Adoptive T-cell therapy for__ melanoma cost of mft
- 格式:pdf
- 大小:1.48 MB
- 文档页数:22
中国肿瘤生物治疗杂志 http :// Chin J Cancer Biother ,Feb.2011,Vol.18,No.1DOI :10.3872/j.issn.1007⁃385X.2011.01.001·述 评·肿瘤过继细胞治疗———老故事新演绎钱其军,吴孟超(第二军医大学东方肝胆外科医院,上海200438) 钱其军,博士、研究员、博士生导师,第二军医大学东方肝胆外科医院基因⁃病毒治疗实验室主任,浙江省基因治疗中心常务副主任;国家杰出青年基金获得者,上海市科技领军人才及优秀学科带头人;中国医药生物技术协会医药生物技术临床应用专业委员会常务委员,中国抗癌协会肿瘤生物治疗专业委员会委员;中华肿瘤杂志、中国肿瘤生物治疗杂志、癌症等杂志编委。
主要从事肿瘤的基因⁃病毒治疗及免疫细胞过继治疗方面的研究。
作为负责人承担国家杰出青年基金项目1项、国家自然科学基金国际合作重大项目1项、国家自然科学基金重点项目1项、国家自然科学基金海外杰出青年项目1项(国内负责人)、国家自然科学基金面上项目3项、国家863项目2项及艾滋病和病毒肝炎等重大传染病防治重点专项子项目1项。
近年来荣获省部级奖项5项,在Cancer Res 、Clin Cancer Res 、Mol Ther 、Plos One 等杂志发表SCI⁃E 论文40余篇,获授权中国发明专利6项、美国发明专利1项。
E⁃mail :qianqj@sino⁃ 。
吴孟超,国际著名肝胆外科专家,中国肝脏外科的开拓者和主要创始人之一,中国科学院院士,主任医师、教授、临床医学博士后流动站导师,2005年度国家最高科学技术奖获得者。
现任第二军医大学东方肝胆外科医院院长、东方肝胆外科研究所所长,兼任中德医学协会副理事长、全国医学专业学位教育指导委员会副主任、解放军医学科学技术委员会副主任、解放军总后勤部专家组副组长、中日消化道外科学顾问等职。
擅长肝胆疾病的各种外科手术治疗,尤其擅长肝癌、肝血管瘤等疾病的外科手术治疗。
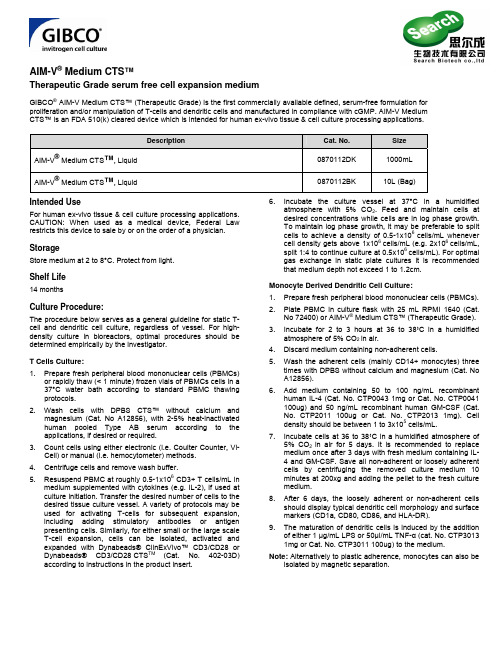
AIM-V® Medium CTS™Therapeutic Grade serum free cell expansion mediumGIBCO® AIM-V Medium CTS™ (Therapeutic Grade) is the first commercially available defined, serum-free formulation for proliferation and/or manipulation of T-cells and dendritic cells and manufactured in compliance with cGMP. AIM-V Medium CTS™ is an FDA 510(k) cleared device which is intended for human ex-vivo tissue & cell culture processing applications.Description Cat. No. SizeAIM-V® Medium CTS™, Liquid 0870112DK 1000mL AIM-V® Medium CTS™, Liquid 0870112BK 10L(Bag)IntendedUseFor human ex-vivo tissue & cell culture processing applications. CAUTION: When used as a medical device, Federal Law restricts this device to sale by or on the order of a physician. StorageStore medium at 2 to 8°C. Protect from light.Shelf Life14 monthsCulture Procedure:The procedure below serves as a general guideline for static T- cell and dendritic cell culture, regardless of vessel. For high-density culture in bioreactors, optimal procedures should be determined empirically by the investigator.T Cells Culture:1. Prepare fresh peripheral blood mononuclear cells (PBMCs)or rapidly thaw (< 1 minute) frozen vials of PBMCs cells in a 37°C water bath according to standard PBMC thawing protocols.2. Wash cells with DPBS CTS™ without calcium andmagnesium (Cat. No A12856), with 2-5% heat-inactivated human pooled Type AB serum according to the applications, if desired or required.3. Count cells using either electronic (i.e. Coulter Counter, Vi-Cell) or manual (i.e. hemocytometer) methods.4. Centrifuge cells and remove wash buffer.5. Resuspend PBMC at roughly 0.5-1x106 CD3+ T cells/mL inmedium supplemented with cytokines (e.g. IL-2), if used at culture initiation. Transfer the desired number of cells to the desired tissue culture vessel. A variety of protocols may be used for activating T-cells for subsequent expansion, including adding stimulatory antibodies or antigen presenting cells. Similarly, for either small or the large scale T-cell expansion, cells can be isolated, activated and expanded with Dynabeads® ClinExVivo™ CD3/CD28 or Dynabeads® CD3/CD28 CTS TM(Cat. No. 402-03D) according to instructions in the product insert. 6. Incubate the culture vessel at 37°C in a humidifiedatmosphere with 5% CO2. Feed and maintain cells at desired concentrations while cells are in log phase growth.To maintain log phase growth, it may be preferable to split cells to achieve a density of 0.5-1x106cells/mL whenever cell density gets above 1x106cells/mL (e.g. 2x106cells/mL, split 1:4 to continue culture at 0.5x106cells/mL). For optimal gas exchange in static plate cultures it is recommended that medium depth not exceed 1 to 1.2cm.Monocyte Derived Dendritic Cell Culture:1. Prepare fresh peripheral blood mononuclear cells (PBMCs).2. Plate PBMC in culture flask with 25 mL RPMI 1640 (Cat.No 72400) or AIM-V® Medium CTS™ (Therapeutic Grade).3. Incubate for 2 to 3 hours at 36 to 38˚C in a humidified atmosphere of 5% CO2 in air.4. Discard medium containing non-adherent cells.5. Wash the adherent cells (mainly CD14+ monocytes) threetimes with DPBS without calcium and magnesium (Cat. No A12856).6. Add medium containing 50 to 100 ng/mL recombinanthuman IL-4 (Cat. No. CTP0043 1mg or Cat. No. CTP0041 100ug) and 50 ng/mL recombinant human GM-CSF (Cat.No. CTP2011 100ug or Cat. No. CTP2013 1mg). Cell density should be between 1 to 3x105 cells/mL.7. Incubate cells at 36 to 38˚C in a humidified atmosphere of5% CO2 in air for 5 days. It is recommended to replace medium once after 3 days with fresh medium containing IL-4 and GM-CSF. Save all non-adherent or loosely adherentcells by centrifuging the removed culture medium 10 minutes at 200xg and adding the pellet to the fresh culture medium.8. After 6 days, the loosely adherent or non-adherent cellsshould display typical dendritic cell morphology and surface markers (CD1a, CD80, CD86, and HLA-DR).9. The maturation of dendritic cells is induced by the additionof either 1 µg/mL LPS or 50µl/mL TNF-α (cat. No. CTP3013 1mg or Cat. No. CTP3011 100ug) to the medium.Note: Alternatively to plastic adherence, monocytes can also be isolated by magnetic separation.Related ProductsDulbecco's Phosphate Buffered Saline CTS™ (DPBS) without calcium, magnesium (1X), liquid (A12856) L-Glutamine-200mM (100X), liquid (25030)Dynabeads ClinExVivo™ CD3/CD28 ®or Dynabeads CD3/CD28 ®CTS TM (402-03D) DynaMag™ CTS™ (121-02)IL-2 CTS™ REC HU (CTP0021 100ug or CTP0023 1mg) IL-7 CTS™ REC HU (CTP0071 100ug or CTP0073 1mg) IL-4 CTS™ REC HU (CTP0041 100ug or CTP0043 1mg) GM-CSF CTS™ REC HU (CTP2011 100ug or CTP2013 1mg) TNF-α CTS™ (CTP3011 100ug or CTP3013 1mg)Technical SupportFor additional product and technical information, such as Material Safety Data Sheets (MSDS), Certificate of Analysis,etc, please visit our website at /celltherapysupport/. For further assistance, please email our Technical Support team at celltherapysupport@The trademarks mentioned herein are the property of Life Technologies Corporation or their respective ownersReferences1.Rebecca J et al., (2010) Natural exposure to cutaneous anthrax gives long lasting T cell immunity encompassing infection-specific Epitopes. J. Immunol., 184: 3814 – 38212.Fabricius D et al., (2010) Prostaglandin E2 inhibits IFN-α secretion and Th1 costimulation by human plasmacytoid dendritic cells via E-prostanoid 2 and E-prostanoid 4 receptor engagement. J. Immunol., 184: 677 – 6843.Nesbit L et al., (2010) Polyfunctional T Lymphocytes Are in the Peripheral Blood of Donors Naturally Immune to Coccidioidomycosis and Are Not Induced by Dendritic Cells . Infect. Immun., 78: 309 - 3154. Jahrsdorfer B et al., (2010) Granzyme B produced by human plasmacytoid dendritic cells suppresses T-cell expansion . Blood, 115: 1156 – 11655.Csillag A et al., (2010) Pollen-Induced Oxidative Stress Influences Both Innate and Adaptive Immune Responses via Altering Dendritic Cell Functions. J. Immunol., 184: 2377 – 23856.Cornberg M et al., (2010) CD8 T Cell Cross-Reactivity Networks Mediate Heterologous Immunity in Human EBV and Murine Vaccinia Virus Infections. J. Immunol., 184: 2825 - 2838.7.Bellone S et al., (2009) Human Papillomavirus Type 16 (HPV-16) Virus-Like Particle L1-Specific CD8 Cytotoxic T Lymphocytes (CTLs) Are Equally Effective as E7-Specific CD8 CTLs in Killing Autologous HPV-16-Positive Tumor Cells in Cervical Cancer Patients: Implications for L1 Dendritic Cell-Based Therapeutic Vaccines ++. J. Virol., 83: 6779 - 67898. Sato K et al., (2009) Impact of culture medium on the expansion of T cells for immunotherapy. Cytotherapy 11: 4-119.Liu ZW et al., (2009) A CD26-Controlled Cell Surface Cascade for Regulation of T Cell Motility and Chemokine Signals . J. Immunol ., 183: 3616 - 3624.10. Megyeri M et al., (2009) Complement Protease MASP-1 Activates HumanEndothelial Cells: PAR4 Activation Is a Link between Complement and Endothelial Function. J. Immunol., 183: 3409 - 3416. 11.Manfred L et al., (2005) Functional characterization of monocyte-derived dendritic cells generated under serum free culture conditions. Immunology letters 99: 209-21612. Nagorsen D et al., (2003) Biased epitope selection by recombinant vaccinia-virus (rVV)-infected mature or immature dendritic cells. Gene Therapy 10: 1754-1765 13. Lotem M et al., (2006) Presentation of tumor antigens by dendritic cells genetically modified with viral and nonviral vectors. J immunotherapy 29: 616-62714.Dietze B et al. (2008) An improved method to generate equine dendritic cells from peripheral blood mononuclear cells: divergent maturation programs by IL-4 and LPS. Immunobiology 213:751–758.15.Meehan KR et al. (2008) Development of a clinical model for ex vivo expansion of multiple populations of effector cells for adoptive cellular therapy. Cytotherapy 10: 30–37.16. Ye Z et al. (2006) Human dendritic cells engineered to express alpha tumornecrosis factor maintain cellular maturation and T-cell stimulation capacity. Cancer Biother Radiopharm 21:613–622.17. Choi BH et al. (2006) Optimization of the concentration of autologous serum forgeneration of leukemic dendritic cells from acute myeloid leukemic cells for clinical immunotherapy. J Clin Apher 21:233–240. 18.Imataki O et al. (2006) Efficient ex vivo expansion of alpha24+ NKT cells derived from G-CSF-mobilized blood cells. J Immunother 29:320–327.19. Peng JC et al. (2005) Generation and maturation of dendritic cells for clinicalapplication under serum-free conditions. J Immunother 28:599–609. 20. Trickett AE et al. (2002) Ex vivo expansion of functional T lymphocytes from HIV infected individuals. J Immunol Methods 262:71–83.21.Carlens S et al. (2000) Ex vivo T lymphocyte expansion for retroviral transduction: influence of serum-free media on variations in cell expansion rates and lymphocyte subset distribution. Exp Hematol 28:1137–1146.22.Kambe N et al. (2000) An improved procedure for the development of human mast cells from dispersed fetal liver cells in serum-free culture medium. J Immunol Methods 240:101–110.23. Gerin PA et al. (1999) Production of retroviral vectors for gene therapy with thehuman packaging cell line FLYRD18. Biotechnol Prog 15:941–948. 24. Slunt JB et al. (1997) Human T-cell responses to Trichophyton tonsurans:inhibition using the serum free medium Aim-V. Clin Exp Allergy 27:1184–1192. 25. Kreuzfelder E (1996) Assessment of peripheral blood mononuclear cellproliferation by [2-3H]adenine uptake in the woodchuck model. Clin Immunol Immunopathol 78:223–227. 26.Causey AL (1994) A serum-free medium for human primary T lymphocyte culture. J Immunol Methods 175:115–121.27. Freedman RS et al. (1994) Large-scale expansion in interleukin-2 oftumorinfiltrating lymphocytes from patients with ovarian carcinoma for adoptive immunotherapy. J Immunol Methods 167:145–160. 28.Nomura K et al. (1993) [Study of adoptive immunotherapy for metastatic renal cell carcinoma with lymphokine-activated killer (LAK) cells and interleukin-2. II. Clinical evaluation.] Nippon Hinyokika Gakkai Zasshi 84:831–840. Japanese.29.Kaldjian EP et al. (1992) Enhancement of lymphocyte proliferation assays by use of serum-free medium. J Immunol Methods 147:189–195.30. Hayakawa K et al. (1991) Study of tumor-infiltrating lymphocytes for adoptivetherapy of renal cell carcinoma (RCC) and metastatic melanoma: sequential proliferation of cytotoxic natural killer and noncytotoxic T cells in RCC. J Immunother 10:313–325. 31.McVicar DW et al. (1991) A comparison of serum-free media for the support of in vitro mitogen-induced blastogenic expansion of cytolytic lymphocytes. Cytotechnology 6:105–113.32. Burg S et al. (1991) [Effect of different media on long-term cultivation of humansynovial macrophages.] Z Rheumatol 50:142–150. German. 33. Helinski EH et al. (1988) Long-term cultivation of functional human macrophagesin Teflon dishes with serum-free media. J Leukoc Biol 44:111–121. 34. Robyn S et al. (2007) RA8, A human anti-CD25 antibody against human Tregcells. Hybridoma 26:119–130. 35.Chena X et al. (2006) Induction of primary anti-HIV CD4 and CD8 T cell responses by dendritic cells transduced with self-inactivating lentiviral vectors. Cell Immunol 243:10–18.36. Grant R et al. (2008) CCL2 increases X4-tropic HIV-1 entry into resting CD4+ Tcells. J Biol Chem 283:30745–30753. 37.Hagihara M et al. (2003) Increased frequency of CD3/8/56-positive umbilical cord blood T lymphocytes after allo-priming in vitro. Ann Hematol 82:166–170.38. Wang Z et al. (2006) Application of serum-free culture medium for preparation ofA-NK cells. Cell Mol Immunol 3:391–395. 39. Morecki S et al. (1991) Retrovirus-mediated gene transfer into CD4+ and CD8+human T cell subsets derived from tumor-infiltrating lymphocytes and peripheral blood mononuclear cells. Cancer Immunol Immunother 32:342–352. 40.Johansen P et al. (2003) CD4 T cells guarantee optimal competitive fitness of CD8 memory T cells. Eur J Immunol 34:91–97.June 2010Form No. 5047。
22 OCTOBER 2010 VOL 330 SCIENCE 440C R ED I T : R Y A N S N O O K , W W W .R Y A N S N O O K .C O MBETHESDA, MARYLAND—O n a corner of Steven Rosenberg’s desk rests a small, gold figurine representing Sisyphus, its arms straining to push a boulder forward. A gift from his wife when he joined the U.S. National Cancer Institute (NCI) here as chief of surgery back in 1974, it is uncan-nily apt: Rosenberg has spent 3 decades roll-ing metaphorical boulders uphill, only to see them tumble back down again.Rosenberg’s specialty is immunotherapy; he tries to harness a patient’s own immune system to fi ght cancer. He and others have seen remnants of immune system attacks on tumors, but the cancer recovers and takes off. Efforts to lend the immune system a hand have raised hopes, leading to large clinical tri-als of cancer vaccines. But all have fl opped. And year after year, nearly all of Rosenberg’s patients, recipients of radical experimental treatments, succumbed to their cancer.Nearly all, that is, until recently.Slowly, new immune-based therapies are registering successes. In some people riddledwith the aggressive skin cancer melanoma, immunotherapy has not only eliminated dis-ease but also kept it at bay for years. Such outcomes are virtually unheard of in patients with metastatic disease that has spread through the body. Last month, NCI awarded $14 million to the Fred Hutchinson Cancer Research Center in Seattle, Washington, so it could launch a new national network of immunotherapy clinical trials.From a patient’s perspective, the achieve-ments are still tenuous. Some individuals respond dramatically. But only a fraction are treated successfully—about 15% at most, though some small trials have hints of higher numbers. What excites immunotherapists is that this modest group of responders—the “tail end of the curve”—keeps showing up in recent studies. This year, it appeared in trials of two antibodies used against several dif-ferent cancers, and in data from Rosenberg’s cell therapy recently published or presented at meetings. With more tinkering, cancer specialists hope to shift additional patientsinto the responder category and devise more powerful combination treatments. Accus-tomed to disappointment, they have rarely been so confi dent.At the same time, their successes are rais-ing deep questions about where cancer ther-apy is headed. Integrating immunotherapy into clinical care will pose challenges of its own. Patients may take months to respond, making it diffi cult to assess whether treatment is helping. Furthermore, some treatments are highly personalized and impossible to admin-ister outside of specialized settings. This makes them extraordinarily expensive. Many specialists wonder whether they can really become part of standard cancer care.Rosenberg is a believer. “The goal right now is to find things that work,” he says. “When you fi nd things that work, industry fi nds ways to make it happen.”Rocky startO ne patient has never left Rosenberg’s thoughts. As a junior resident in a Bos-ton hospital in 1968, Rosenberg met James DeAngelo, then in his 60s, who had been admitted for gallbladder surgery. Twelve years earlier, DeAngelo had developed a stomach cancer that spread to his liver and was sent home to die. Instead, his cancer spontaneously regressed without treatment—“one of the rarest events in all of medicine,” Rosenberg says now.One of Rosenberg’s first surgery cases became part of an experiment. At the time, Rosenberg recalls, “there was someone elseImmune Therapy Steps Up the AttackAfter years of trying, cancer researchers say they are fi nally having success enlisting the body’s own defenses to destroy tumorsPublished by AAASo n O c t o b e r 21, 2010w w w .s c i e n c e m a g .o r g D o w n l o a d e d f r o m SCIENCE VOL 330 22 OCTOBER 2010441NEWS FOCUSin the hospital who had gastric cancer” and whose blood type matched DeAngelo’s. Following the wild theory that something in DeAngelo’s blood could help this desper-ately ill man, Rosenberg transfused blood from DeAngelo into the second patient. Nothing happened, and that man later died of his cancer.But Rosenberg couldn’t shake the memory of that gallbladder surgery, where he ran hishands across DeAngelo’s liver and found no hint of disease. Had DeAngelo’s body fought off cancer on its own?In some ways, the notion didn’t make sense. Cancer cells are a patient’sown, so why would the bodyperceive them as invaders? The answers are now clear. Among them: Tumor cells are geneti-cally unstable and pile on new mutations that render them dis-tinct from the host. In 2007, oncologist Bert Vogelstein of Johns Hopkins University in Baltimore, Maryland, and his colleagues reported in Science that breast and colon cancers can harbor hundreds of gene muta-tions—an “unexpectedly high number,” says Suzanne Topalian, a Johns Hopkins melanoma specialist who was not involved in the work. And those mutations “should be recognized by the immune system,” she says. Studies have confi rmed it: Tumor cells often display antigens not found elsewhere in the body that prompt immune reactions. Immunotherapists targeted melanoma because primary melanoma tumors—as opposed to metastatic ones—are among thefew that can spontaneously disappear. Doc-tors also identified antibodies to melanoma in the blood of patients and a higher inci-dence of the cancer in those who’d received organ transplants and had suppressed immu-nity. All of these clues suggested that theimmune system engaged in an elaborate dance with the disease.Given that roughly 8 million people around the world will die of cancer this year, it’s clear that the immune system alone is nomatch for cancer’s wiles. Robert Schreiber of Washington University School of Medicinein St. Louis, Missouri, advanced a framework in 2001 that’s often cited to explain why. Schreiberargued that the immune systemdoes go after the tumor initially: He called it the elimination phase. This may destroy many cancersbefore they’re detected. But he argued that other tumors develop an immunosuppressive barrier, expressing proteins on their surface that dampen immune attacks. In this equilib-rium phase, the tumor and the person with cancer coexist. At some point, the cancer slips into the escape phase, where the bal-ance tips in its favor. In the past 2 decades, dozens of thera-pies have tried to stimulate the immune system against cancer, including about 20 vaccines that reached mid- and late-stage clinical trials. “We’ve been excited by every single one of these,” says M ario Sznol, an oncologist at the Y ale School of Medi-cine who focuses on melanoma and kidney cancer. But, he concedes, “for the most part, none of those things really did much.”Because tumors evolve to prevent the body from recognizing them as foreign, vaccines need to trigger a massive immune response. Most cancer vaccines just haven’t been potent enough, says Jeffrey Weber, a melanoma specialist at the H. Lee Moffi tt Cancer Cen-ter and Research Institute in Tampa, Florida: “We’ve been giving very wimpy immuniza-tions, in my view.” They may have been inef-fective for another reason: Researchers had only a rudimentary understanding of how the immune system and tumors interact. Slowly, that is changing.Antibody breakthroughs“The science is now guiding the medicine,” says Jedd Wolchok, a melanoma specialist at Memorial Sloan-Kettering Cancer Center in New Y ork City. “The paths that we are taking are built upon a much more solid understand-ing of what is going on molecularly.”Empowering T cells is a key part of the new strategy. One breakthrough came in 1996, when Wolchok’s colleague James Allison reported in Science that a pro-tein called CTLA-4 makes T cells less active (22 March 1996, p. 1734). In mice, Allison found that blocking CTLA-4 with an antibody killed tumors. A biotechnology company called Medarex picked up anti-CTLA-4, which now goes by the generic name ipilimumab, in hopes of turning it into a cancer therapy. Wolchok, Rosenberg, and others began testing it in people.In a small number of patients, the results were dramatic. “I do remember those early days; we were looking at CT scans and say-ing, ‘Oh my goodness, this thing’s really working,’ ” says Topalian. In the summer of 2009, the pharmaceutical giant Bristol-Myers Squibb purchased Medarex for $2.4 billion, gaining rights to both antibodies.In August 2010, the company and its aca-demic collaborators reported on the phase III results of an ipilimumab trial with 676 mela-noma patients. For the fi rst time ever, a ran-domized trial found that people with stage 4 melanoma benefi ted from a new treatment. The advantage was modest: Treated patients survived 10 months, on average, compared with 6.4 months for controls. “What is exciting is when you look at the tail of the curve,” says Allison. “Very few patients sur-vive more than 2 years with metastatic mela-C R ED I T : R Y A N S N O O K , W W W .R Y A N S N O O K .C OMReinforcements! After the immune system tries and fails to fi ght tumors (fi rst two panels), new ther-apies help these T cell knights get the job done.Online Podcast interviewwith authorJennifer Couzin-Frankel.Published by AAASo n O c t o b e r 21, 2010w w w .s c i e n c e m a g .o r g D o w n l o a d e d f r o m22 OCTOBER 2010 VOL 330 SCIENCE 442NEWS FOCUSC R ED I T S : R H O D A B AE R /N A T I O N A L C A N C E R I N S T I T U T E ; R Y A N S N O O K , W W W .R R Y A N S N O O K .C O M (I N S E T S )noma,” and in this trial, just under a quarter of those treated did. Many still have tumors, however, but their disease is stable and they don’t need treatment, says Allison. Only three out of the 540 who received the therapy were free of cancer altogether.Just as chemotherapy comes with risks, so does ipilimumab. Side effects included severe diarrhea, colitis, and endocrine disrup-tion; 14 patients died from the treatment. Still, researchers believe that ipilimumab will gain approval from the U.S. Food and Drug Admin-istration (FDA) in the coming months.Medarex had also been working on another naturally occurring protein called PD-1 that dampens immune responses. Whereas mice without CTLA-4 die of immune defects, those without PD-1 are healthier, suggest-ing that an antibody against PD-1 could have fewer side effects.The response rate for anti-P D-1 looks hopeful. Results from a small trial published in July in the Journal of Clinical Oncology and additional data presented at a cancer meeting in June suggest that about one-third of mela-noma and kidney cancer patients responded—that is, their tumors shrank. “The most amaz-ing thing of all,” says Drew Pardoll of Johns Hopkins, who has been involved in the devel-opment of anti-PD-1, is that up to 3 years after treatment, “not a single responder has yet relapsed. … That’s eye-popping.” Many of them still harbor tumors, but “they’re just sit-ting there” and not growing, says Pardoll. Both antibodies are being tested in other cancers. Responses to ipilimumab have shown up in ovarian, prostate, and lung cancer, in addition to melanoma, says Allison. In theory, if a patient’s T cells are reacting to tumor antigens, this approach “can be used for any kind of cancer.”Narrow successAntibodies like ipilimumab are valuable, Rosenberg says, but in his mind, they’re not nearly enough. If the cancer doesn’t com-pletely disappear, “everybody dies” eventu-ally, he says. Rosenberg wants a cure, and he is willing to go to great lengths to get it.He’s testing a different approach at theNational Institutes of Health (NIH) Clini-cal Center here, which draws people from all over who are running out of options and treats them free of charge. Rosenberg esti-mates his budget for immunotherapy at about $3 million a year, far higher than virtually anywhere else.On this day he drops in on a cheerful woman in her mid-40s with reddish-brown hair and chunky black glasses. She will be the first per-son to receive Rosenberg’s immunotherapy for col-orectal cancer. If it fails, he guesses she has between 4 and 6 months to live.Unlike antibody therapy, which isadministered intravenously in an outpatient setting, Rosenberg’s method requires hospi-talization and a research clinic, at least for now. He focuses on fi nding T cells activated to attack cancer, usually in tumor tissue. Hisgoal is to extract these T cells, grow them into the tens of billions outside the body over several weeks, and give them back. To make this work, Rosenberg discovered several years ago that he first needs to destroy a patient’s existing immune cells with high doses of chemotherapy and some-times total-body irradiation.Rosenberg’s approach is not an option for many patients. T cells can’t be harvested from those with inaccessible tumors, about one-fi fth of melanoma patients. For another fi fth, the cells don’t grow well outside the body. Many can’t wait the month it takes to expand cells in the lab. And the pretreatment chemotherapy, as well as a drug given during treatment, is so toxic that most people over 70 can’t tolerate it.But for those lucky enough to have that precious bag of T cells returned to them, the likelihood of success is impressive. Out of 93 patients with metastatic melanoma who have received the treatment and been followed long-term, 20 saw their cancer disappear completely. Nineteen have remained cancer-free for 3 to 8 years. In another 32, tumors shrank. Nearly all of these patients had failed every available therapy, including, in many cases, ipilimumab.In his office, Rosenberg clicks through a series of CT scans on his computer screen from one of his success stories, a police offi cer coming in for a follow-up visit. Like most of Rosenberg’s patients, the policeman had met-astatic melanoma. Although suffering long-term effects from radiation he received when Rosenberg treated him, he’s been free of can-cer since T -cell therapy 4 years ago.Rosenberg is now trying to get around one big limitation of his strategy: the need for tumor tissue as a source of T cells. He’s experimenting with removing T cells directly from the blood of patients and geneticallyengineering them to recognize antigenson tumors. This would potentially open up the therapy to people with all sorts of cancers, espe-cially those with hard-to-reach tumors that can’t be surgically removed for the T-cell hunt. Rosenberg is also beginning to extend his therapy to lymphoma and sar-coma as well as colon cancer. So far, the few patients treated are doing well.Several large academic medical centers in Seattle, Houston, and elsewhere have also been working on refi ning the therapy, called adoptive T cell transfer (ACT). All report roughly comparable success rates, but none isSummit. Steven Rosenberg says his 30-year push for an immune-based assault on melanoma is working at last.Published by AAASo n O c t o b e r 21, 2010w w w .s c i e n c e m a g .o r g D o w n l o a d e d f r o mdoing as much as Rosenberg at NCI—largely, they say, because of the cost.Although the results are compelling, ACT “is 100 times as hard to export, to do in a repro-ducible fashion, and it’s also a lot more expen-sive than” antibodies, says Pardoll. “Com-panies essentially have no interest in it. It really right now is a purely academic exercise.”ACT has taught us a great deal, says Wolchok at Sloan-Kettering—for example, that people with heavy can-cer burdens can be helped just by expanding and reintro-ducing their T cells. But ACT faces daunting hurdles in “being able to produce the cell product forevery patient who needs it,” he says. Even in Rosenberg’s lab, the cells don’t always grow, says Wolchok, who has referred patients to the program. Sznol at Y ale has looked into setting up an ACT program there, but the logistics have made it too diffi cult to pull off yet. Although Rosenberg agrees that compa-nies haven’t invested in ACT, he is frustrated by those who critique its practicality. He has a lab member working full-time with NIH’s blood bank to determine whether it can grow patients’ cells more effi ciently. NCI recently began a randomized clinical trial of ACT in melanoma. The hope is that if ACT proves superior, payers might cover its cost, which depends on the protocol but can exceed $100,000 per patient.Even doubters recognize that what’s dis-missed as impossible in medicine is always changing. “Monoclonal antibodies had the same stones thrown at them 20 years ago,” with everyone questioning their feasibility, says Wolchok. With ACT, “it may just be time for the technology to catch up with the need.”After much hesitation, pharmaceuti-cal companies have expressed growing enthusiasm for cancer immunotherapy. In April, FDA approved the first cancer vac-cine, called Provenge, for metastatic prostate cancer, made by the company Dendreon inSeattle. Treatment consists of three infu-sions for a total cost of $93,000. Many oncologists are underwhelmed by its effec-tiveness. The vaccine extends survival by 4 months; it does not stop cancer. But just thefact that Dendreon pushed ahead withthe vaccine, which is custom-made for every patient, is heartening to some immunotherapists.Bristol-Myers Squibb has its antibodies—ipili-mumab and anti-PD-1—while another pharma giant, GlaxoSmithKline (GSK), is running several large trials of a new cancer vaccine for lung cancer and melanoma. Unlike Provenge, the GSK vaccine is an off-the-shelf mix. It includes an antigen, MAGE-A3, that commonly appears on cancer cells, and an adjuvant to boost immune reactions; introduced together, these aim to stimulate the immune system to go after cells express-ing MAGE-A3. GSK is trying to use gene profi ling of tumors to carefully pick patients most likely to respond. “We do not want tohave the clinical effi cacy diluted because we don’t select the right patients,” says Vincent Brichard, head of immunotherapeutics at GSK Biologics in Rixensart, Belgium. “This could explain why previous trials have failed.” Skill and subtletyAs immunotherapy edges into the clinic, it’s likely to challenge oncologists’ expertise. When chemotherapy works, it works quickly; immunotherapy is very different. “Y ou might not see responses right away, and they may getworse before they get better,” says Cassian Y ee of the Fred Hutchinson Cancer Research Cen-ter. “It does take a little bit of insight for the person managing the patient to say, ‘OK, your tumor’s only grown by 10%, 20%—we think that you should continue” on ipilimumab. No one yet knows why tumors might grow before they dissipate. Indeed, there’s still much that remains a mystery about how antibodies and ACT behave in the body, how to predict who they’ll help, and how to make them more effective.A subset of patients might have what Thomas Gajewski of the University of Chi-cago in Illinois calls the “infl amed phenotype”: They are capable of “making some smolder-ing immune response against their tumor that you can tip over” in their favor, shrinking the cancer or erasing it altogether. Gajewski esti-mates that at least 30% of patients fall into this category. He’s looking for ways to coax the other 70% to respond: “How do you make the noninfl amed tumors infl amed?” he wonders. Most cancer specialists believe the solution will come from combination therapies. Like Gajewski, Allison theorizes that immuno-therapy is most effective when an immune response is already under way, with T cells activated and tumor cells dying. One way to tip more patients into this category might be by supplementing immunotherapy with direct killing of tumor cells. Bristol-Myers Squibb is running a large prostate cancer trial that com-bines ipilimumab with a single dose of radi-ation to do just that. In theory, the antibody might also enhance the potency of T cells given in ACT, says Y ee.Which treatments will go mainstream? “Everybody’s goals are the same: Let’s try to cure cancer patients,” says Rosenberg. But is it reasonable to set up expensive cell growth facilities, as some want NCI to do, espe-cially if they’ll help only a subset of patients? And who will pay? With immunotherapy, no matter which approach you take, says Y ee, “you’re going to start off with high expenses.” The hope is that long term, the payoff will be worth it. –JENNIFER COUZIN-FRANKEL SCIENCE VOL 330 22 OCTOBER 2010443NEWS FOCUSC R ED I T S : (S O U R CE ) B R I S T O L -M Y E R S S Q U I B B , G L A X O S M I T H K L I N E , A N D S T E V E N R O S E N B E R G ; R Y A N S N O O K , W W W .R Y A N S N O O K .C O M (I N S E T)“The science is now guiding the medicine.”—JEDD WOLCHOK,MEMORIAL SLOAN-KETTERINGCANCER CENTERPublished by AAASo n O c t o b e r 21, 2010w w w .s c i e n c e m a g .o r g D o w n l o a d e d f r o m。
13 Journal of China Prescription Drug Vol.16 No.7·综述·肿瘤浸润性淋巴细胞(TILs)是一类肿瘤浸润性且具有抗原效应的细胞群,由Rosenberg 等于1986 年从荷瘤小鼠肿瘤组织中发现并分离[1]。
TILs包括存在于肿瘤癌巢内的瘤内肿瘤浸润淋巴细胞(iTIL)及间质中的基质肿瘤浸润淋巴细胞(sTIL)[2-3],以淋巴细胞为主的异质性淋巴细胞群体,被认为是免疫生物学标记物。
切除患者肿瘤分选TILs,通过一些培养方法比如体外IL-2、IL-15 、IL-7与抗CD3 抗体刺激扩增培养[4-6],回输患者体内,并在高剂量IL- 2等的管理下进一步刺激在体内增殖[7],然而回输的TIL细胞其实是很多细胞的混合体,并没有经过特异筛选。
有些TIL细胞是对肿瘤特异的,有些并不是特异的,所以通过基因测序寻找肿瘤细胞特异的突变基因,然后筛选针对这个突变的特异TIL细胞回输,效果可能会更好,基于这些想法,TILs细胞疗法逐步发展。
1 TILs作用机制TILs包括T细胞、B细胞和NK细胞。
大多数TILs都有CD3+表型[8],CD3+TILs可进一步细分为细胞毒性T细胞(cytotoxic T cell,CD8+ T)、记忆T细胞(memory T cell,CD45RO +)、辅助T细胞(regulatory T cell,CD4+)[9-10]。
TIL的表型具有异质性,不同肿瘤来源的TILs中,CD4+T细胞、CD8+ T细胞比例也不同[11]。
CD8+T细胞在肿瘤微环境肿瘤发展过程中被认为具有抗肿瘤功能,故CD8+T细胞的数量决定其杀伤靶细胞的效率。
在肿瘤患者中已发现自发的CD4 + T细胞对肿瘤抗原的反应,肿瘤浸润CD4 + Th1细胞密度高的患者几乎所有肿瘤类型预后良好[12],证据表明 CD4 + T细胞在抗肿瘤免疫中起着重要作用。

·专家论坛·肿瘤浸润性淋巴细胞免疫治疗的研究进展杨涵 陈超 王冲(上海药品审评核查中心 上海 201210)摘要肿瘤浸润性淋巴细胞(tumor-infiltrating lymphocytes, TILs)免疫治疗通过体外分离、扩增和回输患者自己的能特异性识别肿瘤组织的肿瘤浸润性T淋巴细胞来治疗肿瘤,是目前主要的过继性细胞免疫治疗类型之一。
TILs已在用于实体瘤治疗的临床试验,尤其是在用于转移性黑色素瘤患者治疗时显现有令人鼓舞的临床效果。
然而,TILs治疗也面临一些挑战,如肿瘤相关抗原反应性T细胞难以分离及其在体内的持久性和安全性等。
本文概要介绍TILs治疗的产品生产过程、临床应用的可行性、临床研究进展,以及TILs治疗面临的挑战和解决措施,供TILs治疗的研究与开发者参考。
关键词肿瘤浸润性淋巴细胞 实体瘤 临床研究中图分类号:R979.19 文献标志码:A 文章编号:1006-1533(2022)11-0017-05引用本文杨涵, 陈超, 王冲. 肿瘤浸润性淋巴细胞免疫治疗的研究进展[J]. 上海医药, 2022, 43(11): 17-21.Research progress in tumor-infiltrating lymphocytes immunotherapyYANG Han, CHEN Chao, WANG Chong(Shanghai Center for Drug Evaluation and Inspection, Shanghai 201210, China)ABSTRACT Tumor-infiltrating lymphocytes (TILs) therapy is one of the main types of adoptive cellular immunotherapyby harvesting infiltrated lymphocytes from tumors followed by ex vivo expansion and then infusing them back to patients themselves. TILs therapy has shown encouraging clinical effects in clinical trials against solid tumors, especially in treating metastatic melanoma. Nevertheless, various barriers restrict the efficacy and prevent the widespread use of TILs therapy, suchas the difficulty of isolating tumor-associated antigen-reactive T cells and their persistence and clinical safety in vivo. Herein, we summarize the manufacturing process of TILs and the feasibility analysis of the clinical application and discuss the advancesin clinical trials and the current obstacles with some strategies to be overcome, shedding light of the development of the next generation of TILs therapy.KEY WORDS tumor-infiltrating lymphocytes; solid tumors; clinical trials细胞免疫治疗,又称过继性细胞免疫治疗,是一种基于细胞的治疗方法,其使用患者自身或供体的经过基因工程改造和/或离体扩增的免疫细胞来改善患者的免疫功能,以对抗肿瘤。

“微移植”治疗急性髓系白血病的研究进展王璇;郭树霞【摘要】近年来,急性髓系白血病(AML)的治疗方案已经发展到了个体化阶段.“微移植”(microtransplantation)是指在治疗AML时,将化学疗法、异基因造血干细胞移植、细胞免疫治疗相结合的一种新的治疗模式.被称为治疗AML的“新利器”.【期刊名称】《中国民康医学》【年(卷),期】2018(030)018【总页数】3页(P65-67)【关键词】急性髓系白血病;微移植【作者】王璇;郭树霞【作者单位】郑州人民医院,河南郑州450000;郑州人民医院,河南郑州450000【正文语种】中文【中图分类】R733.71化疗期间间歇性输注HLA配型不相合或不全相合的G-CSF动员后外周造血细胞(G-PBSC),简称“微移植”,被认为是“分离移植物抗肿瘤效应(GVL)和移植物抗宿主病(GVHD)”治疗急性髓系白血病(AML)的新模式。
该方案借鉴“非清髓移植”方案,无GVHD预防用药,技术门槛比传统移植低,易于操作,不良反应小,治疗费用低,便于基层医院推广应用。
现就其研究成果综述如下。
1 AML治疗现状AML主要的治疗手段是化疗、移植、细胞免疫。
随着细胞遗传学、免疫分型、分子遗传学等的发展,近20年AML最大的治疗进展是根据AML的危险程度选择不同的治疗方案,即预后分层性治疗。
1.1 化疗按目前AML治疗水平,有10%~20%的患者对“蒽环类+阿糖胞苷”的一线标准诱导方案无效,50%~80%已经获得CR(完全缓解)的患者在1年内复发。
除“急性早幼粒细胞白血病”外,化疗普遍存在治疗时间长,脏器毒性、复杂感染的发生率上升,高危患者生存率低,复发风险高,老年患者疗效差等问题[1]。
1.2 移植造血干细胞移植(HSCT)仍是公认的治疗AML最为有效的方法。
HSCT使AML患者长期无病生存率达到了50%[2]。
但自体造血干细胞移植(auto-HSCT)复发率高,异基因造血细胞移植(allo-HSCT)缺乏理想的供者, GVHD及严重感染等均威胁着患者的生存质量甚至生命安全[3]。
靶向调节性T细胞治疗的研究进展李兰芳;任秀宝;王华庆;刘贤明【期刊名称】《临床荟萃》【年(卷),期】2013(028)011【总页数】3页(P1299-1301)【关键词】肿瘤;T淋巴细胞,调节性;免疫毒素类;免疫疗法【作者】李兰芳;任秀宝;王华庆;刘贤明【作者单位】天津医科大学肿瘤医院,国家肿瘤临床医学研究中心,天津市"肿瘤防治"重点实验室,天津市肿瘤免疫与生物治疗重点实验室,淋巴瘤内科,天津,300060;天津医科大学肿瘤医院,国家肿瘤临床医学研究中心,天津市"肿瘤防治"重点实验室,天津市肿瘤免疫与生物治疗重点实验室,淋巴瘤内科,天津,300060;天津医科大学肿瘤医院,国家肿瘤临床医学研究中心,天津市"肿瘤防治"重点实验室,天津市肿瘤免疫与生物治疗重点实验室,淋巴瘤内科,天津,300060;天津医科大学肿瘤医院,国家肿瘤临床医学研究中心,天津市"肿瘤防治"重点实验室,天津市肿瘤免疫与生物治疗重点实验室,淋巴瘤内科,天津,300060【正文语种】中文【中图分类】R979.1调节性T细胞(Tregs)是一群具有免疫抑制功能的细胞,1995年日本学者Sakaguchi等首次分离出了CD4+CD25+调节性细胞亚群,并证实其具有抑制其他T细胞活化的功能,其主要的特性为免疫无能性及免疫抑制性。
Tregs能够显著地抑制宿主的免疫反应和诱导自身免疫耐受。
由于Tregs的免疫抑制作用,有关Tregs与肿瘤关系的研究不断有报道。
在多种恶性肿瘤中,发现Tregs水平增高且提示临床预后不佳。
因此,Tregs在恶性肿瘤中的作用引起了国内外专家的兴趣,不断有针对Tregs靶向治疗的研究报道,试图找到一种治疗肿瘤的新靶点及新途径。
现将目前的研究结果综述如下。
1.1低剂量环磷酰胺环磷酰胺为DNA的烷化剂,自二十世纪五十年代以来,广泛用于多种肿瘤的化疗。
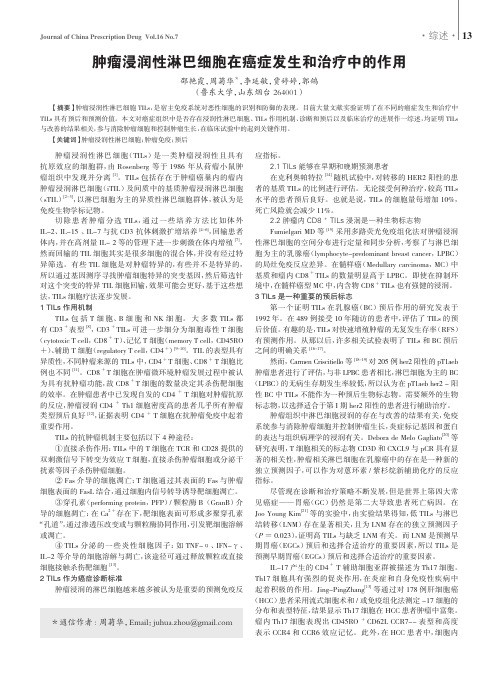
Activated Monocytes Prime Naı¨ve T Cells Against Autologous Cancer:Vigorous Cancer Destruction In Vitro and In Vivoumbacher,S.Gu &R.WankIntroductionNumerous therapeutic modalities have been developed to hinder the growth or induce the destruction of malignant tumour cells.The multitude of modalities reflects the inexhaustible number of strategies that cancer cells use to evade control by immune cells.However,as of yet unrec-ognized immune responses must prevent the rise of carci-noma cells in women carrying resistance-associated immune response genes of the HLA system [1–5].Immune surveillance of cancer growth by T lymphocytes necessarily includes the recognition of tumour-immuno-genic peptides.To present such peptides to T cells,den-dritic cells have been incubated with tumour cell lysates,pulsed with defined tumour peptides or transfected with RNA or DNA from tumour cells [6,7].Gene mutations and their corresponding mutated cellular proteins can serve as tumour markers.For exam-ple,mutations of the p53gene have been identified in free circulating DNA in precancer and cancer patients [8,9].Cytotoxic T cell responses to different and differently mutated tumour targets have been reported [10–16].We have been interested in identifying conditions that would stimulate antigen-presenting cells (APC)to process,express and transfer tumour-immunogenic information to naı¨ve T cells,leading to their maturation to T effector cells,to prevent their inactivation,as has been observed in tumour-infiltrating lymphocytes [17,18].Antigen-presenting cells were stimulated by activating T cells in PBMC cultures with the monoclonal antibody OKT3.Because ligation of CD3chains by OKT3anti-bodies downmodulates the CD3⁄ab TCR complex viaImmunotherapy Research Center,Immunis e.V.,Mu ¨nchen,GermanyReceived 15June 2011;Accepted in revised form 28September 2011Correspondence to :R.Wank,Immunotherapy Research Center,Immunis e.V.,Pettenkoferstr.8,80336Mu ¨nchen,Germany.E-mail:professor-wank@muenchen-mail.deAbstractIt has not been considered so far that antigen-presenting cells (APC)mayphagocytose immunogenic material from autologous cancer cells.Assuming the presence of cancer-immunogenic material in APC,we developed a novel autologous priming method that does not require tumour cells or identified peptides.Cancer-immunogenic information came from CD14+monocytes.When stimulated with CD3-activated T cells,monocytes primed CD3+CD4+and CD3+CD8+resting ⁄naı¨ve T cells to become powerful effector cells within 24h.During priming,depletion of CD14+monocytes but not CD1a +CD83+dendritic cells prevented T cell priming.During cancer cell destruction,den-dritic cells,but not monocytes,enhanced cancer cell lysis.The cascade-primed (CAPRI)immune cell quartet comprising monocytes,dendritic cells,CD4+T and CD8+T cells induced a significant decrease in the number of suppressive CD25high FoxP3+CD4+T cells.CAPRI cells induced a marked upregulation of MHC class I and class II expression in cancer cells,which is crucial for auto-immune-like lysis.We show in vivo evidence of the CAPRI cell concept in nude mice.In humans,we present circumstantial clinical evidence showing the efficacy of CAPRI cells in an adjuvant treatment attempt for breast cancer patients with metastasis (N =42).Compared to patients at the Munich Tumor Center (no CAPRI treatment N =428),almost double the expected number of patients survived 5years (P =1.36·10)14).The CAPRI method is a safe procedure without negative side effects.High numbers of cancer-specific CAPRI cells can be obtained within a week against different cancer types for efficient adoptive cell therapy.C L I N I C A L I M M U N O L O G Y doi:10.1111/j.1365-3083.2011.02652.x ..................................................................................................................................................................Ó2011The Authors.314Scandinavian Journal of Immunology Ó2011Blackwell PublishingLtd.internalization or by preventing their recycling[19,20], we added unstimulated autologous PBMC as a source of naı¨ve T cells expressing the ab TCR.Here,we show that MHC-restricted efficient cancer cell lysis by cascade-primed(CAPRI)cells results from the cooperation of a cellular quartet consisting of T helper cells,T cytotoxic cells,dendritic cells and mono-cytes that upregulate and induce MHC class I and class II expression in cancer cells.Finally,we provide preclinical and circumstantial clin-ical evidence for the CAPRI concept by showing efficient and significant lysis of cancer cells in nude mice and in patients with different cancers in an adjuvant treatment attempt.Materials and methodsTumour samples and establishment of autologous tumour cell lines.Immune cells and autologous tumour samples were donated by informed and consenting patients referred by doctors for the support of radiation or chemotherapy with adjuvant adoptive immunotherapy(ACT).The tumour samples were used to establish cancer cell lines to provide a control for analysing the lytic capacity of activated immune cells.The ethics recommendations of Helsinki with subsequent amendments of Tokyo1975,Hong Kong 1989and Somerset West1996were followed.Tumour samples were minced to small pieces and cul-tured in50-mlflasks using supplemented tumour culture medium(RPMI1640with L-glutamine,supplemented with10%FCS,NEAA,G5Supplement;all from PAA, Coelbe,Germany)and optimized culture conditions. Unused tumour samples were also minced to small pieces and cryopreserved in DMSO,like PBMC[21].The estab-lishment of cell lines that divided at least20times was successful only with samples from patients who had not yet received chemotherapy or radiation therapy.All cell lines originated from Caucasian patients.Isolation of immune cells.PBMC were isolated from venous blood puncture or leukapheresis samples by den-sity gradient centrifugation as described previously[21] using lymphocyte separation medium(LSM;PAA). Immune cells were either used immediately or cryopre-served and stored in the nitrogen gas phase.Isolation, cryopreservation and thawing procedures as well as the use of optimized culture conditions(38.5°C,6.5%CO2) have been described in detail[21].Activation of T cells in PBMC bulk cultures:CD3activa-tion and CAPRI cell generation.Both methods started with the activation of T cells in PBMC bulk cultures using the CD3monoclonal antibody OKT3(Orthoclone; Cilag,Sulzbach⁄Taunus,Germany),which binds to the non-polymorphic e-chain of the CD3molecule,and the addition of interleukin2(IL-2;Proleukin;Chiron,Ratin-gen,Germany).CD3antibodies were immobilized at a concentration of1l g⁄ml in0.05M borate buffer pH8.6and distrib-uted in50-ml tissue cultureflasks(Greiner Bio-One, Frickenhausen,Germany).Coatedflasks were kept at 4°C at least overnight and washed twice with phos-phate-buffered saline prior to incubation with PBMC. PBMC were added at a concentration of2·106cells⁄ml in a total volume of10ml,and IL-2was added within 2–12h at a concentration of20U⁄ml.CD3-activated cells were expanded on day4with IL-2(20U⁄ml)and harvested on day7for immediate use or cryopreservation.For the generation of CAPRI cells,CD3-activated PBMC were removed from theflask after4–6h,washed and then cocultured in a second CD3‘antibody-free’flask with an equal number of unstimulated autologous PBMC,which contained naı¨ve⁄resting T cells,at a con-centration of2·106⁄ml in a total volume of10ml. Cells were expanded on day1with IL-2(20U⁄ml)and harvested on day4.Microscopic classification,preparation of tumour target cells and quantification of cancer cell destruction using the Cr51-release assay.Cancer cells were removed fromflasks by trypsinization,resuspended in culture medium(RPMI 1640with L-glutamine;PAA)supplemented with10% FCS and washed twice.Cancer cells were counted and distributed in different concentrations into96-wellflat-bottom culture plates(Falcon;Becton Dickinson,Heidel-berg,Germany)either for microscopic evaluation of lysis or for the Cr51-release assay.Before the addition of effec-tor cells,cancer cells were allowed to recover overnight to restore their membrane integrity after trypsinization. Reorganization of cancer cells into a coherent cell layer better reflected the situation in vivo and significantly lowered the rate of spontaneous Cr51release,an as yet unresolved problem of the Cr51-release assay for measur-ing tumour cell destruction.The Cr51-release assay was performed in duplicate at varying effector to target ratios using2·103target can-cer cells.Maximum Cr51release was determined using labelled target cells,and spontaneous release was dis-cerned by incubating target cells in medium alone.The per cent of spontaneous release was calculated as follows: (spontaneous cpm:maximum cpm)·100;the per cent of cytotoxicity was calculated as follows:[(experimental cpm)spontaneous cpm):(maximum cpm)spontaneous cpm)]·100.Quantitative lysis of cancer cells using the Cr51-release test was assessed after5–6h and after 18–22h by following the‘classical’guidelines for the cell-mediated lympholysis(CML)assay[22]with the crucial difference in tumour target preparation described earlier.Representation of data followed classical CML papers[23–27].The degree of lysis was estimated by microscopic inspection after18–24h.The scale used corresponded to conventional HLA microscopic estimated evaluation.ThisÓ2011The Authors.Scandinavian Journal of ImmunologyÓ2011Blackwell Publishing Ltd.scale designates a lysis of more than80%as strong posi-tive(++),60–79%as positive,40–59%as weak positive, 20–39%(+)as doubtful positive and<20%())as nega-tive(Fig.2).Microscope used:Fluovert FS,ocular:Periplan GF 12.5·⁄20,objective:170⁄-10⁄0.25PHACO1(Leitz, Wetzlar,Germany).Photosystem MPS48(Leitz).Films used:Kodak Ektachrome64T professional.Imaging medium:RPMI1640with L-glutamine (PAA)supplemented with10%FCS;pictures were taken at room temperature.Figures were prepared with MicrosoftÒPowerpointÒ2000(9.0.2716)and corel PHOTO-PAINT,version 12.0.0.536(Corel Deutschland,Unterschleißheim, Germany).To determine the influence of HLA class I and class II molecules on cancer lysis,monoclonal antibodies were added at the start of the CAPRI cell⁄cancer cell cocul-tures.The antibody W6⁄32(1l g⁄ml)(Abcam,Cam-bridge,UK)was used to block HLA class I,and L243 (1l g⁄ml)(Abcam)was used to block HLA class II.Depletion of CD3,CD4,CD8and CD14positive subpop-ulations from PBMC with magnetic beads.Mouse anti-human CD3,CD4,CD8and CD14conjugated to mag-netic beads;CD14negative isolation kits and Pan Mouse IgG beads were obtained from Dynal(Invitrogen,Paisley, UK)and used according to manufacturer’s instructions.The manufacturer’s depletion protocol was repeated three times for a depletion efficiency>98%.CD4+T cells were isolated from CD3-isolated popula-tions to spare CD14+CD4+monocytes.Tracing of monocytes during CD3and CAPRI stimula-tion.About40·106PBMC were obtained from each donor;20·106PBMC were treated with DynabeadsÒUntouchedÔhuman monocytes kit(Invitrogen)to obtain CD14+monocytes,according to manufacturer’s instructions.Purified CD14+monocytes were labelled with CFSE (eBioscience,San Diego,CA,USA)according to manufac-turer’s instructions.About20·106PBMC were depleted of CD14+monocytes by DynabeadsÒCD14(Invitrogen) according to manufacturer’s instructions.CFSE-labelled CD14+monocytes were added to the CD14-depleted PBMC to reconstitute a PBMC population with CFSE-labelled CD14+monocytes.The reconstituted PBMC were stained with anti-CD14PE,HLA-DR-PE,CD1a-PECy5.5,with anti-CD40-PECy5.5,CD80-PECy5.5,CD-83-PECy5,CD86-PECy5.5and with anti-HLA-A,B, C-PECy5.5(eBioscience)for tracing the phenotype of CFSE-labelled CD14+cells during CD3stimulation or during the CAPRI procedure.Flow cytometry.Expression of cell surface markers was determined byflow cytometry using the Becton-Dickinson FACScan analyzer and C ELL Q UEST software(Becton-Dickinson).CD14+cells were CFSE-labelled to trace the changes in phenotype.In brief,cells were harvested and stained with anti-CD14PE,HLA-DR-PE,CD1a-PECy5.5,with anti-CD40-PECy5.5,CD80-PECy5.5,CD 83-PECy5,CD86-PECy5.5and with anti-HLA-A,B,C-PECy5.5to trace the phenotype of CFSE-labelled CD14 cells during CD3or CAPRI stimulation.For the analyses of cell surface markers on CD3-stimulated and CAPRI cells,cells were collected and stained with anti-CD3-FITC, CD14-PE,CD19-PECy5.5,with anti-CD3-FITC,CD4-PE,CD8-PECy5.5,with anti-CD3-FITC,CD14-PE, CD56-PECy5.5and with anti-CD3-FITC,CD16-PE, CD56-PECy5.5.For Foxp3staining,cells were stainedfirst with anti-CD4-PE,fixed,permeabilized with human Foxp3staining buffer set and then stained with FITC-anti-human Foxp3.The conjugated mouse monoclonal antibodies were obtained from BD Biosciences or eBioscience.The human Foxp3staining buffer set was obtained from eBioscience.Presence of CD4+T lymphocytes could not be replaced in the priming phase or in the cytotoxicity assay by supernatants from CAPRI cell cultures.CAPRI culture supernatants were added to CAPRI cell cultures to clarify whether CD4+T lymphocytes provided only‘cytokine help’to cytotoxic CD8+T cells or participated as effector cells in cancer cell destruction.To avoid the depletion of CD14+CD4+ monocytes,CD3+cells werefirst isolated from PBMC cultures(1),and then CD4+cells were depleted.The CD4+-depleted CD3isolate was added to(1).Supernatants were added before CD3activation or to unstimulated PBMC,which were added in the second step to supply T cells expressing the ab TCR.Cytotoxicity testing of human CAPRI cells against autolo-gous breast cancer cells in nude mice.Animal experiments were authorized by the ethic committee of the University of Wuhan,China,and designed by S.Gu and performed at the Wuhan University under the supervision of S.Gu.Twelve6-week-old nude female mice(BALB⁄c-nu) were obtained from Wuhan University,Center for Animal Experiments,China.Cells from the breast cancer cell line ZB(raised10years ago from one of the patients in the Institute of Immunology of the University of Munich and in culture since then)were washed in PBS and resus-pended in PBS at a concentration of1·106⁄ml.Mice were injected subcutaneously with1·105breast cancer cells in0.1ml of PBS.Mice of the control group(n=6) were injected with1·106autologous PBMC,and verum group mice(n=6)were injected with1·106autolo-gous CAPRI cells every second day until day15.PBMC and CAPRI cells were introduced surrounding the injected tumour locations.Mice were observed for45days after cancer cell injection.Tumour size was measured for thefirst time after21days.Mice were killed if the maxi-mum tumour diameter was>15mm unless the tumour killed the mouse before that point.After45days,the experiment was completed,and all mice were killed.Scandinavian Journal of Immunology,2012,75,314–328Pictures were taken with a Konica Minolta Dimage Z3camera(Konica Minolta Business Solutions Deutsch-land GmbH,Langenhagen,Deutschland),andfigures were prepared with corel PHOTO-PAINT,version 12.0.0.536.,and Adobe Illustrator CS5,version 3.0.0.400.Patient panel,CAPRI cell dose and treatment schedule.All steps of the production of autologous acti-vated immune cells including thefinal therapy(treat-ment attempts)were controlled by the medical doctor (RW)himself.In Germany,medical doctors are allowed to perform such treatment attempts on their own author-ity.The preparation of CAPRI cells as well as the treat-ment was performed at the Institute of Immunology of the Ludwig-Maximilians-Universitaet(LMU),Mu¨nchen.The patients’survival data from the Munich Tumor Center were collected from several hospitals,from gynae-cologists and from surgeons,independently from the type of treatment,the type of chemotherapy or radiation ther-apy.In essence,the data from the Munich Tumor Center are a summary of individual case reports like those from patients treated with CAPRI cells.Each breast cancer patient(T1-4N0-2,G2-3)with diagnosed metastasis(M1,N=42)who had received at least500·106CAPRI cells(although higher cell amounts were recommended and often received)was included in the analysis and compared to breast cancer patients with the same tumour staging(T1-4N0-2M1, G2-3)of the Munich Tumor Center(N=428).Inclusion for treatment was independent of the type of chemother-apy,radiation and⁄or other therapies.The recommended treatment schedule included three injections of60–80·106CAPRI cells per week for6months,which was followed by two injections per week for another 6months.ACT with CAPRI cells has continued for most of the patients once a week for several years.One-third of CAPRI cells were injected i.v.,and two-thirds were given i.m.into the forearm in a1ml volume of PBS.Statistical analysis.The slope and y intercept of the regression lines obtained from CML titrations were evalu-ated using the general linear model(GLM)procedure. The statistical package SPSS10.1(SPSS Inc.,Chicago,IL, USA)was used.ResultsCancer cell lysis by CAPRI cells within24hWe stimulated APC in PBMC bulk cultures by activat-ing T cells with the OKT3antibody,which binds to a conformational epitope expressed by CD3-ed or CD3-ec chains[29],and added unstimulated PBMC to CD3-acti-vated PBMC as a source of T cells expressing the ab TCR.Microscopic inspection indicated little or no reduction in cancer cell numbers after24h of coculture with CD3-activated PBMC(Fig.1A)compared with carcinoma cultures at time zero(Fig.1A,B),but most cancer cells were lysed after being cocultured with CAPRI cells(Fig.1F).In chromium51-release assays, CD3-activated PBMC showed no significant lytic activity (Fig.1G),while CAPRI cells lysed27.1%of cancer cells at a5:1effector to target(E:T)ratio and89.9%of cancer cells at a E:T ratio of20:1(Fig.1G).CAPRI cells lysed MHC-restricted cancer cellsThe generation of cytotoxic T cells depends on interac-tions between the ab TCR and the pMHC[30].MHC restriction was analysed using allogeneic cancer cells and antibodies blocking the pMHC.CAPRI cells from two unrelated breast cancer patients with defined HLA class II DQ alleles were tested along with breast cancer cells from six unrelated patients(Fig.2A).After24h,CAPRI cells lysed the autologous cancer cells robustly and lysed the cancer cells with shared HLA-DQ1alleles approxi-mately half as well,whereas a lack of HLA-DQ sharing resulted in minimal background lysis(Fig.2A).This suggests that HLA class II surface molecules on APC pre-sented tumour-immunogenic peptides,but complete lysis may depend on the sharing of both HLA class I and class II antigens.This was indirectly supported by the observa-tion that cancer cell lysis was blocked with HLA class I and class II antibodies.Lysis was strongly reduced with the antibody W6⁄32binding to all HLA class I mole-cules and the antibody L243binding to HLA class II molecules(Fig.2B,C).Both antibodies,W6⁄32and L243,block the lysis of cancer cells significantly;(B) W6⁄32:P slope=2.49·10)8,P intercept=6.52·10)9, L243:P slope=2.50·10)9,P intercept=4.70·10)9.(C) W6⁄32:P slope=6.04·10)9,P intercept=4.58·10)9, L243:P slope=9.19·10)10,P intercept=2.16·10)9.Isotypic control antibodies do not block the lysis of cancer cells by CAPRI cells.Figure2B,patient1: P slope=0.504,P intercept=0.572,Fig.2C,patient2: P slope=0.881,P intercept=0.678.The required concurrence of HLA class I and class II presentation indicates a comprehensive interdependence of helper and cytotoxic T cells for the successful lysis of cancer cells.CAPRI cells showed very weak activity against the NK target cell K562,which usually does not express HLA antigens(data not shown),perhaps because K562lysis is usually mediated by activated NKT cells in PBMC cultures[31].CAPRI cells enhanced HLA class I and class II surface expression in epithelial and other solid cancer cellsHow can CAPRI cells lyse cancer cells in an HLA-restricted manner,despite cancer cells tending to downre-gulate HLA expression[32,33]?We compared the HLAÓ2011The Authors.Scandinavian Journal of ImmunologyÓ2011Blackwell Publishing Ltd.expression of CFSE(5(6)-carboxyfluorescein diacetate N-succinimidyl ester)-labelled cancer cells after coculture with autologous unstimulated PBMC,only CD3-acti-vated PBMC or CAPRI cells using a low effector to target ratio of5:1(Fig.3).CAPRI cell-stimulated cancer cells showed a40%increase in meanfluorescence inten-sity(MFI)in HLA class I expression(MFI versus MFI) and a60%increase in HLA-DR class II expression(MFI versus MFI)(Fig.3A).The enhanced MHC class II expression in cancer cells could be pivotal for the destruc-tive power of CAPRI cells,as CD4interactions augment cytotoxic T cell responses[34,35].Maturation of monocytes to dendritic cells during the CAPRI procedureStimulated APC express high levels of MHC class I and class II molecules along with B7and other costimulatory molecules[36].We analysed phenotypic markers of CFSE-labelled CD14+monocytes before activation(day0)and 1day(day1)and5days(day5)after activation(Fig.4). In CAPRI cells,a considerable number of monocytes lost CD14expression and matured,as defined by the acquisi-tion of the dendritic cell markers CD1a and CD83at day1 and their marked upregulation at day5(Fig.4B).Upregu-lation of the costimulatory molecules CD80,CD86and CD40,and HLA-DR class II and HLA class I molecules was also observed(Fig.4B).In only CD3-activated PBMC, the number of CD14+monocytes and cells expressing CD83and CD1remained constant.Upregulation of the costimulatory molecules CD80,CD86,CD40and HLA class I and of HLA-DR was clearly lower than in CAPRI cell cultures(Fig.4C).Quantitative analysis of leucocyte subpopulations in CD3-activated PBMC and CAPRI cells fromfive patients with cancer showed significantly more matured dendritic cells in CAPRI cultures than in CD3-activated PBMC(paired t-test,P=0.000096)(Table1) and a higher percentage of monocytes in CD3-activated PBMC compared to CAPRI cells on day5(paired t-test, P=0.023)(Table1).Depletion of CD14+monocytes,CD83+dendritic cells,CD3+CD8+or CD3+CD4+T cells and cancer cell lysis Depletion of subpopulations and the resulting effect on lysis were analysed at the following time points:1)inBreast cancer cells CD3--activated PBMC PBMC after 24hs of co-cultureA C EScandinavian Journal of Immunology,2012,75,314–328unstimulated PBMC before CD3activation;2)in unstimulated PBMC to be added to CD3-activated PBMC;and3)from CAPRI cells before coculture with cancer cells(Fig.5).Depletion of CD3+CD8+T lympho-cytes at each time point prevented CAPRI cells from developing any lytic capacity(Fig.5D),and depletion of CD3+CD4+T cells had the same effect at each time point(Fig.5C).Depletion of CD14+monocytes at time point1)or2)completely abrogated the lytic activity of CAPRI cells(Fig.5A),whereas depletion of monocytes at time point3)did not significantly influence the lysis of cancer cells.Depletion of CD83+dendritic cells reduced the devel-opment of CAPRI cell lytic efficiency by50%(Fig.5B). This‘medium’contribution to the lytic capacity of CAPRI cells may indicate a continuous supply of contact information and⁄or of cytokines to T effector cells during cancer cell destruction.The failure of immune responses as a consequence of rudimentary immunogenic informa-tion from cancer cells has been previously demonstrated [32,33].Depletion of B lymphocytes did not signifi-cantly influence lysis(data not shown).Presence of CD4+T lymphocytes versus replacement by CAPRI culture supernatantsCAPRI culture supernatants should clarify whether CD4+ T lymphocytes only provide cytokine help to cytotoxic CD8+T cells.Supernatants were added at depletion time point1)or2).In the absence of CD4+T cells,cancer cells were only minimally destroyed(not shown).Less increase in the regulatory T cell population(CD4+CD25high Foxp3+)in CAPRI cell culturesSeveral reports have described the suppression of cyto-lytic responses against human cancer cells by CD4+CD25+regulatory T cells[37–45].Modulation and suppression have appeared to be restricted to CD4+CD25high Foxp3+T lymphocytes,either antigen-specific or non-antigen-specific[37–45].The percentage of CD4+CD25high Foxp3+T lymphocytes is strongly increased in CD3-activated cells compared to unstimu-lated PBMC.In CAPRI cultures,this increase is only moderate(Fig.6).Ó2011The Authors.Scandinavian Journal of ImmunologyÓ2011Blackwell Publishing Ltd.Significant lysis of cancer cells by CAPRI cells in nude miceBreast cancer cells were implanted in twelve female mice.After tumour implantation,six mice were injected with autologous PBMC (controls),and the other six were injected with autologous CAPRI cells (verum).In this breast cancer model,the average tumour size was 29.64±6.95mm in the control group,whereas the tumour size was 5.08±1.66mm in the mice receiving CAPRI cell therapy.Furthermore,the verum group showed an average survival time of 43±1.17days,and the control group survived an average of 29.67±1.92days (P =5.06·10)4,Fig.7A,C,D,Table 2).CAPRI cell treatment for patients with breast cancer and survival timeBreast cancer patients (T1-4N0-2M1,G2-3)treated with CAPRI cells in an adjuvant treatment attempt were com-pared with patients of the Munich Tumor Center (T1-4N0-2M1,G2-3)using Kaplan–Meyer statistics.All breast cancer patients with distant metastasis who received at least 500·106CAPRI cells in total were included in the comparative analysis.It was recom-mended that patients should receive 60–80·106CAPRI cells thrice a week for at least 1year.Despite variationsin the frequency of injection and cell number,which are unavoidable in treatment attempts,CAPRI cell-treated patients showed a significant increase in survival (Fig.7B).Patients reported no adverse reactions from CAPRI cells;rather,adverse reactions from chemotherapy were neutralized by the CAPRI cell therapy.Most patients with adjuvant CAPRI cell treatment were able to resume professional activities 1day after chemother-apy.DiscussionThe dramatic power of autologous MHC-restricted immune responses,first recognized by Zinkernagel and Doherty [46],contrasts with the immune surveillance failure of MHC-restricted tumour-infiltrating lympho-cytes (TIL).However,TIL can be successfully revived in vitro [47].ACT using autologous TIL combined with non-myeloablative chemotherapy and irradiation achieved a complete response in seven of 25patients (28%)[47],a fundamental progress for ACT.Unprofessional presentation of tumour-immunogenic peptides and costimulatory molecules by cancer cellsoften induces the inactivation of naı¨ve T cells.To avoid this inactivation,we developed the following priming procedure:we stimulated APC by activating T cells inIncubationwith CAPRI cellsIncubationwith CD3-activated PBMCIncubation with PBMCHLA-class I expressionof carcinoma cellsHLA-DR class II expressionof carcinoma cellsA BCFigure 3Increased HLA class I and HLA class II expression in breast cancer cells after cocultivation with cascade-primed (CAPRI)cells.To save a sufficient number of unlysed cancer cells for observation,a low effector to target (E:T)ratio of 5:1was used.Grey area with black outline represents basic level of expression,and white area with black outline represents expression after adding of CAPRI cells.HLA expression of CFSE-labelled colon cancer cells F2was determined after 5days of coculture with (A)CAPRI cells,(B)CD3-activated PBMC or (C)unstimulated PBMC.CAPRI cells increased cancer cells’mean intensity of fluorescence (MIF)in the expres-sion of HLA class I by 40%and HLA-DR class II antigens by 60%(A).No significant change in cancer cell HLA expression was observed after incubation with CD3-activated (B)or unstimulated PBMC (C).Scandinavian Journal of Immunology ,2012,75,314–328。
·临床研究·医学食疗与健康 2021年6月第19卷第12期58肿瘤微环境在肿瘤免疫治疗中的作用作者简介:高红亮(1992.02-),男,硕士,助教,研究方向为肿瘤病理生理 高红亮(皖南医学院,安徽 芜湖 241000)【摘要】肿瘤免疫治疗,是指通过训练常驻免疫细胞的识别和清除携带肿瘤特异性抗原的细胞来实现,以便提供外部刺激来增强免疫信号介导肿瘤细胞的消除。
当T 细胞被原代转化细胞或介体细胞[如TME 内的抗原呈递细胞(APC )]激活时,T 细胞开始一系列信号事件,导致细胞和非细胞免疫成分的招募、抗原特异性T 细胞的克隆性扩增和刺激性细胞因子的释放,最终杀灭肿瘤细胞。
但是由于肿瘤微环境,往往会导致肿瘤细胞出现逃逸而继续增殖与侵袭。
因此,探索肿瘤微环境在肿瘤免疫治疗中的作用,会明显的改善肿瘤免疫治疗的效果。
【关键词】肿瘤免疫治疗;肿瘤微环境;CTL4;PD-1;PD-L1【中图分类号】R73-36 【文献标识码】A 【文章编号】2096-5249(2021)12-0058-02.................在过去的十年里,免疫疗法经历蜕变,与传统的针对癌细胞生物学过程的化学疗法不同,免疫疗法旨在增强机体对癌症的自然免疫防御能力[1]。
肿瘤微环境(Tumor microenvironment,TME)的细胞和分子成分都会影响免疫治疗的有效性,故针对肿瘤微环境在免疫治疗中的研究很有必要。
抗原特异性免疫识别过程是一个复杂的过程,包括抗原提呈以及淋巴细胞的识别。
自身蛋白和外源蛋白被细胞质中的蛋白酶体消化,形成8~9个氨基酸肽,转运到内质网。
接着,被伴侣分子装载到主要组织相容性复合物(MHC)Ⅰ类蛋白质上,并被运送到细胞表面。
一旦到达表面上,一个带有特定MHC Ⅰ类肽复合物受体的T 细胞可以与之结合,并在共刺激分子的帮助下,触发免疫细胞激活。
但是,这一生理过程在TME 中常常是失调的,因为细胞失去了抗原分解的关键成分,这使肿瘤细胞有效地隐藏在免疫细胞中[2]。