子宫原发弥漫大B细胞淋巴瘤1例
- 格式:pdf
- 大小:2.17 MB
- 文档页数:2
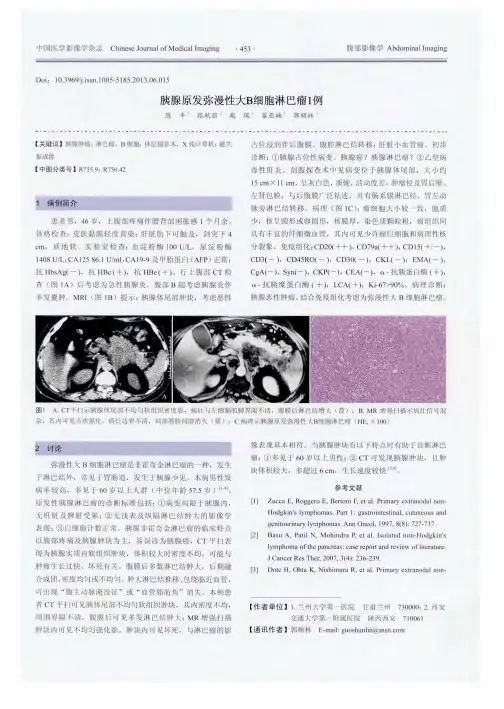
150Chin J Lab Diagn,January ,2021,Vol 25,No. 1ised controlled trial[J]. Eur J Anaesthesiol,2018»35( 10) :766.[3〇]Meng L,Li L,Lu S»et al. The protective effect of dexmedetomi- dine on LPS-induced acute lung injury through the HMGBl-me- diated TLR4/NF-kB and PI3K/Akt/mTOR pathways[J]. Mol Immunol,2018,94 :7.[31] Lee SH,Kim N,Lee CY,et al. Effects of dexmedetomidine on oxygenation and lung mechanics in patients with moderate chro-gery: A randomised double-blinded trial[J]. Eur J Anaesthesiol,2016,33(4):275.[32]Rong X,Sun C,Zhang F,et al. Effect of dexmedetomidine anesthesia on respiratory function in pediatric patients undergoing retinoblastoma resection[J]. Oncol Lett,2019,17(3):2721.[333Keating GM. Dexmedetomidine: A Review of Its Use for Sedation in the Intensive Care Setting [J]. Drugs,2015, 75 ( 10 ): 1119.[34] Rau JC, Dodick DW. Other Preventive Anti-Migraine Treatments: ACE Inhibitors, ARBs, Calcium Channel Blockers, Serotonin Antagonists» and NMDA Receptor Antagonists [J 3. Curr Treat Options Neurol,2019,21(4) : 17.[35] Deegan CA,Murray D,Doran P,et al. Effect of anaesthetic technique on oestrogen receptor-negative breast cancer cell function in vitro[J]. Br J Anaesth,2009,103(5): 685.[36] Uyar AS, Yagmurdur H,Fidan Y,et al. Dexmedetomidine attenuates the hemodynamic and neuroendocrinal responses to skull- pin head-holder application during craniotomy [J]. J Neurosurg Anesthesiol,2008»20(3) : 174.[37] Jiang L,Hu M, Lu Y, et al. The protective effects of dexme-detomicline on ischemic brain injury: A meta-analysis[J]. J Clin Anesth,2〇17,40 : 25.[38] Weingarten TN, Hawkins NM,Beam WB»et al. Factors associated with prolonged anesthesia recovery following laparoscopic bariatric surgery: a retrospective analysis[J]. Obes Surg,2015, 25(6):1024.[39] Apfel CC,Philip BK,Cakmakkaya OS,et al. Who is at risk for postdischarge nausea and vomiting after ambulatory surgery? [J]. Anesthesiology,2012,117(3) :475.[4〇]Sanders JG,Cameron C,Dawes PJD. Gabapentin in the Management of Pain following Tonsillectomy: A Randomized Double- Blind Placebo-Controlled Trial [J]. Otolaryngol Head Neck Surg,2017,157(5):781.[4ljjeffs SA,Hall JE,Morris S. Comparison of morphine alone with morphine plus clonidine for postoperative patient-controlled an- algesia[J]. Br J Anaesth,2002,89(3) :424.[42] Duggan EW,Klopman MA,Berry AJ,et al. The Emory University Perioperative Algorithm for the Management of Hyperglycemia and Diabetes in Non-cardiac Surgery Patients[J]. Curr Di- ab Rep,2016,16(3):34.[43] Abdelmalak BB, Bonilla AM, Yang D,et al. The hyperglycemic response to major noncardiac surgery and the added effect of steroid administration in patients with and without diabetes[J]. Anesth Analg,2013,116(5) : 1116.[44] Preiser JC,Ichai C,Orban JC, et al. Metabolic response to the stress of critical illness[J]. Br J Anaesth,2014,113(6) : 945.(收稿日期:2019 —12 —10)文章编号:1007 — 4287(2021)01 — 0150 —02子宫原发弥漫大B细胞淋巴瘤1例王楠、李梦龙2,赵淑华〃(1•吉林大学第二医院妇产科,吉林长春130041;2.首都医科大学公共卫生学院儿少卫生与妇幼保健学系,北京100069)1临床资料患者,女,70岁,主因间断发热5个月,发现子宫内膜病 变5天于2019年7月入院。患者既往月经规律,已绝经26 年。孕4产2,阴道分娩2女婴,人工流产1次,葡萄胎1次。 无血液病既往史。近半年体重减轻5 kg。5个月前无明显 诱因出现间断发热,常于下午出现,体温最高达38. 2°C,上午 及傍晚体温降至正常。患者于人院前9天就诊于当地医院, 诊断为宫腔积脓,引流出宫腔内脓液的同时加用抗生素治 疗,发热症状未见明显好转。行刮宫术送病理考虑为恶性肿 瘤,遂至我院行手术治疗,乳酸脱氢酶:698U/L。开腹行广*通讯作者泛子宫切除术,双侧附件切除术,盆腔淋巴结切除术,大网膜 切除术。术后病理:子宫:弥漫大B细胞淋巴瘤,浸润肌壁全 层,脉管内见肿瘤浸润,累及宫颈管间质,右侧附件见肿瘤浸 润,左侧盆腔淋巴结(1/8)见肿瘤转移,余未见肿瘤转移。免 疫组化染色结果:Ki67(阳性率90%)、Bcl-2(阳性率40%)、 Bcl-6(-)、MYC定量(阳性率40%)、MUM1(-)。术后于血液 内科行化学治疗,一般状态较差,第1周期给予R + mini- CHOP化疗方案(利妥昔单抗+ 1/2-1/3标准剂量的 CHOP),第2周期给予R-CHOP方案(利妥昔单抗+环磷酰 胺+阿霉素+长春新碱+泼尼松),同时采用甲氨蝶呤鞘内 注射预防中枢神经系统复发,本次化疗8天后出现4级粒细 胞缺乏伴有高热、腹泻,血培养显示有肺炎克雷伯菌生长,
经中国实验诊断学2021年1月第25卷第1期151抗感染、纠正骨髓抑制好转后采用利妥昔单抗进行第3次化 疗,第4-8次化疗方案均为R2方案(利妥昔单抗+来那度 胺)。现患者一般情况尚可。2讨论非霍奇金淋巴瘤是一种起源于淋巴结或其他部位淋巴 组织的恶性肿瘤,其中以弥漫大B细胞淋巴瘤这一组织学类 型最多见,占全部非霍奇金淋巴瘤的40%[1]。原发于女性生 殖系统淋巴瘤十分罕见,占全部结外淋巴瘤的〇. 2%- 1.1%[2],基本均以单个病例和小的病例系列的形式报告。 据报道,原发于女性生殖系统淋巴瘤最常见部位是卵巢 (37%),宫颈(21. 4%)和子宫(16. 5%),最常见的组织学类 型仍是弥漫大B细胞淋巴瘤「3]。原发于子宫的非霍奇金淋 巴瘤仅占子宫恶性肿瘤的〇.〇5%[4]。子宫原发弥漫大B细 胞淋巴瘤多发生于绝经后女性,大多数患者表现为绝经后阴 道流血或排液,也有部分表现为腹痛、盆腔包块,常被误诊为 子宫内膜癌进而收人院行手术治疗,病理回报确诊为弥漫大 B细胞淋巴瘤。本例主要表现为子宫积脓,既往无血液疾病 病史,术前影像学检査未发现肿大的淋巴结,骨髓穿剌与活 检结果未见明显异常,可以确定为子宫是原发部位,目前淋 巴瘤的临床分期仍采用1970年的Arm Arbor分期系统,出 现一个或多个结外器官广泛受累即为IV期,并且根据有无 全身症状,分为A、B两组,本例患者主要受累器官是子宫, 并且间断发热5个月左右,体温>38°C,根据淋巴瘤分期标 准,可以诊断为IV期B组。目前对于子宫原发弥漫大B细胞淋巴瘤的治疗方案尚 无统一标准,大部分学者推荐全子宫及双侧附件切除术,术 后行R-CHOP方案化疗。利妥昔单抗是一种单克隆抗体, 用于CD20( + )的弥漫大B细胞淋巴瘤的治疗,利妥昔单抗 可以降低神经系统复发的风险,明显延长弥漫大B细胞淋巴 瘤患者的总体生存期。中国一项有关老年弥漫大B细胞淋 巴瘤的回顾性研究发现,与单独CHOP化疗方案相比,增加 利妥昔单抗的患者5年总生存率大大提高(63. 1% vs 37. 1%,P<0. 001)⑴。来那度胺是一种新型免疫调节药物, 有抑制血管生成、诱导肿瘤细胞凋亡等抗肿瘤作用,适用于 不能耐受标准化疗方案,有多种合并症者的老年晚期患者, 来那度胺与利妥昔单抗联合化疗毒性较低,耐受性较髙。弥 漫大B细胞淋巴瘤患者的预后取决于多种因素。原发性非 霍奇金淋巴瘤涉及罕见的结外器官,如子宫,则预后较差[6]。 中国一项对42例生殖系统原发性非霍奇金淋巴瘤患者的回 顾性分析发现,乳酸脱氢酶水平是影响患者预后的独立危险 因素⑴。Hans等[8]提出以CD10,Bcl-6,mum-l这3个标志 物将弥漫大B细胞淋巴瘤分为生发中心亚型(GCB)和非生发中心亚型(non-GCB)。非生发中心亚型预后更差。Ki67 是与细胞增殖有关的抗原,Ki67阳性率较高表明肿瘤增殖活 跃,预后较差,B组症状出现也与预后不良相关。国际上广 泛采用IPI评分对淋巴瘤患者预后进行评估,包含5个危险 因素(年龄、体力状况ECOG评分、疾病分期、结外浸润和 LDH),本例患者的IPI得分为4分,高危。结合患者的免疫 组化结果:CD10 (-),Bcl-6 (-),mum-1 (-),为非生发中心亚 型,伴随Ki67阳性率90%并且存在B组症状,均提示预后不 良。综上所述,子宫原发弥漫大B细胞淋巴瘤发病率极低, 多数患者常被诊断为妇科恶性肿瘤行全面分期手术后,经病 理检查和免疫组织化学方法确诊为弥漫大B细胞淋巴瘤。 治疗方案尚无统一标准,以CHOP为基础的化疗方案中添 加利妥昔单抗可以延长患者总生存期,本病患者预后较差。 应建立相关数据库开展临床研究,探索最佳治疗方案,提高 患者生存率。参考文献:[l^Solimando AG,Annese T»Tamma R,et al. New Insights into Diffuse Large B-Cell Lymphoma Pathobiology[J3. Cancers (Basel), 2020,12(7):1869.[2] Wang J,Zeng L,Chen S,et al. Lymphoma of the female genital tract:a clinicopatholngical analysis of 25 cases[J]. Am J Transl Res,2019,11(9):5800.[3] Nasioudis D,Kampaktsis PN»Frey M,et al. Primary lymphoma of the female genital tract: An analysis of 697 cases[J]. Gynecologic Oncology,2017,145(2) :305.[4] Merritt AJ,Shenjere P,Menasce LP,et al. Primary extranodal marginal zone B cell lymphoma of the uterus:a case study and review of the literature[J]. J Clin PathoK2014,67(4) : 375.[5] Liu P, Han Y, Jiang S Y» et al. A retrospective analysis of real- world outcomes of elderly Chinese patients with diffuse large B- cell lymphoma[J]. Chin Med J (Engl) ,2019,132( 15) : 1807.[6] Mandato VD,Palermo R,Falbo A,et al. Primary diffuse large B- cell lymphoma of the uterus:case report and review[J], Anticancer Res,2014,34(8):4377.[7] 蒋学风,杨开选,彭芝兰,等.生殖系统原发性非霍奇金淋巴瘤的 临床病理特征和免疫表型检测[J].中华妇产科杂志,2007,42(4):222.[8] Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray[J]. Blood,2004, 103(1):275.(收稿日期:2019—12 —