Depression,AnxietyandStressScale(DASS21)
- 格式:pdf
- 大小:132.34 KB
- 文档页数:2

·心理卫生评估·价值评估问卷中文版在大学生中的效度和信度检验毕丹丹1,2 丁晴雯1,2 张家萌1,2 陈杰1 李新影1,2(1中国科学院心理研究所,中国科学院心理健康重点实验室,北京100101 2中国科学院大学心理学系,北京100049 通信作者:李新影lixy@psych ac cn)【摘 要】目的:评估价值评估问卷(VQ)中文版在大学生中的效度和信度。
方法:在大学生中收集有效问卷625份,其中224人同时完成幸福感、负性情绪状态和心理灵活性其他成分3类效标工具,选取其中100人进行两周后重测。
结果:探索性因子分析提取VQ“进展”和“障碍”2个因子;验证性因子分析表明,两因子结构拟合可以接受(SBχ2=75 173,df=31,CFI=0 939,TLI=0 912,RMSEA=0 068,SRMR=0 056)。
心理幸福感、生活满意度和积极情绪与进展得分正相关(r=0 55、0 52、0 63),而与障碍得分负相关(r=-0 61、-0 45、-0 41);负性情绪状态得分、心理灵活性的经验性回避得分与进展得分负相关(r=-0 41、-0 38),而与障碍得分正相关(r=0 53、0 47),均P<0 01。
2个因子的Cronbachα系数分别为0 81和0 68,重测信度分别为0 68和0 70。
结论:价值评估问卷(VQ)中文版在大学生中具有可接受的效度和信度。
【关键词】 接纳承诺疗法(ACT);心理灵活性;价值;效度;信度 中图分类号:B841 7 文献标识码:A 文章编号:1000-6729(2021)005-0417-06 doi:10 3969/j issn 1000-6729 2021 05 011(中国心理卫生杂志,2021,35(5):417-422 )ValidityandreliabilityoftheChineseversionoftheValuingQuestionnaireincollegestudentsBIDandan1牞2牞DINGQingwen1牞2牞ZHANGJiameng1牞2牞CHENJie1牞LIXinying1牞21CASKeyLaboratoryofMentalHealth牞InstituteofPsychology牞Beijing100101牞China 2UniversityofChineseAcademyofSci ences牞Beijing100049牞ChinaCorrespondingauthor牶LIXinying牞lixy@psych ac cn【Abstract】Objective牶ToexaminethevalidityandreliabilityoftheChineseversionoftheValuingQuestion naire牗VQ牘incollegestudents Methods牶Totally625collegestudentswereassessedwiththeVQand224ofthemwereaskedtocompletethevalidityquestionnairesatthesametime After2weeks牞100participatesof244filledintheVQtoassessthetest retestreliability Results牶TheexploratoryfactoranalysisshowedthattheVQconsisted2factors牞namelyprogressandobstruction Theconfirmatoryfactoranalysisconfirmedthehypothesized2 factormod el牗SBχ2=75 173牞df=31牞CFI=0 939牞TLI=0 912牞RMSEA=0 068牞SRMR=0 056牘 Thescoresofpsycholog icalwell being牞lifesatisfactionandpositiveaffectwerepositivelycorrelatedwithprogressscore牗r=0 55牞0 52牞0 63牘牞andwerenegativelycorrelatedwithobstructionscore牗r=-0 61牞-0 45牞-0 41牘 Thescoresofnegativeemotionsandexperimentalavoidancewerenegativelycorrelatedwithprogress牗r=-0 41牞-0 38牘牞andwereposi tivelycorrelatedwithobstruction牗r=0 53牞0 47牞Ps<0 01牘 TheCronbachαcoefficientsoftheprogressandob structionwere0 81and0 68牞andthetest retestreliabilitieswere0 68and0 70 Conclusion牶Itsuggeststhatthe714中国心理卫生杂志 2021年 第35卷 第5期基金项目:应激下情绪与记忆的认知神经机制(31530031)ChineseversionoftheValuingQuestionnaire牗VQ牘hasacceptablepsychometricpropertiesincollegestudents【Keywords】 acceptanceandcommitmenttherapy牗ACT牘牷psychologicalflexibility牗PF牘牷values牷validity牷reliability牗ChinMentHealthJ牞2021牞35牗5牘牶417-422 牘 作为认知行为治疗“第三浪潮”的代表,接纳承诺疗法(acceptanceandcommitmenttherapy,ACT)的核心内容和最终目标是培养心理灵活性(psychologicalflexibility,PF),而不是关注症状的减少,因此是一种跨诊断的心理模型。

(完整版)DAM(抑郁量表)
(完整版)抑郁量表(DAM)
介绍
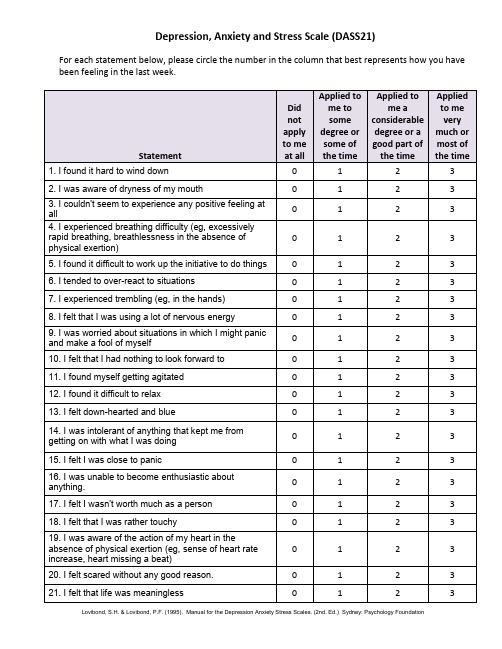
抑郁量表(Depression Anxiety Stress Scale,简称DASS)是一种常用的测量心理健康的工具。
它由最初的抑郁量表(Depression Scale)发展而来,后来增加了焦虑量表(Anxiety Scale)和压力量表(Stress Scale)。
三个维度
DAM包含了三个维度:抑郁、焦虑和压力。
通过填写问题等级表,可以得出被试者在这三个维度上的得分。
应用范围
DAM广泛应用于心理学研究领域和临床实践中,用于评估个人的心理状态和心理健康水平,尤其在诊断抑郁障碍和焦虑障碍等方面具有重要意义。
填写指南
填写DAM的问题等级表时,请在每个问题后选择一个最符合您目前状况的数字。
以下是填写指南:
- 0表示完全不适用
- 1表示在一定程度上适用
- 2表示在相当程度上适用
- 3表示非常适用
分数解读
抑郁维度、焦虑维度和压力维度的分数分别介于0-42之间。
分数越高,表明在该维度上的症状越严重。
注意事项
DAM是量表工具,不能作为独立的诊断依据。
如果您担心自己的心理健康,请咨询专业的心理健康专家进行评估和咨询。
希望DAM对您的心理健康评估有所帮助!。

注意缺陷多动障碍患儿照顾者照顾负担应对方式对负性情绪的影响李光建 曹静 高婷叶 舒京平 王舟 唐小伟[摘 要] 目的 观察注意缺陷多动障碍(ADHD )患儿照顾者照顾负担、应对方式对负性情绪的影响因素。
方法 选取2021年6月至2022年12月常州市德安医院心理科确诊的68例ADHD 儿童的照顾者为ADHD 组,选择同期在医院门诊进行常规体检的83例正常儿童的照顾者作为正常对照组,比较两组抑郁-焦虑-压力自评量表(DASS -21)、照顾者负担量表(ZBI )、简易应对方式问卷(SCSQ )评估结果。
结果 ADHD 组压力、焦虑、抑郁得分分别为10.0(6.0,16.0)、6.0(2.0,11.5)和5(2.0,11.5)分,照顾者的照顾负担为27.0(20.0,45.0)分,均高于正常对照组,差异均有统计学意义(P <0.05);ADHD 组照顾者的压力与照顾负担和消极应对方式呈正相关(P <0.05);ADHD 照顾者的焦虑与照顾负担呈正相关(P <0.05),与积极应对方式呈负相关(P <0.05);ADHD 照顾者的抑郁与照顾负担和消极应对方式呈正相关( P <0.05),与积极应对方式呈负相关(P <0.05);照顾负担、消极应对方式是ADHD 照顾者压力的影响因素(P <0.05),照顾负担、积极应对方式是ADHD 照顾者焦虑的影响因素(P <0.05),照顾负担、积极应对方式、消极应对方式是ADHD 照顾者焦虑的影响因素(P <0.05)。
结论 ADHD 照顾者的负性情绪较多、照顾负担较重,照顾者的照顾负担和应对方式是影响其负性情绪的主要因素。
[关键词]注意缺陷多动障碍;照顾者;照顾负担;负性情绪doi:10.3969/j.issn.1000-0399.2023.10.023Impact of caregiver burden coping styles on negative emotions in children with attention deficit hyperactivity disorder LI Guangjian 1,CAO Jing 2,GAO Tingye 1,SHU Jingping 1,WANG Zhou 1,TANG Xiaowei 31.Department of Psychology,Changzhou De’an Hospital, Changzhou 213003,China 2.Department of Disease,Yucheng District People’s Hospital of Ya ’an, Ya’an 625000,China3.Department of Dsychology,Wutaishan Hospital Affiliated to Medical College of Yangzhou University, Yangzhou 225000,ChinaFunding project:2020 Jiangsu Provincial Health Commission General Project (No.M2020031),Key R&D Plan Project of Changzhou Science and Technology Bureau (No.CE20205049), Key R&D Plan Project of Changzhou Science and Technology Bureau (No.CE20215056)Correspondingauthor:GAOTingye,****************[Abstract ] Objective To observe the influencing factors of caregivers ’ care burden and coping style on negative emotions in childrenwith attention deficit hyperactivity disorder (ADHD). Methods From June 2021 to December 2022, caregivers of 68 ADHD children diag⁃nosed in the Department of Psychology at De ’an Hospital in Changzhou city were selected as the ADHD group, and caregivers of 83 normal children who underwent routine physical examinations at our outpatient department during the same period were selected as the normal control group. The evaluation results of the Depression Anxiety Stress Self Rating Scale (DASS-21), Caregiver Burden Scale (ZBI), and Simple Coping Style Questionnaire (SCSQ) were compared between the two groups. Results The score of stress, anxiety, and depression in the ADHD group was 10.0 (6.0, 16.0), 6.0 (2.0, 11.5)and 5 (2.0, 11.5), respectively. The caregiver ’s care burden was 27.0 (20.0, 45.0), all higher than those of the normal control group, and the differences were statistically significant (P <0.05).The pressure of ADHD caregivers was positively correlated with care burden and negative coping styles (P <0.05). The anxiety of ADHD caregivers was positively correlated with care burden (P<0.05),and negatively correlated with positive coping styles (P <0.05). The depression of ADHD caregivers was positively correlated with care burden and negative coping styles (both P <0.05), and negatively correlated with positive coping styles (P <0.05). The burden of care and negative cop⁃· 卫生服务研究 ·基金项目:2020年度江苏省卫生健康委面上项目(编号:M2020031);常州市科技局重点研发计划项目(编号:CE20205049);常州市科技局重点研发计划项目(编号:CE20215056)作者单位:213003 江苏常州 常州市德安医院心理科(李光建,高婷叶,舒京平, 王舟) 625000 四川雅安 雅安市雨城区人民医院病案科(曹静) 225000 江苏扬州 扬州大学医学院附属五台山医院心理科(唐小伟)通信作者:高婷叶,****************本文引用格式:李光建,曹静,高婷叶,等.注意缺陷多动障碍患儿照顾者照顾负担应对方式对负性情绪的影响[J ].安徽医学,2023,44(10):1255-1259.DOI :10.3969/j.issn.1000-0399.2023.10.023ing style were the influencing factors of stress in ADHD caregivers (P<0.05), the burden of care and positive coping style were the influencing factors of anxiety in ADHD caregivers (P<0.05), and the burden of care, positive coping style, and negative coping style were the influencing factors of anxiety in ADHD caregivers (P<0.05). Conclusions The caregivers of ADHD have more negative emotions and heavy care burden. The care burden and coping style of caregivers are the main factors affecting their negative emotions.[Key words] Attention deficit hyperactivity disorder;Caregiver;Care burden;Negative emotions注意缺陷多动障碍(attention-deficit/hyperactivitydisorder,ADHD)是一种起病于儿童期的神经发育性疾病[1]。

抑郁-焦虑-压力量表简体中文版(DASS-21)在中国大学生中的测试报告龚栩,谢熹瑶,徐蕊,罗跃嘉(认知神经科学与学习国家重点实验室[北京师范大学],北京100875)【摘要】目的:引入抑郁-焦虑-压力量表简体中文版(DASS-21),并对该量表的信效度进行验证。
方法:用DASS-21对1779名大学生施测,对结果进行项目分析、信效度检验和验证性因素分析。
结果:①DASS-21各项目与总分有较高相关;②DASS-21有较高的内部一致性信度和建构信度;③DASS-21有良好的结构效度和效标关联效度,其内在结构符合理论构想;④我国大学生在DASS-21抑郁和压力分量表上的得分低于国外同龄样本,男生的抑郁得分显著高于女生。
结论:DASS-21具有较好的信效度,可作为考察我国大学生负性情绪水平的有效工具。
【关键词】抑郁-焦虑-压力量表简体中文版;信度;效度;大学生中图分类号:R395.1文献标识码:A文章编号:1005-3611(2010)04-0443-04Psychometric Properties of the Chinese Versions of DASS-21in Chinese College StudentsGONG Xu ,XIE Xi-yao ,XU Rui,LUO Yue-jiaState Key Laboratory of Cognitive Neuroscience and Learning ,Beijing Normal University ,Beijing 100875,China【Abstract 】Objective:To evaluate psychometric properties of DASS-21(Chinese Version)in Chinese college students.Methods:A sample of 1779Chinese college students in Beijing was administrated with the Chinese Version of DASS-21and two other inventories.Item analysis,validity/reliability analysis and confirmative factor analysis were applied to the data.Results:①The correlation between each item and its corresponding subscale was high.②The three subscales had high internal consistency and composite reliability.③The whole scale had good construct validity and criterion-related validity.④The independent sample t -test indicated significant gender difference in depression,and Chinese college students had lower scores in depression and stress subscales.Conclusion:The Chinese Version of DASS-21is a reliable and valid instrument,and is suitable for the use in Chinese college students.【Key words 】The Chinese Versions of DASS-21;Reliability ;Validity ;Chinese college students【基金项目】国家自然科学基金重点项目(30670698);教育部创新团队(IRT0710);科技部支撑计划。
IntroductionThe DASS 21 is a 21 item self report questionnaire designed to measure the severity of a range of symptoms common to both Depression and Anxiety. In completing the DASS, the individual is required to indicate the presence of a symptom over the previous week. Each item is scored from 0 (did not apply to me at all over the last week) to 3 (applied to me very much or most of the time over the past week).The essential function of the DASS is to assess the severity of the core symptoms of Depression, Anxiety and Stress. Accordingly, the DASS allows not only a way to measure the severity of a patient’s symptoms but a means by which a patient’s response to treatment can also be measured.The DASS and DiagnosisAlthough the DASS may contribute to the diagnosis of Anxiety or Depression, it is not designed as a diagnostic tool. Indeed, a number of symptoms typical of Depression such as sleep, appetite and sexual disturbances, are not covered by the DASS and will need to be assessed independently. The DASS is not meant to replace a comprehensive clinical interview.SuicideSuicidality is not assessed by the DASS. Accordingly, the clinician will need to address directly this important symptom of Depression in their clinical interview.How often to use the DASS?Although the DASS can provide a comparison of symptoms from week to week, it is best given on first presentation and again after a period of time has lapsed long enough for the chosen treatment to have effect. In the case of antidepressant medication, the second administration should be between the 2-4 week period after the individual has commenced taking the medication. This period is long enough for most antidepressants to be expected to show some change in the patient.Scoring the DASSThe scale to which each item belongs is indicated by the letters D (Depression), A (Anxiety) and S (Stress). For each scale (D, A & S) sum the scores for identified items. Because the DASS 21 is a short form version of the DASS (the Long Form has 42 items), the final score of each item groups (Depression, Anxiety and Stress) needs to be multiplied by two (x2).Interpreting the DASSOnce multiplied by 2, each score can now be transferred to the DASS profile sheet, enabling comparisons to be made between the three scales and also giving percentile rankings and severity labels.DASS Severity Ratings(Don’t forget to multiply summed scores by x 2)As previously mentioned, the DASS should not be used on its own to assess the presence or absence of Depression or Anxiety. High scores on the DASS would certainly alert the clinician to a high level of distress in the patient and this would need to be explored further within the interview process. Similarly, low scores on the DASS should not be a substitute for a comprehensive clinical interview.High DASS scores which are not changing, may prompt the clinician to look for explanations and perhaps augment dosages or change medication. Here again, the DASS should be interpreted along side the clinical interview.Changes in scores in one scale (EG: Depression), with consistently high and unchanging scores in another scale (Anxiety) may alert the clinician to pay particular attention to the presence of a co-existing anxiety disorder which may need specific treatment in its own right. Similarly, decreasing Depression scores alongside unchanging Stress scores may alert the clinician to the presence of some life event or problem, which may need to be addressed directly.DASS 21 NAME DATEPlease read each statement and circle a number 0, 1, 2 or 3 which indicates how much the statement applied to you over the past week. There are no right or wrong answers. Do not spend too much time on any statement.The rating scale is as follows:0 Did not apply to me at all - NEVER1 Applied to me to some degree, or some of the time - SOMETIMES2 Applied to me to a considerable degree, or a good part of time - OFTEN3 Applied to me very much, or most of the time - ALMOST ALWAYSN S O AA1I found it hard to wind down01232I was aware of dryness of my mouth01233I couldn’t seem to experience any positive feeling at all01234I experienced breathing difficulty (eg, excessively rapid breathing,breathlessness in the absence of physical exertion)01235I found it difficult to work up the initiative to do things0123 6I tended to over-react to situations0123 7I experienced trembling (eg, in the hands)0123 8I felt that I was using a lot of nervous energy01239I was worried about situations in which I might panic and make a fool ofmyself012310I felt that I had nothing to look forward to0123 11I found myself getting agitated0123 12I found it difficult to relax0123 13I felt down-hearted and blue012314I was intolerant of anything that kept me from getting on with what I wasdoing012315I felt I was close to panic0123 16I was unable to become enthusiastic about anything0123 17I felt I wasn’t worth much as a person0123 18I felt that I was rather touchy012319I was aware of the action of my heart in the absence of physicalexertion (eg,sense of heart rate increase, heart missing a beat)012320I felt scared without any good reason0123 21I felt that life was meaningless0123FOR OFFICE USETOTALSDASS Severity RatingsThe DASS is a quantitative measure of distress along the 3 axes of depression, anxiety1 and stress2. It is not a categorical measure of clinical diagnoses.Emotional syndromes like depression and anxiety are intrinsically dimensional - they vary along a continuum of severity (independent of the specific diagnosis). Hence the selection of a single cut-off score to represent clinical severity is necessarily arbitrary. A scale such as the DASS can lead to a useful assessment of disturbance, for example individuals who may fall short of a clinical cut-off for a specific diagnosis can be correctly recognised as experiencing considerable symptoms and as being at high risk of further problems.However for clinical purposes it can be helpful to have ‘labels’ to characterise degree of severity relative to the population. Thus the following cut-off scores have been developed for defining mild/moderate/severe/ extremely severe scores for each DASS scale.Note: the severity labels are used to describe the full range of scores in the population, so ‘mild’ for example means that the person is above the population mean but probably still way below the typical severity of someone seeking help (ie it does not mean a mild level of disorder.The individual DASS scores do not define appropriate interventions. They should be used in conjunction with all clinical information available to you in determining appropriate treatment for any individual.1Symptoms of psychological arousal2The more cognitive, subjective symptoms of anxietyDASS 21 SCOREDEPRESSION SCORE ANXIETYSCORESTRESSSCOREDepression Anxiety Stress Normal0 - 40 - 30 - 7 Mild 5 - 6 4 - 58 - 9 Moderate7 - 10 6 - 710 - 12 Severe11 - 138 - 913 - 16 Extremely Severe14 +10 +17 +。
心理治疗常用评定量表大全本文档旨在介绍一些常用的心理治疗评定量表,供心理治疗师和研究人员参考和使用。
1. 抑郁症量表- 汉密尔顿抑郁量表 (Hamilton Depression Rating Scale, HAM-D) - 心理健康问卷 (Patient Health Questionnaire, PHQ-9)- 蒙特利尔心理评估问卷(Montgomery-Asberg Depression Rating Scale, MADRS)- 抑郁自评量表 (Beck Depression Inventory, BDI)2. 焦虑症量表- 康奈尔焦虑量表 (Cornell Scale for Anxiety and Depression, CSAD)- 贝克焦虑自评量表 (Beck Anxiety Inventory, BAI)- 自评量表-焦虑 (Zung Self-Rating Anxiety Scale, SAS)- 广泛性焦虑量表 (Generalized Anxiety Disorder 7, GAD-7)3. 创伤后应激障碍量表- 创伤后应激障碍自评量表 (Posttraumatic Stress Disorder Checklist, PCL)- 创伤后应激障碍量表 (Clinician-Administered PTSD Scale, CAPS)- 创伤后应激障碍临床诊断量表 (Structured Clinical Interview for DSM-5 PTSD, SCID-5-PTSD)4. 自我评价量表- 自尊量表 (Rosenberg Self-Esteem Scale, RSES)- 人际关系满意度量表 (Quality of Relationships Inventory, QRI) - 幸福感量表 (Subjective Happiness Scale, SHS)- 生活满意度量表 (Satisfaction with Life Scale, SWLS)5. 焦虑和抑郁量表- 抑郁和焦虑量表 (Hospital Anxiety and Depression Scale, HADS)- 忧郁和焦虑自评量表 (Depression Anxiety Stress Scales, DASS) - 焦虑抑郁自评量表 (Hospital Anxiety and Depression Scale, HADS)- 应激情绪自评量表 (Perceived Stress Scale, PSS)以上是一些常用的心理治疗评定量表,具体选择和使用要根据个体情况和研究目的来决定。
.) / DASS-21 -壓力量表(中文版情緒自評量表/ 抑鬱-焦慮。
,並根據過去一周的情況,在每個條目中選擇適用於你情況的程度選項?請仔細閱讀以下每個條目請回答每個條目,選擇沒有對錯之分。
3——總是符合————不符合;1 ——有時符合;2常常符合;?評價程度:0樣本特性:採用整群抽樣法,選取北京3所高校的在校學生1795人施測。
回收有效問卷1779份,其中男生555人,女生1224人,平均年齡19歲(18.88±2.54歲)。
樣本中1652人報告了專業,理科599人,文科1053人。
信度指標:三個分量表的內部一致性係數為:0.77,0.79,0.76;總量表的內部一致性係數為:0.89;三個分量表的建構信度為:0.72,0.80,0.76效度指標:進行驗證性因素分析:理論模型與觀察資料擬合度的卡方檢驗χ2(181)=1554.59,擬合度指數(GFI=0.92)、調整後的擬合度指數(AGFI=0.90),NFI=0.87、CFI =0.88、IFI =0.88、RFI=0.85、TLI =0.86,RMSEA =0.065。
..參考文獻:龔栩, 謝熹瑤, 徐蕊, & 羅躍嘉. (2010). 抑鬱-焦慮-壓力量表簡體中文版(DASS-21)在中國大學生中的測試報告. 中國臨川心理學雜誌, 18(4), 443-446....Scoring Instructions: 18 belong to Stress Subscale;、、、Item 1、68、1112、14 7、、9、20 belong to Anxiety Subscale、;15、194Item 2、21 belong to Depression Subscale.、、、、、Item 3510131617、Reference:. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Lovibond, PDepression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviourresearch and therapy, 33(3), 335-343..。