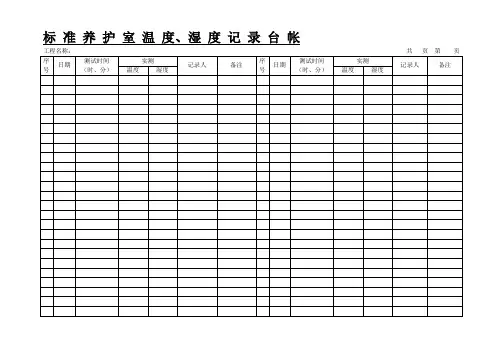
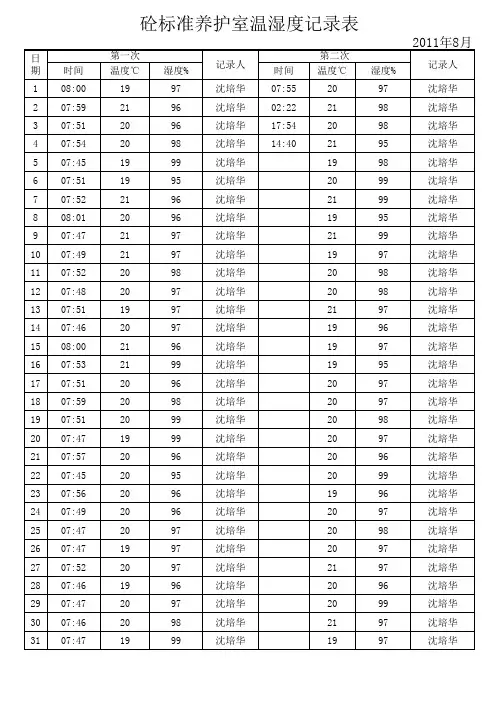
标准养护室记录表
- 格式:doc
- 大小:69.00 KB
- 文档页数:1
标准养护室巡查记录英文回答:STANDARD NURSING UNIT ROUNDING RECORD.Purpose:To assess the overall quality and safety of patient care on the nursing unit.To identify areas for improvement and provide feedback to nursing staff.To promote collaboration and communication among the healthcare team.Participants:Charge nurse.Nurse manager.Attending physician.Resident physician (if applicable)。
Other healthcare professionals (e.g., pharmacist, social worker) as needed.Frequency:Daily or as determined by the unit's policy.Procedure:1. The charge nurse will gather the team and introduce the purpose of the rounding.2. The team will proceed to each patient's room.3. The charge nurse will review the patient's chart and provide an overview of their current condition andtreatment plan.4. The attending physician will examine the patient and discuss their progress with the team.5. The resident physician will present any relevant information from their own assessment of the patient.6. The team will discuss any concerns or issues related to the patient's care.7. The team will make recommendations for any necessary changes in the patient's treatment plan.8. The charge nurse will document the rounding in the patient's chart.Documentation:The following information should be documented in the patient's chart:Date and time of rounding.Participants present.Patient's current condition and treatment plan.Any concerns or issues discussed.Recommendations for changes in treatment plan.Any other relevant information.Evaluation:The effectiveness of the rounding process should be evaluated on a regular basis.Feedback from nursing staff and patients can be used to identify areas for improvement.中文回答:标准护理室巡查记录。