住院病历记录+胸椎压缩性骨折
- 格式:doc
- 大小:26.00 KB
- 文档页数:3

胸腰椎骨折(胸椎压缩性骨折)入院标准:1.中老年患者,有明确外伤史。
2.X线/CT/MRI提示胸椎压缩性骨折。
3.骨折压缩程度小于椎体高度的1/3,无明显脊髓压迫症状。
路径说明:本路径适合于西医诊断为胸椎压缩性骨折的住院患者。
一、胸腰椎骨折(胸椎压缩性骨折)中医临床路径标准住院流程(一)适用对象:中医诊断:第一诊断为胸腰椎骨折(TCD 2019版:A03.06.01.26)。
西医诊断:第一诊断为胸椎压缩性骨折(ICD-10编码:S22.000x003)。
(二)诊断依据1.疾病诊断(1)中医诊断标准:参照《临床诊疗指南-骨科学分册》(中华医学会编著,人民卫生出版社)。
(2)西医诊断标准:参照《外科学(下册)》(8年制和7年制教材临床医学专用、人民卫生出版社)。
患者表现为腰背痛和(或)单(双)侧胁痛,早期大便秘结,有或无明确的外伤史,检查时脊柱外观可正常或可有畸形,伤椎棘突有压痛或叩痛,胁肋无压痛,可合并脊髓损伤,可有不全或完全瘫痪的表现。
影像学检查有助于明确诊断,损伤部位,类型和移位情况。
拍摄胸椎正侧位片,必要时加拍斜位片,CT检查可明确是否有无碎骨片突出于椎管内,并可计算出椎管的前后径与横径损失量。
在MRI片上可以看到椎体骨折出血所致的信号改变和前方的血肿,还可看到因脊髓损伤所表现出的异常高信号。
诊断:结合外伤病史、临床症状及影像学检查综合诊断。
2.证候诊断胸腰椎骨折(腰椎压缩性骨折)临床常见证候:(1)气滞血瘀证:伤后2周内,证属气滞血瘀。
近期胸背部有外伤史,胸背部疼痛剧烈,痛有定处,刺痛,俯仰活动艰难,痛处拒按,舌质紫暗,或有瘀斑,舌苔薄白或薄黄,脉沉涩或弦。
早期常伴有纳呆、胸闷、腹胀痛、恶心呕吐、二便不通等阳明腑实证或蓄血证。
(2)营血不调证:伤后2-4周,证属营血不调。
局部压痛,痛有定处,可按,活动尚可,舌质红,苔薄白或薄黄,脉弦。
(3)肝肾气血亏虚证:伤后4周以上,证属肝肾气血亏虚。
局部轻压痛,活动可,舌质红,苔白或黄,脉沉或细。
椎体压缩性骨折
1急性腰扭伤:有明显腰部扭、闪、挫等外伤史。
伤后一般立即感到腰骶部或骶髂部剧烈疼痛,与此病症状类似,但X线无明显异常改变,多可排除此病。
2 多发性骨髓瘤:1.可表现为多发椎体骨折,多侵犯椎体附件,蛋白电泳可见M峰,此病人有多个椎体压缩,此病需警惕,行相关辅助检查以鉴别。
2.可表现为多发椎体骨折,多侵犯椎体附件,蛋白电泳可见M峰,此病人有多个椎体压缩,但根据腰椎MR影像新鲜骨折以L4节段为主,余为陈旧性骨折,不符合多发性骨髓瘤疾病性质,考虑此病可能性不大,待相关辅助检查以进一步鉴别。
3 椎管内肿瘤:椎管内肿瘤也可表现腰部疼痛等症状,压迫神经时也可表现为神经根刺激症状如放射性下肢痛等,此患者既往无肿瘤病史,无放射性下肢痛,无消瘦,乏力等恶液质症状,腰椎MR未见明显肿瘤征象,暂不考虑此病。
4 盘源性腰痛:表现为单纯性腰部疼痛,病程较长,可向臀部放射,腰椎MRI可见椎间盘退变,但无明显椎间盘突出。
此患症状、体征不支持该诊断,暂不考虑此病。
5腰椎间盘突出症:该病往往表现为腰痛及一侧下肢放射性疼痛。
磁共振检查可见腰椎间盘突出,该患者无下肢放射痛,已予查腰椎MR以进一步鉴别,暂不考虑此病。


胸椎压缩性骨折病历模板范文病历模板:胸椎压缩性骨折患者信息:姓名:_______性别:_______年龄:_______民族:_______婚姻状况:_______住址:_______身份证号:_______联系电话:_______就诊时间:_______年_______月_______日就诊科室:骨科就诊医生:_______病史陈述:患者自诉于_______年_______月_______日无明显外伤史突发背部疼痛,疼痛呈持续性,逐渐加重。
疼痛范围位于背部,无放射痛。
患者无发热、呕吐、腹胀、腹泻等消化系统症状。
无尿频、尿急、尿痛等泌尿系统症状。
无头痛、恶心、呕吐等神经系统症状。
患者就诊于当地医院,经X线片检查发现胸椎压缩性骨折。
为进一步诊治来我院就诊。
既往史:患者既往有“高血压”病史____年,规律口服药物治疗,血压控制尚可。
无其他重大疾病史。
体格检查:生命体征平稳,体型偏瘦,痛苦面容,主动配合检查。
专科检查:脊柱生理弯曲存在,无明显侧弯、旋转畸形。
胸椎_______椎体压缩性骨折,椎体前缘压缩程度约_______%,椎体后缘压缩程度约_______%。
压痛明显,叩痛(+)。
无明显肌肉紧张。
双下肢肌力、肌张力正常,无感觉异常,生理反射存在,病理反射未引出。
辅助检查:1. X线片:胸椎_______椎体压缩性骨折,椎体前缘压缩程度约_______%,椎体后缘压缩程度约_______%。
2. CT扫描:胸椎_______椎体压缩性骨折,椎体前缘压缩程度约_______%,椎体后缘压缩程度约_______%。
骨折周围软组织无明显损伤。
3. 磁共振成像(MRI):胸椎_______椎体压缩性骨折,椎体前缘压缩程度约_______%,椎体后缘压缩程度约_______%。
椎间盘无明显突出,脊髓无明显受压。
诊断:胸椎压缩性骨折治疗方案:1. 保守治疗:包括绝对卧床休息、止痛药物、维生素营养神经、脱水消肿药物等。

(完整版)骨折病病历
患者信息
- 姓名:[患者姓名]
- 年龄:[患者年龄]
- 性别:[患者性别]
- 职业:[患者职业]
- 联系方式:[患者联系方式]
就诊信息
- 就诊日期:[就诊日期]
- 就诊医院:[就诊医院]
- 主治医生:[主治医生姓名]
病情描述
患者在[发生骨折的日期]发生了[骨折部位]骨折,具体描述如下:
[详细描述骨折的发生过程及有关症状、疼痛等适用的病情描述]
检查结果
1. X光检查结果:
- [具体描述骨折的类型、位置、受伤程度等X光检查结果]
2. CT/MRI检查结果(如有):
- [具体描述CT/MRI检查结果]
治疗方案
根据患者的病情和检查结果,医生制定了以下治疗方案:
1. 药物治疗:
- [列出使用的药物,包括药物名称、剂量和用法]
2. 保守治疗:
- [列出采取的保守治疗措施,如石膏固定、休息、物理治疗等]
3. 手术治疗(如有):
- [描述手术的具体过程、手术日期、手术方法等]
治疗效果
患者按照医生的治疗方案积极治疗,取得了如下治疗效果:[描述患者的治疗效果,如疼痛减轻、骨折愈合等]
随访记录
- 第一次随访:[随访日期]
- [记录第一次随访的情况,如疼痛程度、恢复情况等]
- 第二次随访:[随访日期]
- [记录第二次随访的情况,如疼痛程度、恢复情况等]
- 第三次随访:[随访日期]
- [记录第三次随访的情况,如疼痛程度、恢复情况等]
结论
根据患者的病情、治疗方案以及随访记录,患者的骨折病情已取得较好的恢复效果。
以上为患者的(完整版)骨折病病历,仅供参考,详情请咨询医生。

压缩性骨折病例分析-V1压缩性骨折是一种非常常见的骨折类型,很多人都有可能出现这种问题。
在医学方面,对于这种骨折的治疗方法也是有一定的研究的,下面我们就来分析一下一位患有压缩性骨折的病例。
1. 病人的基本情况这位病人是一名35岁的男性,是一位工人,因为从高处摔落所致,造成了腰椎骨折,经过体检和X光摄片的检查,确诊为压缩性骨折。
2. 病情分析经过深入的病情分析,可以发现此次骨折是由于高处坠落造成肌肉、骨头和韧带之间的巨大压力产生导致骨折。
骨折部位是脊柱,这也是人体力量的重要支点,所以一旦发生了这样的骨折,也就代表着人体受到了很大的伤害。
3. 治疗方法针对这种病情,如果不进行治疗,则会对患者的身体产生更大的危害。
因此需要立即采取一些措施进行治疗。
一般针对这种骨折疾病,医生会采用手术的方法,将骨头重新塑形。
通过牵拉和复位,轻轻地将椎骨还原到原来的位置,将压缩的骨头重置,做好固定的手术前和术后护理,同时还需要注意饮食和用药的问题。
4. 术后恢复手术后的恢复期也是非常重要的,因为这关系到骨骼的恢复情况。
这位患者术后坚持定期到医院进行复查,采取科学的恢复训练,同时注意了饮食和卫生的问题。
经过一个月的恢复,这位患者的骨折情况得到了很好的控制,身体情况也得到了较好的恢复,能够进行正常的工作和生活。
综上所述,压缩性骨折是一种比较常见的骨折类型,但是治疗和恢复都需要非常重视。
如果不注意的话,会对患者的身体和骨骼产生更大的危害。
建议患者经常进行体检和检查,以及保持健康的生活方式,及时发现问题并进行处理,能够有效地减少身体的风险。

胸椎压缩性骨折病历模板范文A compression fracture of the thoracic vertebrae is a serious medical condition that can result from trauma, osteoporosis, or other underlying health issues. Thepatient's medical history, including any previous injuriesor bone density issues, should be thoroughly evaluated to determine the cause of the compression fracture. Additionally, a physical examination and diagnostic imaging, such as X-rays or MRI scans, are essential for accurately diagnosing and assessing the extent of the injury. The treatment plan for a compression fracture of the thoracic vertebrae may include pain management, bracing, physical therapy, and in some cases, surgical intervention. It is crucial for healthcare providers to provide comprehensive care and support to patients with this type of injury to ensure optimal recovery and quality of life.From a medical perspective, the documentation of a patient's compression fracture of the thoracic vertebrae should be thorough and detailed. This includes recordingthe mechanism of injury, any associated symptoms, and the results of diagnostic tests. It is essential to accurately describe the location and severity of the fracture, as well as any neurological deficits or other complications that may be present. Additionally, the medical record should document the patient's medical history, including any underlying conditions that may have contributed to the fracture, as well as the treatment plan and follow-up care provided. Proper documentation is crucial for ensuring continuity of care and effective communication among healthcare providers involved in the patient's treatment.From a patient's perspective, a compression fracture of the thoracic vertebrae can be a frightening and painful experience. The sudden onset of severe back pain and potential loss of mobility can be distressing and overwhelming. It is important for healthcare providers to approach patients with empathy and understanding, providing clear and honest communication about their diagnosis and treatment options. Patients may have concerns about their long-term prognosis, ability to perform daily activities, and potential for ongoing pain. It is essential forhealthcare providers to address these concerns and provide support and education to help patients cope with their injury and recovery process.From a rehabilitation perspective, patients with a compression fracture of the thoracic vertebrae may require a comprehensive rehabilitation program to regain strength, mobility, and function. This may include physical therapy to improve posture, strengthen core muscles, and promote safe movement patterns. Occupational therapy may also be beneficial for assisting patients with activities of daily living and adaptive equipment as needed. The rehabilitation team should work closely with the patient to set realistic goals and provide ongoing support and encouragement throughout the recovery process. It is essential for patients to actively participate in their rehabilitation program to achieve the best possible outcomes.From a preventative perspective, patients who have experienced a compression fracture of the thoracic vertebrae should receive education and support to prevent future injuries. This may include guidance on maintainingproper posture, engaging in regular weight-bearing exercise to improve bone density, and minimizing fall risks in the home environment. Additionally, patients with underlying health conditions, such as osteoporosis, should receive appropriate medical management and follow-up care to reduce the risk of future fractures. Healthcare providers play a crucial role in educating and empowering patients to take proactive steps to protect their bone health and overallwell-being.In conclusion, a compression fracture of the thoracic vertebrae is a significant medical issue that requires comprehensive evaluation, treatment, and support.Healthcare providers should approach the management of this condition from a multidisciplinary perspective, addressing the medical, emotional, rehabilitation, and preventative aspects of care. By providing thorough documentation, empathetic support, and proactive rehabilitation and preventative strategies, healthcare providers can help patients with compression fractures of the thoracic vertebrae achieve optimal recovery and long-term well-being.。
腰椎压缩性骨折病历范文英文回答:I recently had a patient who came to me with a complaint of severe back pain. After conducting a thorough examination and reviewing the patient's medical history, I diagnosed the patient with a compression fracture of the lumbar spine, also known as a vertebral compression fracture.A compression fracture occurs when one or more of the vertebrae in the spine collapse or become compressed. This can happen due to trauma, such as a fall or car accident, or due to weakened bones, such as in osteoporosis. In this case, the patient had a history of osteoporosis, which made them more susceptible to this type of fracture.The patient described their pain as a sharp, stabbing sensation in the lower back, which worsened with movement. They also mentioned difficulty in standing or walking forprolonged periods of time. Upon physical examination, I noticed tenderness and limited range of motion in the affected area.To confirm the diagnosis, I ordered imaging tests, such as an X-ray or MRI. These tests revealed a compression fracture in the L3 vertebra. Based on the severity of the fracture and the patient's symptoms, I recommended conservative treatment options, including pain management, rest, and physical therapy.Pain management involved the use of nonsteroidal anti-inflammatory drugs (NSAIDs) and muscle relaxants toalleviate the patient's pain. I also prescribed a backbrace to provide support and stability to the affected area. Rest was essential to allow the fracture to heal properly, and I advised the patient to avoid activities that could exacerbate the pain or further damage the spine.Physical therapy played a crucial role in the patient's recovery. The therapist focused on strengthening the core muscles, improving posture, and increasing flexibility.They also taught the patient proper body mechanics to prevent future injuries. The patient diligently attended physical therapy sessions and practiced the exercises at home, which resulted in significant improvement in pain and mobility.In addition to the medical treatment, I emphasized the importance of adopting a healthy lifestyle to prevent further fractures. This included a balanced diet rich in calcium and vitamin D, regular weight-bearing exercises, and avoiding smoking and excessive alcohol consumption.中文回答:最近我有一个病人来找我,抱怨严重的背痛。
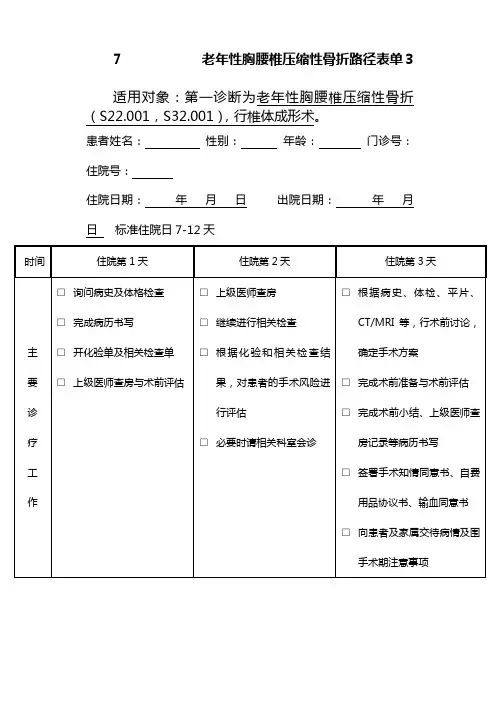
7 老年性胸腰椎压缩性骨折路径表单3适用对象:第一诊断为老年性胸腰椎压缩性骨折(S22.001,S32.001),行椎体成形术。
患者姓名:性别:年龄:门诊号:住院号:住院日期:年月日出院日期:年月日标准住院日7-12天时间住院第1天住院第2天住院第3天主要诊疗工作□询问病史及体格检查□完成病历书写□开化验单及相关检查单□上级医师查房与术前评估□上级医师查房□继续进行相关检查□根据化验和相关检查结果,对患者的手术风险进行评估□必要时请相关科室会诊□根据病史、体检、平片、CT/MRI等,行术前讨论,确定手术方案□完成术前准备与术前评估□完成术前小结、上级医师查房记录等病历书写□签署手术知情同意书、自费用品协议书、输血同意书□向患者及家属交待病情及围手术期注意事项重点医嘱长期医嘱:□骨科护理常规□二级护理□饮食□患者既往基础用药临时医嘱:□血常规、尿常规、大便常规□凝血功能□感染性疾病筛查□肝肾功能、电解质、血糖□胸片、心电图□腰椎平片、CT/MRI□骨密度测定、肺功能、超声心动(根据患者情况选择)长期医嘱:□骨科护理常规□二级护理□饮食□患者既往基础用药临时医嘱:□请相关科室会诊临时医嘱:□术前医嘱:常规准备明日在局麻下行椎体成形术□术前禁食水□抗生素皮试□配血□一次性导尿包□备皮□术前晚灌肠主要护理工作□入院宣教:介绍病房环境、设施和设备□入院护理评估□宣教□观察患者病情变化□心理和生活护理□宣教、备皮等术前准备□提醒患者明晨禁水、禁食病情□无□有,原因:□无□有,原因:□无□有,原因:变异记录1.2.1.2.1.2.护士签名医师签名时间住院第3-5天(手术日)住院第5-6天(术后第1天)住院第6-7天(术后第2天)主要诊疗工作□手术□术者完成手术记录□完成术后病程□上级医师查房□注意神经功能变化□向患者及家属交代病情及术后注意事项□上级医师查房,注意术后病情变化□完成病历书写□注意观察体温□注意神经功能变化□上级医师查房□完成常规病历书写□注意观察体温□注意神经功能变化□注意伤口情况重点医嘱长期医嘱:□麻醉后护理常规□腰椎术后护理常规□一级护理□明日饮食□轴线翻身□留置尿管□抗生素□激素□神经营养药物临时医嘱:□心电血压、血氧监护□吸氧□补液□其他特殊医嘱长期医嘱:□麻醉后护理常规□腰椎术后护理常规□一级护理□饮食□留置尿管□抗生素□激素□神经营养药物□脱水(根据情况)□消炎止痛药物临时医嘱:□通便□镇痛□补液(根据情况)长期医嘱:□麻醉后护理常规□腰椎术后护理常规□一/二级护理□饮食□抗生素□神经营养药物□脱水(根据情况)□消炎止痛药物临时医嘱:□换药、理疗主要护理工作□时观察患者病情变化□术后心理与生活护理□观察患者情况□术后心理与生活护理□指导患者术后功能锻炼□观察患者情况□术后心理与生活护理□指导患者术后功能锻炼病情变异记录□无□有,原因:1.2.□无□有,原因:1.2.□无□有,原因:1.2.护士签名医师签名时间住院第6-8天(术后第3天)住院第6-11天(出院前日)住院第8-12天(出院日)主要诊疗工作□上级医师查房□完成常规病历书写□注意观察体温□注意神经功能变化□注意伤口情况□上级医师查房,进行手术及伤口评估,确定有无手术并发症和切口愈合不良情况,明确是否出院□完成出院记录、病案首页、出院证明书等□向患者交代出院后的注意事项,如:返院复诊的时间、地点,发生紧急情况时的处理等□患者办理出院手续,出院重点医嘱长期医嘱:□麻醉后护理常规□腰椎术后护理常规□一/二级护理□饮食□神经营养药物□脱水(根据情况)□消炎止痛药物□停抗生素临时医嘱:□拍摄术后腰椎平片出院医嘱:□出院带药:神经营养药物、消炎止痛药、口服抗生素□嘱日后拆线换药(根据出院时间决定)□一月后门诊复查□如有不适,随时来诊主要护理工作□观察患者情况□术后心理与生活护理□指导患者术后功能锻炼□指导患者办理出院手续病情变异记录□无□有,原因:1.2.□无□有,原因:1.2.□无□有,原因:1.2.护士签名医师签名。
骨折病历入院记录病程记录出院记录骨折病历入院记录
主要信息
- 患者姓名: [患者姓名]
- 年龄: [患者年龄]
- 性别: [患者性别]
- 住院日期: [住院日期]
- 入院诊断: [入院诊断]
病史陈述
患者于[病史开始日期]因[骨折原因]导致[骨折部位]骨折。
患者描述疼痛程度为[疼痛程度],并出现[其他症状]。
体格检查
- 一般情况: 患者一般状况良好,精神状态正常。
- 皮肤情况: 皮肤完整,无红肿,无渗液。
- 骨折部位: [骨折部位]处可见明显畸形,触及有明显压痛。
- 神经功能: 神经功能正常,无明显感觉丧失。
辅助检查
- X光片: 显示[骨折部位]骨折。
骨折线明显,未见明显移位。
- 其他检查: [其他检查结果]
治疗方案
- 患者接受以下治疗措施:
- [治疗措施1]
- [治疗措施2]
- [治疗措施3]
病程记录
- [病程记录1]
- [病程记录2]
- [病程记录3]
出院记录
经过[住院天数]天的治疗,患者[患者姓名]病情明显好转。
以下是出院记录的详细信息:
- 入院诊断: [入院诊断]
- 出院诊断: [出院诊断]
- 出院医嘱:
- [出院医嘱1]
- [出院医嘱2]
- [出院医嘱3]
随访计划
患者将按照以下随访计划进行复诊:
- [随访计划1]
- [随访计划2]
- [随访计划3]
结论
本次入院记录详细记录了患者骨折情况、治疗方案以及出院情况。
患者目前病情稳定,建议患者按照医嘱进行规定的复诊和康复训练。
一例胸椎压缩性骨折术后病人的护理一、病例简介患者黄东连 , 女 ,62岁,主因:胸背部痛苦伴活动受限 5 天, 于2017-1-18 09:00由家眷陪伴平车住院。
住院诊疗: 胸 10 椎体压缩性骨折胸椎骨质松散症患者向来身体健康,偶有便秘,腰困10年余,于 5 天前往卫生间时摔倒后 , 胸腰部痛苦显然、呈连续性加重 , 严重影响正常生活 , 为求进一步治疗收入我院。
患者自觉病以来无显然体重降落, 营养状态优秀 , 睡眠可 , 便秘 , 小便无显然异样 , 患者为农民 , 有新乡村合作医疗 , 无经济负担。
已婚 , 爱人及二子一女均体健 , 能赐予优秀的心理支持。
患者属于混淆性格 , 能主动与护士交流说出心里想法与要求。
住院后对患者进行安全评估 : 压疮一度风险 , 摔倒二度风险 , 自理能力评估为部分自理。
术前阳性体征回报 :胸椎 1、5TMR平扫 :胸10椎体压缩性骨折胸8、11椎体压缩性改变CT:胸 8、10 楔形变X 线: 胸 10 椎体压缩性骨折。
完美检查后患者无显然手术禁忌于 2017 年 1 月 23 日在基础麻醉下行“胸10 椎体骨质松散性骨折经皮微创椎体成形术”。
术毕返回病房 , 生命体征安稳 , 伤口无溢出 , 术后指导患者轴线翻身 , 行踝泵训练, 第二天依据病情行饮食及直腿抬高功能锻炼指导 , 第三天 , 指导患者进行下地活动。
二、护理查体患者神志清 , 精神可 , 胸腰段脊柱正中及椎旁肌肉紧张 , 压痛 , 叩击痛显然 , 无下肢放射痛 , 胸椎伸屈 , 旋转及侧方活动受限 , 双下肢直腿抬高阴性 , 双下肢感觉活动无显然异样。
三、护理问题 :1、痛苦 : 与手术有关。
客观依照 : 患者伤口疼。
痛苦评分为 5 分。
护理举措 :(1)亲密察看病情变化 , 仔细听取患者的主诉 , 鉴识痛苦的性质。
(2)实时赐予心理劝导 , 向患者解说有关痛苦知识的的有关内容 ,缓解患者的紧张情绪 , 获得家眷的配合。
个案L1压缩性骨折多发肋骨骨折伴血气胸应激性溃疡骨十:李丽英林爱玲2011年7月29日病史简介:骨十19 王圣达,男,56岁,患者于7月11日11:30以腰背部疼痛伴活动受限为主诉平车入院,入院时T:37 P:84 R:20 BP:128/80 ,入院后给予完善各项检查、消炎止痛、消肿治疗。
7.12胸片示左侧多发肋骨骨折伴左侧胸腔积液;腰椎正侧位示L1压缩性骨折继发椎管狭窄,左股骨骨折术后,粪常规示无异常,尿常规示尿中有红细胞,血常规示白细胞升高,达12.1 10.9,中性粒细胞升高,淋巴细胞百分比下降,达11.9%,血气分析示:二氧化碳分压31.7(34—48),ph:7.47升高,氧分压67(83—108),生化示:白蛋白54-9下降,球蛋白18.4下降,谷草83升高,后来复查血常规示:白细胞10.9升高,中性粒细胞百分比升高。
7.13请胸外科会诊,行双肺,肝,脾CT,CT示左肾,包膜下血肿,于17:00行胸腔闭式引流,复查血气Pco2:25.5下降(34-48),PO2:下降59.8mmhg,PH正常,氧含量13.10下降(17.5-23)尿常规示尿酸碱度7.04升高,比重下降,尿中,细胞正常,当天腰椎MR示L1椎体爆裂骨折伴椎管狭窄,L1水平腰背部软组织挫伤,双肺,肝,脾,CT示双下肺挫裂伤,左肺下叶膨胀不良,双肺胸腔积液,左肾包膜下血肿。
7.14手术暂停。
7.15右请胸外科会诊,诉胸廓挤压征(+),仍右胸痛,继续胸腔闭式引流,16:00请消化科会诊。
诉06:00多突然排黑便,之后出现身体无力,出冷汗,BP8560mmhgP110次分,上腹部压痛明显,诉既往有消化性溃疡及肝炎史,即给予止血,补液处理,建议行急诊胃镜及普外会诊。
7.16请外科张孝忠会诊,无外科介入指征,同意内科会诊意见,治疗上给予止血,保护胃粘膜,当天给予输血4U,血浆400ML,补液,抗感染等治疗。
7.18 20:00患者心率140分,不齐,请心内科会诊,后来也请了消化科会诊,考虑上消化道出血,应激性溃疡。
海口市中医院科别:外科床号:6住院病历记录住院号:1000042802姓名:张琼雄出生地:海口市性别:男籍贯:海南省海口市年龄:82岁工作单位:海口市橡胶一厂民族:汉族常住地址:海口市联贵坊66号婚况:已婚入院时间:2010年11日17日16时00分职业:产业工人病史采集时间:2010年11月17日16时00分发病节气:立冬病史陈述者:患者本人及其家属—————————————————————————————————————主诉:不慎跌倒致胸腰部疼痛,活动受限20天,加重1天。
现病史:患者20天前不慎跌倒出现胸腰背部疼痛,转侧困难,咳嗽、如厕时疼痛加重,无畏寒、发热,曾在海口市人民医院诊治,拍胸腰部CT片提示:1.T12椎体压缩性骨折;2.腰椎退行性变;3.L4椎体轻度滑脱。
拟“T12椎体压缩性骨折”治疗(具体不详),胸腰部疼痛症状有好转,但症状反复。
1天前无明显外伤情况下胸腰部疼痛加重,无法下床活动,患者家属为求进一步系统治疗,立即由家人送患者到我院就诊。
门诊拟T12椎体压缩性骨折收入我科。
自起病以来,患者症状如前所述,无咳嗽,无咳痰,无腹痛,患者体重无明显变化,二便调,纳眠可。
既往史:既往史无特殊;否认肝炎、结核病史,否认有药物及食物过敏史,否认手术、输血史,预防接种史不详。
个人史:出生原籍,久居海口。
生活条件、环境一般。
未曾到过疫区,无毒物接触史。
无特殊不良嗜好,无重大精神创伤史。
婚育史:适龄结婚,育有子女。
家族史:家人体健,否认有家族性遗传病史。
体格检查T: 37.5℃ P: 72次/分 R: 20次/分 BP:150/90mmHg 一般情况:神志清晰,发育正常,较消瘦,自动体位,检查合作。
皮肤:温度正常,稍苍白,全身皮肤黏膜无黄染,无出血点,无蜘蛛痣、皮疹。
淋巴结:全身浅表淋巴结未触及肿大。
头部头颅:头颅无畸形,无压痛,无肿块,头发色黑,有光泽,分布均匀。
眼:眉毛无脱落,无倒睫,眼睑无下垂、水肿及内外翻,结合膜无充血、出血及滤泡。
胸骨骨折病历模板范文# 胸骨骨折病历。
一、基本信息。
1. 姓名:[患者姓名]2. 性别:[男/女]3. 年龄:[X]岁。
4. 职业:[具体职业]5. 住址:[详细住址]6. 联系方式:[电话号码]二、就诊时间。
[年/月/日] [具体时刻]三、主诉。
“大夫啊,我这胸口可疼得厉害,就之前不小心撞了一下,感觉骨头都断了似的。
”患者捂着胸口,皱着眉头说道。
四、现病史。
患者于[受伤时间]前,在[受伤地点](例如:家里、工作场所、路上等)发生意外受伤。
当时患者正[描述受伤场景,比如:搬东西没注意,被重物撞到了胸口;走路不小心撞到了电线杆之类的],胸部直接受到[撞击物的描述,如坚硬的桌角、铁棒等]撞击,力量较大。
受伤瞬间即感胸骨处剧痛,疼痛呈持续性,像有一把火在胸口烧似的,随着呼吸、咳嗽或者身体稍微一动就加重,就像有人在伤口上撒盐。
患者当时就不敢乱动了,原地休息了一会儿,可这疼痛一点也没减轻,所以赶紧来咱们医院了。
受伤后患者无昏迷,无恶心、呕吐,无头晕、头痛等不适。
但是因为这胸口疼得厉害,自己感觉呼吸都有点费劲,像有个大石头压在胸口,吸气的时候疼得更明显,只能浅浅地呼吸。
五、既往史。
1. 患者既往身体还算不错,没有什么大病,没得过心脏病、高血压、糖尿病这些让人头疼的慢性病。
2. 之前也没做过什么大手术,就小时候因为调皮摔破了胳膊,做过一次小的缝合手术,恢复得还挺好。
3. 没有药物过敏史,平常感冒发烧吃个药啥的,都没出过啥问题。
六、体格检查。
1. 一般情况。
患者神志清楚,精神状态看起来不太好,毕竟被胸口疼折磨得够呛。
体温正常,血压[具体数值],心率[具体数值],呼吸有点急促,每分钟[具体数值]次,比正常稍微快了点,可能是胸口疼得不敢正常呼吸的原因。
2. 胸部检查。
视诊:胸部皮肤表面有一片轻微的瘀斑,就在胸骨的位置,大概有[描述瘀斑大小],像个小紫茄子似的。
胸骨处有点肿胀,看起来就不太对劲。
触诊:一碰到胸骨,患者就疼得“嘶嘶”吸冷气。
一例胸椎压缩性骨折术后病人得护理一、病例简介患者黄东连,女,62岁,主因:胸背部疼痛伴活动受限5天,于2017-1-18 09:00由家属陪同平车入院、入院诊断:胸10椎体压缩性骨折胸椎骨质疏松症患者平素身体健康,偶有便秘,腰困10年余,于5天前去厕所时跌倒后,胸腰部疼痛明显、呈持续性加重,严重影响正常生活,为求进一步治疗收入我院。
患者自发病以来无明显体重下降,营养状态良好,睡眠可,便秘,小便无明显异常,患者为农民,有新农村合作医疗,无经济负担。
已婚,爱人及二子一女均体健,能给予良好得心理支持、患者属于混合性格,能主动与护士沟通说出内心想法与要求。
入院后对患者进行安全评估:压疮一度风险,跌倒二度风险,自理能力评估为部分自理。
术前阳性体征回报:胸椎1。
5TMR平扫: 胸10椎体压缩性骨折胸8.11椎体压缩性改变CT:胸8、10 楔形变X线:胸10椎体压缩性骨折、完善检查后患者无明显手术禁忌于2017年1月23日在基础麻醉下行“胸10椎体骨质疏松性骨折经皮微创椎体成形术”。
术毕返回病房,生命体征平稳,伤口无渗出,术后指导患者轴线翻身,行踝泵训练,次日根据病情行饮食及直腿抬高功能锻炼指导,第三天,指导患者进行下地活动。
二、护理查体患者神志清,精神可,胸腰段脊柱正中及椎旁肌肉紧张,压痛,叩击痛明显,无下肢放射痛,胸椎伸屈,旋转及侧方活动受限,双下肢直腿抬高阴性,双下肢感觉活动无明显异常。
三、护理问题:1、疼痛:与手术有关。
客观依据:患者伤口疼。
疼痛评分为5分。
护理措施:(1)密切观察病情变化,认真听取患者得主诉,鉴别疼痛得性质、(2)及时给予心理疏导,向患者讲解有关疼痛知识得得相关内容,缓解患者得紧张情绪,取得家属得配合。
(3)若因紧张、恐惧而产生得疼痛,可给予一些自己喜爱得音乐,舒缓情绪,使其沉浸在优美得旋律中而忽略疼痛;或者聊一些感兴趣得话题,转移注意力;也可以温水擦浴,降低不适,增加舒适感。
(4)必要时,及时给予止痛药.效果评价:术后第三天患者疼痛评分为1分,主诉在体位变化时偶有轻微疼痛,可以忍受。
海口市中医院
科别:外科床号:6
住院病历记录住院号:1000042802
姓名:张琼雄出生地:海口市
性别:男籍贯:海南省海口市
年龄:82岁工作单位:海口市橡胶一厂
民族:汉族常住地址:海口市联贵坊66号
婚况:已婚入院时间:2010年11日17日16时00分职业:产业工人病史采集时间:2010年11月17日16时00分发病节气:立冬病史陈述者:患者本人及其家属—————————————————————————————————————主诉:不慎跌倒致胸腰部疼痛,活动受限20天,加重1天。
现病史:患者20天前不慎跌倒出现胸腰背部疼痛,转侧困难,咳嗽、如厕时疼痛加重,无畏寒、发热,曾在海口市人民医院诊治,拍胸腰部CT片提示:1.T12椎体压缩性骨折;2.腰椎退行性变;3.L4椎体轻度滑脱。
拟“T12椎体压缩性骨折”治疗(具体不详),胸腰部疼痛症状有好转,但症状反复。
1天前无明显外伤情况下胸腰部疼痛加重,无法下床活动,患者家属为求进一步系统治疗,立即由家人送患者到我院就诊。
门诊拟T12椎体压缩性骨折收入我科。
自起病以来,患者症状如前所述,无咳嗽,无咳痰,无腹痛,患者体重无明显变化,二便调,纳眠可。
既往史:既往史无特殊;否认肝炎、结核病史,否认有药物及食物过敏史,否认手术、输血史,预防接种史不详。
个人史:出生原籍,久居海口。
生活条件、环境一般。
未曾到过疫区,无毒物接触史。
无特殊不良嗜好,无重大精神创伤史。
婚育史:适龄结婚,育有子女。
家族史:家人体健,否认有家族性遗传病史。
体格检查
T: 37.5℃ P: 72次/分 R: 20次/分 BP:150/90mmHg 一般情况:神志清晰,发育正常,较消瘦,自动体位,检查合作。
皮肤:温度正常,稍苍白,全身皮肤黏膜无黄染,无出血点,无蜘蛛痣、皮疹。
淋巴结:全身浅表淋巴结未触及肿大。
头部
头颅:头颅无畸形,无压痛,无肿块,头发色黑,有光泽,分布均匀。
眼:眉毛无脱落,无倒睫,眼睑无下垂、水肿及内外翻,结合膜无充血、出血及滤泡。
巩膜未见黄染。
角膜透明,双侧瞳孔等大、等圆、对光反射、调节反射存在。
耳:听力正常,外耳道无流脓,乳突无压痛。
姓名:张琼雄住院病历记录续页住院号:1000042802鼻:无畸形,中隔无偏曲,鼻腔通畅,无异常分泌物,鼻旁窦无压痛。
口腔:无特殊气味,唇无发绀,牙齿排列整齐,无龋齿,牙龈无红肿溢脓,舌苔
薄白,咽部轻度充血,后壁无滤泡,声音无嘶哑,腮腺无肿大。
颈部:颈项疼痛,有右肩背部反射疼痛,同时伴有眩晕;尤以体位改变时眩晕明显。
无双上肢放射疼痛,甲状腺无肿大,气管居中,颈静脉无怒张,
胸部:胸廓平坦,胸壁无压痛,胸壁静脉无曲张,乳房扁平,松弛,无硬结。
无皮
下捻发感。
肺脏:
视诊:呼吸运动两侧相等,呼吸较浅快,节律规则。
触诊:呼吸运动正常,两侧相等,读音震颤两侧对称,无胸膜摩擦感。
叩诊:双肺呈清音,右肺尖宽3cm,左肺尖宽4cm,右肺下界在右锁骨中线、腋中线及
肩胛线处分别为第6、第8、第10肋间,两肺下缘移动度约2cm.。
听诊:双肺呼吸音稍减弱,双肺未闻及干湿罗音,未闻及异常呼吸音,语音传导减弱,
未闻及胸膜摩擦音。
心脏:
视诊:心前区无隆起,心尖搏动在左侧第5肋间锁骨中线内1cm外最明显。
搏动范围
2cm。
触诊:心尖搏动位置同上,无抬举感,未触及震颤及心包摩擦感。
叩诊:心浊音界如下所示。
右(cm)肋间左(cm)
3 Ⅱ 2
3 Ⅲ 3.5
4 Ⅳ 6
Ⅴ 7.5
左锁骨中线距前正中线9 cm。
听诊:心率72次/min,节律齐,未闻及病理性杂音、心包摩擦音。
血管检查:桡动脉搏动两侧相等。
脉率80次/min,末见毛细血管搏动,无枪击音或杜氏双重音。
腹部:
视诊;腹部无膨隆,未见腹壁静脉显露及蠕动波。
触诊:腹软,无压痛及反跳痛。
肝脾肋下未触及。
无液波震颤。
未触及包块。
姓名:张琼雄住院病历记录续页住院号:1000042802
叩诊:腹水征(-),双肾区、肝区均无叩痛。
听诊;肠鸣音5次/min,无振水音及血管杂音。
外阴及肛门:无外痔、脱肛。
外生殖器无畸形,发育正常。
脊柱及四肢:四肢无畸形,各关节无红肿,活动自如,无杵状指,四肢肌力、肌张力正常,双下肢无浮肿。
腰椎详见专科情况。
神经系统:双侧肱二头肌、肱三头肌腱反射及双膝腱、跟腱反射均正常。
专科情况:胸腰椎生理曲度减少,未见瘀斑及出血点,T12椎体压痛,叩击痛(+),活动时疼痛加重,双下肢运动、感觉正常,生理反射正常,病理反射未引出;双直腿抬高试验左80°右80°,加强试验(-)、屈髋屈膝试验(-)。
辅助检查:海口市人民胸腰部CT片(2010-10-28)提示:1.T12椎体压缩性骨折;
2.腰椎退行性变;
3.L4椎体轻度滑脱。
我院X片提示:1、右上肺陈旧性肺结核;2、胸12椎体压缩性骨折;3、腰椎退行性变;4、L4椎体前滑Ⅰ度;5、疑L4/5椎间盘病变。
心电图:1、窦性心动过速;2、异常Q波。
病史摘要:患者张琼雄,男性,80岁,因“不慎跌倒致胸腰部疼痛,活动受限20天入院,不能站立和行走,无畏寒发热,入院后,完备各项入院检查,予卧床、腰部中药熏洗,活血化瘀,舒筋通络药物等对症治疗,同时积极治疗其他合并症。
出院时患者胸腰部无疼痛,转侧尚可,腰部压痛不明显,无叩击痛。
入院查体:T12椎体压痛,叩击痛(+),活动时疼痛加重,双下肢运动、感觉正常,双直腿抬高试验左80°右80°,加强试验(-)、屈髋屈膝试验(-)。
X片示:1、右上肺陈旧性肺结核;2、胸12椎体压缩性骨折;3、腰椎退行性变;4、L4椎体前滑Ⅰ度;5、疑L4/5椎间盘病变。
心电图:1、窦性心动过速;2、异常Q波。
初步诊断:
西医诊断:1、T12椎体压缩性骨折
2、高血压病2级高危组
实习医师:
医师签名:。