dose escalation of low molecular weight heparin to manage
- 格式:pdf
- 大小:148.68 KB
- 文档页数:6
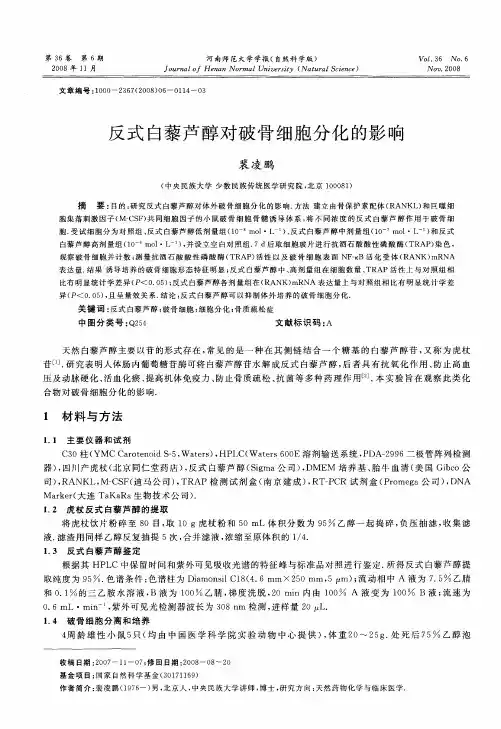
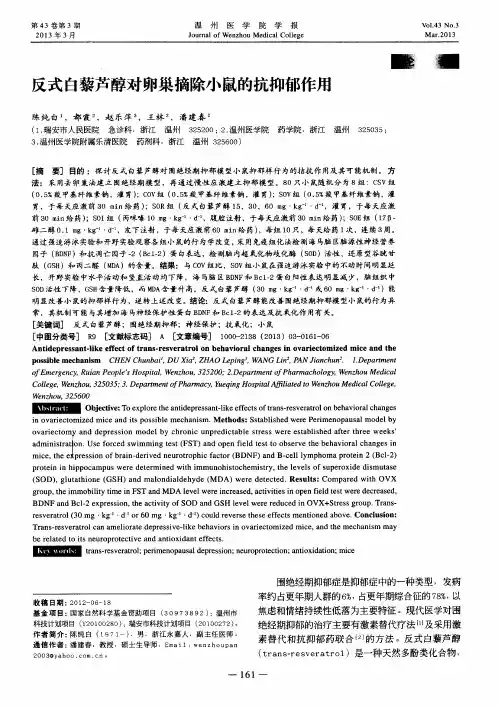
ORIGINAL ARTICLEDose escalation of low molecular weight heparin to manage recurrent venous thromboembolic events despite systemic anticoagulation in cancer patientsM.C A R R I E R,* G.L E G A L,àR.C H O,§S.T I E R N E Y,* M.R O D G E R* and A.Y.L E E–*Thrombosis Program,Division of Hematology,Department of Medicine,University of Ottawa,Ottawa,ON; Clinical Epidemiology Program, The Ottawa Health Research Institute,Ottawa,ON;àDepartment of Internal Medicine and Chest Diseases,EA3878,Brest University Hospital, Brest,France;§Department of Medicine,Michael G.DeGroote School of Medicine,McMaster University,Hamilton,ON;and–Thrombosis Program,Department of Medicine,University of British Columbia,Vancouver,BC and Department of Medicine,McMaster University,Hamilton, ON,CanadaTo cite this article:Carrier M,Le Gal G,Cho R,Tierney S,Rodger M,Lee AY.Dose escalation of low molecular weight heparin to manage recurrent venous thromboembolic events despite systemic anticoagulation in cancer patients.J Thromb Haemost2009;7:760À5.Summary.Background:Cancer patients with venous throm-boembolism(VTE)are at high risk of recurrent VTE despite standard anticoagulation.To date,very little published literature is available to guide the treatment of cancer patients with recurrent VTE.Objectives:To evaluate the benefit and risk of low molecular weight heparin(LMWH) dose escalation in cancer patients with recurrent VTE. Patients and methods:This was a retrospective cohort study of consecutive cancer outpatients referred for management of a symptomatic,recurrent VTE while receiving an anticoag-ulant.Confirmed episodes of recurrent VTE were treated with either dose escalation of LMWH in patients already anticoagulated with LMWH,or initiation of therapeutic dose LMWH in patients who were taking a vitamin K antagonist (VKA).All patients were followed for a minimum of 3months after the index recurrent VTE unless they died during this period.Results:Seventy cancer patients with a recurrent VTE despite ongoing anticoagulation were included.At the time of the recurrence,67%of patients were receiving LMWH,and33%were receiving a VKA.A total of six patients[8.6%;95%confidence interval (CI)4.0À17.5%]had a second recurrent VTE during the 3-month follow-up period,at an event rate of9.9per 100patient-years(95%CI 2.0À17.8%).Three patients (4.3%;95%CI 1.5À11.9%),or 4.8per100patient-years (95%CI0.0À10.3%)of follow-up,had bleeding complica-tions.The median time between the index recurrent VTE to death was11.4months(range,0À83.9months).Conclusions: Cancer patients with recurrent VTE have a short median survival.Escalating the dose of LMWH can be effective for treating cases that are resistant to standard,weight-adjusted doses of LMWH or a VKA.Keywords:cancer,cancer-associated thrombosis,low molecular weight heparin,recurrent venous thromboembolism, treatment.BackgroundPatients with cancer have a four-fold increased risk of developing a venous thromboembolism(VTE)relative to the general population[1,2].They also have a three-fold risk of recurrent VTE and a three-fold to six-fold risk of major bleeding while receiving anticoagulant treatment with a vita-min K antagonist(VKA),as compared with patients without cancer[3À5].Low molecular weight heparin(LMWH)therapy for3À6months is now recommended over VKA as afirst-line treatment to reduce the risk of recurrent VTE in patients with active cancer[6,7],on the basis of several randomized controlled trials that compared the relative efficacy and safety of LMWH with VKA therapy[8,9].In the CLOT trial,a therapeutic dose of dalteparin for thefirst month followed by a ÔmaintenanceÕdose of75À80%of the full therapeutic dose for the next5months reduced the relative risk of recurrent VTE in the dalteparin group by52%[8].Importantly,differences in bleeding and survival were not observed.The CLOT study also demonstrated that9À17%of cancer patients will develop recurrent VTE,despite therapy with LMWH or VKA,over6months of follow-up.Furthermore, the overall survival of these patients was reduced:60%were dead within1year after the diagnosis of VTE.To date,very little published literature is available to guide the treatment ofCorrespondence:Agnes Y.Lee,Director of Thrombosis,Division ofHematology,University of British Columbia,Diamond Health CareCenter,2775Laurel Street10thfloor,Vancouver,BC,V5Z1M9,Canada.Tel.:+16048754952;fax:+16048754696.E-mail:alee14@bccancer.bc.caReceived20November2008,accepted11February2009Journal of Thrombosis and Haemostasis,7:760À765DOI:10.1111/j.1538-7836.2009.03326.xÓ2009International Society on Thrombosis and Haemostasiscancer patients with recurrent VTE despite standard anti-coagulation treatment.The American College of Chest Physicians previously recommended the insertion of an inferior vena cava(IVC)filter in patients with recurrent VTE while on anticoagulant therapy[10].However,this recommendation has been withdrawn from the most recent guidelines published in June2008[7].For cancer patients with recurrent VTE,the American Society of Clinical Oncology recommends the use of an alternate anticoagulant regimen(e.g.switch to LMWH if the patient had been receiving a VKA),or the insertion of an IVCfilter,as a possible management option [6].However,these recommendations are based on weak evidence.Indeed,the risk of recurrent deep vein thrombosis (DVT)after IVCfilter insertion has been reported to be as high as32%in patients with cancer,and is associated with significant morbidity and poor quality of life[5,11À14]. These poor outcomes are not unexpected,asfilters do not control or dampen the hypercoagulable state in these patients,and may introduce another nidus for thrombus formation.Dose escalation of LMWH may represent an alternative to IVCfilter insertion in cancer patients with recurrent VTE.A retrospective study of32patients suggested that LMWH therapy might be effective in the management of recurrent VTE in patients taking a VKA[15].In that particular study,63%of patients had a diagnosis of cancer.It is currently unknown whether dose escalation of LMWH would be effective and safe for treating recurrent VTE in cancer patients already on LMWH.One case report has described successful management of recurrent VTE in a patient with cervical cancer using a supratherapeutic dose of LMWH[16].To further evaluate the benefit and risk of LMWH dose escalation in cancer patients with recurrent VTE,we performed a retrospective study in two large thrombosis clinics. Patients and methodsPatient populationA retrospective cohort study of consecutive cancer outpa-tients referred for management of a symptomatic,recurrent VTE while receiving an anticoagulant was conducted at the Ottawa Hospital Thrombosis Unit,Ottawa,ON(July2004 to June2008;n=31)and the Henderson Hospital Outpa-tient Thrombosis Unit,Hamilton,ON(April2003to June 2007;n=39).Patients were included if they had:(i) documented active malignancy;(ii)objectively provenfirst episode of VTE[proximal lower extremity DVT,upper extremity DVT or pulmonary embolism(PE)];and(iii) objectively documented recurrent VTE(either new or extended proximal lower extremity DVT,upper extremity DVT,or PE)while taking systemic anticoagulation medica-tion(LMWH or a VKA).Only cases with symptomatic VTE were included.Research ethics board approval was obtained for the study.Data collectionThe following variables were prespecified prior to data collection:(i)patient demographics;(ii)management of the initial VTE;(iii)cancer history(site and stage);(iv)dates of diagnosis of the initial and recurrent episodes of VTE;(v) radiologic evidence of the location/extent of the initial and recurrent VTE;(vi)dose of LMWH(therapeutic,maintenance, low dose)or International Normalized Ratio(INR)(thera-peutic or subtherapeutic)at the time of the index recurrent VTE;(vii)management of the index recurrent VTE;(viii) further recurrent VTE or bleeding within3months after the index recurrence;and(ix)death(date and cause).Other information relevant to recurrent VTE or bleeding events,such as withholding of anticoagulation treatment for surgery,was also recorded.For this study,a therapeutic dose of LMWH was defined as dalteparin200units kg)1once daily,tinzaparin175units kg)1 once daily,or enoxaparin1mg kg)1twice daily or1.5mg kg)1 once daily.The maintenance dose of LMWH was defined as 75À80%of the full therapeutic dose.Low dose was defined as any dose less than75%of the full therapeutic dose.The therapeutic anticoagulation for VKA was defined as an INR greater than or equal to2.0.Subtherapeutic INR was defined as less than2.0.Data were extracted independently by two investigators at each site.Disagreements on information were resolved by consensus or retrieving further information from other medical records.ManagementThe management of recurrent VTE was consistent at both thrombosis units.All objectively confirmed episodes of recur-rent VTE were treated with either dose escalation of LMWH in patients already anticoagulated with LMWH or initiation of a therapeutic dose of LMWH in patients who were taking a VKA.Patients on a therapeutic dose of LMWH at the time of the recurrent VTE were managed by increasing the weight-adjusted dose by20À25%for at least4weeks.Patients on a maintenance dose were treated by increasing the LMWH to a therapeutic dose for6À12weeks.Patients on low-dose LMWH were managed by increasing the LMWH to a therapeutic dose for1month,and using a maintenance dose thereafter.Similarly,patients on a VKA(therapeutic or subtherapeutic)were treated with a therapeutic dose of LMWH for1month,followed by a maintenance dose.Anti-factor Xa measurements at the time of the index recurrent VTE or after dose escalation were not routinely performed. Outcome assessment and follow-upAll patients were followed for a minimum of3months after the index recurrent VTE,unless they died during this period.The primary outcome measure was the incidence of a second, symptomatic recurrent VTE diagnosed over a3-month Recurrent venous thromboembolism in patients with cancer761Ó2009International Society on Thrombosis and Haemostasisfollow-up period after thefirst(index)recurrent VTE.Initial proximal lower extremity DVT was defined a non-compressible segment on compression leg vein ultrasound imaging in the popliteal vein or a more proximal leg vein.Initial upper extremity DVT was defined as a non-compressible segment on compression ultrasound in the brachial or internal jugular deep veins,or absentflow in the subclavian vein.Initial PE was defined as a high-probability ventilation/perfusion(V/Q)lung scan or a segmental or larger pulmonary arteryfilling defect on spiral computed tomography(sCT)scan.Recurrent DVT was defined as a new non-compressible site or proximal extension from a previous measurement.Recurrent PE was defined as a new mismatched segmental or greater perfusion defect on V/Q scan or a new intraluminalfilling defect in a segmental or larger pulmonary artery on sCT scan.Secondary outcome measures included minor and major bleeding over the3-month period after the index recurrent VTE (regardless of the status of anticoagulation at the time of the bleed),and overall and VTE-related death.Major bleeding events were defined as:(i)fatal bleeding;(ii)symptomatic bleeding in a critical area or organ,such as intracranial, intraspinal,intraocular,retroperitoneal,intra-articular or peri-cardial,or intramuscular with compartment syndrome;and(iii) bleeding causing a fall in hemoglobin level of20g L)1or more, or leading to transfusion of two or more units of whole blood or red cells[17].Date of last follow-up and date of death(if available in the clinic chart)were recorded.VTE-related death was defined as a fatal PE confirmed on autopsy or as an unexplained sudden death[18].AnalysesA descriptive summary of the baseline characteristics of the cohort is provided.We reported the proportions,with95% confidence intervals(CIs),of patients with a second or more episodes of recurrent VTE and major bleeding during the 3-month follow-up period.The corresponding event rates were calculated on the basis of100patient-years of follow-up.A KaplanÀMeier survival curve was constructed to estimate the time to the index recurrent VTE from the initial diagnosis,and a separate curve was plotted to estimate overall survival following the index recurrent VTE.Patients were censored after the last known date of follow-up or death.The median time between the initial and index recurrent VTE,and the median time between the index recurrent VTE and death,were determined. ResultsSeventy cancer patients with a recurrent VTE despite ongoing anticoagulation are included in this report.The study partic-ipantsÕcharacteristics are summarized in Table1.The median age was60years(range,27À84years).Thirty-eight(54%) were female.Forty-four patients(63%)had metastatic cancer at the time of their initial VTE.The most common type of cancer was lung carcinoma.At the time of the initial VTE,39 patients(56%)had a proximal lower extremity DVT,12(17%)had an upper extremity DVT(five cases were catheter-related), 14(20%)had a PE,andfive(7%)had both a leg DVT and a PE.At the time of the symptomatic index recurrence,47(67%) patients were on LMWH,and23(33%)were on VKAs.Of the 47patients on LMWH,15(32%),24(51%)and eight(17%) were on therapeutic,maintenance and low doses,respectively. Eleven(48%)and seven(30%)of the23patients on VKAs had a therapeutic(‡2)and subtherapeutic INR,respectively, whereasfive(22%)patients did not have a documented INR result at the time of the recurrent VTE event.Of the70index recurrent VTEs,40(57%)involved the lower extremity,13(19%)occurred in an upper extremity(five were catheter-related),and15(21%)presented as PE.Two(3%) patients had a recurrent VTE in the IVC.Table2summarizes the location and extent of the index recurrences.It is of note that67%of the recurrent VTEs developed at a new site(e.g. the initial episode was a right leg DVT,and the recurrent episode presented as a PE).The median time between the initial VTE to recurrence(index episode)was3.5months(range, 0.3À193months)(Fig.1).A total of20patients(29%)had the index recurrent VTE less than4weeks following the initial diagnosis.All70objectively confirmed episodes of recurrent VTE were treated with either dose escalation of LMWH in patients already anticoagulated with LMWH or initiation of therapeu-tic-dose LMWH in patients who were taking a VKA.Three patients also had an IVCfilter inserted.Overall,55patients were treated with a therapeutic dose of LMWH,and15 patients received120%of a therapeutic dose of LMWH for the index recurrent VTE.A total of six patients(8.6%;95%CI 4.0À17.5%)had a second recurrent VTE during the3-month follow-up period,at an event rate of9.9per100patient-years(95%CI 2.0À17.8%).The median time between the index and second recurrent VTE was1.9months(range,0.6À3.0months).Three patients(50%)had their second recurrence while on therapeu-tic doses of LMWH,and the other three were on120%of a therapeutic dose of LMWH.All were treated by increasing the weight-adjusted dose by20À25%for at least4weeks,and one patient had an IVCfilter inserted as well.None of these patients had any further recurrent thrombotic event during the 3-month follow-up period.Of these six patients with a second recurrence,five(83%)had metastatic disease and four(67%) had an underlying diagnosis of lung carcinoma.Only three patients(4.3%;95%CI 1.5À11.9%),or4.8per 100patient-years(95%CI0.0À10.3%)of follow-up,had bleeding complications after their index recurrent VTE.One patient with a malignant brain tumor had an intracranial bleed after the LMWH was increased to a therapeutic dose.Two patients(2.9%;95%CI0.9À9.8%)had a minor bleeding episode while receiving therapeutic LMWH.At the time of the last follow-up,a total of36patients were dead.None of the deaths were related to the recurrent VTE or bleeding.The median time between the index recurrent VTE to death was11.4months(range,0À83.9months)(Fig.2).The762M.Carrier et alÓ2009International Society on Thrombosis and Haemostasismedian survival was only 4.3months (range,0.9À4.9months)after a second recurrence (data not shown).DiscussionThis is the largest report on the management and outcomes of cancer patients following a recurrent episode of VTE while they were being treated with an anticoagulant.Our retrospective cohort study demonstrates that recurrent VTE in cancer patients can be effectively and safely managed by escalating the dose of LMWH or switching to LMWH from warfarin.Although the exact dosing of LMWH for the recurrent VTE differed (depending on the anticoagulant regimen at the time of the recurrence),escalating the dose of LMWH resulted in a second recurrent VTE rate of 8.6%(95%CI 4.0À17.5%),and it was well tolerated,with few bleeding complications.The high rate of response to dose escalation suggests that recurrent VTE in cancer patients might be a consequence of Ôresistance Õto standard doses of LMWH,and that higher doses are needed.This is in contrast to a true failure of LMWH anticoagulation,whereby dose escalation is not successful and other therapeuticTable 1Baseline characteristicsLMWH(N =47)(n ,%)Vitamin K antagonist(N =23)(n ,%)Study population (N =70)(n ,%;95%CI)Female25(53.2)13(56.5)38(54.3;42.7À65.5)Age,years (median;range)58(27À83)64(49À90)60(27À90)Cancer location Lung 15(31.9)6(26.1)21(30.0;20.5À41.6)Colon 9(19.2)1(4.3)10(14.3;8.0À24.4)Breast 3(6.3)2(8.6)5(7.1;3.2À15.7)GI 10(21.3)2(8.6)12(17.1;10.1À27.7)GU1(2.1)3(13.0)4(5.7;2.3À13.8)Gynecological 2(4.3)3(13.0)5(7.1;3.2À15.7)Hematological 4(8.5)2(8.6)6(8.6;4.1À17.5)Other3(6.3)4(17.4)7(10.0;5.0À19.3)Cancer stageNon-metastatic 18(38.3)6(26.1)24(34.3;24.2À46.0)Metastatic 28(59.6)16(69.6)44(62.9;51.1À73.2)NA1(2.1)1(4.3)2(2.9;0.9À9.8)Initial VTELower extremity DVT 24(51.1)15(65.2)39(55.7;44.0À66.8)Upper extremity DVT 9(19.2)3(13.0)12(17.1;10.1À27.7)Catheter-related 5(10.6)05(7.1;3.2À15.7)PE11(23.4)3(13.0)14(20.0;12.3À30.9)DVT and PE3(6.3)2(8.6)5(7.1;3.2À15.7)Anticoagulation at time of recurrence (n ,%;95%CI)(n ,%;95%CI)LMWHTherapeutic dose 15(21.4;13.5À32.4)NA Maintenance dose 24(34.3;24.2À46.0)NA Low dose8(11.4;6.0À21.0)NAVitamin K antagonists Therapeutic NA 11(15.7;9.1À26.0)Subtherapeutic NA 8(11.4;6.0À21.0)UnknownNA4(5.7;2.3À13.8)CI,confidence interval;DVT,deep vein thrombosis;GI,gastrointestinal;GU,genitourinary;LMWH,low molecular weight heparin;NA,not applicable;PE,pulmonary embolism;VTE,venous thromboembolism.Table 2Recurrent venous thromboembolism eventsStudy population (N =70)Recurrent lower extremity DVT (n ,%;95%CI)40(57.4;45.4À68.1)Ipsilateral13(18.6;11.2À29.3)Ipsilateral and new upper extremity DVT 1(1.4;0.3À7.6)Contralateral 12(17.1;10.1À27.7)Bilateral 3(4.3;1.6À11.9)New DVT11(15.7;9.1À26.0)Recurrent upper extremity DVT (n ,%;95%CI)13(18.6;11.2À29.3)Ipsilateral 3(4.3;1.6À11.9)Contralateral1(1.4;0.3À7.6)New upper extremity DVT 9(12.9;7.0À22.7)Recurrent PE (n ,%;95%CI)15(21.4;13.5À32.4)Recurrent PE 7(10.0;5.0À19.3)New PE8(11.4;6.0À21.0)Other (IVC thrombus)(n ,%;95%CI)2(2.9;0.9À9.8)CI,confidence interval;DVT,deep vein thrombosis;PE,pulmonary embolism;IVC,inferior vena cava.Recurrent venous thromboembolism in patients with cancer 763Ó2009International Society on Thrombosis and Haemostasisoptions would be required to suppress the hypercoagulable state.The heightened hypercoagulable state in these patients is also indirectly reflected by the short time to recurrence:29%of the index recurrences occurred within the first 4weeks of treatment.We can only speculate on the mechanism of anticoagulant resistance.Given that the majority of patients responded to a higher dose of LMWH,it is likely that these patients did not achieve therapeutic levels with standard,weight-adjusted doses of LMWH.Whether this is due to lower bioavailability from increased non-specific binding of LMWH to plasma proteins or cells,enhanced renal clearance,or perhaps a large clot burden,is unknown.We were unable to explore these hypotheses,because of the retrospective design of the study and the lack of anti-FXa levels at the time of the recurrence.Our study also shows that the median survival of patientswith recurrent VTE,especially following a second recurrent VTE,is very poor in cancer patients.Previous studies have demonstrated that cancer patients who develop a VTE have a shorter life expectancy than matched cohorts without thrombotic complications [19À21].The short median survival of 11.4months after a recurrent VTE in our study is consistent with a previously published report of a small cohort of cancer patients with recurrent VTE [22].It is unknown whether the early deaths are due to undiagnosed fatal PE or aggressive malignancies,which may have contributed to the anticoagulant resistance or failure.This should be taken into consideration when managing cancer patients with recurrent VTE.There are limitations of our study.First,this is a retrospec-tive cohort study,and the results may be subject to bias,incomplete information,or misdiagnosis.We tried to minimize selection bias by including all consecutive patients assessed at the two different thrombosis units.Charts of all patients with a diagnosis of cancer were fully reviewed by two reviewers independently,to identify patients with recurrent VTE on anticoagulants,and only patients with objectively diagnosed,symptomatic events were included.Second,a control group of cancer patients without a recent VTE were not available for comparison to evaluate the impact on survival or risk factors for recurrent VTE.Third,anti-FXa measurements were not routinely performed at the time of the index recurrent VTE.This is difficult to do in practice,as patients do not present at a time when peak or trough levels can be taken.Also,previous studies have shown a poor correlation between anti-FXa levels and clinical outcome [23,24].Fourth,the total numbers of second recurrent VTEs and bleeding events were rger studies are needed to provide more reliable estimates of the risk of recurrent VTE,bleeding and overall survival after dose escalation with LMWH.ConclusionCancer patients with recurrent VTE have a poor prognosis.Although the evidence is limited,our study suggests that escalating the dose of LMWH can be effective for treating cases that are resistant to standard,weight-adjusted doses of LMWH or a VKA.Prospective trials are required to assess the effectiveness and safety of this management option and to identify those who are at highest risk of anticoagulant resistance.Disclosure of Conflict of InterestsThe authors state that they have no conflict of interest.References1Blom JW,Doggen CJ,Osanto S,Rosendaal FR.Malignancies,pro-thrombotic mutations,and the risk of venous thrombosis.JAMA 2005;293:715À22.12243648607284Numberat risk701182221Time (months)0.00.20.40.60.81.0P r o p o r t i o n o f p a t i e n t s f r e e o f r e c u rr e n t V T E Time to recurrrent VTEFig.1.Time to index recurrent venous thromboembolism (VTE)afterinitial diagnosis of VTE.Number at risk7020103211Tiime (months)0122436486072840.00.20.40.60.81.0C u m u l a t i v e s u r v i v a lSurvival after recurrent VTE in cancer patients Fig.2.Kaplan ÀMeier survival curve after index recurrent venous thromboembolism (VTE).764M.Carrier et alÓ2009International Society on Thrombosis and Haemostasis2Heit JA,Silverstein MD,Mohr DN,Petterson TM,OÕFallon WM, Melton LJ III.Risk factors for deep vein thrombosis and pulmonary embolism:a population-based caseÀcontrol study.Arch Intern Med 2000;160:809À15.3Hutten BA,Prins MH,Gent M,Ginsberg J,Tijssen JG,Bu ller HR.Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both malignancy and achieved international normalized ratio:a retrospec-tive analysis.J Clin Oncol2000;18:3078À83.4Prandoni P,Lensing AW,Piccioli A,Bernardi E,Simioni P,Girolami B,Marchiori A,Sabbion P,Prins MH,Noventa F,Girolami A.Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis.Blood2002;100:3484À8.5Elting LS,Escalante CP,Cooksley C,Avritscher EB,Kurtin D, Hamblin L,Khosla SG,Rivera E.Outcomes and cost of deep venous thrombosis among patients with cancer.Arch Intern Med2004;164: 1653À61.6Lyman GH,Khorana AA,Falanga A,Clarke-Pearson D,Flowers C, Jahanzeb M,Kakkar A,Kuderer NM,Levine MN,Liebman H, Mendelson D,Raskob G,Somerfield MR,Thodiyil P,Trent D, Francis CW.American Society of Clinical Oncology guideline:rec-ommendations for venous thromboembolism prophylaxis and treat-ment in patients with cancer.J Clin Oncol2007;25:5490À505.7Kearon C,Kahn SR,Agnelli G,Goldhaber S,Raskob GE,Comerota AJ.Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Prac-tice Guidelines(8th Edition).Chest2008;133(Suppl.6):454SÀ545S. 8Lee AY,Levine MN,Baker RI,Kakkar AK,Prins M,Rickles FR, Julian JA,Haley S,Kovacs MJ,Gent M.Randomized Comparison of Low-Molecular-Weight Heparin versus Oral Anticoagulant Ther-apy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer(CLOT)Investigators.Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer.N Engl J Med2003;349: 146À53.9Hull RD,Pineo GF,Brant RF,Mah AF,Burke N,Dear R,Wong T, Cook R,Solymoss S,Poon MC,Raskob G.LITE Trial Investigators.Long-term low-molecular-weight heparin versus usual care in proxi-mal-vein thrombosis patients with cancer.Am J Med2006;119: 1062À72.10Buller HR,Agnelli G,Hull RD,Hyers TM,Prins MH,Raskob GE.Antithrombotic therapy for venous thromboembolic disease:the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy.Chest2004;126(Suppl.3):401SÀ28S.11PREPIC Study Group.Eight-year follow-up of patients with perma-nent vena cavafilters in the prevention of pulmonary embolism:the PREPIC(Prevention du Risque dÕEmbolie Pulmonaire par Interrup-tion Cave)randomized study.Circulation2005;112:416À22.12Hann CL,StreiffMB.The role of vena cavalfilters in the management of venous thromboembolism.Blood Rev2005;19:179À202.13Mismetti P,Rivron-Guillot K,Moulin N.Vena cavafilters and treatment of venous thromboembolism in cancer patients.Pathol Biol (Paris)2008;56:229À32.14Jarrett BP,Dougherty MJ,Calligaro KD.Inferior vena cavafilters in malignant disease.J Vasc Surg2002;36:704À7.15Luk C,Wells PS,Anderson D,Kovacs MJ.Extended outpatient therapy with low molecular weight heparin for the treatment of recurrent venous thromboembolism despite warfarin therapy.Am J Med2001;111:270À3.16Cunningham MS,Gilmore R,OÕDonnell D,OÕDonnell JS.Manage-ment of refractory venous thrombosis associated with malignancy using a supra-therapeutic enoxaparin regimen.Ir J Med Sci2009, in press.17Schulman S,Kearon C.Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients.J Thromb Haemost2005;3:692À4.18Douketis JD,Gu CS,Schulman S,Ghirarduzzi A,Pengo V,Prandoni P.The risk for fatal pulmonary embolism after discontinuing antico-agulant therapy for venous thromboembolism.Ann Intern Med2007;147:766À74.19Sorensen HT,Mellemkjaer L,Olsen JH,Baron JA.Prognosis of cancers associated with venous thromboembolism.N Engl J Med2000;343:1846À50.20Mandala M,Reni M,Cascinu S,Barni S,Floriani I,Cereda S,Berardi R,Mosconi S,Torri V,Labianca R.Venous thromboembolism pre-dicts poor prognosis in irresectable pancreatic cancer patients.Ann Oncol2007;18:1660À5.21Alcalay A,Wun T,Khatri V,Chew HK,Harvey D,Zhou H,White RH.Venous thromboembolism in patients with colorectal cancer: incidence and effect on survival.J Clin Oncol2006;24:1112À18.22Descourt R,Le Gal G,Couturaud F,Mottier D,Bressolette L, Robinet G,Roge C,Oger E,Leroyer C.Recurrent venous thrombo-embolism under anticoagulant therapy:a high risk in adenocarci-noma?Thromb Haemost2006;95:912À13.23Bounameaux H,de Moerloose P.Is laboratory monitoring of low-molecular-weight heparin therapy necessary?No.J Thromb Haemost 2004;2:551À4.24Gray E,Mulloy B,Barrowcliffe TW.Heparin and low-molecular-weight heparin.Thromb Haemost2008;99:807À18.Recurrent venous thromboembolism in patients with cancer765Ó2009International Society on Thrombosis and Haemostasis。