
T HERAPY I N P RACTICE1170-229X/04/0010-0655/$31.00/0
Drugs Aging 2004; 21 (10): 655-675
? 2004 Adis Data Information BV. All rights reserved.
Sexual Dysfunction in the
Older Woman
An Overview of the Current Understanding
and Management
Kathleen E. Walsh1,2 and Jennifer R. Berman3
1University of Wisconsin School of Medicine, Madison, Wisconsin, USA
2The Monroe Clinic, Monroe, Wisconsin, USA
3Department of Urology, UCLA Medical Center, Los Angeles, California, USA
Contents
Abstract (656)
1.Sexual Activity and Aging (657)
2.Sexual Dysfunction and the Older Woman (658)
3.Classification of Female Sexual Dysfunction (658)
3.1Hypoactive Sexual Desire Disorder (658)
3.2Sexual Arousal Disorder (658)
3.3Orgasmic Disorder (659)
3.4Sexual Pain Disorders (659)
4.Female Sexual Response Cycle (659)
5.Hormonal Influence on Female Sexual Function (660)
5.1Testosterone (660)
5.2Estrogen (661)
6.Medical Risk Factors Associated with Sexual Dysfunction (661)
6.1Vascular (661)
6.2Hormonal (662)
6.3Neurogenic (662)
6.4Musculogenic (662)
6.5Psychogenic (663)
6.6Medications (663)
7.Physical Examination (663)
8.Treatment (664)
9.Hormonal Medications (665)
9.1Estrogen (665)
9.2Testosterone (665)
10.Investigational Medications and Devices (666)
10.1Phosphodiesterase Inhibitors (666)
10.1.1Sildenafil (666)
10.1.2Vardenafil (666)
10.1.3Tadalafil (669)
10.2Prostaglandin E1 (669)
10.2.1Alprostadil (669)
10.3Adrenoceptor Antagonists (669)
10.3.1Phentolamine (669)
10.4Yohimbine (670)
10.5Prostaglandin E1 and Adrenoceptor Antagonist (670)
10.5.1Arginine and Yohimbine (670)
10.6Neuropeptide and Adrenoceptor Antagonists (670)
10.6.1Vasoactive Intestinal Peptide and Phentolamine (670)
656Walsh & Berman
10.7Dopamine Receptor Agonists (670)
10.7.1Apomorphine (670)
10.8α-Melanocyte Stimulating Hormone (671)
10.8.1PT141 (671)
10.9Serotonin 5-HT Receptor Agonists (671)
10.9.1Flibanserin and VML670 (671)
10.10Selective Androgen Receptor Modulators (671)
10.11Selective Estrogen Receptor Modulators (671)
10.12Synthetic Steroids (671)
10.12.1Tibolone (671)
10.13Medical Devices (672)
10.13.1EROS-CTD? (672)
10.13.2InterStim? Therapy (672)
11.Conclusion (672)
Abstract
Sexuality is one of the most important quality of life issues for both men and
women. Sexual dysfunction is a highly prevalent, age-related and progressive
problem. The various physiological and psychological changes that occur with
aging can have a significant impact on sexual function. The complexity of female
sexual dysfunction remains distinct from that of a man. Thus, we cannot approach
female patients or their sexual function problems in a similar fashion to that of
male patients. A woman’s motivation and ability to find and respond to sexual
stimuli is largely influenced by her emotional intimacy with her partner. Frequent-
ly, the emotional and relationship well-being a woman experiences contributes
more to her sexual enjoyment than does her physiological response. However, it is
imperative to assess for possible physiological barriers a woman may have which
impede a healthy and satisfying sexual life. Therefore, a comprehensive approach,
addressing both the physiological and psychological factors is instrumental to the
evaluation of female patients with sexual complaints.
After years of ardent research and recent therapeutic advances in male sexual
dysfunction, researchers have begun addressing the intricacy of female sexual
complaints. Studies involving both pre- and postmenopausal women have report-
ed that most women do experience some type of sexual dysfunction during their
lifetime. The sexual complaints women experience in their younger years may
follow them into older adulthood, but often times change considerably because of
various age-related changes. In an effort to assist researchers and clinicians in
designing studies and implementing appropriate evaluation and treatment options
for women with sexual complaints, a classification system for female sexual
dysfunction has been designed. The four categories of female dysfunction include:
hypoactive sexual desire disorder, sexual arousal disorder, orgasmic disorder and
sexual pain disorders. Evaluation of women with sexual complaints should
include a detailed psychological, social and medical history and thorough physical
examination including a hormonal profile. Current treatment options are depen-
dent on the diagnosis and include physical therapy, psychological counselling,
hormonal supplements, medication changes and sexual devices. There has also
been a burgeoning interest in investigational medications for female sexual
dysfunction, from centrally acting (e.g. serotonin agonists) to peripheral, localised
treatment (e.g. vasodilating creams). The area of female sexuality and sexual
dysfunction has been undergoing important critical changes within the last 10
years. Researchers and clinicians are continuing to recognise the need to try and
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman657 understand both the psychological and physiological aspects of the female sexual
experience and how they influence one another.
Sexuality is an important quality-of-life issue in questionnaire that was distributed to 202 elderly the elderly.[1-3]In all individuals, particularly the men and women living in retirement facilities. For elderly, illness, medications and life stressors can both men and women, the most common activity have the potential to impact negatively on sexual was touching and caressing without sexual inter-function. Recent advances in understanding male course, followed by masturbation and, less frequent-sexual dysfunction and the available treatment op-ly, sexual intercourse. Of these activities, only tions have facilitated interest in sexual health issues touching and caressing showed a significant decline of women. Basic and social science research in from the 80s to the 90s, and more significantly in female sexuality and sexual dysfunction has also men.[11] In 1993, the Janus report found that whereas expanded over the past several years. As the interest men of all ages have a higher prevalence of sexual and achievement of studies in female sexuality have activity than women, activity for both groups con-increased, the inclusion of older women into these tinues past ‘middle age’. They also reported that studies is the next goal.when compared with earlier years, sexual activity
for women above the age of 65 years increases from
65% to 74%.[12]
1. Sexual Activity and Aging
The predictors of sexual activity and sexual satis-In this century, the rate of growth of the elderly faction in the elderly have been somewhat ambigu-population has greatly exceeded the growth rate of ous. Outcomes from several studies vary depending the population of US as a whole. The number of on the sample studied, the study design and the older Americans (aged 65 years and older) has in-definition of sexual activity and/or sexual satisfac-creased from 3.1 million in 1900 to 33.9 million in tion utilised. In general, the level of sexual activity 1990. In every age category over 65 years of age, the and satisfaction in later life appears to be related to number of women exceeds the number of men and the levels in earlier years. The inconsistent continues to widen with increasing age. Among predictors include age, marital status and gender. those aged 85 years and older, there are 44 men for Starr and Weiner[13] found that sexual frequency every 100 women. By the year 2030, it is projected among senior centre participants did not decline that 22%, or 70 million Americans will be 65 years sharply with age when compared with earlier data of age or older.[4,5]from the same cohort. From a sample of 744 elderly
men and women, Diokno et al.[14] reported that 74% Many of the earlier publications on aging and
of the married men were sexually active compared sexual function were by Kinsey et al.,[6] who report-
with 31% of unmarried men, and 56% of the married ed that the frequency of sexual intercourse de-
women were sexually active compared with 5% of creased with age, particularly in older women. Sub-
unmarried women.
sequent studies reported that there is a greater de-
cline in sexual interest, activity and desire in older Analysis of data from the National Survey of women, compared with older men.[7-10]However,Families and Households, which included 807 men these findings are not unexpected because nearly all and women over the age or 60 years, did not find any the earlier studies defined ‘sexual activity’ primarily gender differences in sexual frequency.[15] The study as intercourse. Therefore, previous studies may have reported that the physical and mental health status of reported a higher prevalence of older women who an individual are the independent predictors found were no longer sexually active. Several studies have to be more consistent with sexual activity and satis-since identified sexual activity in more general faction. Croft[16] found that the two major require-terms such as touching, caressing, kissing and mas-ments for enjoyable sexual activity in later life in-turbation. In 1988, Bretschneider and McCoy[11] de-clude an interested and interesting partner and rea-veloped a self-administered 117-item sexuality sonable good health. In a study focusing on older
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
658Walsh & Berman women, the absence of illness was found to be an 3. Classification of Female
important predictor associated with maintaining Sexual Dysfunction
sexual interest.[17] Analysis of data collected from
In 1998, the American Foundation of Urologic the Medicare Screening and Health Promotion Trial,
Disease Consensus Panel classified female sexual which included 1216 elderly men and women, re-
dysfunction into four categories: desire, arousal, ported that the predictors for sexual activity were
orgasmic and sexual pain disorders.[22]
younger age, male gender and good social net-
works.[3] The predictors for sexual satisfaction in-
3.1 Hypoactive Sexual Desire Disorder cluded good mental health, better functional status
Hypoactive sexual desire disorder is the persis-and female gender.
tent or recurring deficiency (or absence) of sexual
fantasy thoughts and/or receptivity to sexual ac-
2. Sexual Dysfunction and the
tivity, which causes personal distress. The cause Older Woman
may be either physiological, psychological or a
combination of both. Common physiological aeti-Sexual dysfunction has been recognised as a
ologies include hormone deficiencies and medical common medical problem in both sexes and in all
or surgical interventions. Any disruption of the fe-age groups. Large population-based studies of sexu-
male hormonal milieu caused by natural menopause, al dysfunction do exist. However, the majority of
surgically or medically induced menopause, or en-these studies have focused on men and erectile dys-
docrine disorders can result in inhibited sexual de-function. There are a limited number of studies that
sire.[23,24] The lack of sexual desire may also be have addressed sexual dysfunction in women,
secondary to poor sexual arousal, response or pain. particularly older women.
Hypoactive sexual desire is sometimes a psycholog-Data from the National Health and Social Life
ically or emotionally based problem that can result Survey, a study of adult sexual behaviour in the US,
from a variety of reasons beyond a history of sexual found that sexual dysfunction is more prevalent in
abuse or trauma. For instance, depression and the women (43%) than in men (31%). The survey in-
treatment of depression are common problems in cluded 1749 women between the ages of 18 and 59
patients with low sexual desire. Depression can be years. The younger women in the group had a higher
caused by general life events or it can be secondary prevalence of low libido, difficulty with orgasm and
to sexual conflicts in the relationship.[25] Lack of pain during sexual activity compared with the older
sexual arousal can also be secondary to substance women. Older women had more complaints of
abuse, particularly drug and alcohol abuse, resulting trouble lubricating.[18]
in problems of dependency, depression, and lack of
A community-based study involving individual
self-esteem.
interviews with 185 women attending a menopause
Uneven sexual desire in a relationship can also clinic, found that 68% reported sexual problems.
have significant impact on sexual arousal. If one The women described disorders of sexual desire,
partner contains feelings of anger, resentment, fear, sexual response and sexual behaviour.[19] In a study
hostility or disappointment, the results can be a of 329 women, aged 18–73 years, a standardised
withdrawal from the intimate relationship. A con-sexual function questionnaire identified 38.1% with
flicting relationship of long-term with a struggle for anxiety or inhibition during sexual activity, 16.3%
control may result in further voluntary blocking of lacked sexual pleasure and 15.4% had difficulty
sexual appetite perpetuated by the partner who feels achieving orgasm.[20]
less valued or less powerful.[26] Of the 130 postmenopausal women interviewed
in the Yale midlife study, 68% reported having
3.2 Sexual Arousal Disorder
sexual problems. Specific complaints included vagi-
nal dryness (58%), dyspareunia (39%) and a de-Sexual arousal disorder is the persistent or recur-crease in clitoral sensitivity (36%), orgasmic inten-ring inability to attain or maintain adequate sexual sity (35%) and orgasmic frequency (29%).[21]excitement, causing personal distress. It may be
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman659 experienced as a lack of subjective excitement or a the primary care setting, many women describing lack of genital (lubrication/swelling) or other somat-themselves as anorgasmic are in fact experiencing ic responses. Disorders of sexual arousal include,coital anorgasmia. The majority of heterosexual but are not limited to, lack of or diminished vaginal women and their partners believe that they should be lubrication, decreased clitoral and labial sensation,able to obtain orgasm through sexual intercourse. decreased clitoral and labial engorgement, or lack of When this belief, held by either the man or the vaginal smooth muscle relaxation. There is a woman, is incompatible with the actual stimulation medical/physiological basis for these sexual arousal needs of the woman, failure to achieve this goal can disorders such as diminished vaginal/clitoral blood result in sexual dissatisfaction, relationship conflict flow, prior pelvic trauma, pelvic surgery or medica-and a lack of sexual confidence.[32,33]
tions (see section 6). These conditions may also
occur secondary to psychological factors. If the wo-
3.4 Sexual Pain Disorders
man is struggling with body image issues that create
Sexual pain disorders include dyspareunia (geni-self-consciousness in certain sexual situations, her
tal pain with intercourse), vaginismus (involuntary response will be inhibited. Additionally, if she has
muscle spasms of the outer third of the vagina) and low self-esteem, lack of confidence, depression,
other (genital pain caused by noncoital sexual stimu-stress or anxiety her general emotional state may
lation).[22] Pelvic floor disorders can cause pain with preclude her from relaxing into the sexual arousal
sexual activity.[34,35] Disorders of the pelvic floor process.[27,28]
include urinary incontinence, cystocele, rectocele,
enterocele, and vaginal and uterine prolapse. Older
3.3 Orgasmic Disorder
women are at increased risk of pelvic floor disorders Orgasmic disorder is the persistent or recurrent because of muscular and vascular changes asso-difficulty, delay in, or absence of attaining orgasm ciated with age and childbirth. Other aetiological following sufficient sexual stimulation and arousal,explanations for sexual pain disorder include pre-which causes personal distress. Orgasmic disorder vious obstetric or gynaecological trauma to the vagi-may be a primary (never achieved orgasm) or secon-na, radiation atrophy, inflammation of the urinary dary condition (was able to achieve orgasm at one tract, rectum or vagina and fixation of pelvic tis-point in time, but now no longer able). Primary sues.[36,37]
orgasmic disorder is typically secondary to emotion-Psychological issues can play a significant role in al trauma or sexual abuse. Secondary orgasmic dis-patients presenting with dyspareunia. Elements of order is often a result of surgery, trauma or hormone fear, anxiety, and intimacy problems are often iden-deficiencies.tified. Interpersonal conflict can be a primary con-Orgasmic disorder can also be situational, refer-tributing factor in approximately one-third of the ring to the woman who can experience orgasm in cases of dyspareunia.[38] These relationships are cha-some circumstances (e.g. masturbation), but cannot racterised by poor communication, with special dif-in other situations. Situational orgasmic disorder,ficulty in talking about sex and emotions. Psycho-while often also associated with a history of trauma,logical pressure to ‘perform’ sexually can be pre-is also commonly related to emotional stressors and sent, especially when sexual intercourse is the relationship conflicts. However, in both of these primary or sole source of sexual pleasure and coital cases, medical/physical factors, as well as medica-orgasm is a measure of intimacy for one or both tions (e.g. selective serotonin reuptake inhibitors partners.
[SSRIs]), can contribute to, or exacerbate the prob-
lem (see section 6). Coital orgasmic disorder is 4. Female Sexual Response Cycle another kind of anorgasmia commonly experienced
by women. It is the inability to achieve orgasm from Masters and Johnson[39] first characterised the coital thrusting without added sexual stimulation. It female sexual response cycle in 1966. The cycle is estimated that only 30% of women experience consisted of four consecutive phases: excitement, orgasm regularly from sexual intercourse.[29-31]In plateau, orgasm and resolution. In 1974, Kaplan[40]
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
660Walsh & Berman
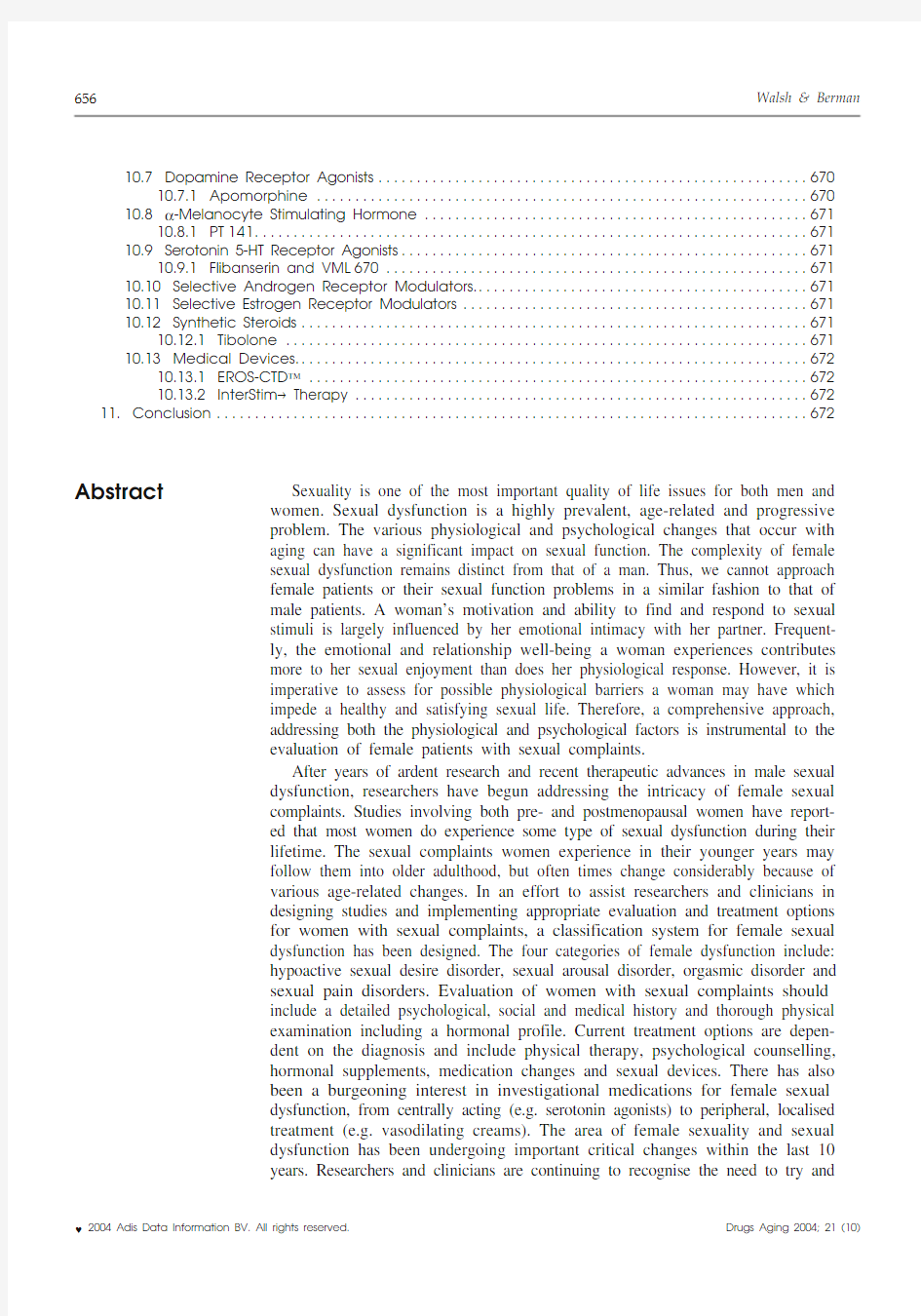
Fig. 1. Five-phase model of female sexual response cycle (reproduced from Basson,[41] with permission from Taylor & Francis, Inc.; http:// https://www.doczj.com/doc/512379057.html,).
proposed a three-phase model, which included sexu-decreases with age. Testosterone levels in a 20-year-al desire, sexual arousal and orgasm. Both of these old female are approximately two times greater than female sexual response cycles depict excitement or in a 40-year-old female. Approximately 50% of the sexual desire as a spontaneous force that by itself daily testosterone synthesis is by the adrenal glands stimulates sexual arousal. In contrast to these cycles,and ovaries. Circulating androstenedione is respon-a five-phase model focusing on intimacy has been sible for formation of the remaining 50% of testos-proposed by Basson (figure 1).[41] Basson suggests terone. Testosterone is carried in the peripheral that for a large majority of women, the wish to blood bound to sex hormone-binding globulin enhance intimacy is the driving force of the female(SHBG). The ovaries and adrenal glands both pro-sexual response cycle. The cycle begins with basic duce androstenedione and DHEA. The adrenal intimacy needs, which include mutuality, respect glands are also the main source of DHEA-S. Testos-and communication. When these needs are met, a terone is metabolised to androgen dihydrotestoster-woman will seek out and will be more receptive to one or aromatised to estradiol (E2) in the peripheral sexual stimuli. The model hypothesises a receptive tissues and target organs.[42]
sexual desire, which stems from sexual arousal and a Only 1–2% of total testosterone circulates un-woman’s conscious choice of sexual stimuli. If there bound. The remainder is bound by SHBG or albu-is an overall positive emotional and physical inter-min. The nonbound (free) testosterone is biological-action, a woman’s intimacy is enhanced and the ly active. In women who have undergone a bilateral-cycle strengthened.[41]ly oophorectomy, testosterone and androstenedione
levels decrease by 50%. DHEA and DHEA-S levels
5. Hormonal Influence on Female
also decrease with age, which further contributes to Sexual Function
the decline in testosterone.[42,43]
Within the central nervous system, testosterone
5.1 Testosterone
has been shown to affect female sexual beha-
viour.[44,45] Low levels of testosterone are associated The major androgens in women, in order of de-
with decreased sexual arousal, libido, sexual respon-scending serum concentration, include dehydroepi-
siveness, genital sensation and orgasm.[46,47] Recent androsterone sulfate (DHEA-S), dehydroepiandros-
evidence suggests that testosterone may help pro-terone (DHEA), androstenedione, testosterone and
mote the expression of endothelial nitric oxide dihydrotestosterone. The mean circulating level of
synthase, the enzyme responsible for the production testosterone, the most potent androgen, gradually
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman661 of nitric oxide which promotes vascular smooth flow.[54] Low E2 levels are associated with thinning muscle relaxation and vascular engorgement.[48]of mucosal epithelium, atrophy of vaginal wall
smooth muscle and an increase in vaginal pH. The There is no direct regulator, stimulator or feed-
less acidic environment within the vaginal canal can back mechanism of androgen production in women.
lead to vaginal infections, urinary incontinence, An increase in ovarian activity or adrenal activity
urinary tract infections and sexual dysfunction.[55] has been shown to cause a rise in androgen produc-
Levels of E2 below 50 pg/mL have been directly tion.[49] In addition to aging, androgen deficiency in
correlated with increased sexual complaints.[56] women can be caused by a number of factors, in-
cluding adrenal, pituitary or ovarian surgery. Condi-Estrogen has also been shown to play a role in tions such as hypopituitarism, adrenal insufficiency,regulating vaginal and clitoral nitric oxide anorexia nervosa, exercise-induced amenorrhoea synthase.[57] In animal models, aging and surgical and premature ovarian failure can also cause andro-castration are associated with decreased vaginal and gen deficiency. Lower androgen levels can occur in clitoral nitric oxide synthase expression, and apop-women taking exogenous corticosteroids and in tosis in vaginal smooth muscle and mucosal epithe-women with chronic illness. Oral administration of lium. Estrogen replacement restored vaginal muco-hormones that elevate SHBG levels and reduce sal health, nitric oxide synthase expression and de-bioavailable androgens can place women at risk of creased vaginal cell death.[58] These findings suggest androgen deficiency. Increased levels of E2, such as that medications such as sildenafil, which increases with the use of oral contraceptive pill or hormone levels of nitric oxide, may have a potential role in replacement therapy (HRT), can increase SHBG,the treatment of female sexual dysfunction, partic-therefore, decreasing biologically available testos-ularly sexual arousal disorder.
terone.[50,51] Measurement of both total and free
6. Medical Risk Factors Associated with testosterone levels in females remains a challenge
Sexual Dysfunction
secondary to the insensitivity of current assays. Cur-
rent commercial assays were developed to measure
Current evidence suggests that up to 60% of the much higher circulating concentrations in men
cases of sexual dysfunction may have some type of and do not take into account the cyclical variation of
organic component. The conditions that have been testosterone in women.
associated with sexual dysfunction (table I) are dis-
cussed in this section.
5.2 Estrogen
In premenopausal women, the ovaries are the 6.1 Vascular
principle source of estrogen. More than 60% of
estrogen is E2 secreted directly by the ovaries and Males and females can experience sexual dys-the remainder is estrone derived from extraglandular function secondary to diabetes mellitus, cardio-conversion of androstenedione. After menopause,vascular disease, hypertension, peripheral vascular the ovarian contribution is reduced and extraglandu-disease and tobacco abuse.[59,60] Diminished blood lar formation of estrone from adrenal androstene-flow in the iliohypogastric/pudendal arterial bed dione predominates.[52]leads to significant compromise in both male and Female sexual function is strongly influenced by female genitalia.[61,62] In females this is termed vagi-estrogen. Both the neurological and vascular sys-nal and clitoral vascular insufficiency syndrome.[63] tems are affected by circulating levels of estrogen.Sufficient blood flow is crucial for maintaining vas-In postmenopausal women, estrogen replacement cular and muscular integrity, both integral compon-has been found to restore clitoral and vaginal vibra-ents in sexual arousal. Diminished blood flow can tion and pressure thresholds to premenopausal lead to vaginal wall and clitoral smooth muscle levels.[53]The vasoprotective and vasodilatory ef-fibrosis that can result in symptoms of vaginal dry-fects of estrogen have also been demonstrated. Es-ness and dyspareunia. Pelvic fractures, blunt trauma, trogen replacement therapy has been shown to in-surgical disruption, radiation or chronic perineal crease vaginal, clitoral and urethral arterial blood pressure from bicycle riding can all lead to dimin-
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
662Walsh & Berman
regulating female sexual function. There is a decline in both estrogen and testosterone levels with age,although the decline in testosterone is much less pronounced. A decrease in estrogen levels is asso-ciated with adverse neurovascular events affecting vaginal, clitoral and urethral tissues.[64,65] Low tes-tosterone levels in females have been associated with a decline in sexual arousal, genital stimulation,libido and orgasm. Therapy with combination es-trogen-androgen compared with estrogen alone has shown to enhance libido, sexual desire, motivation and overall sense of well-being.[66]
6.3 Neurogenic
Neurogenic sexual dysfunction can occur in both men and women with spinal cord injury, or disease of the central or peripheral nervous system. In a study comparing premenopausal women with spinal cord injury, <50% of women with spinal cord inju-ries were able to achieve orgasm, compared with 100% of able-bodied women.[67] The study also reported that only 17% of women with complete lower motor neuron dysfunction affecting the S2–S5spinal segments were able to achieve orgasm, com-pared with 59% of women with other levels of spinal cord injury. Time to orgasm was also significantly increased in women with spinal cord injuries.[67]Women with complete upper motor neuron injuries affecting sacral spinal segments had difficulty achieving psychogenic lubrication.[68] Focus group studies examining diabetes and female sexuality identified complaints of increased fatigue, vaginitis,decreased sexual desire, decreased vaginal lubrica-tion and an increased time to reach orgasm.[69,70]
Table I. Medical risk factors associated with sexual dysfunction Vascular Diabetes mellitus Atherosclerosis Hypertension Lipid disorders
Peripheral vascular disease Hormonal Hypogonadism Hyperprolactinaemia Hypothyroidism Hyperthyroidism Neurogenic Spinal cord injury Multiple sclerosis Musculogenic
Pelvic floor muscle hyper- or hypotonicity Medications a
Antihypertensive drugs Chemotherapeutic drugs CNS drugs
Drugs affecting hormones Psychogenic Depression
Anxiety/obsessive-compulsive disorder Social stressors Religious inhibitions
Post-traumatic sexual experiences Dysfunctional attitudes about sex Other
Autoimmune disorders Renal disease (dialysis)Bowel disease (colostomy)
Bladder disease (urinary incontinence, cystitis)Skin disorders (contact dermatitis, eczema)a
For details of medications see table II.
6.4 Musculogenic
ished vaginal and clitoral blood flow and sexual dysfunction.
The levator ani and perineal membrane make up the pelvic floor musculature that influence female 6.2 Hormonal
responsiveness during sexual activity. The perineal In females, the most common causes of primary membrane consists of the bulbocavernous and ischi-endocrine abnormalities include menopause, surgi-ocavernosus muscles. These muscles contract both cal or medical castration, premature ovarian failure,voluntarily and involuntarily, intensifying sexual dysfunction of the hypothalamic-pituitary axis and arousal and orgasm. The levator ani muscles are long-term birth control use. The percentage of involved in modulating motor responses during vag-women with a primary endocrine dysfunction re-inal receptivity and orgasm. Hypertonicity in the sponsible for their sexual dysfunction is unknown.muscles can occur secondary to trauma (surgery,Estrogen and testosterone play a significant role in
radiation, and childbirth) and aging. This can cause
? 2004 Adis Data Information BV. All rights reserved.
Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman663 vaginal hypoanaesthesia, coital anorgasmia or urin-important to remember that even if the primary
ary incontinence during sexual intercourse or or-aetiologic domain is physiological, there are emo-
gasm. Hypertonicity of the levator ani muscles can tional and relationship issues that are often out-
cause sexual pain disorders such as vaginismus that growths to the problem and should not be ignored.
leads to dyspareunia.[71,72]
6.6 Medications
6.5 Psychogenic There are approximately 1.5 billion prescriptions
written every year in the US. One or more new It is important to remember that, in women, de-
prescriptions are written in over two-thirds of physi-spite the presence or absence of organic disease,
cian office visits.[76] While many prescription medi-psychological issues can significantly affect sexual
cations have been implicated in causing sexual dys-function. In every woman with a sexual complaint,
function, the antihypertensives, antidepressants and there are relationship, emotional and medical factors
antipsychotic medications are those most frequently occurring simultaneously and interacting with one
cited.[77] Controlled research is limited for the ma-another in a nonlinear fashion. From the relationship
jority of medications and substances believed to standpoint, partner’s sexual dysfunction, lack of
cause female sexual dysfunction. Many articles pre-communication, relationship conflict and lack of
sent only subjective evidence or case reports. The information about sexual stimulation can all impact
classes of medications most commonly associated on the sexual response of a woman. Furthermore,
with causing sexual dysfunction are listed in table II. when a woman is struggling with a sexual function
complaint, it may create conflict in the relationship,7. Physical Examination
which then cycles back to negatively affect her
sexual function.[73] The same is true for the emotion-Every patient complaining of sexual dysfunction
al aspect of the equation. Additional mood disorders should undergo a thorough physical examination,
and psychological stressors include depression, low including an external and internal gynaecological
self-esteem, anxiety, obsessive-compulsive disor-examination. During the external gynaecological
der, chronic stress and a history of sexual abuse, all examination, assessment of perineal muscle tone
of which can negatively impact on the sexual func-(ischiocavernosus and bulbocavernosus), skin col-
tion of a woman.[74,75]A psychosexual assessment is our, turgor and texture, and pubic hair distribution
strongly encouraged as part of the work-up for can identify conditions such as vaginismus, vulvar
women with complaints of sexual dysfunction. It is dystrophy, dermatitis and vaginal atrophy. Examin-Table II. Common classes of medications causing sexual dysfunction as an adverse effect
Class Examples
Antihypertensive drugsα1- and α2-adrenoceptor antagonist (clonidine, reserpine, prazosin)
β-adrenoceptor antagonists (metoprolol, propranolol)
Calcium channel antagonists (diltiazem, nifedipine)
Diuretics (hydrochlorothiazide)
Chemotherapeutic drugs Alkylating agents (busulfan, chlorambucil, cyclophosphamide)
CNS drugs Acetylcholine receptor antagonists (diphenhydramine)
Antiepileptic drugs (carbamazepine, phenobarbital, phenytoin)
Antidepressants (monoamine oxidase inhibitors, tricyclic antidepressants, selective serotonin reuptake
inhibitors)
Antipsychotics (phenothiazines, butyrophenones)
Opioids (oxycodone)
Sedatives/anxiolytics (benzodiazepines)
Drugs affecting hormones Antiandrogens (cimetidine, spironolactone)
Antiestrogens (tamoxifen, raloxifene)
Oral contraceptives
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
664Walsh & Berman ation of the posterior forchette and hymenal ring can tations. Lid lag, exophthalmos, hyperreflexia, tre-
mor and tachycardia may be present on clinical help recognise episiotomy scars and possible stric-
examination. Laboratory values include a decreased tures. The monomanual examination should include
TSH and an increased free T4.
palpation of the rectovaginal surface, levator ani and
bladder/urethra in order to identify any rectal dis-Cushing’s syndrome is diagnosed on clinical ease, levator ani myalgia, vaginismus, urethritis,examination by easy bruising, weight gain, truncal cystitis or urinary tract infections. Cervical motion obesity, ‘moon face’, ‘buffalo hump’ and striae. An tenderness may indicate infection or peritonitis. Pal-elevated overnight dexamethasone suppression test pation of the uterus and adnexa are included in the is needed for confirmation of clinical examination. bimanual examination and assist in the identifica-Diabetic patients should be evaluated for peripheral tion of uterine retrogression, fibroids, adnexal mass-neuropathy, retinopathy and abnormal body mass es/cysts and possible endometriosis.index.
Finally, the speculum examination is utilised to A thorough neurological examination is neces-evaluate for discharge, pH, vaginal mucosa, Papan-sary in patients who have known or suspected spinal icolaou smear, and vaginal and uterine prolapse.cord injury, nerve injury (prostate surgery, hysterec-Vaginal pH, an indirect measurement of lubrication,tomy, childbirth), peripheral neuropathy, multiple can be measured using a digital pH probe.sclerosis or Parkinson’s disease. The neurological
examination may uncover sensory or motor impair-Decreased pulses, bruits, elevated blood pressure
ment that will account for residual urine (neuro-and cool extremities are suggestive of vascular dis-
pathic bladder) or urinary incontinence as the blad-ease. Assessment should include a lipid profile and
der and its sphincter are innervated by S2–S4 spinal Doppler examinations.
segments. Somatic function of the spinal cord levels The suggested baseline hormonal profile in-S2–S4 is assessed by touching the perianal skin or cludes follicle stimulating hormone (FSH), luteinis-placing a finger in the patient’s rectum and noting ing hormone (LH), total and free testosterone levels,contraction of the external anal sphincter muscles. SHBG levels, E2 and prolactin levels. Measure-This is termed the bulbocavernosus reflex.
ments of FSH and LH can assist in evaluating for
primary versus secondary hypogonadism. High
levels of FSH and LH are suggestive of primary8. Treatment
gonadal failure, and low or normal levels indicate
hypothalamic or pituitary disease. Low levels of
In patients with sexual dysfunction where an estrogen and testosterone have been associated with
underlying medical condition has been diagnosed, decreased libido, diminished genital sensation, vagi-
treatment to correct or control progression of the nal dryness, dyspareunia and decreased sexual
medical condition is appropriate; however, patients arousal.[78,79] Hyperprolactinaemia can be seen in
should be made aware that treatment of their patients with decreased libido, galactorrhoea, visual
medical condition does not guarantee the elimina-complaints and headaches. Physical examination is
tion of their sexual dysfunction. Consideration sometimes positive for bitemporal hemianopsia. A
should be given to discontinuation of any med-CT or magnetic resonance imaging may be needed
ication suspected of contributing to sexual dysfunc-to assess the pituitary gland.
tion or, if possible, switching to an alternative med-Fatigue and cold intolerance are seen in patients ication. For patients with a component of psycho-with hypothyroidism. Examination for a possible genic dysfunction, referral to a psychologist or goiter, myxoedema, dry skin and coarse hair is war-psychiatrist with expertise in sexual dysfunction ranted. An increased thyroid-stimulating hormone may be beneficial. There are identifiable (TSH) and decreased free thyroxine (T4) are seen on‘psychosexual red flags’ that warrant referral for laboratory tests. Hyperthyroidism can present with further assessment and appropriate therapy (see
table III).
heat intolerance, weight loss, diaphoresis and palpi-
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman 665
there may be a transitory increase in coronary risk after starting hormone therapy in women with estab-lished coronary heart disease, and a decreased risk thereafter. The Women’s Health Initiative (WHI)was another large study encompassing several clin-ical trials of hormone replacement. A particular section of the study, which included a trial of conju-gated equine estrogen 0.625mg, and medroxypro-gesterone 2.5mg (Prempro ?1, Wyeth Ayerst, Phila-delphia, PA, USA), was stopped early because of adverse effects. The women in the study were aged 50–79 years and had reported no history of cardio-vascular disease.[83] After an average follow-up of Table III. ‘Psychosexual red flags’ that warrant referral for further assessment and appropriate therapy a The symptoms are life-long, not acquired
The symptoms are situational (e.g. do not exist when stress is removed or when with another partner)
The patient has a history of sexual abuse or trauma The patient has a psychiatric history
The patient has a history of, or is presently experiencing,depression and/or anxiety or stress
The couple experiences relationship conflicts (e.g. lack of intimacy, conflict, etc.)
The partner has a sexual dysfunction a
None of these factors guarantee the problem is
psychosexually based, but simply point to a need for further clarification by a trained sex therapist.
5.2 years, the HRT group compared with placebo had a higher annual incidence of coronary heart 9. Hormonal Medications
disease (0.37% vs 0.30%; number needed to harm [NNH] = 1429), invasive breast cancer (0.38% vs 0.30; NNH = 1250), stroke (0.29% vs 0.21%; NNH 9.1 Estrogen
= 1250) and venous thromboembolic disease (0.34%vs 0.16%; NNH = 556). All of the differences,Medical management of sexual dysfunction in except thromboembolic disease, lost statistical sig-women has focused on hormonal treatment. Both nificance when adjusting for multiple comparisons.estrogen and testosterone are being used alone and There was no difference in overall mortality and in combination. In postmenopausal women, es-cancer-related mortality between the two groups. It trogen replacement has been found to improve clito-remains uncertain whether there are similar risks ral and vaginal sensitivity, increase libido, restore with lower doses of estrogen and/or progesterone, or vibratory and pressure thresholds, and decrease whether estrogen treatment alone will cause the symptoms of vaginal dryness and pain during inter-same outcomes.[84]
course.[56,80] Estrogen is available in several forms,including oral tablets, dermal patch, vaginal ring and 9.2 Testosterone
cream. The vaginal ring is a therapeutic option for women with breast cancer who are unable to take Testosterone supplementation has been shown to oral or transdermal estrogen.
improve mood and well-being both in women with natural menopause and in women with surgical Estrogen, especially when begun early in meno-menopause.[66,85] Women treated with testosterone pause, has been shown to be beneficial in the pre-and intramuscular estradiol were found to have im-vention and treatment of osteoporosis.[81] Estrogen provements in sexual desire, fantasy, sexual arousal replacement therapy has also been shown to signifi-and orgasm.[47,53,86] Decreased testosterone levels cantly reduce the risk of colon cancer, but not rectal can be seen in women with premature ovarian fail-cancers.[81] Postmenopausal estrogen replacement ure and following natural, surgical or postch-has a generally favourable impact on lipids, im-emotherapy-induced menopause.
proves endothelial function, and has anti-inflamma-tory and antioxidant effects. However, estrogen plus For replacement purposes, testosterone is avail-progestogen supplementation is not without risk.able in oral tablet form, sublingual, dermal patch The results of the Heart and Estrogen/Progestin Re-and cream. Oral methyltestosterone is available in placement Study (HERS) found no overall reduction the US either alone or in combination with estrogen in coronary events among women assigned to active (Estratest ?, Solvay Pharmaceuticals, Brussels,hormone treatment.[82] It was also suggested that
Belgium). In postmenopausal women who experi-
1
The use of trade names is for product identification purposes only and does not imply endorsement.
? 2004 Adis Data Information BV. All rights reserved.
Drugs Aging 2004; 21 (10)
666Walsh & Berman ence inhibited sexual desire, dyspareunia or lack of mediated pathway, thus promoting smooth muscle vaginal lubrication, testosterone can be prescribed in relaxation and vascular engorgement. Theoretically, combination with estrogen. The transdermal testos-sildenafil should also enhance the vaginal engorge-terone patch is under clinical investigation. The ment and lubrication response in women through patches contain testosterone 150μg. Two patches are smooth muscle relaxation. Literature on the use of applied simultaneously twice weekly and prelim-sildenafil in women with sexual arousal disorder has inary results have been promising.[87,88]mixed results. In one large randomised, placebo-
controlled trial, a total of 577 estrogenised and 204 Topical preparations of testosterone can be made
estrogen-deficient women were randomised to re-in 1%, 2% and 3% formulations, and can be applied
ceive sildenafil (10, 50 or 100mg). The results, up to three times per week. Benefits from testoster-
based on several questionnaires, demonstrated no one therapy include improved libido, increased vag-
overall improvement in sexual response.[91] A ran-inal and clitoral sensitivity, increased vaginal lubri-
domised, placebo-controlled trial involving 51 cation and heightened sexual arousal. Adverse ef-
premenopausal women with sexual arousal disorder, fects of testosterone use that need to be monitored
coupled with normal sexual desire, demonstrated for in women include weight gain, clitoral enlarge-
improvement in self-reported sexual arousal inde-ment, increased facial hair and hypercholesterol-
pendent of the dose of sildenafil (25mg vs 50mg).[92] aemia. Measurement of testosterone levels before
There are a limited number of studies involving and after therapy, lipid panels (cholesterol, trig-
postmenopausal women and sildenafil. In one open-lyceride, high-density lipoprotein-cholesterol, low-
label, nonrandomised study, 33 postmenopausal density lipoprotein-cholesterol) and liver function
women with sexual dysfunction received sildenafil tests are recommended.[89,90] Although the studies
50mg (mean usage approximately three times per described earlier reported improvement in symp-
week). They reported no overall improvement in toms (e.g. libido, sexual arousal), there is a definite
sexual function, but there were changes in vaginal need for larger randomised, controlled studies to
lubrication and clitoral sensitivity.[93] In a recently help determine with more certainty the risks, bene-
published study, 34 estrogenised postmenopausal fits and appropriate dosages and routes of testoster-
women (each woman had been receiving at least 6 one supplementation. Whether or not testosterone
weeks of estrogen therapy) with acquired genital therapy in premenopausal women is beneficial for
disorder and impaired orgasm were randomised to sexual dysfunction is under investigation.
receive either sildenafil 50mg or placebo.[94] In the
10. Investigational Medications laboratory session, the investigators reported in-
and Devices creased subjective sexual arousal in all women
during visualisation of an erotic video. However, Secondary to the increase in both clinical and across all women, sildenafil improved neither sexual biological research in female sexual dysfunction,arousal nor orgasm.[94] A number of smaller trials several new medications and devices are now being have reported improvement in sexual functioning investigated in both pre- and postmenopausal with the use of sildenafil in women with sexual women (see table IV). Information regarding several dysfunction related to aging and menopause, spinal of these investigational medications is provided in cord injury and SSRI antidepressant use.[95-97]
this section.
10.1.2 Vardenafil
In August 2003, the US FDA approved
10.1 Phosphodiesterase Inhibitors
vardenafil for the treatment of erectile dysfunction
10.1.1 Sildenafil in men. Vardenafil is a selective inhibitor of cGMP-
Sildenafil is a selective phosphodiesterase (PDE)specific PDE5. Vardenafil is reported to act quickly type 5 inhibitor used for the treatment of male and with few adverse effects. It is presently targeted erectile dysfunction. It works by decreasing the cat-for men who have undergone nerve-sparing prosta-abolism of cyclic guanosine monophosphate tectomy procedure. Vardenafil is reported to be (cGMP), the second messenger in the nitric oxide more specific to PDE5. PDE5 is localised to the
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman
667
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Table IV. Investigational drugs and devices for sexual dysfunction in pre- and postmenopausal women a Drug/device Developing company
Mechanism of action Known and/or probable action Intended use
Sildenafil (tablet)Pfizer, Inc., New York, NY, USA PDE5 inhibitor Genital smooth muscle FSAD
relaxation and vasodilation Male ED (FDA approved)Tadalafil (tablet)Eli Lilly, Indianapolis, IN, USA PDE5 inhibitor Genital smooth muscle FSAD relaxation and vasodilation Male ED
Vardenafil (tablet)Bayer Pharmaceuticals, Wuppertal,PDE5 inhibitor Genital smooth muscle FSAD
Germany
relaxation and vasodilation Male ED (FDA approved)Alprostadil ([Alista ?]Vivus Inc., Mountain View, CA, USA
PGE 1 analogue
Genital vasodilation and FSAD
cream)
increased sensation
Currently used for male ED: topical, transurethral insert (FDA approved)Alprostadil ([Femprox ?]NexMed, Inc., Princeton, NJ, USA PGE 1 analogue
Genital vasodilation and FSAD cream)
increased sensation Phentolamine (tablet,Zonagen, Inc., The Woodlands, TX,α1- and α2-adrenoceptor antagonist Genital smooth muscle FSAD injection)
USA
relaxation and vasodilation Male ED Yohimbine (tablet)Various pharmaceutical companies α2-adrenoceptor antagonist Genital smooth muscle FSAD relaxation and vasodilation Male ED HMP 12 (tablet)Molecular Design International,α1- and α2-adrenoceptor antagonist Genital smooth muscle FSAD Memphis, TN, USA
relaxation and vasodilation Male ED NM1870 (tablet)NitroMed, Inc., Bedford, MA, USA Nitric oxide precursor and Genital smooth muscle FSAD α2-adrenoceptor antagonist relaxation and vasodilation Vasoactive intestinal Senetek PLC, Napa, CA, USA Synthetic version of brain Enhance genital lubrication,FSAD peptide (cream)neuropeptide
sensation and vasodilation Male ED
Uprima ? (tablet)
TAP Pharmaceutical Products Inc.,Short-acting dopamine D 2 receptor Targets the brain and Female and male sexual Lake Forest, IL, USA
agonist
stimulates the release of arousal and desire dopamine, increasing libido disorders
PT 141 (nasal spray)
Palatin Technologies, Inc., Cranbury,Synthetic α-melanocyte stimulating Target the brain stimulating the Female and male sexual NJ, USA
hormone
melanocortin-4 receptors, and arousal and desire increase in sexual arousal and disorders
libido
VML 670 (tablet)Vernalis Group plc, Winnersh, UK Serotonin 5-HT 1A receptor agonist Improve sexual libido Female and male SSRI-induced sexual dysfunction Flibanserin (tablet)
Boehringer Ingelheim Pharma KG,5-HT 1A , 5-HT 2A receptor agonist
Improve sexual libido
Female and male SSRI-Ridgfield, CT, USA
induced sexual dysfunction
Continued next page
668
Walsh & Berman
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Table IV. Contd Drug/device Developing company Mechanism of action
Known and/or probable action Intended use
Tibolone (tablet)
Organon, Roseland, NJ, USA
Tissue-selective estrogen agonist b
Approved in Europe for Menopausal symptoms,menopausal symptoms;osteoporosis, FSAD,improved mood and libido FSDD
(Estrogen [Premarin ? or Wyeth, Madison, NJ, USA; Mead Estrogen agonist
Restore estrogen levels;Menopausal symptoms,Estrace ?] cream)
Johnson Laboratories, Evansville,improves menopausal
FSAD, FSOD
IN, USA
symptoms (genital dryness and irritation)
(Estrogen [Vagifem ?]Pharmacia Upjohn, Kalamzoo, MI,Estrogen agonist
Restore estrogen levels;Menopausal symptoms,cream)
USA
improves menopausal
FSAD, FSOD
symptoms (genital dryness and irritation)
Estratest ? (tablet)
Solvay Pharmaceuticals, Brussels,Estrogen-testosterone combination
Improves menopausal
Menopausal symptoms,Belgium
symptoms (genital dryness and FSAD, FSDD irritation), heightens libido Testosterone (cream)Off-label use made by compounding Androgen receptor agonist Heighten libido FSDD pharmacies
(Testosterone
Novavax, Inc., Columbia, MD, USA Androgen receptor agonist Heighten libido FSDD [Androsorb ?] cream)(Testosterone [Intrinsa ?]Proctor and Gamble, Cincinnati, OH,Androgen receptor agonist Heighten libido FSDD
patch)
USA
(Testosterone [Tostrelle ?]Cellegy Pharmaceuticals, South San Androgen receptor agonist Heighten libido
FSDD (Tostrex gel for gel)
Francisco, CA, USA
male ED)
EROS-CTD ? (device)UroMetrics, Inc., Anoka, MN, USA Clitoral therapy device Increase sensation and blood FSAD (FDA approved)flow to clitoris via gentle suction Interstim ? Therapy Medtronic, Inc., Minneapolis, MN,Sacral nerve stimulator
Anecdotal evidence of improved FDA approved for (device)
USA
sexual arousal and orgasm
treatment of urinary incontinence; under
investigation for FSAD and FSOD
a The only US FDA approved treatment for female sexual dysfunction is the EROS-CTD ? device. All medications and the InterStim ? therapy device listed are currently under investigation for female sexual dysfunction. Many of the medications listed are used, however, off-label for both male and female sexual dysfunction.b
Tibolone also has progestogenic and androgenic properties.
ED = erectile dysfunction; FSAD = female sexual arousal disorder; FSDD = female sexual desire disorder; FSOD = female sexual orgasmic disorder; PDE5 =phosphodiesterase type 5; PGE 1 = prostaglandin E 1; SSRI = selective serotonin reuptake inhibitor.
Sexual Dysfunction in the Older Woman669 pelvic area whereas PDE1, PDE2, PDE3 and PDE4ed labial and clitoral engorgement in all of the are found in the optic, cardiovascular and gastro-women and 12 of 18 women reported a pleasant esophageal regions.[98] Because it is more specific sensation of warmth. There were no systemic ad-and involves primarily PDE5 inhibition, vardenafil verse effects reported. In a randomised, double-has fewer adverse effects. The only study published blind, placebo-controlled study, 94 women present-to date looking at the use of vardenafil in females ing with female sexual arousal disorder of at least 6 involves the animal (dog) model. In the study, pelvic months duration were given alprostadil cream.[102] nerve electrical stimulation was used to obtain a The women were instructed to apply alprostadil baseline increase in blood flow through the vagina(500, 1000 or 1500g) or a placebo cream to the and clitoris. Intravenous vardenafil was then given,vulvar area prior to vaginal intercourse over a period resulting in a significant increase in blood flow.[99]of 6 weeks. The sexual arousal success rate (as
measured by diary responses to the Female Sexual
10.1.3 Tadalafil
Encounter Profile), was highest in the alprostadil Eli Lilly and Co. (Indianapolis, IN, USA) is
1000g group and lowest in the alprostadil 500g investigating its version of a PDE5 inhibitor drug
group. However, the responses were not different tadalafil. It is reported to stay in the system for up to
from that of the placebo cream, at the p = 0.05 level, 24 hours, thus increasing the opportunity for sponta-
for any of the three alprostadil doses.[102] Nexmed, neity.[100] Tadalafil has been through several ran-
Inc. (Robbinsville, NJ, USA) recently completed domised clinical trials in men and has been ap-
phase II testing of topical alprostadil in preme-proved by the FDA for erectile dysfunction. In one
nopausal women with sexual arousal disorder. randomised, double-blind, placebo-controlled trial
Vivus, Inc. (Mountain View, CA, USA) has also involving 214 premenopausal women with sexual
developed a topical alprostadil cream for sexual arousal disorder, each women received either
arousal disorder that is in phase II trials.
tadalafil 20mg or placebo. The women then used
diary reports and a standardised questionnaire to
10.3 Adrenoceptor Antagonists
record their results. There was no conclusive treat-
ment effect noted (Lilly ICOS, Indianapolis, IN,
USA, unpublished data). Tadalafil is currently un-
10.3.1 Phentolamine
Phentolamine functions as a nonspecific adre-dergoing global phase II trials involving females
noceptor antagonist causing vascular smooth muscle with sexual dysfunction.
relaxation and subsequent vasodilation. The drug
10.2 Prostaglandin E1has been previously studied in men for the treatment
of erectile dysfunction.[103,104] It is available in an
10.2.1 Alprostadil oral and injectable preparation. There are also a few
Alprostadil is a naturally occurring form of the studies looking at phentolamine effects in women. hormone prostaglandin E1 and a potent vasodilator.In one study, 41 women were randomised to four It was approved by the FDA in 1995 for the treat-different treatments, including vaginal solutions of ment of erectile dysfunction in men and is available phentolamine 5mg and 40mg, and an oral tablet of in both injection and intraurethral suppository for-phentolamine 40mg and placebo.[105] Results were ms. Although topical alprostadil has not shown to obtained using vaginal photoplethysmograph and a have significant effects in men with erectile dys-subjective questionnaire. Subjective reports and function, recent studies suggest it may have benefi-physiological measurements were significantly dif-cial effects in women with sexual arousal disorder.ferent from placebo in women using HRT and In one pilot study, 18 women underwent clitoral phentolamine 40mg vaginal solution. Only subjec-colour duplex ultrasonography before and after the tive reports were significantly different in the same application of 0.2% alprostadil gel 1g.[101]A statisti-women using phentolamine 40mg oral tablet. No cally significant difference in the peak systolic ve-significant differences were found among women locity and end diastolic velocity after the application not receiving HRT.[105] In a small pilot study involv-of alprostadil was found. There was also document-ing six postmenopausal women with a complaint of
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
670Walsh & Berman lack of lubrication and sexual arousal difficulties of NitroMed Inc. (Bedford, ME, USA) has devel-at least 6 months, each woman received a single oped NMI870, a nitric oxide-enhanced compound dose of oral phentolamine 40mg and placebo in a of the α2-adrenoceptor antagonist yohimbine. It has single-blind, dose-escalation design. Results indi-undergone phase I and II trials in both men and cated significant changes (p < 0.05) in self-reported women. In a randomised, double-blind, three-way lubrication and pleasurable sensations in the vagina,crossover study (arginine glutamate plus yohimbine, and a mild, positive effect across all measures of yohimbine alone and placebo) the sexual response sexual arousal.[106]of 24 postmenopausal women was measured at 30,
60 and 90 minutes postdrug administration.[113] The
women’s response was measured with a self-report
10.4 Yohimbine
instrument and psychophysiological technique
known as vaginal photoplethysmography. They re-Made from the bark of the Yohimbine tree, this
ported a substantially increased vaginal response to ancient aphrodisiac is an α2-adrenoceptor ant-
the erotic film at 60 minutes postdrug administration agonist, which acts as a vasodilator. For unexplained
with the combination drug compared with placebo. reasons, many patients also report increased libido
There was also improvement in the subjective re-with this drug. In the 1960s, studies were conducted
sponses to the erotic stimuli in the combined treat-using a combination drug called Nux Vomica,
ment group, but no differences between treatment which contained yohimbine and methyltestosterone
groups.[113]
for male erectile dysfunction.[107] Since then, rela-
tively few well designed studies have been complet-
10.6 Neuropeptide and
ed;[108] however, from these studies it can be con-
Adrenoceptor Antagonists
cluded that yohimbine as monotherapy possesses
only modest efficacy. There is increasing evidence
10.6.1 Vasoactive Intestinal Peptide
that the erectogenic action of yohimbine can be
and Phentolamine
augmented by concomitant administration of agents
Senetek (Napa, CA, USA) has developed In-that augment the release and/or action of nitric oxide
vicorp?, a combination injection therapy compris-in the corpus cavernosum. A recent study of yohim-
ing vasoactive intestinal peptide and phentolamine. bine use in women with SSRI-induced sexual dys-
Vasoactive intestinal peptide is a 28-amino acid function found no differences between yohimbine
peptide found naturally in the male and female uro-and placebo in improvement of symptoms.[109]
genital tracts, as well as in the central and peripheral
nervous systems. Vasoactive intestinal peptide has
10.5 Prostaglandin E1 and been shown to successfully stimulate erection in
Adrenoceptor Antagonist males.[114] It works by binding to smooth muscle
receptors in the corpus cavernosum, inducing
10.5.1 Arginine and Yohimbine smooth muscle relaxation and increased blood flow.
Arginine is an amino acid precursor to the forma-Phase I studies are now being completed using the tion of nitric oxide. Increased levels of nitric oxide female animal model.
promote the relaxation of vascular and nonvascular
smooth muscle. Preliminary studies in men with10.7 Dopamine Receptor Agonists
erectile dysfunction are promising.[110,111] Arginine
is sold in health food stores, often in combination
10.7.1 Apomorphine
with different herbal supplements, for the treatment Apomorphine is a short-acting dopamine recep-of sexual arousal disorder (e.g. ArginMax?, The tor agonist with affinity for dopamine D2 receptor Daily Wellness company, Sunnyvale, CA, USA). A sites, within the brain known to be involved in recent double-blind placebo controlled study in fe-sexual function. It is suggested that dopamine can males found a significant improvement in overall trigger penile erection by acting on oxytocinergic sexual satisfaction in women using ArginMax?neurons located in the paraventricular nucleus of the compared with placebo.[112]hypothalamus and perhaps on the pro-erectile sacral
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman671 parasympathetic nucleus within the spinal cord.[115]10.10 Selective Androgen
In Europe, TAP Pharmaceutical Products Inc. (Lake Receptor Modulators
Forest, IL, USA) introduced a sublingual apomor-
A novel approach to the treatment of osteo-phine (Uprima?) that has recently been approved
porosis in men, and possibly women, is the develop-for the treatment of erectile dysfunction. To date,
ment of selective androgen receptor modulators published reports on the effects of apomorphine on
(SARMS). Preliminary research indicates that the female sexual response involve only animal
SARMS can stimulate formation of new bone with models.
substantially diminished proliferative activity in the
prostate, as well as having reduced virilising activity
10.8 α-Melanocyte Stimulating Hormone
in women. The discovery of SARMS offers new
10.8.1 PT141therapeutic approaches for both male and female
Palatin Technologies, Inc. (Cranbury, NJ, USA)hormone replacement. SARMS provide the oppor-is currently investigating a centrally acting drug,tunity to design molecules that target the androgen PT141. This drug is a peptide analogue of the receptor in different tissues in order to elicit a de-neuropeptide hormone α-melanocyte stimulating sired effect, such as maintaining or restoring libi-hormone. It is thought to act by stimulating the do.[119]
melanocortin-4 receptors in the brain which play a
role in several behaviours, including appetite and
10.11 Selective Estrogen
sexual arousal.[116] As a result, it may offer signif-
Receptor Modulators
icant safety and efficacy benefits over currently
Selective estrogen receptor modulators (SERMS) available products. PT141 is currently undergoing
are compounds that bind with estrogen receptors and phase I trials in females and phase II trials in males.
exhibit estrogen action in some tissues and anti-
estrogen action in other tissues. SERMS are used in
10.9 Serotonin 5-HT Receptor Agonists
postmenopausal women as an alternative to estrogen
10.9.1 Flibanserin and VML670replacement. Currently FDA approved SERMS in
The most widely prescribed class of antidepres-the US include tamoxifen (breast cancer) and ralox-sant drugs is the SSRIs. They cause an increase in ifene (osteoporosis).[120] The remaining SERMS in-circulating levels of serotonin, a chemical produced clude tibolone, lasofoxifene, droloxifene and idox-in the brain that affects mood. Although the SSRIs ifene. Several SERMS are now in phase I, II and III may prove to be beneficial for many people with trials for female sexual dysfunction. depression, one of the adverse effects of the med-
ication is sexual dysfunction. It is estimated that
10.12 Synthetic Steroids
between 30% and 40% of individuals taking SSRIs
experience some form of sexual dysfunction that10.12.1 Tibolone
may include a loss of sexual desire, erectile dysfunc-Tibolone is a synthetic steroid that has been tion or an inability to achieve an orgasm.[117]licensed for use in Europe and Asia for the manage-SSRIs reduce the activity of the serotonin ment of climacteric symptoms and the prevention of 5-HT1A receptor, which is known to be involved in osteoporosis. Recent evidence suggests that tibolone the mediation of sexual behaviour. It is hypothesised may also help improve mood and libido in postmen-that if individuals who experience sexual dysfunc-opausal women. Tibolone has progestogenic and tion secondary to SSRIs are given a 5-HT1A receptor androgenic properties, as well as estrogenic effects. agonist (e.g. flibanserin or VML670; Vernalis It has been described as a prodrug because, once Group plc, Winnersh, UK), which has potent and ingested, it is quickly metabolised to two estrogenic selective activity for the 5-HT1A receptors, it can metabolites, 3α and 3β, both of which become ac-reactivate these receptors and possibly restore nor-tive when desulfated by the sulfatase enzyme in the mal sexual function.[118] These medications are cur-target tissues. Tibolone and its metabolite 3β may rently in phase II trials.also be converted to a Δ 4-isomer that can bind and
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
672Walsh & Berman transactivate progesterone and androgen receptors,Those women without sexual arousal symptoms al-
thus exerting both progestogenic and androgenic so reported similar changes.[126] Although FDA ap-
effects.[121] Tibolone has also been found to increase proved, further long-term studies with EROS-
circulating free testosterone and lower SHBG levels,CTD? need to be completed.
further increasing its androgenic effects.[122] Several
randomised, placebo-controlled studies of tibolone
10.13.2 InterStim? Therapy
InterStim? (Medtronic, Inc., Minneapolis, MN, in women have reported improvement in sexual
USA) therapy involves mild neurostimulation of the desire. In one study, 28 postmenopausal women
sacral nerve. It was designed to treat urinary inconti-were randomised to receive either tibolone 2.5mg
nence. The therapy involves placing a lead in the daily or placebo for a total of 1 year. At baseline,
region of S2–S4 spinal segments. Many women who and throughout the year, the women completed sex-
have undergone this procedure have anecdotally ual function questionnaires. Results demonstrated
reported that their sexual arousal and ability to an overall improvement in sexual desire in the
achieve orgasm increased. More retrospective and tibolone group compared with those taking place-
prospective research testing of this device for orgas-bo.[123] In another similarly designed study, 38 post-
mic improvement is currently underway. menopausal women were randomised to tibolone
2.5mg daily or placebo for 3 months. Data were
collected using vaginal photoplethysmograph and11. Conclusion
sexual function questionnaires. Tibolone was asso-
ciated with significant increases in sexual desire and Female sexual dysfunction is a multifactorial
the frequency of arousability and sexual fantasies medical problem. Evaluation of the patient should
compared with placebo.[124] In a larger 48-week include a comprehensive and collaborative effort
multicentre trial, which included 437 postmenopau-between a physician and psychologist. Although
sal women, comparing treatment with either there are physiological similarities between males
tibolone 2.5mg or estradiol 2mg plus norethisterone and females, the complexity of female sexual dys-
acetate. Both groups demonstrated overall improve-function remains distinct from that of a man. The
ment in their scores, although when tibolone was context in which a woman experiences her sexuali-
compared with estradiol plus norethisterone acetate ty, regardless of age, is equally, if not more impor-
significantly higher scores were found for the items tant than the physiologic outcome she experiences.
assessing ‘frequency’, ‘satisfaction’ and ‘enjoy-It is imperative that issues regarding how a woman
ment’.[125]views her sexuality be addressed before beginning
medical therapy or determining treatment efficacies.
10.13 Medical Devices There is a need for the development of well or-
ganised, randomised, controlled studies on the most
appropriate assessment and successful intervention
10.13.1 EROS-CTD?
for sexual dysfunction in women. Investigational EROS-CTD? (UroMetrics, Inc., Anoka, MN,
drugs and devices may play a small, but crucial role USA) is the first FDA-approved treatment on the
in the search for safe and effective treatment op-market for sexual arousal and orgasmic disorders in
tions.
women. It is a small, hand-held medical device that
works by applying a gentle vacuum to the clitoris,
increasing blood flow to the clitoris and surrounding Acknowledgements
tissue. In one clinical trial, 19 women (ten with
symptoms of sexual arousal disorder and nine with-Dr Kathleen Walsh has no conflicts of interest or sources
of funding that are directly relevant to this view. Dr Jennifer out) were instructed in the use of the device at home.
Berman has consultancy agreements and/or is a member of The women then completed the Female Intervention
the speakers bureau of the following companies: Qualilife Efficacy Index on a weekly basis. Results demon-Pharmaceuticals; Cellegy Pharmaceuticals; Auxilium; Warn-
strated an overall improvement in all symptoms in er Health Care; Ortho-McNeil Pharmaceutical, Inc.; Pfizer,
women with sexual arousal disorder (p<0.05).Inc.; and Vivus, Inc.
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
Sexual Dysfunction in the Older Woman673
26.Impett EA, Peplau LA. Sexual compliance: gender, motivation-
References
al, and relationship perspectives. J Sex Res 2003 Feb; 40 (1): 1.Bortz II WM, Wallace DH. Physical fitness, aging, and sexuali-87-100
ty. West J Med 1999 Mar; 170 (3): 167-9
27.Basson R. A model of women’s sexual arousal. J Sex Marital 2.Gelfand MM. Secuality among older women. J Womens Health Ther 2002 Jan-Feb; 28 (1): 1-10
Gend Based Med 2000; 9 Suppl. 1: S15-20
28.Barton D, Joubert L. Psychosocial aspects of sexual disorders.
3.Matthias RE, Lubben JE, Atchison KA. Sexual activity and Aust Fam Physician 2000 Jun; 29 (6): 527-31
satisfaction among very old adults: results from a community-29.Mah K, Binik YM. The nature of human orgasm: a critical dwelling medicare population survey. Gerontologist 1997; 37:review of major trends. Clin Psychol Rev 2001 Aug; 21 (6): 6-14823-56
https://www.doczj.com/doc/512379057.html, Bureau of the Census. Projections of the population of the30.Goodlin RC. Orgasm is the thing! Am J Obstet Gynecol 1994
United States: 1977 to 2050. In: Current population reports.Jul; 171 (1): 282-3
Washington, DC: Government Printing Office 1995: P25-704
31.Pierce AP. The coital alignment technique (CAT): an overview https://www.doczj.com/doc/512379057.html, Bureau of the Census. Current population reports, special of studies. J Sex Marital Ther 2000 Jul-Sep; 26 (3): 257-68
studies: 65+ in the United States. Washington, DC: Govern-
32.Mah K, Binik YM. Do all orgasms feel alike? Evaluating a two-
ment Printing Office, 1996: P23-190
dimensional model of the orgasm experience across gender 6.Kinsey AC, Pomeroy WB, Martin CE. Sexual behavior in the and sexual context. J Sex Res 2002 May; 39 (2): 104-13
human male. Philadelphia (PA): WB Saunders, 1953
33.Kelly MP, Strassberg DS, Kircher JR. Attitudinal and experien-7.Masters WH, Johnson VE. Human sexual response. Boston tial correlates of anorgasmia. Arch Sex Behav 1990 Apr; 19
(MA): Little, Brown and Company, 1966(2): 165-77
8.Pfeiffer E, Verwoerdt A, Wang HS. Sexual behavior in aged34.Pauls RN, Berman JR. Impact of pelvic floor disorders and
men and women. Arch Gen Psychiatry 1968; 19: 735-58prolapse on female sexual function and response. Urol Clin 9.Christenson CV, Gagnon JH. Sexual behavior in a group of North Am 2002 Aug; 29 (3): 677-83
older women. J Gerontol 1965; 20: 351-635.Salonia A, Zanni G, Nappi RE, et al. Sexual dysfunction is 10.George LK, Weiler SJ. Sexuality in middle and late life. Arch common in women with lower urinary tract symptoms and
Gen Psychiatry 1981; 38: 919-23urinary incontinence: results of a cross-sectional study. Eur 11.Bretschneider JG, McCoy NL. Sexual interest and behavior in Urol 2004 May; 45 (5): 642-8
healthy 80 to 102 year olds. Arch Sex Behav 1988; 17: 109-2936.Bidmead J, Cardozo LD. Pelvic floor changes in the older 12.Janus SS, Janus CL. The Janus report on sexual behavior. New woman. Br J Urol 1998 Dec; 82 Suppl. 1: 18-25
York: John Wiley & Sons, 199337.Graziottin A. Etiology and diagnosis of coital pain. J Endocrinol 13.Starr BD, Weiner MB. The Starr-Weiner report on sex and Invest 2003; 26 (3 Suppl.): 115-21
sexuality in mature years. Briarcliff Manor (NY): Stein and38.Fry RP, Crisp AH, Beard RW. Sociopsychological factors in Day, 1981chronic pelvic pain, a review. J Psychosom Res 1997 Jan; 42 14.Diokno AC, Brown MB, Herzog AR. Sexual function in the(1): 1-15
elderly. Arch Intern Med 1990; 150: 197-20039.Masters EH, Johnson VE. Human sexual response. Boston 15.Marsiglio W, Donnelly D. Sexual relations in later life: a(MA): Little, Brown and Company, 1966
national study of married persons. J Gerontol 1991; 46:40.Kaplan HS. The new sex therapy. London: Bailliere Tindall, S338-3441974
16.Croft LH. Sexuality in later life: a counseling guide for physi-41.Basson R. Using a different model for female sexual response to
cians. Boston (MA): John Wright–PSG, 1982address women’s problematic low sexual desire. J Sex Marital
Ther 2001 Oct-Dec; 27 (5): 395-403
17.Mooradian AD, Greiff V. Sexuality in older women. Ach Intern
Med 1990; 150: 1033-842.Davison SL, Davis SR. Androgens in women. J Steroid Bio-
chem Mol Biol 2003 Jun; 85 (2-5): 363-6
https://www.doczj.com/doc/512379057.html,umann EO, Paik A, Rosen RC. Sexual dysfunction in the
United States: prevalence and predictors. JAMA 1999; 281:43.Burger HG. Androgen production in women. Fertil Steril 2002 537-44Apr; 77 Suppl. 4: 3-5
19.Sarrel PM, Whitehead MI. Sex and menopause: defining the44.Hutchison JB, Steimer TH. Preoptic formation of 17β oestradiol
issues. Maturitas 1985 Sep; 7 (3): 217-24is influenced by behavioural stimuli in the dove. Brain Res
1985; 360: 366-9
20.Rosen RC, Taylor JF, Leiblum SR, et al. Prevalence of sexual
dysfunction in women: results of a survey study of 329 women45.Katz S, Morales AJ. Dehydroepiandrosterone (DHEA) and in an outpatient gynecological clinic. J Sex Marital Ther 1993;DHEA-sulphate (DHEAS) as therapeutic options in meno-19: 171-88pause. Semin Reprod Endocrinol 1998; 16: 161-70
21.Sarrel PM. Sexuality and menopause. Obstet Gynecol 1990 Apr;46.Rako S. The hormone of desire: the truth about testosterone,
75 (4 Suppl.): 26-S30sexuality and menopause. New York: Three Rivers Press, 1999 22.Basson R, Berman J, Burnett A, et al. Report of the internation-47.Sherwin BB, Gelfand MM. Differential symptom response to
al consensus development conference on female sexual dys-parental estrogen and androgen in the surgical menopause. Am function: definitions and classifications. J Urol 2000; 183:J Obstet Gynecol 1985; 151: 153-60
888-9348.Marin R, Escrig A, Abreu P, et al. Androgen-dependent nitric 23.Bachmann GA, Leiblum SR. The impact of hormones on meno-oxide release in rat penis correlates with levels of constitutive
pausal sexuality: a literature review. Menopause 2004 Jan-Feb;nitric oxide synthase isoenzymes. Biol Reprod 1999; 61:
11 (1): 120-301012-6
24.Warnock JK, Bundren JC, Morris DW. Female hypoactive49.Rittmaster RS. Clinical relevance of testosterone and
sexual desire disorder due to androgen deficiency: clinical and dihydrotestosterone metabolism in women. Am J Med 1995;
psychometric issues. Psychopharmacol Bull 1997; 33 (4):98 Suppl. 1A: 17-21
761-650.Burger HG, Dudley EC, Hopper JL, et al. The endocrinology of 25.Segraves RT. Female sexual disorders: psychiatric aspects. Can menopausal transition: a cross-sectional study of population-
J Psychiatry 2002 Jun; 47 (5): 419-25based sample. J Clin Endocrinol Metab 1995; 80: 3537-47
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)
674Walsh & Berman
51.Davis SR, Burger HG. Androgens and the postmenopausal72.Reissing ED, Binik YM, Khalife S, et al. Vaginal spasm, pain,
woman. J Clin Endocrinol Metab 1996; 81: 2759-64and behavior: an empirical investigation of the diagnosis of
vaginismus. Arch Sex Behav 2004 Feb; 33 (1): 5-17
52.Simpson ER, Davis SR. Minireview: aromatase and the regula-
73.Meston CM. The psychophysiological assessment of female
tion of estrogen biosynthesis: some new perspectives. Endocri-
sexual function. American Association of Sex Educators, nology 2001 Nov; 142 (11): 4589-94
Counselors, and Therapists, Inc. (AASECT). J Sex Educ Ther 53.Sarrel P, Dobay B, Wiita B. Estrogen and estrogen-androgen
2000; 25 (1): 6-16
replacement in postmenopausal women dissatisfied with es-
74.Aksaray G, Yelken B, Kaptanoglu C, et al. Sexuality in women
trogen-only therapy: sexual behavior and neuroendocrine res-
with obsessive compulsive disorder. J Sex Marital Ther 2001;
ponse. J Reprod Med 1998 Oct; 43 (10): 847-56
27 (3): 273-7
54.Sarrel PM. Ovarian hormones and vaginal blood flow: using
75.Clayton AH. Recognition and assessment of sexual dysfunction
laser Doppler velocimetry to measure effects in a clinical trial
associated with depression. J Clin Psychiatry 2001; 62 Suppl.
of post-menopausal women. Int J Impot Res 1998; 10: S91-3
3: 5-9
55.Caillouette JC, Sharp Jr CF, Zimmerman GJ, et al. Vaginal pH
76.Woosley RL, Flockhart D. A case for the development of
as a marker for bacterial pathogens and menopausal status. Am
Centers for Education and Research in Therapeutics (CERT).
J Obstet Gynecol 1997; 176 (6): 1270-5
Pharmacy Week 1995; 4 (23): 1-3
56.Sarrel PM. Sexuality and menopause. Obstet Gynecol 1990; 75
77.Finger WW, Lund M, Slagle MA. Medications that may con-
Suppl. 4: 26-30S
tribute to sexual disorders: a guide to assessment and treatment 57.Wyckoff MH, Chambliss KL, Mineo C, et al. Plasma mem-
in family practice. J Fam Pract 1997 Jan; 44 (1): 33-43 brane estrogen receptors are coupled to endothelial nitric-
78.Shifren JL. The role of androgens in female sexual dysfunction.
oxide synthase through Galpha(i). J Biol Chem 2001; 276:
Mayo Clin Proc 2004 Apr; 79 (4 Suppl.): S19-24 27071-6
79.Davis S. Testosterone deficiency in women. J Reprod Med 2001 58.Berman JR, McCarthy MM, Kyprianou N. Effect of estrogen
Mar; 46 (3 Suppl.): 291-6
withdrawal on nitric oxide synthase expression and apoptosis
80.Collins A, Landgren BM. Reproductive health, use of estrogen
in the rat vagina. Urology 1998; 51: 650-6
and experience of symptoms in postmenopausal women: a 59.Benet AE, Melman A. The epidemiology of erectile dysfunc-
population based study. Maturitas 1994; 20 (2): 101-11 tion. Urol Clin North Am 1995; 22: 699-709
81.Burkman RT, Collins JA, Greene RA. Current perspectives on 60.Kaiser FE, Korenman SG. Impotence in diabetic men. Am J
benefits and risks of hormone replacement therapy. Am J Med 1988; 85: 147-52
Obstet Gynecol 2001 Aug; 185 2 Suppl.: S13-23
61.Morley JE, Korenman SG, Kaiser FE, et al. Relationship of82.Wells G, Herrington DM. The Heart and Estrogen/Progestin
penile brachial pressure index to myocardial infarction and Replacement Study: what have we learned and what questions cerebrovascular accidents in older men. Am J Med 1988; 84:remain? Drugs Aging 1999 Dec; 15 (6): 419-22
445-8
83.Manson JE, Hsia J, Johnson KC, et al. Estrogen plus progestin 62.Park K, Goldstein I, Andry C, et al. Vasculogenic female sexual and the risk of coronary heart disease. N Engl J Med 2003 Aug
dysfunction: the hemodynamic basis for vaginal engorgement7; 349 (6): 523-34
insufficiency and clitoral erectile insufficiency. Int J Impot Res
84.Nelson HD, Humphrey LL, Nygren P, et al. Postmenopausal
1997 Mar; 9 (1): 27-37
hormone replacement therapy: scientific review. JAMA 2002 63.Goldstein I, Berman JR. Vasculogenic female sexual dysfunc-Aug 21; 288 (7): 872-81
tion: vaginal engorgement and clitoral erectile insufficiency85.Montgomery JC, Appleby L, Brincat M, et al. Effect of oes-syndromes. Int J Impot Res 1998; 10 Suppl. 2: S84-90trogen and testosterone implants on psychological disorders in 64.Manonai J, Theppisai U, Suthutvoravut S, et al. The effect of the climacteric. Lancet 1987; I: 297-9
estradiol vaginal tablet and conjugated estrogen cream on86.Shifren JL, Braunstein GD, Simon JA, et al. Transdermal urogenital symptoms in postmenopausal women: a compara-testosterone treatment in women with impaired sexual function tive study. J Obstet Gynaecol Res 2001 Oct; 27 (5): 255-60after oophorectomy. N Engl J Med 2000; 343: 682-8
65.Robinson D, Cardozo LD. The role of estrogens in female lower87.Davis SR, Tran J. Testosterone influences libido and well being
urinary tract dysfunction. Urology 2003 Oct; 62 (4 Suppl. 1):in women. Trends Endocrinol Metab 2001; 12: 33-7
45-51
88.Mazer NA. New clinical applications of transdermal testoster-66.Sherwin BB, Gelfand MM, Brender W. Androgen enhances one delivery in men and women. J Control Release 2000; 65:
sexual motivation in females: a prospective, crossover study of303-15
sex steroid administration in the surgical menopause. Psycho-89.Berman LA, Berman JR, Chhabra S, et al. Novel approaches to som Med 1985; 47: 339-51female sexual dysfunction. Expert Opin Investig Drugs 2001 67.Sipski ML, Alexander CJ, Rosen RC. Sexual response in Jan; 10 (1): 85-95
women with spinal cord injuries: implications for our under-90.Rako S. Testosterone supplemental therapy after hysterectomy standing of the able-bodied. J Sex Marital Ther 1999; 25:with or without concomitant oophorectomy: estrogen alone is 11-22not enough. J Womens Health Gend Based Med 2000; 9: 17-23 68.Sipski ML. Sexual response in women with spinal cord injury:91.Basson R, McInnes R, Smith MD, et al. Efficacy and safety of
neurologic pathways and recommendations for the use of sildenafil citrate in women with sexual dysfunction associated electrical stimulation. J Spinal Cord Med 2001; 24 (3): 155-8with female sexual arousal disorder. J Womens Health Gend 69.Le Mone P. The physical effects of diabetes on sexuality in Based Med 2002 May; 11 (4): 367-77
women. Diabetes Educ 1996; 22 (4): 361-692.Caruso S, Intelisano G, Lupo L, et al. Premenopausal women 70.Sarkadi A, Rosenqvist U. Contradictions in the medical encoun-affected by sexual arousal disorder treated with sildenafil: a
ter: female sexual dysfunction in primary care contacts. Fam double-blind, cross-over, placebo-controlled study. BJOG Pract 2001; 18 (2): 161-62001 Jun; 108 (6): 623-8
71.Shafik A, El-Sibai O. Study of the pelvic floor muscels in93.Kaplan SA, Reis RB, Kohn IJ, et al. Safety and efficacy of
vaginismus: a concept of pathogenesis. Eur J Obstet Gynecol sildenafil in postmenopausal women with sexual dysfunction.
Reprod Biol 2002 Oct 10; 105 (1): 67-70Urology 1999 Mar; 53 (3): 481-6
? 2004 Adis Data Information BV. All rights reserved.Drugs Aging 2004; 21 (10)