鞍区病变影像诊断-(上)
- 格式:ppt
- 大小:18.04 MB
- 文档页数:54
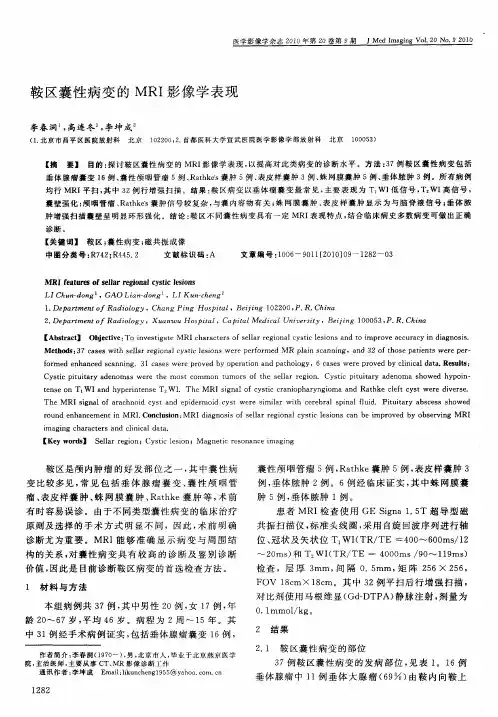

鞍区囊性病变影像学诊断【关键词】鞍区;,,囊肿;,,运算机体层扫描;,,磁共振成像摘要:目的:探讨鞍区囊性病变的CT和MRI表现,提高对该类疾病的诊断和辨别诊断水平。
方式:搜集经手术病理与临床证明的鞍区囊性病变的CT和/或MRI资料72例,其中囊性垂体瘤12例,囊性颅咽管瘤25例,Rathke囊肿16例,蛛网膜囊肿4例,鞍上池下疝继发假性蛛网膜囊肿4例,鞍旁表皮样囊肿4例,鞍旁皮样囊肿3例,垂体脓肿4例。
全数病例均行CT和/或MRI平扫,其中14例行CT增强检查,58例行MRI增强检查。
72例中65例经手术病理证明,7例经临床证明。
结果:12例囊性垂体瘤,其中垂体大腺瘤8例,微腺瘤4例。
6例大腺瘤表现为在实性瘤体内显现囊变区,2例瘤卒中囊变区内可见液平。
4例囊性垂体微腺瘤显示垂体饱满,内部显现异样信号/密度,伴有化验室检查异样。
25例囊性颅咽管瘤以囊性表现为主,发觉囊壁钙化及强化的垂体对辨别诊断成心义。
16例Rathke囊肿信号多样,但以形态饱满,呈短T一、长T2信号为较具特点性的改变。
4例蛛网膜囊肿和鞍上池下疝继发假性蛛网膜囊肿均表现为脑脊液信号,而后者囊壁显现持续或不持续薄壁环形强化,为其特点性表现。
3例皮样囊肿密度/信号较表皮样囊肿复杂,压脂序列对二者辨别诊断有帮忙。
4例垂体脓肿增强均显示环形强化,结合临床病史有助于术前诊断。
结论:鞍区不同性质的囊性病变具有必然的影像学特点,通过详细的影像学检查可对其中多数病变做出正确的定性诊断。
关键词:鞍区;囊肿;运算机体层扫描;磁共振成像Imaging Diagnosis of Rathke’s Cleft CystAbstract: Objective: To analyse CT and MRI findings of cystic lesions in sella region and enhance the level of diagnosis and differential diagnosis for these diseases. Method: CT and MR imaging findings in 72 patients with pathologically and clinically proved cystic lesions in sella region were all patients, cystic pituitary adenoma was found in 12 cases,cystic craniopharyngioma in 25 cases,Rathke’s cleft cyst in 16 cases , arachnoid cyst in 4 cases, suprasellar cistern hernia and secondary pseudo-arachnoid cyst in 4 cases, parasellar epidermoid cyst in 4 cases , parasellar dermoid cysts in 3 cases, Abscess of pituitary in 4 cases. All the patients were examined by plain MRI and CT scan ,among which 58 cases were examined by MRI contrast enhanced scan,14 cases by CT contrasted enhanced scan cases were proved by operation and pathology,7cases were proved by clinical data. Result:There were 12 cases cystic pituitary adenoma, in which macroadenoma 8 cases, microadenoma 4 cases. Mutiple cystic region could be found within the bodyof 6 cases pituitary macroadenoma with necrosis or cystogenesis. Fluid-level could be seen in 2 cases pituitary apoplexy. 4 cases cystic pituitary microadenoma showed abnormal signal intensity or density within well-stacked pituitary gland,accompanied with abnormality of laboratory main imaging manifestation of 25 cases cystic craniopharyngioma mainly showed cystic lesions , calcification of the capsule wall and the viewing of enhanced pituitary have value in differential diagnosis . 16 cases Rathke’s cleft cyst showed diverse signal short T1,long T2 signal intensity and well-stacked shape have feature to Rathke’s cleft cyst relatively .All arachnoid cyst and secondary pseudo-arachnoid cyst demonstrated CSF signal intensity. Continuous or discontinuous thin ring-like enhancement could be seen in secondary pseudo-arachnoid sequence was helpful in diagnosis of epidermoid cyst and dermoid cyst. The relatively thick ring-like enhancement and clinical history were helpful in diagnosis of pituitary abscess before operation. Conclusion: There were many imaging characteristics for differential category cystic lesions in sella is possible to make accuracy diagnosis in majority of these lesions through detailed imaging examinations.Key words: Sella region; Cystic lesion; CT; MRI鞍区囊性病变是以囊变成病理特点的多种疾病的总称,不同疾病其病理性质、生物学行为不同,采取的手术方式亦不同,因此术前诊断超级重要。
鞍区肿瘤的影像学表现鞍区肿瘤是指位于鞍区的肿瘤,鞍区位于颅底的中央部位,是脑下垂体和松果体所在的区域。
鞍区肿瘤的影像学表现可以通过多种影像学方法进行观察和分析,包括磁共振成像(MRI)、计算机断层扫描(CT)和放射性核医学方法等。
下面将对鞍区肿瘤的影像学表现进行详细描述。
1. MRI影像表现:(1) T1加权像:在T1加权像上,脑脊液(CSF)呈明亮信号,正常垂体呈低信号,而肿瘤则表现为明亮信号。
鞍区肿瘤的信号强度取决于其组织成分,如脑膜瘤和生殖细胞瘤通常表现为等或低信号,而垂体腺瘤多数呈高信号,并可呈包膜型、囊变型或实性型。
(2) T2加权像:在T2加权像上,脑脊液呈暗信号,正常垂体呈高信号,而肿瘤则表现为低到高不等的信号。
相对于T1加权像,T2加权像更有助于显示肿瘤的边界和包膜。
(3) 弥散加权成像(DWI):弥散加权成像利用水分子在组织内的自由扩散来产生图像,对于鞍区肿瘤的鉴别诊断具有一定的帮助。
几乎所有的鞍区肿瘤在DWI上呈高信号,而正常垂体则呈低信号。
(4) 造影增强:磁共振造影增强可以更好地显示肿瘤与周围结构的关系,包括肿瘤的包膜、囊变、坏死或出血等特征。
通常使用注射剂通过静脉注射,可以使肿瘤的强化增加,从而使肿瘤与周围正常组织的对比更加明显。
2. CT影像表现:(1) 平扫CT:平扫CT主要用于显示骨骼结构,如蝶鞍的形态、大小和形变等。
由于鞍区肿瘤通常不发生骨质破坏,因此平扫CT对于鞍区肿瘤的检出率有限。
(2) CT增强:蝶鞍增强CT能够更好地显示肿瘤的形态、包膜和囊变等特征。
通常通过静脉注射碘造影剂进行增强扫描,可呈现肿瘤的强化程度和分布特点。
3. 放射性核医学方法:(1) 甲氨蝶呤(99mTc-MIBI)显像:甲氨蝶呤显像能够显示垂体腺瘤和部分垂体腱膜瘤,但对于垂体室管膜的病变则无法显示。
(2) 白血病脑腰液显像:该检查方法主要用于检测鞍区来源的脑脊液恶性肿瘤的转移情况。
综合上述,鞍区肿瘤的影像学表现主要包括:在MRI上,脑脊液信号正常、垂体信号低、肿瘤信号高;在CT上,主要显示骨骼结构变化;在放射性核医学方法中,可观察到甲氨蝶呤显像和白血病脑腰液显像等特征。