病例讨论 CSA09_全国麻醉学年会讲者文稿
- 格式:pdf
- 大小:377.39 KB
- 文档页数:15


时间:2017-08-09地点:麻醉科医生办公室主持人(全名和职称):曹水旺主治医师参加人员(全名和职称):讨论病例:姓名: 欧汪汪性别: 女年龄: 66岁床位: 28床病历摘要(诊疗情况等):女、66岁,全麻下行手术。
术前各项检查基本正常。
麻醉诱导:异丙酚100 mg,芬太尼0.15mg,维库秀胺6mg,手术开始后最后一次静注维库秀胺2mg,术中生命体征平稳,血气分析正常,30min手术结束。
术毕30min病人完全清醒,呼吸频率正常,但潮气量小,静注溴新斯的明2mg和阿托品0.5mg,10min后自主呼吸恢复正常,观察30min各生命体征正常,能有力握手和抬头而拔管,鼻导管吸氧。
拔管后32min患者突然躁动,呼吸困难,心率增快到130次/分,SpO2剧降至60%,立即重新气管插管后自主呼吸和各生命体征迅速恢复正常。
90min后再次予以拔除导管,鼻导管吸氧。
患者诉当时突感到呼吸无力。
讨论目的:1.呼吸困难的原因2.麻醉处理的不足之处和改进。
发言人:梁瑞龙住院医师:该患者术前各项检查正常,排除重症肌无力的诊断,手术中各项生命体征平稳,血气分析正常,排除二氧化碳潴留引起的苏醒延迟,最终考虑患者呼吸困难的原因是肌松药物的残余作用所致。
术中可以采用肌松监测仪,加强对肌松的监测。
黄艳华主治医师:现代全麻技术一般病人应在麻醉终止后15min左右基本恢复意识,能按指令活动肢体和睁眼等,30min意识和自主呼吸功能完全恢复。
该患者拔管后变现呼吸无力,潮气量不足,用溴新斯的明拮抗有效,固考虑该患者呼吸困难的原因是肌松药残余作用所致。
王坚副主任医师:引起术后呼吸困难的原因有:低温、肌松药残余作用、电解质絮乱、低血糖、缺氧和二氧化碳潴留。
根据患者的临床表现,我们可以逐一的排除,该患者术前各项检查正常,术中各项生命体征平稳,血气检查正常,可以排除低血糖、二氧化碳潴留引起的呼吸困难,结合患者的临床表现,该患者拔管后变现呼吸无力,潮气量不足,用溴新斯的明拮抗有效,诊断引起该患者呼吸困难的原因是肌松药残余作用,维库秀安的消除半衰期是60min,术后常有肌松作用残留。
麻醉科疑难危重病例讨论范文一、病例介绍。
今天我们来讨论一个超有挑战性的病例。
这是一位[具体年龄]岁的男性患者,就叫他老张吧。
老张呢,本身就像是一辆到处是小毛病的老汽车,基础疾病那叫一个多。
他有多年的高血压,就像身体里藏着一个随时可能爆发的小火山,血压老是在“蹦迪”,高的时候能冲到[具体血压值]。
还有冠心病,心脏就像一个老化的发动机,时不时地闹点小脾气,供血不太顺畅。
老张这次因为要做一个[具体手术名称]手术被推进了我们麻醉科的地盘。
术前检查那一堆结果,就像天书一样让人头疼,但又得仔仔细细去解读。
他的心电图显示[描述心电图异常情况],心脏功能评估下来也不太乐观,EF值(射血分数)只有[具体数值],就好像这个心脏发动机的动力严重不足。
二、麻醉方案选择的纠结。
1. 最初考虑。
椎管内麻醉呢,就像是局部给身体某个区域来点“小麻痹”,听起来对心肺功能影响小一些。
可是老张的脊柱情况又有点复杂,之前有过[描述脊柱相关情况],而且这个手术的范围还不小,如果椎管内麻醉效果不完全,那手术做到一半患者疼得嗷嗷叫可就麻烦了。
2. 权衡利弊。
我们围在一起讨论得热火朝天。
李医生说:“全身麻醉的话,我们可以更好地控制呼吸和循环,就像给老张的身体安上一个辅助驾驶系统。
但是得小心那些麻醉药物对他脆弱的心脏和血压的打击。
”王医生则皱着眉头反驳:“椎管内麻醉虽然理论上对心肺干扰小,可这不确定性太大了。
要是效果不好,手术台上的老张可就遭罪了,而且万一出现神经损伤啥的,那可就是雪上加霜。
”最后呢,经过我们反复权衡,就像在天平的两端不断加砝码。
我们决定采用一种折中的方案,那就是在全身麻醉的基础上,辅助一些局部麻醉的手段。
就好比给老张的身体上了双重保险,既能保证他在手术中舒舒服服地“睡过去”,又能减少全身麻醉药物的用量,减轻对他心肺功能的负担。
三、麻醉过程中的惊险瞬间。
1. 诱导期。
当我们开始麻醉诱导的时候,就像走在钢丝上一样小心翼翼。
先给老张注射了[具体诱导药物名称],刚一推药,就像触动了身体里的某个敏感开关。
麻醉科疑难危重病例讨论范文英文回答:Critical Case Discussion in Anesthesiology.Today, we are going to discuss a critical case in anesthesiology. The patient is a 65-year-old male who presented with severe respiratory distress and hypotension after a routine surgical procedure. The patient has a history of chronic obstructive pulmonary disease (COPD) and hypertension. The surgical procedure was uneventful, and the patient was stable throughout the surgery. However, shortly after extubation, the patient developed acute respiratory distress and hypotension.Upon initial assessment, the patient was found to be tachypneic with shallow breathing and hypoxemia. Thepatient's blood pressure was also significantly low. The initial management included providing supplemental oxygen, initiating fluid resuscitation, and administeringvasopressors to support the blood pressure. The patient was also re-intubated for respiratory support.Further investigation revealed that the patient had developed acute respiratory distress syndrome (ARDS) and septic shock. Blood cultures were obtained, and broad-spectrum antibiotics were initiated. The patient was transferred to the intensive care unit for close monitoring and continued supportive care.As a team, we need to discuss the possible causes of the patient's deteriorating condition and come up with a comprehensive treatment plan. We also need to consider the challenges of managing a patient with pre-existing comorbidities such as COPD and hypertension.This case highlights the importance of prompt recognition and management of postoperative complications, especially in patients with underlying medical conditions. It also emphasizes the need for effective communication and teamwork in addressing critical cases in anesthesiology.中文回答:麻醉科疑难危重病例讨论。


麻醉科病例讨论xx年xx月xx日•病例介绍•临床诊断与辅助检查•治疗方案与实施目录•治疗效果评估与反思•相关并发症及防治•总结与展望01病例介绍1病例选择标准23选择的病例应具有代表性和典型性,能够反映常见麻醉问题或特殊状况。
典型性病例的复杂性可以锻炼医生的分析和处理能力,包括并发症的处理。
复杂性应选择适合各层次麻醉医生培训需求的病例,如针对初级医生的简单病例或针对高级医生的复杂病例。
培训需求病例基本信息02手术类型、手术时间、麻醉时间等手术相关资料。
03患者既往病史、家族史、过敏史等健康状况。
病例病情简介患者入院原因及诊断。
术中生命体征及重要事件记录,如失血量、尿量、心电图等。
术前评估及准备情况,如实验室检查、影像学检查、特殊用药等。
麻醉诱导、维持和苏醒过程简要描述。
02临床诊断与辅助检查要详细了解患者的病史、症状和体征,包括疼痛部位、性质、程度、持续时间等,以及伴随症状和体征。
临床表现根据患者的临床表现,初步确定疼痛的病因和类型,同时进行必要的鉴别诊断,排除非麻醉科疾病所致的疼痛。
诊断思路临床表现与诊断思路03电生理检查如肌电图、神经传导速度等,有助于了解神经功能状态及损伤情况。
辅助检查的方法及其意义01实验室检查包括血常规、尿常规、生化全项、心电图等,可帮助了解患者的全身情况和重要脏器的功能状态。
02X线、CT和MRI等影像学检查有助于发现疼痛部位及病因,如骨折、结核、肿瘤等。
根据检查结果,综合分析患者的病情和病因,评估手术风险及麻醉耐受能力。
根据检查结果确定最佳的麻醉方案和疼痛治疗方法,同时预测治疗的效果及可能的不良反应。
检查结果及其分析03治疗方案与实施治疗方案的选择原则治疗方案应以保证患者安全为前提,风险与收益比值低。
安全性原则有效性原则适用性原则经济性原则治疗方案应能够有效缓解患者的症状和体征,达到预期的治疗效果。
治疗方案应充分考虑患者的身体状况、病情、治疗需求等因素,适用的才是最好的。
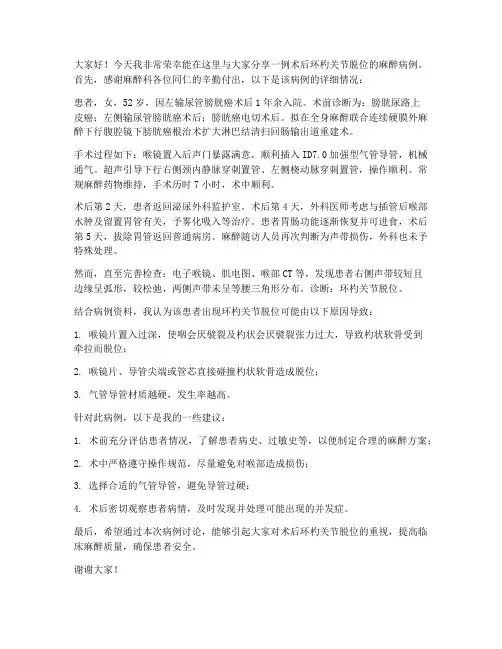
大家好!今天我非常荣幸能在这里与大家分享一例术后环杓关节脱位的麻醉病例。
首先,感谢麻醉科各位同仁的辛勤付出,以下是该病例的详细情况:患者,女,52岁,因左输尿管膀胱癌术后1年余入院。
术前诊断为:膀胱尿路上皮癌;左侧输尿管膀胱癌术后;膀胱癌电切术后。
拟在全身麻醉联合连续硬膜外麻醉下行腹腔镜下膀胱癌根治术扩大淋巴结清扫回肠输出道重建术。
手术过程如下:喉镜置入后声门暴露满意,顺利插入ID7.0加强型气管导管,机械通气。
超声引导下行右侧颈内静脉穿刺置管、左侧桡动脉穿刺置管,操作顺利。
常规麻醉药物维持,手术历时7小时,术中顺利。
术后第2天,患者返回泌尿外科监护室。
术后第4天,外科医师考虑与插管后喉部水肿及留置胃管有关,予雾化吸入等治疗。
患者胃肠功能逐渐恢复并可进食,术后第5天,拔除胃管返回普通病房。
麻醉随访人员再次判断为声带损伤,外科也未予特殊处理。
然而,直至完善检查:电子喉镜、肌电图、喉部CT等,发现患者右侧声带较短且边缘呈弧形,较松弛,两侧声带未呈等腰三角形分布。
诊断:环杓关节脱位。
结合病例资料,我认为该患者出现环杓关节脱位可能由以下原因导致:1. 喉镜片置入过深,使咽会厌襞裂及杓状会厌襞裂张力过大,导致杓状软骨受到牵拉而脱位;2. 喉镜片、导管尖端或管芯直接碰撞杓状软骨造成脱位;3. 气管导管材质越硬,发生率越高。
针对此病例,以下是我的一些建议:1. 术前充分评估患者情况,了解患者病史、过敏史等,以便制定合理的麻醉方案;2. 术中严格遵守操作规范,尽量避免对喉部造成损伤;3. 选择合适的气管导管,避免导管过硬;4. 术后密切观察患者病情,及时发现并处理可能出现的并发症。
最后,希望通过本次病例讨论,能够引起大家对术后环杓关节脱位的重视,提高临床麻醉质量,确保患者安全。
谢谢大家!。
麻醉科死亡病例讨论范文English: The discussion of death cases in anesthesiology is vital for gaining insights and understanding the potential risks and challenges associated with this medical specialty. One such case involved a 45-year-old male patient undergoing a routine procedure under general anesthesia. Despite the presence of an experienced anesthesiologist, the patient developed sudden cardiovascular collapse and failed resuscitation attempts resulted in his unfortunate demise. This case highlights the importance of vigilance and continuous monitoring during anesthesia, as well as the need for prompt recognition and management of potential complications. In retrospect, potential causes of this incident could include an undiagnosed underlying cardiovascular condition or an adverse drug reaction. To minimize the risk of similar events, it is crucial for anesthesiologists to perform thorough preoperative evaluations, conduct appropriate risk stratification, and develop individualized anesthetic plans. Close communication and collaboration with the surgical team, prompt recognition and management of perioperative changes, adequate monitoring, and adherence to safety protocols are vital in preventing and responding to complications duringanesthesia. Regular training and simulation exercises, as well as maintaining up-to-date knowledge about advancements in anesthetic techniques and medications, are essential for anesthesiologists to enhance patient safety and ensure optimal outcomes. This case underscores the need for ongoing education, quality improvement initiatives, and stringent guidelines in the field of anesthesiology to mitigate the risks and minimize adverse events that can occur during anesthesia.中文翻译: 麻醉科中死亡病例的讨论对于获取见解和理解这个医学专业的潜在风险和挑战至关重要。
第1篇尊敬的各位专家、同仁:大家好!今天,我很荣幸能在这里代表我们团队,就近期一例复杂病例的讨论进行总结发言。
首先,请允许我简要回顾一下病例的基本情况。
病例回顾:患者,男性,58岁,主诉为“反复发作性胸痛3个月”。
患者3个月前开始出现胸痛,呈压迫性,位于胸骨后,伴有心悸、出汗,休息后可缓解。
症状时轻时重,近1个月来症状加重,夜间发作频繁。
既往有高血压病史,否认糖尿病、冠心病、心绞痛等病史。
体格检查:血压160/95mmHg,心率88次/分,律齐,各瓣膜听诊区未闻及明显杂音。
心电图检查提示ST-T改变,心肌酶谱正常。
病例讨论:在本次病例讨论中,我们针对患者的症状、体征、辅助检查等方面进行了深入的探讨。
以下是讨论的主要内容:1. 症状分析患者的主要症状为胸痛,呈压迫性,位于胸骨后,伴有心悸、出汗。
结合患者的年龄、高血压病史,首先考虑冠心病、心绞痛等心血管疾病。
但患者心电图检查提示ST-T改变,心肌酶谱正常,不支持急性冠脉综合征的诊断。
2. 体征分析患者血压160/95mmHg,心率88次/分,律齐。
心脏听诊未闻及明显杂音。
考虑到患者高血压病史,应进一步排除其他心脏疾病,如心肌病、心脏瓣膜病等。
3. 辅助检查分析心电图检查提示ST-T改变,考虑为心肌缺血。
但心肌酶谱正常,不支持急性冠脉综合征的诊断。
此外,患者血压控制不佳,应排除高血压性心脏病。
4. 诊断与鉴别诊断结合患者的症状、体征、辅助检查,首先考虑以下诊断:(1)冠心病、心绞痛:患者有高血压病史,胸痛症状符合冠心病、心绞痛的特点,但心电图和心肌酶谱不支持急性冠脉综合征的诊断。
(2)高血压性心脏病:患者血压控制不佳,应排除高血压性心脏病。
(3)心肌病:患者心电图提示ST-T改变,需排除心肌病。
(4)心脏瓣膜病:患者心脏听诊未闻及明显杂音,但需排除心脏瓣膜病。
5. 治疗方案针对患者的病情,我们制定了以下治疗方案:(1)控制血压:给予患者降压药物,控制血压在目标范围内。
2009 年中华麻醉年会投稿作者姓名:童传耀, 医学博士(Name in English: Chuanyao Tong, MD.)工作单位:美国威克大学麻醉科Dept. of AnesthesiologyWake Forest University Health ScienceMedical Center Blvd,Winston-Salem, NC 27157, USA邮编: 2715719107 USA (美国)美国联系电话: (336) 716-4498电子邮件地址: cyt970@论文标题:围术期严重肺栓塞的诊断和抢救治疗Intraoperative massive pulmonary embolism-diagnosis and resuscitation论文分类:临床麻醉病例讨论(PBLD-problem based clinical discussion)Intraoperative massive pulmonary embolism: diagnosis and resuscitationChuanyao Tong, MD, Dept. of Anesthesiology, Wake Forest University Health Science, Winston-Salem, NC 27157, USAObjective:After attending this case, the participants will be able to:1. Understand the circulatory changes associated with intraoperative acute massive pulmonary embolism.2. Learn the diagnosis modalities for intraoperative pulmonary embolism.3. Understand the optimal hemodynamic management, the vasopressors and fluids to maximize the survival possibility.4. Discuss other treatment options and prevention strategy.Stem Case:A 77 years old white female fell 3 days ago and was scheduled for left humeral open reduction and internal fixation (ORIF) and left hip replacement.PMH: hypertension, type 2 diabetes, hyperlipidemia, hypothyroidism.SH: living with dementia husband, active and golfing regularly. Nonsmoker.PE (in ER): BP126/63, HR67, RR22, T95.3, SaO298% in room air.X-ray remarks: 1) complex humeral head and neck fracture with anterior displacement, and 2) mild displaced left femoral neck fracture.Labs: HH 13.4/38.9, Platelet 309; electrolytes were normal, Glucose 194. EKG: SR 80, borderline LAD (left axis deviation). Stress echocardiogram was negative in 1997.Disposition: the patient was admitted to orthopedic floor, continuing her chronic medications, and heparin 5000 u was started, sc bid.On the day of surgery, a left interscalene brachial plexus catheter and a lumbar plexus block were performed with total of 0.5% bupivacaine 55 ml for postoperative analgesia. General anesthesia was induced by iv propofol (100 mg), fentanyl (150 mcg), and rocuronium (50 mg). The patient’s intubation (7.0 ETT) was confirmed by ETCO2 and equal bilateral breath sounds, and maintained with 0.5% isoflurane in O2/air. Shortly after induction, her blood pressure was trending down to 80/45 mmHg, no changes in heart rate and SaO2, which responded to ephedrine (10 mg) and phenylephrine (120 mcg), then iv hetastarch 500 ml was started.•Is this common in elderly patient?•What could be the differential diagnosis?As planned preoperatively, a 2nd iv and a radial arterial line were placed, the patient was moved from stretcher to OR table, turned to right lateral position (20 min later). Arterial BP was again decreased to 75/40 mmHg with HR 95. This time, it did not respond to ephedrine (35 mg) and phenylephrine (600 mcg). The resident was watching the vital signs, noticed SaO2 was 80% with an ill looking ETCO2 waveform (22-27 mmHg). Immediately gave epinephrine (100 mcg, iv) and started hand bagging with 100% O2…•What would be the differential diagnosis again?•Which therapy should be initiated?Breath sounds and ETT position were re-checked, a chest x-ray ordered immediately, and TEE called. Meanwhile, the patient was turned to a supine position and started neophenylephrine and epinephrineinfusion, with both iv fluids wide open. MAP was kept >60 mmHg so as SaO2>90%, but no improvement of ETCO2 waveform.•What would be the findings from TEE?TEE showed a significant dilated right atrium and ventricle with decreased contractility (sluggish or hypokinesia), a rather small LV chamber with good contractility (EF 55%), and deviated sepetal wall towards left, moderate to severe tricuspid regurgitation and evident a frail mitral valve prolapsed. Surprisingly, a patent PFO with left to right shunting was found. There was an estimated pulmonary hypertension (~55 mmHg), but no visible clot.•Do you consider the TEE findings supportive for the diagnosis of PE?•Was this also possible of acute right heart infarction?•If TEE were not available, how could ABG, CXR, EKG, PAC, and CVP help for diagnosis?In next 75 min of continuing resuscitation, the patient’s condition was relatively stabilized, withPaO2>110 mmHg and MAP in range of 70-85 mmHg. Troponin was negative in 2 measurements. EKG later showed junctional tachyarrhythmia (110/min), low voltage QRS (suggesting new pulmonary disease), and new abnormality of nonspecific ST and T changes. At this point, a diagnosis of pulmonary embolism (PE) was made, the original surgery was canceled and the patient was transported to ICU for continue resuscitation and treatments...Discussion:1.Risk factors for PE and the differential diagnosis for hypoxia: Bone fracture and bed resting is the most common cause of deep venous thrombosis (DVT) formation in the low extremities, which has a potential risk of PE when the clot dislodged. The differential diagnosis includes fat embolism syndrome (FES) which is manifested by continues release fatty tissue causing pulmonary vasculature inflammatory responses. Others included pneumothorax, tension pneumothorax from multi-rib fracture or interscalene block, pulmonary contusion, endobronchial intubation, anaphylactic reaction to drugs or latex. All of these could cause sudden unstable hemodynamic and hypoxia, and should be rapidly ruled out for effective management.2.The value of TEE in diagnosis and treatment of PE: a massive PE causes the right ventricle outflow obstruction by its mass and/or inflammatory reaction, results in severe decrease of preload and afterload (hypotension and left heart failure), severe pulmonary hypertension and right ventricle failure, and compromising coronary perfusion; these changes could be instantly characteristically revealed by TEE as dilated right ventricle with impaired contractility and small left chamber volume with preserved function initially. In addition, it may show some unknown preexisting cardiac anomaly, as the finding of a patent PFO with right to left shunt in this patient. The presence of visible clot in the pulmonary arterial confirms the PE diagnosis immediately. TEE is helpful in guiding resuscitation and providing immediately feedbacks concerning the treatments.3.ACLS (Advance Cardiac Life Support) for managing cardiovascular collapse: When encountered such a scenario, the first is checking the airway to ensure a patent airway (intubation and ventilation with 100% oxygen). The administration of inotropics and volume are aimed to rapidly restore the patient’s cardiovascular function. Two-thirds of the mortality following massive PE occurs within one hour of the onset of hemodynamic instability. Generally, there is no rule regarding the dose range (mcg to mg), drug choice (ephedrine, phenylephrine, epinephrine, or norepinephrine), rather how faster and effectively bring the MAP back to baseline. There is no evidence of the value of steroid (dexamethasone). CPR should be initiated if no response to inotropics in 3-5 min or the presence of PEA (puleless electrical activity). Defibrillation should be delivered immediately if presence of ventricle tachycardia or fibrillation.4.Prevention and treatment options: the stabilization and fixation of long bone fractures should take place within 72 hrs, the patient should be resuming ambulation early, starting anticoagulation(subcutaneous heparin or lovenox), placing low extremity compression cuff or/and the inferior vena cava filter; all these measures have been shown some effectiveness in decreasing DVT. The definitive emergency treatment is aimed to remove the clot and restore the cardiovascular stability. Medically, thrombolytic therapy is started with administration of thromboplastin activator (tPA) in adjunction with heparinization. Surgically, embolectomy is achieved by extracting the clot through thoracotomy or interventional radiological procedures. Numerous reports showed an immediate ECMO (extracorporeal membrane oxygenation) could be life saving and create an opportunity for definitive therapy. REFERENCES:1.Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the GoldenHour of hemodynamically significant pulmonary embolism. Chest 2002;877-905.2.Rosenberger P, Shernan SK, Shekar PS, et al: Acute hemodynamic collapse after induction ofgeneral anesthesia for emergent pulmonary embolectomy. Anesth Analg 2006;102:1311-5.3.Goldhaber SZ. Pulmonary embolism. N Engl J Med 1998;339:93-104.4.Memtsoudis SG, Rosenberger P, Loffler M, et al: The usefulness of transesophagealechocardiography during intraoperative cardiac arrest in noncardiac surgery. Anesth Analg2006;102:1653-7.5.Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism of the European Society ofCardiology (ESC). Eur Heart J. 2008; 29 (18):2276-315.6.Stein PD, Yaekoub AY, Matta F, Kleerekoper M: Fat embolism syndrome. Am J Med Sci. 2008;336(6): 472-7.7.Barrett JA, Baron JA, Beach ML: Mortality and pulmonary embolism after fracture in the elderly.Osteoporos Int. 2003; 14(11):889-94.8.Konstantinides S: Clinical practice. Acute pulmonary embolism. NEJM 2008; 359(26):2804-13.fere TB, Sprung J, Case KA, et al: Predicators of mortality following symptomaticpulmonary embolism in patients undergoing noncardiac surgery. Can J Anaesth 2007; 54(8):634-41.2009 年中华麻醉年会投稿作者姓名:夏云, 医学博士,哲学博士(Name in English: Yun Xia, MD, PhD)工作单位:美国俄亥俄州立大学医学中心Dept. of AnesthesiologyOhio State University Medical CenterN-416 Doan Hall410 West Tenth AvenueColumbus, Ohio 43210-1228, USA邮编: 43210-1228 USA (美国)(美国)联系电话:(614) 766-4048电子邮件地址:yun.xia@论文标题:子痫前期产妇的麻醉管理Anesthetic Considerations of a Parturient with Multiple Co-existing Diseases论文分类:临床麻醉病例讨论(PBLD-problem based clinical discussion)Anesthetic Considerations of a Parturient with Multiple Co-existing DiseasesYun Xia, MD, PhD, Ohio State University Medical Center, Columbus, Ohio OBJECTIVESAt the conclusion of this PBLD session, the participants will be able to:1. Know current classification, pathophysiology, diagnosis, and anesthetic consideration of preeclampsia2. Describe anesthetic managements of preeclampsia in an evidence based approach.3. Learn the managements of labor analgesia and Cesarean section in the US.4. Prepare for parturients with multiple co-existing diseases.STEM CASE - KEY QUESTIONSThe patient was a 34 year-old Caucasian female, G2, P0010, 34 weeks gestation, premature rapture of membrane (PROM). She had a VAS score of 4/10 during regular uterine contractions at 3-4 minutes apart. She was admitted for preterm labor. Fetal heart rate (FHT) was 140’s/minute with good variability.She presented complaints of elevated blood pressure (BP) and shortness of breath over the last month. She received corticosteroids a week ago. Her platelet account was105,000 at her last office visit, two weeks ago.Her past medical history was also remarkable with hypertension (HTN), retinopathy, hypercholesterolemia, diabetes mellitus type I (DMI) class H, hypothyroidism, gatroesophageal reflux disease, and smoking. She was diagnosed with antithrombin III deficiency due to an episode of deep venous thrombosis (DVT) at 19 weeks gestation. She has been placed on lovenox (enoxaparin) 60 mg SQ bid since then and her last injection was 24 hours ago. Four years earlier, she experienced a myocardial infarction (MI) with subsequent placement of a single sirolimus-elutung stent (SES) (Cypher TM Cordis) in the proximal left anterior descending coronary artery that was 70% stenosed. On physical examination, she was noted to be a morbid obese patient (Wt. 93.6 kg, Ht. 152 cm, BMI 40.5) with an admission BP 191/107 mmHg. The patient was having increased swelling in her upper and lower extremities; Airway: Malampatti II. Admission medication included levothyroxine, famotidine, and insulin via a Paradigm 7000 series indwelling pump (Medronic). She had been taking clopridogrel 75 mg and aspirin 81 mg for 1 year post placement of the SES.Significant initial laboratory results were a platelet 107,000, Hgb A1c 6.7%, glucose 246 mg/dL, and three plus proteinuria. Cardiac enzymes were negatives times three. Electrocardiogram was normal. Echocardiogram showed a normal left ventricle (LV) systolic function, LV ejection fraction (EF) 65%, normal wall motion, and a mild mitral regurgitation.Initial treatments included: intravenous (IV) labetalol, hydralazine, and magnesium infusion.Her BP was reduced and maintained at150s/90s mmHg. HR 84/min, RR 18/min, Hct 35%. Cervix dilation was 2 cm.1. What is the classification of Hypertensive Disorders in Pregnancy?2. Did this patient have preeclampsia (diagnosis)?3. What is the clinical significance of DM class H?4. What are the anesthetic considerations of this patient?5. What are the factors that contribute to an increased risk of epidural hematoma?6. What other information would you need to formulate your anesthetic plan?7. Can regional techniques be used for this patient’s labor analgesia? If so, when?After discussion among obstetricians, anesthesiologists, and pediatricians, epidural labor analgesia was chosen. After oral administration of sodium citrate, an epidural catheter with a flexible-tip was placed at L3-4 with no noticeable problems. After a negative testing dose, 0.125% bupivacaine 10 mL was given to the patient in three separate doses. Continuous infusion of 0.0625% of bupivacaine and fentanyl 4 mcg/ml was started at 10 mL/hour with a PCEA (dose 5 mL, delay 20 minutes, and lockout 25mL/hour). The patient had a sensory blockage of T10 level and was comfortable in bed and had minimal motor block. Oxytocin was started on the recommendations of obstetricians.7. How would you monitor this patient for the signs and symptoms of epidural hematoma?8. When can the anticoagulation therapy be re-started?Nine hours later, obstetricians noticed a fetal bradycardia which was determined as late decelerations. Despite left uterine displacement, oxygen administration, and stopping oxytocin infusion, the fetal bradycardia during each contraction progressively worsened, so a stat C-section was called.9. What is late deceleration?10. What is your anesthetic plan?After negative aspiration of epidural catheter, a five mL of 1.5% lidocaine was injected via epidural catheter. The patient immediately complained that she could not move both of her legs and she had difficulty of breathing.11. What was happening?12. What is your anesthetic plan now?13. What is the incidence of epidural catheter migration?After oral sodium citrate, intravenous (IV) pepcid (famotidine), and reglan (metoclopramide), general anesthesia was induced and endotracheal intubation wasperformed with cricoid pressure. The patient was hemodynamically stable. A vigorous baby with apgar scores of 9 (1minute) and 9 (5 minute) was delivered 2 minutes after skin incision. Oxytocin IV drip was used to manage uterine tone and estimated total blood loss was 700 mL. At the end of the surgery, epidural catheter aspiration was positive with CSF. Post-operatively, the patient remained hemodynamically stable throughout her hospitalization without any cardiac or neurological issues.14. What could be done to manage her post-operative pain?P ROBLEM B ASED L EARNING D ISCUSSIONThis patient posed a great challenge to our anesthesiologists for her anesthetic management during her labor and delivery. She not only had preeclampsia, but also significant other co-existing diseases, namely, chronic HTN, retinopathy, hypercholesterolemia, diabetes mellitus type I class H, hypothyroidism, gatroesophergeal reflux disease, coagulopathy, CAD, and a history of smoking.Preeclampsia occurs in the United States about 2.3-7.6%, on average about 5%, of all pregnancies. The incidence of preeclampsia is 23.6 cases per 1,000 deliveries in the United States. The global incidence of preeclampsia has been estimated at 5-14% of all pregnancies. Preeclampsia is the third leading pregnancy-related cause of death, after hemorrhage and embolism. Preeclampsia is the cause of an estimated 790 maternal deaths per 100,000 live births.Parturients with hypertensive disorders can be classified into the following four categories: (1) gestational hypertension; (2) chronic hypertension; (3) preeclampsia; and (4) chronic hypertension with superimposed preeclampsia.The etiology of preeclampsia is unknown. The hypotheses associated with the etiology are: (1) abnormal trophoblast invasion; (2) vascular endothelial damage; (3) immunologic abnormality; (4) genetic predisposition; and (5) dietary irregularity. Some authors believe that coagulation abnormalities and cardiovascular maladaptation may also play roles in preeclampsia.Morbidity and mortality are related to systemic endothelial dysfunction; vasospasm and small-vessel thrombosis leading to tissue and organ ischemia; CNS events such as seizures, strokes, and hemorrhage; acute tubular necrosis; coagulopathies; and placental abruption in the mother. In the fetus, ischemic encephalopathy, growth retardation, and the various sequelae of premature birth can occur.Current criteria for diagnosis of preeclampsia include hypertension and proteinuria. There are two subtypes of preeclampsia: mild preeclampsia (BP>140/90 and proteinuria > 300 mg/24 hours) and severe preeclampsia (BP>160/110 and proteinuria > 2 g/24 hours).Delivery is still believed to be the cure for preeclampsia. However, early prenatal detection, fetal and maternal surveillance, necessary hospitalization, antihypertension therapy, seizure prevention and treatment, and proper peripartum managements are also important for the treatment of preeclampsia.We believe that knowing the pathophysiological changes in preeclampsia and knowing the nature and severity of preeclampsia in each patient will enable us to formulate the optimal anesthetic plan for our patients with preeclampsia. If there is no contraindication, regional analgesia has many advantages to offer and has the potential to be the superior choice for labor analgesia and obstetric anesthesia. However, general anesthesia provides the shortest time from induction of anesthesia to fetus delivery. Therefore, in certain situations, general anesthesia can be life-saving for parturients and their babies. We will discuss these in detail during our PBLD.Through evidence-based approaches, we hope this discussion will help our participants to (1) achieve knowledge of current classification, pathophysiology, diagnosis, and anesthetic consideration of preeclampsia; (2) achieve the ability to describe anesthetic managements of preeclampsia; (3) learn the management of labor analgesia and Cesarean section in the US; and (4) prepare for paturients with multiple co-existing diseases.R EFERENCES[1] ACOG Practice Bulletin. Clinical Management Guidelines for Obstetrician-Gynecologists. Number 33, January 2002. (In: 2007Compendium, Volume II: pp 640-648. 2007). 2002.[2] Ananth CV, et al. Trends in preterm birth and perinatal mortality among singletons: United States, 1989 through 2000. ObstetGynecol. 105: 1084-1091. 2005.[3] Aya AGM, et al. Patients with severe preeclampsia experience less hypotension during spinal anesthesia for elective cesareandelivery than healthy parturients: a prospective cohort comparison. Anesth Analg. 97:867-872. 2003.[4] Sibai BM. Hypertension. In: Obstetrics: Normal and Problem Pregnancies (Eds. Gabbe S., et al). pp 863-912. 2007[5] Cunningham FG, et al. Hypertensive disorders in pregnancy. In: Williams Obstetrics (22th Edition). McGraw-Hill. pp759-808.2005.[6] Fischer T et al. Vascular reactivity in patients with preeclampsia and HELLP syndrome. Am J Obstet Gynecol 183: 1489-1494.2000.[7] Gambling DR. Hypertensive disorders. In: Obstetric Anesthesia 3rd edition (Chestnut DH ed). pp794-845. 2004.[8] Matchaba P and Moodley J. Corticosteroids for HELLP syndrome in pregnancy. Cochrane Database Syst Rev CD002076. 2004[9] Villar J, et al. Heterogeneity of perinatal outcomes in the preterm delivery syndrome. Obstet Gynecol. 104: 78-87. 2004.[10] Wang Y, et al. Evidence of endothelial dysfunction in preeclampsia. Am J Obstet Gynecol. 190: 817. 2004[11] Xia Y. Progress in Preeclampsia. Chinese Journal of Practical Gynecology and Obstetrics. 23 (7): 573-574. 2007.2009 年中华麻醉年会投稿作者姓名: 刘虹, 医学博士(Name in English: Hong Liu, M.D.)工作单位: 美国, 加利福尼亚州, 萨克拉门托市, 加州大学戴维斯分校 University of California Davis Health System4150 V Street, Suite 1200Sacramento, CA 95817, USA联系地址: 5424 Cowell Blvd.Davis, CA 95618, USA邮编: 95618 USA (美国)联系电话: (530)-848-5895电子邮件地址:hualiu@论文标题: 术中液体评估和管理的新概念论文分类:临床麻醉病例讨论(PBLD-problem based learning discussion)Intra-operative Volume AssessmentHong Liu, MD, Associate Professor, Department of Anesthesiology and Pain Medicine University of California Health System, Sacramento, California, USAObjectives:At the conclusion of this session the participant will have a better understanding the new concept of patient intraoperative fluid assessment and management.Stem Case:Patient details:64 years old, female, height: 162cm, weight: 65kg, 40 pack/year smoking history. Medical history:Hypertension, type II diabetics, peripheral vascular disease (PVD), hypercholesteremia, hypothyroidismCase Notes:The patient was scheduled for an exploratory laparotomy and Whipple procedure. Her medical history is significant for hypertension, PVD, hypercholesteremia, diabetics, and hypothyroidism. Her electrocardiogram showed some non-specific ST-T depression. Pre-operative stress echocardiography showed a left ventricular ejection fraction between 50 to 55%.Patient was taken to the operating room at 3:00 pm. One 18G intravenous (IV) catheter was placed in the left hand. Thoracic epidural catheter was placed prior to induction of general anesthesia. General anesthesia was induced with 2 mg of versed, 140 mg of propofol, and 70 mg of rocuronium. After induction, endotracheal tube was placed and verified for correct positioning.You are her anesthesiologist.1. How do you estimate her fluid deficit?2. How are you going to monitor her fluid status?3. What kind of monitor are you going to use?4. With patient’s past medical history, any special monitor you going to use? The surgeon suggested for a central line placement.5. What is your response to the surgeon’s request?6. What evidence are you going to use to backup your argument?7. Is an arterial line indicated in this case?8. Is a Vigileo/FloTrac system indicated in this case?Because of her PVD status, a central venous pressure (CVP) catheter was placed for IV access and an intra-arterial catheter with a Vigileo/FloTrac system was used for cardiac output (CO), SVV, and continues blood pressure (Bp) monitoring. Patient’s heart rate (HR) was 82/min, Bp was 128/72 mmHg, CVP: 10 cmH20,CO: 5.3 L/min and SVV: 10%.9. What are the numbers tell you?10. What is the normal range SVV?After the general anesthesia and at the early stage of surgery the patient’s SVV and CO was very stable throughout this period. Fifty minutes into surgery, the surgeon encountered some bleeding and the anesthesiologist noticed that about 500 ml of blood were lost. At the same time the SVV was increased from 11% to 41% and CO decreased from 4.6 to 3.2 L/min. The patient’s HR increased to 105/min, CVP 8 mmHg and an acute decrease in BP (90/50 mmHg).11. What is this SVV number telling you?12. What do you think of the CO?13. Are there connections between SVV and APCO?After immediate transfusion of 500 ml of colloid solution the patient’s HR went to 85/min, CVP: 10 mmHg, BP: 120/70 mmHg, the SVV to 13%, CO: 5.2 L/min. Due to the location of the tumor, it was difficult to control the bleeding. In order to completely control the bleeding, the surgeon decided to resect the tumor first. During next 10 minutes while the surgeon was resecting the tumor, the anesthesiologist was replacing the blood volume with packed red blood cell and colloid solution. The SVV was again increased and CO decreased during this time. After the bleeding was controlled, the SVV and CO went back to the baseline. The rest of the surgical procedure and hospital cause was uneventful. The patient was discharged home 6 days after surgery.14. Which is more sensitive to blood loss, SVV or CVP?15. Do you think SVV is a good indicator for circulatory volume status in yourdaily practice?16. What are the indications for the use of SVV/APCO?Discussion:Hemodynamic monitoring and fluid status assessment are essential for cardiovascular care in the patient undergoing major surgeries. Knowing when a patient’s hemodynamic instability comes from hypovolemia or other causes is imperative in providing a safe patient care. Adequate volume replacement to achieve optimal cardiac performance is a primary goal of hemodynamic management in those patients. However, in only half of such patients the CO increases after a fluid challenge and thus only these can be considered as responders to fluid therapy. Therefore, physicians need reliable criteria to distinguish those two patient populations to avoid any deleterious consequences of fluid overload.There are several parameters the clinicians use to guide fluid management in their everyday patient care. CVP and pulmonary artery pressure (PAP) are most commonly used in major hemodynamic instability cases. However, these standard preload index(CVP, PAP) values nor their changes in response to fluid challenges reflected their respective ventricular end diastolic volumes or changes in patients receiving a fluid challenge for hemodynamic instability, and are not capable of predicting cardiac response to fluid therapy. Therefore, they could not serve as the standards for the patient’s volume status.Believe or not, we still use formula to calculate the fluid need simply based on patient’s weight, the length of NPO, types and length of surgery to guide intra-operative fluid management. Let’s use this case as an example. The deficient from NPO overnight for 10 hrs: 1050 ml; maintenance for 4.5 hour surgery: 8 ml /kg/hr for 3rd spacing: 2340 ml; insensitive loss for 4.5 hours: 2ml/kg/hr: 585 ml; blood loss: 600 ml and you can give colloid or blood 1:1 ratio or you can use crystalloid at 1:3 ratio. The total amount of fluid the patient would receive during 4.5 hours of surgery could be about 6000 ml.The accuracy of about preload index and the method of calculation have been challenged in recent years. Studies have shown that they do not accurately reflect the left ventricular end diastolic area and volume values, even when trends are followed after the administration of a fluid challenge during hemodynamic instability. As the minimal invasive technology becoming more mature, stroke volume (SV), SVV or pulse pressure variation (PVV) in conjunction with APCO have been used more and more in recent years by clinicians to guide intra-operative fluid therapy. We hope the goal-directed intraoperative fluid management by using SVV/PVV or other parameters will replace the old methods and be the choice to guide fluid therapy in hemodynamic instable patients. References1.Kumar A, Anel R, Bunnell E, Habet K, Zanotti S, Marshall S, Neumann A, Ali A,Cheang M, Kavinsky C, Parrillo JE. Pulmonary artery occlusion pressure andcentral venous pressure fail to predict ventricular filling volume, cardiacperformance, or the response to volume infusion in normal subjects. Crit. CareMed. 2004;32: 691-992.Hamilton-Davies C, Mythen MG, Salmon JB, Jacobson D, Shukla A, Webb AR.Comparison of commonly used clinical indicators of hypovolaemia withgastrointestinal tonometry. Intensive Care Med. 1997 Mar;23(3):276-813.Bouchard MJ, Denault A, Couture P, Guertin MC, Babin D, Ouellet P, Carrier M,Tardif JC. Poor correlation between hemodynamic and echocardiographic indexes of left ventricular performance in the operating room and intensive care unit. .Crit. Care Med. 2004;32: 644-484.Michard F. Changes in Arterial Pressure during Mechanical Ventilation.Anesthesiology 2005;103: 419-285.Reuter DA, Bayerlein J, Goepfert MS, Weis FC, Kilger E, Lamm P, Goetz AE.Influence of tidal volume on left ventricular stroke volume variation measured by pulse contour analysis in mechanically ventilated patients. Intensive Care Med.2003 Mar;29(3):476-80。