Drug News Perspect 21(3), April 2008
Drug News Perspect 21(3), April 2008LOOKING AHEAD
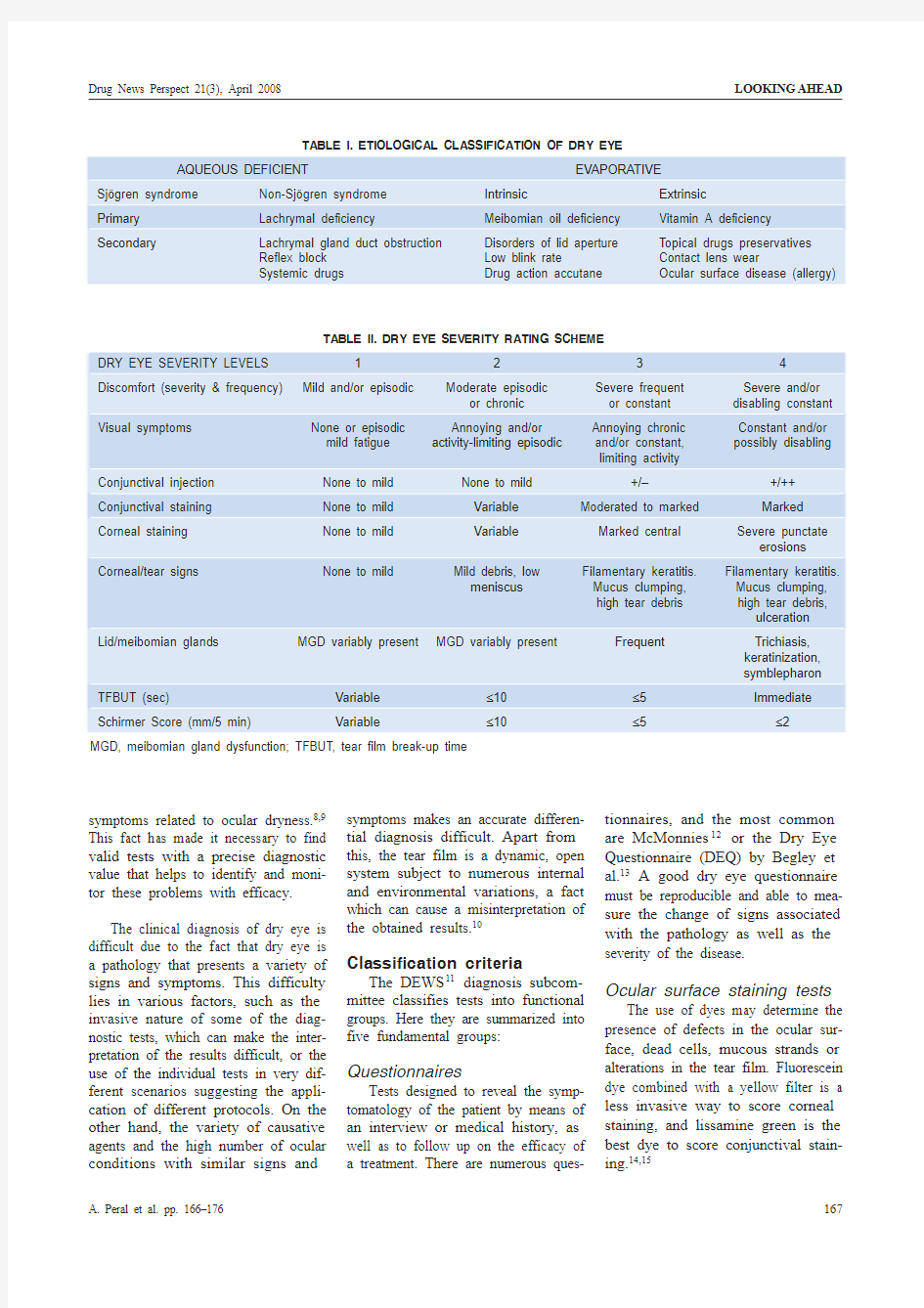
Tear film stability tests
These tests measure the time it takes tear film to lose its equilibrium.It is an indirect way to determine the tear film evaporation rate. The tear film break-up time (TFBUT) trial is an invasive test performed with fluores-cein that evaluates the stability of the tear film. There are other noninvasive tests to determine the stability of the film such as NIBUT (noninvasive break-up time [or test]) or the obser-vation of the meibomian glands.
Tear volume tests
This kind of test determines the total amount of tears as well as the reflex or basal tear secretion. The most common one is the Schimer I test that measures the volume of the tear that has wetted a filter strip of Whatman no. 1 paper. Other tests traditionally used—such as the phenol red thread test,16the Norn test or tear turnover rate (TTR),17or observing tear menis-cus height—are a less invasive alter-native and can be a good combination with other tests.
Tests to measure biological components
There are several tests that esti-mate certain components of the tear film related to dry eye. Among them,the measurements of osmolarity and protein levels in tears (lysozyme,lactoferrin, etc.) can provide a para-meter directly related to the dry eye mechanism, although they do not offer adequate information regarding the severity of the condition. These tests are not widely available and most of them are not available in the clinic. In the last DEWS meeting, osmo-larity was claimed as the main way to diagnose dry eye from an objective point of view; however, the measure of other biological constituents in tears has recently been described as bio-markers for dry eye. In 2002 a group of dinucleotides were described for the first time in tears.18These compounds,termed diadenosine polyphosphates,abbreviated ApnA, change their con-centrations in different dry eye situa-tions. Indeed, Peral and coworkers described that, independently of the
LOOKING AHEAD Drug News Perspect 21(3), April 2008
tear volume, there was a good correla-tion of one of these dinucleotides,Ap 4A, and the symptomatology.19This is a critical point since in those cases where the patient presents very low tear production, Ap 4A levels are high-er than in those patients with symp-toms and normal tear volume (but bad quality). In any case, whatever the symptoms or signs, Ap 4A concentra-tions are always higher than in healthy individuals.
This is even more patent in pathologies such as Sj?gren syndrome or aniridia. Patients presenting Sj?gren syndrome presented high con-centrations of dinucleotides Ap 4A and Ap 5A. In aniridia patients, it is inter-esting to note that eye dryness increases with aging and that con-comitant increases of Ap 4A with aging have been observed. Concentrations of the aforementioned molecule change for different dry eye states in a given pathology, affording information about the severity of the disease.Therefore, it seems that the quantifica-tion of this molecule may provide valuable information on the existence or not of a dry eye condition but also indicates the severity of this patholo-gy. In this sense the patent WO 2007128851 claims the use of this compound for the diagnosis, severity and the monitoring of the effective-ness of dry eye treatments.4
Apart from all of these tests, there are other tests and techniques not included in the previous groups. These techniques test different aspects of lipid layer and secretion pathology,like interferometry for tear observa-tion or the meibometry for meibomian gland function; with regard to tear film dynamics, tests include high-speed video-photography and optical coher-ence tomography; for the observation of mucins, tests include an impression cytology sample by means of the con-focal laser scanning microscopy.21Recently, stress tests such as the Staring Tear Break-UP Dynamic test (S-TBUD) or the study of the tear film in a controlled adverse environment (CAE)22have been developed.
The combination of several tests and sequences in detecting dry eye such as measuring the tear meniscus height together with tear crystalliza-tion or estimating tears production (TTR) together with osmolarity and evaporation tests can improve diagno-sis capabilities. Any of these combina-tions must be as sensitive as possible both in the detection as well as diag-nosis. TFBUT could be considered a good alternative in combination with some of the mentioned tests.Once the tests involved in tear analysis have been revised, we would like to suggest that those tests that pro-vide the best results and with minimal invasiveness be considered for use in clinical practice. A protocol according to our criteria is shown in Table III.
Management and therapy of dry eye
In order to identify the appropriate therapeutic methods for the manage-ment of dry eye disease and to know the proper sequence or strategy in which to apply them, the different cur-rent therapies have been divided into two groups: current treatment options and experimental therapies.
Current treatment options Tear supplements: Lubricants
Although they do not mimic the composition of the human tears, artifi-cial lubricants, also known as “artifi-cial tears,” are characterized by hypo-tonic or isotonic buffered solutions containing electrolytes, surfactants and various types of viscosity agents.Their physicochemical properties include a neutral or slightly alkaline pH and an osmolarity between 181 and 354 mOsm/L.23Ideally they should be preservative-free.24,25
It is difficult to prove the efficacy of an ocular lubricant either because it is not possible to detect the effects or because the currently available agents do not have any discernable activity beyond a lubrication effect. Despite this difficulty, most clinical trials will
Drug News Perspect 21(3), April 2008LOOKING AHEAD
LOOKING AHEAD Drug News Perspect 21(3), April 2008
Recently it has been suggested that absorption of tears by the naso-lachry-mal ducts into surrounding tissues and blood vessels may provide a feedback mechanism to the lachrymal gland regulating the production of tears.39A study showed a significant decrease in tear production for up to 2 weeks after plug insertion in patients with normal tear production.40
Moisture chamber spectacles. It has been reported that increases in periocular humidity can cause an increase in the lipid layer tear film thickness and also that spectacle wear-ers with dry eye have a longer interblink interval than those who do not wear spectacles.41For this reason, moisture chamber spectacles have been developed to increase the perioc-ular humidity, the interblink interval and to alleviate the ocular discomfort associated with dry eye.42Although there are advantages to this kind of device, just a few practitioners recom-mend its use.
Contact lenses. In cases of severe dry eye conditions, the use of contact lenses has been evaluated, and it has been reported that they may help to protect and hydrate the corneal sur-face.43–45Experimental therapies
Tear stimulation compounds:
secretagogues
One interesting approach is the
search for compounds with secreta-
gogue properties. This approach is of
special interest since three main tar-
gets need to be stimulated in order to
obtain an appropriate tear: the aque-
ous, the lipid and the mucin compo-
nents. It is clear that pharmacological
strategies can be developed to selec-
tively activate one or another, but there
are cases which with a single molecule
it is possible to act on the three targets.
Improving all tear components:
diquafosol. One of these compounds is
diquafosol (Prolacria TM), formerly
named as INS-365. This is a puriner-
gic P2Y receptor agonist with the abil-
ity to stimulate water, lipid and mucin
secretion. Therefore, this is an attrac-
tive approach with the major advan-
tage of providing a tear that exactly
simulates the features of the healthy
tear. This compound, which has been
favorably evaluated in clinical trials, is
just waiting for FDA last requirements
to be the first pharmaceutical com-
pound for the treatment of dry eye.
Double-blind trials demonstrated a
clear reduction in corneal staining as
well as good safety and tolerability in
humans.46Studies in animal models
have demonstrated that this compound
improves corneal epithelial function
mainly due to the increase in tear
secretion, mucin and lipid compo-
nents.47The product will be distrib-
uted by Inspire Pharmaceuticals and
Allergan as drops containing 2%
diquafosol (Table IV).
Compounds increasing the aque-
ous component.The peptidic com-
pound duramycin is also under inves-
tigation for the treatment of dry eye.
Duramycin (MOLI-1901) is a com-
pound that promotes chloride efflux. It
was originally developed for the treat-
ment of cystic fibrosis but is currently
undergoing phase II clinical develop-
ment at Lantibio for the treatment of
dry eye. Duramycin is a compound of
natural origin that promotes the hydra-
tion of epithelial tissue by promoting
chloride efflux. This efflux permits
better hydration of the ocular surface
thereby reducing the signs and pre-
sumably the symptoms of eye dryness,
especially in those patients presenting
low tear production. For results of
clinical studies see the Lantibio web
site (https://www.doczj.com/doc/b11328709.html,).48
Improving mucin secretion: Reba-
pamide, gefarnate, ecabet, 15-HETE,
pilocarpine, cevimeline. Another Source: Prous Science Integrity?
interesting compound acting as a selective secretagogue of the mucin component is rebamipide (OPC-12759), an amino acid analogue of quinolinone. This compound was orig-inally designed for mucosal protec-tion, healing of gastroduodenal ulcers and intestinal problems such as gastri-tis. It works by enhancing mucosal defense and scavenging free radicals.This compound is able to stimulate mucin secretion on the ocular sur-face,49and it is now in clinical trials (https://www.doczj.com/doc/b11328709.html, Identifiers NCT00475319 and NCT00201981).Preliminary results from a double-blind, dose-response clinical study conducted in 200 patients with dry eye syndrome showed that 2% rebamipide was safe, well tolerated and superior to placebo.50
Another interesting attribute of this substance is its properties of protect-ing against free radicals generated as a consequence of UV-B light, conse-quently damaging the cornea. This compound is now in phase III clinical trials (https://www.doczj.com/doc/b11328709.html, Identifier NCT00201981) and is being in-vestigated by Otsuka and Novartis (Table IV).
In the same line of the previous compound, gefarnate, produced by Santen, also increases mucin produc-tion. Chemically speaking this sub-stance is a water-insoluble terpene fatty acid used in the treatment of gas-trointestinal ulcers that basically facil-itates the healing and function of mucosal tissue. This compound when applied to the ocular surface stimu-lates epithelial cell mucin like glyco-protein production and also increases PAS-positive cells in the conjunctiva in animal studies.51
Ecabet sodium is a compound pro-duced by Senju and ISTA Pharma-ceuticals and has been tested in clini-cal trials all over the world. This compound is a dehydroabietic acid derivative originally purified from pine resin. Although initially it was used for the treatment of gastric ulcer and gastritis, it seems to present inter-Drug News Perspect 21(3), April 2008LOOKING AHEAD
esting properties in the treatment of dry eye. Ecabet sodium represents a new class of molecules that increases the quantity and quality of mucin pro-duced by conjunctival goblet cells and corneal epithelia. In the third quarter 2006, ISTA started a 100-patient phase IIb clinical trial designed to finalize the entry criteria and other clinical parameters for future registration stud-ies. A preliminary analysis of this phase IIb study of ecabet sodium reported a strong trend in the objective sign of blink rate, a strong trend in the Ocular Surface Disease Index (OSDI)and a positive trend in the subjective assessment of patients’most bother-some symptom. Additionally, 14% of patients in the treatment group report-ed increases in the quantity of tears produced, as compared to only 1.8% in the placebo group. There were serious ocular adverse events compared with placebo. Phase III studies are planned for 2008.52
A very selective compound stimu-lating just the mucin MUC1, a trans-membrane mucin present in corneal epithelial cells, is the substance 15(S )-HETE (15-S -hydroxyeicosatetraenoic acid; icomucret). This compound,apart from inducing the occurrence of MUC1, was found to stimulate glyco-protein secretion in human ocular tis-sue at submicromolar concentrations.Indeed, this compound is able to pre-vent desiccation due to the increase of these glycoproteins. Results from the latest clinical study of 15(S )-HETE did not show statistical significance of the active ingredient versus placebo.Alcon announced in 2006 they were evaluating clinical study designs to test the drug in specific subgroups of dry eye patients where the clinical benefit may be more evident.53According to Prous Science Inte-grity ?, Alcon discontinued the project in 2007 due to lack of statistical sig-nificance of the phase III clinical results.
It is interesting to see how some laboratories have started to use cholin-ergic agonists for the treatment of dry eye. Orally administered pilocarpine
has been evaluated in clinical trials for those cases of Sj?gren syndrome.54Doses of 5 mg q.i.d. helped patients improve blurred vision and other ocu-lar problems associated with this pathology. It has been demonstrated that pilocarpine increases the number of goblet conjunctival cells after 1–2months treatments. As a clear incon-venience, some patients complain of sweating and some other side effects that have obligated some of them to withdraw from this study.55
Cevimeline is another oral cholin-ergic agonist under study. This com-pound reduces the symptoms of dry-ness and increases tear production when it is administered in doses of 15–30 mg t.i.d. Compared to pilo-carpine, this compound seems to have fewer side effects.56–58
Antiinflammatory experimental drugs: Rimexolone,pimecrolimus, CF-101, NP-50301
Rimexolone is an interesting com-pound already available under the name Vexol ?(Alcon). This compound,which chemically is a corticosteroid,is used for the treatment of uveitis and inflammation derived from ocular surgery. Rimexolone is already in phase II for the treatment of ocular inflammation linked to dry eye (https://www.doczj.com/doc/b11328709.html, Identifier NCT00471419).
The compound pimecrolimus is an ascomycin macrolactam derivative that inhibits calcineurin, thereby blocking the activation immune sys-tem cytokines (immunomodulator).This substance was originally devel-oped for the treatment of derma-titis and other skin problems. It is undergoing phase II clinical studies at Novartis in the forms of 0.3%and 1% ophthalmic suspension (https://www.doczj.com/doc/b11328709.html, Identifier NCT00128245).
An analogue of adenosine acting via A 3adenosine receptor is currently in phase II at Can-Fite Biophar-ma (https://www.doczj.com/doc/b11328709.html, Identifier
NCT00349466). This compound,called CF-101, significantly con-tributed to reducing inflammation either alone or with methotrexate. An estrogen ester receptor agonist which is in phase II at Nascent Pharmaceuticals is the compound iDESTRIN TM , also called NP-50301.This compound has been assayed specifically in postmenopausal women significantly reducing dry eye symptoms and not presenting adverse side effects.59
Biological tear substituents
Autologous serum . The topical application of naturally occurring bio-logical fluids like saliva and serum can be used to substitute natural tears.These fluids contain growth factors,neurotrophins, vitamins, immuno-globulins and extracellular matrix pro-teins involved in the corneal surface maintenance.
Since the work by Tsubota in 1990,60the published evidence of the autologous serum application has been recently revised 61and an optimized protocol for its production has been published.62The concentrations used in the serum application vary from 20–100%, and its efficacy seems to be dose dependent. It has been described that 20% autologous serum improved TFBUT and decreased conjunctival rose bengal and corneal fluorescein staining 1–3 months postoperatively compared to treatment with artificial tears.63
Salivary gland autotransplanta-tion . Although this is not a pharmaco-logical therapy, it has been reported that the salivary submandibular gland transplantation is able to replace mucin and the aqueous phase of the tear film, providing improvement of Schirmer test, TFBUT, rose bengal staining as well as a reduction of dis-comfort and the need for pharmaceuti-cals tear substitutes. However, due to the hyposmolarity of saliva, excessive salivary tearing can induce a micro-cystic corneal edema that can lead to epithelial defects.64
LOOKING AHEAD Drug News Perspect 21(3), April 2008
Essential fatty acids
Recently, the ingestion of essential fatty acids has been included as a new possibility in dry eye therapy. It has been shown that linoleic acid and γ-linolenic acid administered orally twice a day produced a significant improvement in ocular irritation symptoms and ocular surface lis-samine green staining.65
Future therapies
for the treatment of dry eye (patents)
Apart from those approaches try-ing to mimic natural tears by means of combinations of viscous agents or nat-ural substitutes of tears, such as serum or salivary gland transplantations,many compounds remain in the pi-peline of pharmaceutical companies.Here, we highlight some of the drugs currently being investigated in clinical trials and others that have been identi-fied in the patent literature. A summa-ry of current development status of these investigational therapies is depicted in Table IV .
Organizing all these compounds is not easy since they present a huge variability in their structure and mech-anisms of actions, nevertheless they can be tentatively organized into the following groups:
Glucocorticoids and compounds treating dry eye as an inflammatory disease, including anticytokines.Glucocorticoids such as loteprednol,66alone or together with cyclosporin 67may be suitable for the treatment of the inflammatory component of this pathology, although it would not treat the origin of the disease. Nonsteroidal antiinflammatory agents have also been suggested as attractive com-pounds, especially when they are com-plemented with artificial tears.68Another interesting approach is to inhibit cytokine action, thereby pre-venting the inflammatory process associated with dry eye.69
Linked with some of the previous compounds due to a common chemi-cal structure, isoprene derivatives and
steroids such as 17β-estradiol and derivatives 70or sex steroids have been cited in patents.71Tear film quality depends on fine regulatory mecha-nisms affected by hormonal influ-ences. These steroid hormones are claimed to modify the activity of mei-bomian glands, thereby improving the lipid quality of tear. This may be of special interest in those cases when the dry eye is evaporative, since in most of the cases the excess in evaporation is due to a lack of tear lipids. Also diter-pene teprenone 72and isoprenoid vita-mins A and D have been claimed as useful for the treatment of ocular dry-ness,73although the latter is applied for the prophylaxis of dry eye. It is important to point out that a deficien-cy in vitamin A can produce ocular dryness that may finally produce xerophthalmia.
Nucleosides, nucleotides and dinu-cleotides are interesting candidates,since receptors for these substances have been described in the lachrymal,meibomian and goblet cells.74The pharmacology of these compounds is broad in terms of the receptors that can be activated, and the different ap-proaches are evident in the several existing patents. For instance, nucleo-sides such as uridine and its deriva-tives have also been claimed as possi-ble agents for the treatment of this disease.75These uridine compounds would act as scavengers reducing the presence of nitric oxide, which is asso-ciated with inflammatory processes,and then avoiding the consequence of the ocular surface dryness. Dinu-cleoside polyphosphates can be good agents for the treatment of dry eye.76In the group of the dinucleoside polyphosphates, the compound diqua-fosol should be included since it is a diuridine tetraphosphate, but there are additional agents that can also com-plete this group since diadenosine polyphosphates have been described in human tears.18Moreover, concen-trations of these dinucleotides are modified in dry eye patients, indicat-ing the close relationship between eye dryness and these molecules in this regard. Indeed, the topical application
of the dinucleotide Ap 4A, the close diquafosol congener, increases tear secretion in experimental animals in a similar fashion to diquafosol.77In addition, another dinucleotide, flavin adenine dinucleotide (FAD) has been patented as an active agent for the treatment of dry eye when considering the inflammatory process.78 This idea is not new since vitamin B 2has been used for the treatment of ocular inflammations unrelated to the dry eye pathology.
Most of the physiological process-es involved in the complex phenome-non of tearing are controlled by the nervous system. It is not surprising then to find patents based on the use of neurotransmitters to improve tearing.WO 200706751979is one such patent that is claimed for almost any neuro-transmitter or neuropeptide as a possi-ble agent for the treatment of dry eye.Beside these broad-reaching patents,others are more focused on specific aspects of neurotransmission. For instance, there are patents that are claimed for nondrying antihistamine agents.80In particular, the use of H 1histamine antagonists reduces the symptoms of dry eye because corneal nerves will not react to the allergic response that histamine provides. The opposite approach has also been taken into account; for instance, H 2hista-mine receptor agonists can be used.81In this case, H 2agonist stimulates mucins from goblet cells. This therapy would be suitable for those cases in which mucins are not synthesized in an adequate amount because the lack of these proteins leads to unstable tear film. Other entities under development depict more classical approaches, such as the claim for nicotinic agonists,82which may mimic the acetylcholine released by the parasympathetic termi-nals in the main lachrymal glands, the main neurotransmitter that produces tear secretion. Also, patents can be found that are claimed for the use of nitric oxide (NO) or any of the NO generating agents, since these can stimulate mucin secretion.83It is nev-ertheless contradictory to see the application of NO for mucin stimula-Drug News Perspect 21(3), April 2008LOOKING AHEAD
tion and NO scavenging by uridines considering its relation with the inflammatory process (see above).Amino acids, peptides and proteins are also biomolecules investigated for their ability to provide relief from dry eye. Cysteine,84acetylcysteine and their derivatives can restore normal conditions in the ocular surface since they have mucolytic action adequate for dry eye cases in which mucins are altered.85Some peptides isolated from plants such as the trefoil have been claimed to be active in reversing dry eye.86These peptides present a com-mon structural motif, and have some properties that help in healing injury.In this case, these peptides may help to heal the ocular surface from the dam-age caused by severe dry eye. Proteins such as interferon have been described as active in the treatment of ocular dryness; the corresponding patent has been filed in Japan.87A more obvious approach is presented in patent US 2003109509,88where a mixture of MUC1 (mucin type 1) together with other agents is claimed. This would be especially interesting in those cases in which dry eye is caused by a problem with mucins’absence or reduction.Galectin-1, a lectin with antiinflam-matory properties, has also been indi-cated as a treatment for the inflamma-tory process associated with dry eye.89Proteins with enzymatic activities have also been investigated mostly in the search for inhibitors whose action may help restore normal ocular sur-face conditions. In this sense,inhibitors of phosphodiesterase IV 90block the inflammatory process asso-ciated with dry eye by controlling the levels of cAMP in inflammatory cells.Finally, proteasome inhibitors 91seem to be effective for dry eye treatment,since proteasome inhibition blocks the release of factors such as nuclear fac-tor-κB (NF-κB), among others, which may upregulate the production of sev-eral inflammatory mediators. Dealing with the same target, the patent WO 200209570492claims the use of NF-κB inhibitors to treat the inflam-matory process accompanying ocular dryness.
Sugars and derivatives such as the macrolide FK-50693or glycosides 94have been investigated and patented.These compounds stabilize tears as indicated by the beneficial changes observed in TBUT and fluid produc-tion. Also, mixtures of polysaccha-rides and polyols have been claimed for dry eye treatment 95together with a preparation containing glycosamino-glycans and hydrogen peroxide, which is more useful in providing moisture in the ocular surface as opposed to hav-ing a pharmacological effect.96
For a general overview of the patented compounds and the targets they stimulate in ocular surface tissues see Figure 1.
Conclusions
Research in the field of dry eye has two branches. On the one hand, it is essential to develop clinical tests valid for the detection, quantification and monitoring of the signs and symp-toms. On the other hand, there is the need to discover the molecular mech-anisms that are produced by dry eye as well as biomarkers for detecting and grading the disease.
Currently, the tests used to detect dry eye signs and symptoms have been divided into five groups according to functionality. Once the etiology of dry eye has been classified, it is important to grade the severity of the disease and select the proper therapy. Among the diagnostic tests, osmolarity seems to be the parameter that draws the line between dry eye and non-dry eye, but it does not rate the severity of this con-dition. Recently, the measure of Ap 4A in different dry eye states and patholo-gies has suggested this molecule as a potential biomarker in this pathology (see above).
Diadenosine tetraphosphate,Ap 4A, is opening new remarkable per-spectives in the treatment of dry eye.Apart from the fact that Ap 4A can stimulate tear secretion, we have recently demonstrated that the combi-nation of this dinucleotide with the neurohormone melatonin can improve
LOOKING AHEAD Drug News Perspect 21(3), April 2008
scanning electron microscopic evaluation (ARVO abstract).Invest Ophthalmol Vis Sci 1991, 32(Suppl.): 733.
26. Nelson, J.D. and Gordon, J.F. Topical
fibronectin in the treatment of keratocon-junctivitis sicca. Chiron Keratoconjunc-tivitis Sicca Study Group.Am J Ophthalmol 1992, 114(4): 441–7.
27. Luo, L., Li, D., Corrales, R. et al. Hyper-osmolar saline is aproinflammatory stress on the mouse ocular surface.Eye Contact Lens 2005, 31(5): 186–93.
28. Luo, L., Li, D.Q., Doshi, A. et al. Experi-mental dry eye stimulates production of inflammatory cytokines and MMP-9 and activates MAPK signaling pathways on the ocular surface.Invest Ophthalmol Vis Sci 2004, 45(12): 4293–301.
29. Johnson, M.E. and Murphy, P.J. Changes in
the tear film and ocular surface from dry eye syndrome.Progr Retin Eye Res 2004,23(4): 449–74.
30. Ta, C.N., Shine, W.E., McCulley, J.P. et al.
Effects of minocycline on the ocular flora of patients with acne rosacea or seborrheic blepharitis.Cornea 2003, 22(6): 545–8.31. Solomon, A., Rosenblatt, M., Li, D.Q. et al.
Doxycycline inhibition of interleukin-1 in the corneal epithelium.Invest Ophthalmol Vis Sci 2000, 41(9): 2544–57.32. Tamargo, R.J., Bok, R.A. and Brem, H.
Angiogenesis inhibition by minocycline.Cancer Res 1991, 51(2): 672–5.
33. Macdonald, A. and Feiwel, M. Perioral der-matitis: Aetiology and treatment with tetra-cycline.Br J Dermatol 1972, 87(4): 315-9.34. Jansen, T. and Plewig, G. Rosacea:
Classification and treatment.J R Soc Med 1997, 90(3): 144-50.35. Dougherty, J.M., McCulley, J.P., Silvany,
R.E. et al. The role of tetracycline in chron-ic blepharitis.Invest Ophthalmol Vis Sci 1991, 32(11): 2970–5.
36. Alacrity Biosciences announces positive
results from a phase 2 study of its dry eye treatment ALTY-0501 [news release].Laguna Hills: Alacrity Biosciences;October 9, 2007. https://www.doczj.com/doc/b11328709.html,/pdf/ALTY0501%20news%20release%20FINAL.pdf. Accessed March 10, 2008.37.SmartPLUG TM – The intelligent solution for
dry eyes . Medennium Web site. https://www.doczj.com/doc/b11328709.html,/prof_smartplug.htm.Accessed March 10, 2008.
38. Baxter, S.A. and Laibson, P.R. Punctal
plugs in the management of dry eyes.Ocul Surf 2004, 2(4): 255–65.
39. Paulsen, F. The human lacrimal glands.Adv
Anat Embryol Cell Biol 2003, 170: III-XI,1-106.
40. Yen, M.T., Pflugfelder, S.C. and Feuer, W.J.
The effect of punctal occlusion on tear pro-duction, tear clearance, and ocular surface sensation in normal subjects.Am J Ophthalmol 2001, 131(3): 314–23.Drug News Perspect 21(3), April 2008LOOKING AHEAD
41. Korb, D.R., Greiner, J.V ., Glonek, T. et al.
Effect of periocular humidity on the tear film lipid layer.Cornea 1996, 15(2):129–34.
42. Tsubota, K., Yamada, M. and Urayama, K.
Spectacle side panels and moist inserts for the treatment of dry-eye patients.Cornea 1994, 13(3): 197–201.
43. Pullum, K.W., Whiting, M.A. and Buckley,
R.J. Scleral contact lenses: The expanding role.Cornea 2005, 24(3): 269–77.
44. Romero-Rangel, T., Stavrou, P., Cotter, J. et
al. Gas-permeable scleral contact lens ther-apy in ocular surface disease.Am J Ophthalmol 2000, 130(1): 25–32.45. Rosenthal, P., Cotter, J.M. and Baum, J.
Treatment of persistent corneal epithelial defect with extended wear of a fluid-venti-lated gas-permeable scleral contact lens.Am J Ophthalmol 2000, 130(1): 33–41.46. Tauber, J., Davitt, W.F., Bokosky, J.E. et al.
Double-masked, placebo-controlled safety and efficacy trial of diquafosol tetrasodium (INS365) ophthalmic solution for the treat-ment of dry eye.Cornea 2004, 23(8):784–92
47. Fujihara, T., Murakami, T., Fujita, H. et al.
Improvement of corneal barrier function by the P2Y(2) agonist INS365 in a rat dry eye model.Invest Ophthalmol Vis Sci 2001,42(1): 96–100
48. Moli1901 Dry Eye Studies . Lantibio, Inc.
Web site. https://www.doczj.com/doc/b11328709.html,/Moli_dryEyeStudies.htm. Accessed March 10,2008.
49. Urashima, H., Okamoto, T., Takeji, Y . et al.
Rebamipide increases the amount of mucin-like substances on the conjunctiva and cornea in the N-acetylcysteine-treated in vivo model.Cornea 2004, 23(6): 613–9.50. Donshik, P.C., Foulks, G ., Monica, M. et al.
Multicenter, randomized, double–masked,dose–response, placebo–controlled, paral-lel–group study of the safety and efficacy of rebamipide (OPC–12759) sterile oph-thalmic suspension in the treatment of dry eye.Invest Ophthalmol Vis Sci 2005, 46: E-Abstract 2037.
51. Nakamura, M., Endo, K., Nakata, K. and
Hamano, T. Gefarnate increases P AS posi-tive cell density in rabbit conjunctiva.Br J Ophthalmol 1998, 82(11): 1320-3.
52. ISTA Pharmaceuticals announces positive
preliminary results from ecabet sodium phase IIb study [news release]. Irvine: ISTA Pharmaceuticals, Inc.; May 31, 2007. http ://https://www.doczj.com/doc/b11328709.html,/phoenix.zhtml?c=121179&p =i r o l -n e w s A r t i c l e &I D =1009801&highlight=. Accessed March 10,2008.
53. Alcon's fourth quarter sales rise 10.7 per-cent [news release]. Hunenberg, Switzer-land: Alcon, Inc. February 8, 2006 https://www.doczj.com/doc/b11328709.html,/phoenix.zhtml?c=130946&p=irol-newsArchiveArticle&ID=814685&highlight= . Accessed March 10,2008.54. Papas, A.S., Sherrer, Y .S., Charney, M. et al.
Successful treatment of dry mouth and dry eye symptoms in Sj?gren’s syndrome patients with oral pilocarpine: A random-ized, placebo-controlled, dose-adjustment study.J Clin Rheumatol 2004, 10(4):169–77.
55. Aragona, P., Di Pietro, R., Spinella, R. and
Mobrici, M. Conjunctival epithelium improvement after systemic pilocarpine in patients with Sj?gren’s syndrome.Br J Ophthalmol 2006, 90(2): 166–70.
56. Ono, M., Takamura, E., Shinozaki, K. et al.
Therapeutic effect of cevimeline on dry eye in patients with Sj?gren’s syndrome: A ran-domized, double-blind clinical study.Am J Ophthalmol 2004, 138(1): 6–17.
57. Petrone, D., Condemi, J.J., Fife, R. et al.
Double-blind randomized placebo-con-trolled study of cevimeline in Sj?gren’s syn-drome patients with xerostomia and kerato-conjunctivitis sicca.Arthritis Rheum 2002,46(3): 748–54
58. Leung, K.C., McMillan, A.S., Wong, M.C.,
Leung, W.K., Mok, M.Y . and Lau, C.S. The efficacy of cevimeline hydrochloride in the treatment of xerostomia in Sj?gren's syn-drome in southern Chinese patients: A ran-domised double-blind, placebo-controlled crossover study.Clin Rheumatol 2007 Sep 26, Advance publication.
59. Nascent reports positive results for phase II
dry eye treatment [news release]. Burlin-game: Nascent Pharmaceuticals, Inc.; Ja-nuary 4, 2006. https://www.doczj.com/doc/b11328709.html,/News11.html. Accessed March 10,2008.
60. Tsubota, K., Goto, E., Fujita, H. et al. Treat-ment of dry eye by autologous serum appli-cation in Sj?gren’s syndrome.Br J Ophthalmol 1999, 83(4): 390–5.61. Geerling, G . and Hartwig, D. Autologous
serum eyedrops for ocular surface disor-ders.In: Cornea and External Eye Disease.Reinhard, T., Larkin, F. (Eds.). Spinger:Berlin, Heidelberg 2005, 2–19.
62. Liu, L., Hartwig, D., Harloff, S. et al. An
optimised protocol for the production of autologous serum eyedrops.Graefes Arch Clin Exp Ophthalmol 2005, 243(7):706–14.
63. Noda-Tsuruya, T., Asano-Kato, N., Toda, I.
et al. Autologous serum eye drops for dry eye after LASIK.J Refract Surg 2006, 22(1):61–6.
64. Geerling, G ., Honnicke, K., Schroder, C. et
al. Quality of salivary tears following autol-ogous submandibular gland transplantation for severe dry eye.Graefes Arch Clin Exp Ophthalmol 2000, 238(1): 45–52.
65. Barabino, S., Rolando, M., Camicione, P. et
al. Systemic linoleic and gammalinolenic acid therapy in dry eye syndrome with an infl ammatory component.Cornea 2003,22(2): 97–101.
66. Bartels, S.P. (Bausch & Lomb Inc.). Use of
loteprednol etabonate for the treatment of dry eye. WO 2005094836. October 13, 2005.
67. Xia, E., Hu, Z., Tyle, P. and Bartels, S.
(Bausch & Lomb Inc.). Ophthalmic compo-sitions comprising steroid and cyclosporine for dry eye therapy. WO 2006073786. July 13, 2006.
68. Ousler, G.W., Chapin, M.J. and Abelson,
M.B. (Ophthalmic Research Associates, Inc.). Formulations and methods for treat-ing dry eye. WO 2007087609. August 2, 2007.
69. Gamache, D.A. (Alcon, Inc.). Use of
cytokine synthesis inhibitors for the treat-ment of dry eye disorders. WO 2004026406.
April 1, 2004.
70. Mee, C., Barnett, G. and Coy, M. (Nascent
Pharmaceuticals, Inc.). Combination thera-py for topical application in the treatment of dry eye syndrome. WO 2006094028.
September 8, 2006.
71. Lubkin, V. Drugs for topical application of
sex steroids in the treatment of dry eye syn-drome, and methods of preparation and application. US 6096733. August 1, 2000.
72. Toshihiko, V., Shimamura, I., Yorii, H.,
Ohashi, Y., Shimizu, D., Nishihara, M.
(Eisai Co., Ltd.). Agent for treating dry eye.
JP8133967. May 28, 1996.
73. Ishii, Y., Itoh, S., Kita, K. and Mukai, K.
Composition for prophylaxis and/or treat-ment of dry eye syndrome comprising vita-min D. US 2001027188. October 4, 2001.
74. Cowlen, M.S., Zhang, V.Z., Warnock, L. et
al. Localization of ocular P2Y2 receptor gene expression by in situ hybridization.
Exper Eye Res 2003, 77: 77–84.
75. Park, M.-G. and Kuon, M.-K. (MD
BioAlpha Co., Ltd.). Composition having effect on treatment and prevention of dry eye syndrome. WO 2007061200. May 31, 2007.
76. Yerxa, B.R., Jacobus, K.M., Rideout, J.L.
and Pendergast, W. (Inspire Pharma-ceuticals, Inc.). Method of treating dry eye disease with purinergic receptor agonists.
WO 9834593. August 13, 1998.
77. Pintor, J,, Peral, A., Hoyle, C.H. et al.
Effects of diadenosine polyphosphates on tear secretion in New Zealand white rabbits.
J Pharmacol Exp Ther. 2002, 300(1): 291–7.78. Coquelet, C. and Latour, E. (Chauvin Lab
SA). Use of flavine-adenine-dinucleotide for the preparation of ophthalmic composi-tions for the treatment of the dry eye.
EP0930071. July 21, 1999.
79. Ousler, G.W. III, Chapin, M.J. and Abelson,
M.B. (Ophthalmic Research Associates, Inc.). Use of neurotransmitters and neu-ropeptides for the treatment of dry eye dis-eases and related conditions. WO 2007067519. June 14, 2007.
80. Yerxa, B.R., Vittitow, J.L. and Ice, J.C. Jr.
(Inspire Pharmaceuticals, Inc.). Method of treating dry eye disease with non-drying antihistamines. WO 2007022541. February 22, 2007.
81. Miller, S.T., Gamache, D.A. and Yanni, J.M.
(Alcon Laboratories, Inc.). Methods of use of histamine H2 agonists in treating dry eye.
US6274160. August 14, 2001.
82. Yerxa, B., Peterson, W. (Inspire Pharma-
ceuticals, Inc.). Method of treating dry eye disease with nicotinic acetylcholine recep-tor agonist.WO 0180844. November 11, 2001.
83. Gamache, D., Miller, S. (Alcon Labs, Inc.;
Gamache Daniel A.). The use of nitric oxide generations for the treatment of dry eye dis-orders.WO9930716. June 24, 1999.
84. Ceddaha, M. (LMD SA). Cysteine for oral
administration for dry eye treatment. WO 2002055068. July 18, 2002.
85. Chetoni, P., Burgalassi, S., Saettone, M.F.,
Giannaccini, B. and Boldrini, E. (Farmigea SpA). Ophthalmic composition containing N-acetylcysteine for the treatment of dry-eye syndrome. WO 2003011249. February 13, 2003.
86. Bakhit, P.G., Graham, R. and Olejnik, O.
(Allergan, Inc.). Ophthalmic compositions comprising trefoil factor family peptides.
WO 2005009459. February 3, 2005.
87. Tsubota, K. (R-Tech Ueno, Ltd.). Drug
composition comprising albumin as active ingredient. US6043213. March 28, 2000.
88. Gamache, D.A., Yanni, J.M. and Van
Duzee, B.F. (Alcon, Inc.). Methods for treating dry eye. US2003109509. June 12, 2003.
89. Panjwani, N. (Tufts University). Compo-
sitions and uses of a galectin for treatment of dry eye syndrome. WO 2006113311.
October 26, 2006.
LOOKING AHEAD Drug News Perspect 21(3), April 2008
用六个步骤建立平衡计分卡 作者:杨序国 目前,平衡计分卡应用与推广的热潮正从国外袭入国内。根据Gartner Group 的调查表明,到2000年为止,在《财富》杂志公布的世界前1000位公司中有40%的公司采用了平衡计分卡系统。在最近由William M. Mercer 公司对214个公司的调查中发现,88%的公司提出平衡计分卡对于员工报酬方案的设计与实施是有帮助的,并且平衡计分卡所揭示的非财务的考核方法在这些公司中被广泛运用于员工奖金计划的设计与实施中。然而,国内不少企业设计与实施的平衡计分卡与真正的平衡计分卡的初衷存在一些背离。在国外,平衡计分卡被比作飞机驾驶舱内的仪表盘,里面有各种指标,管理层借此观察企业运行是否良好。而国内的公司更多的只是单纯将平衡计分卡作为一种绩效考评工具,往往以解决价值分配问题为初衷,而不是作为一种战略实施划执行工具,首先以支撑企业战略目标的达成为目的。 如图1所示(图略),建立平衡计分卡是一个系统化的过程。这里必须强调的是,必须根据公司战略来制定平衡计分卡,再按照战略与平衡计分卡来制定战略的实施计划,而不是相反。否则平衡计分卡就成为对战略实施计划的监测工具和绩效管理工具,这与KPI没有什么区别。这是多数公司会犯的错误。 下表1是笔者2003年上半年在深圳特区某高科技民营企业做BSC咨询项目时的工作计划表: 表1:BSC项目时间表 第一阶段:战略明确与前期工作
第一步,制定公司战略。 公司战略的制定虽不是本文所要解决的问题,但要明白公司在生命周期不同的阶段有不同的战略重点,如表2: 表2:处于生命周期不同阶段的公司的战略重点 第二步,调查与明确客户价值定位 客户的价值定位就是为什么客户从您的公司,而不是从您的竞争对手那里购买产品?他们会为了什么(价格、质量、时间、功能、服务、关系、品牌、形象)而付出钞票?公司如何比竞争对手做得更好?公司的产品/服务是否能为客户提供与众不同的价值?如何让公司的产品/服务优于竞争对手?
建立平衡计分卡实务案例 用六个步骤建立平衡计分卡 目前,平衡计分卡应用与推广的热潮正从国外袭入国内。根据Gartner Group 的调查表明,到2000年为止,在《财富》杂志公布的世界前1000位公司中有40%的公司采用了平衡计分卡系统。在最近由William M. Mercer 公司对214个公司的调查中发现,88%的公司提出平衡计分卡对于员工报酬方案的设计与实施是有帮助的,并且平衡计分卡所揭示的非财务的考核方法在这些公司中被广泛运用于员工奖金计划的设计与实施中。然而,国内不少企业设计与实施的平衡计分卡与真正的平衡计分卡的初衷存在一些背离。在国外,平衡计分卡被比作飞机驾驶舱内的仪表盘,里面有各种指标,管理层借此观察企业运行是否良好。而国内的公司更多的只是单纯将平衡计分卡作为一种绩效考评工具,往往以解决价值分配问题为初衷,而不是作为一种战略实施划执行工具,首先以支撑企业战略目标的达成为目的。 建立平衡计分卡是一个系统化的过程。这里必须强调的是,必须根据公司战略来制定平衡计分卡,再按照战略与平衡计分卡来制定战略的实施计划,而不是相反。否则平衡计分卡就成为对战略实施计划的监测工具和绩效管理工具,这与KPI没有什么区别。这是多数公司会犯的错误。 下表1是笔者2003年上半年在深圳特区某高科技民营企业做BSC咨询项目时的工作计划表: 表1:BSC项目时间表 第一阶段:战略明确与前期工作
第二阶段:制定平衡计分卡
第三阶段,制定战略与测评指标的实施计划
第四阶段,战略监测、反馈与修正 2004全年战略考察与流程重组利用BSC这一战略管理工具每月、每季进行定期战略考察与反馈,并针对公司流程绩效差距对公司流程进行分解与分析,予以重组或优化。战略管理部人力资源部 第一步,制定公司战略
平衡计分卡系统实施步骤(new) 学习导航 通过学习本课程,你将能够: ●了解实施平衡计分卡系统的前期准备; ●学会如何将战略转化为可操作的行动; ●掌握平衡计分卡系统实施步骤。 平衡计分卡系统实施步骤(new) 一、实施平衡计分卡系统的前期准备 应用平衡计分卡的过程实际上就是对战略中心型组织框架的导入过程,实质就在于如何把握战略中心型组织框架导入的时机。 1.不适合使用平衡计分卡的情况 在下列两种情况下,企业的平衡计分卡实施成功率会很低: 企业高层不认可 平衡计分卡不是一个简单的人力资源绩效考核系统。为了提高企业的执行力,它必须从高层做起、从战略做起,而且要协调各个部门之间的关系和相互的责任。 不具备合适的企业文化 平衡计分卡是一套全员动员、全员参与的管理系统,如果一个企业没有学习、创新、积极发展、不断改进的文化,就不适合实施平衡计分卡,否则在实施过程中会有很多人持反对意见、设置障碍。 2.导入的时机选择 企业战略变革 一个企业的经营环境发生了变化,迫使企业必须改变策略时,就需要实施平衡计分卡;企业发生了重大的高层人事变动,如新的高层主管与大多数员工还没有建立管理的默契时,也需要运用平衡计分卡作为一个系统来促进全员的沟通。 业绩不佳
当企业出现业绩不佳时,价值观会出现差距,员工也会有不同的想法,应用平衡计分卡让员工的想法、价值观趋于一致;当产品或者服务的质量不好时,也需要平衡计分卡改善不足和弥补缺陷;同时,导入平衡计分卡还能提升企业业务操作环节的效率。 图1 导入战略中心型组织框架的时机示意图 业务增长期 当企业要进行一些新的业务管理时,也是导入平衡计分卡的良好时机。比如,并购新的企业后,被并购企业与并购企业在文化、战略以及想法上都不同,就需要通过战略中心型组织的框架促使双方更好地沟通,更好地执行公司的战略;同样,企业在全球进行地区性扩张以及建立新的公司时,由于地区的差异,很多东西不能面对面沟通,就需要使用平衡计分卡。 资源整合阶段 企业的目标是形成新的组织架构,当企业进行各种类型的整合时,可以用平衡计分卡来勾勒各个组织架构需要做的重点事情。 3.组织实施平衡计分卡项目失败的原因 根据平衡计分卡协会的调查,在全球实施平衡计分卡的众多企业中,有将近50%没有取得最后成功,主要原因体现在三方面,如图2所示。
基于平衡记分卡的绩效管理体系构建步骤 基于平衡记分卡绩效管理系统是将企业的战略和一整套财务和非财务考核手段相结合,达到改善企业财务状况,最终实现企业战略目标的目的。基本思路如下:从企业的战略出发,将其按照战略管理的内在要求(即因果关系链),分财务、客户、内部流程和学习与成长四个维度分别确立战略目标,然后通过对于战略目标相联的CSF和KPI的定义和描述,将定性战略目标转化为考核指标,从而构建一套以战略为核心、目标指标与过程指标并存、财务指标与非财务指标并重、长期与短期相平衡的绩效管理系统。步骤如下: 第一步:高层的认可和参与 企业的高层领导对平衡记分卡的认可和参与对成功实施平衡记分卡至关重要,可以说没有他们的参与,就没有平衡记分卡的成功,因为他们对战略制定、财务指标制定和绩效管理实施有相当重要的作用。 第二步:理清战略目标 平衡记分卡是一套战略管理系统,是对已形成的战略进行贯彻、实施、反馈和修正的系统,因此实施平衡记分卡之前首先确定清晰的战略目标。 第三步:战略分解,形成战略因果图 明确企业的战略目标后,将企业战略所内含的一连串假设转化为一系列具体的因果关系链。因果关系链的建立一方面可以有助于将企业的战略转化为平衡记分卡的考核指标,另一方面有助于将企业战略顺利传达给业务部门和员工,保持三者目标一致性。 第四步:设计平衡记分卡,开发CSF和KPI 关键成功因素(CSF是对企业成功起决定作用的某个战略要素的定性描述,关键业绩指标(KPI)是对CSF的定量描述,是定量指标。CSF和KPI在平衡记分卡中的同时应用,使得企业的战略目标来源于战略,符合实际并可以被计量,这也就使得企业的战略目标可以被控制。 第五步:实施和评估平衡记分卡绩效管理系统
平衡计分卡推行步骤 建立平衡计分卡是一个系统化的过程。需强调的是必须根据公司战略来制定平衡计分卡,再按照战略与平衡计分卡来制定战略的实施计划,而不是相反。否则平衡计分卡就成为对战略实施计划的监测工具和绩效管理工具,这与KPI没有什么区别。公司战略的制定虽不是本文所要解决的问题,但要明白公司在生命周期不同的阶段有不同的战略重点,如表1: 表1:处于生命周期不同阶段的公司的战略重点 平衡计分卡建设步骤如下: 第一步:前期准备 前期准备是战略绩效管理推进的第一步,主要工作内容包括:组建BSC推进团队、编制推进计划、进行前期的调查、宣传培训、收集所需信息资料。 1、BSC推进团队的组建:推进团队必须由公司总经理带领,由了解公司整体运作,熟悉各个职能领域现状的各部门经理/主管,以及拥有平衡计分卡与绩效管理专业知识的人力资源部参与(后期可聘请专业团队)。只有这样的团队组合才能保证这场管理变革的强大推动力。 2、推进计划:明确战略绩效管理推动的时间表,确保推进工作有条不紊的进行。主要包含工作活动内容、责任人、时间进度安排和产出成果等四个方面。 3、前期调查:主要为了澄清以下四个方面的问题:
1)全体员工对战略的认识与认同程度 2)全体员工对平衡计分卡与绩效管理的认识与认同程度 3)掌握公司现在绩效管理的现状:可见《公司绩效管理现状分析》 4)在公司内部发出一个信号:公司将进入平衡计分卡与绩效管理的时代 前期调查的方法:一是访谈法,二是问卷调查 详细可见《BSC访谈提纲》和《调查问卷模板》 4、宣传培训:明确推进BSC的意义,同时使管理层掌握战略绩效管理设计和操作技巧。 5、收集所需信息资料:信息来源于与内部与外部,目前以《商业计划书》为主要参考资料。 第二步:编制公司平衡计分卡和绩效计划 设计公司的平衡计分卡与绩效计划分两项工作: 1、第一项工作运用战略地图来描述公司战略,在此基础上可再细分为三个相互支持的细分步骤: 1)战略环境描述 运用工具:PESTEL、波特五力分析、竞争对标分析、企业内部价值链分析、SWOT分析等。 2)绘制公司层面战略地图 无论绘制哪个层面的战略地图,都应建立在前面战略环境扫描基础上,同时运用工具:BCG、GE矩阵、利益相关者需求分析、市场细分、核心能力界定等的支持。 3)设计图、卡、表文件 根据各层级“战略地图”转化为对应的“平衡计分卡”、“战略行动计划表”,图、卡、表是用来描述战略的三个必备文件。 【文件1】战略地图:是各层级战略描述的一个集成平台。 根据公司战略,设定四个方面的CSF(关键成功因素),如表2: 表2设计CSF应考虑的问题清单:
在设定好指标的权重和目标值之后,可拿出《绩效合同》的初稿与直接下级进行有效的沟通。总之,通过有效沟通,对《绩效合同》的内容达成共识。沟通方式是灵活的,可单独面谈,也可以会议形式集体沟通。 —签订《绩效合同》 在准备好前面的工作之后,组织签订《绩效合同》,双方确认签字,体现绩效管理的严肃性。对与合同的签订,管理人员可以组织签字仪式,在公司内宣传绩效管理思想,培养绩效考核文化;对基层可组织集体签订。 第三步:编制部门、员工平衡计分卡与绩效计划 部门绩效与员工绩效指标设计是指将公司经营绩效转化为部门、员工绩效的过程。 经营绩效:又称组织绩效,包括公司绩效、部门绩效,其监控部门为行政部。 员工绩效:是指个人绩效,监控部门为人力资源部。 两者虽有区别但又是关联的:员工绩效实施得好坏影响到部门乃至公司拟绩效的实现,而公司当期绩效的实现又影响到公司整体战略的实现。 在公司战略转化为经营绩效、部门绩效和员工绩效图、卡、表的过程中,可运用工具“绩效指标分解矩阵”、“内部利益相关者需求分析法”、“指标五因素分析法”、“绩效指标实操性检查”、“绩效指标解释表”整合在考核指标的设计之中。 绩效计划的具体操作与公司层面绩效计划的操作相同。 第四步:设计平衡计分卡与绩效管理运作系统 平衡计分卡与绩效管理设计的总体原则是“以流程为核心,制度与表单配套”主要由三方面内容构成: 1、平衡计分卡与绩效管理流程; 2、平衡计分卡与绩效管理制度; 3、平衡计分卡与绩效管理流程运作的表单。 以上三个方面的内容是相互联系、相互支持的:战略与绩效管理运作是按照一定的流程规则来执行的,它是日常运作的核心;制度和表单能支持设定的运作流程,是日常运作的支持性文件。 第五步:切换实施 本步骤是将设计的方案付诸实施,其中有三项活动应当特别注意: 1、组织设计方案的学习 在组织学习时,中层管理者的参与程度是最重要的。中层干部是公司的中流砥柱,在公司里祈祷承上启下的作用。推进平衡计分卡每个环节的工作都和中层管理者的参与程度息息相关,因为战略绩效管理工具最终要求他们在日常的管理中操作和使用。