生的可能性给出的定义。
肯定的支架内血栓(Definite/Confirmed)指通过造影或者病理确定的支架内血栓。
通过造影判断证实的支架内血栓并且至少下列中的一项在48小时内发生:休息时新出现的急性缺血症状,新出现的急性缺血的心电图表现,典型的心肌坏死标记物动态变化作为证据,或经过尸检或者血栓切除后经病理检查确定的近期支架内血栓。
可能的支架内血栓(Probable):在支架置入一个月内发生的不能解释的死亡;支架置入后与时间无关的,但没有经造影证实的支架内血栓和无任何明确原因的与支架置入血管相关的急性缺血。
可疑的支架内血栓(Possible):从支架置入后30天一直到试验随访结束期间发生的不能解释的死亡。
二、支架内血栓的发生率相关研究显示,急性和亚急性支架内血栓发生率为0.9%~1.8%,其中亚急性支架内血栓有71%发生在术后3.8±4.1天左右。
晚期支架内血栓发生率约为0.6%~0.8%,同时晚期支架内血栓有53%发生在术后57天左右(即3个月内)。
但无论何种支架内血栓,一旦发生,都面临着严重的后果:总体支架内血栓9个月随访时的死亡率为45%~50%。
冠状动脉支架后血栓形成的原因及防治进展
陈国柱;史忠
【期刊名称】《西部医学》
【年(卷),期】2008(20)6
【摘要】支架血栓形成(Stent Thrombosis,ST)是冠心痛介入治疗的严重并发症,可对人体造成灾难性的后果.与普通金属支架(BMS)比较,药物洗脱支架(DES)可明显减少再狭窄率和靶病变的血运重建率.植入支架后可发生早期、晚期、极晚期支架血栓形成,其发生机制并不完全相同.抗血小板、抗凝、调脂治疗可能降低ST的发生率.个体化手术及个体化药物治疗,在解决冠脉血运重建的同时,可减少再狭窄率和降低ST的发生率.ST高危病人在植入支架后应该规律随访,加强对患者的健康教育.【总页数】3页(P1296-1298)
【作者】陈国柱;史忠
【作者单位】第三军医大学新桥医院急救部,重庆,400037;第三军医大学新桥医院急救部,重庆,400037
【正文语种】中文
【中图分类】R815
【相关文献】
1.冠状动脉支架植入术后采取不同的护理干预模式对于患者急性血栓形成的影响[J], 胡清凤
2.药物洗脱支架术后极晚期血栓形成原因及防治进展 [J], 王春玲
3.冠状动脉支架置入后血栓形成的原因和机制 [J], 庞兴学;王显
4.国产盐酸替罗非班治疗冠状动脉支架植入后急性血栓形成1例 [J], 薛朝阳;陆民
5.后64排CT评估冠状动脉支架再狭窄的应用进展 [J], 李琳;王照谦;贾崇富
因版权原因,仅展示原文概要,查看原文内容请购买。