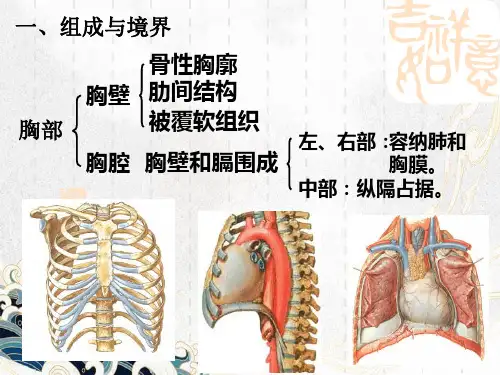
胸部正常组织勾画-Spring
- 格式:pdf
- 大小:5.51 MB
- 文档页数:16


IJROBP在放射肿瘤学领域称为“红皮杂志”,是美国放射治疗及肿瘤学会(ASTRO)官方杂志,为国际肿瘤放疗领域权威的、影响力最大的杂志。
红皮杂志列出2011年下载次数排名前10位文章,来自哈佛医学院肿瘤放疗中心的Zietman教授,现任ASTRO主席和红皮杂志主编,对这些文章撰写了评论。
强烈推荐大家阅读这些文章,这些文章对中国从事肿瘤放疗的医生必将有所启迪和帮助。
文章列表:1、骨转移的姑息放疗:ASTRO循证指南(Lutz等,2011)Palliative radiotherapy for bone metastases: an ASTRO evidence-based guideline.2、共识指南:宫颈癌调强盆腔放疗的临床靶区描绘(Lim等,2011)Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy for the definitive treatment of cervix cancer.3、临床上使用的正常组织并发症概率模型(Marks等,2010)Use of normal tissue complication probability models in the clinic.4、胸部放疗脏器风险的剂量限值考虑:肺、近端支气管树、食管、脊髓、肋骨和臂丛神经的图谱(Kong等,2011)Consideration of dose limits for organs at risk of thoracic radiotherapy: atlas for lung, proximal bronchial tree, esophagus, spinal cord, ribs, and brachial plexus.5、临床正常组织效应量化分析(QUANTEC):对一些科学命题的简介(Bentzen等,2010)Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC): an introduction to the scientific issues.6、开发并验证一项描绘臂神经丛轮廓的标准方法:在接受调强放疗的头颈部肿瘤患者中进行辐射剂量的初步分析(Hall 等,2008)Development and validation of a standardized method for contouring the brachial plexus: preliminary dosimetric analysis among patients treated with IMRT for head-and-neck cancer.7、综述表皮生长因子受体生物学(Herbst等,2004)Review of epidermal growth factor receptor biology.8、预后不良的中高危前列腺癌患者的盆腔淋巴结放射治疗:证据、推理以及未来方向(Morikawa等,2011)Pelvic nodal radiotherapy in patients with unfavorable intermediate and high-risk prostate cancer: evidence, rationale, and future directions.9、子宫内膜癌和宫颈癌术后盆腔调强放疗临床靶区划定的共识指南(Small等,2008)Consensus guidelines for delineation of clinical target volume for intensity-modulated pelvic radiotherapy in postoperative treatment of endometrial and cervical cancer.10、放疗在恶性黑色素瘤治疗中的应用进展(Khan等,2011)The evolving role of radiation therapy in the management of malignant melanoma.文献解读:Top 1为ASTRO以循证为依据制定的关于骨转移姑息放疗临床推荐指南,另一姊妹篇脑转移的姑息放疗指南也已发表,可于ASTRO网站下载(https:///Clinical-Practice/Guidelines/Brain-meta stases.aspx)。
CLINICALINVESTIGATIONNormalTissueCONSIDERATIONOFDOSELIMITSFORORGANSATRISKOFTHORACICRADIOTHERAPY:ATLASFORLUNG,PROXIMALBRONCHIALTREE,ESOPHAGUS,SPINALCORD,RIBS,ANDBRACHIALPLEXUS
FENG-MING(SPRING)KONG,M.D.,PH.D.,*TIMOTHYRITTER,PH.D.,*DOUGLASJ.QUINT,M.D.,
y
SURESHSENAN,M.D.,zLAURIEE.GASPAR,M.D.,xRITSUKOU.KOMAKI,M.D.,{COENW.HURKMANS,PH.D.,kROBERTTIMMERMAN,M.D.,#ANDREABEZJAK,M.D.,**JEFFREYD.BRADLEY,M.D.,yyBENJAMINMOVSAS,M.D.,zzLONMARSH,C.M.D.,*PAULOKUNIEFF,M.D.,
xx
HAKCHOY,M.D.,#ANDWALTERJ.CURRAN,JR.,M.D.{{
*DepartmentofRadiationOncology,UniversityofMichiganandAnnArborVeteranAffairsMedicalSystem,AnnArbor,MI;yDepartmentofRadiology,UniversityofMichigan,AnnArbor,MI;zDepartmentofRadiationOncology,VUUniversityMedical
Center,Amsterdam,TheNetherlands;xDepartmentofRadiationOncology,UniversityofColoradoDenver,Denver,CO;{Department
ofRadiationOncology,UniversityofTexasM.D.AndersonCancerCenter,Houston,TX;kDepartmentofRadiationOncology,
CatharinaHospital,Eindhoven,TheNetherlands;#DepartmentofRadiationOncology,UniversityofTexasSouthwesternMedical
CenteratDallas,Dallas,TX;**DepartmentofRadiationOncology,PrincessMargaretHospital,Toronto,ON,Canada;yyDepartment
ofRadiationOncology,WashingtonUniversity,St.Louis,MO;zzDepartmentofRadiationOncology,HenryFordHospital,Detroit,MI;
xxDepartmentofRadiationOncology,UniversityofFlorida,Gainesville,FL;and{{DepartmentofRadiationOncology,Emory
UniversityCancerCenter,andWinshipCancerinstitute,Atlanta,GA
Purpose:Toreviewthedoselimitsandstandardizethethree-dimenional(3D)radiographicdefinitionfortheor-gansatrisk(OARs)forthoracicradiotherapy(RT),includingthelung,proximalbronchialtree,esophagus,spinalcord,ribs,andbrachialplexus.MethodsandMaterials:ThepresentstudywasperformedbyrepresentativesfromtheRadiationTherapyOncol-ogyGroup,EuropeanOrganizationforResearchandTreatmentofCancer,andSoutwesternOncologyGrouplungcancercommittees.Thedosimetricconstraintsofmajormulticentertrialsof3D-conformalRTandstereotac-ticbodyRTwerereviewedandthechallengesof3DdelineationoftheseOARsdescribed.Usingknowledgeofthehumananatomyand3Dradiographiccorrelation,draftatlasesweregeneratedbyaradiationoncologist,medicalphysicist,dosimetrist,andradiologistfromtheUnitedStatesandreviewedbyaradiationoncologistandmedicalphysicistfromEurope.Theatlaseswerethencriticallyreviewed,discussed,andeditedbyanother10radiationoncologists.Results:Three-dimensionaldescriptionsofthelung,proximalbronchialtree,esophagus,spinalcord,ribs,andbrachialplexusarepresented.Twocomputedtomographyatlasesweredeveloped:oneforthemiddleandlowerthoracicOARs(exceptfortheheart)andonefocusingonthebrachialplexusforapatientpositionedsupinewiththeirarmsupforthoracicRT.ThedosimetriclimitsofthekeyOARsarediscussed.Conclusions:WebelievetheseatlaseswillallowustodefineOARswithlessvariationandgeneratedosimetricdatainamoreconsistentmanner.ThiscouldhelpusstudytheeffectofradiationontheseOARsandguidehigh-qualityclinicaltrialsandindividualizedpracticein3D-conformalRTandstereotacticbodyRT.Ó2011ElsevierInc.
Atlas,Lung,Esophagus,Spinalcord,Brachialplexus.
INTRODUCTIONIntheUnitedStates,>400,000peoplewerediagnosedwithbreast,lung,andesophagealcancersin2009(1),andap-
proximately50–60%ofthesewillundergoradiotherapy(RT)(2).Thenormaltissueswithinthethorax,includingthelungs,mainbronchi,esophagus,ribs/chestwall,heart,
Reprintrequeststo:Feng-Ming(Spring)Kong,M.D.,Ph.D.,De-partmentofRadiationOncology,UniversityofMichiganMedicalCenter,1500E.MedicalCenterDr.,AnnArbor,MI48109.Tel:(734)936-7810;Fax:(734)763-7370;E-mail:fengkong@med.umich.eduSupportedinpartbyNationalInstitutesofHealthGrantsR21CA127057andP01CA50827.Conflictofinterest:none.Acknowledgments—WeappreciatethesupportofDrs.JamesD.CoxandTheodoreS.LawrenceandthelungsteeringcommitteesoftheRadiationTherapyOncologyGroup,EuropeanOrganizationforResearchandTreatmentofCancer,andSouthwesternOncologyGroup.WearegratefultoDanielTatro,C.M.D.,andVickiEvans,C.M.D.,fortheirtechnicalassistance,andStevenKronenbergforstructurelabelingofthepictures.ReceivedFeb6,2010,andinrevisedformJuly22,2010.AcceptedforpublicationJuly22,2010.
1442
Int.J.RadiationOncologyBiol.Phys.,Vol.81,No.5,pp.1442–1457,2011CopyrightÓ2011ElsevierInc.PrintedintheUSA.Allrightsreserved0360-3016/$-seefrontmatter
doi:10.1016/j.ijrobp.2010.07.1977